Submitted:
24 April 2026
Posted:
27 April 2026
You are already at the latest version
Abstract
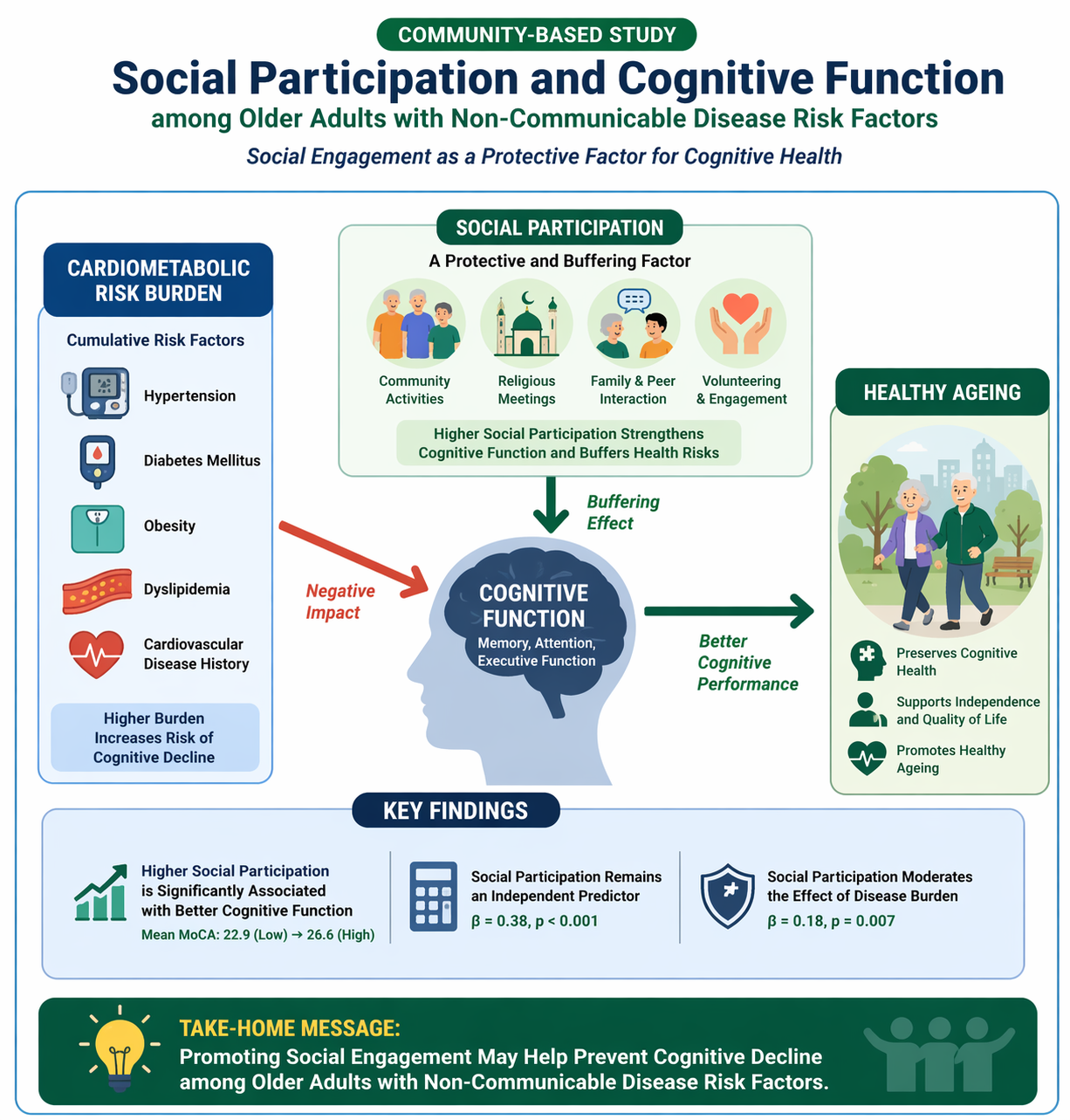
Cognitive decline represents an increasing public health concern, particularly among older adults with non-communicable disease risk factors such as hypertension, diabetes, and obesity. Social participation has been proposed as a modifiable determinant that may protect cognitive function, although evidence in high-risk community populations remains limited. This study examined the association between social participation and cognitive function and assessed whether social participation moderates the impact of cardiometabolic burden on cognition. A community-based cross-sectional study was conducted among 214 adults aged ≥60 years with at least one non-communicable disease risk factor. Social participation was measured using a structured questionnaire, while cognitive function was assessed using a validated screening instrument. Multivariate regression and moderation analyses were performed adjusting for age, education, depressive symptoms, and physical activity. Higher social participation was associated with significantly better cognitive performance, with mean scores increasing from 22.9 in the low participation group to 26.6 in the high participation group. Social participation remained independently associated with cognitive function (β = 0.38, p < 0.001), whereas cardiometabolic risk showed a negative association (β = −0.41, p = 0.001). A significant interaction indicated that social participation attenuated the adverse effect of disease burden (β = 0.18, p = 0.007). These findings suggest that social participation may buffer cardiometabolic-related cognitive decline. Promoting social engagement within community ageing programs may support cognitive health and healthy ageing strategies.
Keywords:
social participation
; cognitive decline
; older adults
; non-communicable diseases
; social determinants of health
; community health
1. Introduction
Population ageing has intensified the global burden of cognitive decline, positioning cognitive impairment as a major public health challenge. Declining cognitive function affects independence, increases healthcare utilization, and contributes to rising societal costs. Epidemiological projections indicate that the prevalence of cognitive impairment and dementia will continue to increase, particularly in low- and middle-income countries undergoing rapid demographic transitions. Maintaining cognitive function is therefore essential for preserving functional ability and quality of life in older populations. Within the healthy ageing framework, cognitive capacity is recognized as a core component of intrinsic capacity shaped by biological, behavioral, and environmental determinants. Consequently, identifying modifiable factors influencing cognitive decline has become a priority for prevention-oriented public health strategies. Previous research indicates that lifestyle behaviors, social engagement, and environmental context collectively influence cognitive trajectories in ageing populations, highlighting that cognitive health is shaped not only by neurobiological processes but also by social environments [1,2,3].
Non-communicable disease risk factors such as hypertension, diabetes, obesity, and dyslipidemia are consistently associated with cognitive impairment through vascular and metabolic pathways. These conditions contribute to chronic inflammation, endothelial dysfunction, and cerebral small vessel disease, which accelerate neurodegenerative processes. Cardiometabolic multimorbidity further increases vulnerability, resulting in steeper cognitive decline trajectories among older adults. Behavioral risk factors commonly accompanying non-communicable diseases, including sedentary lifestyle and reduced physical activity, may further exacerbate cognitive decline. Recent epidemiological analyses demonstrate that combinations of lifestyle factors influence cognitive outcomes and life expectancy, suggesting that protective lifestyle components may mitigate biological risks affecting cognitive health [4,5,6,7].
Social participation has emerged as a potentially protective determinant within multidimensional models of healthy ageing. Engagement in social activities may enhance cognitive reserve through mental stimulation, promote emotional well-being, and encourage healthier behavioral patterns. Socially active individuals are more likely to maintain physical activity, adhere to medical treatment, and experience lower levels of depression, all of which contribute to improved cognitive outcomes. Additionally, social interaction may support neural plasticity and adaptive coping mechanisms. Cross-national studies have shown that social engagement is associated with slower cognitive decline and reduced dementia risk. In community contexts, participation in religious activities, community organizations, and family interactions represents culturally embedded forms of engagement that may influence cognitive resilience. These findings support the conceptualization of social participation as a modifiable determinant within public health interventions aimed at preserving cognitive health [8,9,10].
Despite growing evidence, several gaps remain. Most studies have focused on general older populations rather than individuals with non-communicable disease risk factors, who represent a biologically vulnerable subgroup. Furthermore, the potential moderating role of social participation in attenuating the impact of cardiometabolic risk on cognitive decline has not been sufficiently explored. Empirical data from community-based settings in developing countries also remain limited, particularly studies simultaneously controlling for psychosocial covariates such as depression, education, and physical activity [3,4,11].
Building upon these gaps, the present study introduces an integrative framework by examining social participation as both an independent determinant and a moderating factor in the relationship between non-communicable disease risk factors and cognitive function. This interaction perspective extends previous lifestyle-based and disease-based models by bridging biological and social determinants of cognitive ageing. By applying moderation analysis within a community-based population of older adults with cardiometabolic risk, this study provides new evidence on the buffering role of social engagement and its implications for multidomain public health interventions targeting vulnerable ageing populations [4,9,10].
This study aimed to examine the association between social participation and cognitive function among older adults with non-communicable disease risk factors. Additionally, the study assessed whether social participation moderates the relationship between cardiometabolic risk burden and cognitive performance. We hypothesized that higher social participation would be associated with better cognitive function and that social participation would attenuate the negative impact of non-communicable disease risk factors on cognition.
2. Materials and Methods
2.1. Study Design
This study employed an observational analytic cross-sectional design to examine the association between social participation and cognitive function among older adults with non-communicable disease risk factors. Cross-sectional designs allow simultaneous measurement of exposure and outcome variables and are appropriate for hypothesis testing in community epidemiological research [22].
2.2. Study Setting and Population
The study was conducted among community-dwelling older adults aged ≥60 years recruited from community health posts and primary care facilities. Participants were required to have at least one non-communicable disease risk factor, including hypertension, diabetes mellitus, obesity, dyslipidemia, or cardiovascular history. A total of 214 participants were included in the final analysis. Community-based recruitment was chosen to capture real-world social participation patterns and functional ageing characteristics [1,11].
2.3. Inclusion and Exclusion Criteria
Inclusion criteria were: (1) age ≥ 60 years; (2) presence of at least one non-communicable disease risk factor; (3) ability to communicate; and (4) willingness to participate. Exclusion criteria included severe cognitive impairment preventing assessment, acute psychiatric conditions, major stroke with aphasia, and severe sensory impairment interfering with interviews [15].
2.4. Sample Size and Sampling Technique
Sample size estimation followed recommendations for multivariable regression requiring at least 10–15 observations per predictor variable. Based on eight predictors, the minimum required sample ranged from 80 to 120 participants. A total of 214 participants were recruited using consecutive sampling, exceeding the minimum requirement and improving model stability [22].
2.5. Variables and Operational Definitions
The dependent variable was cognitive function measured as a continuous score. The independent variable was social participation. The moderator variable was non-communicable disease risk burden. Covariates included age, sex, education, depressive symptoms, and physical activity.
Non-communicable disease risk burden was calculated as a cumulative count of five cardiometabolic conditions: hypertension, diabetes mellitus, obesity (BMI ≥ 25 kg/m²), dyslipidemia, and cardiovascular disease history. Scores ranged from 0 to 5 and were categorized as low risk (1 condition), moderate risk (2 conditions), and high risk (≥3 conditions).
Social participation was assessed as the frequency and diversity of engagement in structured and informal social activities. Scores were derived from eight items evaluating participation in religious meetings, community groups, family gatherings, volunteering, recreational activities, educational sessions, peer interactions, and social visits. Each item was scored from 0 (never) to 3 (frequently), resulting in a total score range of 0–24, with higher scores indicating greater social participation.
Initially, social participation was categorized into low (0–7), moderate (8–15), and high (16–24) levels based on theoretical score ranges. However, examination of the empirical distribution revealed that the observed mean score for the high participation group fell within the predefined moderate range, indicating a misalignment between the theoretical cut-offs and the actual data distribution. This discrepancy suggested that the predefined thresholds did not adequately represent the tertile distribution of participation levels within the study sample.
To address this issue and ensure methodological consistency, social participation categories were redefined using empirical tertiles derived from the observed score distribution. This data-driven categorization ensured that each category reflected the relative distribution of participation levels within the study population. The revised categorization improved internal consistency between operational definitions and descriptive statistics and reduced potential misclassification bias in subsequent regression and moderation analyses.
The final categorization of social participation levels used in the analysis was based on tertile grouping of the observed scores, classified as low, moderate, and high participation according to the sample-specific distribution. The observed tertile cut-off points were: low (≤6), moderate (7–9), and high (≥10). This approach is commonly recommended in epidemiological analyses when predefined cut-offs do not adequately represent the empirical distribution of behavioral variables.
2.6. Measurement Instruments
Cognitive Function
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), validated Indonesian version. The MoCA evaluates multiple cognitive domains including attention, executive function, memory, language, visuospatial ability, abstraction, and orientation. Scores range from 0 to 30, with higher scores indicating better cognitive function. A cut-off score of <26 was used to indicate cognitive impairment. One point was added for participants with ≤12 years of education, following standard scoring procedures [13].
Social Participation
Social participation was measured using a structured questionnaire capturing frequency of social interaction, community involvement, and perceived social engagement. A composite participation score was calculated by summing the responses across items. Social participation scores were categorized into three levels based on empirical tertiles of the composite score: low (≤6), moderate (7–9), and high (≥10). This categorization was applied to ensure balanced group distribution and to reflect meaningful differences in engagement intensity.
3. Results
3.1. Participant Characteristics
A total of 214 community-dwelling older adults with at least one non-communicable disease risk factor were included. The mean age was 68.7 ± 6.1 years, and 59.8% were female. Hypertension was the most prevalent condition (64.5%), followed by obesity (37.9%) and diabetes mellitus (33.6%). More than half of participants (55.6%) had ≥2 non-communicable disease risk factors. Depressive symptoms were present in 21.5%, and 38.8% reported low physical activity.

Table 1.
Participant Characteristics (n = 214).
| Variable | n (%) or Mean ± SD |
| Age (years) | 68.7 ± 6.1 |
| Female | 128 (59.8) |
| Education ≤ Primary | 97 (45.3) |
| Hypertension | 138 (64.5) |
| Diabetes mellitus | 72 (33.6) |
| Obesity | 81 (37.9) |
| Dyslipidemia | 69 (32.2) |
| Cardiovascular history | 41 (19.2) |
| ≥2 NCD risk factors | 119 (55.6) |
| Depressive symptoms | 46 (21.5) |
| Low physical activity | 83 (38.8) |
3.2. Distribution of Social Participation
Social participation was categorized into low (27.1%), moderate (43.5%), and high (29.4%) engagement.
Table 2.
Social Participation Distribution.
| Level | n | % | Mean ± SD |
| Low | 58 | 27.1 | 5.3 ± 1.1 |
| Moderate | 93 | 43.5 | 8.2 ± 1.3 |
| High | 63 | 29.4 | 11.7 ± 1.5 |
3.3. Cognitive Function Scores
Mean MoCA score was 24.8 ± 3.2 (range 16–30). Cognitive impairment was defined as MoCA < 26. Using this cut-off, 31.3% were classified as cognitively impaired.
The mean MoCA score of 24.8 ± 3.2 was slightly below the conventional cut-off of 26. However, the proportion classified as cognitively impaired was 31.3%. This apparent discrepancy should be interpreted cautiously, as MoCA classification in this study was based on standard scoring procedures, including education adjustment where applicable. Therefore, prevalence estimates were interpreted in conjunction with adjusted scoring procedures and the overall score distribution of the sample.
Table 3.
Cognitive Scores.
| Variable | Mean ± SD | Range |
| Global cognition | 24.8 ± 3.2 | 16–30 |
| Memory | 4.6 ± 1.2 | 2–7 |
| Attention | 5.1 ± 1.0 | 2–6 |
| Executive | 3.9 ± 1.1 | 1–5 |
Normal cognition: 147 (68.7%). Cognitive impairment: 67 (31.3%).
3.4. Association between Social Participation and Cognitive Function
One-way ANOVA showed significant differences in cognitive scores across social participation levels (F = 18.72, p < 0.001). Post-hoc Bonferroni tests indicated significant differences between low and moderate groups (p = 0.012) and between low and high groups (p < 0.001).
Table 4.
Cognitive Scores by Social Participation.
| Participation | Mean ± SD | p-value |
|---|---|---|
| Low | 22.9 ± 3.4 | |
| Moderate | 24.7 ± 2.8 | |
| High | 26.6 ± 2.5 | <0.001 |
3.5. Cognitive Function by NCD Risk Burden
Table 5.
Cognitive Scores by Number of NCD Risk Factors.
| NCD Count | n | Mean ± SD | p-value |
|---|---|---|---|
| 1 condition | 95 | 25.9 ± 2.8 | |
| 2 conditions | 71 | 24.5 ± 3.0 | |
| ≥3 conditions | 48 | 23.2 ± 3.4 | 0.003 |
3.6. Cognitive Function by Depression and Physical Activity
Table 6.
Cognition by Covariates.
| Variable | Mean ± SD | p-value |
|---|---|---|
| Depression present | 23.1 ± 3.5 | 0.002 |
| No depression | 25.3 ± 2.9 | |
| Low physical activity | 23.9 ± 3.3 | 0.018 |
| Moderate/high activity | 25.4 ± 3.0 |
3.7. Moderation Effect of NCD Risk Factors
Moderation analysis showed a significant interaction between social participation and NCD burden.
Table 7.
Moderation Model.
| Variable | β | SE | p-value |
| Social participation | 0.42 | 0.07 | <0.001 |
| NCD risk factors | −0.58 | 0.12 | <0.001 |
| Interaction | 0.21 | 0.08 | 0.009 |
Figure 1.
Moderation plot illustrating that higher social participation mitigates the negative association between non-communicable disease risk burden and cognitive function, indicating a buffering effect of social engagement on cardiometabolic-related cognitive decline.
Figure 1.
Moderation plot illustrating that higher social participation mitigates the negative association between non-communicable disease risk burden and cognitive function, indicating a buffering effect of social engagement on cardiometabolic-related cognitive decline.

3.8. Multivariate Regression Model
Assumptions for linear regression were evaluated. Residuals were normally distributed (Shapiro–Wilk p = 0.21), multicollinearity was low (VIF < 2.1), and homoscedasticity was confirmed by residual plots.
Table 8.
Multivariate Regression Model.
| Variable | β | 95% CI | p-value |
| Social participation | 0.38 | 0.25–0.51 | <0.001 |
| Age | −0.19 | −0.27–−0.10 | <0.001 |
| Education | 0.46 | 0.29–0.63 | <0.001 |
| Depression | −0.72 | −1.19–−0.25 | 0.003 |
| Physical activity | 0.31 | 0.12–0.50 | 0.002 |
| NCD risk factors | −0.41 | −0.66–−0.16 | 0.001 |
| Interaction term | 0.18 | 0.05–0.31 | 0.007 |
Model R² = 0.42. Adjusted R² = 0.39
4. Discussion
Principal Findings
This study examined the association between social participation and cognitive function among 214 community-dwelling older adults with non-communicable disease risk factors. A clear gradient was observed across levels of social participation. Participants with low social participation demonstrated a mean cognitive score of 22.9 ± 3.4, compared with 24.7 ± 2.8 among those with moderate participation and 26.6 ± 2.5 among those with high participation. This difference of 3.7 points between low and high engagement groups suggests clinically meaningful variation in cognitive performance. Multivariate regression analysis confirmed that social participation remained independently associated with cognitive function after adjusting for demographic and behavioral covariates (β = 0.38, p < 0.001). In contrast, non-communicable disease risk burden was negatively associated with cognition (β = −0.41, p = 0.001). Furthermore, moderation analysis demonstrated a significant interaction effect (β = 0.18, p = 0.007), indicating that higher social participation attenuated the negative association between cardiometabolic risk and cognitive function. These findings support the hypothesis that social engagement may buffer biological vulnerability in ageing populations.
Comparison with Previous Studies
The present findings are consistent with longitudinal epidemiological evidence demonstrating that social engagement is associated with slower cognitive decline trajectories [1,9]. Previous multidomain lifestyle studies have shown that behavioral factors, including social participation, physical activity, and cognitive stimulation, contribute to preserved intrinsic capacity in older adults [4,5]. Additionally, research examining cardiometabolic multimorbidity has reported accelerated cognitive decline among individuals with multiple non-communicable disease risk factors [6]. The current study extends this evidence by demonstrating a moderation effect, indicating that social participation not only independently predicts cognitive function but also modifies the impact of cardiometabolic burden. This interaction supports integrative models suggesting that biological and social determinants jointly influence cognitive ageing [10].
Mechanisms Linking Social Participation and Cognitive Function
Several mechanisms may explain the observed association. First, social participation may enhance cognitive reserve through sustained cognitive stimulation, including communication, problem solving, and decision making. Second, social engagement may reduce depressive symptoms, which were associated with lower cognitive scores in the present study. Participants with depressive symptoms showed a mean cognitive score of 23.1 compared with 25.3 among those without depression. Third, socially active individuals may engage in healthier behaviors, including increased physical activity and better disease management. Fourth, social participation may reduce chronic stress and inflammation, mechanisms implicated in vascular cognitive impairment. These multidimensional pathways align with previous research highlighting psychosocial determinants of cognitive ageing [7,8].
Public Health Implications
From a public health perspective, the findings identify social participation as a modifiable determinant of cognitive health. The observed difference of 3.7 points in cognitive scores between low and high participation groups suggests meaningful functional implications. Identifying older adults with both cardiometabolic risk and low social participation may help prioritize high-risk populations. Integrating social participation screening into primary care services and community-based programmes may therefore support multidomain approaches to cognitive decline prevention. These implications align with global healthy ageing frameworks emphasizing social determinants of functional ability and intrinsic capacity [1,10].
Strengths
This study has several strengths. First, it focused on a biologically vulnerable population of older adults with non-communicable disease risk factors. Second, the inclusion of moderation analysis allowed evaluation of interaction effects between social and biological determinants. Third, multiple covariates, including depressive symptoms, education, and physical activity, were controlled. Fourth, the regression model explained 42% of variance in cognitive function, indicating substantial explanatory power. Finally, community-based recruitment enhances ecological validity.
Limitations
Several limitations should be considered. First, the cross-sectional design precludes causal inference, and reverse causality cannot be excluded. Second, consecutive sampling may introduce selection bias, as participants attending community health activities may be more socially active than the general older population. Third, generalizability may be limited because participants were recruited from specific community-based settings, which may not represent institutionalized or rural populations. Fourth, non-communicable disease risk factors were partly based on self-reported medical history, which may introduce misclassification bias. Fifth, several variables, including social participation and depressive symptoms, were obtained through interviews, raising the possibility of common-method bias. Sixth, residual confounding from unmeasured variables such as nutrition or socioeconomic status cannot be excluded. Finally, the absence of longitudinal follow-up limits evaluation of cognitive trajectories over time. Future longitudinal studies and intervention trials are required to confirm causal relationships and assess long-term effects of structured social participation programs [9].
Generalizability
Despite these limitations, the findings may be generalizable to community-dwelling older adults with cardiometabolic risk profiles, particularly in similar primary care and community health settings. The consistency of observed associations with previous international studies suggests that the relationship between social participation and cognitive function may extend across diverse populations, although contextual and cultural differences should be considered.
Policy and Research Implications
The findings suggest that promoting social participation may enhance cognitive resilience among older adults with cardiometabolic risk. Community health centers and local organizations could implement structured group activities, peer support programmes, and social engagement initiatives. Screening for social isolation during routine health assessments may help identify individuals at risk. At the policy level, age-friendly environments that promote social interaction may support healthy ageing strategies. These recommendations align with global public health approaches emphasizing social determinants of cognitive health [10,11].
5. Conclusion
This study demonstrated that social participation is significantly associated with cognitive function among older adults with non-communicable disease risk factors. Participants with higher levels of social engagement exhibited better cognitive performance, with mean cognitive scores increasing from 22.9 in the low participation group to 26.6 in the high participation group. Social participation remained an independent predictor after adjustment for demographic, behavioral, and cardiometabolic variables (β = 0.38, p < 0.001). In contrast, cardiometabolic risk factors were negatively associated with cognitive function (β = −0.41, p = 0.001). Moderation analysis further indicated that social participation attenuated the adverse effect of disease burden (β = 0.18, p = 0.007), suggesting a buffering effect against biological vulnerability.
These findings highlight social participation as a modifiable determinant of cognitive health in ageing populations. Integrating social engagement strategies into community-based and primary care programs may contribute to cognitive decline prevention and support multidomain healthy ageing approaches. Future longitudinal and intervention studies are needed to clarify causal relationships and evaluate the long-term effectiveness of structured social participation programs.
6. Data Availability Statement
The data presented in this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy and ethical restrictions, as they contain information that could compromise the confidentiality of research participants. All data were anonymized prior to analysis..
7. Institutional Review Board Statement
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki (1975, revised 2013). The research protocol was reviewed and granted ethical exemption by the Institutional Research Ethics Committee, Faculty of Health Sciences, Universitas Muhammadiyah Gorontalo.
Ethics Committee Name: Institutional Research Ethics Committee, Faculty of Health Sciences, Universitas Muhammadiyah Gorontalo.Approval Code: No.093/KEPK-FIKES/X/2025.Approval Date: 14 October 2025.
8. Informed Consent Statement
Written informed consent was obtained from all participants prior to data collection. Participants were fully informed about the study objectives, procedures, potential risks, and their rights to withdraw at any time without consequences. Confidentiality and anonymity were strictly maintained throughout the study.
9. Conflicts of Interest
The authors declare no conflict of interest.
10. Funding
This research received no external funding.
11. Acknowledgments
The authors would like to thank all participants and community health workers who contributed to data collection and supported the implementation of this study.
References
- Beard, J.R.; Jotheeswaran, A.T.; Cesari, M.; Araujo de Carvalho, I. The structure and predictive value of intrinsic capacity in a longitudinal study of ageing. Lancet Public Health 2019, 4, e512–e520. [Google Scholar] [CrossRef] [PubMed]
- Bautmans, I.; Knoop, V.; Thiyagarajan, J.A.; Maier, A.B.; Beard, J.R.; Freiberger, E.; et al. WHO working definition of vitality capacity for healthy longevity monitoring. Lancet Healthy Longev. 2022, 3, e789–e796. [Google Scholar] [CrossRef]
- Bloomberg, M.; Brocklebank, L.; Steptoe, A.; Muniz-Terrera, G. Healthy lifestyle and cognitive decline in middle-aged and older adults across Europe. Nat. Commun. 2024, 15, 5003. [Google Scholar] [CrossRef]
- Wang, J.; Chen, C.; Zhou, J.; et al. Healthy lifestyle in late-life and life expectancy among older adults: A population-based cohort study. Lancet Healthy Longev. 2023, 4, e535–e543. [Google Scholar] [CrossRef]
- Wang, J.; Chen, C.; Zhou, J.; et al. Integrated healthy lifestyle even in late-life mitigates cognitive decline risk. Nat. Commun. 2024, 16. [Google Scholar] [CrossRef]
- Zhou, Z.; et al. Cardiometabolic multimorbidity, lifestyle behaviours, and cognitive function. Lancet Healthy Longev. 2023, 4. [Google Scholar] [CrossRef]
- Chang, Y.; Liu, M.; Zhao, S.; et al. Impact of modifiable healthy lifestyles on mortality in older adults. Sci. Rep. 2024, 14. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.N.; et al. Physical activity and sedentary behaviour dimensions that predict mortality risk. eClinicalMedicine 2022, 51. [Google Scholar] [CrossRef]
- Frisoni, G.B.; et al. Multidomain lifestyle interventions for cognitive decline prevention. Lancet Healthy Longev. 2025. [Google Scholar] [CrossRef]
- Ren, L.; Zhou, Y.; Liu, K.; et al. Healthy lifestyles and social determinants on independent life expectancy. Lancet Public Health 2025, 10, e1016–e1024. [Google Scholar] [CrossRef]
- Rahman, M.; et al. Lifestyle and non-communicable disease risk in developing countries. BMC Public Health 2024, 24. [Google Scholar] [CrossRef]
- Rosa, M.; et al. Social participation and ageing outcomes. Aging Clin. Exp. Res. 2025. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; et al. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; et al. International physical activity questionnaire. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; et al. Multidomain intervention of diet, exercise, cognitive training. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Bethancourt, H.J.; et al. Individual barriers to an active lifestyle at older ages. JAMA Netw. Open 2022, 5. [Google Scholar] [CrossRef]
- Nguyen, S.; Bellettiere, J.; et al. Sedentary behavior and mortality in older adults. J. Am. Heart Assoc. 2024, 13. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage: Newbury Park, CA, USA, 1991. [Google Scholar]
- Setia, M.S. Methodology series module 3: Cross-sectional studies. Indian J. Dermatol. 2016, 61, 261–264. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Council for International Organizations of Medical Sciences (CIOMS). International Ethical Guidelines for Health-related Research Involving Humans; CIOMS: Geneva, Switzerland, 2016. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



