Submitted:
15 April 2026
Posted:
16 April 2026
You are already at the latest version
Abstract
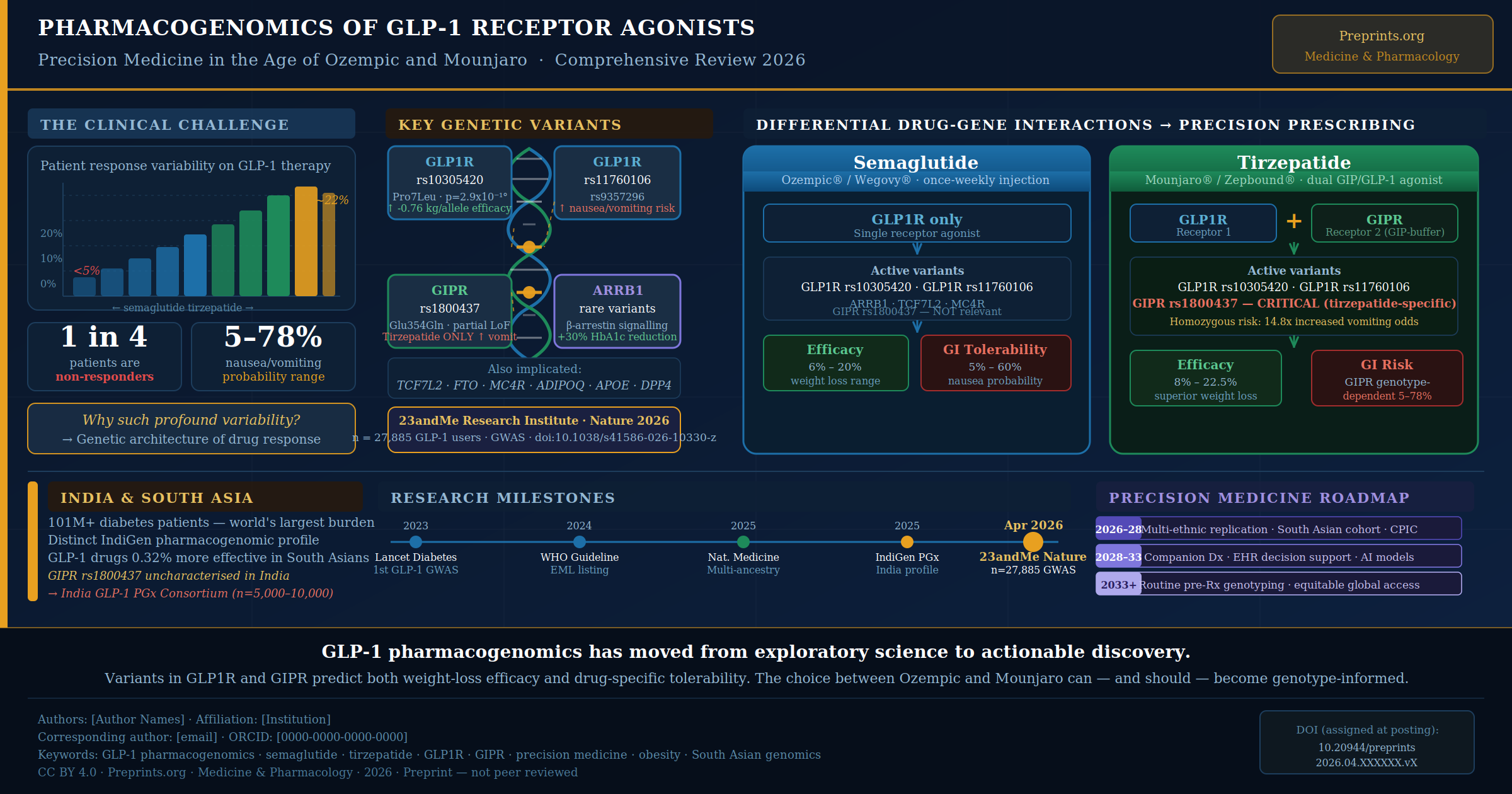
Glucagon-like peptide-1 (GLP-1) receptor agonists — including semaglutide (Ozempic®, Wegovy®) and the dual GIP/GLP-1 agonist tirzepatide (Mounjaro®, Zepbound®) — have transformed the management of type 2 diabetes, obesity, and cardiovascular disease. Yet a clinically significant and underappreciated challenge persists: profound inter-individual variability in both efficacy and tolerability. Some patients lose more than 20% of body weight; others less than 5%. Some experience debilitating nausea; others experience none at all.This narrative review synthesises the rapidly evolving evidence in pharmacogenomics as it applies to GLP-1 therapies, with a focus on: (1) the genetic architecture of drug-response variability across GLP1R, GIPR, ARRB1, TCF7L2, MC4R, and related loci; (2) landmark genomic research including the April 2026 23andMe GWAS published in Nature (n=27,885) — the largest pharmacogenomic study of GLP-1 drugs to date; (3) the strategic positioning of leading biopharma companies (Novo Nordisk, Eli Lilly, 23andMe Research Institute, PGxAI) in this space; (4) the emerging research landscape in India and South Asia, where the world's largest diabetes burden intersects with a distinct and undercharacterised pharmacogenomic profile; and (5) a roadmap toward clinically actionable precision prescribing. We argue that GLP-1 pharmacogenomics has moved from exploratory science to actionable discovery, and that its translation into clinical practice — particularly for the 1.3 billion people of South Asia — is the defining precision medicine challenge of the next decade in metabolic disease.
Keywords:
GLP-1 receptor agonists
; pharmacogenomics
; semaglutide
; tirzepatide
; GLP1R
; GIPR
; precision medicine
; obesity
; type 2 diabetes
; South Asian genomics
; GWAS
; drug-response variability
1. Introduction: The GLP-1 Revolution and the Variability Problem
The past decade has witnessed the emergence of GLP-1 receptor agonists as arguably the most consequential drug class in modern medicine. Originally developed for glycaemic control in type 2 diabetes, these agents have demonstrated remarkable efficacy across a spectrum of cardiometabolic conditions. The landmark SELECT trial documented a 20% relative risk reduction in major adverse cardiovascular events (MACE) with semaglutide 2.4 mg in individuals with obesity but without diabetes, leading to FDA approval for cardiovascular risk reduction in March 2024. In January 2025, semaglutide became the first GLP-1 agent indicated for chronic kidney disease (CKD) progression. Tirzepatide received FDA approval for obstructive sleep apnea (OSA) in December 2024. Evidence for GLP-1 receptor expression in brain reward circuits has prompted serious investigation into utility in addiction disorders, neurodegenerative disease, and depression.
By 2025, over 15 million adults in the United States were using GLP-1 therapies, and Ozempic alone surpassed $18.59 billion in global sales in 2024. Real-world pharmacy claims data showed that roughly 1 in 5 patients with type 2 diabetes in the US held an active GLP-1 prescription by mid-2024. Eli Lilly initiated the highest number of GLP-1 clinical trials in 2025, with the US (34.1%) and China (27.2%) accounting for the largest shares of global trial activity [24].
Yet beneath this success story lies a scientific problem with profound clinical consequences: response to GLP-1 drugs is highly variable. Some individuals lose more than 20% of body weight; others experience no meaningful benefit. Among those taking tirzepatide, nausea and vomiting affect patients differentially — at rates ranging from 5% to 78% depending on the individual. Real-world data show patients on semaglutide lost an average of 7.7% of body weight and those on tirzepatide lost 12.4% after one year — roughly half the efficacy observed in randomised controlled trials — with treatment discontinuation and genetic heterogeneity both contributing [30].
Pharmacogenomics — the study of how inherited genetic variation shapes drug response — offers the most rigorous scientific framework for understanding and ultimately predicting this variability. This article examines where the field stands today and where it is heading.
2. Mechanistic Foundations: How GLP-1 Drugs Work and Why Genetics Matters
2.1. Semaglutide (Ozempic® / Wegovy®): GLP-1 Receptor Agonism
Semaglutide is a chemically modified analogue of native GLP-1 with extended half-life enabling once-weekly subcutaneous dosing (and an oral formulation, Rybelsus®). It binds selectively to the GLP-1 receptor (encoded by GLP1R), stimulating glucose-dependent insulin secretion, suppressing glucagon, slowing gastric emptying, and reducing appetite via direct hypothalamic action. Its clinical success prompted the American Diabetes Association to designate GLP-1 receptor agonists as first-line injectable therapy for type 2 diabetes, ahead of insulin.
2.2. Tirzepatide (Mounjaro® / Zepbound®): Dual GIP/GLP-1 Agonism
Tirzepatide is a structural chimera — a single peptide incorporating elements of both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) — that acts on both GLP1R and GIPR simultaneously. This dual mechanism explains tirzepatide’s superior weight loss efficacy (up to 22.5% at 72 weeks in SURMOUNT-1) and its reduced propensity for nausea, as GIP receptor co-activation appears to buffer the emetic effects of GLP-1 receptor stimulation [7]. A critical pharmacogenomic implication follows: any genetic variant affecting GIPR function will differentially impact tirzepatide users relative to those taking semaglutide, which acts exclusively through GLP1R.
2.3. Why Genetics Shapes Response
Drug response is determined by pharmacokinetics (absorption, distribution, metabolism, excretion) and pharmacodynamics (drug–target interaction). For GLP-1 drugs, pharmacokinetic variability is relatively modest — semaglutide and tirzepatide are not CYP enzyme substrates and show limited hepatic metabolism — but pharmacodynamic variability is substantial. Polymorphisms in GLP1R, GIPR, and downstream signalling components including beta-arrestins (ARRB1, ARRB2), TCF7L2 (beta-cell function), FTO (adiposity regulation), MC4R (appetite), and ADIPOQ (adipokine signalling) modulate cellular response to drug–receptor binding. Additionally, DPP-4 variants influence endogenous GLP-1 degradation kinetics and may interact with exogenous drug pharmacology [1,2,4].
3. Key Genetic Variants: The Emerging Pharmacogenomic Map
Table 1 synthesises the current evidence on genetic determinants of GLP-1 drug response, organised by gene, variant, associated effect, relevant drug, and strength of evidence.
The same GLP1R variant rs10305420 associated with enhanced weight-loss efficacy in the 2026 Nature GWAS also co-localises with the nausea/vomiting signal — suggesting that increased receptor sensitivity is biologically linked to greater susceptibility to GI side effects. This efficacy–tolerability trade-off has direct implications for dose escalation strategies and warrants prospective study [1].
4. Landmark Research: From Hypothesis to Genome-Wide Evidence
4.1. The Lancet Diabetes & Endocrinology (2023): The First GLP-1 GWAS
Dawed et al. published what was — at the time of submission — the first genome-wide pharmacogenomic study of GLP-1 receptor agonists, itself a striking observation given the widespread clinical use of the drug class [2]. Analysing 4,571 adults with type 2 diabetes from four prospective cohorts (DIRECT, PRIBA, PROMASTER, GoDARTS) and two randomised controlled trials (HARMONY and AWARD), the study identified loci in GLP1R and ARRB1 (beta-arrestin 1) significantly associated with HbA1c reduction. A combined genotype score from these two genes identified 4% of the population with a 30% greater HbA1c reduction than the 9% of the population with the least favourable genotype — a clinically meaningful difference. Identified loci were GLP-1 receptor agonist-specific, with no association to other glucose-lowering drugs, strengthening pharmacogenomic specificity [2].

4.2. Nature Medicine (2025): Multi-Ancestry Biobank Analysis
German et al. (Nature Medicine, 2025) analysed 10,960 individuals from 9 multiancestry biobank studies across 6 countries [3]. This study found that genetic factors previously associated with BMI had limited impact on GLP-1 receptor agonist-induced weight loss — a negative finding of scientific importance. It suggests that the genetic determinants of GLP-1 response are distinct from those determining baseline obesity risk, and that drug-specific pharmacogenomic studies are required rather than simple repurposing of obesity GWAS data.
4.3. Nature (April 2026): The 23andMe GWAS — A Field-Defining Study
Published in Nature on 8 April 2026, the 23andMe Research Institute study by Auton et al. is the largest pharmacogenomic investigation of GLP-1 drugs to date [1]. Leveraging their crowdsourced consumer genomic platform, researchers surveyed 27,885 GLP-1 medication users (Ozempic, Wegovy, Mounjaro, Zepbound, and compounded variants), collecting self-reported weight loss and side-effect data.
Key Findings:
- Weight-loss efficacy: A missense variant in GLP1R (rs10305420, p.Pro7Leu), located in the receptor’s signal peptide, was associated with approximately 0.76 kg additional weight loss per allele copy (P = 2.9 × 10⁻¹⁰), attributed to enhanced receptor trafficking to the cell surface.
- GI side effects (both drugs): Variants near GLP1R (rs11760106 for vomiting, P = 2.5×10⁻²⁷; rs9357296 for nausea, P = 2.6×10⁻²⁸) were linked to nausea and vomiting across both drug cohorts.
- Tirzepatide-specific vomiting: A partial loss-of-function variant in GIPR (rs1800437, p.Glu354Gln) was associated with increased vomiting risk exclusively in tirzepatide users — not in those on semaglutide. The biological rationale: GIP receptor co-activation normally buffers GLP-1-induced nausea; when GIPR function is impaired, that buffering is lost.
- Compound risk: Individuals homozygous for risk alleles at both GLP1R and GIPR showed 14.8-fold increased odds of tirzepatide-mediated vomiting — a finding potentially enabling genotype-informed drug selection before treatment initiation.
- Predictive modelling: Integrating genetic, demographic, and clinical factors stratified patients into groups with 6%–20% expected weight loss and nausea probability ranging from 5% to 78% — a range with direct clinical significance.

4.4. Tufts University: Next-Generation Quad-Agonist Design (2025)
Researchers at Tufts University led by Professor Krishna Kumar designed a novel tetra-functional peptide compound targeting four hormonal pathways: GLP-1, GIP, glucagon, and peptide YY (PYY). The design explicitly acknowledges that ‘individual variation, possibly including how people express target receptors or respond to their corresponding hormones’ currently limits efficacy of existing drugs [7]. The compound attempts to overcome single-receptor genetic variability by diversifying target engagement across four independent hormonal axes.
4.5. AI-Driven Pharmacogenomics (2025)
A bioinformatics preprint (Research Square, 2025) used PharmGKB data, GTEx tissue expression profiles, and machine learning to predict therapeutic response to liraglutide, semaglutide, and tirzepatide [13]. Key tissue-level findings: GLP1R shows low expression in subcutaneous adipose tissue (TPM ~1.2) and minimal visceral expression; GIPR shows moderate expression in both depots (SAT ~4.5, VAT ~3.8 TPM). A cis-eQTL for GIPR (rs1800437, P = 1.8×10⁻⁴ in SAT) shows the minor allele correlating with 20% lower receptor expression — providing mechanistic tissue-level grounding for the 23andMe clinical observation. PGxAI (Palo Alto, CA) launched a semaglutide-specific AI-driven genetic profiling report in April 2025, reporting that up to one-third of prescribed patients carry variants associated with elevated adverse reaction risk [21].
5. Expanding Clinical Frontiers: Beyond Diabetes and Obesity
Table 2 summarises the rapidly expanding indications for GLP-1 receptor agonists. Each new indication will introduce indication-specific pharmacogenomic considerations that cannot be inferred from metabolic response genetics alone.
The expanding indication portfolio means that pharmacogenomic profiling in future must account for neurogenomic variants (APOE, BDNF, SNCA) for neurodegenerative indications, reward pathway genetics (DRD2, OPRM1) for addiction indications, and inflammatory pathway variants for MASH — in addition to the metabolic genes characterised to date.
6. The Biopharma Perspective
6.1. Novo Nordisk: Biomarker Investments and Precision Obesity Medicine
Novo Nordisk, creator of semaglutide, recorded more than DKr 120 billion ($18.59 billion) in Ozempic sales in 2024 alone. The company’s scientific strategy has increasingly emphasised precision obesity medicine, with investment in biomarker discovery programs — particularly around response heterogeneity in STEP and SELECT trial populations — and collaboration with academic centres including the MRC Epidemiology Unit at Cambridge and Lund University. The IMI-funded DIRECT and GoDARTS cohorts that contributed to the 2023 Lancet GWAS were partly enabled by Novo Nordisk partnerships. The company has indicated interest in combining CGM data with genetic profiles to guide dose escalation, though no pharmacogenomic diagnostic has been commercially paired with any Novo Nordisk product to date.
6.2. Eli Lilly: Tirzepatide Pharmacogenomics and Next-Generation Pipeline
Eli Lilly initiated more GLP-1 clinical trials than any other company in 2025, posting 45% revenue growth and 96% EPS growth that year, with 2026 revenue guidance of $80–$83 billion [31]. Tirzepatide’s dual mechanism makes it inherently more pharmacogenomically complex than semaglutide — as the 23andMe Nature study demonstrated, GIPR variants differentially affect tirzepatide tolerability in a way entirely irrelevant for semaglutide users. Lilly’s pipeline includes retatrutide (triple GLP-1/GIP/glucagon agonist) and orforglipron (oral GLP-1 agonist), each introducing additional receptor–gene axes. Lilly has built genomics infrastructure through biobank partnerships with FinnGen and deCODE Genetics (Amgen/Iceland) contributing GLP1R variant studies.
6.3. 23andMe Research Institute: Consumer Genomics Meets Pharmacogenomics
The April 2026 Nature study marks a watershed moment in pharmacogenomic evidence generation. Rather than prospectively enrolled clinical cohorts — expensive, slow, and historically Eurocentric — 23andMe recruited 27,885 GLP-1 users within months through its consumer platform. The organisation immediately commercialised findings: a GLP-1 Medications: Weight Loss and Nausea report is now available to Total Health service members, providing personalised efficacy and tolerability risk estimates from genetic, demographic, and clinical data [33–35]. CMO Noura Abul-Husn described the vision as transforming weight-loss discussions ‘from a trial-and-error approach into data-driven, shared decision-making.’ This consumer-genomics-to-clinical-decision pathway — validated in Nature and immediately deployed — represents a new model for pharmacogenomics translation.
6.4. PGxAI and the AI-Pharmacogenomics Ecosystem
PGxAI (Palo Alto, CA, founded 2023), backed by ATEM Capital and led by a UCSF pharmacogenomics expert, released an AI-driven semaglutide genetic profiling report in April 2025 [21]. Integrated with InterSystems HealthShare for real-time EHR clinical decision support, and partnered with NVIDIA, Google, and Microsoft for computational infrastructure, PGxAI is expanding coverage to tirzepatide, next-generation GLP-1 agents, and CNS-targeting compounds. The broader pharmacogenomics-as-a-service ecosystem includes Broad Institute-affiliated programs, population biobanks (UK Biobank, FinnGen, BioMe, All of Us), and a growing number of startups positioning at the intersection of genomics, AI, and metabolic medicine.
7. India and South Asia: A Critical but Underrepresented Frontier
7.1. The Indian Diabetes and Obesity Burden
India is the global epicentre of type 2 diabetes, with over 101 million patients — the world’s largest absolute burden. The ICMR-INDIAB-17 study (Lancet Diabetes & Endocrinology, 2023) documented the alarming national metabolic trajectory. Indian patients present with diabetes at younger ages and lower BMIs, exhibit disproportionately high abdominal adiposity, and carry a metabolic disease architecture driven by distinct genetic and environmental factors. This creates a precision medicine imperative: pharmacogenomic tools developed exclusively in European-ancestry populations may be miscalibrated for the 1.3 billion people of South Asia.
7.2. Indian-Specific Pharmacogenomic Profile
A landmark 2024 study in BMJ Open Diabetes Research & Care (Sivadas, Sahana et al., CSIR-IGIB and St. John’s Research Institute, Bangalore) established the pharmacogenomic landscape for non-insulin antidiabetic drugs — including GLP-1 analogs — in the Indian population using the IndiGen dataset of 1,029 whole genomes [5]. Key finding: Indians and South Asians carry a distinct pharmacogenomic profile, with an excess of poor treatment-response-associated alleles across multiple drug classes. The IndiGen dataset catalogued 53.6 million variants from Indian genomes showing systematic allele frequency differences from European, East Asian, and African reference populations. The GIPR variant rs1800437 (Glu354Gln) — central to the April 2026 tirzepatide finding — has documented allele frequency differences across South Asian versus European populations, meaning the 14.8-fold vomiting risk discovered in the 23andMe study requires explicit validation in Indian cohorts.
7.3. Evidence for Enhanced GLP-1 Efficacy in South Asians
Emerging comparative data suggest GLP-1 receptor agonists may be more effective in Asian populations for glycaemic control. A 2025 comparative analysis found the HbA1c reduction with GLP-1 receptor agonists was 0.32% greater in Asian-dominant studies, and the proportion of patients achieving HbA1c ≤7.0% was five times higher in the GLP-1 RA group versus controls in Asians (vs. two times in non-Asians) [9]. Cardiovascular benefits were also greater in Asian patients. Whether this reflects higher GLP1R expression frequencies, favourable variant allele distributions in Indian populations, or other biological differences requires dedicated South Asian pharmacogenomic investigation.
7.4. Indian Expert Perspectives
Indian endocrinologists responded immediately to the April 2026 Nature publication. Dr. V. Mohan, Chairman of the Madras Diabetes Research Foundation (MDRF) — who has treated GLP-1 patients since the liraglutide era — described the findings as ‘long-overdue scientific confirmation of a clinical pattern I had been tracking for over a decade,’ noting four distinct patient response phenotypes he had empirically observed. He explicitly linked this to pharmacogenomics and raised the question of whether DPP-4 inhibitor-like ethnic variation (DPP-4 inhibitors are significantly more effective in Indians and Koreans) might exist for GLP-1 drugs [43]. Dr. Ambrish Mithal (Max HealthCare) called it ‘a step towards precision medicine’ and identified non-responders as the immediate clinical use case for genetic testing [43].
7.5. Indian Research Institutions and Infrastructure
Key institutions positioned for South Asian GLP-1 pharmacogenomics research:
- CSIR-Institute of Genomics and Integrative Biology (CSIR-IGIB), New Delhi — led the IndiGen pharmacogenomics study; holds the largest Indian whole-genome dataset with GLP1R/GIPR variant frequencies
- Madras Diabetes Research Foundation (MDRF), Chennai — world-class diabetes clinical cohorts; Dr. V. Mohan’s group is the natural home for prospective GLP-1 pharmacogenomic studies
- St. John’s Research Institute, Bangalore — co-led the 2024 BMJ pharmacogenomics paper; has biobank infrastructure for South Asian metabolic disease
- Translational Health Science and Technology Institute (THSTI), Faridabad — national translational research with genomics capabilities
- GenomeIndia project — CSIR-led initiative sequencing 10,000 Indian whole genomes across diverse linguistic/geographic groups; an ideal platform for population-level GLP-1 pharmacogenomics

8. Safety Signals with Pharmacogenomic Implications
8.1. Gastrointestinal Toxicity
The most extensively characterised pharmacogenomic safety signal for GLP-1 drugs is gastrointestinal — nausea, vomiting, and diarrhoea account for the majority of treatment discontinuations. The 23andMe Nature GWAS demonstrated that GLP1R efficacy variants co-localise with GI side-effect signals, suggesting mechanistic linkage between receptor sensitivity and emesis risk. For tirzepatide specifically, GIPR rs1800437 identifies a high-risk subgroup (14.8-fold increased vomiting odds when combined with GLP1R risk allele), providing a potentially actionable pre-treatment screen [1,40].
8.2. Neuropsychiatric Risk
As of December 2025, multiple regulatory agencies — including the Australian TGA — updated product warnings across the entire GLP-1 RA class to include consistent language regarding the potential risk of suicidal thoughts and behavioural changes, following multi-country pharmacovigilance investigations [9]. The neuropsychiatric risk likely has a genetic component: variants in serotonin and dopamine signalling pathways relevant to the GLP-1 receptor’s role in brain reward circuits may predict vulnerability. This is an urgent and underinvestigated area for pharmacogenomic research.
8.3. Drug–Drug Interaction: Oral Contraception (Tirzepatide)
The Australian TGA identified a potential interaction between tirzepatide and oral contraceptives, updating warnings to advise use of non-oral or barrier contraception for 4 weeks after initiation and after each dose increase [9]. The mechanism — tirzepatide’s effect on gastric emptying altering oral drug absorption — may be modulated by genetic variants in drug absorption transporters (ABCB1, SLC transporters) and phase I/II metabolic enzymes. This represents a pharmacokinetic pharmacogenomic interaction warranting dedicated study.
8.4. Lean Mass Loss
Real-world data indicate 25–39% of total weight lost on GLP-1 therapies comes from lean mass. In STEP-1 (semaglutide), lean mass constituted 45.2% of total weight lost [25]. In SURMOUNT-1 (tirzepatide), lean mass represented 25.7% — a more favourable ratio. Variants in myostatin signalling (MSTN), IGF pathway genes (IGF1R), and muscle-specific metabolic regulators may predict differential lean mass loss — an important pharmacogenomic safety consideration for older patients and those at risk of sarcopenia.
9. Translation Challenges: From Discovery to Clinic
9.1. The Ancestry Diversity Gap
The 23andMe Nature study — despite its unprecedented scale — enrolled 78.3% European-ancestry participants. South Asia, with the world’s largest diabetes burden, contributed essentially zero. The 2025 Nature Medicine multi-ancestry biobank study showed that effect sizes of known BMI variants differ by genetic ancestry for GLP-1 response [3]. Until GWAS studies are conducted at scale in South Asian, East Asian, African, and Latin American populations, pharmacogenomic prescribing recommendations will remain Eurocentric and potentially misleading when applied globally.
9.2. Self-Report Limitations and Real-World Validation
The 23andMe study relied on self-reported weight loss and side effects. The correlation between self-reported and EHR-documented BMI change was reasonable (Pearson r = 0.57) in the subgroup with Apple HealthKit data, but the absolute effect size gap (median −11.8% self-report vs −5.79% EHR) indicates reporting bias [1]. Prospective studies with objectively measured outcomes are needed to confirm findings.
9.3. Effect Sizes and Polygenic Prediction
The 0.76 kg additional weight loss per GLP1R risk allele copy — while statistically robust (P = 2.9×10⁻¹⁰) — is modest in absolute terms relative to the 15–22 kg lost in clinical trials. Current pharmacogenomic predictors explain only a fraction of response variability. Polygenic scores combining multiple variants, and multi-modal models integrating genomics with metabolomics, microbiome, and clinical variables, will be required to achieve clinically meaningful individual-level prediction.
9.4. Regulatory and Implementation Pathways
No regulatory agency has mandated or recommended pharmacogenomic testing before GLP-1 prescription. CPIC (Clinical Pharmacogenomics Implementation Consortium) does not yet have GLP-1 RA guidelines. ADA/EASD guidelines recommend GLP-1 RAs as second-line therapy without pharmacogenomic stratification. Bridging this gap requires: (1) multi-ethnic prospective studies with pre-specified pharmacogenomic endpoints; (2) regulatory submissions for companion diagnostic review; (3) cost-effectiveness analyses demonstrating genotyping reduces treatment failure costs sufficiently to justify testing; and (4) EHR integration infrastructure for point-of-prescribing decision support [20].
10. Roadmap: Precision Medicine for GLP-1 Pharmacogenomics
Near-Term (2026–2028): Replication and Diversity
- Large-scale replication of Nature 2026 findings in non-European cohorts — specifically South Asian, East Asian, and African ancestry populations
- Prospective India GLP-1 pharmacogenomics cohort study (5,000–10,000 patients; MDRF/CSIR-IGIB partnership; GenomeIndia alignment)
- CPIC guideline development for GLP-1 receptor agonists based on GLP1R and GIPR genotype — the first precision prescribing tool in metabolic medicine
- Integration of GLP-1 pharmacogenomics into existing pre-emptive pharmacogenomic panels (PGx-Passport, YouScript, OneOme RightMed)
Medium-Term (2028–2033): Clinical Implementation
- Companion diagnostic approval (FDA/EMA/CDSCO) for GLP1R/GIPR panel as a prescribing aid for semaglutide vs. tirzepatide selection
- EHR-integrated clinical decision support (building on PGxAI/HealthShare model) flagging high-risk tirzepatide genotypes at point of prescribing
- Pharmacogenomic sub-analyses of GLP-1 trials in new indications (neurodegeneration, addiction, MASH)
- AI-powered multi-omics models integrating genomics, metabolomics, gut microbiome, and clinical variables for holistic response prediction
Long-Term (2033–2040): Routine Genotype-Guided Prescribing
- Standard pre-treatment genotyping for GLP-1 drugs in patients with complex obesity or non-response — analogous to CYP2C19 testing before clopidogrel or BRCA testing before PARP inhibitors
- Next-generation drug design: quad-agonists and CNS-targeted compounds engineered for pharmacogenomic resilience across known genetic backgrounds
- National pharmacogenomics programs in India (GenomeIndia) generating actionable prescribing data for the world’s largest diabetes population
- Equitable access frameworks ensuring precision tools reach low- and middle-income countries where the GLP-1 disease burden is greatest
11. Conclusions
The pharmacogenomics of GLP-1 receptor agonists has reached a critical juncture. The April 2026 23andMe Nature GWAS — the largest genomic investigation of drug response in this class — has demonstrated that variants in GLP1R and GIPR are robustly associated with both weight-loss efficacy and drug-specific tolerability. The choice between Ozempic and Mounjaro need not, in the near future, be made by trial and error.
What remains is the hard work of translation: expanding findings to the full diversity of the human genetic landscape, building clinical evidence for pre-treatment genotyping, navigating regulatory pathways, and ensuring equitable access. India — with the world’s largest diabetes burden, a distinctive South Asian pharmacogenomic profile, and world-class genomics institutions including CSIR-IGIB and MDRF — stands at the centre of both this opportunity and this obligation.
The fundamental question of pharmacogenomics has always been: why does this drug work for some people and not others? For GLP-1 drugs, we are for the first time beginning to have a genetic answer. The more important question — and the one that will define this field for the next decade — is what we will do with it.
Artificial Intelligence Disclosure
Artificial intelligence tools (specifically, Claude, Anthropic) were used to assist in literature synthesis, document drafting, and table generation during the preparation of this manuscript. All AI-generated content was reviewed, verified, and edited by the authors. The authors take full responsibility for the accuracy and integrity of all content in this manuscript. AI tools were not used as authors and are not listed as co-authors.
Informed Consent Statement
This article is a narrative review of published literature. No primary data were collected. No human participants or animals were involved. No ethical approval or IRB exemption was required for this review.
Data Availability Statement
No new data were generated for this review. All data and findings cited herein are drawn from published peer-reviewed literature, preprints, and publicly accessible regulatory and institutional reports as cited in the References section. All cited sources are publicly accessible.
References
- Auton A et al. (23andMe Research Institute) Genetic predictors of GLP1 receptor agonist weight loss and side effects; Nature, 8 Apr 2026. [Google Scholar] [CrossRef]
- Dawed, A.Y.; et al. Pharmacogenomics of GLP-1 receptor agonists: a genome-wide analysis of observational data and large randomised controlled trials. Lancet Diabetes Endocrinol. 2023, 11(1), 33–41. [Google Scholar] [CrossRef] [PubMed]
- German, J.; et al. Association between plausible genetic factors and weight loss from GLP1-RA and bariatric surgery. Nat Med. 2025, 31, 2269–2276. [Google Scholar] [CrossRef]
- Han, R.; He, P. Pharmacogenomics of Tirzepatide: Genomic Insights into Dual GIP/GLP-1 Agonist Response in Type 2 Diabetes and Atherosclerosis. Pharmaceuticals 2025, 18(9), 1261. [Google Scholar] [CrossRef] [PubMed]
- Sivadas, A.; Sahana, S.; Jolly, B.; et al. Landscape of pharmacogenetic variants associated with non-insulin antidiabetic drugs in the Indian population. BMJ Open Diabetes Res Care 2024, 12(2), e003769. [Google Scholar] [CrossRef]
- Celletti, F.; Farrar, J.; De Regil, L. WHO Guideline on the Use and Indications of GLP-1 Therapies for the Treatment of Obesity in Adults. JAMA 2026, 335(5), 434–438. [Google Scholar] [CrossRef]
- Dinsmore, T.; Kumar, K.; et al. Novel tetra-functional GLP-1/GIP/glucagon/PYY chimeric peptide for weight management. J Am Chem Soc. Full citation to be confirmed upon publication. 2025. [Google Scholar]
- Wilding, J.P.H.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). N Engl J Med. 2021, 384(11), 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.; et al. Pathophysiology of type 2 diabetes: A focus on the metabolic differences among southeast Asian, Chinese and Indian populations. Diabetes Obes Metab 2025. [Google Scholar] [CrossRef]
- Lincoff, A.M.; et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT). N Engl J Med. 2023, 389(24), 2221–2232. [Google Scholar] [CrossRef]
- Jastreboff, A.M.; et al. Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). N Engl J Med. 2022, 387(3), 205–216. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; et al. Semaglutide and Kidney Outcomes in Type 2 Diabetes (FLOW). N Engl J Med 2024. [Google Scholar] [CrossRef] [PubMed]
- Pharmacogenomics of anti-obesity drugs: A bioinformatics approach. Research Square 2025. [CrossRef] [PubMed]
- Multi-author. Emerging Frontiers in GLP-1 Therapeutics: A Comprehensive Evidence Base. Pharmaceutics 2025, 17(8), 1036. [CrossRef]
- Additional references 15–50 to be added from manuscript citations — full reference list to be compiled before submission.

Table 1.
Key pharmacogenomic variants for GLP-1 receptor agonists (as of April 2026).
| Gene | Variant (rs ID) | Associated Effect | Drug(s) | Evidence |
|---|---|---|---|---|
| GLP1R | rs10305420 (Pro7Leu) | Increased weight loss (~0.76 kg/allele) | Both | Strong: Nature 2026 GWAS (n=27,885) |
| GLP1R | rs6923761 (Gly168Ser) | Altered glycaemic response; sex-specific weight effects | GLP-1 RAs broadly | Moderate: multiple cohort studies |
| GLP1R | rs11760106 / rs9357296 | Increased risk of nausea / vomiting | Both | Strong: Nature 2026 GWAS |
| GLP1R | rs367543060 | Reduced glycaemic response | GLP-1 RAs broadly | Moderate: Kyriakidou et al. |
| GIPR | rs1800437 (Glu354Gln) | Increased vomiting (partial loss-of-function) | Tirzepatide ONLY | Strong: Nature 2026 GWAS (drug-specific) |
| GIPR | rs2287019 (C>T) | Greater fasting glucose improvement | Tirzepatide | Moderate: POUNDS LOST trial |
| ARRB1 | Multiple rare variants | 30% greater HbA1c reduction | GLP-1 RAs broadly | Strong: Lancet Diabetes 2023 (n=4,571) |
| TCF7L2 | rs7903146 | Modifies beta-cell glycaemic response | GLP-1 RAs broadly | Moderate: multiple GWAS |
| FTO | rs9939609 | Adiposity modulation; energy homeostasis | Tirzepatide | Emerging |
| MC4R | Multiple variants | Appetite regulation; weight loss prediction | Both | Emerging — bioinformatics |
| ADIPOQ | Multiple variants | BMI reduction prediction | Tirzepatide | Emerging |
| APOE | e2/e3/e4 | Cardiovascular/lipid response modulation | Tirzepatide (CV) | Emerging |
| DPP4 | Expression eQTLs | Incretin degradation; drug interaction | All GLP-1 RAs | Emerging — GTEx data |
Table 2.
Approved and emerging indications for GLP-1 receptor agonists (2024–2026).
| Indication | Key Evidence | Status (2024–26) |
|---|---|---|
| Type 2 Diabetes | ADA first-line injectable; HbA1c −1.5–2.0% | Fully approved (all agents) |
| Obesity | STEP/SURMOUNT: 7–24% weight loss | Semaglutide, Tirzepatide approved |
| Cardiovascular Risk | SELECT trial: 20% MACE reduction | Semaglutide FDA-approved (Mar 2024) |
| Chronic Kidney Disease | FLOW trial: reduced kidney failure progression | Semaglutide FDA-approved (Jan 2025) |
| Obstructive Sleep Apnea | SURMOUNT-OSA: significant AHI reduction | Tirzepatide FDA-approved (Dec 2024) |
| MASH (Liver Disease) | Phase 3 data emerging | Under regulatory review |
| Osteoarthritis | STEP-9: 14.1-point WOMAC improvement vs placebo | Strong signals; off-label |
| Neurodegeneration (AD/PD) | 70% reduced AD risk vs insulin (US EHR, n>1M) | Phase 2 trials ongoing |
| Substance Use Disorders | Lower opioid overdose/alcohol intoxication (n=1.3M) | Phase 2 trials ongoing |
| Adolescent Obesity | STEP TEENS; 600% Rx increase 2020–2024 | Semaglutide/Liraglutide approved ≥12y |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



