Submitted:
17 April 2026
Posted:
21 April 2026
You are already at the latest version
Abstract
Congestion is the main driver of symptoms, hospitalization, and adverse outcomes in heart failure (HF), yet its clinical assessment remains suboptimal. Traditional ap-proaches, largely focused on estimating intravascular volume through clinical exami-nation, biomarkers, or inferior vena cava assessment, fail to capture the complexity of venous congestion and its impact on organ function.
Emerging evidence supports a paradigm shift from a static, volume-centered view to a dynamic, physiology-based model in which congestion is defined by elevated ve-nous pressure, impaired organ drainage, and its interaction with systemic perfusion.
In this context, point-of-care ultrasound (POCUS) has gained increasing attention as a tool for bedside evaluation of congestion. The Venous Excess Ultrasound (VExUS) score integrates inferior vena cava assessment with Doppler analysis of hepatic, portal, and intrarenal veins, providing a comprehensive evaluation of systemic venous con-gestion at the organ level.
VExUS has been shown to correlate with invasive hemodynamic parameters and to identify patients at increased risk of acute kidney injury, rehospitalization, and mortal-ity. Importantly, dynamic changes in VExUS appear to carry greater prognostic signif-icance than single measurements.
This review provides a pathophysiological and clinical paradigm for understanding venous congestion in HF, with a focus on the role of VExUS and multimodal ultrasound.
By shifting the focus from fluid quantity to venous pressure and organ perfusion, this approach may improve congestion assessment, risk stratification, and therapeutic guidance.
Keywords:
acute heart failure
; heart failure
; venous congestion
; VExUS
; point-of-care ultrasound
; cardiorenal syndrome
; intrarenal venous Doppler
; lung ultrasound
; decongestive therapy
; diuretic
1. Introduction
Heart failure (HF) remains a leading cause of morbidity and hospitalization worldwide, with congestion representing the primary driver of symptoms, disease progression, and adverse outcomes [1]. Despite advances in pharmacological and device-based therapies, the persistence of congestion continues to account for a substantial proportion of rehospitalizations and mortality [2]. Notably, residual congestion at the time of discharge has been consistently associated with worse clinical outcomes, even in patients deemed clinically stable [3].
Traditionally, the assessment of congestion in HF has relied on a combination of clinical examination, invasive hemodynamic measurements, and surrogate imaging or biochemical markers. However, each of these approaches carries significant limitations [4]. Physical examination lacks sensitivity and reproducibility, often failing to detect early or subclinical congestion. Invasive measures such as central venous pressure (CVP) provide only a partial representation of systemic hemodynamics and do not reliably reflect organ-level congestion. Similarly, echocardiographic surrogates such as inferior vena cava (IVC) diameter offer limited specificity, while biomarkers capture cardiac wall stress but do not directly quantify venous congestion or its impact on end-organ function [5,6].
These limitations highlight a fundamental issue in contemporary HF management: the incomplete characterization of venous congestion. Congestion is often conceptualized as a simple excess of intravascular volume, yet accumulating evidence suggests a far more complex pathophysiological process. Venous congestion reflects the interplay between cardiac function, venous return, and organ-specific drainage, ultimately leading to elevated venous pressures and impaired organ perfusion. This process may occur independently of overt volume overload and may not be adequately captured by conventional diagnostic tools [7,8].
In this context, point-of-care ultrasound (POCUS) has emerged as a promising modality for the bedside assessment of congestion. Among the available techniques, the Venous Excess Ultrasound (VExUS) score represents a novel, integrative approach that combines Doppler assessment of the IVC, hepatic, portal, and intrarenal veins to quantify systemic venous congestion [9]. By directly evaluating venous flow patterns across multiple organ systems, VExUS provides a physiologically grounded assessment of congestion that extends beyond traditional measures [10].
VExUS has been shown to correlate with invasive hemodynamic parameters, including right atrial pressure, and to identify patients at increased risk of adverse outcomes, particularly acute kidney injury and rehospitalization [11,12]. Furthermore, dynamic changes in VExUS over time appear to carry greater prognostic significance than single measurements, underscoring the importance of serial assessment in clinical practice [13]. These observations support a paradigm shift from a static, volume-centered view of congestion to a dynamic, physiology-based one driven by venous pressure and organ-level dysfunction.
This review aims to provide a pathophysiological and clinical paradigm for understanding venous congestion in heart failure, with a particular focus on the role of VExUS and multimodal ultrasound in improving its assessment, prognostic stratification, and therapeutic guidance.
2. Materials and Methods
A structured literature search was performed using PubMed to identify relevant studies from inception to March 2026, without any language restriction. The search strategy included combinations of keywords such as “heart failure”, “venous congestion”, “VExUS”, “point-of-care ultrasound”, “cardiorenal syndrome”, “renal Doppler”, “lung ultrasound”. Additional references were identified through manual screening of the bibliographies of selected articles. Eligible studies included original research articles, observational cohort studies, systematic reviews, and meta-analyses addressing the mechanisms, diagnostic assessment, and clinical impact of venous congestion. Particular attention was given to studies evaluating Doppler-based ultrasound techniques, including VExUS and intrarenal venous flow assessment, as well as investigations exploring the relationship between congestion, organ dysfunction, and clinical outcomes.
Priority was given to contemporary studies reflecting current clinical practice and advances in ultrasound-based assessment. Abstract-only publications were considered when providing relevant or emerging data but were interpreted with caution. Study selection and data interpretation were performed with a focus on methodological consistency and clinical relevance.
Given the narrative nature of the review, no formal meta-analytic techniques or quantitative pooling of results were undertaken. The available evidence was synthesised to provide a mechanism-based, clinically oriented framework linking diagnostic modalities to coronary endotypes and targeted management strategies.
3. Rethinking Congestion: Beyond Volume Overload
For decades, congestion in heart failure has been predominantly conceptualized as a consequence of volume overload. This paradigm, although clinically intuitive, fails to capture the complexity of the underlying hemodynamic and organ-level interactions that characterize congestive states. Emerging evidence suggests that congestion is not merely the result of excess intravascular volume, but rather the expression of an altered equilibrium between cardiac function, venous return, and organ-specific drainage [14].
A central determinant of congestion is right atrial pressure, which reflects the downstream resistance encountered by venous return [15]. Elevated right atrial pressure increases systemic venous pressure and is transmitted retrogradely to the venous circulation of multiple organs, including the kidneys, liver, and splanchnic system. This retrograde transmission of pressure, rather than absolute volume, represents a key driver of organ dysfunction (7,16). In this context, the concept of retrograde venous afterload provides a useful conceptual approach to understand the pathophysiology of congestion.
As venous pressures rise, the pressure gradient between arterial inflow and venous outflow is reduced, leading to impaired organ perfusion despite preserved or only mildly reduced cardiac output [17]. This mechanism is particularly evident at the renal level, where increased venous pressure directly reduces renal perfusion pressure and glomerular filtration, independently of systemic arterial hypotension [7,18].
Venous congestion may occur even in the absence of overt fluid overload. Clinical and experimental observations indicate that patients with similar degrees of volume expansion may exhibit markedly different levels of congestion depending on cardiac function, vascular compliance, and neurohormonal activation [19]. In particular, the redistribution of blood volume within the splanchnic compartment plays a crucial role, acting as a dynamic reservoir that can acutely increase central venous pressures without a significant change in total body fluid [8,20].
These considerations challenge the traditional dichotomy between “volume overload” and “euvolemia,” suggesting that congestion should instead be interpreted as a hemodynamic state characterized by elevated venous pressures and impaired venous drainage. In line with this view, studies have shown that markers of venous congestion, rather than cardiac output, are more closely associated with organ dysfunction, particularly acute kidney injury [16].
Recent data suggest that venous congestion assessed by ultrasound may reflect underlying cardiac function more than intravascular volume alone. In critically ill populations, VExUS has been shown to correlate with cardiac performance parameters, supporting the concept that congestion represents the downstream manifestation of cardiac dysfunction rather than a purely volumetric phenomenon [21].
Another key aspect of congestion is its interaction with systemic perfusion. The relationship between perfusion and congestion is not mutually exclusive but deeply interconnected. Patients may simultaneously exhibit elevated venous pressures and reduced forward flow, resulting in a combined state of congestion and hypoperfusion [22]. This interaction has important clinical implications, as therapies targeting only one component, such as diuretics for volume reduction or inotropes for cardiac output, may fail to adequately address the underlying pathophysiology.
Finally, the dynamic nature of congestion must be emphasized. Congestion is not a static condition but a fluctuating process that evolves in response to treatment and disease progression [23]. Changes in congestion over time, assessed through serial ultrasound evaluation, have been shown to carry greater prognostic significance than single timepoint measurements, highlighting the limitations of snapshot-based assessment [13,24].
These observations support a fundamental shift in the conceptualization of congestion in heart failure: from a static model of fluid accumulation to a dynamic, multi-dimensional process driven by venous pressure, organ-level dysfunction, and their interaction with systemic perfusion.
The key differences between traditional and contemporary conceptualizations of congestion are summarized in Table 1.
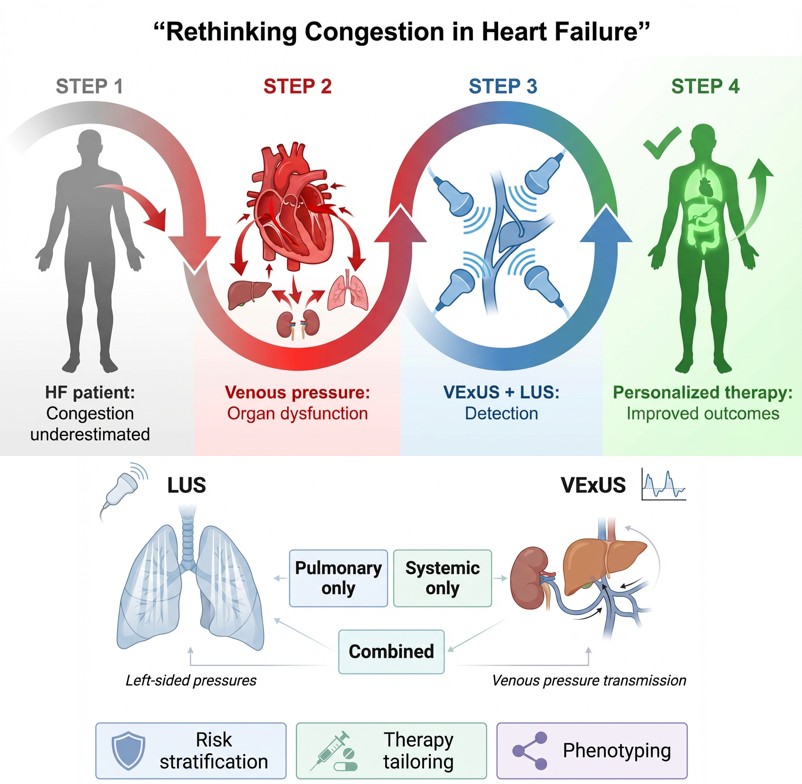
The transition from a volume-centered interpretation of congestion to a dynamic model based on venous pressure transmission and organ dysfunction is schematically summarized in Figure 1.
4. The Concept of Organ-Relevant Congestion
A critical limitation of traditional approaches to congestion lies in the implicit assumption that all forms of congestion are clinically equivalent. In reality, increasing evidence indicates that not all congestion is clinically relevant, and that its clinical impact is largely determined by its effects at the level of individual organs [25].
Among the various organ systems involved, the kidney represents the most extensively studied and clinically relevant target of venous congestion. In the context of acute heart failure, renal dysfunction has traditionally been attributed to reduced cardiac output and impaired arterial perfusion.
However, this paradigm has been increasingly challenged by data demonstrating that venous congestion plays a central, and often dominant, role in the development of acute kidney injury [16,18].Intrarenal Doppler studies have provided key insights into this mechanism. Under normal conditions, renal venous flow is continuous, reflecting unobstructed venous drainage [25]. In contrast, elevated right atrial and systemic venous pressures lead to progressive alterations in intrarenal venous flow patterns, ranging from biphasic to monophasic discontinuous flow [26].
These abnormalities reflect increasing renal venous stasis and congestion and have been shown to correlate with both the presence and severity of acute kidney injury and, importantly, occur independently of cardiac output. In patients with acute decompensated heart failure, abnormal intrarenal venous flow patterns have been observed despite similar cardiac index values, highlighting that renal dysfunction may arise primarily from impaired venous outflow rather than reduced arterial inflow [18]. This observation fundamentally shifts the understanding of cardiorenal syndrome, emphasizing the role of backward pressure transmission rather than forward flow limitation.
The pathophysiological consequences of venous congestion on renal function can be interpreted as a reduction in the effective renal perfusion gradient, defined as the difference between arterial inflow and venous outflow pressure. As venous pressure rises, this gradient progressively narrows, impairing glomerular filtration despite preserved systemic arterial pressure or only mildly reduced cardiac output.
This mechanism, illustrated in Figure 2, further supports the concept that renal dysfunction in heart failure is often driven by backward pressure transmission rather than by reduced forward flow.
The concept of congestive nephropathy reinforces this perspective. Clinical studies have shown that venous congestion is associated with reduced diuretic efficiency and worsening renal function, suggesting a direct pathophysiological link between elevated venous pressures and renal dysfunction [27].
In parallel, multimodal approaches integrating ultrasound and biomarkers have identified a substantial proportion of patients with congestion-driven renal impairment, supporting the clinical relevance of this entity [28].
Another important implication is the temporal dissociation between organ congestion and conventional markers of organ dysfunction. Structural and hemodynamic alterations at the organ level often precede measurable changes in laboratory parameters [29]. In particular, abnormal intrarenal venous flow patterns may be detected before any rise in serum creatinine, indicating that organ congestion represents an early and potentially reversible stage of injury [30].
This has direct clinical consequences. Reliance on delayed markers such as creatinine may lead to under-recognition of early congestion-related injury and inappropriate therapeutic decisions. In clinical practice, worsening renal function is often interpreted as a consequence of hypoperfusion, prompting reduction or discontinuation of diuretic therapy. However, in the presence of persistent venous congestion, such an approach may be detrimental, as it fails to address the primary driver of renal dysfunction [18].
Beyond the kidney, similar principles apply to other organ systems. Hepatic and splanchnic congestion, reflected by alterations in portal and hepatic venous flow, contribute to systemic inflammation, intestinal edema, and impaired drug absorption [31].
The splanchnic compartment, in particular, acts as a dynamic reservoir that modulates venous return and central pressures, further influencing the development and progression of congestion [8].
The clinical relevance of congestion extends beyond the acute setting. Studies in ambulatory HF populations have shown that subclinical congestion, detectable only through ultrasound-based techniques, is associated with a significantly increased risk of rehospitalization and adverse outcomes [32]. These findings suggest that clinically silent congestion may represent an underrecognized therapeutic target across the spectrum of heart failure.
All these observations support a shift toward an organ-centered model of congestion, in which the clinical significance of congestion is determined by its impact on organ function rather than by global estimates of volume status. In this construct, the assessment of venous congestion should aim to identify early, organ-specific alterations that precede overt dysfunction and guide targeted therapeutic interventions.
This perspective provides a strong rationale for the use of Doppler-based ultrasound techniques, including VExUS and intrarenal venous assessment, which enable direct visualization of congestion at the organ level and allow for a more precise characterization of its clinical relevance.
5. VexUS: Technical Principles and Interpretation
The VExUS score is a structured POCUS protocol designed to assess and quantify systemic venous congestion and its impact on peripheral organs. By integrating morphological assessment of the IVC with Doppler evaluation of multiple venous territories, VExUS provides a comprehensive evaluation of venous congestion at both central and organ levels [33].
From a technical standpoint, ultrasound acquisition should ideally be performed at end-expiration in order to minimize the influence of intrathoracic pressure variations on venous return and Doppler signals [34]. When feasible, simultaneous electrocardiographic monitoring may facilitate accurate temporal interpretation of venous Doppler waveforms, particularly in distinguishing systolic and diastolic components [7].
5.1. Inferior Vena cava
The assessment of the IVC represents the initial step of the VExUS protocol [35]. Measurement of IVC diameter is typically performed in the subcostal view, and a diameter greater than 2 cm and/or reduced inspiratory collapsibility < 50% suggests elevated right atrial pressure [36]. However, reliance on IVC diameter alone is limited by multiple confounding factors that may affect its accuracy independently of intravascular volume status.
These include respiratory mechanics, particularly in patients undergoing positive pressure ventilation, as well as vigorous inspiratory efforts, which can significantly alter venous return. In addition, conditions such as cirrhosis, portal hypertension, and significant tricuspid regurgitation may influence IVC size and collapsibility independently of systemic congestion [37,38]. These limitations highlight the need for complementary assessment of downstream venous flow.
5.2. Hepatic Veins
Hepatic vein Doppler interrogation is typically performed using subcostal or lateral acoustic windows. Under normal conditions, hepatic venous flow is pulsatile and reflects right atrial pressure variations, with a predominant systolic (S) wave over the diastolic (D) component [7].
With increasing venous congestion, the systolic component progressively decreases, eventually becoming smaller than the diastolic wave, and in advanced stages may reverse direction entirely. These changes reflect the direct transmission of elevated right atrial pressure to the hepatic venous system. Interpretation may be limited in the presence of conditions such as severe tricuspid regurgitation, atrial fibrillation, or intrinsic liver disease, which can independently alter Doppler morphology [39].
5.3. Portal Vein
Portal vein flow is normally continuous and minimally pulsatile. In the presence of systemic venous congestion, right atrial pressure oscillations are transmitted to the splanchnic circulation, resulting in increased pulsatility of portal flow. This phenomenon can be quantified using the pulsatility index, calculated as (Vmax − Vmin) / Vmax × 100% [39].
Progressive increases in pulsatility reflect worsening congestion, although interpretation must consider confounding factors. Advanced cirrhosis may alter portal flow patterns independently of systemic congestion [40]. Furthermore, portal vein pulsatility is influenced by a complex interplay between cardiac function, splanchnic capacitance, and volume status, and may therefore be observed even in non-congested states under specific physiological conditions [20,21,34].
5.4. Intrarenal Venous Doppler
Intrarenal venous Doppler provides a direct assessment of the impact of venous congestion on renal hemodynamics. Examination is typically performed using a lateral approach at the mid-axillary line, targeting interlobar veins, which provide optimal Doppler alignment [39,41].
In euvolemic conditions, intrarenal venous flow is continuous and monophasic. With increasing venous congestion, flow becomes biphasic and discontinuous, reflecting partial impedance to venous outflow. In severe congestion, systolic flow may disappear entirely, resulting in a discontinuous monophasic pattern with flow limited to the diastolic phase [33].
Interpretation of renal venous flow is influenced by both systemic and local factors. These include renal interstitial edema, reduced vascular compliance, decreased arterial inflow, and increased intra-abdominal pressure, all of which may affect venous outflow independently of systemic volume status [42]. In addition, technical limitations related to vessel size and sampling location may affect measurement accuracy.
5.5. VExUS Scoring System
The final VExUS grade is determined by integrating IVC assessment with Doppler findings from the hepatic, portal, and intrarenal veins. A normal IVC diameter (≤2 cm) generally excludes significant systemic venous congestion, whereas a dilated IVC (>2 cm) prompts further evaluation using Doppler analysis [41].
In the presence of a dilated IVC, congestion severity is graded according to the extent and severity of Doppler abnormalities across venous territories. Mild congestion is characterized by normal or minimally altered Doppler patterns, while moderate and severe congestion are defined by progressively abnormal waveforms, including systolic reversal in hepatic veins, marked portal pulsatility, and discontinuous intrarenal flow [36].
The main technical components and Doppler interpretation of the VExUS protocol are summarized in Table 2.
Figure 3 provides a schematic overview of the VExUS protocol, including the main venous territories assessed and the progressive waveform abnormalities associated with increasing congestion severity.
5.6. Interpretation and Physiological Integration
Although initially conceptualized as a tool to assess volume status, VExUS should be interpreted within a broader hemodynamic framework. Doppler abnormalities reflect the retrograde transmission of venous pressure to peripheral organs and therefore represent markers of congestion-related organ dysfunction rather than simple intravascular volume excess [43].
Importantly, VExUS integrates multiple physiological determinants, including cardiac function, venous compliance, and intravascular volume. As a result, high VExUS grades may be observed in patients with cardiac dysfunction even in the absence of overt fluid overload, while conversely, patients with positive fluid balance may not exhibit severe congestion in the presence of preserved cardiac function [44,45].
These observations underscore the need for careful clinical interpretation. VExUS should not be viewed as a direct surrogate of volume status, but rather as a marker of the inability of the cardiovascular system to accommodate circulating volume at acceptable filling pressures [46]. Consequently, its interpretation should always be integrated with assessment of biventricular function and global hemodynamics [21].
5.7. Extension and Alternative Approaches
Recent developments have explored simplified or extended approaches to venous congestion assessment. Doppler interrogation of the femoral vein has been proposed as a technically simpler alternative, demonstrating moderate correlation with VExUS grading [36,47]. Similarly, extended VExUS (e-VExUS) approaches incorporating additional venous territories, such as the superior vena cava or splenic vein, have been described in cases where conventional windows are not available [48].
However, while these approaches may improve feasibility, their clinical role remains to be fully defined.
6. VExUS vs. Other Congestion Assessment Tools
The evaluation of congestion in heart failure has traditionally relied on a combination of clinical examination, imaging surrogates, and biochemical markers. However, each of these tools captures only a limited component of the congestive process, often resulting in incomplete or misleading assessments [49].
In this context, the emergence of VExUS highlights the limitations of conventional approaches and supports a more integrative evaluation of systemic venous congestion.
Clinical examination remains the first-line method for assessing congestion but is intrinsically limited by low sensitivity and significant interobserver variability. Signs such as peripheral edema, jugular venous distension, and pulmonary rales often appear late in the course of disease and may be absent in patients with subclinical congestion [50].
Importantly, a substantial proportion of patients considered clinically decongested at discharge continue to exhibit evidence of congestion when assessed with ultrasound, which is associated with a significantly increased risk of rehospitalization [3].
Among imaging tools, IVC diameter is widely used as a surrogate of right atrial pressure. Although simple and rapid to obtain, IVC assessment provides only a central estimate of venous pressure and does not reflect downstream organ congestion [51]. As a result, patients with similar IVC findings may have markedly different degrees of organ-level involvement, limiting its specificity for clinically relevant congestion [10]. Furthermore, recent data showed that venous congestion may be present even in patients with IVC diameters below conventional thresholds and that alternative morphological indices, such as the inferior vena cava shape change index, may provide improved diagnostic performance compared with diameter alone [52].
In contrast, by directly assessing the hemodynamic consequences of elevated venous pressures at the organ level, VExUS improves the identification of clinically relevant congestion compared with isolated parameters. Comparative studies have shown that while simplified venous Doppler indices may offer higher sensitivity, integrated approaches such as VExUS provide greater specificity for predicting organ dysfunction and adverse outcomes [36].
Lung ultrasound (LUS) represents a complementary modality that specifically assesses pulmonary congestion [53]. The presence of B-lines reflects extravascular lung water and has been consistently associated with adverse outcomes in heart failure [54]. However, LUS primarily captures left-sided filling pressures and does not provide information on systemic venous congestion. Consequently, discordant patterns may occur, with patients exhibiting significant systemic congestion in the absence of pulmonary edema, or vice versa.
This distinction between pulmonary and systemic congestion is clinically relevant. Pulmonary congestion is predominantly driven by elevated left-sided pressures, whereas systemic congestion reflects right-sided hemodynamics and venous return impairment [55].
The dissociation between these compartments underscores the limitations of single-modality assessment and supports the need for integrated evaluation.
Recent studies have demonstrated that multimodal approaches combining different ultrasound techniques provide superior prognostic stratification compared with individual tools. In particular, the integration of VExUS with lung ultrasound significantly improves risk prediction, reflecting the multi-compartmental nature of congestion [28,56].
Furthermore, dynamic changes in pulmonary congestion, assessed by serial LUS, have been shown to carry important prognostic information, reinforcing the concept that congestion should be evaluated as a dynamic process rather than a static condition [24].
Biomarkers, including natriuretic peptides, remain essential for the diagnosis and risk stratification of heart failure. However, they primarily reflect myocardial wall stress and do not directly quantify venous congestion or its impact on organ function. Their levels may also be influenced by age, renal function, and comorbidities, limiting their specificity in the assessment of congestion [5].
Importantly, each modality captures a distinct compartment of congestion, and no single tool is sufficient to fully characterize its multi-organ nature. Collectively, these observations highlight a central limitation of traditional approaches: the risk of misclassification of congestion when relying on isolated parameters.
Patients may be categorized as decongested based on clinical examination or single-modality assessment while still harboring significant organ-level congestion. Conversely, abnormal findings in one compartment may not necessarily reflect clinically relevant congestion.
VExUS represents a significant advancement by enabling the direct assessment of systemic venous congestion across multiple organ systems. However, its optimal use lies not in replacing existing tools, but in complementing them within a multimodal approach that integrates pulmonary, systemic, and hemodynamic information.
The physiological domains captured by different modalities used in congestion assessment are summarized in Table 3.
7. Clinical Applications in Heart Failure
7.1. Acute Heart Failure
In the setting of acute heart failure (AHF), early identification and quantification of congestion are essential for risk stratification and therapeutic decision-making [57,58]. Conventional assessment strategies often fail to detect subclinical or organ-level congestion, particularly in the early phases of hospitalization. In this context, VExUS and multimodal ultrasound approaches provide a more sensitive and physiologically grounded evaluation of systemic venous congestion.
Several observational studies have demonstrated that higher degrees of venous congestion, as assessed by VExUS, are associated with worse clinical outcomes, including increased mortality and rehospitalization. In particular, severe congestion patterns have been linked to a markedly higher risk of in-hospital death and early readmission, outperforming traditional markers such as natriuretic peptides [59].
Similarly, VExUS grading has been shown to correlate with clinical severity and the need for more intensive decongestive therapy, reinforcing its role in early risk stratification [28]. Importantly, VExUS allows for the detection of congestion even in patients without overt clinical signs [33]. This is particularly relevant in the acute setting, where clinical examination may underestimate the true burden of congestion. The identification of subclinical congestion has prognostic implications, as patients with persistent venous congestion despite apparent clinical improvement are at increased risk of adverse outcomes [60].
In intensive care unit settings, VExUS has also been applied to critically ill patients with hemodynamic instability. While its prognostic performance appears stronger in cardiac populations, studies suggest that dynamic changes in venous congestion during the early phase of hospitalization may provide clinically relevant information even in heterogeneous ICU cohorts [13]. This highlights the importance of serial assessment rather than reliance on single measurements.
7.2. Cardiorenal Syndrome
The clinical relevance of venous congestion is particularly evident in the context of cardiorenal syndrome, where renal dysfunction is closely linked to elevated venous pressures [61]. Traditional interpretations have emphasized reduced cardiac output as the primary driver of renal impairment; however, accumulating evidence indicates that renal venous congestion plays a central role [62].
Ultrasound-based assessment of renal venous flow has provided key insights into this mechanism. Abnormal intrarenal Doppler patterns, reflecting impaired venous drainage, have been shown to correlate with the presence and severity of acute kidney injury, independently of cardiac output [18].
These findings support the concept that renal dysfunction in heart failure is largely driven by backward pressure transmission rather than forward flow limitation.
VExUS extends this concept by integrating renal venous assessment into a broader evaluation of systemic congestion. Studies in patients with cardiorenal syndrome have demonstrated that higher VExUS grades are associated with reduced diuretic efficiency and worsening renal function.
Conversely, improvement in venous congestion is associated with better renal outcomes, suggesting a direct pathophysiological link between congestion and kidney function [27].
The concept of congestive nephropathy emphasizes the importance of early detection. In many patients, renal dysfunction may represent a late manifestation of ongoing venous congestion [63]. Ultrasound-based markers, including intrarenal venous flow and VExUS grading, allow for the identification of early congestion-related alterations before changes in serum creatinine become apparent [30].
From a therapeutic perspective, this has important implications. Misinterpretation of renal dysfunction as a consequence of hypoperfusion may lead to inappropriate reduction of diuretic therapy, thereby perpetuating congestion [64]. In contrast, identifying venous congestion as the primary driver supports continued or intensified decongestive strategies, even in the presence of worsening renal function.
7.3. Guiding Decongestive Therapy
One of the most promising applications of VExUS lies in its potential to guide decongestive therapy through dynamic assessment of congestion. Unlike static parameters, ultrasound-based evaluation allows for real-time monitoring of the response to treatment, enabling a more individualized and physiologically guided approach.
Several studies have demonstrated that changes in venous congestion over time are more informative than baseline measurements. In particular, reductions in VExUS grade during hospitalization have been associated with improved clinical outcomes, while persistent or worsening congestion is linked to higher risk of adverse events, supporting the use of serial VExUS assessment as a tool for monitoring treatment response. [13,65].
The integration of VExUS into therapeutic decision-making may also improve the management of diuretic resistance. Venous congestion has been shown to impair renal sodium excretion and reduce the effectiveness of diuretic therapy, contributing to persistent volume overload [66]. By identifying patients with significant venous congestion, clinicians may optimize diuretic strategies or consider alternative approaches, such as ultrafiltration [67].
Furthermore, ultrasound-guided decongestion may help avoid both under- and over-treatment. In patients with persistent congestion, escalation of therapy may be warranted despite apparent clinical improvement. Conversely, normalization of venous flow patterns may indicate adequate decongestion, reducing the risk of excessive fluid removal and hemodynamic instability [68].
The role of VExUS in guiding fluid management extends beyond heart failure. Studies evaluating fluid challenges have shown that increases in venous congestion may occur without improvement in perfusion, highlighting the potential harm of indiscriminate fluid administration in patients with elevated venous pressures [69].
These findings reinforce the importance of assessing both congestion and perfusion when guiding therapy. The use of VExUS as a dynamic monitoring tool represents a shift toward a more precise and individualized approach to decongestive therapy, with the potential to improve both short- and long-term outcomes.
A practical strategy for integrating serial VExUS assessment into decongestive decision-making is proposed in Figure 4.
7.4. Current Evidence
The growing interest in venous congestion and ultrasound-based assessment has led to an expanding body of literature evaluating the prognostic and clinical relevance of VExUS and related Doppler techniques. While the available evidence is predominantly observational, it provides consistent signals supporting the role of venous congestion as a key determinant of outcomes in heart failure.
Multiple cohort studies have demonstrated a strong association between venous congestion and adverse clinical outcomes. Across different clinical settings, higher VExUS grades have been consistently linked to increased mortality, rehospitalization, and organ dysfunction. In acute heart failure populations, severe congestion patterns are associated with markedly worse outcomes, even after adjustment for traditional risk factors [28,59].
Importantly, these associations extend beyond static measurements. Several studies have highlighted that dynamic changes in congestion carry greater prognostic significance than baseline values.
Improvements in VExUS score during hospitalization have been associated with reduced mortality risk, whereas persistent or worsening congestion identifies patients at particularly high risk [13,65]. This finding has been reproduced across heterogeneous populations, including both cardiac and general ICU cohorts, suggesting that the trajectory of congestion is a key determinant of clinical evolution.
In addition to global VExUS grading, individual Doppler components also provide prognostic information. Abnormal portal vein pulsatility and intrarenal venous flow patterns have been associated with adverse outcomes, including in-hospital mortality and readmission [70].
However, studies comparing composite scores with individual parameters suggest that while single Doppler indices may be sensitive, integrated approaches such as VExUS improve specificity for clinically relevant congestion [47].
More recently, a meta-analysis evaluating the association between VExUS and acute kidney injury reported a significant increase in the risk of acute kidney injury (AKI) among patients with higher congestion grades, with an odds ratio of approximately 2.6 [12].
These findings reinforce the pathophysiological link between venous congestion and renal dysfunction observed in individual studies, but the strength of the association appears to vary across clinical contexts. The predictive value of VExUS is more pronounced in populations with primary cardiac dysfunction, whereas its performance is less consistent in heterogeneous intensive care unit (ICU) cohorts, where multiple competing mechanisms contribute to organ injury. This variability underscores the importance of clinical context when interpreting congestion-related findings.
7.5. Clinical Outcomes
Across studies, venous congestion has emerged as a strong predictor of mortality and heart failure–related outcomes. Patients with higher degrees of congestion at admission or discharge exhibit significantly higher rates of rehospitalization and death. Notably, the presence of residual congestion at discharge is particularly relevant, as it identifies a subgroup of patients at high risk despite apparent clinical stability [3].
These findings are consistent with large-scale clinical data showing that incomplete decongestion is common and associated with adverse outcomes. Importantly, reductions in body weight or clinical signs do not necessarily reflect true decongestion, suggesting that traditional markers may underestimate the persistence of congestion [71].
The relationship between venous congestion and renal dysfunction is one of the most consistently reported findings in the literature. Both individual studies and meta-analytic data support a strong association between elevated venous pressures and the development of acute kidney injury. Intrarenal Doppler abnormalities and higher VExUS grades have been linked to increased incidence and severity of AKI, reinforcing the concept of congestion-driven renal impairment [12,18].
Importantly, this association appears to be largely independent of cardiac output, further supporting the role of backward failure as a key mechanism in cardiorenal syndrome.
Another important aspect of the evidence relates to the response to decongestive therapy. Studies evaluating serial ultrasound assessments have shown that reductions in venous congestion are associated with improved outcomes, whereas persistent congestion identifies patients at risk of treatment failure. In this regard, ultrasound-based monitoring may provide a more accurate reflection of therapeutic efficacy compared with conventional clinical or laboratory parameters.
7.6. Interpretation of the Evidence
The available evidence supports several consistent conclusions. First, venous congestion is a major determinant of clinical outcomes in heart failure, particularly in relation to renal dysfunction and rehospitalization.
Second, dynamic assessment of congestion provides greater prognostic information than single timepoint measurements, highlighting the importance of serial evaluation.
Third, multimodal and integrative approaches outperform isolated parameters, reflecting the multi-organ nature of congestion.
However, important limitations must be acknowledged. The majority of studies are observational and relatively small, with significant heterogeneity in patient populations, ultrasound protocols, and outcome definitions. Randomized controlled trials evaluating VExUS-guided management strategies are currently lacking, limiting the ability to draw definitive conclusions regarding causality and therapeutic impact.
Despite these limitations, the consistency of findings across studies and clinical settings provides a strong rationale for incorporating venous congestion assessment into the clinical evaluation of heart failure, particularly when integrated with other hemodynamic and imaging parameters.
8. Limitation of VExUS
Despite the growing interest in VExUS and venous Doppler assessment, several important limitations must be acknowledged before its widespread adoption in clinical practice.
First, VExUS is inherently operator-dependent. The acquisition and interpretation of Doppler waveforms (particularly at the level of the hepatic, portal, and intrarenal veins) require specific technical expertise and adequate acoustic windows. Variability in operator experience may affect both image quality and diagnostic accuracy, limiting reproducibility across different clinical settings [3,10]. This issue is particularly relevant for intrarenal Doppler assessment, which may be technically challenging and not feasible in all patients.
Closely related to this is the issue of interobserver variability. Although some components of ultrasound assessment, such as lung ultrasound, have demonstrated high reproducibility, Doppler-based venous assessment is more complex and subject to interpretation. Differences in waveform classification and grading may lead to inconsistencies in VExUS scoring, particularly in borderline cases.
Another key limitation is the lack of standardization. While the original VExUS grading system provides a structured approach, variations in acquisition techniques, definitions of abnormal patterns, and thresholds for severity have been reported across studies. In some cases, simplified or modified versions of the score have been used, further contributing to heterogeneity and limiting comparability between studies [46]. Furthermore, VExUS does not directly measure venous pressure, but rather infers congestion from flow patterns, which may be influenced by multiple hemodynamic factors. This distinction is critical when interpreting its findings and integrating them into clinical decision-making.
From an evidence standpoint, the current literature is predominantly observational. Although consistent associations between venous congestion and adverse outcomes have been reported, there is a lack of randomized controlled trials evaluating VExUS-guided management strategies. As a result, the causal impact of VExUS-based decision-making on clinical outcomes remains uncertain.
The applicability of VExUS outside specific clinical contexts also deserves consideration. While its performance appears robust in patients with heart failure and cardiorenal syndrome, results are less consistent in heterogeneous ICU populations, where multiple competing mechanisms contribute to organ dysfunction. In such settings, venous congestion may represent only one of several pathophysiological factors, reducing the predictive value of VExUS [13].
Several confounding clinical conditions may affect the interpretation of venous Doppler findings. Significant tricuspid regurgitation, pulmonary hypertension, and right ventricular dysfunction can alter venous flow patterns independently of congestion severity. Similarly, mechanical ventilation and changes in intrathoracic pressure may influence Doppler waveforms, potentially leading to misinterpretation [72].
An additional conceptual limitation relates to the interpretation of VExUS as a surrogate of volume status. Emerging data suggest that VExUS may reflect underlying cardiac dysfunction and venous pressure transmission rather than absolute intravascular volume. In particular, studies have shown that VExUS grading does not necessarily correlate with traditional markers of fluid overload, such as body weight, and may instead be more closely linked to ventricular function [46].
This distinction is important, as it challenges the assumption that congestion can be equated with volume excess.
Finally, the feasibility of comprehensive VExUS assessment in routine clinical practice may be limited by time constraints and resource availability. Full evaluation requires the acquisition of multiple Doppler signals, which may not be practical in all clinical settings, particularly in emergency or high-acuity environments.
This has led to interest in simplified approaches focusing on selected components, although the trade-off between feasibility and accuracy remains to be fully defined. These limitations highlight that VExUS should not be considered a standalone diagnostic tool, but rather as part of an integrated, multimodal assessment of congestion.
A careful understanding of its technical constraints, clinical context, and interpretative nuances is essential to avoid misapplication and to maximize its potential clinical utility.
9. Conclusions and Future Directions
The assessment of congestion in heart failure is undergoing a conceptual transformation. Traditional approaches, largely centered on the estimation of intravascular volume, fail to capture the complexity of venous congestion and its impact on organ function. The emerging evidence reviewed in this manuscript supports a shift toward a physiology-based model in which congestion is defined by elevated venous pressures, impaired organ drainage, and their interaction with systemic perfusion.
Within this evolving paradigm, ultrasound-based techniques, and in particular the VExUS score, offer a unique opportunity to directly visualize and quantify systemic venous congestion at the bedside. By integrating information from multiple venous territories, VExUS provides a more comprehensive and organ-relevant assessment compared with conventional tools. Importantly, dynamic changes in congestion, rather than static measurements, appear to be the most informative markers of clinical evolution and therapeutic response [13].
The clinical implications of this approach are substantial. Venous congestion has emerged as a key determinant of adverse outcomes, particularly in relation to renal dysfunction and heart failure rehospitalization. The recognition of congestion as a dynamic and multi-organ process opens the door to more precise and individualized management strategies, including the use of serial ultrasound assessment to guide decongestive therapy.
However, several challenges remain. The current evidence base is largely observational, and the lack of randomized trials limits the ability to establish causality and define standardized therapeutic algorithms. Technical complexity, operator dependency, and variability in acquisition and interpretation also represent important barriers to widespread implementation. Moreover, the role of VExUS must be considered within a broader clinical context, as its performance may vary across different patient populations and clinical scenarios.
Future research should focus on several key areas. First, randomized controlled trials are needed to evaluate whether VExUS-guided management strategies translate into improved clinical outcomes. Second, efforts toward standardization of acquisition protocols and interpretation criteria are essential to enhance reproducibility and facilitate broader adoption. Third, the integration of VExUS with other modalities (such as lung ultrasound, biomarkers, and flow-based parameters) should be further explored to develop comprehensive, multimodal congestion assessment strategies.
Technological advances may also play a role in overcoming current limitations. The development of automated or artificial intelligence-assisted Doppler analysis has the potential to reduce operator dependency and improve consistency, making advanced ultrasound techniques more accessible in routine clinical practice.
In conclusion, VExUS should be viewed as a complementary tool that enhances, rather than replaces, existing methods of congestion assessment. Its greatest value lies in its ability to shift the clinical focus from fluid quantity to venous pressure and organ perfusion, enabling earlier detection of clinically relevant congestion, improved risk stratification and more targeted therapeutic interventions.
Author Contributions
Conceptualization, M.M., L.G.G.; methodology, M.M., L.G.G.; resources, M.M., L.G.G., A.R.N., F.C., S.G.; data curation, M.M., L.G.G., S.G.; writing—original draft preparation, M.M., L.G.G., A.R.N., F.C.; writing—review and editing, M.M., L.G.G.; visualization, M.M., L.G.G., S.G., G.M.F., G.M.S.; supervision, G.M.S., G.M.F.; project administration, L.G.G., M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created.
Acknowledgments
During the preparation of this manuscript, the authors used AI tools exclusively for grammar/syntax refinement and for assisting in the generation of figures. No AI system was involved in generating the scientific content or drafting the manuscript. The authors have reviewed and edited the output and take full responsibility for the content of this publication. The views and opinions expressed in this manuscript are those of the authors and do not necessarily reflect those of their affiliated institutions.
Conflicts of Interest
The authors declare no conflicts of interest.
Permissions/Copyright
No third-party copyrighted material has been used in the manuscript figures. All images/figures were entirely created by the authors specifically for this submission; therefore, no permissions are required and no copyright attribution is applicable.
Abbreviations
The following abbreviations are used in this manuscript
| AHF | acute heart failure |
| AKI | acute kidney injury |
| CVP | central venous pressure |
| e-VExUS | extended venous excess ultrasound |
| HF | heart failure |
| ICU | intensive care unit |
| IVC | inferior vena cava |
| LUS | lung ultrasound |
| POCUS | point-of-care ultrasound |
| VExUS | venous excess ultrasound |
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2023, 44(37), 3627–39. [Google Scholar] [CrossRef]
- Lozano-Jiménez, S.; García Sebastian, C.; Vela Martín, P.; García Magallón, B.; Martín Centellas, A.; de Castro, D.; Mitroi, C.; del Prado Dìaz, S.; Hernàndez-Pèrez, F.; Jimènez-Blanco Bravo, M.; et al. Prevalence and prognostic impact of subclinical venous congestion in patients hospitalized for acute heart failure. Eur Heart J Acute Cardiovasc Care 2026, 14(12), 749–53. [Google Scholar] [CrossRef] [PubMed]
- Velasco Malagón, S.; Acosta-Gutiérrez, E.; Nuñez-Ramos, J.A.; Salinas, S.; Mora Pabón, G. Subclinical Congestion Evaluated by Point of Care Ultrasound (POCUS) at Discharge Predicts Readmission in Patients with Acute Heart Failure: Prognostic Cohort Study. POCUS Journal 2024, 9(2), 125–32. [Google Scholar] [CrossRef] [PubMed]
- Ganapathy, A.; Dungu, J.N.; Dimarco, A.D.; Madu, A.; Li, B.; Langley, S.; Watters, P.; Savage, H.; et al. Advances in Congestion Assessment in Decompensated Heart Failure. Card Fail Rev. 2026, 12, e02. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, V.; Del Punta, L.; De Biase, N.; Pellicori, P.; Gargani, L.; Dini, F.L.; Armenia, S.; Li Vigni, M.; Maremmani, D.; Masi, S.; et al. Integrative assessment of congestion in heart failure using ultrasound imaging. Intern Emerg Med 2025, 20(1), 11–22. [Google Scholar] [CrossRef]
- Wainstein, M.V.; Machado, G.P.; Telo, G.H.; da Silveira, A.D.; Nasi, L.A.; de Araujo, G.N. Point-of-care ultrasound in the evaluation of STEMI patients. Front Cardiovasc Med 2025, 12. [Google Scholar] [CrossRef]
- Argaiz, E.R.; Rola, P.; Haycock, K.H.; Verbrugge, F.H. Fluid management in acute kidney injury: from evaluating fluid responsiveness towards assessment of fluid tolerance. Eur Heart J Acute Cardiovasc Care 2022, 11(10), 786–93. [Google Scholar] [CrossRef]
- Giangregorio, F.; Centenara, E.; Mazzocchi, S.; Gerra, L.; Tursi, F.; Imberti, D.; Aschieri, D. Assessing Venous Congestion in Acute and Chronic Heart Failure: A Review of Splanchnic, Cardiac and Pulmonary Ultrasound: Part 1: Conventional B-Mode, Colordoppler, and Vexus Protocol. J Clin Med. 2025, 14(22), 8147. [Google Scholar] [CrossRef]
- Anastasiou, V.; Peteinidou, E.; Moysidis, D. V.; Daios, S.; Gogos, C.; Liatsos, A.C.; Didagelos, M.; Gossios, T.; Efthimiadis, G.; Karamitsos, T.; et al. Multiorgan Congestion Assessment by Venous Excess Ultrasound Score in Acute Heart Failure. Journal of the American Society of Echocardiography 2024, 37(10), 923–33. [Google Scholar] [CrossRef]
- Antit, S.; Romdhane, S.; Mtiri, I.; Zakhama, L. The Role of Venous Excess Ultrasound Score in Optimizing Acute Heart Failure Diagnosis and Prognosis. J Saudi Heart Assoc. 2025, 37(1). [Google Scholar] [CrossRef]
- Longino, A.; Martin, K.; Leyba, K.; Siegel, G.; Thai, T.N.; Riscinti, M.; Douglas, I.; Gill, E.; Burke, J. Prospective Evaluation of Venous Excess Ultrasound for Estimation of Venous Congestion. Chest 2024, 165(3), 590–600. [Google Scholar] [CrossRef] [PubMed]
- Melo, R.H.; Gioli-Pereira, L.; Lourenço, I.D.; Da Hora Passos, R.; Bernardo, A.T.; Volpicelli, G. Diagnostic accuracy of multi-organ point-of-care ultrasound for pulmonary embolism in critically ill patients: a systematic review and meta-analysis. Crit Care 2025, 29(1), 162. [Google Scholar] [CrossRef] [PubMed]
- Trigkidis, K.K.; Siempos, I.I.; Kotanidou, A.; Zakynthinos, S.; Routsi, C.; Kokkoris, S. EARLY TRAJECTORY OF VENOUS EXCESS ULTRASOUND SCORE IS ASSOCIATED WITH CLINICAL OUTCOMES OF GENERAL ICU PATIENTS. Shock 2024, 61(3), 400–5. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.L. Fluid Volume Overload and Congestion in Heart Failure. Circ Heart Fail 2016, 9(8). [Google Scholar] [CrossRef]
- Gelman, S. Venous function and central venous pressure: a physiologic story. Anesthesiology 2008, 108(4), 735–48. [Google Scholar] [CrossRef]
- Patsalis, N.; Kreutz, J.; Chatzis, G.; Syntila, S.; Choukeir, M.; Schieffer, B.; Markus, B. Early risk predictors of acute kidney injury and short-term survival during Impella support in cardiogenic shock. Sci Rep. 2024, 14(1), 17484. [Google Scholar] [CrossRef]
- Ehrman, R.R.; Sherwin, R.L.; Reynolds, C.A.; Korzeniewski, S.J.; Welch, R.D.; Kline, J.A.; Ying, H.; Levy, P. Impact of Venous CONgestion on Organ Function and Outcomes in Sepsis (ICON-Sepsis): a prospective observational cohort study protocol. BMJ Open 2025, 15(6), e098987. [Google Scholar] [CrossRef]
- Trpkov, C.; Grant, A.D.M.; Fine, N.M. Intrarenal Doppler Ultrasound Renal Venous Stasis Index Correlates With Acute Cardiorenal Syndrome in Patients With Acute Decompensated Heart Failure. CJC Open 2021, 3(12), 1444–52. [Google Scholar] [CrossRef]
- Fallick, C.; Sobotka, P.A.; Dunlap, M.E. Sympathetically mediated changes in capacitance: redistribution of the venous reservoir as a cause of decompensation. Circ Heart Fail 2011, 4(5), 669–75. [Google Scholar] [CrossRef]
- Balan, C.; Morosanu, B.; Fodoroiu, A.; Dobre, V.; Dumitrache, A.; Barbulescu, R.T.; Valeanu, L.; Robu, C.; Boros, C.; Nica, A.; et al. Decoding portal vein pulsatility: hemodynamic determinants in a post-hoc analysis of a prospective observational trial. Ann Intensive Care 2025, 15(1), 81. [Google Scholar] [CrossRef]
- Andrei, S.; Nguyen, M.; Bouhemad, B.; Guinot, P.G. High VExUS grades are linked to cardiac function in general intensive care unit patients. Eur Heart J Acute Cardiovasc Care 2025, 14(1), 24–30. [Google Scholar] [CrossRef]
- Scagliola, R.; Bonino, B.; Viazzi, F.; Balbi, M.; Ameri, P. Relationship between venous congestion and systemic hypoperfusion in cardiorenal syndrome. Eur Heart J 2021, 42 (Supplement_1). [Google Scholar] [CrossRef]
- Castro, R.; Kattan, E.; Retamal, J.; Hernández, G.; Pinsky, M.R. Venous congestion from a vascular waterfall perspective: reframing congestion as a dynamic Starling resistor phenomenon. Intensive Care Med Exp. 2025, 13(1), 119. [Google Scholar] [CrossRef] [PubMed]
- Harrison, N.E.; Ehrman, R.; Collins, S.; Desai, A.A.; Duggan, N.M.; Ferre, R.; Gargani, L.; Goldsmith, A.; Kapur, T.; Lane, K.; et al. The prognostic value of improving congestion on lung ultrasound during treatment for acute heart failure differs based on patient characteristics at admission. J Cardiol. 2024, 83(2), 121–9. [Google Scholar] [CrossRef] [PubMed]
- Shirakabe, A.; Matsushita, M.; Shibata, Y.; Shighihara, S.; Nishigoori, S.; Sawatani, T.; Kiuchi, K.; Asai, K. Organ dysfunction, injury, and failure in cardiogenic shock. J Intensive Care 2023, 11(1), 26. [Google Scholar] [CrossRef]
- Puzzovivo, A.; Monitillo, F.; Guida, P.; Leone, M.; Rizzo, C.; Grande, D.; Ciccone, M.; Iacoviello, M. Renal Venous Pattern: A New Parameter for Predicting Prognosis in Heart Failure Outpatients. J Cardiovasc Dev Dis. 2018, 5(4). [Google Scholar] [CrossRef]
- Abu-Naeima, E.; Fatthy, M.; Shalaby, M.A.A.S.; Ayeldeen, G.; Verbrugge, F.H.; Rola, P.; Beaubien-Souligny, W.; Fayed, A. Venous Excess Doppler ultrasound assessment and loop diuretic efficiency in acute cardiorenal syndrome. BMC Nephrol 2025, 26(1), 157. [Google Scholar] [CrossRef]
- Campos Sáenz de Santamaría, A.; Alcaine Otín, A.; Crespo Aznarez, S.; Josa Laorden, C.; Esterellas Sánchez, L.; Sánchez Marteles, M.; Garcès Horna, V.; Albines Fiestas, Z.; Gimènez Lòpez, I.; Rubio Gracia, J. Multimodal analysis of congestion and prognostic utility of the VExUS protocol in hospitalized heart failure patients at a tertiary care hospital. Revista Clínica Española (English Edition) 2025, 225(7), 502332. [Google Scholar] [CrossRef]
- Samad, M.; Malempati, S.; Restini, C.B.A. Natriuretic Peptides as Biomarkers: Narrative Review and Considerations in Cardiovascular and Respiratory Dysfunctions. Yale J Biol Med 2023, 96(1), 137–49. [Google Scholar] [CrossRef]
- Barone, R.; Di Terlizzi, V.; Goffredo, G.; Paparella, D.; Brunetti, N.D.; Iacoviello, M. Renal Arterial and Venous Doppler in Cardiorenal Syndrome: Pathophysiological and Clinical Insights. Biomedicines 2024, 12(6), 1166. [Google Scholar] [CrossRef]
- Haddadin, R.; Aboujaoude, C.; Trad, G. Congestive Hepatopathy: A Review of the Literature. Cureus 2024, 16(4), e58766. [Google Scholar] [CrossRef]
- Hassan, A.; Khalil, A.A.; Mostafa, A.; Yehia, H. Venous Excess Ultrasound (VExUS) score and short-term outcomes in ambulatory patients with heart failure with reduced ejection fraction: an exploratory study. The Egyptian Heart Journal 2025, 77(1), 60. [Google Scholar] [CrossRef] [PubMed]
- Ponor, C.G.; Cepoi, M.R.; Spiridon, M.R.; Tudorancea, I.; Bobu, A.M.; Badescu, M.C.; et al. Assessment of Congestion in Heart Failure Using VExUS: Current Evidence, Limitations and Clinical Perspectives. 2026, 16(3), 518. [Google Scholar] [CrossRef] [PubMed]
- Koratala, A.; Ibrahim, M.; Gudlawar, S. VExUS to Guide Ultrafiltration in Hemodialysis: Exploring a Novel Dimension of Point of Care Ultrasound. POCUS journal 2024, 9(1), 16–9. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, M.; Rudski, L.G.; Addetia, K.; Afilalo, J.; D’Alto, M.; Freed, B.H.; Gargani, L.; Grapsa, J.; Hassoun, P.; Hua, L.; et al. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults and Special Considerations in Pulmonary Hypertension: Recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography 2025, 38(3), 141–86. [Google Scholar] [CrossRef]
- Bhardwaj, V.; Samprathi, A.; Saha, K.; Orozco, N.; Hegde, P.; Nizamudin, M.; Chacko, J.; Varma, M.; Denault, A. G. V.; Rola, P.; et al. Dual doppler dynamics: integrating femoral venous doppler and VExUS for predicting organ dysfunction in acute heart failure. Journal of Anesthesia, Analgesia and Critical Care 2025, 5(1), 65. [Google Scholar] [CrossRef]
- Magnino, C.; Omedè, P.; Avenatti, E.; Presutti, D.; Iannaccone, A.; Chiarlo, M.; Moretti, C.; Gaita, F.; Veglio, F.; Milan, A. Inaccuracy of Right Atrial Pressure Estimates Through Inferior Vena Cava Indices. Am J Cardiol. 2017, 120(9), 1667–73. [Google Scholar] [CrossRef]
- Guo, X.; Tang, M.; Jiang, X.; Lin, J.; Chen, W.; Song, Y. Ultrasound of the inferior vena cava for fluid therapy decisions: Strengths, limitations, and an integrated approach. J Int Med Res. 2026, 54(2), 3000605261417916. [Google Scholar] [CrossRef]
- Soliman-Aboumarie, H.; Denault, A.Y. How to assess systemic venous congestion with point of care ultrasound. Eur Heart J Cardiovasc Imaging 2023, 24(2), 177–80. [Google Scholar] [CrossRef]
- Campos-Sáenz de Santamaría, A.; Albines Fiestas, Z.S.; Crespo-Aznarez, S.; Esterellas-Sánchez, L.K.; Sánchez-Marteles, M.; Garcés-Horna, V.; Josa-Laorden, C.; Alcaine-Otìn, A.; Gimenez-Lopez, I.; Rubio-Gracia, J. VExUS Protocol Along Cardiorenal Syndrome: An Updated Review. J Clin Med. 2025, 14(4). [Google Scholar] [CrossRef]
- Piccione, M.C.; Colarusso, L.; Agricola, E.; Cameli, M.; De Luca, A.; Manganaro, R.; Barchitta, A.; D’Andrea, A.; parato, V.; Trambaiolo, P.; et al. How to Do Echo for Noninvasive Hemodynamic Evaluation of the Patient in the Intensive Care Unit: A Consensus Statement of the Italian Society of Echocardiography and Cardiovascular Imaging. J Cardiovasc Echogr. 2025, 35(1), 79–90. [Google Scholar] [CrossRef]
- Nijst, P.; Martens, P.; Dupont, M.; Tang, W.H.W.; Mullens, W. Intrarenal Flow Alterations During Transition From Euvolemia to Intravascular Volume Expansion in Heart Failure Patients. JACC Heart Fail 2017, 5(9), 672–81. [Google Scholar] [CrossRef]
- Rola, P.; Miralles-Aguiar, F.; Argaiz, E.; Beaubien-Souligny, W.; Haycock, K.; Karimov, T.; et al. Clinical applications of the venous excess ultrasound (VExUS) score: conceptual review and case series. Ultrasound J 2021, 13(1), 32. [Google Scholar] [CrossRef]
- Guinot, P.G.; Longrois, D.; Andrei, S.; Nguyen, M.; Bouhemad, B. Exploring congestion endotypes and their distinct clinical outcomes among ICU patients: A post-hoc analysis. Anaesth Crit Care Pain Med 2024, 43(3), 101370. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, F.; Born, P.; Bruna, M.; Ulloa, R.; González, C.; Philp, V.; Mondaca, R.; Blanco, J.; Valenzuela, E.; Retamal, J.; et al. Coexistence of a fluid responsive state and venous congestion signals in critically ill patients: a multicenter observational proof-of-concept study. Crit Care 2024, 28(1), 52. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Olusanya, O.; Watchorn, J.; Bramham, K.; Hutchings, S. Utility of the Venous Excess Ultrasound (VEXUS) score to track dynamic change in volume status in patients undergoing fluid removal during haemodialysis—the ACUVEX study. Ultrasound J 2024, 16(1), 23. [Google Scholar] [CrossRef] [PubMed]
- Torres-Arrese, M.; Mata-Martínez, A.; Luordo-Tedesco, D.; García-Casasola, G.; Alonso-González, R.; Montero-Hernández, E.; Cobo-Marcos, M.; Sànchez-Sauce, B.; Cuervas-Mons, V.; Tung-Chen, Y. Usefulness of Systemic Venous Ultrasound Protocols in the Prognosis of Heart Failure Patients: Results from a Prospective Multicentric Study. J Clin Med. 2023, 12(4), 1281. [Google Scholar] [CrossRef]
- Turk, M.; Robertson, T.; Koratala, A. Point-of-care ultrasound in diagnosis and management of congestive nephropathy. World J Crit Care Med. 2023, 12(2), 53–62. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Ruocco, G.; Pellicori, P.; Gargani, L.; Coiro, S.; Lamiral, Z.; Ambrosio, G.; Rastogi, T.; Girerd, N. Multi-modality assessment of congestion in acute heart failure: Associations with left ventricular ejection fraction and prognosis. Curr Probl Cardiol. 2024, 49(3), 102374. [Google Scholar] [CrossRef]
- Cox, E.G.M.; Koster, G.; Baron, A.; Kaufmann, T.; Eck, R.J.; Veenstra, T.C.; et al. Should the ultrasound probe replace your stethoscope? A SICS-I sub-study comparing lung ultrasound and pulmonary auscultation in the critically ill. Crit Care 2020, 24(1), 14. [Google Scholar] [CrossRef]
- Jobs, A.; Vonthein, R.; König, I.R.; Schäfer, J.; Nauck, M.; Haag, S.; Fichera, C.; Stiermaier, T.; Ledwoch, J.; Schneider, A.; et al. Inferior vena cava ultrasound in acute decompensated heart failure: design rationale of the CAVA-ADHF-DZHK10 trial. ESC Heart Fail 2020, 7(3), 973–83. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Xu, Y.; Chen, X.; Huang, W. Assessing venous congestion in critical illness: advantages of the inferior vena cava shape change index over diameter. Ann Intensive Care 2026, 16, 100032. [Google Scholar] [CrossRef] [PubMed]
- Soldati, G.; Demi, M.; Demi, L. Ultrasound patterns of pulmonary edema. Ann Transl Med 2019, 7 (Suppl 1), S16. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Girerd, N.; Platz, E.; Pellicori, P.; Stankovic, I.; Palazzuoli, A.; Pivetta, E.; Miglioranza, M.; Soliman-Aboumarie, H.; Agricola, E.; et al. Lung ultrasound in acute and chronic heart failure: a clinical consensus statement of the European Association of Cardiovascular Imaging (EACVI). Eur Heart J Cardiovasc Imaging 2023, 24(12), 1569–82. [Google Scholar] [CrossRef]
- Grigore, M.; Nicolae, C.; Grigore, A.M.; Balahura, A.M.; Păun, N.; Uscoiu, G.; Verde, I.; Ilieșiu, A. Contemporary Perspectives on Congestion in Heart Failure: Bridging Classic Signs with Evolving Diagnostic and Therapeutic Strategies. Diagnostics (Basel) 2025, 15(9). [Google Scholar] [CrossRef]
- Kobalava, Z.D.; Vladimirovna, T.V.; Kanatbekovich, S.B.; Aslanova, R.S.; Alekseevich, L.A.; Sergeevich, N.I.; Pavlovich, S.; Vatsik-Gorodetskaya, M.; Tabatabaei, G.; Al-Zakwani, I.; et al. Prognostic Role of Ultrasound Diagnostic Methods in Patients with Acute Decompensated Heart Failure. Oman Med J 2024, 39(3), e625–e625. [Google Scholar] [CrossRef]
- Rossini, R.; Valente, S.; Colivicchi, F.; Baldi, C.; Caldarola, P.; Chiappetta, D.; Cipriani, M.; Ferlini, M.; Gasparetto, N.; Gilardi, R.; et al. ANMCO POSITION PAPER: Role of intra-aortic balloon pump in patients with acute advanced heart failure and cardiogenic shock. European Heart Journal Supplements 2021, 23 (Supplement_C), C204–20. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Filippatos, G.; De Luca, L.; Burnett, J. Congestion in Acute Heart Failure Syndromes: An Essential Target of Evaluation and Treatment. Am J Med 2006, 119(12), S3–10. [Google Scholar] [CrossRef]
- Landi, I.; Guerritore, L.; Iannaccone, A.; Ricotti, A.; Rola, P.; Garrone, M. Assessment of venous congestion with venous excess ultrasound score in the prognosis of acute heart failure in the emergency department: a prospective study. European Heart Journal Open 2024, 4(5). [Google Scholar] [CrossRef]
- Rivas-Lasarte, M.; Maestro, A.; Fernández-Martínez, J.; López-López, L.; Solé-González, E.; Vives-Borrás, M.; Montero, S.; Mesado, N.; Pirla, M.; Mirabet, S.; et al. Prevalence and prognostic impact of subclinical pulmonary congestion at discharge in patients with acute heart failure. ESC Heart Fail;PubMed 2020, 7(5), 2621–8. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; van Deursen, V.M.; Navis, G.; Voors, A.A.; van Veldhuisen, D.J.; Hillege, H.L. Increased Central Venous Pressure Is Associated With Impaired Renal Function and Mortality in a Broad Spectrum of Patients With Cardiovascular Disease. J Am Coll Cardiol. 2009, 53(7), 582–8. [Google Scholar] [CrossRef] [PubMed]
- Tamayo-Gutierrez, A.; Ibrahim, H.N. The Kidney in Heart Failure: The Role of Venous Congestion. Methodist Debakey Cardiovasc J;PubMed 2022, 18(4), 4–10. [Google Scholar] [CrossRef] [PubMed]
- Cops, J.; Mullens, W.; Verbrugge, F.H.; Swennen, Q.; De Moor, B.; Reynders, C.; Penders, J.; Achten, R.; Driessen, A.; Dendooven, A.; et al. Selective abdominal venous congestion induces adverse renal and hepatic morphological and functional alterations despite a preserved cardiac function. Sci Rep. 2018, 8(1), 17757. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Damman, K.; Testani, J.M.; Martens, P.; Mueller, C.; Lassus, J.; Tang, W.; Skouri, H.; Verbrugge, F.; Orso, F.; et al. Evaluation of Kidney Function Throughout the Heart Failure Trajectory—A Position Statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2020, 22(4), 584–603. [Google Scholar] [CrossRef]
- Saadi, M.; Silvano, G.P.; Telo, G.H.; Scolari, F.L.; Machado, G.P.; Almeida, R.F.; Biolo, A.; Silveira, A. VExUS score improvement is associated with better outcomes in acute decompensated heart failure. Eur Heart J 2024, 45 (Supplement_1). [Google Scholar] [CrossRef]
- Lim, S.Y.; Kim, S. Pathophysiology of Cardiorenal Syndrome and Use of Diuretics and Ultrafiltration as Volume Control. Korean Circ J. 2021, 51(8), 656. [Google Scholar] [CrossRef]
- Sovetova, S.; Charaya, K.; Erdniev, T.; Shchekochikhin, D.; Bogdanova, A.; Panov, S.; Plaksina, N.; Mutalieva, E.; Ananicheva, N.; Fomin, V.; et al. Venous Excess Ultrasound Score Is Associated with Worsening Renal Function and Reduced Natriuretic Response in Patients with Acute Heart Failure. J Clin Med. 2024, 13(20), 6272. [Google Scholar] [CrossRef]
- Di Maria, A.; Siligato, R.; Bondanelli, M.; Fabbian, F. Venous Doppler flow patterns, venous congestion, heart disease and renal dysfunction: A complex liaison. World J Cardiol. 2024, 16(1), 5–9. [Google Scholar] [CrossRef]
- Ruste, M.; Reskot, R.; Schweizer, R.; Mayet, V.; Fellahi, J.L.; Jacquet-Lagrèze, M. Changes in portal pulsatility index induced by a fluid challenge in patients with haemodynamic instability and systemic venous congestion: a prospective cohort study. Ann Intensive Care 2024, 14(1), 167. [Google Scholar] [CrossRef]
- Beaubien-Souligny, W.; Benkreira, A.; Robillard, P.; Bouabdallaoui, N.; Chassé, M.; Desjardins, G.; Lamarche, Y.; White, M.; Bouchard, J.; Denault, A. Alterations in Portal Vein Flow and Intrarenal Venous Flow Are Associated With Acute Kidney Injury After Cardiac Surgery: A Prospective Observational Cohort Study. J Am Heart Assoc. 2018, 7(19), e009961. [Google Scholar] [CrossRef]
- Pagnesi, M.; Staal, L.; ter Maaten, J.M.; Beldhuis, I.E.; Cotter, G.; Davison, B.A.; Jongs, N.; Felker, G.; Filippatos, G.; Greenberg, B.; et al. Decongestion and Outcomes in Patients Hospitalized for Acute Heart Failure. JACC Heart Fail 2025, 13(3), 414–29. [Google Scholar] [CrossRef]
- Hovgaard, H.L.; Nielsen, R.R.; Laursen, C.B.; Frederiksen, C.A.; Juhl-Olsen, P. When appearances deceive: Echocardiographic changes due to common chest pathology. Echocardiography 2018, 35(11), 1847–59. [Google Scholar] [CrossRef]
Figure 1.
From volume overload to venous pressure–driven congestion. Traditional models conceptualize congestion as intravascular fluid accumulation assessed through clinical and surrogate markers. However, this approach fails to capture subclinical and organ-level congestion. Contemporary evidence supports a physiology-based paradigm in which congestion is driven by elevated venous pressures and impaired venous drainage. Retrograde transmission of right atrial pressure affects peripheral organs, reducing the effective perfusion gradient and contributing to organ dysfunction independently of cardiac output. Multimodal ultrasound, including VExUS, enables direct assessment of venous congestion and supports a more precise and clinically relevant evaluation. Abbreviations: JVD, jugular vein distension; BNP, brain natriuretic peptide; IVC, inferior cava vein.
Figure 1.
From volume overload to venous pressure–driven congestion. Traditional models conceptualize congestion as intravascular fluid accumulation assessed through clinical and surrogate markers. However, this approach fails to capture subclinical and organ-level congestion. Contemporary evidence supports a physiology-based paradigm in which congestion is driven by elevated venous pressures and impaired venous drainage. Retrograde transmission of right atrial pressure affects peripheral organs, reducing the effective perfusion gradient and contributing to organ dysfunction independently of cardiac output. Multimodal ultrasound, including VExUS, enables direct assessment of venous congestion and supports a more precise and clinically relevant evaluation. Abbreviations: JVD, jugular vein distension; BNP, brain natriuretic peptide; IVC, inferior cava vein.

Figure 2.
Venous congestion as the primary driver of renal dysfunction in heart failure: the role of impaired perfusion gradient. Renal dysfunction in heart failure has traditionally been attributed to reduced cardiac output and impaired arterial perfusion (“forward failure”). However, accumulating evidence supports a dominant role of venous congestion in the pathophysiology of cardiorenal syndrome. Elevated right atrial and systemic venous pressures are transmitted retrogradely to the renal venous circulation, increasing renal interstitial pressure and reducing the effective renal perfusion gradient, defined as the difference between arterial inflow and venous outflow pressure.
Figure 2.
Venous congestion as the primary driver of renal dysfunction in heart failure: the role of impaired perfusion gradient. Renal dysfunction in heart failure has traditionally been attributed to reduced cardiac output and impaired arterial perfusion (“forward failure”). However, accumulating evidence supports a dominant role of venous congestion in the pathophysiology of cardiorenal syndrome. Elevated right atrial and systemic venous pressures are transmitted retrogradely to the renal venous circulation, increasing renal interstitial pressure and reducing the effective renal perfusion gradient, defined as the difference between arterial inflow and venous outflow pressure.

Figure 3.
VExUS protocol and physiological interpretation. The VExUS score integrates IVC morphology with Doppler assessment of hepatic, portal, and intrarenal veins. Progressive waveform abnormalities reflect increasing venous pressure transmission and organ-level congestion. Higher VExUS grades are associated with increased risk of organ dysfunction, particularly acute kidney injury. VExUS reflects hemodynamic congestion rather than intravascular volume alone.
Figure 3.
VExUS protocol and physiological interpretation. The VExUS score integrates IVC morphology with Doppler assessment of hepatic, portal, and intrarenal veins. Progressive waveform abnormalities reflect increasing venous pressure transmission and organ-level congestion. Higher VExUS grades are associated with increased risk of organ dysfunction, particularly acute kidney injury. VExUS reflects hemodynamic congestion rather than intravascular volume alone.

Figure 4.
VExUS-guided therapeutic approach. Serial assessment of venous congestion enables dynamic tailoring of decongestive therapy. Improvement in VExUS grade is associated with better outcomes, whereas persistent congestion identifies high-risk patients.
Figure 4.
VExUS-guided therapeutic approach. Serial assessment of venous congestion enables dynamic tailoring of decongestive therapy. Improvement in VExUS grade is associated with better outcomes, whereas persistent congestion identifies high-risk patients.


Table 1.
Traditional vs Contemporary Conceptualization of Congestion in Heart Failure.
| Domain | Traditional View | Contemporary (VExUS-Based) View |
|---|---|---|
| Definition of congestion | Fluid overload | Venous pressure–driven hemodynamic state |
| Pathophysiological driver | Intravascular volume excess | Elevated venous pressure and impaired organ drainage |
| Primary mechanism | Forward failure (low cardiac output) | Backward failure (venous congestion) |
| Organ involvement | Global/systemic | Organ-specific (renal, hepatic, splanchnic, pulmonary) |
| Key determinant of dysfunction | Reduced perfusion | Reduced perfusion gradient (arterial inflow—venous pressure) |
| Clinical assessment | Physical exam, weight, CVP | Multimodal ultrasound (VExUS, LUS, Doppler) |
| Nature of congestion | Static | Dynamic and evolving |
| Prognostic relevance | Based on symptoms/signs | Based on organ-level congestion and its trajectory |
| Therapeutic target | Volume removal | Reduction of venous pressure and restoration of organ perfusion |
Abbreviations: CVP: central vein pressure; LUS: lung ultrasound; VExUS: venous excess ultrasound
Table 2.
VExUS Protocol: Technical Components and Doppler Interpretation.Abbreviations: IVC, inferior vena cava; RAP, right atrial pressure; VExUS, venous excess ultrasound.
Table 2.
VExUS Protocol: Technical Components and Doppler Interpretation.Abbreviations: IVC, inferior vena cava; RAP, right atrial pressure; VExUS, venous excess ultrasound.
| Component | Normal Pattern | Moderate Congestion | Severe Congestion | Physiological Meaning |
|---|---|---|---|---|
| IVC | ≤ 2 cm, normal variation | > 2 cm and inspiratory collapsibility >50% | Markedly dilated and inspiratory collapsibility <50% | Elevated RAP |
| Hepatic veins | S > D | S < D | S wave reversal | Direct transmission of RAP |
| Portal vein | Continuous flow (<30% pulsatility) | Pulsatility 30–50% | Pulsatility >50% | Loss of splanchnic compliance |
| Intrarenal veins | Continuous monophasic flow | Biphasic/discontinuous | Monophasic diastolic only | Renal venous congestion and impaired drainage |
| Integrated VExUS score | Normal IVC or normal Doppler | Mild Doppler abnormalities | Severe abnormalities in ≥1 territory | Organ-level congestion severity |
Table 3.
Clinical Interpretation Approach. Abbreviations: BNP: B-type Natriuretic Peptide; JVD: jugular vein distension; LUS: lung ultrasound; NT-proBNP: NT-proBNP = N-terminal pro–B-type Natriuretic Peptide;VExUS: venous excess ultrasound.
Table 3.
Clinical Interpretation Approach. Abbreviations: BNP: B-type Natriuretic Peptide; JVD: jugular vein distension; LUS: lung ultrasound; NT-proBNP: NT-proBNP = N-terminal pro–B-type Natriuretic Peptide;VExUS: venous excess ultrasound.
| Modality | What it Assesses | Physiological Domain | Strengths | Limitations |
|---|---|---|---|---|
| Clinical examination | Peripheral edema, JVD, rales | Late systemic/pulmonary congestion | Widely available, rapid | Low sensitivity, poor reproducibility |
| Biomarkers (BNP/NT-proBNP) | Myocardial wall stress | Cardiac pressure/volume load | Diagnostic and prognostic value | Not specific for venous congestion |
| IVC ultrasound | Central venous pressure | Right atrial pressure | Simple, rapid | Does not reflect organ-level congestion |
| Lung ultrasound (LUS) | B-lines (extravascular lung water) | Pulmonary congestion | Sensitive, reproducible | Does not assess systemic congestion |
| Intrarenal Doppler | Venous flow patterns | Renal congestion | Early marker of organ dysfunction | Technically challenging |
| Portal/hepatic Doppler | Venous pulsatility | Splanchnic/hepatic congestion | Reflects systemic venous pressure transmission | Operator-dependent |
| VExUS score | Multi-organ venous Doppler integration | Systemic venous congestion | Integrates organ-level physiology, higher specificity | Complexity, lack of standardization |
| Multimodal approach (VExUS + LUS ± flow) | Combined congestion and perfusion | Global hemodynamic profile | Improved risk stratification | Requires expertise and integration |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



