Submitted:
29 April 2026
Posted:
30 April 2026
You are already at the latest version
Abstract
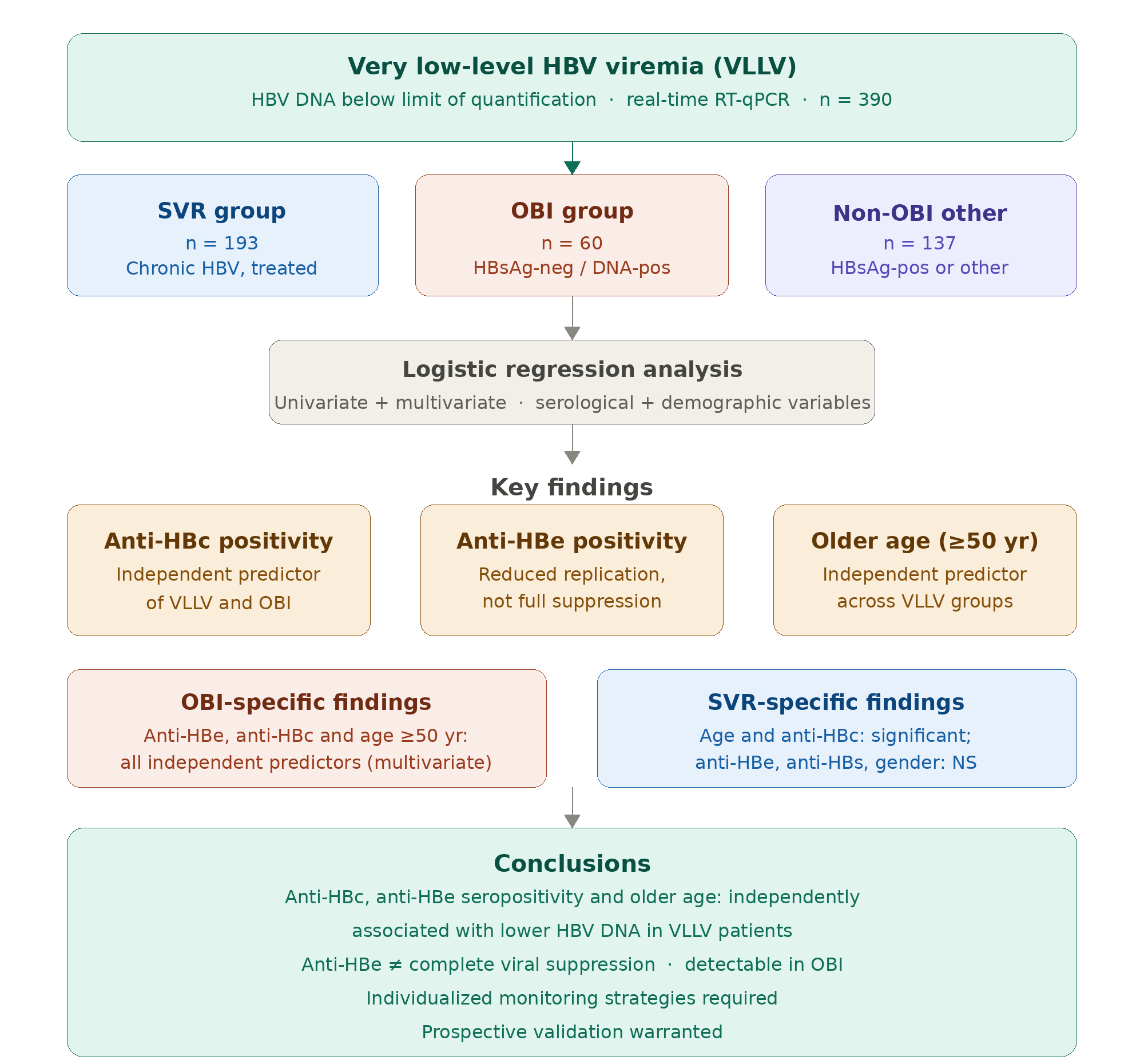
Objectives: This study aimed to evaluate very low HBV DNA viral load below the limit of quantification and to identify associated risk factors in different patient groups, including individuals with chronic hepatitis B, occult HBV infection (OBI) and others. Methods: We retrospectively analyzed 390 patients with very low-level viremia (VLLV). HBV DNA levels were measured in plasma samples using real-time RT-qPCR. Serological markers were evaluated in serum samples using chemiluminescence microparticle immunoassay (CMIA). Demographic variables, HBV serological markers (anti-HBs, anti-HBe, anti-HBc), and DNA results were evaluated. Results: The study included 193 patients in the sustained virological response (SVR) group and 197 patients in the other group; 60 of these patients had occult hepatitis B infection (HBV DNA positive, HBsAg negative) and 137 had no occult hepatitis B infection. Very low viral load was more common in men (53.3%) and in individuals aged ≥50 years (63.3%). In univariate analysis, OBI was associated with anti-HBe (odds ratio (OR)=2.874, 95%CI:1.256-6.172, p=0.012), anti-HBc seropositivity (OR=2.368; 95%CI:1.216-4.527, p=0.008), and being ≥50 years age (OR=1.845, 95% CI:0.963-3.473, p=0.077). In multivariate analysis, being ≥50 years of age, anti-HBe positivity, and anti-HBc positivity were independently associated with OBI. Among SVR patients, VLLV was associated with older age and anti-HBc positivity, but no significant association was observed with gender, anti-HBe, or anti-HBs status. Conclusions: In patients with VLLV, anti-HBc and anti-HBe seropositivity, along with older age, were independently associated with lower HBV DNA levels. Although anti-HBe positivity reflects reduced viral replication, it does not indicate complete viral suppression and may be detected at very low viremia levels, particularly in occult HBV infection. These findings highlight the complex interplay between viral replication dynamics and host immune responses across the VLLV spectrum, and emphasize the need for individualized monitoring strategies. Further validation through prospective studies is warranted.
Keywords:
hepatitis B virus
; very low-level viremia
; lower limit of quantification
; risk factors
; occult hepatitis B virus infection
1. Introduction
Hepatitis B virus (HBV) infection remains a major global health concern, affecting approximately 296 million people and causing nearly 1.1 million deaths annually due to HBV-related complications [1]. Despite the widespread implementation of universal vaccination, the incidence of new infections has decreased; however, chronic hepatitis B (CHB) continues to impose a significant burden on global healthcare systems [2]. Nonetheless, contemporary antiviral approaches predominantly employ nucleos(t)ide analogs (NAs), including entecavir (ETV) and tenofovir, which proficiently inhibit virus replication, a significant number of patients do not attain a complete virological response, resulting in the clinical occurrences of occult HBV infection (OBI) and chronic very low-level viremia (VLLV) [3,4,5]. The fundamental mechanism driving both OBI and VLLV is the enduring presence of covalently closed circular DNA (cccDNA) in the nucleus of infected hepatocytes [2,6]. Current nucleic acid therapeutics incorporate into viral DNA to inhibit replication but are incapable of immediately eradicating or silencing the persistent cccDNA reservoir [7]. Host immunological failure, which is characterized by insufficient T-cell and B-cell responses that fail to achieve complete viral clearance, exacerbates this persistence. Additionally, this pattern may exhibit a sustained virological response (SVR) to antiviral treatment for CHB [8,9,10].
VLLV refers to a specific subset of low-level viremia where HBV DNA remains detectable at extremely low concentrations, typically defined as <20 IU/mL. The advancement of the PCR technology facilitates highly sensitive detection of HBV DNA, attaining a lower limit of detection (LOD) below 10 IU/mL [11]. The Limit of Detection is generally less than the Limit of Quantification (LOQ). Methodologically, VLLV and OBI management is intricately linked to a precise comprehension of the technical differentiation between the LOD and LOQ [5,12,13]. In diagnostic approaches, confusion in clinical practice between the LOD and LOQ may lead to the misdiagnosis of actual persistent viremia and OBI cases [14].
Currently, contemporary high-sensitivity PCR assays (LOD <10 IU/mL) have demonstrated that in roughly 20% to 40% of patients undergoing antiviral therapy, the virus is not entirely eradicated, and very low-level replication persists [4,11]. Laboratory reports often classify results into three categories: “Target Not Detected” (<LOD), “<LOQ” (detectable but not quantifiable), or a specific numerical value within the linear range. A major issue in clinical practice and research is being utilized the erroneous application of the LOQ value instead of the LOD. This variability frequently results in inconsistent outcomes across various studies and misinterpretation by laboratory specialists and clinicians so influences clinical decision-making. Positive PCR findings may be achieved sometimes above the detection limit (>LOD) but below the quantification limit (<LOQ). It is essential for identifying missed OBI diagnoses, diagnostic discrepancies and evaluating CHB progression risk in some case under the therapy [9,15]. It is also crucial for assessing the risk of occult HBV infection (OBI) reactivation or transmission. This limitation restricts clinicians to determining the presence of HBV DNA in the patient’s blood, which may lead to misinterpretation of findings suggestive of OBI.
The objective of our study is to examine very low-level viremia below the quantification threshold in HBV DNA assays and its contributing factors for diagnostic and therapeutic monitoring, thereby establishing a foundation for a deeper comprehension of the significance of viral load between >LOD and <LOQ in clinical practice. Additionally, our study seeks to interfere with the misinterpretation of significant results between the detection limit and quantification limit, taking into account the diagnostic sensitivity of HBV DNA tests, and to examine the impact of these results on the OBI detection rate when assessed alongside Anti-HBe and other serological markers.
2. Materials and Methods
2.1. Study Design, Measurements and Ethical Approval
This study performed a retrospective analysis of data from patients who attended the infectious diseases, gastroenterology, and some other internal medicine clinics at Gulhane Training and Research Hospital in Ankara Province. Plasma samples sent for laboratory diagnosis and viral load assessment of Hepatitis B from January 2020 to October 2025 was incorporated into the retrospective investigation. The analysis encompassed factors such as gender, age, reason for visit/initial diagnosis, HBV serological markers, including HBsAg, anti-HBs, anti-HBe, anti-HBc and HBV DNA test results.
HBV DNA was quantified by real-time fluorescent quantitative polymerase chain reaction (qPCR), considering the analytical sensitivity and detection limits of the assay. Amplification was carried out on plasma samples using the Montania 4896 Real-Time PCR system (Anatolia Geneworks, Turkey), while serological markers were assessed in serum samples using the chemiluminescent microparticle immunoassay (CMIA) method on the Cobas e801 analyzer (Roche Diagnostics, Mannheim, Germany) and the Architect i2000sr system (Abbott, USA).
HBV serological assays acquired from using the CMIA method on Architect i2000sr and Cobas e801 instruments, HBsAb <10 IU/mL, HBsAg <1.00 S/CO, HBeAb >1.00 S/CO were classified as negative. While HBcAb <1.00 S/CO test results are evaluated as negative on Architect system, on the Cobas e801 analyzer a S/CO value >1.0 was regarded as positive due to competitive binding process.
The limit of detection (LOD) by PROBIT at a 95% hit rate for this detection method is <10 IU/mL when analyzing 400 μL of plasma. The anticipated linear range of test kit HBV extends from the limit of quantification (LOQ) at 10 IU/mL in a 400 μL sample volume to the upper limit of quantitation at 1.00E + 09 IU/mL. All experimental procedures and analyses were conducted in strict accordance with the protocols, following the manufacturer’s instructions. The test results are presented in the subsequent formats: Target Not identified (<LOQ), or HBV DNA was identified within a value in the linear range where LOQ<x <ULOQ.
We screened 390 patients with VLLV. The main requirements for inclusion were (i) being at least 18 years old; (ii) having chronic HBV infection under antiviral medication for years; (iii) patients with biochemical abnormalities believed to be associated with hepatocellular diseases from the clinicians’ perspective. The exclusion criteria; encompassed concurrent infection with viruses other than HBV such as HIV and hepatitis C, were not included. And also unavailable data was excluded.
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Health Sciences University-Gülhane Scientific Research (decision no: 2025-592) on December 23, 2025.
2.2. Description of OBI Diagnosis and SVR Group in the Study
The serological diagnosis of OBI is characterized by the absence of HBsAg and the presence of detectable HBV DNA in the serum or plasma. In this study, the findings of single high-sensitivity HBV DNA testing were analyzed independently for participants who underwent multiple tests. For the purposes of this study, the CHB group was classified as the SVR group due to the history of antiviral therapy screening routine follow-up.
2.3. Statistical Analysis
Statistical analyses were conducted utilizing GraphPad Prism programme 10.6.1 (892) at a 95% confidence level. The Shapiro–Wilk test and visual methods (histogram/Q-Q plot) were used to check how continuous data were spread out. Variables that were regularly distributed were shown as mean ± SD, while variables that were not normally distributed were shown as median (IQR). And for categorical variables, counts (n) or percentages (%) were applied, with comparisons conducted using the paired chi-square test. Variables with p values less than 0.10 in univariate analysis were incorporated into multivariate logistic regression analysis to identify independent factors for OBI and SVR groups.
A multivariate logistic regression analysis was employed to assess the correlation between HBV DNA levels under the LOQ (VLLV) and serological/demographic factors within the OBI and SVR groups. Independent variables include anti-HBe (±), total anti-HBc (±), anti-HBs (±), age <50 (years), age ≥50 (years), and gender (male/female). The results were given as OR, 95% CI, and p-value.
3. Results
3.1. Summary of Baseline Characteristics of the Patients
This retrospective study conducted from january 2020 to october 2025 comprised a total of 390 patients: 193 in the SVR group, 197 other group. Other groups consist of 60 OBI (HBV DNA–positive and HBsAg negative) and 137 non-OBI patients. CHB patients receiving antiviral treatment were classified as the SVR group. All result exhibits VLLV below the LOQ. Groups for SVR, OBI and non-OBI; the fundamental demographic attributes and serum virological marker of all participants are shown clearly in Table 1. The mean age of all CHB patients was 49.1 years, with 52.8% being male. Patients with VLLV were primarily male (n = 208; 53.3%) and 247 (63.3%) were aged 50 and over years. Likewise, the non-OBI group consisted mainly of males (n = 78; 56.9%); 82 (59.9%) were older 50 years of age. OBI and non-OBI patient groups had some clinical features such as previous or resolved HBV infection, cirrhosis, abnormal liver function tests of unidentified etiology, diabetes mellitus (DM), liver disease, hepatocellular carcinoma and high level hepatic function chemistry parameters, involving alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin, gamma-glutamyl transpeptidase (GGT), alpha-fetoprotein (AFP), lactate dehydrogenase (LDH) and alkaline phosphatase (ALP).
3.2. Comparison of Specific Characteristics within OBI and SVR Groups
The results of the univariate analysis indicated significant differences in age ≥50 years between OBI, and non-OBI groups. On the other hand when compared the SVR and non-SVR status; it was concluded that univariate analysis showed significant differences in age older than 50. Likewise the other parameters including sex, Anti-HBe, Anti-HBc and Anti-HBs status were calculated separately in univariate analysis (Table 2 and Table 3). Indicators having a p value <0.1 in the univariate analysis were incorporated into the multivariate logistic regression model to examine the correlational factors for VLLV in patients with OBI, and SVR group.
3.3. Variables of OBI and Non-OBI Groups
In the univariate analysis, we observed a significant correlation between the incidence of OBI and HBeAb seropositivity (odds ratio (OR) =2.874, 95% confidence interval (CI): 1.256- 6.172, p =0.012), as well as HBcAb (OR =2.368; 95% CI: 1.216-4.527, p =0.008) and age in years ≥50 (OR =1.845, 95% CI: 0.963-3.473, p =0.077) projects, as detailed in Table 2. Furthermore, male sex, and HBsAb levels exhibited no correlation with the incidence of OBI patients with VLLV. In multivariable logistic regression analysis, patients in age ≥50 years, Anti-HBe and Anti-HBc positivity remained independently associated with OBI (OR =4.055, 95% CI: 2.236-6.981, p = 0.044; OR =7.893, 95% CI: 4.117-12.660, p =0.005; OR =11.410, 95% CI: 4.149-26.180, p <0.001 respectively). Anti-HBs positivity and sex were not independently associated with OBI.
3.4. Analysis of Specific Factors Among SVR Patients
The univariate analysis of SVR individuals exhibiting VLLV, a substantial correlation existed between the occurrence of VLLV and some characteristics, including older age ≥50 years, anti-HBc positivity (OR =0.596, 95%CI: 0.396-0.888, p =0.014; OR =13.76, 95%CI: 3.69-59.56, p <0.001 consequently). However, anti-HBs positivity, anti-HBe, and sex did not exhibit any associations with the incidence of VLLV in the SVR group (Table 3). When observed the results in multivariate analysis; SVR patients with older age ≥50 correlated with the occurrence of VLLV (OR =5.500, 95%CI: 2.087-12.547, p =0.019). HBcAb seropositivity elevated the probability of VLLV in SVR status (OR =21.180, 95% CI: 6.011-60.266, p <0.001) in comparison to the other groups. Nonetheless, no substantial correlation was observed between the occurrence of VLLV in SVR group and other variables, including male gender, HBeAb, and HBsAb seropositivity (Table 3). In other words; anti-HBe positivity, anti-HBs and sex variables were not independently associated with SVR groups exhibiting VLLV in the multivariate logistic regression analysis.
4. Discussion
This study examined the association between very low-level HBV viremia and serological markers, such as anti-HBe, anti-HBs, and total anti-HBc, alongside demographic characteristics in groups of OBI, non-OBI and SVR patients. In addition our research underscores the challenges of clinical management especially in instances of very low-level viremia in CHB patients undergoing nucleoside analog therapy, as well as in cases of occult HBV infection and non-OBI patients accompanying the existence of other prevalent liver conditions performed by highly sensitive HBV DNA assay.
Several academic studies indicate that persistent very low viral replication occurs in around one-third of patients despite efficient antiviral treatment, and that the incorrect application of LOD/LOQ values in the HBsAg-negative cohort results in a substantial diagnostic deficiency in OBI diagnosis [14]. While the principal objective in HBV management is the total suppression of viral replication, both studies highlight that specific virological markers (including elevated HBsAg or HBeAg levels, anti-HBc and anti-HBe status) are significant risk factors for low-level viral persistence in both CHB and OBI patients, thus emphasizing the necessity for a more dynamic monitoring approach [11,16,17]. The mechanisms driving the development of VLLV are inadequately comprehended and are probably affected by many circumstances. Prior research indicates possible correlations with the cccDNA reservoir [7], host immunological variables, nucleoside analog resistance and constraints, in addition to patient compliance [11]. Nonetheless, several baseline clinical features and virological data may operate as predictive indicators for the emergence of LLV. Kim et al. recognized baseline HBV DNA burden as a significant risk factor for LLV (18). Within the cohort examined by Li et al. [19], the proportion of patients with baseline HBV DNA ≥ 6.0 log10 IU/mL was substantially greater in the LLV group (63.8%) than in the CVR group (45.1%). In our study, we did not assess the correlation between the emergence of VLLV and baseline DNA levels. Our analysis evaluated the association between the emergence of VLLV and age factor, HBV biomarkers such as anti-HBc, anti-HBe, and anti-HBs. Our analysis revealed that in individuals aged 50 and older, the anti-HBc and anti-HBe factors were independently associated with the VLLV profile. Our findings are consistent with previous studies.
Various examination results suggest that in over 90% of OBI patients; the DNA concentration is often <20 IU/mL [15]. Inconsistencies in research findings may result from differences in defined limits of detection, although employing identical methodologies. Improper use of the LOD for HBV DNA detection kits will substantially impact the detection rate of occult hepatitis B infection. Pronier et al. [20] conducted a study revealing that out of 52 OBI cases, only 23 cases (44.2%, 23/52) exhibited HBV DNA levels ≥ 10 IU/mL, utilizing the lower limit of quantification (LOQ = 10 IU/mL) as the diagnostic criterion. Conversely, 29 cases (55.8%) were identified (detection limit unspecified) but could be overlooked as the test results were below 10 IU/mL. Incorrectly using LOQ as LOD and interpreting results below LOQ as negative for HBV DNA could lead to diagnostic error of OBI, necessitating our focus in clinical practice. Our findings indicate that when the limit of quantification is erroneously applied as the limit of detection, HBV DNA results for all patient groups in our study were reported as ‘target not detected.’ This finding may not be clinically significant for patients with SVR, as virological success achieved under antiviral therapy, together with very low-level viremia positivity or a negative (‘target not detected’) result, may be considered clinically equivalent from the clinician’s perspective. However, ensuring that OBI is not overlooked remains clinically important, particularly in high-risk groups and in the presence of underlying diseases or other predisposing factors.
Our study results demonstrate that, the prevalence of occult hepatitis B infection was 15.3% among all VLLV outpatients at the Gulhane Training and Research Hospital Medical Microbiology Department in Turkey. Among these cases, 85% of OBI (51 out of 60) were anti-HBc positive. When viewed from a different perspective among those who were anti-HBc-positive, 13.07% (51 out of 390) exhibited OBI. In the anti-HBc-positive cohort, the prevalence of OBI is affected by the presence of anti-HBe and anti-HBs; notably, larger detection rates occur in anti-HBe-positive individuals, whereas lower rates are observed in anti-HBs-positive people. These findings indicate that anti-HBe serves as both a risk and a protective factor for OBI, as supported by the multivariate analysis. Individuals who are anti-HBe–positive have a 7.89-fold higher relative risk of being diagnosed with OBI compared to those who are anti-HBe–negative. In light of these serological findings, anti-HBe should be considered an important factor when evaluating the risk of OBI in individuals with a history of HBV infection. In other words, our study demonstrates a clinically meaningful association between anti-HBe positivity and very low HBV DNA levels, consistent with the natural course of chronic HBV infection.
Numerous studies performed to assess the factors affecting low-level viral replication in chronic hepatitis B patients on extended entecavir therapy [4,21]. In a study conducted by Chen et al. clinical data were collected from chronic hepatitis B patients who had received entecavir treatment for at least one year. At the end of the observation period, patients were divided into two groups based on their HBV DNA levels: low-level viremia with 180 cases and SVR with 337 cases. The results showed that there were big differences between the LLV and SVR groups in terms of age, gender, cirrhosis status, HBeAg positivity rate, pre-treatment baseline HBV DNA load, and baseline HBsAg level. It has been observed that 20.0% to 37.9% of CHB patients on first-line antiviral medication have LLV [21]. This finding suggests that the initial viral load and serological markers have a stronger and more long-lasting effect on treatment efficacy. And probably it stems not only from treatment adherence but also from a complex interaction between viral characteristics and host immunological regulation, both of which could contribute to partial viral suppression. Although it is known that all the SVR group in our research consisted of patients diagnosed with CHB who were under treatment follow-up and the SVR group consisted entirely of patients exhibiting the VLLV pattern rather than including patients in the CHB group with LLV (<2000 IU/mL). Consequently, we cannot estimate the proportion of CHB patients on antiviral therapy who exhibit a VLLV pattern. However we thought that our findings are useful in terms of clinician’s perspective.
Considering that the age and viral dynamics in recent studies; the connection between age and VLLV presumably reflects the cumulative impact of immune control over time. In normally older individuals are more frequently in HBeAg-negative phase, characterized by reduced replication levels [22,23]. However, this link may indicate an extended host–virus adaptation, in which ongoing immunological pressure gradually reduces replicative activity without achieving complete viral eradication. The intricate dynamics of immunological maturation, antigen exposure, and potential immunological exhaustion likely affects the VLLV/LLV phenotype across different age groups. Our study offers that anti-HBe and anti-HBc positivity increases in correlation with age. In addition, our multivariate analysis findings confirmed that individuals aged 50 and older were a risk factor for the OBI (OR:4.055, 95%CI: 2.236-6.981, p=0.044) and SVR groups (OR:5.500, 95%CI: 2.087-12.547, p=0.019). We believe this findings may be related to the influence of immune exhaustion and host factors. This study comprehensively evaluated the viro-serologic profile of patients with very low-level HBV viremia and determined that anti-HBe and anti-HBc positivity and advanced age (≥50) were independently associated with lower HBV DNA levels within the VLLV spectrum, whereas anti-HBs and gender status did not act as an independent predictor after multivariable adjustment. Our findings suggest that anti-HBe positivity is associated with a lower likelihood of viral replication. However, the presence of anti-HBs does not necessarily indicate complete viral suppression. From a clinical perspective, careful monitoring of patients with very low-level viremia—particularly those with persistently low-level replication—remains essential, even when favorable serological markers are present.
4.1. Limitations
This study has several limitations. First, its retrospective design limits the ability to draw causal inferences. Second, the sample size of the OBI cohort exhibiting a very low-level viremia pattern was insufficient. Third, treatment conditions and duration may have influenced viral dynamics, and long-term clinical outcomes were not evaluated. Fourth, quantitative measurements of anti-HBc and intrahepatic markers—particularly relevant to OBI—were not available. Finally, the findings related to the VLLV pattern were not replicated with a new sample or re-test.
5. Conclusion
Among individuals with low-level HBV viremia, anti-HBc and anti-HBe seropositivity and older age were independently correlated with lower HBV DNA levels; conversely, anti-HBs status did not independently forecast very low viral load. Very low levels of HBV DNA in anti-HBe–positive patients suggest that this marker reflects an active immune response rather than complete viral eradication. Although anti-HBe seropositivity is generally associated with suppression of viral replication and transition to the immune control phase, it does not exclude the presence of persistent low-level viral activity, particularly in cases of OBI. Therefore, anti-HBe status should not be interpreted in isolation but rather in conjunction with HBV DNA levels and other serological markers in clinical practice.
Careful evaluation for OBI is particularly important in anti-HBc positive individuals. These findings highlight the complex relationship between viral replication and host immune response in the VLLV spectrum and support the need for individualized monitoring strategies. The clinical significance of VLLV is not yet fully understood and requires further research. The advancement of nucleic acid detection technologies may enhance the monitoring of DNA levels and facilitate the identification of additional VLLV pattern. Due to the lack of comparison information about the advantages of either maintaining the original treatment or altering the method for patients with VLLV, additional clinical research are necessary to elucidate these alternatives.
References
- World Health Organization. Global Hepatitis Report 2024: Action for Access in Low- and Middle-Income Countries; WHO: Geneva, Switzerland, 2024. Available online: https://www.who.int/publications/i/item/9789240091672 (accessed on 31 August 2024).
- Xie, L.; Liu, G.; Liu, Y.; Li, P.; Guo, H. Prevalence of low-level viremia in the treatment of chronic hepatitis B in China: a systematic review and meta-analysis. BMJ Open 2025, 15, e088756. [CrossRef]
- Han, J.; Guo, Y.; Zhang, X.; Zhang, Y.; Sun, J.; He, J.; Mao, R.; Huang, Y.; Zhang, J. Prevalence and associated factors of low-level viremia in chronic hepatitis B patients after long-term therapy with nucleos(t)ide analogs. Turk. J. Gastroenterol. 2023, 34, 53–61. [CrossRef]
- Yin, G.Q.; Li, J.; Zhong, B.; Yang, Y.F.; Wang, M.R. New therapeutic options for persistent low-level viremia in patients with chronic hepatitis B virus infection: increase of entecavir dosage. World J. Gastroenterol. 2021, 27, 666–676. [CrossRef]
- Amponsah-Dacosta, E.; Selabe, S.G.; Mphahlele, M.J. Evolution of the serologic and virologic course of occult HBV infection in therapy experienced HIV co-infected patients. J. Med. Virol. 2018, 90, 291–303. [CrossRef]
- Thu, H.H.K.; Ostankova, Y.V.; Shchemelev, A.N.; Serikova, E.N.; Davydenko, V.S.; Ton, T.; Lien, T.T.X.; Ramsay, E.S.; Totolian, A.A. Unveiling the Hidden Reservoir: High Prevalence of Occult Hepatitis B and Associated Surface Gene Mutations in a Healthy Vietnamese Adult Cohort. Microorganisms 2026, 14, 238. [CrossRef]
- Allweiss, L.; Dandri, M. The Role of cccDNA in HBV Maintenance. Viruses 2017, 9, 156. [CrossRef]
- Sun, F.; Liu, Z.; Wang, B. Correlation between low-level viremia and hepatitis B-related hepatocellular carcinoma and recurrence: a retrospective study. BMC Cancer 2021, 21, 1103. [CrossRef]
- Zhang, Q.; Peng, H.; Liu, X.; Wang, H.; Du, J.; Luo, X.; Ren, H.; Hu, P. Chronic hepatitis B infection with low level viremia correlates with the progression of the liver disease. J. Clin. Transl. Hepatol. 2021, 9, 850–859. [CrossRef]
- Sun, Y.; Wu, X.; Zhou, J.; Meng, T.; Wang, B.; Chen, S.; Liu, H.; Wang, T.; Zhao, X.; Wu, S.; Kong, Y.; Ou, X.; Wee, A.; Theise, N.D.; Qiu, C.; Zhang, W.; Lu, F.; Jia, J.; You, H. Persistent low level of hepatitis B virus promotes fibrosis progression during therapy. Clin. Gastroenterol. Hepatol. 2020, 18, 2582–2591.e6. [CrossRef]
- Zhang, Q.; Cai, D.C.; Hu, P.; Ren, H. Low-level viremia in nucleoside analog-treated chronic hepatitis B patients. Chin. Med. J. 2021, 134, 2810–2817. [CrossRef]
- Im, Y.R.; Jagdish, R.; Leith, D.; Kim, J.U.; Yoshida, K.; Majid, A.; Ge, Y.; Ndow, G.; Shimakawa, Y.; Lemoine, M. Prevalence of occult hepatitis B virus infection in adults: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 932–942. [CrossRef]
- Wang, C.; Xue, R.; Wang, X.; Xiao, L.; Xian, J. High-sensitivity HBV DNA test for the diagnosis of occult HBV infection: commonly used but not reliable. Front. Cell. Infect. Microbiol. 2023, 13, 1186877. [CrossRef]
- Wang, B.; Wang, X.; Xiao, L.; Xian, J. Misuse of the lower limit of detection in HBV DNA testing and anti-HBe positive status will significantly impact the diagnosis of occult HBV infection. J. Viral Hepat. 2025, 32, e14046. [CrossRef]
- Saitta, C.; Pollicino, T.; Raimondo, G. Occult Hepatitis B Virus Infection: An Update. Viruses 2022, 14, 1504. [CrossRef]
- Jiang, X.; Tian, J.; Song, L.; Meng, J.; Yang, Z.; Qiao, W.; Zou, J. Multi-omic molecular characterization and diagnostic biomarkers for occult hepatitis B infection and HBsAg-positive hepatitis B infection. Front. Endocrinol. 2024, 15, 1409079. [CrossRef]
- Wang, B.; Zeng, T.; Yin, W.; Ren, C.; Chen, Y.; Qian, L.; Huang, P.; Zhu, C.; Yue, M. Unveiling low level viremia in chronic hepatitis B: challenges and new horizons. Front. Cell. Infect. Microbiol. 2025, 15, 1663858. [CrossRef]
- Kim, T.S.; Sinn, D.H.; Kang, W.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W. Hepatitis B virus DNA levels and overall survival in hepatitis B-related hepatocellular carcinoma patients with low-level viremia. J. Gastroenterol. Hepatol. 2019, 34, 2028–2035. [CrossRef]
- Li, Z.B.; Chen, D.D.; Jia, Y.F.; He, Q.J.; Cui, L.; Du, F.X.; Kang, Y.J.; Feng, X.; He, M.; Jin, X.Y.; Chen, J.; Wang, Y.; Ji, D.; Lau, G.; Wu, S.G. Risk factors related to low-level viraemia in chronic hepatitis B patients receiving entecavir treatment. Front. Cell. Infect. Microbiol. 2024, 14, 1413589. [CrossRef]
- Pronier, C.; Candotti, D.; Boizeau, L.; Bomo, J.; Laperche, S.; Thibault, V. The contribution of more sensitive hepatitis B surface antigen assays to detecting and monitoring hepatitis B infection. J. Clin. Virol. 2020, 129, 104507. [CrossRef]
- Chen, H.; Fu, J.J.; Li, L.; Wang, X.; Pan, X.C. Risk factors of low-level viremia in chronic hepatitis B patients receiving entecavir monotherapy: a retrospective cohort study. J. Gastroenterol. Hepatol. 2024, 39, 180–184. [CrossRef]
- Lu, J.; Zhang, C.; He, P.; Ou, M.; Xia, J.; Huang, M. Risk factors for very low-level viremia in patients with chronic hepatitis B virus infection: a single-center retrospective study. Liver Res. 2022, 6, 39–44. [CrossRef]
- Wu, J.; Yu, Y.; Dai, Y.; Zhang, Y.; Cheng, J. Research progress on the mechanism of persistent low-level HBsAg expression in the serum of patients with chronic HBV infection. J. Immunol. Res. 2022, 2022, 1372705. [CrossRef]

Table 1.
Baseline characteristics of CHB, OBI and non-OBI groups with VLLV under LOQ.
| Variable | All group (n=390) | CHB group (n=193) | OBI group (n=60) | Non-OBI group (n=137) |
| Age, years (mean±sd) | 50.9±14.2 | 49.1±13.7 | 55.6±12.6 | 51.5±14.7 |
| <50 years, n (%) | 143 (36.7) | 72 (37.3) | 16 (26.7) | 55 (40.1) |
| ≥50 years, n (%) | 247 (63.3) | 121 (62.7) | 44 (73.3) | 82 (59.9) |
| Gender | ||||
| Male, n (%) | 208 (53.3) | 102 (52.8) | 28 (46.7) | 78 (56.9) |
| Female, n (%) | 182 (46.7) | 91 (47.2) | 32 (53.3) | 59 (43.1) |
| HBcAb status | ||||
| Negative, n (%) | 89 (22.8) | 2 (1) | 9 (15) | 69 (50.4) |
| Positive, n (%) | 301 (77.2) | 191 (99) | 51 (85) | 68 (49.6) |
| HBeAb status | ||||
| Negative, n (%) | 79 (20.3) | 29 (15) | 8 (13.3) | 42 (30.7) |
| Positive, n (%) | 311 (79.7) | 164 (85) | 52 (86.7) | 95 (69.3) |
| HBsAb status | ||||
| Negative, n (%) | 310 (79.5) | 189 (97.9) | 42 (70) | 79 (57.7) |
| Positive, n (%) | 80 (20.5) | 4 (2.1) | 18 (30) | 58 (42.3) |
Abbreviations: VLLV, very low-level viremia; LOQ, limit of quantification; HBsAb, hepatitis B surface antibody; HBeAb, hepatitis B e antibody; HBcAb, hepatitis B core antibody; CHB, chronic hepatitis B; OBI, occult HBV infection; SD, standard deviation.
Table 2.
Comparison of specific variables within OBI and non-OBI populations by logistic regression analysis.
Table 2.
Comparison of specific variables within OBI and non-OBI populations by logistic regression analysis.
| Variables | Univariate analysis | Multivariate analysis | |||||||
| OR (95% CI) | P-value | OR (95% CI) | P-value | ||||||
| Age (years) ≥50 vs <50 Sex Male vs Female Anti-HBe Pos. vs Neg. Anti-HBc Pos. vs Neg. Anti-HBs Pos. vs Neg. |
1.845 (0.963-3.473) 1.511 (0.806-2.728) 2.874 (1.256- 6.172) 2.368 (1.216-4.527) 0.583 (0.304-1.089) |
0.077 0.215 0.012 0.008 0.113 |
4.055 (2.236-6.981) / 7.893 (4.117-12.66) 11.41 (4.149-26.18) / |
0.044 / 0.005 <0.001 / |
|||||
Abbreviations: ‘/’, not available. Abbreviations: OR, odds ratio; CI, confidence interval; OBI, occult hepatitis B infection. Variables clinically relevant in univariate analysis (p <0.10) were entered into the multivariable logistic regression model.
Table 3.
Determinants of SVR groups categorized by logistic regression analysis.
| Variables | Univariate analysis | Multivariate analysis | |||||||
| OR (95% CI) | P-value | OR (95% CI) | P-value | ||||||
| Age (years) ≥50 vs <50 Sex Male vs Female Anti-HBe Pos. vs Neg. Anti-HBc Pos. vs Neg. Anti-HBs Pos. vs Neg. |
0.596 (0.396-0.888) 1.265 (0.853-1.882) 1.505 (0.884- 2.545) 13.76 (3.69-59.56) 0.170 (0.062-0.482) |
0.014 0.264 0.144 <0.001 0.176 |
5.500 (2.087-12.547) / / 21.18 (6.011-60.266) / |
0.019 / / <0.001 / |
|||||
Abbreviations: OR, odds ratio; CI, confidence interval; OBI, occult hepatitis B infection; SVR, sustained virological response. Variables with p <0.10 in univariate analysis were included in the multivariable model. Patients with chronic hepatitis B (CHB) under treatment were classified as the SVR group for analysis. ‘/’ means not available.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



