Submitted:
14 April 2026
Posted:
14 April 2026
You are already at the latest version
Abstract
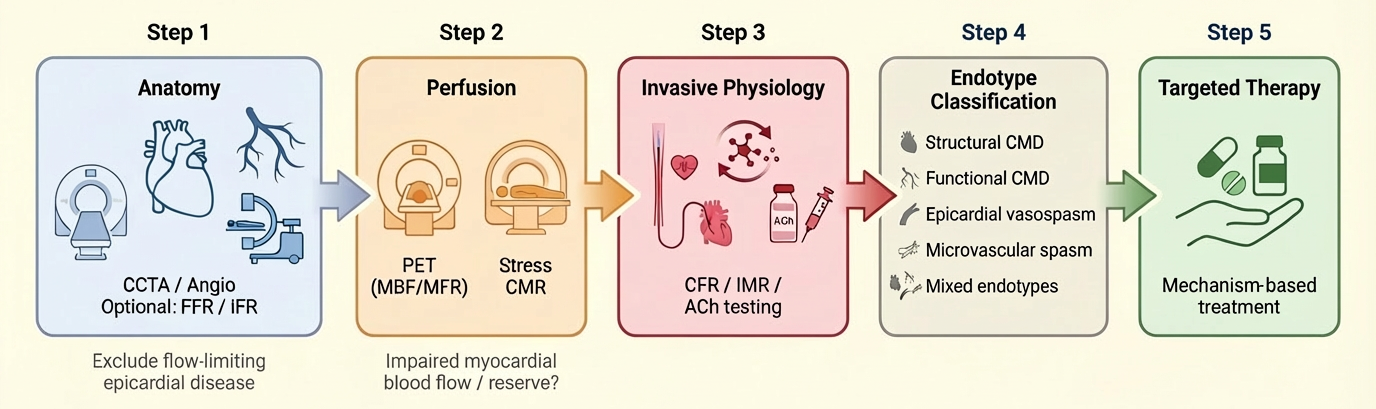
Angina or objective myocardial ischaemia in the absence of obstructive coronary artery disease, referred to as ANOCA/INOCA, represents a prevalent and clinically significant condition associated with persistent symptoms, impaired quality of life, and increased healthcare utilisation. Contemporary evidence has reframed these syndromes as manifestations of coronary vascular dysfunction, encompassing structural and functional coronary microvascular dysfunction, epicardial vasospasm, microvascular spasm, and mixed phenotypes. In this context, multimodality imaging should not be conceptualised as sequential test accumulation, but rather as a structured, mechanism-based diagnostic strategy aimed at defining the underlying coronary endotype. The 2024 ESC Guidelines for chronic coronary syndromes endorse dedicated diagnostic pathways beyond a stenosis-centred paradigm and support the use of invasive coronary function testing (ICFT) in selected patients with persistent symptoms or inconclusive non-invasive findings. An integrated approach combining anatomical assessment (coronary computed tomography angiography or invasive angiography ± pressure-based indices), quantitative perfusion imaging (positron emission tomography or stress cardiovascular magnetic resonance), and ICFT (including coronary flow reserve, microvascular resistance indices, and acetylcholine provocation testing) enables comprehensive characterisation of coronary physiology and vasomotor function. This review proposes a pragmatic framework linking diagnostic findings to targeted therapy through a test-to-endotype-to-therapy paradigm. We summarise the strengths and limitations of each modality, discuss implementation challenges, and highlight the clinical relevance of endotype-driven management. By shifting from a stenosis-centred to a physiology- and mechanism-based approach, this strategy has the potential to close the longstanding gap between diagnosis and treatment in patients with ischaemia beyond obstructive coronary disease.
Keywords:
ANOCA
; INOCA
; coronary microvascular dysfunction
; coronary vasospasm
; myocardial blood flow
; coronary flow reserve
; invasive coronary function testing
; multimodality imaging
; PET
; CMR
1. Introduction
A substantial proportion of patients undergoing evaluation for chronic chest pain or suspected myocardial ischaemia are found to have non-obstructive coronary arteries at invasive coronary angiography (ICA) or coronary computed tomography angiography (CCTA). Historically, these patients were frequently reassured or labelled as having non-cardiac symptoms, reflecting a diagnostic paradigm largely centred on the presence or absence of flow-limiting epicardial stenosis. However, this approach fails to account for the complexity of myocardial ischaemia and overlooks a substantial burden of coronary vascular dysfunction (1,2).
Contemporary evidence has fundamentally redefined angina or ischaemia with non-obstructive coronary arteries (ANOCA/INOCA) as a clinically meaningful syndrome rather than a diagnosis of exclusion. In many patients, symptoms are driven by abnormalities of coronary vascular function, including structural and functional coronary microvascular dysfunction, epicardial vasospasm, microvascular spasm, or mixed endotypes (2,3). Standardized diagnostic criteria from the Coronary Vasomotion Disorders International Study Group (COVADIS) have provided a reproducible framework for defining vasospastic angina and microvascular angina, enabling more consistent phenotyping across studies and clinical practice (4,5).
Importantly, ischaemic findings in this population, historically considered “false positive” in the absence of obstructive coronary disease, may instead reflect true coronary microvascular or vasomotor dysfunction. In a contemporary invasive physiology study, abnormal exercise electrocardiographic findings in patients with ANOCA were closely associated with coronary microvascular dysfunction, challenging the traditional assumption that the absence of obstructive epicardial disease implies a non-ischaemic mechanism (6).
The 2024 ESC Guidelines for chronic coronary syndromes formally integrate ANOCA/INOCA within the CCS framework and support structured diagnostic pathways extending beyond anatomical imaging alone (1). Within this paradigm, the central clinical question is no longer limited to whether ischaemia is present, but rather which underlying mechanism is responsible and how this should guide treatment. This shift reflects a broader transition from anatomy-based to mechanism-based cardiovascular medicine, with increasing emphasis on comprehensive functional assessment of the coronary circulation (7).
A major limitation of traditional approaches is the reliance on anatomical assessment alone. The severity of epicardial stenosis does not reliably predict its physiological significance, and pressure-based indices such as fractional flow reserve (FFR), while essential for evaluating obstructive disease, do not fully capture coronary flow dynamics. Discordance between pressure-based and flow-based indices is common and reflects the independent contribution of the coronary microcirculation to myocardial perfusion (8). Consequently, patients may exhibit persistent symptoms and objective ischaemia despite non-obstructive coronary arteries or non-significant pressure gradients.
In this context, multimodality imaging requires redefinition. Rather than representing sequential test accumulation, it should be understood as a structured, endotype-oriented diagnostic strategy. A pragmatic approach integrates: (i) anatomical assessment to exclude obstructive coronary artery disease and define plaque burden, (ii) quantitative perfusion imaging to detect global or regional flow impairment and (iii) invasive coronary function testing (ICFT) to define coronary endotypes and guide stratified therapy (1–3,7).
This review aims to provide a clinically actionable and ESC-aligned synthesis of multimodality imaging and invasive coronary function testing in ANOCA/INOCA. We propose a mechanism-based framework linking diagnostic findings to pathophysiological endotypes and targeted treatment, with the goal of transitioning from descriptive diagnosis to precision cardiovascular care.
2. Materials and Methods
This narrative review was conducted using a structured and iterative literature search to identify studies addressing the pathophysiology, diagnosis, and management of ANOCA/INOCA, with a specific focus on multimodality imaging and invasive coronary function testing.
Electronic searches were performed in PubMed, Embase, and Web of Science, covering literature published up to January 2026. The search strategy combined controlled vocabulary and free-text terms, including “ANOCA”, “INOCA”, “coronary microvascular dysfunction”, “vasospastic angina”, “microvascular spasm”, “coronary vasomotor disorders”, “positron emission tomography”, “stress cardiovascular magnetic resonance”, “coronary flow reserve”, “index of microcirculatory resistance”, and “coronary function testing”.
Study selection was guided by clinical relevance and methodological robustness. Priority was given to contemporary guideline documents, expert consensus statements, pivotal randomized clinical trials, prospective studies, and multicentre observational registries, particularly those informing current diagnostic and therapeutic strategies. Reference lists of key articles were manually screened to identify additional relevant studies.
Given the narrative nature of this review, no formal systematic review protocol or quantitative synthesis was undertaken. Instead, the available evidence was synthesised to provide a mechanism-based, clinically oriented framework linking diagnostic modalities to coronary endotypes and targeted management strategies.
3. Definitions and Clinically Actionable Endotypes
ANOCA/INOCA comprises multiple coronary endotypes with distinct diagnostic and therapeutic implications. A pragmatic classification into four principal endotypes is clinically useful, while acknowledging frequent overlap in real-world practice (1–3).
3.1. Structural Coronary Microvascular Dysfunction (CMD)
This endotype is characterised by impaired vasodilatory capacity and/or increased minimal microvascular resistance, reflecting structural alterations of the coronary microcirculation, including rarefaction, remodelling and perivascular fibrosis. It is typically identified by reduced myocardial flow reserve (MFR) on quantitative perfusion imaging, positron emission tomography (PET) or stress cardiovascular magnetic resonance (CMR), or by reduced coronary flow reserve (CFR) in association with elevated microvascular resistance indices, such as the index of microcirculatory resistance (IMR), during invasive coronary function testing (4,5,7).
3.2. Functional/Endothelial CMD
Functional CMD is characterised by impaired endothelial-mediated vasodilation and abnormal regulation of vascular tone. In contrast to structural CMD, microvascular resistance may be normal or only mildly elevated, while abnormalities are primarily related to endothelial dysfunction and impaired nitric oxide bioavailability. This phenotype may present with reduced CFR and/or abnormal vasoreactivity during invasive testing and frequently overlaps with vasospastic disorders (2,5).
3.3. Epicardial Vasospasm (Vasospastic Angina)
Epicardial vasospasm is defined by transient, reversible constriction of epicardial coronary arteries leading to myocardial ischaemia. According to COVADIS criteria, diagnosis requires the reproduction of symptoms with ischaemic electrocardiographic changes and angiographic evidence of ≥90% vasoconstriction during provocative testing, typically with intracoronary acetylcholine (3). This endotype reflects hyperreactivity of vascular smooth muscle and endothelial dysfunction and represents a dynamic disorder of coronary tone regulation and is increasingly recognised in contemporary clinical practice (9).
3.4. Microvascular Spasm
Microvascular spasm is characterised by angina and ischaemic electrocardiographic changes during acetylcholine provocation in the absence of significant epicardial constriction. This phenotype reflects abnormal vasomotor reactivity (hyperreactivity) at the level of the microcirculation and cannot be detected without dedicated functional testing and is therefore frequently underdiagnosed (3,7).
Importantly, all these endotypes are not mutually exclusive. Mixed phenotypes, particularly the coexistence of CMD and vasospasm, are common and clinically relevant. Contemporary registry data suggest that a large proportion of ANOCA patients exhibit overlapping mechanisms, highlighting the need for comprehensive functional evaluation rather than binary classification (5,10). This reinforces the concept that endotyping should be viewed as a spectrum of interacting mechanisms rather than discrete categories.
Emerging data further suggest that the distribution of endotypes may be influenced by biological factors such as sex, with microvascular dysfunction more frequently observed in women and epicardial vasomotor disorders more prevalent in men (11). These findings highlight the need for comprehensive physiological assessment rather than reliance on single-modality testing.
Overall, this framework reinforces that ANOCA/INOCA should be approached as a spectrum of coronary vascular dysfunction. Accurate endotype definition requires integration of anatomical imaging, quantitative perfusion assessment, invasive coronary function testing, and represents the cornerstone of mechanism-based management.
4. Pathophysiological Rationale
Coronary vascular dysfunction represents the main pathophysiological substrate underlying ANOCA/INOCA and includes a heterogeneous spectrum of abnormalities involving both the epicardial coronary arteries and the coronary microcirculation (12,13). Despite their mechanistic diversity, these mechanisms ultimately converge on a final common pathway of inadequate myocardial blood flow relative to metabolic demand, resulting in myocardial ischaemia (14).
4.1. Coronary Flow as the Final Common Pathway
A fundamental principle of coronary physiology is that myocardial oxygen extraction at rest is already high and only modestly augmentable; accordingly, increases in myocardial oxygen demand are met predominantly through proportional increases in coronary blood flow rather than further oxygen extraction (15,16). Consequently, the capacity of the coronary circulation to augment flow, rather than the mere presence of anatomical stenosis, is the key determinant of perfusion adequacy (15,17). This concept highlights a critical limitation of stenosis-centred paradigms: epicardial coronary stenosis represents only one of several possible determinants of impaired flow and its anatomical severity does not reliably predict its physiological impact (17–20). Conversely, even in the absence of obstructive epicardial disease, impaired coronary flow reserve may arise from microvascular dysfunction, vasospastic disorders, or both (3,12).
4.2. Pressure-Based Versus Flow-Based Physiology
The distinction between pressure-based and flow-based indices is central to understanding ANOCA/INOCA. FFR quantifies pressure gradients across epicardial stenoses and remains the reference standard for defining the haemodynamic significance of obstructive coronary artery disease (13,18,20). However, as a pressure-derived index, FFR does not directly measure coronary blood flow and therefore does not account for abnormalities related to non-focal atherosclerotic disease or the coronary microcirculation, both of which are key determinants of ischaemia in ANOCA/INOCA (2,17,19,21).
This limitation becomes evident in the presence of discordance between pressure- and flow-based indices. A preserved FFR does not exclude impaired myocardial perfusion, as coronary flow may be limited by microvascular dysfunction, extensive epicardial disease, or altered resting haemodynamics (8,21–23).
In contrast, flow-based indices such as CFR and MFR reflect the integrated capacity of the coronary circulation to augment blood flow, capturing the combined contribution of epicardial and microvascular compartments (3). Accordingly, patients with preserved FFR but reduced CFR or MFR represent a distinct physiological phenotype, typically associated with coronary microvascular dysfunction and/or generalised atherosclerotic burden, and characterised by persistent symptoms and worse clinical outcomes despite the absence of focal flow-limiting stenosis (22–25).
Therefore, a normal FFR should not be interpreted as evidence of normal coronary physiology in patients with ANOCA/INOCA.
4.3. Mechanisms of Coronary Microvascular Dysfunction
CMD encompasses a spectrum of structural and functional abnormalities affecting vessels below the resolution of conventional angiography. Structural CMD is characterised by microvascular remodelling, luminal narrowing, rarefaction, and perivascular fibrosis, leading to increased minimal microvascular resistance and impaired vasodilatory capacity (26).
Functional CMD, in contrast, is primarily driven by endothelial dysfunction and impaired nitric oxide bioavailability, resulting in abnormal regulation of vascular tone and attenuated vasodilatory responses. These abnormalities may be exacerbated by inflammation, oxidative stress, and cardiometabolic comorbidities, including diabetes, obesity, and hypertension (27).
Additional contributors include extravascular compressive forces, particularly in the setting of left ventricular hypertrophy, diastolic dysfunction, or increased filling pressures, as well as autonomic dysregulation, which may further impair microvascular function (28,29). Collectively, these mechanisms reduce the capacity of the coronary microcirculation to augment flow during stress, thereby leading to myocardial ischaemia in the absence of obstructive epicardial coronary disease (12,27).
4.4. Vasomotor Disorders and Dynamic Flow Limitation
In contrast to CMD, vasospastic disorders are characterised by dynamic, reversible reductions in coronary blood flow due to transient vasoconstriction. These abnormalities may involve the epicardial arteries or the microcirculation and are related to a complex interplay between endothelial dysfunction and vascular smooth muscle cell hyperreactivity (30–33). Key molecular pathways implicated in vasospasm include enhanced Rho-kinase activity, increased calcium sensitivity of vascular smooth muscle, and impaired endothelial-derived vasodilatory signalling. These mechanisms result in episodic reductions in coronary blood flow that may occur at rest or in response to triggers such as emotional stress, cold exposure, or pharmacological stimuli (33–35). Importantly, vasospastic and microvascular mechanisms frequently coexist. The interaction between impaired vasodilation (CMD) and enhanced vasoconstriction (vasospasm) contributes to the heterogeneity of clinical presentation and may explain variability in symptoms, test results, and treatment response (3,12,36).
4.5. Prognostic Implications of Flow Impairment
A key advance in the field has been the recognition that coronary vascular dysfunction is not a benign condition. Impaired coronary flow reserve, assessed either invasively or by quantitative imaging, has consistently been associated with an increased risk of major adverse cardiovascular events, independent of the presence of obstructive coronary artery disease (37,38).
Large cohort studies using PET have demonstrated that reduced myocardial flow reserve is a strong and independent predictor of mortality and cardiovascular events, even in patients with angiographically normal or non-obstructive coronary arteries.8 Similarly, invasive physiological studies have shown that abnormalities in CFR and microvascular resistance indices are associated with adverse outcomes and persistent symptom burden (39).
These findings reinforce that coronary vascular dysfunction is a pathophysiologically relevant and prognostically important disease process rather than a benign or merely functional condition. Moreover, they provide the mechanistic rationale for a shift towards physiology-guided, endotype-based diagnostic and therapeutic strategies (2,3,24,40,41).
4.6. From Pathophysiology to Mechanism-Based Care
The clinical relevance of these mechanisms lies in their therapeutic implications. Distinct ANOCA/INOCA endotypes are driven by different pathophysiological abnormalities and therefore typically benefit from mechanism-based treatment strategies (2). Vasospastic angina is predominantly mediated by abnormal coronary vasoconstriction and typically responds to vasodilator therapy, particularly calcium-channel blockers and nitrates, whereas structural coronary microvascular dysfunction reflects impaired vasodilatory capacity and increased microvascular resistance, often in the context of cardiometabolic risk, and therefore requires a broader risk factor–modifying and microvascular-directed approach (12,13,42–44).
This concept is supported by interventional evidence demonstrating that a diagnostic strategy incorporating invasive coronary function testing, followed by stratified therapy based on identified endotypes, leads to significant improvements in angina and quality of life (45,46).
Together, these observations establish coronary vascular dysfunction as a central determinant of myocardial ischaemia in ANOCA/INOCA and provide the pathophysiological foundation for a mechanism-based diagnostic and therapeutic paradigm.
5. Non-Invasive Testing: From Ischaemia Detection to Functional Endotyping
Non-invasive imaging plays a central role in the evaluation of ANOCA/INOCA, but its value extends beyond the documentation of inducible ischaemia (1,3). In this setting, a major objective is the quantitative assessment of coronary flow and flow reserve, with the aim of identifying the underlying functional endotype rather than merely demonstrating regional perfusion defects (2,41,47).
5.1. CCTA: An Anatomic Gatekeeper and Plaque Phenotype Tool
CCTA provides a robust non-invasive assessment of coronary anatomy, enabling reliable exclusion of obstructive coronary artery disease and characterisation of plaque burden and morphology (48,49).
Its primary role is to define the presence or absence of epicardial disease and to identify an atherosclerotic substrate that may warrant preventive therapy, even in the absence of flow-limiting stenosis (1,3). Beyond stenosis assessment, CCTA provides incremental value through plaque characterisation, allowing identification of high-risk features such as low-attenuation plaque, positive remodelling, and spotty calcification, which are associated with adverse cardiovascular outcomes and may influence preventive strategies (1,50).
Importantly, a normal or non-obstructive CCTA does not exclude coronary vascular dysfunction. Rather, it increases the likelihood that symptoms arise from microvascular or vasomotor abnormalities, thereby strengthening the indication for downstream functional testing (3). This distinction is critical to avoid misclassification and inappropriate reassurance in symptomatic patients.
In ANOCA/INOCA, the role of CCTA remains adjunctive, as it is fundamentally an anatomical modality and does not directly assess coronary microvascular dysfunction or vasomotor abnormalities. It cannot replace dedicated functional or invasive endotype-oriented testing. Although primarily anatomical, emerging techniques such as CT-derived fractional flow reserve (FFR-CT) provide a non-invasive estimation of lesion-specific haemodynamic significance. However, in ANOCA/INOCA, where diffuse disease and microvascular dysfunction predominate, FFR-CT has limited ability to capture the full spectrum of coronary vascular dysfunction and should be interpreted within a broader physiological framework (8,21).
5.2. PET: Absolute Myocardial Blood Flow and Flow Reserve
PET is the most established non-invasive modality for quantitative assessment of myocardial blood flow (MBF) and MFR (51,52). Unlike relative perfusion imaging techniques, PET enables absolute measurement of MBF (mL/min/g) at rest and during pharmacological stress, allowing detection of both regional and global impairments in coronary perfusion that may be missed by conventional approaches (53,54).
From a physiological perspective, MFR is defined as the ratio of stress to resting MBF and provides an integrated index of the vasodilatory capacity of the entire coronary circulation (55). In clinical practice, MFR <2.0 is generally considered abnormal, with values <1.5 identifying higher-risk phenotypes. Importantly, reduced MFR is not specific for a single mechanism and may result from (22,56,57):
- epicardial flow-limiting disease,
- diffuse atherosclerosis,
- structural or functional coronary microvascular dysfunction,
- or combinations thereof
5.2.1. Diagnostic Patterns and Endotype Inference
The interpretation of PET findings in ANOCA/INOCA relies not only on absolute values but also on flow patterns (52,55):
A global reduction in MFR is suggestive of CMD, although extensive epicardial atherosclerosis or increased resting flow may contribute (51,52)
Regional reductions in stress MBF or MFR, particularly when aligned with a vascular territory, raise suspicion for focal epicardial disease or mixed physiology (58)
Normal relative perfusion with reduced MFR may indicate generalised coronary vascular dysfunction not apparent on semiquantitative imaging alone (37,59).
This pattern-based interpretation is critical, because relative perfusion imaging may appear normal despite balanced or global impairment in coronary flow.
5.2.3. Thresholds and Standardisation Challenges
Although PET-derived myocardial flow reserve is a powerful integrative marker of coronary vascular health, its interpretation requires methodological caution.
Although thresholds vary across tracers and protocols, in clinical practice, an MFR value <2.0 is generally considered abnormal and suggestive of impaired coronary vasodilator capacity. More severe reductions, particularly < 1.5 have been associated with higher-risk phenotypes and a greater likelihood of clinically relevant coronary vascular dysfunction. However, these thresholds should not be interpreted in isolation, because PET flow values are influenced not only by disease severity but also by the technical characteristics of image acquisition and post-processing, including tracer properties, motion correction, reconstruction methods, and the specific kinetic model used for quantification (52,55,60).
A further source of complexity is that MFR is a ratio and can therefore be reduced either because stress MBF is truly impaired or because resting MBF is disproportionately elevated. For this reason, interpretation should always consider resting haemodynamics, particularly heart rate, systolic blood pressure, and rate-pressure product, all of which can increase baseline myocardial blood flow and artifactually lower MFR despite near-normal hyperaemic flow (55,61,62). Age and sex also influence physiological reference ranges: resting flow tends to increase with ageing, and sex-specific differences in MBF and MFR have been consistently documented (63). Accordingly, isolated interpretation of a single global MFR value without clinical and haemodynamic context may lead to overcalling disease in some patients and under-recognising it in others (55).
These considerations explain why recent documents have strongly emphasized standardisation. Contemporary frameworks recommend structured reporting that includes, at minimum, global and regional rest MBF, stress MBF, and MFR, together with technical details relevant to reproducibility and quality control. This is particularly important in ANOCA/INOCA, where clinical interpretation often depends less on the binary presence of a perfusion defect and more on the integration of absolute flow values, regional distribution, haemodynamic context, and the likelihood of specific endotypes such as structural CMD, generalised atherosclerotic disease, or mixed physiology. Standardisation is therefore not merely a technical issue, but a prerequisite for broader clinical adoption and for meaningful comparison across centres (52,60,64).
5.2.4. Prognostic Implications
In ANOCA/INOCA patients, a global reduction in MFR is a hallmark of structural coronary microvascular dysfunction and provides both diagnostic and prognostic information. The prognostic relevance of PET-derived flow impairment is one of its major strengths. Reduced MFR has been consistently associated with adverse cardiovascular outcomes, including major adverse cardiovascular events and all-cause mortality across a broad range of populations. Importantly, this prognostic signal is not confined to patients with obstructive epicardial coronary disease, reinforcing its clinical relevance (51). Even when angiography does not show flow-limiting stenoses, impaired MFR identifies a subgroup with a higher-risk coronary vascular phenotype, consistent with underlying diffuse atherosclerosis, coronary microvascular dysfunction, or both (24,57).
This point is especially relevant in ANOCA/INOCA. In these patients, a reduced MFR should not be viewed as a benign functional curiosity or as an incidental abnormality in the absence of obstructive CAD. Rather, it reflects a pathophysiologically meaningful disturbance of coronary flow regulation, with direct implications for symptom burden, risk stratification, and treatment intensity.
In practical terms, PET-derived evidence of impaired flow reserve strengthens the case for mechanism-based management, more aggressive control of cardiometabolic risk factors, and closer follow-up in patients who might otherwise be falsely reassured by “normal” coronary anatomy (2,3,24).
5.2.5. Limitations
Despite its considerable strengths, PET has important limitations that constrain its widespread implementation. The first is availability: quantitative cardiac PET requires dedicated infrastructure, radiotracer access, specialised software, and local expertise, making it substantially less accessible than stress echocardiography, SPECT, or CMR in many healthcare systems. Cost remains a major barrier, and although radiation exposure is generally acceptable and lower than with many older nuclear protocols, it is not negligible and must still be considered in patient selection, especially when serial assessments are contemplated (51,55).
A second limitation is pathophysiological specificity. PET is excellent for quantifying abnormalities in coronary flow and vasodilator reserve, but it does not directly test vasomotor reactivity. Consequently, PET cannot by itself diagnose coronary spasm, nor can it reliably distinguish epicardial vasospasm from microvascular spasm. In patients in whom vasospastic angina is suspected, a normal or mildly abnormal PET study does not exclude dynamic vasomotor dysfunction, and invasive coronary function testing with vasoreactivity provocation remains necessary when endotype clarification is clinically important. PET should therefore be viewed as a powerful tool for identifying impaired flow regulation, but not as a complete substitute for invasive phenotyping when the diagnostic question specifically concerns coronary spasm (2,52,65).
5.3. Stress CMR: Quantitative Perfusion and Myocardial Phenotyping
5.3.1. Quantitative Perfusion Mapping
Stress CMR has undergone a major methodological transition, evolving from a predominantly qualitative technique to a quantitative modality capable of measuring myocardial blood flow (MBF) and myocardial perfusion reserve (MPR) (54). Recent developments in automated pixel-wise perfusion mapping allow absolute quantification of MBF (mL/min/g) at rest and during pharmacological stress, with improved reproducibility and reduced operator dependence, bridging the gap between non-invasive imaging and invasive physiology. These techniques enable detection of diffuse or balanced perfusion abnormalities that may be missed by visual assessment alone, particularly in patients with coronary microvascular dysfunction or extensive atherosclerosis (66,67). Importantly, quantitative CMR-derived MBF shows good agreement with invasive physiological indices, including coronary flow reserve and microvascular resistance, supporting its role as a non-invasive surrogate of coronary vascular function (68). In centres where PET is not available, quantitative stress CMR represents a powerful alternative for assessing coronary flow impairment, playing a central role in a multimodality, mechanism-based diagnostic strategy.
5.3.2. Integrated Myocardial Characterisation
A major strength of CMR is its ability to combine perfusion assessment with tissue characterisation within a single examination. In addition to perfusion imaging, CMR provides late gadolinium enhancement (LGE), native T1 mapping, and extracellular volume (ECV) quantification. This multiparametric approach allows identification of alternative or concomitant myocardial pathologies, including prior infarction, myocarditis, infiltrative diseases, or cardiomyopathies, thereby reducing diagnostic misclassification in patients presenting with angina and non-obstructive coronary arteries and enabling more tailored management strategies. (69–71).
5.3.3. Diagnostic Performance and Incremental Value
Quantitative stress CMR provides incremental diagnostic value over qualitative perfusion imaging alone. Multicentre studies have demonstrated that absolute MBF and perfusion reserve outperform qualitative interpretation in detecting physiologically significant coronary artery disease, particularly in intermediate lesions and in patients with reduced ejection fraction, highlighting the added value of objective quantification (72–74). In ANOCA/INOCA, this is particularly relevant, as quantitative CMR enables identification of microvascular dysfunction, often characterised by globally reduced perfusion without focal defects, and helps differentiate it from regional abnormalities suggestive of focal epicardial disease or mixed physiology (68,75).
5.3.4. Limitations and Technical Considerations
Despite its strengths, quantitative stress CMR has several limitations. Image quality may be affected by arrhythmias, respiratory motion artefacts, breath-hold limitations, and contrast timing issues, all of which may reduce accuracy. Moreover, variability across vendors, acquisition protocols, and post-processing algorithms remains a significant challenge, limiting inter-centre reproducibility. Absolute MBF thresholds are also less well standardised compared with PET, and interpretation often requires integration with clinical and haemodynamic context (76).
5.4. PET Versus CMR: Complementary Rather than Competitive
PET and CMR should be considered complementary rather than competing modalities within a physiology-based diagnostic pathway. PET provides highly reproducible absolute quantification of myocardial blood flow and robust prognostic stratification, with well-established thresholds (55,56). By contrast, CMR offers integrated myocardial phenotyping, combining quantitative perfusion with tissue characterisation in a single examination (69,70).
In clinical practice, the choice between PET and CMR is often driven by local availability and expertise. However, both modalities enable a quantitative, flow-based assessment of coronary physiology and should be viewed as complementary tools within a mechanism-oriented diagnostic framework. By identifying abnormalities in myocardial blood flow and flow reserve, they represent a critical step toward endotype-based diagnosis and guide subsequent invasive or targeted therapeutic strategies (2,3,52).
The complementary roles of PET and stress CMR in the quantitative assessment of coronary physiology and endotype-oriented diagnosis are illustrated in Figure 1.
5.5. Bridge: from Anatomy to Physiology to Mechanism
Taken together, these considerations highlight the limitations of an anatomy-centred diagnostic approach and support a stepwise transition toward physiology-guided evaluation. While CCTA provides an essential first-line assessment to exclude obstructive coronary artery disease and define atherosclerotic burden, it does not capture the functional integrity of the coronary circulation (1,3). In contrast, non-invasive functional imaging with PET or quantitative stress CMR enables the assessment of myocardial blood flow and flow reserve, thereby identifying patients with impaired coronary vasodilator capacity despite non-obstructive coronary arteries (51,52,54).
However, although these techniques allow detection of flow impairment, they do not fully resolve the underlying mechanism. Reduced flow reserve may reflect different pathophysiological endotypes, including structural coronary microvascular dysfunction, extensive atherosclerosis, or vasomotor abnormalities, which cannot be reliably distinguished on the basis of non-invasive imaging alone (2,3).
In this context, invasive coronary function testing (ICFT) represents the critical next step, enabling comprehensive physiological characterisation of both the epicardial and microvascular compartments. This integrated pathway, from anatomical assessment to quantitative flow evaluation and ultimately to invasive mechanistic testing, reflects a paradigm shift from stenosis-centred to physiology- and endotype-oriented care in patients with ANOCA/INOCA.
6. Invasive Coronary Function testing: ESC-Aligned “Complete the Endotype” Strategy
6.1. Why ICFT Is Increasingly Central: Concept and Rationale
ICFT represents the most comprehensive diagnostic modality for mechanistic characterisation, enabling integrated assessment of epicardial physiology, coronary flow, microvascular resistance, and vasomotor function within a single procedural framework (1,3,7,77). Unlike non-invasive imaging, which identifies the presence of flow impairment, ICFT allows direct interrogation of the underlying pathophysiological mechanisms, thereby enabling definitive endotype classification, identifying otherwise occult abnormalities, including coronary microvascular dysfunction and vasospastic disorders (3,77).
ICFT is based on a structured multiparametric assessment combining indices of coronary flow, microvascular resistance, and vasomotor reactivity. Each component provides complementary information and contributes to endotype classification (2,3,65).
Contemporary evidence and recent guideline updates have progressively repositioned ICFT from a niche investigation to a central component of ANOCA/INOCA evaluation in selected patients, particularly those with persistent symptoms despite initial assessment or with discordant or inconclusive non-invasive findings (78). Structured diagnostic pathways incorporating coronary function testing are increasingly recognised as essential for accurate diagnosis and targeted management of patients with ANOCA (2,3,45).
From a pragmatic perspective, the clinical value of ICFT lies in its ability to move beyond descriptive diagnosis and to establish a mechanism-based framework, in which the identification of a specific endotype is expected to meaningfully influence therapeutic decision-making, in patients with persistent symptoms despite initial evaluation or in cases of discordant or inconclusive non-invasive testing.
Contemporary guidelines and consensus documents increasingly support the use of ICFT in patients with persistent symptoms and non-obstructive coronary arteries, particularly when non-invasive testing is inconclusive or discordant (1,3,42,78).
6.2. Core Invasive Measurements: Epicardial Physiology, CFR, and Microvascular Resistance
A comprehensive invasive assessment requires the integration of multiple physiological domains rather than reliance on a single parameter. Epicardial physiology is typically assessed using FFR or non-hyperaemic pressure indices, with the primary aim of excluding flow-limiting stenoses.
Maximal hyperaemia is generally induced using adenosine, administered either intravenously or intracoronarily, to enable reliable assessment of pressure- and flow-derived indices, including FFR, CFR, and IMR. Adequate hyperaemia is essential for accurate interpretation, as underestimation may lead to misclassification of both epicardial and microvascular physiology (25,29,79,80).
However, the absence of a significant pressure gradient does not imply normal coronary physiology, as myocardial perfusion ultimately depends on flow rather than pressure alone (7,21).
Within this framework, CFR represents a key parameter, reflecting the capacity of the coronary circulation to augment blood flow in response to increased demand. CFR reflects the vasodilatory capacity of the coronary circulation and integrates both epicardial and microvascular contributions. A reduced CFR (<2.0–2.5, depending on methodology) indicates impaired coronary flow augmentation (19,77). Nevertheless, CFR should be interpreted with caution, because it does not distinguish between epicardial stenosis and microvascular dysfunction as it integrates both components and therefore lacks specificity for isolating microvascular dysfunction (26,81). Reduced CFR may reflect non-focal atherosclerosis, microvascular disease, or altered haemodynamic conditions, including elevated resting flow.
To overcome these limitations, indices of microvascular resistance, most commonly the IMR, provide a more direct assessment of the microcirculation by quantifying minimal resistance under hyperaemic conditions. Elevated IMR values are indicative of structural coronary microvascular dysfunction and offer greater specificity compared with flow-based indices alone (79,80). IMR provides a quantitative and relatively flow-independent measure of microvascular resistance, allowing specific assessment of the coronary microcirculation. Elevated IMR (≥25 units) is indicative of structural coronary microvascular dysfunction and has been associated with adverse outcomes (82).
A critical principle in ICFT interpretation is therefore the integrated analysis of epicardial physiology, CFR, and microvascular resistance. CFR may be influenced by haemodynamic variability and non-focal epicardial disease, whereas resistance indices provide a more direct measure of microvascular integrity (21).
Only by combining these parameters can clinicians avoid misclassification and achieve an accurate definition of the underlying endotype.
6.3. Acetylcholine Provocation Testing: Epicardial vs Microvascular Spasm
In addition to flow and resistance assessment, the evaluation of vasomotor function represents a fundamental component of ICFT. Intracoronary acetylcholine (ACh) testing is the reference standard for the diagnosis of coronary vasospastic disorders and is essential for distinguishing between epicardial vasospasm and microvascular spasm (4,83).
Pharmacological provocation testing with acetylcholine enables assessment of endothelial function and identification of epicardial and microvascular vasospasm. Epicardial vasospasm is defined by severe (>90%) transient and reversible coronary constriction associated with symptoms and/or ischaemic electrocardiographic changes, whereas microvascular spasm is diagnosed in the presence of symptoms and ECG changes without angiographic evidence of significant epicardial constriction and may be present in approximately 48 % of patients (4,84).
Contemporary data have demonstrated a favourable safety profile of ACh testing when performed in experienced centres, and a positive response carries prognostic significance, identifying patients at increased risk of adverse cardiovascular events (83). Accurate documentation of symptoms, ECG changes, angiographic findings, and response to nitrates is essential for correct interpretation.
From an implementation perspective, protocol standardisation and operator expertise are critical. Furthermore, ACh testing should be embedded within structured programmes with predefined safety protocols and post-test management pathways (43).
6.4. Integrated ICFT: Completing the Endotype
Based on ICFT findings, patients with ANOCA/INOCA can be stratified into distinct endotypes, each associated with specific pathophysiological mechanisms and therapeutic implications. This classification represents the cornerstone of mechanism-based management. The defining strength of ICFT lies not in individual measurements but in their integration within a unified physiological framework.
By combining epicardial pressure assessment, flow reserve, microvascular resistance, and vasoreactivity testing, ICFT enables classification into clinically actionable endotypes, including structural and functional coronary microvascular dysfunction, epicardial vasospasm, microvascular spasm, and mixed phenotypes (3,78).
Discordant physiological patterns, such as preserved FFR with reduced CFR or normal resistance indices with abnormal vasoreactivity, should be interpreted as expressions of the multidimensional nature of coronary dysfunction rather than inconsistencies (21,26).
Key invasive physiological measurements, their diagnostic interpretation, and principal limitations are summarised in Table 2.
6.5. Evidence of Clinical Utility: CorMicA and Stratified Therapy
The clinical relevance of ICFT is supported by prospective evidence demonstrating that a stratified, mechanism-based approach improves patient outcomes. The CorMicA trial demonstrated that an interventional diagnostic strategy incorporating coronary function testing, followed by stratified therapy based on identified endotypes, resulted in significant improvements in angina symptoms and quality of life compared with standard care (45). Importantly, these benefits were sustained at one-year follow-up, reinforcing the durability of this approach (46).
More recent real-world data further confirm the feasibility, safety, and high diagnostic yield of comprehensive coronary function testing, with a large proportion of ANOCA patients demonstrating identifiable endotypes when systematically evaluated (78).
These findings confirm that coronary vascular dysfunction is not a benign condition but a clinically actionable disease process, in which accurate mechanistic diagnosis directly translates into more effective, individualised treatment strategies. Collectively, these data support a paradigm in which ICFT is not merely a diagnostic adjunct but a central tool for implementing precision medicine in ANOCA/INOCA (3,7).
7. Linking Endotype to Therapy
7.1. From Mechanism to Management: A Paradigm Shift
The management of ANOCA/INOCA has historically been limited by a mismatch between diagnosis and treatment, with therapeutic strategies often applied empirically in the absence of a clearly defined mechanism. The recognition of coronary vascular dysfunction as the principal substrate underlying these syndromes has enabled a transition toward a mechanism-based paradigm, in which treatment is guided by the identification of specific coronary endotypes (14).
Within this framework, the goal of diagnostic evaluation extends beyond confirming the presence of ischaemia to defining the dominant pathophysiological process driving symptoms. This approach enables clinicians to move beyond non-specific antianginal therapy and implement targeted, endotype-oriented strategies aligned with the underlying biology of disease (2,3).
Importantly, contemporary physiological insights highlight that discordance between anatomical and functional indices is not uncommon and reflects complex coronary pathophysiology rather than measurement error, reinforcing the need for integrated assessment of coronary flow and resistance (78).
Invasive physiological assessment, including indices such as coronary flow reserve and index of microcirculatory resistance, provides mechanistic insight into this phenotype and may guide therapeutic decisions (79,80).
7.2. Structural Coronary Microvascular Dysfunction: A Systemic Cardiometabolic Target
Structural CMD is characterised by impaired vasodilatory capacity and increased microvascular resistance, reflecting fixed alterations of the coronary microcirculation (25,79).
Accordingly, therapeutic strategies should primarily target systemic determinants of microvascular dysfunction rather than isolated coronary vasodilation. Aggressive optimisation of cardiovascular risk factors represents the cornerstone of management, including lipid-lowering therapy, blood pressure and glycaemic control, and lifestyle interventions (24,55). Pharmacological strategies such as statins and renin–angiotensin system inhibitors may exert beneficial effects beyond risk reduction, including improvement in endothelial function and microvascular remodelling (55,84,85).
From a symptomatic perspective, beta-blockers are often considered first-line therapy, particularly when elevated heart rate and myocardial oxygen demand contribute to symptom burden. In selected patients, ivabradine may also be considered as a heart rate-lowering strategy, especially when reduction of myocardial oxygen demand and prolongation of diastolic perfusion time are desirable, although evidence in ANOCA/INOCA remains less robust than for broader cardiometabolic optimization (44,84,85).
Ranolazine may be considered in patients with persistent angina despite conventional therapy. By inhibiting the late sodium current, it reduces intracellular calcium overload, improves diastolic relaxation, and may enhance subendocardial perfusion. This mechanism may be particularly relevant in patients with diabetes, in whom metabolic derangements, impaired myocardial relaxation, and microvascular dysfunction frequently coexist, potentially making ranolazine especially attractive in this phenotype, although therapeutic response remains heterogeneous (44,56,84,85).
These therapeutic considerations are supported by physiological studies demonstrating the association between microvascular dysfunction, impaired perfusion during stress, and symptom burden (81). Overall, structural CMD should be conceptualised as a systemic cardiometabolic disease of the microcirculation requiring comprehensive risk factor modification rather than purely antianginal therapy.
7.3. Functional CMD: Targeting Endothelial Dysfunction
Functional (endothelial-dependent) CMD represents a dynamic phenotype characterised by impaired endothelial-mediated vasodilation and abnormal regulation of vascular tone (12,27). Therapeutic strategies should aim to restore endothelial function and improve vasomotor regulation.
Optimisation of cardiovascular risk factors remains essential, with particular emphasis on interventions known to improve endothelial function, including renin-angiotensin system inhibition, statins, and lifestyle modification (2,55,85). However, treatment response is often heterogeneous, reflecting the complex interplay between endothelial dysfunction, microvascular resistance, and vasomotor abnormalities (12,14).
In selected symptomatic patients, antianginal agents such as ranolazine or ivabradine may be considered on an individual basis, particularly when persistent microvascular angina, elevated heart rate, or impaired diastolic perfusion remain clinically relevant, although supportive evidence is less consistent than in obstructive chronic coronary syndromes (44,84,85).
Importantly, functional CMD frequently overlaps with vasospastic disorders, and treatment strategies may require incorporation of vasodilator agents when vasomotor dysfunction is present (3,14).
7.4. Vasospastic Angina and Microvascular Spasm: Suppressing Abnormal Vasoconstriction
Vasospastic angina is characterised by transient coronary vasoconstriction driven by vascular smooth muscle hyperreactivity and endothelial dysfunction. In contrast to CMD, where impaired vasodilation predominates, the primary therapeutic target is suppression of abnormal vasoconstrictive activity (30,32,42,43).
Calcium-channel blockers represent first-line therapy and are highly effective in preventing vasospastic episodes, while long-acting nitrates may be used as adjunctive therapy in patients with persistent symptoms (42,43,85). Avoidance of triggers, including smoking, sympathomimetic agents, and emotional stress, is essential. Non-selective beta-blockers may exacerbate vasospasm and should be used with caution (30,32,42,43).
Microvascular spasm shares similar mechanisms but occurs at the level of the microcirculation and is not detectable on angiography. Its diagnosis relies on invasive vasoreactivity testing, including acetylcholine provocation, which has demonstrated both diagnostic and prognostic value (83).
Therapeutic management is broadly aligned with that of epicardial vasospasm, although treatment response is often more variable and requires individualisation (64,84,85).
7.5. Mixed Endotypes: The Rule Rather than the Exception
Contemporary evidence indicates that mixed endotypes are highly prevalent in ANOCA/INOCA, with overlapping features of CMD and vasospastic disorders observed in a substantial proportion of patients (10,36,41). This overlap reflects the complex interplay between microvascular dysfunction and vasomotor abnormalities and may explain discordant findings across diagnostic modalities (22,23). In clinical practice, combination therapy is frequently required. Calcium-channel blockers may be used to control vasospasm, while concurrent optimisation of cardiometabolic factors and microvascular-directed therapies address underlying CMD (27,55,84).
The identification of mixed endotypes represents a major advantage of comprehensive physiological assessment, enabling tailored therapy and reducing reliance on empiric treatment strategies.
7.6. Evidence Supporting Stratified Therapy
The clinical relevance of endotype-based management is supported by interventional evidence. In the CorMicA trial, a diagnostic strategy incorporating invasive coronary function testing followed by stratified therapy resulted in significant improvements in angina severity and quality of life (45,46). Mechanistic studies further support the link between coronary microvascular dysfunction, impaired stress perfusion, and clinical outcomes, reinforcing the rationale for targeted treatment strategies (81,82). Collectively, these findings support the integration of endotype-guided therapy into routine clinical practice.
The main therapeutic implications of endotype classification, including first-line and adjunctive treatment options, are summarised in Table 3.
7.7. Toward Precision Medicine in ANOCA/INOCA
Taken together, these observations support a paradigm in which ANOCA/INOCA is no longer considered a homogeneous entity but rather a spectrum of pathophysiological processes requiring tailored management. The integration of multimodality imaging and invasive coronary function testing enables identification of clinically actionable endotypes, providing the foundation for precision medicine in coronary vascular dysfunction.
In line with recent national consensus efforts, increasing attention is being directed towards mechanism-based diagnostic pathways in ANOCA/INOCA, incorporating both invasive functional assessment and advanced non-invasive imaging [86].
Future research should focus on refining endotype classification, improving non-invasive surrogates of invasive physiology, and evaluating the impact of mechanism-based therapies on long-term cardiovascular outcomes.
A summary of endotype-specific therapeutic strategies within a mechanism-based framework is provided in Figure 3.
8. Future Prospects and Conclusions
Future progress in the management of ANOCA/INOCA will depend on the integration of quantitative physiology into routine clinical practice and the transition from descriptive diagnosis to mechanism-based care. A key priority is the broader implementation of quantitative perfusion imaging, including both PET and stress CMR, supported by harmonised acquisition protocols and standardised reporting frameworks. Although PET-derived myocardial blood flow and flow reserve currently represent the non-invasive reference standard for coronary physiology, advances in quantitative CMR, including automated pixel-wise perfusion mapping, are expanding access to flow-based assessment and reducing reliance on operator-dependent interpretation (66,75).
Standardisation remains a critical challenge. Variability in thresholds for myocardial blood flow and flow reserve across tracers, imaging platforms, and software pipelines limits comparability and clinical adoption. The development of validated, population-adjusted reference values and consensus reporting standards will be essential to ensure reproducibility and facilitate integration into clinical decision-making. In parallel, the incorporation of artificial intelligence–assisted analysis may improve efficiency, reduce interobserver variability, and enable wider dissemination of quantitative imaging beyond specialised centres.
Equally important is the development of integrated clinical pathways embedding invasive coronary function testing within catheterisation laboratory programmes. Implementation studies aligned with ESC recommendations emphasise the need for dedicated training, standardised protocols, and structured reporting systems to ensure safe and effective delivery of ICFT in routine practice (17).
Such programmes are essential to translate guideline recommendations into real-world care and to reduce the persistent diagnostic gap in ANOCA/INOCA. From a research perspective, the next frontier lies in endotype-guided clinical trials. While current evidence supports the symptomatic benefit of stratified therapy, further studies are needed to evaluate the impact of mechanism-based treatment on long-term outcomes, including major adverse cardiovascular events and healthcare utilisation (24,39,45,46,82).
In addition, prospective studies integrating non-invasive imaging and invasive physiology will be crucial to refine diagnostic algorithms and validate non-invasive surrogates of coronary endotypes. In conclusion, ANOCA/INOCA represents a paradigm in which traditional stenosis-centred approaches are insufficient to explain symptoms, guide therapy, or predict outcomes.
Multimodality evaluation should therefore be reframed as a structured endotyping strategy rather than sequential test accumulation. An ESC-aligned approach integrates anatomical assessment to exclude obstructive coronary artery disease, quantitative perfusion imaging to identify diffuse flow abnormalities, and invasive coronary function testing to define specific endotypes.
Evidence demonstrates that an invasive diagnostic strategy linked to stratified therapy improves symptoms and quality of life, highlighting the clinical value of mechanism-based care. By linking diagnostic findings to targeted treatment, a test-to-endotype-to-therapy framework has the potential to close the longstanding gap between diagnosis and management in patients with ischaemia beyond stenosis.
Author Contributions
Conceptualization, LG.G.; methodology, L.G.G., M.M.; resources, L.G.G., M.M., S.G.; data curation, L.G.G, M.M., S.G., G.A.; writing—original draft preparation, L.G.G., M.M.; writing—review and editing, L.G.G.; visualization, L.G.G., S.G., G.M.F., G.A.; supervision, G.M.F., G.A.; project administration, L.G.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
During the preparation of this manuscript, the authors used AI tools exclusively for grammar/syntax refinement and for assisting in the generation of figures. No AI system was involved in generating the scientific content or drafting the manuscript. The authors have reviewed and edited the output and take full responsibility for the content of this publication. The views and opinions expressed in this manuscript are those of the authors and do not necessarily reflect those of their affiliated institutions.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACh, acetylcholine; ACEi, angiotensin-converting enzyme inhibitors; ANOCA, angina with non-obstructive coronary arteries; ARB, angiotensin receptor blockers; CAD, coronary artery disease; CCB, calcium-channel blockers; CCS, chronic coronary syndromes; CCTA, coronary computed tomography angiography; CFR, coronary flow reserve; CMD, coronary microvascular dysfunction; CMR, cardiovascular magnetic resonance; COVADIS, Coronary Vasomotion Disorders International Study Group; ECG, electrocardiogram; ECV, extracellular volume; ESC, European Society of Cardiology; FFR, fractional flow reserve; FFR-CT, computed tomography-derived fractional flow reserve; ICA, invasive coronary angiography; ICFT, invasive coronary function testing; iFR, instantaneous wave-free ratio; IMR, index of microcirculatory resistance; INOCA, ischaemia with non-obstructive coronary arteries; LGE, late gadolinium enhancement; MBF, myocardial blood flow; MFR, myocardial flow reserve; MPR, myocardial perfusion reserve; NO, nitric oxide; PET, positron emission tomography; VSA, vasospastic angina. |
References
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al.; ESC Scientific Document Group 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J 2024, 45(36), 3415–3537. [Google Scholar] [CrossRef]
- Samuels, B.A.; Shah, S.M.; Widmer, R.J.; Kobayashi, Y.; Miner, S.E.S.; Taqueti, V.R.; Jeremias, A.; Albadri, A.; Blair, J.A.; Kearney, K.E.; et al. Microvascular Network (MVN). Comprehensive Management of ANOCA, Part 1-Definition, Patient Population, and Diagnosis: JACC State-of-the-Art Review. J Am Coll Cardiol. 2023, 82(12), 1245–1263. [Google Scholar] [CrossRef]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.H.E.M.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur Heart J 2020, 41(37), 3504–3520. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Bairey Merz, C.N. Coronary Vasomotion Disorders International Study Group (COVADIS). International standardization of diagnostic criteria for vasospastic angina. Eur Heart J 2017, 38(33), 2565–2568. [Google Scholar] [CrossRef]
- Ong, P.; Camici, P.G.; Beltrame, J.F.; Crea, F.; Shimokawa, H.; Sechtem, U.; Kaski, J.C.; Bairey Merz, C.N. Coronary Vasomotion Disorders International Study Group (COVADIS). International standardization of diagnostic criteria for microvascular angina. Int J Cardiol 2018, 250, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Rahman, H.; Perera, D. Reply: Rethinking False Positive Exercise Electrocardiographic Stress Tests by Assessing Coronary Microvascular Function. J Am Coll Cardiol. 2024, 83(20), e195–6. [Google Scholar] [CrossRef]
- Leone, A.M.; Galante, D.; Viceré, A.; Marrone, A.; Verardi, F.M.; Giuliana, C.; Pollio Benvenuto, C.; Viccaro, V.; Todisco, S.; Erriquez, A.; G.; et al. Functional coronary assessment in angina with intermediate coronary stenosis: the #FullPhysiology approach. Eur Heart J 2025, 46(10), 978–980. [Google Scholar] [CrossRef] [PubMed]
- van de Hoef, T.P.; Lee, J.M.; Boerhout, C.K.M.; de Waard, G.A.; Jung, J.H.; Lee, S.H.; Mejía-Rentería, H.; Hoshino, M.; Echavarria-Pinto, M.; Meuwissen, M.; et al. Combined Assessment of FFR and CFR for Decision Making in Coronary Revascularization: From the Multicenter International ILIAS Registry. JACC Cardiovasc Interv. 2022, 15(10), 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Seitz, A.; Martínez Pereyra, V.; Sechtem, U.; Ong, P. Update on coronary artery spasm 2022 - A narrative review. Int J Cardiol 2022, 359, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Suda, A.; Takahashi, J.; Hao, K.; Kikuchi, Y.; Shindo, T.; Ikeda, S.; Sato, K.; Sugisawa, J.; Matsumoto, Y.; Miyata, S.; et al. Coronary Functional Abnormalities in Patients With Angina and Nonobstructive Coronary Artery Disease. J Am Coll Cardiol. 2019, 74(19), 2350–2360. [Google Scholar] [CrossRef] [PubMed]
- Woudstra, J.; Dimitriu-Leen, A.C.; Crooijmans, C.; Yosofi, B.; Meeder, J.G.; Meuwissen, M.; De Vos, A.M.J.; Paradies, V.; Bijvank, E.G.M.O.; Winkler, P. for NL-CFT. Microvascular vasomotor dysfunction is more prevalent in female versus epicardial vasomotor dysfunction in male ANOCA patients. Int J Cardiol. 2026, 450, 134226. [Google Scholar] [CrossRef]
- Del Buono, M.G.; Montone, R.A.; Camilli, M.; Carbone, S.; Narula, J.; Lavie, C.J.; Niccoli, G.; Crea, F. Coronary Microvascular Dysfunction Across the Spectrum of Cardiovascular Diseases: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021, 78(13), 1352–1371. [Google Scholar] [CrossRef]
- Pijls, N.H.; De Bruyne, B.; Peels, K.; Van Der Voort, P.H.; Bonnier, H.J.; Bartunek, J.; Koolen, J.J.; Koolen, J.J. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. 1996, 334(26), 1703–8. [Google Scholar] [CrossRef]
- Parlati, A.L.M.; Nardi, E.; Sucato, V.; Madaudo, C.; Leo, G.; Rajah, T.; Marzano, F.; Prastaro, M.; Gargiulo, P.; Paolillo, S.; Vadalà, G.; et al. ANOCA, INOCA, MINOCA: The New Frontier of Coronary Syndromes. J Cardiovasc Dev Dis. 2025, 12(2), 64. [Google Scholar] [CrossRef] [PubMed]
- Duncker, D.J.; Koller, A.; Merkus, D.; Canty, J.M. Regulation of coronary blood flow in health and ischemic heart disease. Prog Cardiovasc Dis. 2015, 57(5), 409–22. [Google Scholar] [CrossRef] [PubMed]
- Camici, P.G.; Crea, F. Coronary microvascular dysfunction. N Engl J Med 2007, 356(8), 830–40. [Google Scholar] [CrossRef]
- Gould, K.L. Does coronary flow trump coronary anatomy? JACC Cardiovasc Imaging 2009, 2(8), 1009–23. [Google Scholar] [CrossRef]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; van’ t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009, 360(3), 213–24. [Google Scholar] [CrossRef]
- Gould, K.L.; Kirkeeide, R.L.; Buchi, M. Coronary flow reserve as a physiologic measure of stenosis severity. J Am Coll Cardiol. 1990, 15(2), 459–74. [Google Scholar] [CrossRef]
- Berry, C.; Corcoran, D.; Hennigan, B.; Watkins, S.; Layland, J.; Oldroyd, K.G. Fractional flow reserve-guided management in stable coronary disease and acute myocardial infarction: recent developments. Eur Heart J 2015, 36(45), 3155–64. [Google Scholar] [CrossRef] [PubMed]
- Stegehuis, V.E.; Wijntjens, G.W.; Piek, J.J.; van de Hoef, T.P. Fractional Flow Reserve or Coronary Flow Reserve for the Assessment of Myocardial Perfusion : Implications of FFR as an Imperfect Reference Standard for Myocardial Ischemia. Curr Cardiol Rep. 2018, 20(9), 77. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.P.; Kirkeeide, R.L.; Gould, K.L. Is discordance of coronary flow reserve and fractional flow reserve due to methodology or clinically relevant coronary pathophysiology? JACC Cardiovasc Imaging 2012, 5(2), 193–202. [Google Scholar] [CrossRef]
- Ahn, S.G.; Suh, J.; Hung, O.Y.; Lee, H.S.; Bouchi, Y.H.; Zeng, W.; Gandhi, R.; Eshtehardi, P.; Gogas, B.D.; Samady, H. Discordance Between Fractional Flow Reserve and Coronary Flow Reserve: Insights From Intracoronary Imaging and Physiological Assessment. JACC Cardiovasc Interv. 2017, 10(10), 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Kelshiker, M.A.; Seligman, H.; Howard, J.P.; Rahman, H.; Foley, M.; Nowbar, A.N.; Rajkumar, C.A.; Shun-Shin, M.J.; Ahmad, Y.; Sen, S. Coronary Flow Outcomes Reviewing Committee. Coronary flow reserve and cardiovascular outcomes: a systematic review and meta-analysis. Eur Heart J 2022, 43(16), 1582–1593. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Jung, J.H.; Hwang, D.; Park, J.; Fan, Y.; Na, S.H.; Doh, J.H.; Nam, C.W.; Shin, E.S.; Koo, B.K. Coronary Flow Reserve and Microcirculatory Resistance in Patients With Intermediate Coronary Stenosis. J Am Coll Cardiol. 2016, 67(10), 1158–1169. [Google Scholar] [CrossRef] [PubMed]
- Rahman, H.; Demir, O.M.; Khan, F.; Ryan, M.; Ellis, H.; Mills, M.T.; Chiribiri, A.; Webb, A.; Perera, D. Physiological Stratification of Patients With Angina Due to Coronary Microvascular Dysfunction. J Am Coll Cardiol. 2020, 75(20), 2538–2549. [Google Scholar] [CrossRef]
- Crea, F.; Camici, P.G.; Bairey Merz, C.N. Coronary microvascular dysfunction: an update. Eur Heart J 2014, 35(17), 1101–11. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Cecchi, F.; Olivotto, I.; Camici, P.G. Microvascular Dysfunction in Hypertrophic Cardiomyopathy. J Clin Med. 2022, 11(21), 6560. [Google Scholar] [CrossRef] [PubMed]
- Collet, C.; Yong, A.; Munhoz, D.; Akasaka, T.; Berry, C.; Blair, J.E.A.; Collison, D.; Engstrøm, T.; Escaned, J.; Fearon, W.F.; et al. A Systematic Approach to the Evaluation of the Coronary Microcirculation Using Bolus Thermodilution: CATH CMD. J Soc Cardiovasc Angiogr Interv. 2024, 3(7), 101934. [Google Scholar] [CrossRef]
- Lanza, G.A.; Careri, G.; Crea, F. Mechanisms of coronary artery spasm. Circulation 2011, 124(16), 1774–82. [Google Scholar] [CrossRef]
- Hubert, A.; Seitz, A.; Pereyra, V.M.; Bekeredjian, R.; Sechtem, U.; Ong, P. Coronary Artery Spasm: The Interplay Between Endothelial Dysfunction and Vascular Smooth Muscle Cell Hyperreactivity. Eur Cardiol 2020, 15, e12. [Google Scholar] [CrossRef]
- Picard, F.; Sayah, N.; Spagnoli, V.; Adjedj, J.; Varenne, O. Vasospastic angina: A literature review of current evidence. Arch Cardiovasc Dis 2019, 112(1), 44–55. [Google Scholar] [CrossRef]
- Takahashi, J.; Suda, A.; Nishimiya, K.; Godo, S.; Yasuda, S.; Shimokawa, H. Pathophysiology and Diagnosis of Coronary Functional Abnormalities. Eur Cardiol 2021, 16, e30. [Google Scholar] [CrossRef]
- Masumoto, A.; Mohri, M.; Shimokawa, H.; Urakami, L.; Usui, M.; Takeshita, A. Suppression of coronary artery spasm by the Rho-kinase inhibitor fasudil in patients with vasospastic angina. Circulation 2002, 105(13), 1545–7. [Google Scholar] [CrossRef]
- Matta, A.; Bouisset, F.; Lhermusier, T.; Campelo-Parada, F.; Elbaz, M.; Carrié, D.; Roncalli, J. Coronary Artery Spasm: New Insights. J Interv Cardiol. 2020, 2020, 5894586. [Google Scholar] [CrossRef] [PubMed]
- Mileva, N.; Nagumo, S.; Mizukami, T.; Sonck, J.; Berry, C.; Gallinoro, E.; et al. Prevalence of Coronary Microvascular Disease and Coronary Vasospasm in Patients With Nonobstructive Coronary Artery Disease: Systematic Review and Meta-Analysis. J Am Heart Assoc. 2022, 11(7), e023207. [Google Scholar] [CrossRef] [PubMed]
- Ziadi, M.C.; Dekemp, R.A.; Williams, K.A.; Guo, A.; Chow, B.J.; Renaud, J.M.; Ruddy, T.D.; Sarveswaran, N.; Tee, R.E.; Beanlands, R.S. Impaired myocardial flow reserve on rubidium-82 positron emission tomography imaging predicts adverse outcomes in patients assessed for myocardial ischemia. J Am Coll Cardiol. 2011, 58(7), 740–8. [Google Scholar] [CrossRef] [PubMed]
- Højstrup, S.; Hansen, K.W.; Talleruphuus, U.; Marner, L.; Bjerking, L.; Jakobsen, L.; Christiansen, E.H.; Bouchelouche, K.; Wiinberg, N.; Guldbrandsen, K.; et al. Myocardial Flow Reserve, an Independent Prognostic Marker of All-Cause Mortality Assessed by 82Rb PET Myocardial Perfusion Imaging: A Danish Multicenter Study. Circ Cardiovasc Imaging 2023, 16(8), e015184. [Google Scholar] [CrossRef]
- Boerhout, C.K.M.; de Waard, G.A.; Lee, J.M.; Mejia-Renteria, H.; Lee, S.H.; Jung, J.H.; Hoshino, M.; Echavarria-Pinto, M.; Meuwissen, M.; Matsuo, H.; et al. Prognostic value of structural and functional coronary microvascular dysfunction in patients with non-obstructive coronary artery disease; from the multicentre international ILIAS registry. EuroIntervention 2022, 18(9), 719–728. [Google Scholar] [CrossRef]
- Hwang, D.; Park, S.; Koo, B.K. Reply: Ischemia With Nonobstructive Coronary Artery Disease. JACC Asia;PubMed 2023, 3(4), 687. [Google Scholar] [CrossRef] [PubMed]
- Miner, S.; Mejia-Renteria, H.; Leone, A.M.; Velollari, O.; Sykes, R.; Biscaglia, S.; Esposito, G.; Galante, D.; Oreglia, J.; Ang, D.; et al. Endotypes of angina with non-obstructive coronary arteries: a prospective multicentre study. Eur Heart J. 2026, 47(5), 594–604. [Google Scholar] [CrossRef] [PubMed]
- Hokimoto, S.; Kaikita, K.; Yasuda, S.; Tsujita, K.; Ishihara, M.; Matoba, T.; Matsuzawa, Y.; Mitsutake, Y.; Mitani, Y.; Murohara, T. Japanese Circulation Society and Japanese Association of Cardiovascular Intervention and Therapeutics and Japanese College of Cardiology Joint Working Group. Electronic address: jcsGL@j-circ.or.jp. JCS/CVIT/JCC 2023 guideline focused update on diagnosis and treatment of vasospastic angina (coronary spastic angina) and coronary microvascular dysfunction. J Cardiol. 2023, 82(4), 293–341. [Google Scholar] [CrossRef]
- Jenkins, K.; Pompei, G.; Ganzorig, N.; Brown, S.; Beltrame, J.; Kunadian, V. Vasospastic angina: a review on diagnostic approach and management. Ther Adv Cardiovasc Dis. 2024, 18, 17539447241230400. [Google Scholar] [CrossRef]
- Welch, I.; Case, B. Treatment options for patients with coronary microvascular dysfunction. Future Cardiol 2025, 21(10), 735–8. [Google Scholar] [CrossRef]
- Ford, T.J.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J Am Coll Cardiol. 2018, 72 23 Pt A, 2841–2855. [Google Scholar] [CrossRef]
- Ford, T.J.; Stanley, B.; Sidik, N.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; et al. 1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA). JACC Cardiovasc Interv. 2020, 13(1), 33–45. [Google Scholar] [CrossRef] [PubMed]
- Hansen, B.; Holtzman, J.N.; Juszczynski, C.; Khan, N.; Kaur, G.; Varma, B.; Gulati, M. Ischemia with No Obstructive Arteries (INOCA): A Review of the Prevalence, Diagnosis and Management. Curr Probl Cardiol 2023, 48(1), 101420. [Google Scholar] [CrossRef]
- Kolossváry, M.; Szilveszter, B.; Merkely, B.; Maurovich-Horvat, P. Plaque imaging with CT-a comprehensive review on coronary CT angiography based risk assessment. Cardiovasc Diagn Ther 2017, 7(5), 489–506. [Google Scholar] [CrossRef] [PubMed]
- Nieman, K.; García-García, H.M.; Hideo-Kajita, A.; Collet, C.; Dey, D.; Pugliese, F.; Weissman, G.; Tijssen, J.G.P.; Leipsic, J.; Opolski, M.P. Standards for quantitative assessments by coronary computed tomography angiography (CCTA): An expert consensus document of the society of cardiovascular computed tomography (SCCT). J Cardiovasc Comput Tomogr. 2024, 18(5), 429–443. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, S.; Sarai, M.; Harigaya, H.; Anno, H.; Inoue, K.; Hara, T.; Naruse, H.; Ishii, J.; Hishida, H.; Wong, N.D.; et al. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol. 2009, 54(1), 49–57. [Google Scholar] [CrossRef] [PubMed]
- Murthy, V.L.; Lee, B.C.; Sitek, A.; Naya, M.; Moody, J.; Polavarapu, V.; Ficaro, E.P.; Di Carli, M.F. Comparison and prognostic validation of multiple methods of quantification of myocardial blood flow with 82Rb PET. J Nucl Med. 2014, 55(12), 1952–8. [Google Scholar] [CrossRef]
- Schindler, T.H.; Fearon, W.F.; Pelletier-Galarneau, M.; Ambrosio, G.; Sechtem, U.; Ruddy, T.D.; Patel, K.K.; Bhatt, D.L.; Bateman, T.M.; Gewirtz, H.; et al. Myocardial Perfusion PET for the Detection and Reporting of Coronary Microvascular Dysfunction: A JACC: Cardiovascular Imaging Expert Panel Statement. JACC Cardiovasc Imaging 2023, 16(4), 536–548. [Google Scholar] [CrossRef]
- Vohra, S.; Sakul, S.; Agarwal, V.; Patel, K.K. Quantification of myocardial blood flow using PET: Current status, clinical applications, and future directions. Prog Cardiovasc Dis. 2025, 93, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Kato, Y.; Chehab, O.; Ambale-Venkatesh, B.; Lima, J.A.C. Quantitative myocardial perfusion imaging across PET, SPECT, CMR, and CT. Front Radiol. 2026, 6, 1760241. [Google Scholar] [CrossRef] [PubMed]
- Sciagrà, R.; Lubberink, M.; Hyafil, F.; Saraste, A.; Slart, R.H.J.A.; Agostini, D.; Nappi, C.; Georgoulias, P.; Bucerius, J.; Rischpler, C.; Verberne, H.J.; Cardiovascular Committee of the European Association of Nuclear Medicine (EANM). EANM procedural guidelines for PET/CT quantitative myocardial perfusion imaging. Eur J Nucl Med Mol Imaging 2021, 48(4), 1040–1069. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Di Carli, M.F. Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic Options: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018, 72(21), 2625–41. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, G.; Builoff, V.; Miller, R.J.H.; Lemley, M.; Carvajal-Juarez, I.; Alexanderson, E.; Rosamond, T.L.; Song, N.; Travin, M.I.; Slipczuk, L.; et al. Multicenter Evaluation of Myocardial Flow Reserve as a Prognostic Marker for Mortality in 13N-Ammonia PET Myocardial Perfusion Imaging. Circ Cardiovasc Imaging 2026, e018729. [Google Scholar] [CrossRef]
- Valenta, I.; Quercioli, A.; Schindler, T.H. Diagnostic value of PET-measured longitudinal flow gradient for the identification of coronary artery disease. JACC Cardiovasc Imaging PubMed. 2014, 7(4), 387–96. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Javadi, M.S.; Higuchi, T.; Bravo, P.E.; Chien, D.; Lautamäki, R.; Merrill, J.; Nekolla, S.G.; Bengel, F.M. Impaired global myocardial flow dynamics despite normal left ventricular function and regional perfusion in chronic kidney disease: a quantitative analysis of clinical 82Rb PET/CT studies. J Nucl Med. 2012, 53(6), 887–93. [Google Scholar] [CrossRef] [PubMed]
- deKemp, R.A. Toward improved standardization of PET myocardial blood flow. J Nucl Cardiol. 2023, 30(4), 1297–9. [Google Scholar] [CrossRef] [PubMed]
- Czernin, J.; Müller, P.; Chan, S.; Brunken, R.C.; Porenta, G.; Krivokapich, J.; Chen, K.; Chan, A.; Phelps, M.E.; Schelbert, H.R. Influence of age and hemodynamics on myocardial blood flow and flow reserve. Circulation 1993, 88(1), 62–9. [Google Scholar] [CrossRef]
- Huck, D.M.; Weber, B.N.; Brown, J.M.; Lopez, D.; Hainer, J.; Blankstein, R.; Dorbala, S.; Divakaran, S.; Di Carli, M.F. Prognostic value of myocardial flow reserve vs corrected myocardial flow reserve in patients without obstructive coronary artery disease. J Nucl Cardiol. 2024, 37, 101854. [Google Scholar] [CrossRef] [PubMed]
- Sperry, B.W.; Metzinger, M.P.; Ibrahim, A.O.; Thompson, R.C.; Cho, Y.J.; Jones, P.G.; McGhie, A.I.; Bateman, T.M. Age- and Sex-Specific Myocardial Blood Flow Values in Patients Without Coronary Atherosclerosis on Rb-82 PET Myocardial Perfusion Imaging. Circ Cardiovasc Imaging 2024, 17(7), e016577. [Google Scholar] [CrossRef] [PubMed]
- Packard, R.R.S.; Maddahi, J.; Pelletier-Galarneau, M.; Al-Mallah, M.H.; Coelho, M.; Dorbala, S.; Galt, J.; Hyun, M.; Menon, N.; Miller, E.J.; et al. SNMMI/EANM/ASNC/ACNM Procedure Standard/Practice Guideline for 18F-Flurpiridaz PET Myocardial Perfusion Imaging and Blood Flow Quantitation. J Nucl Med. 2025, 66(10), 1538–1554. [Google Scholar] [CrossRef] [PubMed]
- Bijloo, I.; Woudstra, J.; Aribas, E.; Elias-Smale, S.E.; Vink, C.; Piek, J.J.; Duncker, D.J.; Roeters van Lennep, J.E.; Kavousi, M.; Appelman, Y. Non-invasive and invasive diagnostic modalities for the assessment of coronary vasomotor dysfunction in ANOCA patients. EuroIntervention 2026, 22(5), e283–e291. [Google Scholar] [CrossRef]
- Kotecha, T.; Martinez-Naharro, A.; Boldrini, M.; Knight, D.; Hawkins, P.; Kalra, S.; Patel, D.; Coghlan, G.; Moon, J.; Plein, S.; et al. Automated Pixel-Wise Quantitative Myocardial Perfusion Mapping by CMR to Detect Obstructive Coronary Artery Disease and Coronary Microvascular Dysfunction: Validation Against Invasive Coronary Physiology. JACC Cardiovasc Imaging 2019, 12(10), 1958–1969. [Google Scholar] [CrossRef]
- Hsu, L.Y.; Jacobs, M.; Benovoy, M.; Ta, A.D.; Conn, H.M.; Winkler, S.; Greve, A.M.; Chen, M.Y.; Shanbhag, S.M.; Bandettini, W.P.; et al. Diagnostic Performance of Fully Automated Pixel-Wise Quantitative Myocardial Perfusion Imaging by Cardiovascular Magnetic Resonance. JACC Cardiovasc Imaging 2018, 11(5), 697–707. [Google Scholar] [CrossRef]
- Crawley, R.; Kunze, K.P.; Milidonis, X.; Highton, J.; McElroy, S.; Frey, S.M.; Hoefler, D.; Karamanli, C.; Wong, N.C.K.; Backhaus, S.J.; et al. High-resolution free-breathing automated quantitative myocardial perfusion by cardiovascular magnetic resonance for the detection of functionally significant coronary artery disease. Eur Heart J Cardiovasc Imaging 2024, 25(7), 914–925. [Google Scholar] [CrossRef] [PubMed]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson. Erratum in: J Cardiovasc Magn Reson. 2018 Feb 7;20(1):9. doi: 10.1186/s12968-017-0408-9. 2017, 19(1), 75. [Google Scholar] [CrossRef] [PubMed]
- Dorfman, A.L.; Geva, T.; Samyn, M.M.; Greil, G.; Krishnamurthy, R.; Messroghli, D.; Festa, P.; Secinaro, A.; Soriano, B.; Taylor, A.; et al. SCMR expert consensus statement for cardiovascular magnetic resonance of acquired and non-structural pediatric heart disease. J Cardiovasc Magn Reson. 2022, 24(1), 44. [Google Scholar] [CrossRef]
- Plein, S.; Kozerke, S.; Suerder, D.; Luescher, T.F.; Greenwood, J.P.; Boesiger, P.; Schwitter, J. High spatial resolution myocardial perfusion cardiac magnetic resonance for the detection of coronary artery disease. Eur Heart J 2008, 29(17), 2148–55. [Google Scholar] [CrossRef]
- Nagel, E.; Greenwood, J.P.; McCann, G.P.; Bettencourt, N.; Shah, A.M.; Hussain, S.T.; Perera, D.; Plein, S.; Bucciarelli-Ducci, C.; Paul, M.; et al. MR-INFORM Investigators. Magnetic Resonance Perfusion or Fractional Flow Reserve in Coronary Disease. N Engl J Med. 2019, 380(25), 2418–2428. [Google Scholar] [CrossRef]
- Ge, Y.; Antiochos, P.; Steel, K.; Bingham, S.; Abdullah, S.; Chen, Y.Y.; Mikolich, J.R.; Arai, A.E.; Bandettini, W.P.; Shanbhag, S.M.; et al. Prognostic Value of Stress CMR Perfusion Imaging in Patients With Reduced Left Ventricular Function. JACC Cardiovasc Imaging 2020, 13(10), 2132–2145. [Google Scholar] [CrossRef]
- Wang, S.; Kim, P.; Wang, H.; Ng, M.Y.; Arai, A.E.; Singh, A.; Mushtaq, S.; Sin, T.H.; Tada, Y.; Hillier, E.; et al. Myocardial Blood Flow Quantification Using Stress Cardiac Magnetic Resonance Improves Detection of Coronary Artery Disease. JACC Cardiovasc Imaging 2024, 17(12), 1428–1441. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.; Kang, N.; Chung, J.; Gupta, A.R.; Parwani, P. Evaluation of Ischemia with No Obstructive Coronary Arteries (INOCA) and Contemporary Applications of Cardiac Magnetic Resonance (CMR). Medicina (Kaunas) 2023, 59(9), 1570. [Google Scholar] [CrossRef] [PubMed]
- Chiribiri, A.; Arai, A.E.; DiBella, E.; Hsu, L.Y.; Ishida, M.; Jerosch-Herold, M.; Kozerke, S.; Milidonis, X.; Nezafat, R.; Plein, S.; et al. Society for cardiovascular magnetic resonance expert consensus statement on quantitative myocardial perfusion cardiovascular magnetic resonance imaging. J Cardiovasc Magn Reson. 2025, 27(2), 101940. [Google Scholar] [CrossRef]
- Ford, T.J.; Yii, E.; Sidik, N.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; et al. Ischemia and No Obstructive Coronary Artery Disease: Prevalence and Correlates of Coronary Vasomotion Disorders. Circ Cardiovasc Interv. 2019, 12(12), e008126. [Google Scholar] [CrossRef]
- Namba, H.F.; Boerhout, C.K.M.; Damman, P.; Kunadian, V.; Escaned, J.; Ong, P.; Perera, D.; Berry, C.; van de Hoef, T.P.; Piek, J.J. Invasive coronary function testing in clinical practice: Implementing the 2024 ESC guidelines on chronic coronary syndromes. Int J Cardiol 2025, 430, 133176. [Google Scholar] [CrossRef] [PubMed]
- Fearon, W.F.; Kobayashi, Y. Invasive Assessment of the Coronary Microvasculature: The Index of Microcirculatory Resistance. Circ Cardiovasc Interv 2017, 10(12), e005361. [Google Scholar] [CrossRef]
- Gallinoro, E.; Bertolone, D.T.; Fernandez-Peregrina, E.; Paolisso, P.; Bermpeis, K.; Esposito, G.; Gomez-Lopez, A.; Candreva, A.; Mileva, N.; Belmonte, M.; et al. Reproducibility of bolus versus continuous thermodilution for assessment of coronary microvascular function in patients with ANOCA. EuroIntervention 2023, 19(2), e155–e166. [Google Scholar] [CrossRef]
- Rahman, H.; Ryan, M.; Lumley, M.; Modi, B.; McConkey, H.; Ellis, H.; Scannell, C.; Clapp, B.; Marber, M.; Webb, A.; et al. Coronary Microvascular Dysfunction Is Associated With Myocardial Ischemia and Abnormal Coronary Perfusion During Exercise. Circulation 2019, 140(22), 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Li, X.; Feng, W.; Zhou, H.; Peng, W.; Wang, X. Diagnostic and prognostic value of angiography-derived index of microvascular resistance: a systematic review and meta-analysis. Front Cardiovasc Med. 2024, 11, 1360648. [Google Scholar] [CrossRef] [PubMed]
- Montone, R.A.; Rinaldi, R.; Del Buono, M.G.; Gurgoglione, F.; La Vecchia, G.; Russo, M.; Caffè, A.; Burzotta, F.; Leone, A.M.; Romagnoli, E.; et al. Safety and prognostic relevance of acetylcholine testing in patients with stable myocardial ischaemia or myocardial infarction and non-obstructive coronary arteries. EuroIntervention 2022, 18(8), e666–e676. [Google Scholar] [CrossRef] [PubMed]
- Ashokprabhu, N.D.; Quesada, O.; Alvarez, Y.R.; Henry, T.D. INOCA/ANOCA: Mechanisms and novel treatments. Am Heart J Plus 2023, 30, 100302. [Google Scholar] [CrossRef]
- Montone, R.A.; Rinaldi, R.; Niccoli, G.; Andò, G.; Gragnano, F.; Piccolo, R.; Pelliccia, F.; Moscarella, E.; Zimarino, M.; Fabris, E.; et al. Interventional Cardiology Working Group of the Italian Society of Cardiology. Optimizing Management of Stable Angina: A Patient-Centered Approach Integrating Revascularization, Medical Therapy, and Lifestyle Interventions. J Am Coll Cardiol. 2024, 84(8), 744–760. [Google Scholar] [CrossRef] [PubMed]
- Masiero, G.; Aurigemma, C.; Biscaglia, S.; Bruno, F.; Burzotta, F.; Campo, G.; Cangemi, S.; Chieffo, A.; Di Mario, C.; Esposito, G.; et al. Implementazione delle nuove raccomandazioni sull’impiego dei test funzionali coronarici e dell’imaging intravascolare nell’angioplastica coronarica per le sindromi coronariche croniche: documento di consenso GISE/ANMCO/SIC [GISE/ANMCO/SIC Consensus document on the implementation of the new recommendations for the use of coronary functional testing and intravascular imaging in coronary angioplasty for chronic coronary syndromes]. G Ital Cardiol (Rome);Italian 2025, 26(12), 941–953. [Google Scholar] [CrossRef]
Figure 1.
Complementary roles of PET and stress CMR in ANOCA/INOCA. Schematic comparison of PET and stress CMR in the non-invasive evaluation of coronary vascular dysfunction. PET provides highly reproducible absolute quantification of MBF and MFR, with robust prognostic value and established thresholds for risk stratification. In contrast, stress CMR enables integrated myocardial phenotyping by combining quantitative perfusion assessment with tissue characterisation, including LGE and parametric mapping. Rather than competing modalities, PET and CMR should be considered complementary tools within a mechanism-based diagnostic pathway, providing quantitative assessment of coronary flow and supporting endotype-oriented clinical decision-making. Abbreviations: PET, positron emission tomography; CMR, cardiovascular magnetic resonance; ANOCA, angina with non-obstructive coronary arteries; INOCA, ischaemia with non-obstructive coronary arteries; MBF, myocardial blood flow; MFR, myocardial flow reserve; LGE, late gadolinium enhancement.
Figure 1.
Complementary roles of PET and stress CMR in ANOCA/INOCA. Schematic comparison of PET and stress CMR in the non-invasive evaluation of coronary vascular dysfunction. PET provides highly reproducible absolute quantification of MBF and MFR, with robust prognostic value and established thresholds for risk stratification. In contrast, stress CMR enables integrated myocardial phenotyping by combining quantitative perfusion assessment with tissue characterisation, including LGE and parametric mapping. Rather than competing modalities, PET and CMR should be considered complementary tools within a mechanism-based diagnostic pathway, providing quantitative assessment of coronary flow and supporting endotype-oriented clinical decision-making. Abbreviations: PET, positron emission tomography; CMR, cardiovascular magnetic resonance; ANOCA, angina with non-obstructive coronary arteries; INOCA, ischaemia with non-obstructive coronary arteries; MBF, myocardial blood flow; MFR, myocardial flow reserve; LGE, late gadolinium enhancement.

Figure 2.
Mechanism-based diagnostic pathway in ANOCA/INOCA. Proposed stepwise diagnostic framework integrating anatomical imaging, quantitative perfusion assessment, and invasive coronary function testing in patients with angina and non-obstructive coronary arteries. The pathway illustrates the transition from exclusion of obstructive epicardial disease to identification of impaired coronary flow and final endotype definition, linking diagnostic findings to targeted therapy within a precision medicine approach.
Figure 2.
Mechanism-based diagnostic pathway in ANOCA/INOCA. Proposed stepwise diagnostic framework integrating anatomical imaging, quantitative perfusion assessment, and invasive coronary function testing in patients with angina and non-obstructive coronary arteries. The pathway illustrates the transition from exclusion of obstructive epicardial disease to identification of impaired coronary flow and final endotype definition, linking diagnostic findings to targeted therapy within a precision medicine approach.

Figure 3.
Endotype-based therapeutic approach in ANOCA/INOCA. Schematic representation of the principal ANOCA/INOCA endotypes and their corresponding mechanism-based treatment strategies. Structural and functional coronary microvascular dysfunction, epicardial vasospasm, microvascular spasm, and mixed phenotypes are linked to targeted therapies, emphasising the transition from empirical treatment to precision, endotype-driven management. Abbreviations: ACEi, angiotensin-converting enzyme inhibitors; ANOCA, angina with non-obstructive coronary arteries; ARB, angiotensin receptor blockers; CCB, calcium-channel blockers; CMD, coronary microvascular dysfunction; INOCA, ischaemia with non-obstructive coronary arteries;
Figure 3.
Endotype-based therapeutic approach in ANOCA/INOCA. Schematic representation of the principal ANOCA/INOCA endotypes and their corresponding mechanism-based treatment strategies. Structural and functional coronary microvascular dysfunction, epicardial vasospasm, microvascular spasm, and mixed phenotypes are linked to targeted therapies, emphasising the transition from empirical treatment to precision, endotype-driven management. Abbreviations: ACEi, angiotensin-converting enzyme inhibitors; ANOCA, angina with non-obstructive coronary arteries; ARB, angiotensin receptor blockers; CCB, calcium-channel blockers; CMD, coronary microvascular dysfunction; INOCA, ischaemia with non-obstructive coronary arteries;


Table 1.
Endotype-driven diagnostic framework in ANOCA/INOCA. Summary of the main diagnostic modalities used in the evaluation of patients with ANOCA/INOCA, including their key outputs, associated endotype signals, clinical role, limitations, and therapeutic implications. The table highlights the complementary contribution of anatomical imaging, quantitative perfusion assessment, and invasive coronary function testing within a mechanism-based diagnostic strategy.
Table 1.
Endotype-driven diagnostic framework in ANOCA/INOCA. Summary of the main diagnostic modalities used in the evaluation of patients with ANOCA/INOCA, including their key outputs, associated endotype signals, clinical role, limitations, and therapeutic implications. The table highlights the complementary contribution of anatomical imaging, quantitative perfusion assessment, and invasive coronary function testing within a mechanism-based diagnostic strategy.
| Modality/Test | Key outputs | Endotype signal | Clinical role | Limitations | Therapeutic implications |
| CCTA | Stenosis severity; plaque burden and phenotype | Non-obstructive plaque → atherosclerotic substrate; normal CCTA does not exclude CMD or vasospasm | Anatomical gatekeeper; selection for functional testing | Heavy calcification; motion artefacts | Intensify preventive therapy; proceed to functional testing if symptoms persist |
| Stress PET (MBF/MFR) | Rest and stress MBF; global and regional MFR | Global reduction in MFR/MBF → structural CMD or diffuse coronary dysfunction | First-/second-line functional assessment | Haemodynamic variability; tracer and software differences; limited detection of spasm | Supports CMD diagnosis; risk stratification; guides cardiometabolic optimisation |
| Stress CMR (quantitative) | Stress MBF/MPR; regional perfusion; LGE; T1/ECV | Extesnvie perfusion impairment → CMD; tissue abnormalities may suggest alternative myocardial pathology” | Alternative to PET; integrated “one-stop” evaluation | Arrhythmias; motion artefacts; variability in analysis pipelines | Guides CMD management; avoids misclassification; identifies alternative myocardial pathology |
| ICA + FFR/iFR | Epicardial physiology | Flow-limiting epicardial disease | Assessment of obstructive CAD prior to ICFT; excludes focal flow-limiting epicardial disease | Does not directly assess coronary blood flow or microvascular dysfunction; non-focal atherosclerotic disease may affect interpretation | Guides revascularisation decisions; a normal FFR/iFR does not exclude coronary vascular dysfunction |
| CFR (wire-based) | Coronary flow reserve | Reduced CFR suggests CMD but lacks specificity | Component of ICFT | Influenced by haemodynamics and epicardial disease | Requires integration with resistance indices and vasoreactivity testing |
| Microvascular resistance (IMR) | Microvascular resistance index | Elevated resistance → structural CMD | Core component of microvascular assessment | Technique-dependent | Supports CMD-targeted therapy; avoids inappropriate vasodilator-only strategies |
| Acetylcholine provocation | Vasomotor response; symptoms; ECG changes | Epicardial vs microvascular spasm; mixed phenotypes | Diagnosis of vasospastic disorders | Requires expertise; protocol variability | Calcium-channel blockers first-line; nitrates and trigger modification |
| Integrated ICFT | Comprehensive physiological assessment | CMD, vasospasm, or mixed endotypes | ESC-recommended in persistent symptoms | Requires dedicated infrastructure | Enables stratified therapy; improves symptoms and quality of life |
Abbreviations: ANOCA, angina and non-obstructive coronary arteries; ACh, acetylcholine; CAD, coronary artery disease; CCTA, coronary computed tomography angiography; CFR, coronary flow reserve; CMD, coronary microvascular dysfunction; CMR, cardiovascular magnetic resonance; ECV, extracellular volume; FFR, fractional flow reserve; ICA, invasive coronary angiography; ICFT, invasive coronary function testing; iFR, Instantaneous Wave-Free Ratio; INOCA, ischemia and non-obstructive coronary arteries; IMR, index of microcirculatory resistance; LGE, late gadolinium enhancement; MBF, myocardial blood flow; MFR, myocardial flow reserve; PET, positron emission tomography.
Table 2.
Core invasive coronary function testing parameters and endotype classification. Overview of the principal ANOCA/INOCA endotypes as defined by invasive coronary function testing, including underlying pathophysiology, characteristic physiological findings, clinical implications, and corresponding treatment strategies. The table illustrates how integration of coronary flow reserve, microvascular resistance indices, and vasoreactivity testing enables mechanism-based classification. Cut-off values may vary according to methodology and haemodynamic conditions and should always be interpreted within the clinical context.
Table 2.
Core invasive coronary function testing parameters and endotype classification. Overview of the principal ANOCA/INOCA endotypes as defined by invasive coronary function testing, including underlying pathophysiology, characteristic physiological findings, clinical implications, and corresponding treatment strategies. The table illustrates how integration of coronary flow reserve, microvascular resistance indices, and vasoreactivity testing enables mechanism-based classification. Cut-off values may vary according to methodology and haemodynamic conditions and should always be interpreted within the clinical context.
| Endotype | Pathophysiology | ICFT findings (with cut-offs) (FFR ≤0.80 indicates haemodynamically significant epicardial disease) | Clinical implication | Treatment approach |
| Structural CMD | Microvascular remodelling, increased minimal resistance | ↓ CFR (<2.0–2.5 depending on methodology) + ↑ IMR (≥25) | Impaired vasodilatory capacity | Risk factor optimisation; ACEi/ARB; statins |
| Functional CMD | Endothelial dysfunction, impaired vasomotor regulation | ↓ CFR (<2.0–2.5 depending on methodology) + normal IMR (<25); ± abnormal vasoreactivity | Dynamic microvascular dysfunction | Endothelial-targeted therapy; antianginal agents |
| Epicardial vasospasm | Vascular smooth muscle hyperreactivity | ACh-induced epicardial constriction ≥90% + symptoms and/or ECG changes | Variant angina phenotype | Calcium-channel blockers; nitrates |
| Microvascular spasm | Microvascular hyperreactivity | ACh-induced symptoms + ECG changes without epicardial constriction (<90%) | INOCA with vasomotor dysfunction | Calcium-channel blockers; tailored antianginal therapy |
| Mixed endotype | Overlapping CMD and vasospastic mechanisms | Combination of ↓ CFR and/or ↑ IMR with abnormal ACh response | Complex and heterogeneous phenotype | Combination therapy targeting CMD and vasospasm |
Abbreviations: ACh, acetylcholine; ACEi, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; CFR, coronary flow reserve; CMD, coronary microvascular dysfunction; ICFT, invasive coronary function testing; IMR, index of microcirculatory resistance.
Table 3.
Endotype-specific therapeutic strategies in ANOCA/INOCA. Overview of mechanism-based therapeutic approaches according to coronary endotype, including key diagnostic features, underlying pathophysiology, first-line treatments, adjunctive therapies, and clinical considerations. The table reflects a test-to-endotype-to-therapy paradigm, emphasising the importance of aligning treatment with the dominant pathophysiological mechanism. Therapeutic responses may vary, particularly in overlapping or mixed endotypes, requiring individualised management strategies.
Table 3.
Endotype-specific therapeutic strategies in ANOCA/INOCA. Overview of mechanism-based therapeutic approaches according to coronary endotype, including key diagnostic features, underlying pathophysiology, first-line treatments, adjunctive therapies, and clinical considerations. The table reflects a test-to-endotype-to-therapy paradigm, emphasising the importance of aligning treatment with the dominant pathophysiological mechanism. Therapeutic responses may vary, particularly in overlapping or mixed endotypes, requiring individualised management strategies.
| Endotype | Key diagnostic features | Pathophysiology | Mechanistic target | First-line therapy | Adjunctive therapy | Clinical pearls / pitfalls |
| Structural CMD | ↓ MFR (PET/CMR); ↓ CFR + ↑ IMR | Impaired vasodilatory capacity; microvascular remodelling; increased minimal resistance | Improve microvascular vasodilation and reduce resistance | Risk factor control; beta-blockers | ACEi/ARB; statins; ranolazine (selected patients) | Systemic cardiometabolic disease; prioritise risk factor optimisation over escalation of antianginal therapy; avoid reassurance based on “normal angiogram” |
| Functional / endothelial CMD | ↓ CFR with normal or mildly ↑ IMR; ± abnormal vasoreactivity | Endothelial dysfunction; impaired NO-mediated vasodilation; altered vascular tone regulation | Restore endothelial function and nitric oxide bioavailability | Risk factor control | ACEi/ARB; statins; lifestyle intervention; ranolazine or ivabradine (selected patients) | Heterogeneous phenotype; frequent overlap with vasospasm; variable therapeutic response; reassess if symptoms persist |
| Epicardial vasospasm (VSA) | ACh-induced epicardial constriction ≥90% + symptoms and/or ECG changes | Vascular smooth muscle hyperreactivity; endothelial dysfunction | Suppress abnormal vasoconstriction and smooth muscle hyperreactivity | Calcium-channel blockers | Nitrates; nicorandil (selected cases) | Avoid triggers (smoking, stress, sympathomimetics); avoid non-selective beta-blockers; high response to vasodilator therapy |
| Microvascular spasm | ACh-induced symptoms and ECG changes without epicardial constriction (<90%) | Microvascular hyperreactivity; abnormal vasomotor regulation | Reduce microvascular vasoconstriction | Calcium-channel blockers | Nitrates; tailored antianginal therapy | Diagnosis requires invasive testing; often underdiagnosed; symptoms may be disproportionate to imaging findings; response less predictable |
| Mixed endotypes | Combination of ↓ CFR and/or ↑ IMR with abnormal ACh response | Overlapping CMD and vasospastic mechanisms | Combined modulation of vasodilation and vasoconstriction pathways | Combination therapy (CCB + CMD-directed therapy) | Individualised strategy | Most common phenotype; avoid single-mechanism treatment; requires integrated interpretation of physiology |
| Non-obstructive atherosclerosis (modifier) | Plaque on CCTA/ICA without flow-limiting stenosis | Diffuse atherosclerotic burden; endothelial dysfunction; inflammatory activation | Stabilise plaque and reduce atherogenic and inflammatory burden | Lipid-lowering therapy; risk factor control | Antiplatelet therapy (selected cases) | Major prognostic driver even without stenosis; do not undertreat; integrate with CMD management |
Abbreviations: ACEi, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; ACh, acetylcholine; CCB, calcium-channel blockers; CFR, coronary flow reserve; CMD, coronary microvascular dysfunction; CCTA, coronary computed tomography angiography; ICA, invasive coronary angiography; IMR, index of microcirculatory resistance; MFR, myocardial flow reserve; NO, nitric oxide; PET, positron emission tomography; CMR, cardiovascular magnetic resonance; VSA, vasospastic angina.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



