Submitted:
15 April 2026
Posted:
20 April 2026
You are already at the latest version
Abstract
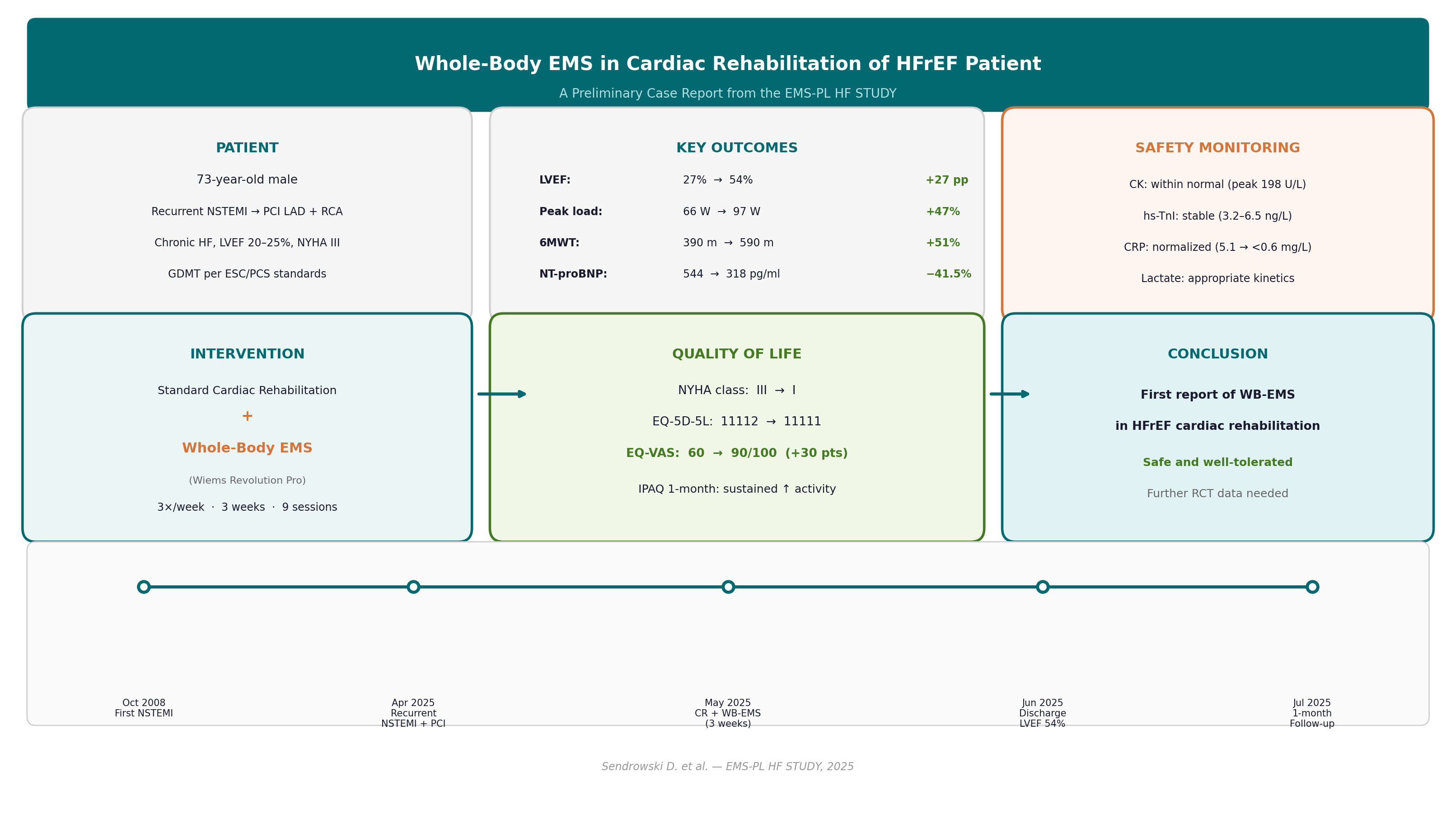
Background and Purpose: Whole-body electrical muscle stimulation (WB-EMS) is an emerging modality that activates multiple large muscle groups simultaneously via a wearable electrode suit. Although neuromuscular electrical stimulation (NMES) has demonstrated efficacy as an adjunctive strategy in cardiac rehabilitation (CR), WB-EMS has not previously been investigated in patients with heart failure and reduced ejection fraction (HFrEF) undergoing CR. This report presents preliminary findings from the active arm of an ongoing randomized trial. Methods: A 73-year-old male with recurrent non-ST-elevation myocardial infarction (NSTEMI), chronic HF (left ventricular ejection fraction [LVEF] 20–25%), and NYHA functional class III was admitted for inpatient CR. Standard CR (cycle ergometry, treadmill, resistance exercises, respiratory physiotherapy, and patient education, five days/week for 24 days) was augmented with WB-EMS (Wiems Revolution Pro device; 85 Hz bipolar, 350 μs, 4s on/4s off, 20-minute sessions) three times per week (~9 sessions). Safety was monitored with serial creatine kinase (CK), high-sensitivity troponin I (hs-TnI), NT-proBNP, C-reactive protein (CRP), and venous blood gas with lactate, measured before and 2–3 hours after each session. Results: LVEF improved from 27% to 54% (Simpson biplane); peak workload from 66 to 97 W (+47%); six-minute walk test (6MWT) distance from 390 to 590 m (+51%); and NT-proBNP declined from 544 to 318 pg/ml (−41.5%). EQ-5D-5L EQ-VAS improved from 60 to 90/100. One-month IPAQ data demonstrated sustained increases in daily physical activity. All safety biomarkers remained within acceptable limits throughout the programme. No adverse events were recorded. Discussion: To our knowledge, this is the first report of WB-EMS combined with standard CR in an HFrEF patient. The comprehensive serial biomarker monitoring confirmed a favorable safety profile. The striking improvements observed across functional, echocardiographic, neurohormonal, and quality-of-life domains are promising but require confirmation in the ongoing randomized trial, as multiple concurrent therapeutic interventions preclude causal attribution to WB-EMS alone.
Keywords:
cardiac rehabilitation
; electrical stimulation
; heart failure
; physiotherapy
Introduction
Heart failure with reduced ejection fraction
(HFrEF) remains a leading cause of morbidity and mortality worldwide.
Exercise-based cardiac rehabilitation (CR) is a Class I recommendation for HF
patients, demonstrating significant improvements in exercise capacity, quality
of life, and reduced hospitalization risk (Molloy et al., 2024; Bozkurt et al.,
2021). Despite this evidence, participation in CR remains critically low,
particularly among frail elderly patients with advanced disease and severe
deconditioning who cannot fully engage in conventional exercise programmes.
Neuromuscular electrical stimulation (NMES) has
emerged as an adjunctive strategy for patients with limited exercise tolerance.
Meta-analyses have demonstrated that NMES significantly improves peak oxygen
consumption (VO₂max), six-minute walk test (6MWT) distance, quality of life,
and peripheral muscle strength in HF patients (Gomes Neto et al., 2016; Wang et
al., 2022). Recent randomized controlled trials have confirmed these benefits
in frail elderly populations, including home-based NMES in elderly patients
with HF (Ono et al., 2025), NMES following percutaneous coronary intervention
in frail elderly patients (Pu et al., 2024), and the ACTIVE-EMS trial of
neuromuscular electrical stimulation in acute HF (Tanaka et al., 2022). A
companion systematic review by the present authors confirmed that peripheral
muscle electrostimulation (PME) is a safe, feasible adjunct to conventional CR
in frail elderly cardiac patients, improving peripheral muscle function and
physical performance without cardiovascular stress (Sendrowski et al., in
press).
Whole-body electromyostimulation (WB-EMS) differs
fundamentally from localized NMES in that it simultaneously activates multiple
large muscle groups — including the upper arms, chest, back, abdomen, gluteal
region, and thighs — via a wearable electrode suit. WB-EMS has shown benefits
in non-athletic adults across a range of health-related outcomes including body
composition, muscle strength, and cardiorespiratory fitness (Kemmler et al.,
2018). However, to our knowledge, WB-EMS has not previously been investigated
in patients with HFrEF undergoing cardiac rehabilitation, representing a
significant gap in the evidence base.
This report presents the first application of
WB-EMS as an adjunct to standard inpatient CR in an HFrEF patient, drawn from
the active arm of an ongoing randomized controlled trial. The case is reported
in accordance with the CARE guidelines (Gagnier et al., 2014; Riley et al.,
2017). The primary aim is to describe the safety profile and clinical outcomes
of this novel intervention in order to provide proof-of-concept data for the
ongoing trial.
Methods
Design
This is a single-patient preliminary report from
the active WB-EMS arm of a randomized, three-arm controlled trial (EMS-PL HF
STUDY) comparing standard inpatient CR alone, standard CR with WB-EMS, and
standard CR with sham EMS (45 patients planned). The trial received ethics
approval from the Bioethics Committee at the District Medical Chamber in Gdańsk
(Opinion No. KB-14/24, May 7, 2024). Written informed consent was obtained from
the patient for participation and publication, in accordance with the Declaration
of Helsinki. The report follows the CARE guidelines (Gagnier et al., 2014;
Riley et al., 2017).
Patient
A 73-year-old male (height 170 cm, weight 90 kg,
BMI 31.1 kg/m²) was admitted to the inpatient CR department on May 20, 2025,
following revascularization for recurrent NSTEMI. His cardiac history included
an initial NSTEMI in October 2008 managed with percutaneous coronary
intervention (PCI) of the right coronary artery (RCA) with a drug-eluting stent
(DES). The index event was a recurrent NSTEMI on April 30, 2025, treated with
PCI of the left anterior descending artery (LAD) with two DES, followed by staged
PCI of the RCA with one DES on May 5, 2025. The hospital course was complicated
by Staphylococcus aureus bacteraemia treated with cloxacillin.
Comorbidities included chronic HF with severely
reduced LVEF (20–25%), NYHA functional class III (downgraded from IV during the
acute episode), arterial hypertension, type 2 diabetes mellitus with vascular
complications, and frequent premature ventricular complexes (PVCs) with
non-sustained ventricular tachycardia (nsVT) requiring amiodarone initiation.
Guideline-directed medical therapy (GDMT) per ESC recommendations (McDonagh et
al., 2021, 2023) included sacubitril/valsartan 97/103 mg twice daily, metoprolol
succinate 47.5 mg once daily, eplerenone 25 mg once daily, empagliflozin 10 mg
once daily, amiodarone 200 mg once daily, dual antiplatelet therapy (aspirin 75
mg and prasugrel 10 mg), torasemide 5 mg, lercanidipine 10 mg,
rosuvastatin/ezetimibe 40/10 mg, metformin 1000 mg twice daily, and
pantoprazole 20 mg.
Procedure
Standard CR comprised supervised aerobic exercise
(cycle ergometry and treadmill at training heart rate 120–125/min, maximum
workload 60–65 W), resistance exercises, respiratory physiotherapy, and patient
education, conducted five days per week over 24 days (May 20—June 13, 2025).
WB-EMS was delivered using a Wiems Revolution Pro
device (CE marked, FDA cleared), a wearable suit with electrodes covering the
upper arms, chest, back, abdomen, gluteal region, and thighs. Sessions were
conducted three times per week (nine sessions over approximately three weeks),
each lasting 20 minutes with low-frequency bipolar impulses (85 Hz, pulse width
350 μs, duty cycle 4 s on/4 s off), intensity titrated to the maximum tolerated
level. The patient performed isometric exercises during stimulation-on phases.
Protifar protein supplementation (13.2 g/day) was provided for sarcopenia
prevention throughout the programme.
A comprehensive serial safety monitoring protocol
was implemented. Venous blood samples for CK, hs-TnI, NT-proBNP, CRP, and
point-of-care venous blood gas with lactate were collected before and 2–3 hours
after each WB-EMS session.
Outcome Measures
Primary outcome measures were: (1) transthoracic
echocardiography with LVEF measured by Simpson biplane method; (2)
cardiopulmonary exercise testing (CPET) using a modified Bruce ramp protocol on
a treadmill, reporting peak workload (W), VO₂max (ml/min/kg), and arrhythmia
assessment; (3) six-minute walk test (6MWT) distance (m); and (4) serial safety
biomarkers as described above. Secondary outcomes included the EQ-5D-5L health
utility questionnaire with visual analogue scale (EQ-VAS; Herdman et al., 2011)
and the International Physical Activity Questionnaire (IPAQ) at one-month
follow-up. Functional class was assessed using the NYHA classification.
Results
Baseline Assessment
Table 1 presents the timeline of key clinical events. Baseline echocardiography (May
21, 2025) revealed an enlarged left ventricle (LV end-diastolic diameter
[LVEDd] 67 mm, LV end-systolic diameter [LVESd] 55 mm) with severe global
systolic dysfunction and dyssynchrony. LVEF was 27% by Simpson biplane
(automated 23%). Global longitudinal strain was markedly impaired (two-chamber
−10.9%, parasternal long-axis −5.5%). Mild mitral regurgitation was present.
Right ventricular function was preserved (TAPSE 23 mm, TRV 2.1 m/s, estimated
right ventricular systolic pressure [RVSP] <36 mmHg).
Baseline
CPET (May 20, 2025) using a modified Bruce ramp protocol demonstrated peak
workload 66 W (46% predicted), VO₂max 17.42 ml/min/kg, peak METs 5.0, and peak
heart rate 132/min (90% predicted; RER 1.03). ECG monitoring documented
frequent PVCs, bigeminy, couplets, and nsVT salvos (maximum 3 consecutive
ectopic beats), suppressed at peak exercise but increased during recovery.
Pressor and chronotropic responses were classified as excessive. Training
parameters were set at heart rate 120–125/min, maximum workload 60–65 W.
Baseline 6MWT distance was 390 m. Baseline EQ-5D-5L profile was 11112 (slight
anxiety), EQ-VAS 60/100. Baseline IPAQ indicated minimal physical activity
(retired, no occupational activity).
Baseline
laboratory values (May 22–23, 2025): NT-proBNP 544 pg/ml, hs-TnI 4.9 ng/L, CK
64 U/L, CRP 5.1 mg/L, creatinine 1.41 mg/dL (eGFR 49 ml/min/1.73m²), fasting
glucose 126 mg/dL, total protein 7.1 g/dL, albumin 4.0 g/dL, sodium 141 mmol/L,
potassium 4.6 mmol/L.
Safety Monitoring
Serial biomarker data are summarized in Table 2. CK peaked at
198 U/L on May 26 (after the second WB-EMS session), remaining within the
normal reference range (20–200 U/L) and well below the 4× upper limit of normal
safety threshold for WB-EMS-related rhabdomyolysis. CK subsequently declined
progressively to 49–64 U/L by the final monitoring timepoints, consistent with
physiological adaptation. hs-TnI remained stable throughout (range 3.2–6.5
ng/L) with no exercise-induced elevations, providing no evidence of myocardial
injury.
Pre-exercise NT-proBNP demonstrated a progressive decline across the programme: 544 pg/ml at baseline to 318 pg/ml at final measurement (−41.5%), indicating improving neurohormonal status. CRP declined from 5.1 mg/L at admission to values consistently <0.6 mg/L from June 2 onward, reflecting resolution of the preceding inflammatory episode. Post-exercise venous lactate ranged 2.0–4.4 mmol/L (pre-exercise values 1.1–1.6 mmol/L, within normal limits), with pH stable throughout (7.37–7.47), confirming appropriate lactate kinetics without metabolic acidosis. No adverse events, hypotensive episodes, significant arrhythmias attributable to WB-EMS, or musculoskeletal injuries were recorded during any session.
Discharge Assessment
Discharge echocardiography (June 10, 2025) demonstrated marked improvement: LVEF 54% by Simpson biplane (automated 51%), LVESd reduced from 55 to 50 mm, LVEDd 66 mm. LV systolic function was reclassified from severely to mildly impaired. Regional wall motion abnormalities included akinesia of the basal inferior segment and hypokinesia of the apical/mid posterior, lateral, and anterior walls. Dyssynchrony persisted. GLS partially improved (parasternal long-axis from −5.5% to −8.6%). TAPSE improved from 23 to 26 mm; S’RV was 29 cm/s. New findings included mild aortic stenosis (Vmax 210 cm/s, mean gradient 10 mmHg) and a patent foramen ovale without shunt.
Discharge CPET (June 12, 2025) demonstrated: peak workload 97 W (67% predicted; +47% from baseline), VO₂max 19.02 ml/min/kg (+9.2%), peak METs 5.5, peak heart rate 130/min (88% predicted; RER 0.96). Arrhythmia burden was markedly reduced to isolated PVCs with complete suppression at peak exercise. Pressor and chronotropic responses were normal (blood pressure rest 140/80, maximum 160/90 mmHg). Resting ECG showed sinus rhythm 83/min, diffuse bundle branch block, old anteroseptal MI pattern, QRS 132 ms, QTc 465 ms. 6MWT distance improved from 390 to 590 m (+51%). NYHA functional class improved from III to I. EQ-5D-5L profile normalized from 11112 to 11111, EQ-VAS improved from 60 to 90/100 (+30 points).
One-month follow-up IPAQ (July 2025) demonstrated a substantial increase in physical activity: daily walking seven days per week approximately 1.5–2 hours; cycling one day per week; intensive domestic activity seven days per week approximately 1.5 hours; moderate domestic activity seven days per week. The patient was discharged on June 13, 2025, in good general condition, without complications throughout the 24-day admission.

Table 3.
Summary of clinical outcomes at baseline and discharge.
| Outcome Measure | Baseline | Discharge | Change |
|---|---|---|---|
| LVEF (Simpson biplane) | 27% | 54% | +27 pp |
| LVESd (mm) | 55 | 50 | −5 mm |
| TAPSE (mm) | 23 | 26 | +3 mm |
| Peak workload (W) | 66 (46% pred.) | 97 (67% pred.) | +47% |
| VO₂max (ml/min/kg) | 17.42 | 19.02 | +9.2% |
| Peak METs | 5.0 | 5.5 | +0.5 |
| 6MWT distance (m) | 390 | 590 | +51% |
| NT-proBNP (pg/ml) | 544 | 318 | −41.5% |
| NYHA class | III | I | −2 |
| EQ-5D-5L profile | 11112 | 11111 | Normalized |
| EQ-VAS (/100) | 60 | 90 | +30 |
Note. LVEF = left ventricular ejection fraction; LVESd = left ventricular end-systolic diameter; TAPSE = tricuspid annular plane systolic excursion; VO₂max = peak oxygen consumption; METs = metabolic equivalents; 6MWT = six-minute walk test; NT-proBNP = N-terminal pro-brain natriuretic peptide; NYHA = New York Heart Association; EQ-VAS = EQ-5D-5L visual analogue scale; pp = percentage points; pred. = predicted.
Discussion
This case describes the first application of WB-EMS as an adjunct to standard inpatient CR in HFrEF, demonstrating improvements across all assessed domains: echocardiographic function (LVEF 27% to 54%), exercise capacity (peak workload +47%, 6MWT +51%), neurohormonal status (NT-proBNP −41.5%), arrhythmia burden, and quality of life (EQ-VAS +30 points), with an excellent safety profile throughout the 24-day programme.
The existing NMES literature in HF provides biological plausibility for these findings. Gomes Neto et al. (2016) conducted a systematic review with meta-analysis demonstrating that localized NMES significantly improved peak VO₂, 6MWT distance, quality of life, peripheral muscle strength, and endothelial function in HF patients. Wang et al. (2022) similarly reported that functional electrical stimulation (FES) of the lower limbs improved cardiopulmonary function and quality of life across randomized controlled trials in HF. Parissis et al. (2015) studied elderly CHF patients (mean age 75 years, NYHA II/III) — a population closely resembling the present patient — reporting improvements in functional status, quality of life, and endothelial function with FES. Kadoglou et al. (2017) and Iliou et al. (2017) further confirmed cardiovascular and functional benefits of FES/combined EMS in HF populations. Notably, prior EMS studies in HF predominantly employed localized quadriceps or calf stimulation; the WB-EMS approach activates larger muscle mass simultaneously across multiple groups, potentially amplifying the metabolic and haemodynamic stimuli. The companion systematic review by the present authors (Sendrowski et al., in press) confirmed that PME is safe and feasible in frail elderly cardiac patients, with no cardiovascular adverse events reported across the included trials, consistent with the present findings. Van Buuren et al. (2013) specifically demonstrated improvements in LVEF and peak VO₂ with localized electrical myostimulation in chronic HF, and Kemmler et al. (2018) confirmed the efficacy and safety of WB-EMS in non-athletic adults.
The safety profile observed in this case is reassuring. CK remained below the 4× upper limit of normal safety threshold throughout, with the transient peak on day 3 followed by progressive decline consistent with physiological adaptation — a pattern consistent with findings of Ono et al. (2025), who reported 100% adherence and zero cardiovascular adverse events in home-based NMES in frail elderly HF patients, and with Tanaka et al. (2022) in the ACTIVE-EMS trial. hs-TnI stability without exercise-induced rises provides no evidence of WB-EMS-related myocardial injury. Appropriate lactate kinetics (post-exercise elevation with rapid normalization and stable pH) confirm that sessions were conducted within safe metabolic limits.
The dramatic LVEF improvement from 27% to 54% warrants careful interpretation. This magnitude of recovery most likely reflects reversal of myocardial stunning following coronary revascularization combined with optimized GDMT (sacubitril/valsartan, empagliflozin, beta-blocker, eplerenone) per ESC guidelines (McDonagh et al., 2021, 2023) and the comprehensive CR programme (Molloy et al., 2024; Bozkurt et al., 2021), rather than an isolated WB-EMS effect. The precise contribution of WB-EMS to the observed improvements in LVEF, exercise capacity, and quality of life cannot be determined from a single-arm observation and requires further investigation in a larger, controlled cohort within the ongoing randomized trial.
Strengths of this report include comprehensive serial biomarker monitoring before and after each session, providing granular safety data rarely available in NMES studies; use of validated patient-reported outcome measures (EQ-5D-5L [Herdman et al., 2011], IPAQ); and adherence to CARE guidelines (Gagnier et al., 2014; Riley et al., 2017). Limitations include the single-case design, which precludes causal inference or generalizability. The short follow-up period limits conclusions about durability of improvement. Major confounders include concurrent initiation of optimized GDMT, post-revascularization myocardial recovery (stunning reversal), and the multicomponent nature of the CR programme, each of which independently contributes to improvement. Results from the full randomized trial cohort (EMS-PL HF STUDY, planned n=45) will be required to determine the independent efficacy of WB-EMS in HFrEF cardiac rehabilitation.
Implications for Physiotherapy Practice
The findings of this preliminary case report carry several implications for physiotherapy practice, pending confirmation in larger controlled studies:
- WB-EMS may represent a safe adjunctive modality in supervised inpatient cardiac rehabilitation for elderly patients with HFrEF and limited exercise tolerance, offering a complementary approach to conventional aerobic and resistance exercise training.
- A comprehensive serial biomarker monitoring protocol — including CK, high-sensitivity troponin, NT-proBNP, and point-of-care venous lactate — measured before and 2–3 hours after each session provides a feasible and informative safety framework for implementing WB-EMS alongside conventional rehabilitation programmes.
- Physiotherapists should be aware that WB-EMS simultaneously recruits multiple large muscle groups (upper limbs, trunk, lower limbs) and may offer advantages over localized stimulation in severely deconditioned patients in whom targeted exercise is insufficient to generate an adequate metabolic stimulus.
- Randomized controlled trial evidence is needed before routine clinical implementation of WB-EMS in cardiac rehabilitation for HFrEF; the ongoing EMS-PL HF STUDY will provide the controlled data necessary to establish both efficacy and optimal protocol parameters.
Illustrations were created based on clinical photographs to protect patient identity.

Figure 1_WB-EMS

Figure 2_WB-EMS

Figure 3_WB-EMS

Figure 4-WB-EMS
References
- Anderson, L., Oldridge, N., Thompson, D. R., Zwisler, A.-D., Rees, K., Martin, N., & Taylor, R. S. (2016). Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. Journal of the American College of Cardiology, 67(1), 1–12. [CrossRef]
- Bozkurt, B., Fonarow, G. C., Goldberg, L. R., Guglin, M., Josephson, R. A., Forman, D. E., & Thomas, R. J. (2021). Cardiac rehabilitation for patients with heart failure: JACC expert panel. Journal of the American College of Cardiology, 77(11), 1454–1469. [CrossRef]
- Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., … Zamboni, M. (2019). Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. [CrossRef]
- Gagnier, J. J., Kienle, G., Altman, D. G., Moher, D., Sox, H., Riley, D., & the CARE Group. (2014). The CARE guidelines: Consensus-based clinical case reporting guideline development. Journal of Clinical Epidemiology, 67(1), 46–51. [CrossRef]
- Gomes Neto, M., Oliveira, F. A., Reis, H. F., Rodrigues, E. S., Jr., Bittencourt, H. S., & Ribeiro, N. (2016). Effects of neuromuscular electrical stimulation on physiologic and functional measurements in patients with heart failure: A systematic review with meta-analysis. Journal of Cardiopulmonary Rehabilitation and Prevention, 36(3), 157–166. [CrossRef]
- Herdman, M., Gudex, C., Lloyd, A., Janssen, M. F., Kind, P., Parkin, D., … Badia, X. (2011). Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research, 20(10), 1727–1736. [CrossRef]
- Iliou, M. C., Blanchard, J.-C., Lamar-Tanguy, A., Cristofini, P., & Ledru, F. (2017). Electrical stimulation in patients with heart failure. European Journal of Preventive Cardiology, 24(12), 1274–1282. [CrossRef]
- Kadoglou, N. P. E., Mandila, C., Karavidas, A., Farmakis, D., Parissis, J., Vlahodimitris, I., … Iliou, M.-C. (2017). Effect of functional electrical stimulation on cardiovascular outcomes in patients with chronic heart failure. European Journal of Preventive Cardiology, 24(8), 833–839. [CrossRef]
- Kemmler, W., Weissenfels, A., Willert, S., Fröhlich, M., Ludwig, O., Berber, M., … von Stengel, S. (2018). Efficacy and safety of low frequency whole-body electromyostimulation (WB-EMS) to improve health-related outcomes in non-athletic adults: A systematic review. Frontiers in Physiology, 9, 573. [CrossRef]
- McDonagh, T. A., Metra, M., Adamo, M., Gardner, R. S., Baumbach, A., Böhm, M., … ESC Scientific Document Group. (2021). 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal, 42(36), 3599–3726. [CrossRef]
- McDonagh, T. A., Metra, M., Adamo, M., Gardner, R. S., Baumbach, A., Böhm, M., … ESC Scientific Document Group. (2023). 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal, 44(37), 3627–3639. [CrossRef]
- Molloy, C., Long, L., Mordi, I. R., Bridges, C., Rees, K., Davies, E., … Taylor, R. S. (2024). Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database of Systematic Reviews, 3, CD003331. [CrossRef]
- Ono, S., Takahashi, T., Watanabe, M., & Izawa, H. (2025). Safety and efficacy of home-based neuromuscular electrical stimulation in frail elderly patients with heart failure: A randomized controlled trial. Circulation Reports, 7(4), 231–238. [CrossRef]
- Parissis, J., Karavidas, A., Farmakis, D., Papoutsidakis, N., Matzaraki, V., Arapi, S., … Filippatos, G. (2015). Efficacy and safety of functional electrical stimulation of lower limb muscles in elderly patients with chronic heart failure: A pilot study. European Journal of Preventive Cardiology, 22(7), 831–836. [CrossRef]
- Pu, X., Zhao, J., Li, J., He, Q., Chen, M., & Tang, Y. (2024). Effect of neuromuscular electrical stimulation on frail elderly patients after percutaneous coronary intervention: A randomized controlled trial. Clinical Interventions in Aging, 19, 1163–1176. [CrossRef]
- Riley, D. S., Barber, M. S., Kienle, G. S., Aronson, J. K., von Schoen-Angerer, T., Tugwell, P., … Gagnier, J. J. (2017). CARE guidelines for case reports: Explanation and elaboration document. Journal of Clinical Epidemiology, 89, 218–235. [CrossRef]
- Sendrowski, D., Polańska-Szczap, A., Hus-Budziszewska, B., Vlaieva, A., Kozłowski, D., Carlé-Calo, A., & Markowski, S. (in press). Theoretical and scientific underpinnings of peripheral muscle electrostimulation in cardiac rehabilitation of the elderly: A systematic review. [Unpublished companion paper].
- Tanaka, S., Kamiya, K., Hamazaki, N., Matsuzawa, R., Nozaki, K., Maekawa, E., … Ako, J. (2022). ACTIVE-EMS: Efficacy of electrical muscle stimulation in patients hospitalized with acute heart failure — A randomized controlled study. Journal of Cardiovascular Development and Disease, 9(4), 99. [CrossRef]
- van Buuren, F., Mellwig, K. P., Prinz, C., Korber, B., Fritzsche, D., Bogunovic, N., … Horstkotte, D. (2013). Electrical myostimulation improves left ventricular function and peak oxygen consumption in patients with chronic heart failure: Results from the exEMS study comparing different stimulation settings. Clinical Research in Cardiology, 102(7), 523–534. [CrossRef]
- Wang, H. Y., Chen, Y. H., Kuan, Y. C., Cheng, H. T., Lin, Y. J., Huang, P. H., … Chang, G. J. (2022). The effectiveness of functional electrical stimulation of the legs in patients with heart failure: A systematic review and meta-analysis of randomized controlled trials. Clinical Rehabilitation, 36(3), 303–316. [CrossRef]
Table 1.
Timeline of key clinical events.
| Date | Event |
|---|---|
| October 2008 | Initial NSTEMI; PCI RCA with DES |
| April 30, 2025 | Recurrent NSTEMI; PCI LAD with 2×DES |
| May 5, 2025 | Staged PCI RCA with 1×DES |
| May 20, 2025 | Admission to inpatient cardiac rehabilitation; baseline CPET |
| May 21, 2025 | Baseline echocardiography: LVEF 27% |
| May 22–23, 2025 | Baseline laboratories; first WB-EMS session |
| May 23–June 13, 2025 | Standard CR + WB-EMS programme (9 sessions) |
| June 10, 2025 | Discharge echocardiography: LVEF 54% |
| June 12, 2025 | Discharge CPET; 6MWT 590 m |
| June 13, 2025 | Discharge in good general condition; NYHA I |
| July 2025 | One-month follow-up: substantially increased physical activity (IPAQ) |
Note. NSTEMI = non-ST-elevation myocardial infarction; PCI = percutaneous coronary intervention; RCA = right coronary artery; LAD = left anterior descending artery; DES = drug-eluting stent; CPET = cardiopulmonary exercise testing; CR = cardiac rehabilitation; WB-EMS = whole-body electrical muscle stimulation; LVEF = left ventricular ejection fraction; 6MWT = six-minute walk test; NYHA = New York Heart Association.
Table 2.
Serial safety biomarker monitoring (pre-exercise / post-exercise values).
| Date | CK (U/L) [ref 20–200] | hs-TnI (ng/L) | NT-proBNP (pg/ml) | CRP (mg/L) [ref 0–5] |
|---|---|---|---|---|
| May 22–23 | 64 / 87 | 4.9 / 5.7 | 544 / 701 | 5.1; 3.1 / 3.1 |
| May 26 | 141 / 198* | 4.1 / 4.5 | 452 / 660 | 1.2 / 1.3 |
| May 28 | 106 / 107 | 4.4 / 5.3 | 381 / 535 | 1.2 / 0.8 |
| May 30 | 60 / 64 | 4.0 / 3.2 | 509 / 668 | 0.8 / 0.8 |
| June 2 | 54 / 62 | 6.3 / 6.5 | 603 / 786 | <0.6 |
| June 4 | 51 / 53 | 5.0 / 5.3 | 435 / 544 | <0.6 |
| June 6 | 49 / 55 | 4.4 / 5.2 | 448 / 658 | <0.6 |
| June 9 | 56 / 64 | 4.4 / 3.9 | 389 / 507 | <0.6 |
| June 11 | 55 / 58 | 5.0 / 4.9 | 318 / 442 | 1.7 / 1.7 |
| June 13 | 53 | — | — | 1.1 |
Note. Values presented as pre-exercise / post-exercise (2–3 h after WB-EMS session). CK = creatine kinase; hs-TnI = high-sensitivity troponin I; NT-proBNP = N-terminal pro-brain natriuretic peptide; CRP = C-reactive protein. * CK peak of 198 U/L on May 26 remained within the normal reference range and well below the 4× upper limit of normal safety threshold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



