Submitted:
14 April 2026
Posted:
14 April 2026
You are already at the latest version
Abstract
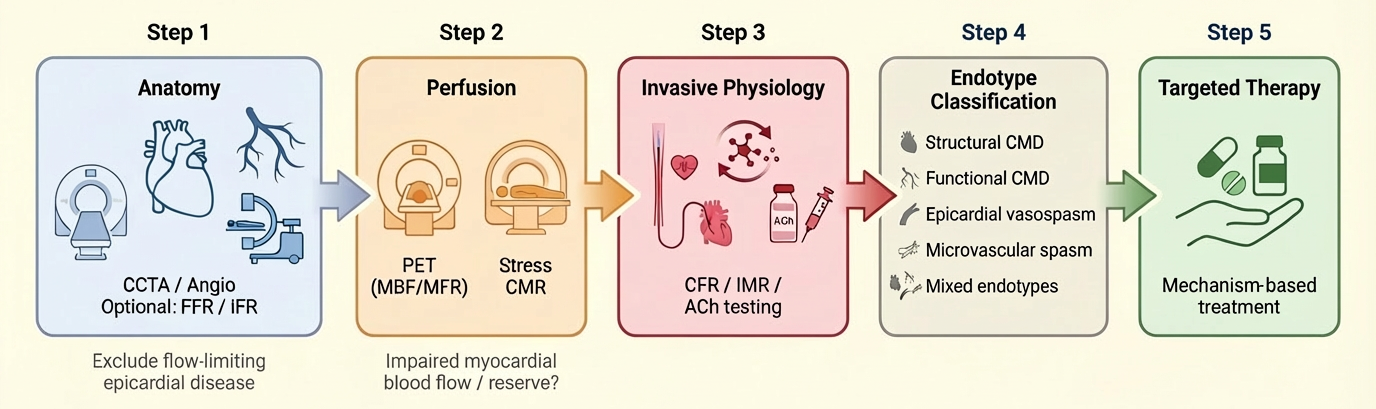
Angina or objective myocardial ischaemia in the absence of obstructive coronary artery disease, referred to as ANOCA/INOCA, represents a prevalent and clinically significant condition associated with persistent symptoms, impaired quality of life, and increased healthcare utilisation. Contemporary evidence has reframed these syndromes as manifestations of coronary vascular dysfunction, encompassing structural and functional coronary microvascular dysfunction, epicardial vasospasm, microvascular spasm, and mixed phenotypes. In this context, multimodality imaging should not be conceptualised as sequential test accumulation, but rather as a structured, mechanism-based diagnostic strategy aimed at defining the underlying coronary endotype. The 2024 ESC Guidelines for chronic coronary syndromes endorse dedicated diagnostic pathways beyond a stenosis-centred paradigm and support the use of invasive coronary function testing (ICFT) in selected patients with persistent symptoms or inconclusive non-invasive findings. An integrated approach combining anatomical assessment (coronary computed tomography angiography or invasive angiography ± pressure-based indices), quantitative perfusion imaging (positron emission tomography or stress cardiovascular magnetic resonance), and ICFT (including coronary flow reserve, microvascular resistance indices, and acetylcholine provocation testing) enables comprehensive characterisation of coronary physiology and vasomotor function. This review proposes a pragmatic framework linking diagnostic findings to targeted therapy through a test-to-endotype-to-therapy paradigm. We summarise the strengths and limitations of each modality, discuss implementation challenges, and highlight the clinical relevance of endotype-driven management. By shifting from a stenosis-centred to a physiology- and mechanism-based approach, this strategy has the potential to close the longstanding gap between diagnosis and treatment in patients with ischaemia beyond obstructive coronary disease.
Keywords:
ANOCA
; INOCA
; coronary microvascular dysfunction
; coronary vasospasm
; myocardial blood flow
; coronary flow reserve
; invasive coronary function testing
; multimodality imaging
; PET
; CMR
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



