Submitted:
03 May 2026
Posted:
05 May 2026
You are already at the latest version
Abstract
BACKGROUND For patients with multivessel coronary artery disease (MVD) treated with coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI), we proposed novel pulmonary risk factors identified by machine learning (ML) that have impact on long-term revascularization outcomes.
METHODS A total of 1035 consecutive patients with three-vessel disease (3-VD) and/or left main disease (LMD) treated with either CABG or PCI were followed up to 5 years in tertiary cardiovascular care centre that systematically screened their candidates for revascularization. Participants were stratified for the presence of absence of PH (pulmonary hypertension) and /or chronic obstructive pulmonary disease (COPD), and the impact of each on revascularization outcomes was examined.
RESULTS Five-year mortality in overall cohort was 12.6%. A higher mortality was demonstrated for patients with diagnosis of COPD or PH (n=125) as compared with population who had neither COPD nor PH (n=910) [68.8% vs 4.8%, P< 0.001]. Among the 125 patients in COPD/PH population, a higher 5-year mortality was observed in those who underwent surgery as compared with PCI-group (85.2% vs 64.3%, P=0.04). We observed a significant interaction between COPD and revascularization strategy (P=0.014), but no association between PH and CABG/PCI was found. Cox regression analysis showed outstanding HRs of mortality for PH (6.01 [3.47-10.40]) and COPD (5.65 [3.21-9.96]) as compared with conventional risk factors.
CONCLUSIONS In the overall cohort, novel pulmonary risk factors suggested by ML had a huge impact on 5-year mortality, hence a detailed diagnosis of pulmonary disease in the population with MVD has a paramount importance to predict long-term mortality.
Keywords:
chronic migraine
; Alzheimerʹs dementia
; cortical spreading depression
; glymphatic system
; brain insulin resistance
; TNF-alpha
; Mendelian randomisation
; CGRP
; feed-forward hypothesis
Highlights
- Patients with severe coronary artery disease (CAD) and concomitant chronic obstructive pulmonary disease (COPD) or pulmonary hypertension (PH) have a higher risk of major adverse cardiac and cerebrovascular events (MACCE) than those with CAD without pulmonary disease.
- Despite high prevalence and clinical importance, there is a paucity of data regarding the impact of COPD and PH on the outcomes of multivessel coronary artery disease (MVD) interventional treatment.
- Using machine learning approach, we demonstrated pulmonary factors associated with adverse outcome after revascularization using coronary artery bypass grafting or percutaneous coronary intervention for the treatment of MVD.
Background
The World Health Organization (WHO) estimates that in 2019 the leading causes of death worldwide were respectively ischaemic heart disease (IHD), stroke and chronic obstructive pulmonary disease (COPD). Coronary artery disease (CAD), which constitutes the vast majority of IHD was responsible for 16% and COPD for 15.8% of total deaths worldwide, which are responsible for over 12 million of deaths yearly. Moreover, COPD and IHD are the most frequent causes of disability in Poland in 2019 (first and ninth place according to WHO estimation, respectively) measured by disability-adjusted life years (DALYs) rate, which totalled 4565.27 per 100 000 population for IHD and 821.16 per 100 000 population for COPD [1].
Coronary artery disease (CAD) is a disease characterized by progressive atherosclerosis in coronary arteries that leads to a reduction of blood flow and thus myocardial ischemia [2,3]. Diffused pattern of atherosclerosis, which is often present in multivessel coronary artery disease (MVD), results in a worse prognosis and high risk of death (over 3% per year) [4,5]. In this specific group of patients, revascularization with the use of percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG), completeness of revascularization is an important prognostic factor [3,6,7]. In severe CAD, including MVD, both PCI and CABG are recommended for revascularization by ESC and AHA to improve prognosis and reduce symptoms of CAD. The choice of the method of revascularization for MVD-patients, is often complex. Hence, the European Society of Cardiology (ESC) and American Heart Association (AHA) strongly recommend to consult MVD-patients within highly experienced multidisciplinary Heart Team (HT) consisting of noninvasive and interventional cardiologists, imaging specialists as well as cardiac surgeons [6,7]. The HT approach has been proven to have good replicability and positive influence of further treatment outcomes [8].
The choice between these two strategies made by the HT is based on careful evaluation of risk and benefits of each one [7]. ESC and AHA recommend implementing dedicated methods to estimate the perioperative risk of mortality based on preprocedural clinical, angiographic and echocardiographic characteristics, Society of Thoracic Surgeons (STS) risk score and European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) scale being the most commonly used.
However, the decision regarding optimal treatment strategy should not be only based on scales. The clinical characteristics of patients such as concomitant diseases, frailty, active cancer or patient preference should also be take into account. Despite the advancements in surgical and transcatheter techniques, MVD treatment outcomes remain poor. The 5-year mortality is around 12% according to various registries [9,10]. Better understanding of the prognostic factors associated with MVD could improve the qualification process and patient outcomes. The new method used successfully in search for new mortality predictors is a machine learning approach [11]. Previously, we had demonstrated that chronic obstructive pulmonary disease (COPD), pulmonary hypertension (PH) and insulin-dependent diabetes are the risk factors that strongly influenced long-term mortality in patients with severe CAD. In this article, we would like to assess the impact of novel pulmonary factors – COPD and PH on outcomes of real-life MVD-patients who underwent revascularization following HT evaluation. We know from clinical practice that pulmonary diseases as COPD and PH commonly coexist with CAD [12,13,14]. Moreover, COPD is associated with the complexity of CAD [14]. Nevertheless, guidelines for the optimal management of MVD-patients with concomitant pulmonary disease are still not well established, and data regarding the selection of optimal treatment approach – surgery or PCI for these vulnerable cohort remains scarce, asking for more evidence.
Objectives
In this retrospective cohort study we wanted to determine the pulmonary risk factor associated with worse outcome in patients with multivessel coronary artery disease.
Patients and Methods
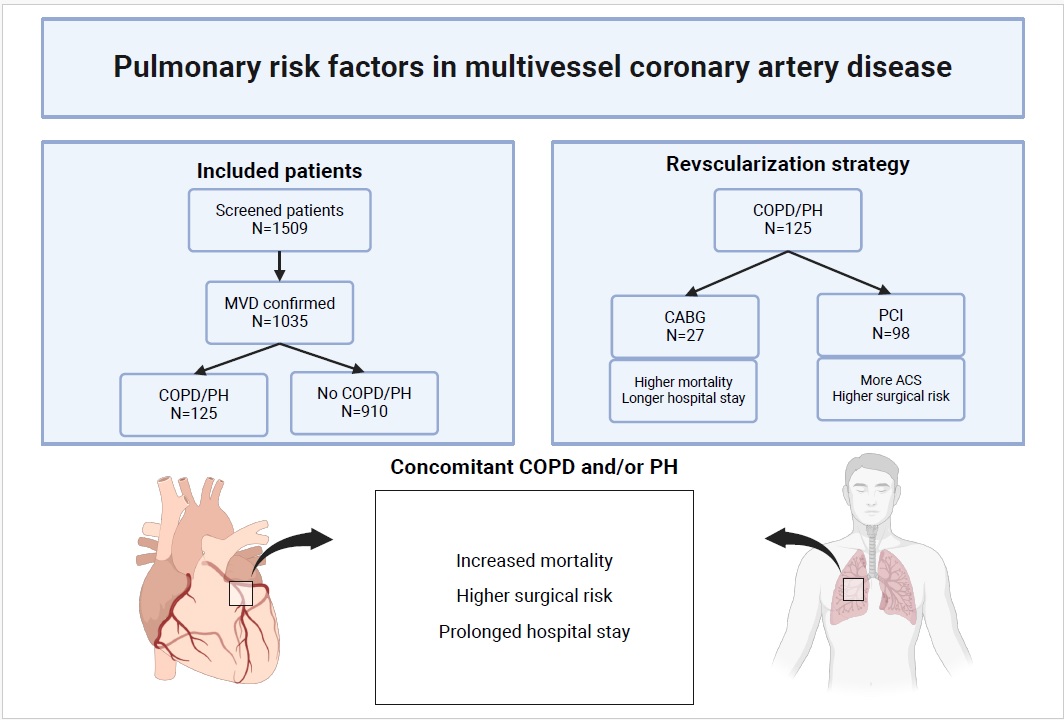
The overall study plan and detailed methods have already been described precisely earlier [15]. Summarizing, from 2016 to 2019, 1509 individuals with severe CAD were presented during 176 HT consultations in our department, a large tertiary cardiovascular care center in Poland. We included patients above 18 years of age with complete clinical, echocardiographic and angiographic characteristics. The exclusion criteria were: pregnancy or lactation at baseline, known disseminated neoplastic process, a life expectancy not exceeding 1 year and a lack of informed, written consent. The severe CAD was defined as three-vessel disease (3-VD) and/or left main disease (LMD). All presented patients have undergone evaluation in a weekly multidisciplinary HT consultations and qualified for revascularization with either CABG or PCI with subsequent optimal medical therapy (OMT) or OMT alone. Out of a total population, a final analysis was performed for 1035 patients that were diagnosed with severe CAD based on angiography criteria and qualified after HT discussion to invasive revascularization strategy – CABG or PCI. In the analyzed population 125 (12.1%) individuals presented with diagnosis of COPH or PH, while 910 (87.9%) had no confirmed pulmonary disease – neither COPD nor PH. In all patients COPD was confirmed with spirometry using FEV1/FVC (forced expiratory volume in 1 second/forced vital capacity) < 0.7 after inhalation of bronchodilatator as a diagnostic criterium. Frailty scale was defined using clinical frailty scale in Rockwood Frailty Scale. They presented with symptoms of chronic airways obstruction requiring long-term use of bronchodilatators or steroids. PH was defined as a pulmonary artery systolic pressure (PASP) of above 55 mmHg measured using echocardiography, which corresponds to high PH echocardiographic possibility. Out of an overall cohort of MVD-patients with COPD/PH, one fifth were qualified and had performed CABG (27 (21.6%)), while 98 (78.4%) were treated percutaneously. All of the patient that have undergone invasive treatment with CABG or PCI were followed with OMT defined as using of drugs with proven impact on survival or reducing symptoms of CAD. The pharmacotherapy included treatment with aspirin or dual antiplatelet therapy (DAPT) combined with angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs) and beta-blockers (BB), statins and/or aldosterone antagonists. The definitions of concomitant diseases that were used in our study, such as chronic kidney disease (CKD), anemia, 3-VD and LMD were described previously [9,15]. The primary endpoint used in our study was an all-cause death. The secondary endpoints were defined as major adverse cardiac or cerebrovascular events (MACCE) [including overall mortality, stroke, myocardial infarction (MI), or repeat revascularization (RR)] as well as the separate components of MACCE. Secondary endpoints have been stated using commonly available and used definitions – MI was defined using Fourth Universal Definition of Myocardial Infarction, stroke as clinical signs of local or global disturbance of cerebral function, lasting more than 24 hours or leading to death, with no evident cause other than of vascular origin, while RR as repeat PCI or bypass graft placement for restenosis at the lesion treated during baseline revascularization. The main outline of the study was presented in Figure 1. The protocol for this study has been approved by the Medical University of Warsaw. An informed consent was obtained from all participating subjects or their legal guardians.
Statistical Analysis
For all statistical analysis the PQStat software (version 1.6.6, PQStat, Poznań, Poland) was used. The normality of distribution for continuous variables was confirmed with the Shapiro–Wilk test. Normally distributed variables are presented as mean ± standard deviation (SD), whereas non-normally distributed variables are presented as the median and interquartile range (IQR). Comparisons between groups were performed using the Pearson’s Chi-squared test for categorical variables, and Student’s t test or Mann-Whitney U test for unpaired continuous variables, and Wilcoxon rank-sum test for paired variables, according to data distribution. Cox regression analysis was used to calculate hazard ratios (HRs) with 95% confidence intervals (95% CI) for risk factors associated with increased mortality. We used a log-rank test for survival analysis to compare Kaplan-Meier survival curves. The proportional hazards assumption was verified via visual inspection of Kaplan-Meier curves for crossing. Variance Inflation Factor (VIF) was used to detect multicollinearity among predictor variables. Variables with VIF values less than 5 are considered acceptable. Survival curves were estimated using the Kaplan–Meier method, and differences in survival between groups were assessed using the log-rank test.
All the statistical significance (p) were given with an accuracy of 2 decimal places; however, if p was less than 0.01, we use the expression “p < 0.01”. p value lower than 0.05 were considered statistically significant. Based on a sample-size calculation, inclusion of 1.033 patients provides 80% power to detect an absolute difference of 11.2% in mortality at a two-sided α = 0.05.
We used the RMSEA (Root Mean Square Error of Approximation) with the result 0.06 and SRMR (Standardized Root Mean Square Residual) with the result 0.04, both indicating a good fit. For multivariate models we used Henze-Zirkler test.
In addition to traditional regression models, machine learning algorithms were employed to enhance predictive robustness and handle potential non-linearities in the dataset. This dual approach follows Recommendations for Reporting Machine Learning Analyses by providing a clear rationale for ML use when it offers marked advantages over standard statistical methods, such as improved model interpretability or the ability to process high-dimensional ‘big data’ without prior rules-based assumptions.
Results
Overall study population
From January 2016 to December 2019 during 176 HT meetings, a total number of 1035 patients with MVD (3-VD or/and LM disease) were qualified after HT evaluation to invasive treatment (CABG or PCI) and subsequent OMT. These patients were followed up for a mean (SD) of 60 (21) months. The mean (SD) age of overall cohort was 68.2 (9.9) years. There was a higher number of men compared to women – 75.7% were men. Pulmonary disease – COPD or/and PH were diagnosed in 125 (12.1%) patients, while 910 (87.9%) had no COPD or PH. Patients in the two cohorts were well balanced with regard to most of the baseline demographic and clinical characteristics – Table 1. Smoking was more frequent in COPD/PH group (78.4% vs 10.9% in non COPD/PH cohort, p<0.01). The patients presented with a surgical risk measured by EuroSCORE II [European System for Cardiac Operative Risk Evaluation II] and STS [Society of Thoracic Surgeons] score (median, Q1-Q3) of 5 (4-9) and 3 (2-4), respectively and was higher in COPD/PH cohort (median, Q1-Q3) [EuroSCORE II: 8 (4-10) vs 5 (3-6)) for non-COPD/PH group; STS score: 5 (3-6) vs 3 (2-4) for non-COPD/PH group, p<0.001]. The median (Q1-Q3) age in COPD/PH cohort was 67 (64-68) years, 76.8% were male and 13.6% presented with frailty syndrome. Approximately one third of these patients had been diagnosed with diabetes before index time, of whom about one third required treatment with insulin. The most prevalent concomitant diseases were hypertension, dyslipidemia and HF and their prevalence was relatively high in overall cohort – 83.9%, 81.2% and 70.9%, respectively. The left-ventricular ejection fraction (LVEF, median, Q1-Q3) was 38 (32-39)%. About 26.1% of participants presented with chronic kidney failure (CKD), nearly one third anaemia and 6.1% with peripheral artery disease (PAD). A total number of 8.3% of patients had a diagnosis of previous stroke/transient ischemic attack (TIA) and 2.6% of active cancer. Almost half of overall cohort had experienced myocardial infarction in the past, and 38.6% underwent prior revascularization. Chronic coronary symptoms were present in 57.8%, while 42.2% presented with ACS.
The number of diagnosed lesions (median, Q1-Q3) in overall population was 4 (1-6), while 25.8% of participants had concomitant LM disease. A nonsignificantly greater proportion of patients in COPD/PH cohort had characteristics of complex lesions – including larger percentage of patients with bifurcation (74.4%), severe calcification (33.6%) and total occlusion (20.0%). Overall, these features resulted in higher SYNTAX score (median, Q1-Q3) in COPD/PH cohort (31 (27-31) vs 30 (26-31) in non-COPD/PH group; p=0.75).
COPD/PH cohort – CABG vs PCI groups
Out of overall cohort of COPD/PH, a total number of 27 (21.6%) patients were qualified and had performed CABG, while 98 (78.4%) were treated with PCI. Both groups generally did not demostrate significant differences in clinical characteristics. Among the few, LVEF (median, Q1-Q3) was higher in CABG-cohort [40 (31-42) % vs 36 (31-40) % for PCI-group; p<0.01], while patients qualified for PCI presented more often with diagnosis of STEMI (15.3% vs 0.0%, p=0.03). PCI-cohort had higher cardiovascular risk (median, Q1-Q3) in EuroSCORE II and STS (EuroSCORE II: 9 (4-11) vs 6 (5-8) for CABG-group, p<0.001; STS: 6 (3-8) vs 4 (1-6) for CABG-group, p<0.01). Complete revascularization was achieved in 66.7% of patients treated with surgery and 58.2% of patients treated percutaneously.
No significant differences in angiographic parameters between both cohorts were found, however mean number of lesion and ratios of LM disease and bifurcation were higher in CABG-group, whereas patients undergoing PCI presented with higher proportion of severe calcification and total occlusion. The median (Q1-Q3) SYNTAX scores were 32 (25-35) and 31 (25-33) for CABG and PCI, respectively, p=0.08 – detailed in Table 2.
Overall outcomes
Five-year mortality in overall study population was 12.6%. A higher mortality was demonstrated for patients with diagnosis of COPD or PH as compared with population who had neither COPD nor PH (68.8% vs 4.8%, p<0.01) – Figure 1. Rates of MI, strokes and RR were comparable between these two groups. At 5 years, the incidence of MACCE was found to be more than 2-fold higher in COPD/PH-cohort (96.8 % vs 44.4% for PCI, p<0.01). Furthermore, this patient subset had also an increased rate of in-hospital mortality (8.0% vs 3.5% for PCI, p<0.01) and significantly prolonged postprocedural hospital stay [median (Q1-Q3): 9 (2-13) vs 6 (1-9) days for PCI, p<0.01] – Table 3.
COPD/PH population – outcomes in CABG– and PCI–cohorts
Among the 125 patients in COPD/PH population, higher 5-year mortality was observed in those who underwent surgery as compared with PCI-group (85.2% vs 64.3%, p=0.04) – Figure 1. The rates of MACCE, MI and RR did not significantly differ between both cohorts, however patients treated with CABG experienced stroke more often (14.8% vs 3.1% for PCI, p=0.02). Furthermore, surgery group was also characterized by higher in-hospital mortality (22.2% vs 4.1% for PCI, p<0.01) and prolonged postprocedural hospital stay [median (Q1-Q3): 14 (3-24) vs 7 (1-10) days for PCI, p<0.01] – Table 4.
We observed a significant interaction between COPD and revascularization strategy (p=0.0145), but no association between PH and CABG/PCI was found. We observed a significant interaction between CABG/PCI and frailty, and diabetes/diabetes with insulin, as well. Cox regression analysis showed outstanding HRs of mortality for PH (6.01 [3.47-10.40]) and COPD (5.65 [3.21-9.96]) as compared with conventional risk factors – Figure 2.
Discussion
The main finding of our study are increased rates of death and adverse cardiovascular events in short- and long-term follow-up in MVD-patients with concomitant COPD and/or PH compared to individuals without pulmonary disease, despite similar rates of complete revascularization in both groups. Moreover, in participants with severe CAD and concomitant pulmonary disease surgery was associated with higher rates of overall mortality and adverse events as compared with PCI-cohort.
Despite the multiple developments in therapy, the overall mortality in subgroup of patients with severe MVD remains unacceptably high, which allows us to hypothesize that some variables associated with increased mortality or MACCE have not been sufficiently evaluated so far.
Pulmonary diseases like COPD or PH are commonly coexisting with CAD [12,13,16,17,18]. Moreover, concomitance of COPD and/or PH makes CAD more advanced and significantly hinder effective management and worsen prognosis [13,18,19,20]. The severity of lung impairment is associated with frequency and severity of MVD as well [19]. However, so far, the long-term outcomes of MVD-patients with pulmonary diseases remain poorly investigated.
In our study we demonstrated COPD and PH as strong risk factors for increased mortality and rates of adverse events in individuals with severe CAD. We performed analysis which showed that over 5 years of follow-up patients with MVD and COPD and/or PH had much higher all-cause mortality as compared to cohort without COPD or PH (68.8% vs 4.8%, respectively, p<0.01).
We found that the occurrence of any adverse event was 2-folds higher than in population with severe CAD and coexisting pulmonary disease, than in those without COPD or PH (96.8% vs 44.4%, respectively, p<0.01).
In our cohort of MVD-patients pulmonary diseases were associated with the greatest increase in overall mortality – PH increased the 5-year risk up to 6-fold, while COPD over 5-fold.
The results of our analysis indicate that COPD and PH should be seriously considered in clinical management of MVD-patients, however the mechanisms underlying the relation between CAD and pulmonary diseases are non-obvious, thus the lack of targeted and risk-modifying treatment. Among predominantly postulated mechanisms linking CAD and pulmonary disorders are inflammation, hypoxemia and impaired vessel function [13,17]. It has been postulated that hypoxemia is a trigger for inflammation [21], which could precipitate to atherosclerosis acceleration, both in coronary and cerebral arteries leading to MI or stroke [13,16,17]. Bromodomain containing protein 4 (BRD4) is a promising target for treatment as a protein participating in epigenetic modifications leading to inflammation and smooth muscle proliferation in patients with CAD and PH [16]. Furthermore, dedicated biomarkers are being sought that could help diagnose groups at high risk [22].
Both COPD and PH are an integral part of the perioperative risk assessment in STS and EuroSCORE II, but in clinical practice to commonly COPD and PH are neglected among the variables assessed during patient selection for PCI [6,7].
The powerful prognostic value of COPD and PH in patients with MVD, which we revealed in this study, allows us to hypothesize that COPD and PH have a significant impact on the periprocedural risk and adverse events, not only for heart surgery, but also when qualifying for percutaneous revascularization and should be undoubtedly considered when deciding between PCI and CABG as a future management strategy.
Regarding short-term outcomes in our study, coexistence of COPD and/or PH was also associated with higher rates of in-hospital mortality and significantly prolonged in-hospital stay. Furthermore, almost 2-fold longer in-hospital stay and much higher in-hospital mortality were demonstrated for COPD/PH-patients treated with CABG (14.3 (3.2) vs 7.1 (1.3) days for non-PCI and 22.2% vs 4.1% for PCI, respectively, p<0.01).
An increased mortality after surgery reached 85.2% in total after 5-years of follow-up and was significantly higher compared to population after PCI, for which 5-year rate of all-cause death was lower, but still excessively high (64.3%), p=0.04. This finding proves how significant is an impact of pulmonary diseases on prognosis of MVD-patients in our study
Moreover, in MVD-patients with coexistence of COPD or PH who underwent revascularization with CABG, the incidence of stroke was observed more often as compared to cohort after PCI (14.8% vs 3.1%, respectively, p=0.02). However, for interaction effect (HR for CABG to PCI) COPD (p=0.015), non-insulin diabetes and frailty, but not PH were revealed as variables associated significantly with revascularization strategy.
The results of our study remain coherent with previous studies. Recent meta-analysis of 13 studies showed increased short- and long-term mortality for patients with CAD and coexisting COPD versus those without COPD, despite comparable revascularization rates. However, no significant difference in stroke frequency was demonstrated [21]. Hence, higher mortality after CABG compared to PCI seem to be persistent in all patients with CAD and COPD. Despite limited data regarding revascularization strategy in MVD-patients with PH, analysis of outcomes in subgroup undergoing CABG do not reveal an increased mortality in this cohort [23], which remains consistent with our results.
In patients with severe CAD and COPD or PH, lung impairment could be considered as an additional risk factor during the HT decision about revascularization strategy, but further multi-centre trials are required.
Limitations
Despite advantages of this study, it should be considered with some limitations. Even though we collected and analyzed patients’ characteristics with reasonable accuracy, the risk of bias could be greater than within RCTs. Although the risk of PH was assessed, there was no differentiation of PH phenotypes. The small, but still existing differences between baseline characteristics of study cohorts should be underlined, although these disparities were expected due to the nature of this research. The HT evaluations may be one-specific and do not reflect decisions made in other hospitals. The experience of surgical and percutaneous teams cannot be overlooked. A regular use of medications by participants cannot be objectively measured. Moreover, a hierarchy within HT also exists, which can lead to a bias as well.
Conclusions
In patients with MVD, lung impairment (COPD and/or PH) should be considered as an additional, important variable during Heart Team consultation and further referring to given revascularization strategy. Nevertheless, further multicenter trials or bigger registries are required.
Author Contributions
SJ conceived the concept of the study and collected the data. SJ and AP contributed to the design of the research and analysis. JK, ZH, GO, MG and TM were responsible for scientific supervision. All authors read and approved the final version of manuscript.
Funding
There were no external funding sources.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors reported no conflict of interest in relation to the submitted manuscript.
References
- WHO. WHO - causes of death. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 1 December 2024).
- Libby, P.; Theroux, P. Pathophysiology of coronary artery disease. Circulation 2005, 111, 3481–3488. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Barringhaus, K.G.; Park, K.L.; McManus, D.D.; et al. Outcomes from patients with multi-vessel disease following primary PCI: Staged PCI imparts very low mortality. Catheter Cardiovasc Interv. 2011, 77, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Ahn, J.M.; Lee, C.W.; et al. Long-Term Mortality After Coronary Revascularization in Nondiabetic Patients With Multivessel Disease. J. Am. Coll. Cardiol. 2016, 68, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Dehmer, G.J.; Grines, C.L.; Bakaeen, F.G.; et al. 2023 AHA/ACC Clinical Performance and Quality Measures for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Performance Measures. Circ. Cardiovasc Qual. Outcomes 2023, 16, e00121. [Google Scholar] [CrossRef]
- Patterson, T.; McConkey, H.Z.R.; Ahmed-Jushuf, F.; et al. Long-Term Outcomes Following Heart Team Revascularization Recommendations in Complex Coronary Artery Disease. J. Am. Heart Assoc. 2019, 8, e011279. [Google Scholar] [CrossRef]
- Jonik, S.; Kageyama, S.; Ninomiya, K.; et al. Five-year outcomes in patients with multivessel coronary artery disease undergoing surgery or percutaneous intervention. Sci. Rep. 2024, 14, 3218. [Google Scholar] [CrossRef]
- Legrand, V.M.; Serruys, P.W.; Unger, F.; et al. Three-year outcome after coronary stenting versus bypass surgery for the treatment of multivessel disease. Circulation 2004, 109, 1114–1120. [Google Scholar] [CrossRef]
- Schwalbe, N.; Wahl, B. Artificial intelligence and the future of global health. Lancet 2020, 395, 1579–1586. [Google Scholar] [CrossRef]
- Harikrishnan, S.; Sanjay, G.; Ashishkumar, M.; et al. Pulmonary hypertension registry of Kerala, India (PRO-KERALA) - Clinical characteristics and practice patterns. Int. J. Cardiol. 2018, 265, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Shimony, A.; Eisenberg, M.J.; Rudski, L.G.; et al. Prevalence and impact of coronary artery disease in patients with pulmonary arterial hypertension. Am. J. Cardiol. 2011, 108, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Liang, B.M.; Xu, Z.B.; Yi, Q.; Ou, X.M.; Feng, Y.L. Association of chronic obstructive pulmonary disease with coronary artery disease. Chin. Med. J. (Engl) 2013, 126, 3205–3208. [Google Scholar] [CrossRef] [PubMed]
- Jonik, S.; Marchel, M.; Pedzich-Placha, E.; et al. Optimal Management of Patients with Severe Coronary Artery Disease following Multidisciplinary Heart Team Approach-Insights from Tertiary Cardiovascular Care Center. Int. J. Env. Res. Public Health 2022, 19. [Google Scholar] [CrossRef]
- Dutta, P.; Gomez, D.; Gladwin, M.T. Do BRD(4)S of a Feather Flock Together? How an Inflammation-Driven Epigenetic Regulator May Link Pulmonary Hypertension and Coronary Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1428–1430. [Google Scholar] [CrossRef]
- Roversi, S.; Roversi, P.; Spadafora, G.; Rossi, R.; Fabbri, L.M. Coronary artery disease concomitant with chronic obstructive pulmonary disease. Eur. J. Clin. Invest 2014, 44, 93–102. [Google Scholar] [CrossRef]
- Dursunoglu, N.; Dursunoglu, D.; Yildiz, A.I.; Uludag, B.; Alacam, Z.N.; Saricopur, A. Severity of coronary atherosclerosis in patients with COPD. Clin. Respir. J. 2017, 11, 751–756. [Google Scholar] [CrossRef]
- Almagro, P.; Lapuente, A.; Pareja, J.; et al. Underdiagnosis and prognosis of chronic obstructive pulmonary disease after percutaneous coronary intervention: A prospective study. Int. J. Chron. Obstruct Pulmon Dis. 2015, 10, 1353–1361. [Google Scholar] [CrossRef]
- Huang, L.; Pang, L.; Gu, Q.; et al. Prevalence, risk factors, and survival associated with pulmonary hypertension and heart failure among patients with underlying coronary artery disease: A national prospective, multicenter registry study in China. Chin. Med. J. (Engl) 2022, 135, 1837–1845. [Google Scholar] [CrossRef]
- Li, Y.; Zheng, H.; Yan, W.; et al. The impact of chronic obstructive pulmonary disease on the prognosis outcomes of patients with percutaneous coronary intervention or coronary artery bypass grafting: A meta-analysis. Heart Lung 2023, 60, 8–14. [Google Scholar] [CrossRef]
- Casselbrant, A.; Fedorowski, A.; Frantz, S.; Engstrom, G.; Wollmer, P.; Hamrefors, V. Common physiologic and proteomic biomarkers in pulmonary and coronary artery disease. PLoS ONE 2022, 17(3), e0264376. [Google Scholar] [CrossRef] [PubMed]
- Velioglu, Y.; Yuksel, A.; Topal, D.; et al. Does pulmonary hypertension affect early-term outcomes of off-pump coronary artery bypass surgery? Rev. Assoc. Med. Bras. (1992) 2022, 68, 1747–1752. [Google Scholar] [CrossRef]
Figure 1.
A mortality rates in patients with COPD and/or PH and patients with neither COPD nor PH. Outcomes with CABG and PCI in patients with COPD and/or PH. CABG – coronary artery bypass grafting; COPD – chronic obstructive pulmonary disease; PCI – percutaneous coronary intervention; PH – pulmonary hypertension.
Figure 1.
A mortality rates in patients with COPD and/or PH and patients with neither COPD nor PH. Outcomes with CABG and PCI in patients with COPD and/or PH. CABG – coronary artery bypass grafting; COPD – chronic obstructive pulmonary disease; PCI – percutaneous coronary intervention; PH – pulmonary hypertension.

Figure 2.
Impact of some variables of clinical characteristics identified by machine learning and their interaction with revascularization modalities – CABG or PCI. PCI – percutaneous coronary intervention; CABG – coronary artery bypass grafting; COPD – chronic obstructive pulmonary disease; PH – pulmonary hypertension.
Figure 2.
Impact of some variables of clinical characteristics identified by machine learning and their interaction with revascularization modalities – CABG or PCI. PCI – percutaneous coronary intervention; CABG – coronary artery bypass grafting; COPD – chronic obstructive pulmonary disease; PH – pulmonary hypertension.


Table 1.
COPD/PH patients 125/1035 (12.1%) vs non-COPD/PH 910 (87.9%) – clinical and angiographic characteristics. ACS – acute coronary syndrome; BMI – body mass index; CABG – coronary artery bypass grafting; CAD – coronary artery disease; CKD – chronic kidney disease; COPD – chronic obstructive pulmonary disease; EuroSCORE II – European System for Cardiac Operative Risk Evaluation II; LM – left main; LVEF – left ventricle ejection fraction; MI – myocardial infarction; NSTEMI – non ST-segment elevation myocardial infarction; PAD – peripheral artery disease; PCI – percutaneous coronary intervention; PH – pulmonary hypertension; STEMI – ST-segment elevation myocardial infarction; STS – Society of Thoracic Surgeons score; SYNTAX – Synergy between PCI with Taxus and Cardiac Surgery; TIA – transient ischemic attack; UA – unstable angina.
Table 1.
COPD/PH patients 125/1035 (12.1%) vs non-COPD/PH 910 (87.9%) – clinical and angiographic characteristics. ACS – acute coronary syndrome; BMI – body mass index; CABG – coronary artery bypass grafting; CAD – coronary artery disease; CKD – chronic kidney disease; COPD – chronic obstructive pulmonary disease; EuroSCORE II – European System for Cardiac Operative Risk Evaluation II; LM – left main; LVEF – left ventricle ejection fraction; MI – myocardial infarction; NSTEMI – non ST-segment elevation myocardial infarction; PAD – peripheral artery disease; PCI – percutaneous coronary intervention; PH – pulmonary hypertension; STEMI – ST-segment elevation myocardial infarction; STS – Society of Thoracic Surgeons score; SYNTAX – Synergy between PCI with Taxus and Cardiac Surgery; TIA – transient ischemic attack; UA – unstable angina.
| Characteristics | Overall (1035) | COPD/PH (125) | Non-COPD/PH (910) | p Value | |
|---|---|---|---|---|---|
| Preprocedural | Age, years; median (Q1-Q3) | 68 (64-69) | 67 (64-68) | 68 (64-69) | 0.07 |
| Gender, male; n(%) | 784 (75.7) | 96 (76.8) | 688 (75.6) | 0.77 | |
| BMI, kg/m2; median (Q1-O3) | 28 (25-29) | 27 (26-28) | 28 (25-29) | 0.06 | |
| Frailty; n(%) | 98 (9.5) | 17 (13.6) | 81 (8.9) | 0.09 | |
| Current smoking; n(%) | 197 (19.0) | 98 (78.4) | 99 (10.9) | <0.01 | |
| Diabetes; n(%) | 317 (30.6) | 40 (32.0) | 277 (30.4) | 0.72 | |
| with insulin; n(%) | 105 (10.1) | 13 (10.4) | 92 (10.1) | 0.93 | |
| Hypertension; n(%) | 868 (83.9) | 106 (84.8) | 762 (83.7) | 0.76 | |
| Dyslipidemia; n(%) | 840 (81.2) | 99 (79.2) | 741 (81.4) | 0.56 | |
| Heart failure; n(%) | 734 (70.9) | 91 (72.8) | 643 (70.7) | 0.63 | |
| LVEF, %; median (Q1-Q3) | 38 (32-39) | 37 (32-38) | 38 (32-39) | 0.12 | |
| CKD; n(%) | 270 (26.1) | 33 (26.4) | 237 (26.0) | 0.93 | |
| Anemia; n(%) | 332 (32.1) | 41 (32.8) | 291 (32.0) | 0.85 | |
| Prior MI; n(%) | 507 (49.0) | 62 (49.6) | 445 (48.9) | 0.88 | |
| Prior revascularization; n(%) | 399 (38.6) | 51 (40.8) | 348 (38.2) | 0.58 | |
| Indication; n(%) | |||||
| Stable CAD | 598 (57.8) | 74 (59.2) | 524 (57.6) | 0.74 | |
| ACS | 437 (42.2) | 51 (40.8) | 386 (42.4) | 0.75 | |
| STEMI | 121 (11.7) | 15 (12.0) | 106 (11.6) | 0.92 | |
| NSTEMI/UA | 316 (30.5) | 36 (28.8) | 280 (30.8) | 0.65 | |
| PAD; n(%) | 63 (6.1) | 11 (8.8) | 52 (5.7) | 0.19 | |
| Prior stroke/TIA; n(%) | 86 (8.3) | 14 (11.2) | 72 (7.9) | 0.21 | |
| Active cancer; n(%) | 27 (2.6) | 6 (4.8) | 21 (2.3) | 0.10 | |
| EuroSCORE II, %; median (Q1-Q3) | 5 (4-9) | 8 (4-10) | 5 (3-6) | <0.01 | |
| STS score, %; median (Q1-Q3) | 3 (2-4) | 5 (3-6) | 3 (2-4) | <0.01 | |
| Procedural | Complete revascularization; n(%) | 630 (60.9) | 75 (60.0) | 555 (61.0) | 0.84 |
| Angiographic | Number of lesion; median (Q1-Q3) | 4 (1-6) | 4 (1-7) | 4 (1-6) | 0.89 |
| LM disease; n(%) | 267 (25.8) | 32 (25.6) | 235 (25.8) | 0.96 | |
| Bifurcation; n(%) | 752 (72.7) | 93 (74.4) | 659 (72.4) | 0.64 | |
| Severe calcification; n(%) | 292 (28.2) | 42 (33.6) | 250 (27.5) | 0.15 | |
| Total occlusion; n(%) | 171 (16.5) | 25 (20.0) | 146 (16.0) | 0.26 | |
| SYNTAX score; median (Q1-Q3) | 30 (26-31) | 31 (27-31) | 30 (26-31) | 0.75 | |
Table 2.
COPD/PH patients – CABG vs PCI – clinical and angiographic characteristics. CABG – coronary artery bypass grafting; PCI – percutaneous coronary intervention.
Table 2.
COPD/PH patients – CABG vs PCI – clinical and angiographic characteristics. CABG – coronary artery bypass grafting; PCI – percutaneous coronary intervention.
| Characteristics | Overall (125) | CABG (27) | PCI (98) | p Value | |
|---|---|---|---|---|---|
| Preprocedural | Age, years; median (Q1-Q3) | 67 (63-70) | 66 (64-67) | 68 (63-70) | 0.06 |
| Gender, male; n(%) | 96 (76.8) | 22 (81.5) | 74 (75.5) | 0.52 | |
| BMI, kg/m2; median (Q1-Q3) | 27 (25-28) | 26 (25-27) | 27 (25-28) | 0.09 | |
| Frailty; n(%) | 17 (13.6) | 2 (7.4) | 15 (15.3) | 0.29 | |
| Current smoking; n(%) | 98 (78.4) | 21 (77.8) | 77 (78.6) | 0.93 | |
| Diabetes; n(%) | 40 (32.0) | 8 (29.6) | 32 (32.7) | 0.78 | |
| with insulin; n(%) | 13 (10.4) | 3 (11.1) | 10 (10.2) | 0.90 | |
| Hypertension; n(%) | 106 (84.8) | 23 (85.2) |
83 (84.7) | 0.95 | |
| Dyslipidemia; n(%) | 99 (79.2) | 21 (77.8) | 78 (79.6) | 0.85 | |
| Heart failure; n(%) | 91 (72.8) | 18 (66.7) | 73 (74.5) | 0.42 | |
| LVEF, %; median (Q1-Q3) | 37 (31-41) | 40 (31-42) | 36 (31-40) | <0.01 | |
| CKD; n(%) | 33 (26.4) | 4 (14.8) | 29 (29.6) | 0.12 | |
| Anemia; n(%) | 41 (32.8) | 5 (18.5) | 36 (36.7) | 0.08 | |
| Prior MI; n(%) | 62 (49.6) | 12 (44.4) | 50 (51.0) | 0.55 | |
| Prior revascularization; n(%) | 51 (40.8) | 9 (33.3) | 42 (42.9) | 0.38 | |
| Indication; n(%) | |||||
| CCS | 74 (59.2) | 17 (63.0) | 57 (58.2) | 0.66 | |
| ACS | 51 (40.8) | 10 (37.0) | 41 (41.8) | 0.67 | |
| STEMI | 15 (12.0) | 0 (0.0) | 15 (15.3) | 0.03 | |
| NSTEMI/UA | 36 (28.8) | 10 (37.0) | 26 (26.5) | 0.29 | |
| PAD; n(%) | 11 (8.8) | 2 (7.4) | 9 (9.2) | 0.78 | |
| Prior stroke/TIA; n(%) | 14 (11.2) | 2 (7.4) | 12 (12.2) | 0.48 | |
| Active cancer; n(%) | 6 (4.8) | 0 (0.0) | 6 (6.1) | 0.19 | |
| EuroSCORE II, %; mean(SD) | 8 (4-10) | 6 (5-8) | 9 (4-11) | <0.01 | |
| STS score, %; median(Q1-Q3) | 5 (3-8) | 4 (1-6) | 6 (3-8) | <0.01 | |
| Procedural | Complete revascularization; n(%) | 75 (60.0) | 18 (66.7) | 57 (58.2) | 0.43 |
| Angiographic | Number of lesion; median (Q1-Q3) | 4 (1-5) | 4 (1-6) | 4 (1-5) | 0.13 |
| LM disease; n(%) | 32 (25.6) | 10 (37.0) | 22 (22.4) | 0.14 | |
| Bifurcation; n(%) | 93 (74.4) | 21 (77.8) | 72 (73.5) | 0.65 | |
| Severe calcification; n(%) | 42 (33.6) | 8 (29.6) | 34 (34.7) | 0.64 | |
| Total occlusion; n(%) | 25 (20.0) | 5 (18.5) | 20 (20.4) | 0.83 | |
| SYNTAX score; median (Q1-Q3) | 31 (25-34) | 32 (25-35) | 31 (25-33) | 0.08 | |
Table 3.
COPD/PH vs non-COPD/PH patients – endpoints. CABG – coronary artery bypass grafting; MACCE – major adverse cardiac and cerebrovascular event; MI – myocardial infarction; PCI – percutaneous coronary intervention.
Table 3.
COPD/PH vs non-COPD/PH patients – endpoints. CABG – coronary artery bypass grafting; MACCE – major adverse cardiac and cerebrovascular event; MI – myocardial infarction; PCI – percutaneous coronary intervention.
| Endpoints | Overall (1035) | COPD/PH (125) | Non-COPD/PH (910) | p Value |
|---|---|---|---|---|
| All-cause death, n(%) | 130 (12.6) | 86 (68.8) | 44 (4.8) | <0.01 |
| MI, n(%) | 121 (11.7) | 16 (12.8) | 105 (11.5) | 0.70 |
| Stroke, n(%) | 47 (4.5) | 7 (5.6) | 40 (4.4) | 0.55 |
| Repeat revascularization, n(%) | 261 (25.2) | 29 (23.2) | 232 (25.5) | 0.59 |
| MACCE, n(%) | 525 (50.7) | 121 (96.8) | 404 (44.4) | <0.01 |
| In-hospital mortality, n(%) | 42 (4.1) | 10 (8.0) | 32 (3.5) | 0.02 |
| Postprocedural hospital stay, days; median (Q1-Q3) | 7 (2-11) | 9 (2-13) | 6 (1-9) | <0.01 |
Table 4.
COPD/PH patients: CABG vs PCI – endpoints. CABG – coronary artery bypass grafting; MACCE – major adverse cardiac and cerebrovascular event; MI – myocardial infarction; PCI – percutaneous coronary intervention.
Table 4.
COPD/PH patients: CABG vs PCI – endpoints. CABG – coronary artery bypass grafting; MACCE – major adverse cardiac and cerebrovascular event; MI – myocardial infarction; PCI – percutaneous coronary intervention.
| Endpoints | Overall (125) | CABG (27) | PCI (98) | p Value |
|---|---|---|---|---|
| All-cause death, n(%) | 86 (68.8) | 23 (85.2) | 63 (64.3) | 0.04 |
| MACCE, n(%) | 121 (96.8) | 26 (96.3) | 95 (96.9) | 0.16 |
| MI, n(%) | 16 (12.8) | 2 (7.4) | 14 (14.3) | 0.42 |
| Stroke, n(%) | 7 (5.6) | 4 (14.8) | 3 (3.1) | 0.02 |
| Repeat revascularization, n(%) | 29 (23.2) | 4 (14.8) | 25 (25.5) | 0.26 |
| In-hospital mortality, n(%) | 10 (8.0) | 6 (22.2) | 4 (4.1) | <0.01 |
| Postprocedural hospital stay, days; median (Q1-Q3) | 9 (3-14) | 14 (6-24) | 7 (1-10) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



