Submitted:
28 April 2026
Posted:
30 April 2026
You are already at the latest version
Abstract
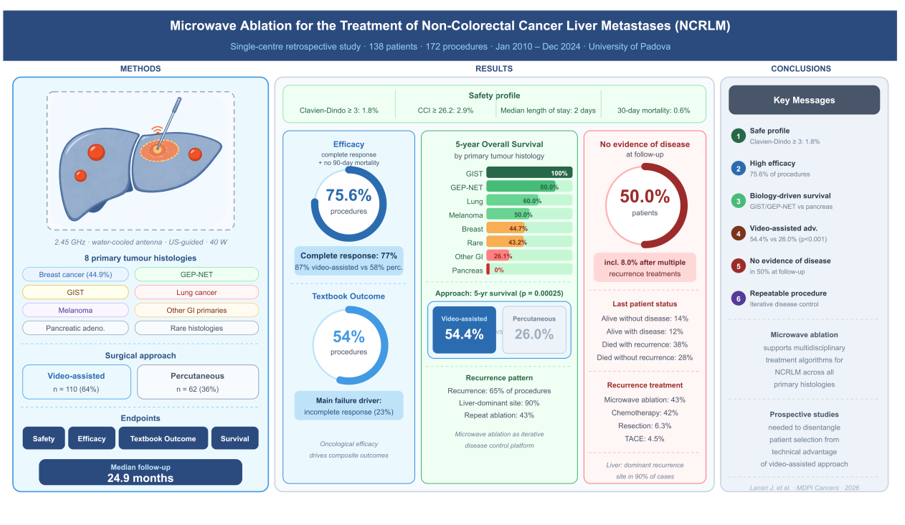
Background: Non-colorectal cancer liver metastases (NCRLM) represent a therapeutically challenging condition with poorly defined locoregional treatment options. This study evaluates the safety, oncological efficacy, and survival outcomes of microwave ablation (MWA) for NCRLM in a large single-centre series. Methods: Retrospective analysis of a prospectively collected database of patients undergoing MWA for NCRLM between January 2010 and December 2024 at a high-volume hepatobiliary centre. Endpoints were safety, efficacy, Textbook Outcome (TO) achievement, and overall survival (OS). Results: A total of 138 patients underwent 172 MWA across eight primary tumour categories. Major complications (Clavien-Dindo≥3) occurred in 1.8% of procedures, with a median hospital stay of 2 days and a 30-day mortality of 0.6%. Complete response (CR) was achieved in 77% of procedures. TO was achieved in 54% of procedures, with incomplete CR as the primary driver of failure. Five-year OS varied markedly by histology: 100% for GIST, 80.0% for GEP-NET, 44.7% for breast cancer, and 0% for pancreatic adenocarcinoma. The video-assisted approach was associated with superior OS compared to percutaneous ablation (5-year OS 54.4% vs. 26.0%, p=0.00025). Repeat MWA was the most frequent treatment for first hepatic recurrence (43%), and 50.0% of patients achieved non-evidence of disease (NED) at final follow-up. Conclusions: MWA is a safe and repeatable locoregional treatment for NCRLM, with outcomes driven by primary tumour biology. The high rate of liver-dominant recurrence treated with repeat MWA, combined with a final NED rate of 50%, supports MWA as a platform for iterative locoregional disease control in selected patients.
Keywords:
microwave ablation
; thermal ablation
; liver metastasis
; survival
; textbook outcome
1. Introduction
Liver metastases from non-colorectal cancer represent a growing therapeutic challenge, often portending poor prognoses and limited treatment options. Whereas surgical resection remains the gold standard for isolated lesions, many patients are deemed inoperable due to lesion number, location, comorbidities, or underlying hepatic dysfunction. Microwave ablation (MWA) has emerged as a minimally invasive modality capable of rapidly delivering high temperatures and producing predictable, confluent zones of tumour necrosis—even in proximity to large vessels where heat-sink effects compromise alternative thermal techniques. Although MWA is well established for hepatocellular carcinoma (HCC) and colorectal cancer liver metastases (CRLM) [1,2,3], its role in non-colorectal malignancies has been less rigorously defined [4,5]. In this retrospective observational study, we aim to delineate the potential of MWA to improve outcomes in patients with liver metastases originating from non-colorectal primaries, specifically measuring its safety, efficacy, the Textbook Outcome (TO) achievement, and patient survival.
2. Materials and Methods
This is a retrospective analysis from a prospectively collected database of patients treated with microwave ablation (MWA) between January 2010 and December 2024 at General Surgery 2-Hepato-pancreato-biliary Surgery and Liver transplantation Unit, Padua University Hospital, Padua, Italy.
Patients included in the study were those undergoing MWA for Non-colorectal cancer liver metastasis (NCRLM), either for de novo, treatment-naïve, or recurrent cases after liver resection (LR) or other treatments. Adult patients (≥ 18 years of age) undergoing MWA for NCRLM were eligible for the study. Procedures performed via open surgery (laparotomy) were excluded.
The procedure involves the insertion of a 14-G water-cooled coaxial antenna into the tumour under ultrasound guidance. All MWA 2ospital a 2.45 MHz microwave generator (AMICA GEN; HS Hospital Service S.p.A., Aprilia, Italy) with power settings at a median of 40 watts (interquartile range [IQR], 40–60 watts).
Our centre’s selection criteria for laparoscopic MWA were previously outlined [3], alongside the surgical procedure [6]. Notably, the laparoscopic approach is recommended when the percutaneous method is not feasible [1]. Thoracoscopic transdiaphragmatic liver ablations were evaluated within the framework of laparoscopic surgery, given their shared minimally invasive nature.
Liver metastases have been classified according to the tumour of origin in 8 categories as follows: 1) breast cancer; 2) gastrointestinal stromal tumour (GIST); 3) lung cancer; 4) melanoma; 5) gastro-entero-pancreatic neuroendocrine tumours (GEP-NET); 6) other gastrointestinal primaries (i.e., oesophageal, gastric, Vater’s papilla, ileal, gallbladder, perihilar and distal cholangiocarcinoma [CCA]); 7) other rare histology (i.e., tonsil carcinoma, parotid gland, laryngeal, thyme, adrenal gland, epithelioid haemangioendothelioma, kidney, leiomyosarcoma, endometrial, ovarian, vaginal, and prostatic cancer); 8) pancreatic adenocarcinoma.
Tumour burden (number and dimension of nodules) was measured at the last CT scan or MRI before ablation. In addition, the tumour burden score (TBS) was calculated according to Sasaki et al. [7].
The Charlson Comorbidity Index [8] was used to describe patients’ comorbidities.
Liver resection, MWA, radiofrequency ablation (RFA), and percutaneous ethanol injection (PEI) performed for metastatic disease before study inclusion were classified as ‘liver-directed surgical procedures’. The broader term ‘liver-directed treatments’ was used when trans-arterial procedures were also included.
Radical intent surgery was defined as a surgical procedure performed with the goal of complete ablation of hepatic tumour burden. Non-radical intent surgery refers to procedures aiming to reduce morbidity and preserve liver function (i.e., debulking, palliative).
Intraoperative complications were recorded and classified according to the Oslo classification [9]. Post-MWA complications were censored within 30 days after surgery; complications were recorded as follows: fever (requiring prolongation or change in antimicrobial therapy), nausea and vomiting, pleural effusion (if treated with albumin infusion and diuretic therapy or thoracentesis), pneumothorax (if pleural drainage was needed), ascites (requiring albumin supplementation or diuretics), haemoperitoneum, and liver function impairment according to the 50-50 criteria [10]. Safety was assessed using the Clavien–Dindo classification [11] and the Comprehensive Complication Index (CCI) [12], both of which were used to grade postoperative complications. A CCI ≥ 26.2 was used as the cutoff for severe postoperative morbidity after liver surgery [13]. Post-MWA mortality was censored in cases of death during ospitalization or within 30 and 90 days after the procedure. Readmission due to any treatment-related complication was recorded within 30 days after MWA. Prolonged length of stay (LOS) was censored if discharge occurred after 3 days [1].
Contrast-enhanced CT or MRI was repeated one month after MWA to assess the efficacy of ablation: the disappearance of any intra-tumoral arterial enhancement in the target lesion/s defined a complete response (CR) [14].
The analysis was designed per patient and per procedure. For each patient, each MWA procedure during follow-up was considered.
The efficacy of the procedure was assessed based on the CR achieved in the target lesion and the absence of mortality within 90 days.
As recently proposed [1,15], the Textbook Outcome (TO) was defined as follows: absence of post-MWA complications, a hospital stay of three days, no mortality or re-admission within 30 days, and complete response of the target lesion at 1-month post-MWA CT scan.
Overall survival (OS) is calculated from the time of surgery to the last follow-up available or death. Non-evidence of disease (NED) is defined as the absence of disease at the patient’s last available follow-up or death.
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study is conducted in accordance with the Declaration of Helsinki (as revised in 2013). Data is collected and managed in accordance with GDPR 2016/679. Each patient gives written consent for every procedure performed and for the use of data for research and publication purposes. All procedures were performed in accordance with the Declaration of Istanbul. No one received compensation or was offered any incentive for participating in this study. The study was approved by the Territorial Ethics Committee Central—Eastern Veneto Area (CET—ACEV) (protocol number 6344/A0/25, 12 June 2025).
2.1. Statistical Analysis
Values for categorical variables are expressed as totals and percentages, whereas for continuous variables they are expressed as medians and interquartile ranges (IQR). Statistical analyses are performed using Pearson’s chi-squared test or Fisher’s test for categorical variables and the Wilcoxon rank sum test for continuous variables. The length of follow-up is calculated from the date of surgery to the date of the patient’s latest follow-up date. The duration of follow-up is expressed as median (IQR). Recurrence curves are calculated using the Kaplan–Meier technique and compared with the log-rank test. The univariable and multivariable Cox proportional-hazard models are used to evaluate variables associated with DFS. Logistic regression models were used to estimate odds ratios (OR) with 95% confidence intervals (95% Cis) for factors associated with Efficacy, based on univariable analyses. A P-value < 0.05 indicated statistical significance; variables with a P-value < 0.1 were considered of marginal statistical significance. Statistical analyses are performed using R, R, Rstudio 4.5 (2025).
3. Results
Between January 2010 and December 2024, 138 patients underwent 172 MWA procedures eligible for the study. One hundred patients (72%) were female, and 61.5 (51.0, 70.0) years was the median age. Although only a negligible proportion of patients had a history of liver parenchyma disease, the median Charlson Comorbidity Index was as high as 8.0 (6.0, 9.0), with just 2 (1.5%) patients scoring ≤ 5. The study population was followed up for 24.9 (10.3, 55.8) months. The main indication for ablation was breast cancer’s liver metastasis in 62 (44.9%) patients. Primary cancer pathology, as well as the other features of the study population, are described in Figure 1 and Table 1.
One hundred and ten procedures were conducted via a minimally invasive video-assisted approach. The vast majority were laparoscopic, and 2 (1.2%) procedures involved thoracoscopic transdiaphragmatic liver ablation. Several concurrent procedures were fashioned with the ablation as detailed in Table S1.
A smaller tumor burden was significantly more frequent for percutaneous procedures. In both cohorts, more than 30% of procedures were preceded by a previous liver treatment. Video-assisted procedures were significantly longer, however more nodules were treated per session. The complete response (CR) rate registered for video-assisted procedure was as high as 87% compared after percutaneous ones (p < 0.001). Detailed description of perioperative characteristics is reported in Table 2.
Ablations were conducted with non-radical intent in 40 out of 172 (23.3%) procedures. Patients treated with radical intent showed significantly less neoplastic burden compered to non-radical counterparts, as demonstrated by inferior TBS (3 (2.1, 4.1) vs. 4.1 (2.7, 6.3), p = 0.001), less frequent bilobar disease (18 (14%) vs. 14 (35%), p = 0.002), and extrahepatic metastasis (7 (5.3%) vs. 19 (48%), p <0.001). Detailed description of perioperative characteristics stratified according to surgical intent is reported in Table S2.
Open conversion was needed just in one case for peritoneal adhesions. No transfusions were needed during any procedures. In one case was registered an Oslo Grade I intraoperative complication.
Postoperative course was uneventful for 149 (86%) procedures, with severe postoperative complications in just 3 (1.8%) cases. Comprehensive Complication Index (CCI) ≥ 26.2 was 5 (2.9%). Just one procedure needed postoperative intensive care admission for delayed extubation. One patient died due to acute liver decompensation three days after surgery, corresponding to a 30-day mortality rate of 0.6%. Median length of hospital stay (LOS) was 2.0 (1.0, 3.0) days. Main postoperative outcomes are summarized in Table 3.
The textbook outcome (TO) was achieved in 93 (54%) procedures. The lowest achievement rate among the items was the failure to attain a complete response of the target lesion, occurring in 77% of cases (Figure 2). Notably, this observation was not valid for video-assisted procedures, which showed higher CR rates and prolonged LOS. The proportion of procedures that achieved each desired health outcome in the whole series, in the video-assisted, and percutaneous approach, is depicted in Figure S1.
The stacked bar plots shown in Figure 2 depict the distribution of postoperative complication burden, complete response persistence, and 90-day mortality across primary tumour histologies.
3.1. Survival Analysis
Overall survival (OS) has been calculated per patient. Survival rate at 1, 3 and 5 years according to the tumour histology was as follows: breast cancer 92.7%, 61.1%, and 44.7% respectively; GIST 100.0%, 100.0%, and 100.0% respectively; lung cancer 87.5%, 60.0%, and 60.0% respectively; melanoma 100%, 83.3%, and 50.0% respectively; GEP-NET 100.0%, 100.0%, and 80.0% respectively; other gastrointestinal primaries 69.6%, 34.8%, and 26.1% respectively; other rare histology 80.6%, 51.8%, and 43.2% respectively; and pancreatic adenocarcinoma 41.7%, 20.8%, and 0.0% (Figure 3).
We then conducted a sub-analysis in those 104 patients who were treated with radical intent upfront. Survival rate at 1, 3 and 5 years according to the tumour histology was as follows: breast cancer 92.9%, 68.8%, and 54.5% respectively; GIST 100.0%, 100.0%, and 100.0% respectively; lung cancer 83.3%, 83.3%, and 83.3% respectively; melanoma 100%, 80.0%, and 40.0% respectively; GEP-NET 100.0%, 100.0%, and 80.0% respectively; other gastrointestinal primaries 81.8%, 40.9%, and 30.7% respectively; other rare histology 78.6%, 59.5%, and 59.5% respectively; and pancreatic adenocarcinoma 50.0%, 50.0%, and 0.0% (Figure S2).
Figure 3.
Kaplan–Meier survival curves of the study population stratified according to primary tumor histology.
Figure 3.
Kaplan–Meier survival curves of the study population stratified according to primary tumor histology.

No difference in short- and long-term OS was observed after MWA that achieved TO compared to procedures that did not. One, 3 and 5 years OS after MWA achieving TO was 88.9%, 57.5% and 46.3%, compared to 1, 3 and 5 years OS after not achieving TO MWA 82.2% 56.3% and 38.4%, p = 0.32 (Figure S3).
Nonetheless, a different survival was observed when procedures were stratified by surgical approach. One, 3, and 5 years OS associated after video-assisted approach was 90.7%, 66.2%, and 54.4%, compared to 77.5%, 41.9% and 26.0% at 1, 3, and 5 years, respectively, associated with the percutaneous approach (p = 0.00025) (Figure 4A).
Recurrence was registered after 112 (65%) procedures, and the liver was the main site of recurrence. Table S3 describes the recurrence pattern observed in our series.
The recurrence probability was calculated per procedure. Recurrence rate at 1, 3 and 5 years according to the tumor histology was as follows: breast cancer 47.7%, 55.8%, and 62.4% respectively; GIST 42.9%, 57.1%, and 57.1% respectively; lung cancer 59.6%, 73.1%, and 73.1% respectively; melanoma 25.0%, 37.5%, and 37.5% respectively; GEP-NET 42.9%, 71.4%, and not available respectively; other gastrointestinal primaries 84.7%, 89.9%, and 89.9% respectively; other rare histology 73.1%, 88.0%, and 88.0% respectively; and pancreatic adenocarcinoma 91.7%, not available, and not available respectively (Figure 5).
Video-assisted procedures registered a 1, 3 and 5 years recurrence probability rate of 50.5%, 64.1%, and 31.8%, respectively; conversely, 1, 3 and 5 years recurrence probability after percutaneous procedures were 74.3%, 79.4% and 20.6%, respectively (p = 0.0045) (Figure 4B).
Surgery was the recurrence treatment modality of choice in 55 out of 112 (49.1%) of cases, and MWA was the preferred option for surgical treatment of recurrence in 48 (43%) cases (Table S3).
At the end of the available follow-up, 69 (50.0%) patients achieved non-evidence of disease (NED), of which 11 (8.0%) after multiple recurrence treatment.
3.2. Factors Associated with Procedure Efficacy
One hundred and thirty (75.6%) procedure were effective according to our definition: CR of the target lesion and absence of 90-day mortality. The univariable analysis recorded pancreatic adenocarcinoma primary (OR 0,20; 95% CI 0.06, 0.66; p = 0.009), ECOG PS ≥ 2 (OR 0,16; 95% CI 0.02, 0.84; p = 0.037), previous liver resection (OR 0.30; 95% CI 0.13, 0.73; p = 0.007), number of previous liver surgery (OR 0.76; 95% CI 0.58, 0.98; p = 0.039), and percutaneous technique (OR 0.24; 95% CI 0.11, 0.48; p < 0.001) as factors significantly reducing the efficacy. Conversely, radical surgical intent (OR 2.33; 95% CI 1.07, 5.01; p < 0.030) and operative time (OR 1.01; 95% CI 1.00, 1.02; p < 0.013) were positively associated with it. However, it should be noted that surgical intent and operative time have very little clinical relevance or are subject to a high degree of uncertainty (Table 4).
4. Discussion
In this single-centre retrospective analysis of 138 patients who underwent 172 MWA procedures for NCRLM over a 14-year period, we evaluated the safety and efficacy of thermal ablation in a heterogeneous cohort spanning eight primary tumour histologies. Three main findings emerged. First, MWA was associated with a favourable safety profile, with severe complications (Clavien-Dindo ≥ 3) in 1.8% of procedures, CCI ≥ 26.2 in 2.9%, a median length of stay of 2 days, and a 30-day mortality of 0.6%. Second, oncological efficacy — defined as complete response of the target lesion combined with absence of 90-day mortality — was achieved in 130 (75.6%) procedures; the CR rate alone was 77%, and it differed markedly between surgical approaches, with video-assisted ablation outperforming the percutaneous approach (87% vs. 58%, p < 0.001). Third, five-year overall survival was profoundly influenced by primary tumour biology, ranging from 100% in patients with GIST-related metastases to 0% in those with pancreatic adenocarcinoma. Collectively, these findings support MWA as a versatile and repeatable locoregional modality whose clinical value is modulated by technical approach, patient selection, and — most importantly — the biological behaviour of the primary tumour.
The safety profile observed in our series compares favourably with published experiences on thermal ablation of liver malignancies. In the Phase III COLLISION trial, which compared thermal ablation with hepatic resection for colorectal liver metastases, van der Lei and colleagues reported zero procedure-related mortality and a significantly lower complication burden in the ablation arm than in the resection arm [16]. Similarly, in the setting of neuroendocrine liver metastases, Frilling and colleagues reported RFA-related morbidity in approximately 5% of patients and no procedure-related mortality [17]. In their recent comparative review of ablative therapies for hepatic metastases, Torielli et al. described radiofrequency and microwave ablation as procedures whose complication profiles are dominated by minor adverse events — pain, infection, bleeding, and rare thermal injury to adjacent structures — without explicitly quantifying procedure-related mortality in the pooled literature [18]. Our Clavien-Dindo ≥ 3 rate of 1.8% and 30-day mortality of 0.6% are therefore consistent with these benchmarks. The use of two complementary and independent metrics — the Clavien-Dindo classification, which identifies the worst single complication, and the Comprehensive Complication Index (CCI), which aggregates the cumulative burden of all postoperative events — provides a more granular assessment of safety than either instrument alone. Because a CCI ≥ 26.2 represents the validated threshold for severe postoperative morbidity after hepatobiliary surgery [13], the low proportion of procedures reaching this cutoff in our series (2.9%) directly reflects the overall safety of MWA; stated conversely, in more than 97% of procedures the cumulative postoperative morbidity remained below the threshold of clinical concern. This profile is particularly relevant in a NCRLM population characterised by substantial comorbidities (73% of our cohort had Charlson Comorbidity Index ≥ 7), where repeatability and minimal physiological cost are essential to support iterative locoregional strategies over extended disease trajectories.
When evaluated through the composite endpoint adopted in this study, oncological efficacy was achieved in 130 of 172 procedures (75.6%). The two components of this definition behaved asymmetrically: 90-day mortality was exceedingly rare (1.7% of procedures), while the complete response of the target lesion emerged as the dominant determinant of efficacy, with an overall CR rate of 77% that was strongly modulated by surgical approach. Video-assisted procedures achieved CR in 87% of cases, compared with 58% for the percutaneous approach (p < 0.001), and the percutaneous route persisted as the single strongest modifiable predictor of reduced efficacy in the univariable logistic regression (OR 0.24; 95% CI 0.11–0.48; p < 0.001). These figures are aligned with our institutional experience in HCC, where laparoscopic MWA has been shown to deliver high rates of radical ablation and textbook outcome, particularly in lesions unfavourably located or difficult to access percutaneously [3,1]. The Textbook Outcome rate of 54% observed in the overall series should be interpreted in light of its main driver of failure — namely, incomplete CR of the target lesion in 23% of procedures; post-ablation safety events contributed only marginally to TO failure. This reinforces the concept — already suggested for HCC [15] and here extended to NCRLM — that in modern ablation practice the bottleneck of composite outcomes is oncological completeness rather than perioperative morbidity.
The univariable analysis of factors associated with efficacy identified five variables that significantly reduced the probability of achieving the composite endpoint: pancreatic adenocarcinoma primary (OR 0,20; 95% CI 0.06, 0.66; p = 0.009), ECOG PS ≥ 2 (OR 0.16; 95% CI 0.02–0.84; p = 0.037), previous liver resection (OR 0.30; 95% CI 0.13–0.73; p = 0.007), number of previous liver surgeries (OR 0.76; 95% CI 0.58–0.98; p = 0.039), and percutaneous approach (OR 0.24; 95% CI 0.11–0.48; p < 0.001). Two additional variables — radical surgical intent (OR 2.33; 95% CI 1.07–5.01; p = 0.030) and operative time (OR 1.01; 95% CI 1.00–1.02; p = 0.013) — were positively associated with efficacy but warrant cautious interpretation. The association with radical intent is biologically coherent but reflects a pre-selection bias, as patients with lower tumour burden, unilobar disease, and absence of extrahepatic metastases were preferentially treated with curative intent (Table S2); it therefore describes the consequence of appropriate patient selection rather than an independent technical determinant of efficacy. The association with operative time is quantitatively minimal (OR 1.01 per minute) with a confidence interval that approaches unity, implying that clinical relevance is negligible despite statistical significance; this likely reflects the greater complexity — and therefore longer duration — of video-assisted procedures, which in turn are those with higher CR rates. Both observations illustrate the interpretive limits of univariable analysis in a heterogeneous cohort and underscore the need for prospective multivariable modelling to disentangle technical, oncological, and patient-level determinants of ablation efficacy.
Five-year overall survival varied across a broad spectrum according to primary tumour histology, from 100% for GIST-related metastases to 0% for pancreatic adenocarcinoma, with GEP-NET (80.0%), melanoma (50.0%), lung cancer (60.0%), breast cancer (44.7%), rare histologies (43.2%), and other gastrointestinal primaries (26.1%) falling in between. These gradients are concordant with the biology of each primary and with the available literature. Frilling and colleagues reported a 5-year OS of 53% after RFA for neuroendocrine liver metastases, a figure very close to our GEP-NET result and reflecting the indolent disease course of well-differentiated neuroendocrine neoplasms [17]. Narayanan and colleagues, in a multicentre evaluation of ablation for breast cancer liver metastases, reported 1- and 2-year OS of 90.1% and 55.9%, respectively [19]; our breast cancer cohort — the largest subgroup in the present series, accounting for 44.9% of patients — showed comparable 1-year OS (92.7%) and a 5-year OS of 44.7%, consistent with the natural history of a systemic disease where liver-directed therapy must be integrated within multimodal oncological care. At the opposite end of the biological spectrum, the uniformly poor survival of patients with pancreatic adenocarcinoma metastases calls into question the appropriateness of locoregional ablation in this setting and argues for extremely selective indications, ideally within dedicated clinical trials. The 2023 Appropriate Use Criteria issued by Hallemeier and colleagues on behalf of the American Radium Society, which support liver-directed therapy across selected non-colorectal primaries, provide a useful framework within which our histology-stratified outcomes can be interpreted [20]. Our histology-stratified data offer empirical corroboration of this framework, while also refining it: the striking contrast between the sustained survival observed in GIST and GEP-NET patients and the uniformly dismal outcomes in pancreatic adenocarcinoma suggests that future iterations of such recommendations should move beyond a binary "colorectal vs. non-colorectal" dichotomy toward a more granular, histology-specific stratification of appropriateness.
The survival advantage associated with the video-assisted approach (5-year OS 54.4% vs. 26.0% for percutaneous, p = 0.00025), together with a lower recurrence probability at all time points, deserves cautious interpretation. These differences are unlikely to reflect a purely technical effect of the approach itself; rather, they are probably driven by the confluence of patient and tumour selection, technical completeness, and adjunctive procedures. In our centre, the choice between video-assisted and percutaneous MWA follows institutional criteria developed over more than two decades of HCC experience [3], whereby laparoscopic ablation is preferred when the percutaneous route is not feasible or when concurrent procedures are indicated — circumstances present in 44% of video-assisted procedures versus 4.8% of percutaneous ones (p < 0.001). The video-assisted approach allows for direct visualisation of the liver surface, intraoperative ultrasound with higher spatial resolution, active protection of adjacent organs, and the simultaneous treatment of multiple nodules (median 2 vs. 1, p = 0.001). These factors likely contribute to the higher CR rate and, in turn, to improved long-term disease control. Distinguishing the independent contribution of technique from that of patient selection will require prospective studies or propensity-score-matched analyses.
This study has several limitations. First, its retrospective single-centre design carries inherent selection bias, although the use of a prospectively maintained database mitigates concerns regarding data completeness. Second, the histological heterogeneity of the cohort — while reflecting the real-world case-mix of a tertiary hepatobiliary unit — limits the statistical power of histology-specific survival analyses, particularly for smaller subgroups. Third, the univariable logistic regression of factors associated with efficacy, although hypothesis-generating, does not account for the interdependence of variables; multivariable modelling in a larger cohort will be necessary to identify independent predictors. Fourth, our safety definition, while methodologically robust, may not capture the full burden of minor or functional sequelae relevant to patient-reported outcomes. Finally, the comparison between video-assisted and percutaneous approaches reflects institutional allocation criteria and is therefore susceptible to confounding by indication. Despite these limitations, the size of the cohort, the 14-year time frame, the breadth of histologies represented, and the adoption of contemporary safety and efficacy definitions provide a comprehensive portrait of MWA as currently practised for NCRLM at a high-volume European hepatobiliary centre, and identify the video-assisted approach, patient performance status, and primary tumour biology as the key axes around which future prospective evaluation should be structured.
5. Conclusions
In this 14-year single-centre experience, microwave ablation emerged as a safe and oncologically effective locoregional treatment for non-colorectal cancer liver metastases, with severe complications in 1.8% of procedures, a CCI ≥ 26.2 rate of 2.9%, and a composite efficacy endpoint achieved in 75.6% of procedures. The video-assisted approach was associated with substantially higher complete response rates and superior long-term survival compared with the percutaneous route, though these differences likely reflect the combined effect of patient selection, technical completeness, and the opportunity to perform concurrent procedures. Five-year overall survival varied widely across primary tumour histologies, reaffirming that the ultimate prognostic driver remains the biology of the primary cancer rather than the ablation technique itself. Within this framework, MWA offers a repeatable, minimally invasive platform for iterative locoregional disease control - in many cases aimed at avoiding tumour-related liver morbi-mortality or to prolong the interval between chemotherapeutic cycles - most effective when integrated into multidisciplinary treatment pathways and calibrated to the specific histology, performance status, and prior treatment history of each patient. Prospective, histology-stratified studies are warranted to refine patient selection and to disentangle the independent contributions of technique and biology to long-term outcomes.
Supplementary Materials
The following supporting information can be downloaded atthe website of this paper posted on Preprints.org. Figure S1: The proportion of procedures that achieved each desired health outcome forming the textbook outcome (TO) in the whole series, in the video-assisted, and percutaneous approach; Figure S2: Kaplan–Meier survival curves of patients who were treated with radical intent upfront, stratified according to primary tumor histology; Figure S3: Kaplan–Meier survival curves of MWA procedures stratified according to textbook outcome (TO) achievement; Table S1: Concurrent procedures fashioned with the ablation; Table S2: Perioperative characteristics of radical vs. non-radical intent procedures; Table S3: Recurrence pattern and treatments.
Author Contributions
Conceptualization, JL and UC; methodology, JL, IB and UC; software, IB; validation, JL and IB; formal analysis, IB; investigation, JL; resources, JL; data curation, JL, SL, CN, CDN, GT, DV, AF, FED; writing—original draft preparation, JL and SL; writing—review and editing, JL, SL and UC; visualization, JL; supervision, AV, EG and UC; project administration, JL. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Territorial Ethics Committee Central—Eastern Veneto Area (CET—ACEV) (protocol number 6344/A0/25, 12 June 2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets generated during and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Acknowledgments
The graphical abstract was created with the assistance of Claude (Anthropic, San Francisco, CA, USA), an AI-based language and image processing tool, and DALL-E (OpenAI, San Francisco, CA, USA), an AI-based image generation tool.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BSC | Best Supportive Care |
| CCA | Cholangiocarcinoma |
| CCI | Comprehensive Complication Index |
| CR | Complete Response |
| CRLM | Colorectal Cancer Liver Metastases |
| CSPH | Clinically Significant Portal Hypertension |
| ECOG PS | Eastern Cooperative Oncology Group Performance Status |
| GEP-NET | Gastro-Entero-Pancreatic Neuroendocrine Tumours |
| GIST | Gastrointestinal Stromal Tumour |
| HCC | Hepatocellular Carcinoma |
| HCV | Hepatitis C Virus |
| ICU | Intensive Care Unit |
| LOS | Length of Hospital Stay |
| LR | Liver Resection |
| MWA | Microwave Ablation |
| NAFLD | Non-Alcoholic Fatty Liver Disease |
| NCRLM | Non-Colorectal Cancer Liver Metastasis |
| NED | Non-Evidence of Disease |
| OS | Overall Survival |
| PEI | Percutaneous Ethanol Injection |
| pRBC | Packed Red Blood Cells |
| RFA | Radiofrequency Ablation |
| TACE | Trans-Arterial Chemoembolization |
References
- Lanari, J.; Caregari, S.; Billato, I.; Gringeri, E.; D’Amico, F.; Gemo, G.; et al. Textbook Outcome of Laparoscopic Microwave Ablation for Hepatocellular Carcinoma. Cancers 2023, 15(2), 436. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Lanari, J.; Masutti, M.; D’Amico, F.E.; Vitale, A.; Gringeri, E. Percutaneous and Laparoscopic-Assisted Ablation of Hepatocellular Carcinoma; Hepatocellular Carcinoma [Internet]; Ettorre, G.M., Ed.; Springer International Publishing: Cham, Switzerland, 2023; pp. 63–70, [cited 2025 Oct 30]. [Google Scholar] [CrossRef]
- Cillo, U.; Bertacco, A.; Fasolo, E.; Carandina, R.; Vitale, A.; Zanus, G.; et al. Videolaparoscopic microwave ablation in patients with HCC at a European high-volume center: Results of 815 procedures. J. Surg. Oncol. 2019, 120(6), 956–65. [Google Scholar] [CrossRef] [PubMed]
- Del Basso, C.; Usai, S.; Levi Sandri, G.B. Non-colorectal non-neuroendocrine liver metastasis: a narrative review of surgical treatment. Chin. Clin. Oncol. 2022, 11(4), 28. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, G.M.; Braghiroli, M.I.F.M.; Pirola Kruger, J.A.; Coelho, F.F.; Herman, P. Is There a Role for Locoregional Therapies for Non-colorectal Gastrointestinal Malignancies? Hematol. Oncol. Clin. North Am. 2025, 39(1), 125–41. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Noaro, G.; Vitale, A.; Neri, D.; D’Amico, F.; Gringeri, E.; et al. Laparoscopic microwave ablation in patients with hepatocellular carcinoma: a prospective cohort study. HPB 2014, 16(11), 979–986. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Morioka, D.; Conci, S.; Margonis, G.A.; Sawada, Y.; Ruzzenente, A.; et al. The Tumor Burden Score: A New “Metro-ticket” Prognostic Tool For Colorectal Liver Metastases Based on Tumor Size and Number of Tumors. Ann. Surg. 2018, 267(1), 132. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 1987, 40(5), 373–383. [Google Scholar] [CrossRef] [PubMed]
- 9 Rosenthal, R.; Hoffmann, H.; Clavien, P.A.; Bucher, H.C.; Dell-Kuster, S. Definition and Classification of Intraoperative Complications (CLASSIC): Delphi Study and Pilot Evaluation. World J. Surg. 2015, 39(7), 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Balzan, S.; Belghiti, J.; Farges, O.; Ogata, S.; Sauvanet, A.; Delefosse, D.; et al. The “50-50 Criteria” on Postoperative Day 5. Ann. Surg. 2005, 242(6), 824–829. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240(2), 205–213. [Google Scholar] [CrossRef] [PubMed]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.A. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann. Surg. 2013, 258(1), 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cloyd, J.M.; Mizuno, T.; Kawaguchi, Y.; Lillemoe, H.A.; Karagkounis, G.; Omichi, K.; et al. Comprehensive Complication Index Validates Improved Outcomes Over Time Despite Increased Complexity in 3707 Consecutive Hepatectomies. Ann. Surg. 2020, 271(4), 724–731. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatocellular carcinoma. J. Hepatol. 2025, 82(2), 315–374. [Google Scholar] [CrossRef] [PubMed]
- Serra, C.; Cossiga, V.; Serenari, M.; Felicani, C.; Mazzotta, E.; Pinato, D.J.; et al. Safety and efficacy of percutaneous radiofrequency ablation for hepatocellular carcinoma: a textbook outcome analysis. HPB 2022, 24(5), 664–671. [Google Scholar] [CrossRef] [PubMed]
- van der Lei, S.; Puijk, R.S.; Dijkstra, M.; Schulz, H.H.; Vos, D.J.W.; De Vries, J.J.J.; et al. Thermal ablation versus surgical resection of small-size colorectal liver metastases (COLLISION): an international, randomised, controlled, phase 3 non-inferiority trial. Lancet Oncol. 2025, 26(2), 187–199. [Google Scholar] [CrossRef] [PubMed]
- Frilling, A.; Modlin, I.M.; Kidd, M.; Russell, C.; Breitenstein, S.; Salem, R.; Kwekkeboom, D.; Lau, W.Y.; Klersy, C.; Vilgrain, V.; Davidson, B.; Siegler, M.; Caplin, M.; Solcia, E.; Schilsky, R. Working Group on Neuroendocrine Liver Metastases. Recommendations for management of patients with neuroendocrine liver metastases. Lancet Oncol. 2014, 15(1), e8–e21. [Google Scholar] [CrossRef] [PubMed]
- Torielli, P.; McGale, J.; Liao, M.J.; Rhaiem, R.; Bouche, O.; Botsen, D.; Gerin, O.; Lamane, A.; Lawrence, Y.; Madelis, G.; Rozenblum, L.; Sajan, A.; Tordjman, M.; Dercle, L.; Beddok, A. Hepatic metastases management: A comparative review of surgical resection, thermal ablation, and stereotactic body radiation therapy. Eur. J. Cancer 2025, 228, 115691. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, G.; Ruiz, E.M.; Dijkstra, M.; Gentile, N.T.; Donahue, D.; Gandhi, R.T.; Mahtani, R.L.; Mautner, S.; van den Bemd, B.A.T. Clinical Efficacy of Percutaneous Image-Guided Ablation in Breast Cancer Metastases to the Liver. Cancers 2025, 17(23), 3823. [Google Scholar] [CrossRef] [PubMed]
- Hallemeier, C.L.; Sharma, N.; Anker, C.; Selfridge, J.E.; Lee, P.; Jabbour, S.; Williams, V.; Liu, D.; Kennedy, T.; Jethwa, K.R.; Kim, E.; Kumar, R.; Small, W., Jr.; Tchelebi, L.; Russo, S. American Radium Society Appropriate Use Criteria for the use of liver-directed therapies for nonsurgical management of liver metastases: Systematic review and guidelines. Cancer 2023, 129(20), 3193–3212. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Category of Liver Metastases according to the Primary Tumours.

Figure 2.
Outcome distribution by primary tumour histology. Stacked bar plots display the percentage of patients in each histological subgroup for three key outcomes: (A) proportion with a Comprehensive Complication Index (CCI) ≥ 26.2, indicating high postoperative complication burden; (B) complete response vs. persistence; (C) 90-day mortality. Abbreviations: CCI, Comprehensive Complication Index; GI, gastrointestinal; GIST, gastrointestinal stromal tumour; GEP-NET, gastro-entero-pancreatic neuroendocrine tumours.
Figure 2.
Outcome distribution by primary tumour histology. Stacked bar plots display the percentage of patients in each histological subgroup for three key outcomes: (A) proportion with a Comprehensive Complication Index (CCI) ≥ 26.2, indicating high postoperative complication burden; (B) complete response vs. persistence; (C) 90-day mortality. Abbreviations: CCI, Comprehensive Complication Index; GI, gastrointestinal; GIST, gastrointestinal stromal tumour; GEP-NET, gastro-entero-pancreatic neuroendocrine tumours.

Figure 4.
A) Kaplan–Meier survival curves of MWA procedures stratified according to the surgical approach. B) Kaplan–Meier recurrence probability curves of MWA procedures stratified according to the surgical approach.
Figure 4.
A) Kaplan–Meier survival curves of MWA procedures stratified according to the surgical approach. B) Kaplan–Meier recurrence probability curves of MWA procedures stratified according to the surgical approach.

Figure 5.
Kaplan–Meier recurrence probability curves of MWA procedures stratified according to primary tumour histology.
Figure 5.
Kaplan–Meier recurrence probability curves of MWA procedures stratified according to primary tumour histology.


Table 1.
Patients’ demographics and characteristics.
| Variables | N = 1381 |
|---|---|
| Age (years) | 61.5 (51.0, 70.0) |
| Sex (female) | 100 (72%) |
| ECOG PS ≥ 2 *missing | 4 (3.1%) *10 |
| CCI ≥ 7 *missing | 98 (73%) *4 |
| Diabetes (yes) *missing | 12 (8.8%) *1 |
| Cirrhosis (yes) | 4 (2.9%) |
| HCV positive | 1 (0.7%) |
| NAFLD | 2 (1.4%) |
| CSPH | 2 (1.4%) |
| Last patient status | |
| Died with recurrence | 52 (38%) |
| Died without recurrence | 38 (28%) |
| Alive with disease | 17 (12%) |
| Alive without disease | 20 (14%) |
| Alive without disease after last recurrence treatment | 11 (8.0%) |
| Mean follow-up (months) | 24.9 (10.3, 55.8) |
| 1 Median (Q1, Q3); n / N (%) | |
ECOG PS, Eastern Cooperative Oncology Group Performance Status; CCI, Charlson comorbidity Index; HCV, hepatitis C virus; NAFLD, non-alcoholic fatty liver disease; CSPH, clinically significant portal hypertension.
Table 2.
Perioperative characteristics of video-assisted vs percutaneous procedures.
| Variable | Video-assisted N = 1101 |
Percutaneous N = 621 |
p2 |
|---|---|---|---|
| Pre-operative variables | |||
| Platelets (109/L) *missing | 208(165.0,267.0) *3 | 213(166.0,277.0) *7 | 0.81 |
| Bilirubin (umol/L) *missing | 10.4 (7.4, 16.4) *6 | 10 (6.9, 13.5) *11 | 0.23 |
| Nodules (n) | 2 (1.0, 3.0) | 1 (1.0, 2.0) | 0.001 |
| Major diameter | 2.3 (1.6, 3.2) | 1.9 (1.4, 3.5) | 0.36 |
| TBS | 3.4 (2.4, 5.2) | 2.7 (1.8, 4.3) | 0.009 |
| Bilobar disease | 22 (20%) | 10 (16%) | 0.53 |
| Major vassels invasion | 1 (0.9%) | 0 (0%) | >0.99 |
| Extrahepatic metastasis | 14 (13%) | 12 (19%) | 0.24 |
| Previous liver-dir. surgery | |||
| None | 76 (69%) | 37 (60%) | 0.27 |
| 1 | 21 (19%) | 17 (27%) | |
| 2 - 4 | 11 (9.9%) | 6 (9.6%) | |
| ≥5 | 2(1.8%) | 2 (3.2%) | |
| Previous liver-dir. treatments | 0.25 | ||
| None | 72 (65%) | 35 (56%) | |
| 1 | 23 (21%) | 19 (31%) | |
| 2 - 4 | 12 (10.9%) | 5 (8%) | |
| ≥5 | 3 (2.7%) | 3 (4.8%) | |
| Intra-operative variables | |||
| Radical Intent | 89 (81%) | 43 (69%) | 0.085 |
| Concurrent procedure | 48 (44%) | 3 (4.8%) | <0.001 |
| Operative time (min) *missing | 100 (80.0, 125.0) *2 | 25 (15.0, 32.5) *2 | <0.001 |
| Nodules treated *missing | 2 (1.0, 3.0) *2 | 1 (1.0, 1.0) *2 | <0.001 |
| Duration, Σ (min) *missing | 12 (8.0, 18.0) *2 | 7 (5.0, 10.0) *1 | <0.001 |
| Power (Watt) | 40 (40.0, 60.0) | 40 (40.0, 60.0) | 0.062 |
| Post-operative variables | |||
| LOS | 2.5 (2.0, 3.0) | 1 (1.0, 1.0) | <0.001 |
| Postoperative complications | 21 (19%) | 2 (3.2%) | 0.003 |
| Reoperation | 2 (1.8%) | 0 (0%) | 0.54 |
| Clavien-Dindo ≥ 3 | 3 (2.7%) | 0 (0%) | 0.70 |
| CCI > 26.2 | 5 (4.5%) | 0 (0%) | 0.16 |
| CR of the target lesion | 96 (87%) | 36 (58%) | <0.001 |
| TO (achieved) | 61 (55%) | 32 (52%) | 0.63 |
| 90-day mortality | 2 (1.8%) | 1 (1.6%) | >0.99 |
|
1 n / N (%); Median (Q1, Q3). 2 Pearson’s Chi-squared test; Fisher’s exact test; Wilcoxon rank sum test; NA. | |||
TBS, tumour burden score; MWA, microwave ablation; PEI, percutaneous alcohol injection; RFA, radiofrequency ablation; TACE, trans-arterial chemoembolization; LOS, length of hospital stay; CCI, comprehensive complication index; CR, complete response; TO, Textbook outcome.
Table 3.
Postoperative outcomes.
| Variable | N (%) |
|---|---|
| LOS > 3 | 27 (15.6%) |
| Fever | 13 (7.6%) |
| Nausea and vomiting | 7 (4.1%) |
| Pleural effusion | 2 (1.2%) |
| Pneumothorax | 0 (0.0%) |
| Ascites | 1 (0.6%) |
| Liver function impairment (50-50) | 1 (0.6%) |
| Hemoperitoneum | 1 (0.6%) |
| Readmission within 30 days | 9 (5.2%) |
| 30 days mortality | 1 (0.6%) |
| No CR | 40 (23%) |
| LOS, length of hospital stay; CR, complete response. | |
Table 4.
Univariable analysis of factors associated with efficacy.
| Variable | OR | 95% CI | p |
|---|---|---|---|
| Breast cancer | 1.15 | 0.57, 2.36 | 0.7 |
| GIST | 0.80 | 0.17, 5.74 | 0.8 |
| Lung cancer | 1.49 | 0.36, 10.0 | 0.6 |
| Other gastrointestinal primaries | 0.90 | 0.35, 2.66 | 0.8 |
| Other rare histologies | 0.87 | 0.36, 2.23 | 0.8 |
| Pancreatic adenocarcinoma | 0.20 | 0.06, 0.66 | 0.009 |
| Age | 0.99 | 0.97, 1.02 | 0.7 |
| Sex (male) | 0.89 | 0.42, 1.94 | 0.8 |
| ECOG PS ≥ 2 | 0.16 | 0.02, 0.84 | 0.037 |
| Number of nodules: | |||
| • 1 | - | - | - |
| • 2 -3 | 1.02 | 0.46, 2.29 | >0.9 |
| • > 3 | 0.40 | 0.16, 1.03 | 0.054 |
| Major diameter | 0.96 | 0.82, 1.15 | 0.6 |
| TBS | 0.94 | 0.84, 1.04 | 0.2 |
| Bilobar disease | 0.54 | 0.24, 1.28 | 0.15 |
| Extrahepatic metastasis | 0.86 | 0.34, 2.34 | 0.7 |
| Previous Liver Resection | 0.30 | 0.13, 0.73 | 0.007 |
| Previous Liver Ablation | 0.77 | 0.37, 1.65 | 0.5 |
| Previous Liver Treatments | 0.66 | 0.33, 1.35 | 0.3 |
| Number of previous liver surgery | 0.76 | 0.58, 0.98 | 0.039 |
| Number of previous liver treatments | 0.80 | 0.62, 1.02 | 0.066 |
| Percutaneous approach | 0.24 | 0.11, 0.48 | <0.001 |
| Concurrent procedure | 1.47 | 0.68, 3.42 | 0.3 |
| Radical Surgical Intent | 2.33 | 1.07, 5.01 | 0.030 |
| Operative time (min) | 1.01 | 1.00, 1.02 | 0.013 |
| Nodules treated | 0.98 | 0.81, 1.21 | 0.8 |
| Duration, Σ (min) | 1.02 | 0.97, 1.07 | 0.5 |
| Power (Watt) | 1.01 | 0.99, 1.04 | 0.4 |
| LOS | 1.09 | 0.90, 1.39 | 0.4 |
| Postoperative complications | 1.63 | 0.57, 5.87 | 0.4 |
| Clavien-Dindo ≥ 3 | 0.56 | 0.09, 1.30 | 0.3 |
| CCI ≥ 26.2 | 1.30 | 0.19, 25.8 | 0.8 |
CI, Confidence Interval; OR, Odds Ratio; GIST, gastrointestinal stromal tumour; GEP-NET, gastroenteropancreatic-neuroendocrin tumour; ECOG PS, Eastern Cooperative Oncology Group Performance Status; TBS, tumour burden score; LOS, length of hospital stay; CCI, comprehensive complication index
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



