Submitted:
10 April 2026
Posted:
13 April 2026
You are already at the latest version
Abstract
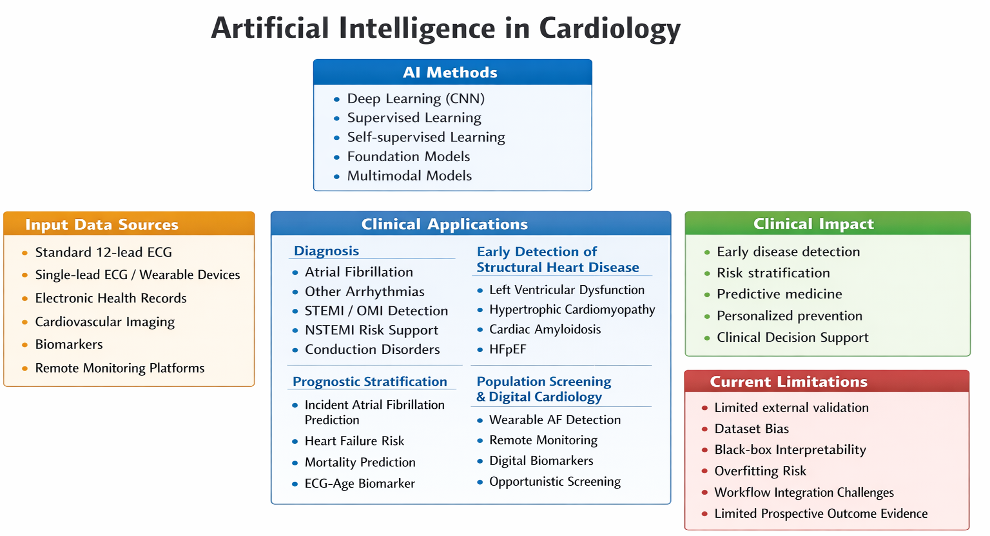
In recent years, Artificial Intelligence (AI) applied to the electrocardiogram (ECG) has shown increasing potential in improving diagnosis, prognostic stratification, and cardiovascular screening through the identification of electrophysiological patterns not detectable with conventional interpretation. This narrative review, incorporating elements of a scoping review, summarizes the main available evidence on the use of AI-ECG across the entire continuum of cardiovascular disease, including arrhythmia detection, early identification of structural heart disease, decision support in acute coronary syndromes, prediction of clinical outcomes, and applications in population screening using wearable devices.
Deep learning models applied to both the standard 12-lead ECG and simplified re-cordings have demonstrated high diagnostic performance in identifying atrial fibrillation (AF), left ventricle (LV) dysfunction, hypertrophic cardiomyopathy (HCM), cardiac amyloidosis, and heart failure with preserved ejection fraction (HFpEF), as well as a potential role in cardiovascular risk stratification and in the identification of systemic digital biomarkers.
Despite these promising results, the clinical adoption of AI-ECG is still limited by the need for prospective multicenter validation and by challenges related to model interpretability and their integration into clinical workflows. Overall, AI-ECG represents an emerging diagnostic platform with potential applications in predictive, preventive, and personalized cardiology.
Keywords:
artificial intelligence
; electrocardiography
; deep learning
; cardiovascular disease
; arrhythmia detection
; digital biomarkers
; heart failure
; cardiac screening
; wearable devices
; precision cardiology
1. Introduction
In recent years, AI has assumed an increasingly important role in cardiovascular medicine, owing to its ability to analyze large volumes of clinical data and biological signals and to identify complex patterns that cannot be recognized using traditional interpretation methods [1]. In cardiology, this evolution has been facilitated by the progressive digitalization of instrumental examinations and by the availability of large-scale datasets, which have enabled the development of predictive models applicable to both diagnosis and cardiovascular risk stratification [1].
Among the various sources of cardiovascular data, the ECG represents one of the most suitable tools for the application of machine learning algorithms, as it is a non invasive, low-cost, universally available test that can be easily stored in digital format. Traditionally, the ECG has been interpreted through visual analysis of well-defined morphological features, such as intervals, amplitudes, and ST-segment deviations; however, the introduction of deep learning models has enabled direct analysis of the complete digital electrocardiographic signal—that is, the sequence of voltages recorded over time—allowing the identification of latent information not accessible through conventional interpretation [2,3].
In particular, convolutional neural networks (CNN), a class of artificial neural networks designed to automatically recognize complex patterns within signals and images, have demonstrated high performance in ECG analysis, making it possible not only to automate arrhythmia classification but also to identify subclinical structural cardiac conditions, such as LV dysfunction, HCM, and cardiac amyloidosis [4,5].
At the same time, AI applied to the ECG has shown increasing potential in prognostic stratification, enabling the identification of patients at increased risk of AF, heart failure, and cardiovascular mortality even in the presence of apparently normal tracings. These observations suggest that the ECG may be considered not only an electrical diagnostic tool but also an integrated digital biomarker of cardiovascular health status [6].
More recently, the evolution toward AI models capable of integrating electrocardiographic data with cardiovascular imaging, biomarkers, and longitudinal information derived from electronic health records has opened new perspectives toward increasingly predictive and personalized cardiovascular medicine [7]. In this context, the emergence of systems based on generative AI and large language models could facilitate integrated clinical data interpretation and improve the efficiency of healthcare workflows, although their application still requires rigorous prospective validation and appropriate clinical governance frameworks [7].
In light of these considerations, the present review critically summarizes the main available evidence on the use of AI applied to the ECG across the entire continuum of cardiovascular disease, including arrhythmia diagnosis, early identification of structural heart disease, decision support in acute coronary syndromes, prognostic stratification, and applications in population screening using wearable devices.
2. Materials and Methods
A structured narrative literature review was conducted, incorporating methodological elements consistent with a scoping review, with the aim of analyzing the main clinical applications of AI applied to the ECG across the entire cardiovascular care continuum, from early diagnosis to prognostic stratification and population screening.
The literature search was performed by reviewing original studies, systematic reviews, scientific statements, and narrative review articles published in recent years in the field of cardiovascular AI, with particular attention to AI-ECG applications in the diagnosis of arrhythmias, structural cardiomyopathies, acute coronary syndromes, and the prediction of clinical outcomes.
A total of 48 articles considered relevant to contemporary cardiology practice were included, comprising large-scale retrospective studies, multicenter analyses, prospective trials, meta-analyses, and position papers from international scientific societies. Given the heterogeneity of the available studies—characterized by differences in analyzed populations, algorithmic architectures, and performance metrics—a quantitative synthesis of the results was not performed; instead, the data were analyzed using a descriptive and thematic approach, consistent with the exploratory objective of the review.
3. Fundamentals of AI Applied to the ECG
AI applied to the ECG is primarily based on machine learning techniques, a set of computational methods that allow algorithms to learn relationships between data and clinical conditions from previously observed examples, without being explicitly programmed according to predefined rules [8]. In the context of electrocardiographic analysis, these models are trained using large repositories of digital tracings associated with known diagnoses, enabling the automatic identification of electrophysiological features correlated with specific cardiovascular diseases [4].
Among the various available methodologies, deep learning currently represents the most widely used approach in ECG analysis [3]. This term refers to a subclass of machine learning based on multilayer artificial neural networks capable of directly analyzing the original digital electrocardiographic signal—that is, the numerical sequence of voltages recorded over time—without the need for manual selection of variables to be analyzed. This approach enables the identification of complex and nonlinear patterns that are difficult to detect through conventional interpretation of the ECG tracing [3].
In particular, CNNs represent one of the most commonly used architectures for automated ECG analysis. These models are designed to recognize recurring structures within signals or images through the analysis of small portions of the signal itself, allowing the automatic identification of subtle morphological features distributed throughout the entire electrocardiographic tracing [9].
From a methodological perspective, algorithms applied to ECG analysis can be classified into supervised and self-supervised models [10]. In supervised models, the algorithm learns to recognize diseases using ECGs already labeled by experts, establishing a direct relationship between signal and diagnosis; however, this approach requires large manually annotated datasets, which are often difficult to obtain and not always homogeneous across different clinical settings. In self-supervised models, by contrast, the algorithm is initially trained on unlabeled ECGs, autonomously learning the morphological and statistical characteristics of the signal through techniques such as masked-lead modeling, in which some leads are temporarily hidden and reconstructed by the model, and contrastive learning, which enables the recognition of similarities and differences between segments from different tracings. This approach allows the extraction of signal representations that can be reused for multiple diagnostic applications even when annotated data are limited [10].
The performance of AI algorithms is generally evaluated using statistical indicators such as sensitivity, specificity, and the area under the curve (AUC), a summary index that measures the model’s ability to correctly distinguish between patients with and without the condition under investigation [4]. In numerous recent studies, deep learning–based models applied to ECG analysis have demonstrated diagnostic accuracy values comparable to or higher than those obtained with traditional approaches, suggesting an increasingly important role for AI as a decision-support tool in cardiology practice [4].
More recently, the evolution toward multimodal models capable of integrating electrocardiographic data with cardiovascular imaging, biomarkers, and longitudinal information derived from electronic health records has further expanded the potential applications of AI in cardiology. These approaches make it possible to develop predictive models that more closely reflect the complexity of real-world clinical reasoning and represent one of the main future directions in cardiovascular AI development [7].
4. Applications of AI-ECG in Arrhythmia Diagnosis
Automated identification of arrhythmias represents one of the most established applications of AI applied to the ECG and constitutes the first area in which these algorithms demonstrated clinically relevant performance [11]. Automated analysis of the electrocardiographic signal using deep learning models enables recognition of complex morphological and temporal variations across the entire tracing, reducing reliance on visual interpretation and improving diagnostic standardization, particularly in settings characterized by high examination volumes or limited availability of expert cardiologists [3].
Among the various arrhythmias studied, AF represents the main application domain of AI-ECG (Table 1). Recent studies have shown that algorithms based on CNN are capable of identifying AF even in patients presenting with sinus rhythm at the time of ECG recording. This finding suggests that the electrocardiographic signal may contain indirect information on electrical and structural atrial remodeling, potentially useful for identifying individuals with previously undiagnosed AF [12,13,14].
AI applied to the ECG has demonstrated the ability to identify patients with AF even in the presence of apparently normal sinus rhythm by exploiting latent electrophysiological signatures associated with subclinical atrial remodeling. In a large retrospective study involving 180,922 patients with 649,931 ECGs recorded in sinus rhythm, a CNN–based algorithm identified AF from a single standard 10-second 12-lead ECG with an AUC of 0.87, sensitivity of 79.0%, and specificity of 79.5%; analysis of serial ECGs from the same patient further improved diagnostic performance, with AUC values up to 0.90, sensitivity of 82.3%, and specificity of 83.4% [12].
A retrospective study conducted on 59,212 patients with more than 950,000 ECGs recorded in sinus rhythm evaluated the temporal trajectory of AF probability estimated using an AI-ECG algorithm before and after the first documented arrhythmic episode, demonstrating a progressive increase in estimated risk already in the years preceding clinical onset [13]. In particular, the mean probability of AF was 19.8% at 2–5 years, 23.6% at 1–2 years, and 34.0% in the 3 months preceding the first episode, with a further increase immediately after the initial event (40.9%), suggesting the presence of subclinical atrial electrophysiological alterations detectable early by the algorithm. The increase in risk was more pronounced in individuals aged ≥50 years and in patients with CHA₂DS₂-VASc scores ≥4, and the mean interval between the first algorithm-positive ECG and clinical diagnosis of AF was approximately 5.4 years, indicating a potential role for AI-ECG in early identification of the arrhythmic substrate and temporal risk stratification in patients eligible for targeted monitoring [13].
A deep learning model developed by Raghunath et al. [14] demonstrated that AI applied to standard 12-lead ECGs can predict incident AF in patients without prior AF and identify individuals at increased risk of AF-related stroke. Trained on approximately 1.6 million ECGs from ~430,000 patients, the model achieved an AUC of 0.85 for predicting new-onset AF within 1 year of the index ECG, with 69% sensitivity and 81% specificity in a simulated deployment scenario. Importantly, individuals classified as high risk showed a markedly increased long-term incidence of AF (hazard ratio 7.2 vs low-risk patients), and the algorithm identified 62% of patients who later experienced AF-related stroke within 3 years prior to the event. These findings support the potential role of AI-ECG as a scalable screening tool to enable targeted rhythm monitoring and early preventive strategies in populations at risk for occult AF and thromboembolic complications.
Integration of AI with continuous monitoring devices has further expanded application possibilities in the study of paroxysmal arrhythmias. Algorithms developed for the analysis of single-lead electrocardiographic signals recorded using wearable devices have demonstrated high accuracy in detecting AF, enabling early identification of intermittent arrhythmic episodes that are often not documented by conventional short-duration recordings. This approach opens new perspectives for primary stroke prevention strategies based on large-scale remote monitoring [15,16,17].
A multicenter study conducted on 9,750 participants from the Health eHeart cohort, with more than 139 million heart rate and physical activity measurements acquired through commercial smartwatches, developed a deep neural network for passive detection of AF, demonstrating high diagnostic performance in external validation on 51 patients undergoing cardioversion compared with standard 12-lead ECG (C-statistic 0.97; sensitivity 98.0%; specificity 90.2%) [16]. In an exploratory analysis of 1,617 outpatient subjects, accuracy was more moderate (C-statistic 0.72; sensitivity 67.7%; specificity 67.6%), likely reflecting greater physiological variability in real-world data acquisition conditions. Overall, these findings support the feasibility of large-scale continuous AF screening using wearable devices, while highlighting the need for further studies to define their clinical impact in uncontrolled settings [16].
A large-scale pragmatic prospective study (Apple Heart Study), conducted on 419,297 participants monitored for a median of 117 days using smartwatches with photoplethysmography-based algorithms, showed that 0.52% of individuals received irregular pulse notifications, with higher prevalence among those aged ≥65 years (3.14%) compared with those aged 22–39 years (0.16%) [17]. Among the 450 participants who returned an ECG patch after notification, AF was confirmed in 34% of cases (35% in those aged ≥65 years), with a positive predictive value of 0.84 for irregular pulse notification and 0.71 for individual irregular tachograms. Furthermore, 43% of notified individuals reported a new diagnosis of AF compared with 1.0% of non-notified participants, highlighting the potential of algorithms integrated into wearable devices to identify individuals at high arrhythmic risk and to enable early activation of diagnostic pathways in large-scale digital screening settings [17].
Beyond AF, AI applied to ECG has also shown promising results in the automated classification of other supraventricular and ventricular arrhythmias, including conduction disturbances and complex tachyarrhythmias. In these contexts, the use of deep learning models reduces inter-observer variability and improves the efficiency of automated reporting systems, with potential applications in telecardiology programs and high-volume electrocardiographic triage systems [4,18,19].
Overall, available evidence indicates that AI-ECG represents a reliable tool for automated arrhythmia diagnosis and early identification of patients at arrhythmic risk, with potentially important implications both in hospital settings and in community-based screening programs supported by digital technologies.
5. Identification of Structural Heart Disease Using AI-ECG
In recent years, the application of AI to the ECG has demonstrated that the electrocardiographic signal contains information not only about cardiac electrical activity but also about structural and functional myocardial characteristics that are not evident through conventional interpretation. Algorithmic analysis of the ECG tracing enables recognition of latent electrophysiological patterns associated with specific cardiomyopathies, opening the possibility of using the ECG as a tool for early identification of subclinical heart disease [4].
One of the most extensively studied areas is the identification of LV dysfunction (Table 2). This condition, often asymptomatic in its early stages, may remain undiagnosed until overt heart failure develops if targeted echocardiographic evaluation is not performed. Deep learning models applied to the standard 12-lead ECG have demonstrated the ability to identify patients with reduced LV ejection fraction (LVEF) even in the absence of specific electrocardiographic abnormalities, suggesting a potential role for AI-ECG as an opportunistic screening tool in outpatient or community settings [5,20,21,22,23].
The randomized pragmatic clinical EAGLE trial evaluated the integration of an AI algorithm applied to the 12-lead ECG into routine clinical practice for early identification of reduced LVEF (≤50%) in 22,641 patients without a known diagnosis of heart failure, demonstrating a significant increase in new diagnoses within 90 days compared with standard care (2.1% vs 1.6%; OR 1.32), with an even greater effect in patients with a positive AI result (19.5% vs 14.5%; OR 1.43) [20]. Use of the algorithm did not increase the overall utilization of echocardiography in the general population but improved its appropriateness among individuals with positive screening results (49.6% vs 38.1%), also facilitating identification of additional clinically relevant echocardiographic findings and initiation of guideline-directed therapies, supporting the potential role of AI-ECG in early screening for LV dysfunction in real-world primary care settings [20].
AI applied to the 12-lead ECG has also demonstrated the ability to noninvasively identify LV dysfunction in patients with Coronavirus Disease 2019 (COVID-19) infection, a condition associated with increased mortality risk. In a case series of 27 patients who underwent ECG and echocardiography within 14 days of diagnosis, the AI-ECG algorithm identified LVEF ≤40% with an AUC of 0.95, correctly identifying the 3 patients (11.1%) with LV dysfunction; in one case of COVID-19–associated myocarditis, the estimated probability of LVEF ≤40% was 90.2%, confirmed by echocardiography (LVEF 35%) [21]. These findings suggest that the diagnostic performance of AI-ECG remains high even in the presence of acute viral infection, supporting its potential use as a rapid bedside screening tool for early identification of LV dysfunction.
A study involving 97,829 patients with more than 625,000 paired ECG–echocardiogram datasets demonstrated that a deep learning algorithm applied to the standard 12-lead ECG was able to identify LV systolic dysfunction (LVEF ≤35%) with high diagnostic performance, achieving in the independent test dataset (52,870 patients) an AUC of 0.93, sensitivity of 86.3%, specificity of 85.7%, and a negative predictive value of 98.7%, with even higher performance in individuals without comorbidities (AUC 0.98) [22]. Moreover, among patients with ECGs classified as abnormal by the algorithm but with initially normal LVEF, the risk of subsequently developing LV dysfunction was approximately fourfold higher (HR 4.1; 95% CI 3.3–5.0), with an incidence of 9.5% at 5 years and 20.8% at 10 years, suggesting that AI-ECG can identify early subclinical abnormalities before the onset of overt systolic dysfunction and supporting its potential role as a large-scale noninvasive screening tool [22].
A multicenter retrospective study involving 55,163 ECGs from 22,765 patients who underwent echocardiography within 4 weeks developed and validated a deep learning algorithm for identification of LV dysfunction using the standard 12-lead ECG, demonstrating good diagnostic performance with an AUC of 0.843 in internal validation and 0.889 in external validation for LVEF ≤40%, and AUC values of 0.821 and 0.850, respectively, for LVEF≤50%, outperforming logistic regression and random forest models. The model, based exclusively on demographic variables and standard electrocardiographic parameters, confirms the feasibility of early identification of patients with LV dysfunction without the need for advanced imaging techniques, supporting the potential role of AI-ECG as a scalable screening tool in heart failure [23].
Another study developed and validated two AI models applied to standard 12-lead ECGs digitized via smartphone for identification of LV systolic dysfunction, using 109,809 paired ECG–echocardiogram datasets from 56,236 patients derived from more than 1,205,370 ECGs and 291,433 echocardiograms collected between 2011 and 2021 [24]. In the validation dataset (25,510 patients), the model for identifying LVEF ≤40% showed an AUC of 0.963 (95% confidence interval (CI)) 0.959–0.966), sensitivity 0.924, specificity 0.887, positive predictive value (PPV) 0.318, and negative predictive value (NPV) 0.995, whereas the model for LVEF <50% achieved an AUC of 0.952 (95% CI 0.947–0.956), sensitivity 0.899, specificity 0.875, PPV 0.382, and NPV 0.990, with prevalences of 5.4% and 7.9%, respectively, in the analyzed cohort. Integration with smartphone-based ECG digitization technology enables rapid and scalable identification of patients with LV dysfunction directly at the point of care, supporting the use of AI-ECG as a preliminary screening tool for selecting individuals eligible for echocardiographic evaluation and for early identification of patients at risk of developing heart failure in both clinical and community settings [24].
An additional area of application concerns HCM. Recent studies have shown that deep learning algorithms are capable of identifying electrophysiological signatures associated with the disease even in the absence of traditional diagnostic electrocardiographic criteria, suggesting a potential role for AI-ECG in screening at-risk individuals, particularly first-degree relatives of affected patients [4,25,26,27,28].
AI–based electrocardiographic analysis has demonstrated significant potential in the early screening of HCM, a condition that remains undiagnosed in up to 85% of cases. In a prospective real-world study involving 103,492 ECGs from 45,873 consecutive patients, the AI-ECG algorithm identified 1,265 individuals (2.7%) with suspected disease, among whom 63 (5%) received a new diagnosis following algorithmic alert. Using a probability threshold ≥0.85, the model achieved sensitivity of 100%, specificity of 98.4%, accuracy of 98.4%, and a NPV of 100%, whereas higher thresholds increased specificity up to 99.6% with a reduction in sensitivity. External validation on independent datasets confirmed high performance (AUC 0.975; sensitivity 68.4%; specificity 99.1%), supporting the role of AI-ECG as an effective digital biomarker for early identification of HCM and for activating targeted screening strategies in clinical practice [25].
A study involving 300 children and adolescents with HCM compared with 18,439 healthy controls validated a deep learning algorithm applied to the standard 12-lead ECG for disease identification in the pediatric population, demonstrating high diagnostic accuracy (AUC 0.98; sensitivity 92%; specificity 95%; NPV 99%). Performance remained high even in patients with apparently normal ECGs according to conventional criteria (AUC 0.96) and improved with age, reaching an AUC of 0.99 between 15 and 18 years, whereas lower values were observed in genotype-positive but phenotype-negative individuals, suggesting a correlation with phenotypic disease expression. These findings support the potential of AI-ECG as a non invasive screening tool for early diagnosis of HCM in pediatric and adolescent populations [26].
A study involving 3,060 patients with HCM and 63,941 controls developed a CNN applied to the standard 12-lead ECG for disease identification, demonstrating high diagnostic performance in the test dataset (AUC 0.96; sensitivity 87%; specificity 90%; negative predictive value 99%). Accuracy was particularly high in individuals younger than 40 years (sensitivity 95%; specificity 92%) and remained elevated even in patients with apparently normal ECGs (AUC 0.95) and in cases with LV hypertrophy, suggesting the ability of the algorithm to distinguish HCM from other causes of hypertrophy. Population screening simulations with estimated prevalence between 1:500 and 1:200 confirmed robust performance (AUC 0.95–0.96), with specificity increasing up to 99% when higher decision thresholds were applied, supporting the potential role of AI-ECG as a noninvasive screening tool to identify individuals eligible for further echocardiographic evaluation [27].
A study conducted in a real-world cohort of patients with HCM demonstrated that AI–based electrocardiographic analysis tools are capable of identifying characteristic electrophysiological patterns of the disease even in the presence of tracings considered nondiagnostic according to conventional criteria, with good discriminative accuracy (AUC 0.92). Performance remained high even in subgroups with apparently normal ECGs or nonspecific LV hypertrophy and showed a significant correlation with structural echocardiographic parameters such as ventricular wall thickness and myocardial mass, suggesting that AI-ECG may represent a useful non invasive tool for early identification of HCM and for selecting patients eligible for further imaging investigations or genetic evaluation [28].
Promising results have also been observed in the identification of cardiac amyloidosis, an infiltrative disease that is frequently underdiagnosed in its early stages because of the limited specificity of clinical and instrumental findings [29]. Automated analysis of the electrocardiographic tracing enables recognition of subtle alterations associated with myocardial infiltration before the appearance of typical imaging findings, suggesting a possible role for AI-ECG as an early screening tool in at-risk patients [30,31].
A study involving 2,541 patients with cardiac amyloidosis and 2,454 controls developed an AI-ECG algorithm applied to the standard 12-lead ECG for early disease identification, demonstrating high diagnostic performance with an AUC of 0.91 (95% CI 0.90–0.93), sensitivity 0.84, specificity 0.85, and positive predictive value 0.86. The algorithm identified the disease more than 6 months before clinical diagnosis in 59% of patients with ECGs available prior to onset, including 46% of Amyloid Light-chain (AL) amyloidosis cases and 70% of Transthyretin Wild-Type amyloidosis (ATTRwt) cases, maintaining good performance regardless of age, sex, and amyloidosis subtype, and even in the presence of apparently normal ECGs according to conventional criteria. Reduced configurations with single-lead or 6-lead ECGs also showed high diagnostic accuracy (AUC up to 0.90), supporting the potential of AI-ECG as an early, scalable screening tool applicable even in point-of-care settings or with wearable devices [30].
The study by Goto et al. developed and validated an automated AI–based pipeline for identifying cardiac amyloidosis through integration of ECG and apical four-chamber echocardiographic imaging in international multicenter cohorts, demonstrating good performance of the ECG-based model with C-statistics between 0.85 and 0.91 in external validation and even higher accuracy for the echocardiographic model (C-statistic 0.89–1.00), effective up to one year before clinical diagnosis. The model also demonstrated the ability to distinguish cardiac amyloidosis from phenotypically overlapping conditions such as HCM and hypertensive hypertrophy, and a sequential screening strategy with ECG-based preselection followed by echocardiographic evaluation improved the positive predictive value from 33% to 74–77%, supporting the role of multimodal AI-based approaches in screening rare infiltrative cardiomyopathies [31].
More recently, AI applied to ECG has shown the ability to contribute to identification of HFpEF [32]. In this context, AI-ECG may represent a useful tool for selecting patients eligible for further diagnostic evaluation, facilitating early disease detection strategies even in community-based healthcare settings.
A deep learning model applied to the standard 12-lead ECG was developed and validated in 34,103 patients for early identification of HFpEF, demonstrating good diagnostic accuracy with an AUC of 0.866 in internal validation and 0.869 in external validation, maintained even with reduced configurations using 6 leads (AUC 0.808–0.858) and single-lead ECGs (AUC 0.784–0.845). Among individuals initially without HFpEF on echocardiography, the model also identified a high-risk subgroup with a greater likelihood of developing the condition within 24 months (33.6% vs 8.4%; p < 0.001), and it showed good accuracy in detecting LV diastolic dysfunction in asymptomatic cohorts (AUC 0.837), supporting the potential of AI-ECG as a non invasive tool for early identification of HFpEF [32].

Table 3.
AI for cardiomyopathies and HFpEF detection.
| Study | Population | AI model | ECG type | Task | Main results | Clinical implication |
|---|---|---|---|---|---|---|
| Desai et al., 2025 [25] | 103,492 ECGs from 45,873 consecutive adult patients (real-world tertiary-care cohort) | Convolutional neural network (Viz-HCM AI-ECG algorithm) | Standard 12-lead ECG | Detection of hypertrophic cardiomyopathy | At probability threshold ≥0.85: sensitivity 95–100%, specificity >98%, accuracy >98%; AI-ECG identified 5% previously undiagnosed HCM cases among flagged patients | Demonstrates feasibility of large-scale real-world AI-ECG screening for HCM and supports its role as an early detection tool to trigger downstream imaging and family screening |
| Siontis et al., 2021 [26] | 300 pediatric HCM patients (≤18 years) vs 18,439 matched controls | Deep learning convolutional neural network (AI-ECG) | Standard 12-lead ECG | Detection of HCM in children and adolescents | AUC 0.98; sensitivity 92%; specificity 95%; NPV 99%; performance remained high even in patients with normal ECG by conventional interpretation | Supports feasibility of AI-ECG as a non-invasive screening tool for early detection of pediatric HCM and surveillance of at-risk individuals such as athletes and genotype-positive relatives |
| Ko et al., 2020 [27] | 3,060 HCM patients vs 63,941 controls (Mayo Clinic dataset; separate training/validation/testing cohorts) | Convolutional neural network (deep learning) | Standard 12-lead ECG | Identification of hypertrophic cardiomyopathy | AUC 0.96; sensitivity 87%; specificity 90%; NPV 99%; high performance even with normal ECG and in patients meeting ECG-LVH criteria; accuracy particularly high in subjects <40 years | Supports feasibility of ECG-based AI screening for HCM, especially in young individuals and populations with familial risk |
| Bos et al., 2023 [28] | Multicenter real-world cohort of patients with HCM vs controls | Deep learning AI-ECG algorithm | Standard 12-lead ECG | Identification of hypertrophic cardiomyopathy | AUC 0.92; performance maintained in subgroups with apparently normal ECG or nonspecific LVH; predicted probability correlated with LV wall thickness and myocardial mass; performance independent of age, sex, and genotype | Supports use of AI-ECG as a non-invasive screening tool for HCM and for selecting patients for advanced imaging or genetic evaluation |
| Grogan et al., 2021 [30] | 2,541 patients with cardiac amyloidosis (AL + ATTR) vs 2,454 age- and sex-matched controls (Mayo Clinic cohort) | Convolutional neural network (deep learning AI-ECG) | Standard 12-lead ECG (with additional analysis of 6-lead and single-lead configurations) | Detection of cardiac amyloidosis | AUC 0.91 (95% CI 0.90–0.93); sensitivity 84%; specificity 85%; PPV 0.86; NPV 0.84; disease identified >6 months before clinical diagnosis in 59% of patients with prior ECGs; maintained performance with 6-lead (AUC 0.90) and single-lead ECG (AUC 0.86) | Supports use of AI-ECG as a non-invasive early screening tool for cardiac amyloidosis, including point-of-care and reduced-lead device settings |
| Goto et al., 2021 [31] | International multicenter cohorts with cardiac amyloidosis vs phenotypically overlapping conditions (HCM, hypertensive LVH, ESRD) | Multimodal CNN (2D CNN for ECG; 3D CNN for echocardiography) | Standard 12-lead ECG + apical four-chamber echocardiographic view | Detection of cardiac amyloidosis | ECG model C-statistic 0.85–0.91 in external validation; echocardiographic model C-statistic 0.89–1.00; sequential ECG→echo strategy increased PPV from ~33% to 74–77%; disease identified up to 1 year before clinical diagnosis; echocardiographic model outperformed cardiologist interpretation of images alone | Demonstrates effectiveness of multimodal ECG-first AI screening strategies for early identification of cardiac amyloidosis and improved diagnostic discrimination from phenotypically similar hypertrophic conditions |
| Liu et al., 2022 [32] | 34,103 patients from two centers (32,671 ECG training; 13,934 ECG internal/external validation) | Deep learning neural network (AI-ECG) | Standard 12-lead ECG (with additional analysis of 6-lead and single-lead configurations) | Detection of HFpEF | AUC 0.866 (internal) and 0.869 (external); maintained performance with 6-lead ECG (AUC 0.808–0.858) and single-lead ECG (AUC 0.784–0.845); among patients initially without HFpEF, predicted high-risk subgroup showed 24-month incidence 33.6% vs 8.4% (p<0.001); diastolic dysfunction detection AUC 0.837 | Supports use of AI-ECG as a non-invasive early screening tool for HFpEF, including simplified-lead and ambulatory/wearable-compatible ECG configurations |
Studies evaluating AI–enabled electrocardiography for the detection of structural and infiltrative cardiomyopathies and heart failure with preserved ejection fraction. AI-ECG models show high performance in identifying hypertrophic cardiomyopathy, cardiac amyloidosis, and HFpEF, supporting non-invasive early screening and facilitating timely referral for advanced imaging and specialist evaluation. Abbreviations: 2D: Two-Dimensional, 3D: Three-Dimensional, AI: Artificial Intelligence, AI-ECG: Artificial Intelligence Electrocardiogram–based model output, AL: Amyloid Light-chain, ATTR: Transthyretin Amyloidosis, AUC: Area Under the Curve, CI: Confidence Interval, CNN: Convolutional Neural Network, ECG: Electrocardiogram, ESRD: End-Stage Renal Disease, HCM: Hypertrophic Cardiomyopathy, HFpEF: Heart Failure with Preserved Ejection Fraction, LVH: Left Ventricular Hypertrophy, NPV: Negative Predictive Value, PPV: Positive Predictive Value, Viz-HCM: Visualization Hypertrophic Cardiomyopathy algorithm, vs: versus.
Overall, these findings suggest that algorithmic ECG analysis may significantly contribute to the early identification of structural heart disease, transforming a widely available and low-cost test into a potentially valuable tool for large-scale cardiovascular screening strategies and for selecting patients eligible for more advanced diagnostic evaluations.
6. AI-ECG in Acute Coronary Syndromes
The ECG represents one of the fundamental tools in the initial evaluation of patients with suspected acute coronary syndrome, as it allows rapid identification of time-dependent conditions such as ST-segment elevation myocardial infarction (STEMI) [33]. However, in less typical clinical presentations—particularly in patients with non–ST-segment elevation myocardial infarction (NSTEMI)—interpretation of the tracing may be more complex and less sensitive. In this context, the application of AI to ECG has shown increasing potential as a tool for early risk stratification in patients presenting with chest pain [33].
A prospective multicenter study involving 8,493 patients with suspected acute myocardial infarction (AMI) demonstrated that an AI-ECG algorithm applied to the 12-lead ECG enables early risk stratification with high diagnostic accuracy (AUC 0.878), comparable to the HEART score—a clinical tool used in emergency departments for rapid chest pain assessment based on clinical history, electrocardiographic changes, age, cardiovascular risk factors, and troponin levels—and superior to the GRACE score, a more complex prognostic model used in patients with acute coronary syndrome to estimate mortality risk based on clinical, electrocardiographic, and laboratory parameters [33]. The algorithm showed sensitivity of 76.7%, specificity of 84.8%, and a NPV of 94.1%, identifying a low-risk subgroup corresponding to 8.2% of patients with a negative predictive value of 99.1% and a missed infarction rate below 1%. Performance was particularly high in STEMI (AUC 0.971; sensitivity 92.5%; negative predictive value 99.2%) and more moderate in NSTEMI (AUC 0.814; negative predictive value 94.6%). Furthermore, integration with the HEART score further improved prognostic stratification (C-index 0.926; net reclassification improvement 19.6%), supporting the role of AI-ECG as a rapid and noninvasive digital biomarker for decision support in patients presenting with chest pain in the emergency department [33].
Applications of AI-ECG are also particularly promising in recognizing patterns compatible with STEMI, in which diagnostic speed is crucial for activation of urgent revascularization pathways [34].
An international multicenter study evaluated an AI algorithm applied to the 12-lead ECG for identification of Occlusion Myocardial Infarction (OMI), demonstrating high diagnostic performance in external validation cohorts with AUC values between 0.93 and 0.95 and sensitivity higher than conventional STEMI criteria [34]. The algorithm enabled identification of a greater number of patients with angiographically confirmed coronary occlusion even in the absence of ST-segment elevation, improving early recognition of cases eligible for urgent revascularization and showing consistent performance across different international healthcare settings, supporting the potential role of AI-ECG in the triage of acute coronary syndromes, particularly in OMI non-STEMI equivalents [34].
Although traditional ECG interpretation remains highly effective in this context, automated signal analysis may help improve diagnostic standardization and support triage systems, particularly in settings characterized by high patient volumes or limited availability of specialists [4].
Another area of interest concerns the reduction of inappropriate activation of STEMI pathways. A multicenter U.S. study involving 1,032 patients with suspected STEMI undergoing urgent cardiac catheterization laboratory activation evaluated the impact of an AI-ECG algorithm in initial electrocardiographic triage, demonstrating a significant improvement in diagnostic accuracy compared with conventional interpretation. Specifically, the model achieved sensitivity of 92.0% compared with 71.0% for standard evaluation, specificity of 81.0% compared with 29.0%, and an AUC of 0.94, with a marked reduction in inappropriate catheterization laboratory activations (7.9% vs 41.8%). Moreover, the algorithm correctly reclassified 91% of biomarker-negative false-positive activations, maintaining high performance even in clinically more complex subgroups, supporting the potential role of AI-ECG in optimizing triage of patients with suspected STEMI and reducing diagnostic and therapeutic delays in emergency care pathways [35].
Overall, the available evidence suggests that AI-ECG may represent a useful decision-support tool in the initial management of patients with acute coronary syndrome, particularly as a complement to clinical assessment, biomarkers, and traditional risk scores.
Table 4.
AI for acute myocardial infarction and coronary occlusion detection.
| Study | Population | AI model | ECG type | Task | Main results | Clinical implication |
|---|---|---|---|---|---|---|
| Lee et al., 2025 (ROMIAE multicentre study) [33] | 8,493 adult patients presenting to 18 emergency departments within 24 h of symptom onset suspicious for AMI; AMI prevalence 18.6% (1,586/8,493) | Residual neural network–based AI-ECG model (AiTiAMI v1.00.00) | Standard 12-lead ECG (initial ED ECG only; raw signal 500 Hz) | Early detection and risk stratification of AMI and prediction of 30-day MACE | AMI detection: AUC 0.878, sensitivity 76.7%, specificity 84.8%, PPV 53.6%, NPV 94.1%; low-risk threshold sensitivity 99.6% and NPV 99.1%; high-risk threshold PPV 60.4%; STEMI AUC 0.971; NSTEMI AUC 0.814; 30-day MACE AUC 0.866; performance comparable to HEART score and superior to GRACE score, physician assessment, and initial hs-troponin; integration with HEART improved discrimination (C-index 0.926; NRI 19.6%) | Supports AI-ECG as a rapid ECG-only triage tool for early rule-out and rule-in of AMI in the emergency department, enabling accelerated chest-pain pathways and improved pre-biomarker risk stratification |
| Herman et al., 2023 [34] | International multicenter cohorts of patients with suspected acute coronary syndrome undergoing 12-lead ECG | Convolutional neural network (AI-ECG) | Standard 12-lead ECG | Detection of acute coronary occlusion myocardial infarction (OMI) | External validation AUC ≈ 0.93–0.95; improved identification of acute coronary occlusion compared with traditional STEMI criteria, including cases without ST elevation | Supports early AI-ECG–based decision support for identifying OMI missed by conventional STEMI criteria and prioritizing urgent reperfusion strategies |
| Herman et al., 2024 [35] | 1,032 patients with suspected STEMI undergoing urgent catheterization laboratory activation across 3 PCI centers in the United States | Convolutional neural network AI-ECG (Queen of Hearts, PMcardio) | Standard 12-lead ECG | Improvement of diagnostic accuracy in STEMI triage and detection of STEMI mimics | STEMI confirmed in 601/1,032 patients (58.2%); AI-ECG showed higher sensitivity than conventional triage and significantly reduced false catheterization laboratory activations while maintaining diagnostic performance | Supports early AI-assisted decision-making in STEMI triage, optimizing resource utilization and reducing unnecessary cath-lab activation without delaying reperfusion |
Studies investigating AI–enabled electrocardiography for early diagnosis and risk stratification in acute coronary syndromes. AI-ECG models improve detection of acute myocardial infarction and coronary occlusion compared with conventional ECG criteria, support rapid rule-out strategies in emergency settings, and enhance triage for urgent reperfusion therapy. Abbreviations: AI: Artificial Intelligence, AI-ECG: Artificial Intelligence Electrocardiogram–based model output, AMI: Acute Myocardial Infarction, AUC: Area Under the Curve, C-index: Concordance Index, ED: Emergency Department, ECG: Electrocardiogram, GRACE: Global Registry of Acute Coronary Events (risk score), HEART: History, ECG, Age, Risk factors, Troponin (risk score), Hz: Hertz, hs-troponin: High-sensitivity Troponin, MACE: Major Adverse Cardiovascular Events, NPV: Negative Predictive Value, NRI: Net Reclassification Improvement, NSTEMI: Non–ST-Elevation Myocardial Infarction, OMI: Occlusion Myocardial Infarction, PCI: Percutaneous Coronary Intervention, PMcardio: Powerful Medical Cardiology (AI-ECG software platform), PPV: Positive Predictive Value, ROMIAE: Risk-stratification Of Myocardial Infarction using Artificial intelligence in the Emergency department, STEMI: ST-Elevation Myocardial Infarction.
7. Prognostic Stratification and Prediction of Cardiovascular Outcomes Using AI-ECG
Beyond diagnostic applications, AI applied to the ECG has shown increasing potential in the prognostic stratification of cardiovascular patients. Several studies have demonstrated that algorithmic analysis of the electrocardiographic signal enables identification of latent information associated with the risk of future events, suggesting that the ECG may be used not only for diagnosing existing conditions but also for predicting clinical evolution in the medium and long term [1,6].
One of the most extensively studied areas concerns prediction of the development of heart failure. In particular, deep learning models initially developed to identify LV dysfunction have demonstrated the ability to recognize individuals at increased risk of developing heart failure during follow-up, even in the absence of clinically evident abnormalities at the time of ECG recording [36]. This finding suggests a potential role for AI-ECG as a tool for early identification of patients eligible for closer monitoring or targeted diagnostic evaluation.
AI has also shown promising results in prognostic stratification of patients with acute heart failure. Models developed by integrating clinical, laboratory, echocardiographic, and electrocardiographic data have demonstrated good ability to predict both in-hospital and long-term mortality, suggesting that algorithmic analysis of cardiovascular signals may contribute to early risk definition in more complex patients and support therapeutic decision-making in high-intensity care settings [37].
Another area of interest concerns prediction of all-cause mortality. Recent studies have shown that deep learning models applied to standard ECGs are capable of estimating long-term mortality risk even in unselected populations, suggesting that the electrocardiographic tracing contains summary information on the patient’s overall cardiovascular health status. In particular, the discrepancy between chronological age and biological age estimated through algorithmic ECG analysis has been associated with worse prognosis, reinforcing the concept of the ECG as an integrated digital biomarker of cardiovascular risk [4,36,38,39].
A study involving 1,558,415 patients from the CODE (Clinical Outcomes in Digital Electrocardiography) cohort developed a deep learning model capable of estimating directly from the standard 12-lead ECG the so-called ECG-age, an index of cardiovascular biological age derived from the electrophysiological characteristics of the tracing and distinct from chronological age. The discrepancy between ECG-age and chronological age proved to be a powerful independent predictor of mortality: specifically, an ECG-age more than 8 years higher than actual age was associated with a significant increase in mortality risk (HR 1.79; 95% CI 1.69–1.90), whereas an ECG-age more than 8 years lower than actual age was associated with reduced risk (HR 0.78; 95% CI 0.74–0.83), with results confirmed in independent external cohorts. This association remained significant after adjustment for traditional cardiovascular risk factors and persisted in individuals with apparently normal ECGs (HR up to 1.53), suggesting that ECG-age reflects subclinical cardiovascular aging processes not detectable through conventional interpretation and may represent a useful digital biomarker for large-scale prognostic stratification [38].
Overall, these findings suggest that AI-ECG may contribute to the development of increasingly predictive cardiovascular medicine strategies by enabling early identification of higher-risk patients and promoting a more personalized approach to clinical monitoring and prevention of cardiovascular events.
8. Population Screening, Wearable Devices, and Digital Biomarkers
The growing diffusion of AI applied to the ECG has progressively expanded the role of the ECG from a diagnostic tool used in selected clinical settings to a potential platform for large-scale cardiovascular screening. At the same time, the widespread adoption of wearable devices has further broadened the application possibilities of AI-ECG in population-based cardiovascular screening [40,41]. Algorithms developed for the analysis of single-lead electrocardiographic signals recorded using smartwatches, ECG patches, and optical sensors based on photoplethysmography have demonstrated high accuracy in detecting AF, enabling early identification of paroxysmal arrhythmic episodes that are often not documented with conventional short-duration recordings. This approach opens new perspectives for primary stroke prevention strategies based on continuous remote monitoring of large cohorts [15,40,41].
In addition to early diagnosis of arrhythmias and structural heart disease, algorithmic analysis of the electrocardiographic signal has demonstrated the ability to identify systemic conditions not directly related to cardiac electrical function. In particular, deep learning models applied to ECG have been used to estimate cardiovascular biological age and to detect electrolyte abnormalities such as hyperkalemia, suggesting that AI-enhanced ECG may be considered an integrated digital biomarker of the patient’s overall health status [5,15,42].
Overall, these findings indicate that AI-ECG may play an increasingly important role in future cardiovascular screening programs, particularly when integrated with remote monitoring systems and longitudinal digital platforms, contributing to the development of personalized prevention strategies based on early identification of at-risk individuals.
9. Multimodal Integration and Future Perspectives of AI-ECG
The most recent evolution of AI applied to the ECG is progressively moving beyond isolated signal analysis toward models capable of integrating information from multiple clinical data sources. The combination of ECG data with cardiovascular imaging, serum biomarkers, and longitudinal information from electronic health records enables the development of predictive models that more closely reflect the complexity of real-world clinical decision-making, improving individual risk stratification and supporting the development of more personalized therapeutic strategies [43,44].
In this context, integration between electrophysiological signals and cardiovascular imaging represents one of the most promising directions of development. Multimodal approaches have demonstrated the ability to improve arrhythmic risk classification in patients eligible for implantable cardioverter-defibrillators, suggesting that the combination of electrical and structural information may contribute to more accurate patient selection for invasive therapies and sudden cardiac death prevention strategies [36].
At the same time, the development of so-called foundation models for ECG interpretation is opening new perspectives for the simultaneous classification of multiple cardiovascular conditions [10]. A recent multicenter study developed and compared two AI models for automated ECG interpretation based respectively on supervised learning, trained directly on labeled ECGs, and self-supervised learning, initially pre-trained on large quantities of unlabeled signals and subsequently fine-tuned on specific clinical datasets. Both models, designed as foundation models—that is, models trained on large and heterogeneous datasets to learn general signal representations reusable across multiple diagnostic tasks—were trained on more than one million ECGs and validated on 13 independent datasets totaling 881,403 tracings, showing comparable performance in the classification of 77 electrocardiographic diagnoses (AUC 0.980–0.992). However, the self-supervised model demonstrated superior performance in predicting ECG-derived digital biomarkers, including LVEF ≤40% (AUC 0.926 vs 0.917), 5-year AF risk (0.742 vs 0.734), and long QT syndrome genotype (0.931 vs 0.850), with a particularly evident advantage in settings characterized by limited availability of annotated data, where it maintained improved performance up to ΔAUC 0.09 using only 1% of the labeled dataset [10].
In recent years, the emergence of systems based on generative AI and large language models has further expanded the potential clinical applications of AI in cardiology [7]. Generative AI includes models capable of creating new content—such as text, images, or structured data—based on information learned during training, whereas large language models are trained on massive text corpora to understand and generate natural language in a contextual and coherent manner [7]. These tools may support automated clinical documentation synthesis, facilitate integrated interpretation of multimodal data, and contribute to the generation of structured reports, thereby improving the efficiency of healthcare workflows. However, their implementation still requires rigorous prospective validation and appropriate clinical governance frameworks to ensure system safety, transparency, and reliability [7].
Overall, multimodal integration of cardiovascular data, the development of next-generation models, and the increasing diffusion of digital technologies suggest that AI-ECG may assume an increasingly central role in future diagnostic and prognostic pathways for cardiovascular patients, contributing to the transition toward predictive, preventive, and personalized cardiology.
10. Current Limitations of AI-ECG and Barriers to Clinical Implementation
Despite the promising results reported in recent years, integration of AI applied to the ECG into routine clinical practice remains limited by several methodological, organizational, and regulatory factors. Most available studies have evaluated algorithm performance in terms of diagnostic accuracy or predictive capability, whereas relatively few prospective multicenter studies and randomized controlled trials have demonstrated a direct impact on clinical outcomes or optimization of care pathways [45].
Many AI algorithms are developed using single-center datasets or selected populations, resulting in reduced generalizability of performance when applied to different clinical settings. Furthermore, the quality and independence of training and validation datasets represent critical factors in preventing overfitting, that is, the tendency of the model to adapt excessively to the specific characteristics of the data on which it was trained, learning noise or local peculiarities and therefore showing apparently high performance in development datasets but lower performance when applied to external populations [46]. Another limitation concerns the difficulty of algorithms in transferring knowledge across different types of clinical data and achieving true multimodal integration comparable to human clinical reasoning. Most available applications also remain confined to proof-of-concept studies, often with modest benefits compared with the current standard of care. Finally, challenges persist related to dataset annotation quality, the risk of demographic bias, and the need for independent external validation—key elements to ensure safe, equitable, and sustainable implementation of machine learning tools in clinical cardiology [46].
Another critical aspect of AI in cardiology concerns the limited interpretability of many deep learning models, often described as “black box” systems [47]. This term refers to the fact that although the algorithm can provide predictions or classifications with high accuracy, it is not always possible to clearly understand which information guided the final decision. In other words, clinicians receive the result but cannot easily reconstruct the reasoning followed by the model. This limited transparency represents an important barrier to integration of AI into routine clinical practice, as the use of automated diagnostic tools requires not only strong performance but also results that are understandable, verifiable, and reliable within the medical decision-making process [47].
According to the Scientific Statement of the American Heart Association, another critical issue in the use of AI-ECG concerns the risk of algorithmic bias, that is, the possibility that model performance may not be uniform across all patient groups [48]. This problem arises when algorithms are trained on datasets that are not sufficiently representative of the real population: if certain subgroups are underrepresented in the training data, the model may be less accurate precisely in those patients. Since clinical datasets often derive from selected populations or specific healthcare settings, algorithms may reflect these limitations and perform worse in groups that are already underrepresented in clinical research. For this reason, it is essential that models be developed and validated using large and diverse populations, with explicit evaluation of performance across different demographic and clinical subgroups [48].
Despite the growing use of wearable devices for remote cardiovascular monitoring, several relevant limitations remain. First, signal quality may vary significantly across devices and between individual patients, with a non-negligible proportion of ECG recordings being uninterpretable due to artifacts or noise [40]. Moreover, many consumer devices still require manual activation of recordings, with the risk of failing to document transient or asymptomatic arrhythmias. Another limitation concerns the not yet optimal accuracy of some emerging technologies, particularly cuffless blood pressure measurement, which may show significant variability depending on patient characteristics, conditions of use, and clinical context [40]. Additional challenges persist regarding patient adherence to continuous device use, variability across technological platforms, and the lack of standardized organizational models for integration into clinical workflows [40].
Finally, although observational studies have shown improvements in short-term physiological parameters, evidence remains limited regarding the impact of wearable devices on major cardiovascular outcomes and long-term mortality [40].
Introduction of these tools implies the definition of shared technical standards, clear regulatory pathways, and organizational models capable of supporting their use in routine practice [7]. Moreover, the recent development of systems based on multimodal models and generative AI raises additional challenges in terms of clinical governance, data security, and decision-making responsibility, making a structured approach to evaluation and adoption of these technologies within healthcare systems necessary [7].
Overall, AI-ECG has reached a high level of technological maturity, but its full integration into cardiology practice will require prospective multicenter studies, large-scale independent validation, and shared strategies to ensure transparency, reliability, and clinical sustainability of future applications.
11. Conclusions
AI applied to the ECG represents one of the most significant developments in contemporary digital cardiology, with applications ranging from automated arrhythmia diagnosis to early identification of structural heart disease, as well as prognostic stratification and population-based cardiovascular screening. Available evidence indicates that algorithmic analysis of the electrocardiographic signal enables extraction of clinically relevant information not evident through conventional interpretation, suggesting that AI-enhanced ECG may be considered an integrated digital biomarker of cardiovascular health status.
Despite the promising results observed in numerous experimental and real-world settings, full integration of AI-ECG into clinical practice still requires large-scale prospective validation and a clearer definition of its impact on clinical outcomes and organization of care pathways. In particular, model generalizability, interpretability, and integration into clinical workflows represent central elements for safe and effective dissemination of these technologies.
However, the evolution toward multimodal models capable of integrating electrocardiographic data, cardiovascular imaging, longitudinal information, and signals derived from wearable devices suggests that AI-ECG will play an increasingly important role in the cardiovascular medicine of the future. In this scenario, the ECG is no longer configured solely as a traditional diagnostic tool but as a dynamic digital platform capable of supporting prevention strategies, early diagnosis, and personalized risk stratification across the entire continuum of cardiovascular disease.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
The author has reviewed and edited the output and take full responsibility for the content of this publication. During the preparation of this manuscript, the author used ChatGPT (OpenAI, San Francisco, CA, USA; GPT-4 model) for language editing and improvement of readability.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
| AF | Atrial Fibrillation |
| AI | Artificial Intelligence |
| AL | Amyloid Light-chain |
| AMI | Acute Myocardial Infarction |
| ATTRwt | Transthyretin Wild-Type amyloidosis |
| AUC | Area Under the Curve |
| CI | Confidence Interval |
| CNN | Convolutional Neural Network |
| CODE | Clinical Outcomes in Digital Electrocardiography |
| COVID-19 | Coronavirus Disease 2019 |
| ECG | Electrocardiogram |
| ED | Emergency Department |
| ESRD | End-Stage Renal Disease |
| GRACE | Global Registry of Acute Coronary Events (risk score) |
| HCM | Hypertrophic Cardiomyopathy |
| HEART | History, ECG, Age, Risk factors, Troponin (risk score) |
| HFpEF | Heart Failure with preserved Ejection Fraction |
| HFrEF | Heart Failure with reduced Ejection Fraction |
| HR | Hazard Ratio |
| LV | Left Ventricle |
| LVEF | Left Ventricular Ejection Fraction |
| LVH | Left Ventricular Hypertrophy |
| MACE | Major Adverse Cardiovascular Events |
| NPV | Negative Predictive Value |
| NRI | Net Reclassification Improvement |
| NSTEMI | Non–ST-segment Elevation Myocardial Infarction |
| OMI | Occlusion Myocardial Infarction |
| OR | Odds Ratio |
| PCI | Percutaneous Coronary Intervention |
| PMcardio | Powerful Medical Cardiology (AI-ECG software platform) |
| PPG | Photoplethysmography |
| PPV | Positive Predictive Value |
| ROMIAE | Risk-stratification Of Myocardial Infarction using Artificial intelligence in the Emergency department |
| STEMI | ST-Elevation Myocardial Infarction |
| TTE | Transthoracic Echocardiography |
| Viz-HCM | Visualization Hypertrophic Cardiomyopathy algorithm |
References
- Krittanawong, C.; Virk, H.U.H.; Bangalore, S.; Wang, Z.; Johnson, K.W.; Pinotti, R.; Zhang, H.; Kaplin, S.; Narasimhan, B.; Kitai, T.; Baber, U.; Halperin, J.L.; Tang, W.H.W. Machine learning prediction in cardiovascular diseases: a meta-analysis. Sci Rep. 2020, 10(1), 16057. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Attia, Z.I.; Harmon, D.M.; Behr, E.R.; Friedman, P.A. Application of AI to the ECG. Eur Heart J 2021, 42(46), 4717–4730. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Somani, S.; Russak, A.J.; Richter, F.; Zhao, S.; Vaid, A.; Chaudhry, F.; De Freitas, J.K.; Naik, N.; Miotto, R.; Nadkarni, G.N.; Narula, J.; Argulian, E.; Glicksberg, B.S. Deep learning and the ECG: review of the current state-of-the-art. Europace 2021, 23(8), 1179–1191. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ose, B.; Sattar, Z.; Gupta, A.; Toquica, C.; Harvey, C.; Noheria, A. AI Interpretation of the ECG: A State-of-the-Art Review. Curr Cardiol Rep. 2024, 26(6), 561–580. [Google Scholar] [CrossRef] [PubMed]
- Siontis, K.C.; Noseworthy, P.A.; Attia, Z.I.; Friedman, P.A. AI-enhanced electrocardiography in cardiovascular disease management. Nat Rev Cardiol 2021, 18(7), 465–478. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kashou, A.H.; Adedinsewo, D.A.; Siontis, K.C.; Noseworthy, P.A. AI-Enabled ECG: Physiologic and Pathophysiologic Insights and Implications. Compr Physiol. 2022, 12(3), 3417–3424. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jain, S.S.; Elias, P.; Poterucha, T.; Randazzo, M.; Lopez Jimenez, F.; Khera, R.; Perez, M.; Ouyang, D.; Pirruccello, J.; Salerno, M.; Einstein, A.J.; Avram, R.; Tison, G.H.; Nadkarni, G.; Natarajan, V.; Pierson, E.; Beecy, A.; Kumaraiah, D.; Haggerty, C.; Avari Silva, J.N.; Maddox, T.M. AI in Cardiovascular Care-Part 2: Applications: JACC Review Topic of the Week. J Am Coll Cardiol. 2024, 83(24), 2487–2496. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rjoob, K.; Bond, R.; Finlay, D.; McGilligan, V.; Leslie, S.J.; Rababah, A.; Iftikhar, A.; Guldenring, D.; Knoery, C.; McShane, A.; Peace, A.; Macfarlane, P.W. Machine learning and the ECG over two decades: Time series and meta-analysis of the algorithms, evaluation metrics and applications. Artif Intell Med 2022, 132, 102381. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.W.; Olgin, J.E.; Avram, R.; Abreau, S.A.; Sittler, T.; Radia, K.; Hsia, H.; Walters, T.; Lee, B.; Gonzalez, J.E.; Tison, G.H. Performance of a Convolutional Neural Network and Explainability Technique for 12-Lead ECG Interpretation. JAMA Cardiol. 2021, 6(11), 1285–1295. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nolin-Lapalme, A.; Sowa, A.; Delfrate, J.; Tastet, O.; Corbin, D.; Kulbay, M.; Ozdemir, D.; Noël, M.J.; Marois-Blanchet, F.C.; Harvey, F.; Sharma, S.; Ansari, M.; Chiu, I.M.; D’souza, V.; Friedman, S.F.; Chassé, M.; Potter, B.J.; Afilalo, J.; Elias, P.A.; Jabbour, G.; Bahani, M.; Dubé, M.P.; Boyle, P.M.; Chatterjee, N.A.; Barrios, J.; Tison, G.H.; Ouyang, D.; Maddah, M.; Khurshid, S.; Cadrin-Tourigny, J.; Tadros, R.; Hussin, J.; Avram, R. Foundation models for ECG interpretation: clinical implications Epub ahead of print. Eur Heart J Erratum in: Eur Heart J. 2026 Mar 13:ehag139. doi: 10.1093/eurheartj/ehag139. PMID: 41568699. 2026, ehaf1119. [Google Scholar] [CrossRef] [PubMed]
- Ansari, Y.; Mourad, O.; Qaraqe, K.; Serpedin, E. Deep learning for ECG Arrhythmia detection and classification: an overview of progress for period 2017-2023. Front Physiol. 2023, 14, 1246746. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Attia, Z.; Noseworthy, P.; Lopez-Jimenez Fet, a.l. An AI-enabled ECG algorithm for the identification of patients with AF during sinus rhythm: a retrospective analysis of outcome prediction. The Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef]
- Christopoulos, Georgios; Attia, Zachi I; Van Houten, Holly K; Yao, Xiaoxi; Carter, Rickey E; Lopez-Jimenez, Francisco; Kapa, Suraj; Noseworthy, Peter A; Friedman, Paul A. AI—electrocardiography to detect AF: trend of probability before and after the first episode. European Heart Journal - Digital Health 2022, 3(Issue 2), 228–235. [Google Scholar] [CrossRef]
- Raghunath, S.; Pfeifer, J.M.; Ulloa-Cerna, A.E.; Nemani, A.; Carbonati, T.; Jing, L.; vanMaanen, D.P.; Hartzel, D.N.; Ruhl, J.A.; Lagerman, B.F.; Rocha, D.B.; Stoudt, N.J.; Schneider, G.; Johnson, K.W.; Zimmerman, N.; Leader, J.B.; Kirchner, H.L.; Griessenauer, C.J.; Hafez, A.; Good, C.W.; Fornwalt, B.K.; Haggerty, C.M. Deep Neural Networks Can Predict New-Onset AF From the 12-Lead ECG and Help Identify Those at Risk of AF-Related Stroke. Circulation 2021, 143(13), 1287–1298. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Elias, P.; Jain, S.S.; Poterucha, T.; Randazzo, M.; Lopez Jimenez, F.; Khera, R.; Perez, M.; Ouyang, D.; Pirruccello, J.; Salerno, M.; Einstein, A.J.; Avram, R.; Tison, G.H.; Nadkarni, G.; Natarajan, V.; Pierson, E.; Beecy, A.; Kumaraiah, D.; Haggerty, C.; Avari Silva, J.N.; Maddox, T.M. AI for Cardiovascular Care-Part 1: Advances: JACC Review Topic of the Week. J Am Coll Cardiol. 2024, 83(24), 2472–2486. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Sanchez, J.M.; Ballinger, B.; Singh, A.; Olgin, J.E.; Pletcher, M.J.; Vittinghoff, E.; Lee, E.S.; Fan, S.M.; Gladstone, R.A.; Mikell, C.; Sohoni, N.; Hsieh, J.; Marcus, G.M. Passive Detection of AF Using a Commercially Available Smartwatch. JAMA Cardiol 2018, 3(5), 409–416. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Perez, MV; Mahaffey, KW; Hedlin, H; Rumsfeld, JS; Garcia, A; Ferris, T; Balasubramanian, V; Russo, AM; Rajmane, A; Cheung, L; Hung, G; Lee, J; Kowey, P; Talati, N; Nag, D; Gummidipundi, SE; Beatty, A; Hills, MT; Desai, S; Granger, CB; Desai, M; Turakhia, M.P. Apple Heart Study Investigators Large-Scale Assessment of a Smartwatch to Identify, A.F. N Engl J Med 2019, 381(20), 1909–1917. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trayanova, N.A.; Popescu, D.M.; Shade, J.K. Machine Learning in Arrhythmia and Electrophysiology. Circ Res. 2021, 128(4), 544–566. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory ECGs using a deep neural network. Nat Med. Erratum in: Nat Med. 2019 Mar;25(3):530. doi: 10.1038/s41591-019-0359-9. PMID: 30617320; PMCID: PMC6784839. 2019, 25(1), 65–69. [Google Scholar] [CrossRef]
- Yao, X.; Rushlow, D.R.; Inselman, J.W.; et al. AI–enabled ECGs for identification of patients with low ejection fraction: a pragmatic, randomized clinical trial. Nat Med 2021, 27, 815–819. [Google Scholar] [CrossRef]
- Attia, Z.I.; Kapa, S.; Noseworthy, P.A.; Lopez-Jimenez, F.; Friedman, P.A. AI ECG to Detect LV Dysfunction in COVID-19: A Case Series. Mayo Clin Proc. 2020, 95(11), 2464–2466. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Attia, Z.I.; Kapa, S.; Lopez-Jimenez, F.; McKie, P.M.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Enriquez-Sarano, M.; Noseworthy, P.A.; Munger, T.M.; Asirvatham, S.J.; Scott, C.G.; Carter, R.E.; Friedman, P.A. Screening for cardiac contractile dysfunction using an AI-enabled ECG. Nat Med. 2019, 25(1), 70–74. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.M.; Kim, K.H.; Jeon, K.H.; Kim, H.M.; Kim, M.J.; Lim, S.M.; Song, P.S.; Park, J.; Choi, R.K.; Oh, B.H. Development and Validation of Deep-Learning Algorithm for Electrocardiography-Based Heart Failure Identification. Korean Circ J 2019, 49(7), 629–639. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Demolder, A; Herman, R; Vavrik, B; Martonak, M; Boza, V; Herman, M; Palus, T; Kresnakova, V; Bahyl, J; Iring, A; Hatala, R; Bartunek, J; Vanderheyden, M; Heggermont, W; Penicka, M. A smartphone based AI model to detect LV systolic dysfunction on 12-lead ECG. European Heart Journal 2024, 45, ehae666.3477. [Google Scholar] [CrossRef]
- Desai, M.Y.; Jadam, S.; Abusafia, M.; Rutkowski, K.; Ospina, S.; Gaballa, A.; Sultana, S.; Thamilarasan, M.; Xu, B.; Popovic, Z.B. Real-World AI-Based Electrocardiographic Analysis to Diagnose Hypertrophic Cardiomyopathy. JACC Clin Electrophysiol Epub 2025 Mar 17. 2025, 11(6), 1324–1333. [Google Scholar] [CrossRef] [PubMed]
- Siontis, K.C.; Liu, K.; Bos, J.M.; Attia, Z.I.; Cohen-Shelly, M.; Arruda-Olson, A.M.; Zanjirani Farahani, N.; Friedman, P.A.; Noseworthy, P.A.; Ackerman, M.J. Detection of HCMby an AI ECG in children and adolescents. Int J Cardiol. 2021, 340, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Ko, W.Y.; Siontis, K.C.; Attia, Z.I.; Carter, R.E.; Kapa, S.; Ommen, S.R.; Demuth, S.J.; Ackerman, M.J.; Gersh, B.J.; Arruda-Olson, A.M.; Geske, J.B.; Asirvatham, S.J.; Lopez-Jimenez, F.; Nishimura, R.A.; Friedman, P.A.; Noseworthy, P.A. Detection of HCMUsing a Convolutional Neural Network-Enabled ECG. J Am Coll Cardiol. 2020, 75(7), 722–733. [Google Scholar] [CrossRef] [PubMed]
- Babur Guler, G.; Guler, A.; Surgit, O.; Turkmen, I.; Atmaca, S.; Sahin, H.; Pay, D.; Almasri, M.; Coskun, G.; Yartasi, U.; Salduz, D.; Kuru Gorgulu, B.; Aydin, S.; Serbest, N.G.; Turkvatan Cansever, A.; Tanboga, I.H. Evaluation of AI-based ECG analysis tools in patients with hypertrophic cardiomyopathy. Eur Heart J Digit Health 2026, 7(2), ztag026. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kittleson, M.; Ambardekar, A.; Cheng, R.; et al. Transthyretin Cardiac Amyloidosis Evaluation and Management: 2025 ACC Concise Clinical Guidance. JACC 2026, 87(5), 549–565. [Google Scholar] [CrossRef] [PubMed]
- Grogan, M; Lopez-Jimenez, F; Cohen-Shelly, M; Dispenzieri, A; Attia, ZI; Abou Ezzedine, OF; Lin, G; Kapa, S; Borgeson, DD; Friedman, PA; Murphree, DH, Jr. AI-Enhanced ECG for the Early Detection of Cardiac Amyloidosis. Mayo Clin Proc. Erratum in: Mayo Clin Proc. 2023 Jan;98(1):211. doi: 10.1016/j.mayocp.2022.10.002. PMID: 34218880. 2021, 96(11), 2768–2778. [Google Scholar] [CrossRef]
- Goto, S.; Mahara, K.; Beussink-Nelson, L.; et al. AI-enabled fully automated detection of cardiac amyloidosis using ECGs and echocardiograms. Nat Commun 2021, 12, 2726. [Google Scholar] [CrossRef]
- Kwon, J.M.; Kim, K.H.; Eisen, H.J.; Cho, Y.; Jeon, K.H.; Lee, S.Y.; Park, J.; Oh, B.H. AI assessment for early detection of HFpEFbased on electrocardiographic features. Eur Heart J Digit Health Erratum in: Eur Heart J Digit Health. 2021 Nov 21;3(1):115-116. doi: 10.1093/ehjdh/ztab098. PMID: 36711179; PMCID: PMC9707919. 2020, 2(1), 106–116. [Google Scholar] [CrossRef]
- Lee, MS; Shin, TG; Lee, Y; Kim, DH; Choi, SH; Cho, H; Lee, MJ; Jeong, KY; Kim, WY; Min, YG; Han, C; Yoon, JC; Jung, E; Kim, WJ; Ahn, C; Seo, JY; Lim, TH; Kim, JS; Choi, J; Kwon, JM; Kim, K. ROMIAEstudy group AIapplied to ECGto rule out acute myocardial infarction: the ROMIAEmulticentre study Eur Heart, J. 2025, 46(20), 1917–1929. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Herman, R.; Meyers, H.P.; Smith, S.W.; Bertolone, D.T.; Leone, A.; Bermpeis, K.; Viscusi, M.M.; Belmonte, M.; Demolder, A.; Boza, V.; Vavrik, B.; Kresnakova, V.; Iring, A.; Martonak, M.; Bahyl, J.; Kisova, T.; Schelfaut, D.; Vanderheyden, M.; Perl, L.; Aslanger, E.K.; Hatala, R.; Wojakowski, W.; Bartunek, J.; Barbato, E. International evaluation of an AI-powered ECG model detecting acute coronary occlusion myocardial infarction. Eur Heart J Digit Health 2023, 5(2), 123–133. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Herman, R.; Mumma, B.E.; Hoyne, J.D.; Cooper, B.L.; Johnson, N.P.; Kisova, T.; Demolder, A.; Rafajdus, A.; Iring, A.; Palus, T.; Belmonte, M.; Barbato, E.; Baron, S.J.; Hatala, R.; Smith, S.W.; Meyers, H.P.; Sharkey, S.W.; Bartunek, J.; Henry, T.D. AI-Enabled ECG Analysis Improves Diagnostic Accuracy and Reduces False STEMI Activations: A Multicenter U.S. Registry. JACC Cardiovasc Interv. 2026, 19(2), 145–156. [Google Scholar] [CrossRef] [PubMed]
- Khera, R.; Oikonomou, E.K.; Nadkarni, G.N.; Morley, J.R.; Wiens, J.; Butte, A.J.; Topol, E.J. Transforming Cardiovascular Care With AI: From Discovery to Practice: JACC State-of-the-Art Review. J Am Coll Cardiol. 2024, 84(1), 97–114. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kwon, J.M.; Kim, K.H.; Jeon, K.H.; Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Kim, J.J.; Hwang, K.K.; Chae, S.C.; Baek, S.H.; Kang, S.M.; Choi, D.J.; Yoo, B.S.; Kim, K.H.; Park, H.Y.; Cho, M.C.; Oh, B.H. AI algorithm for predicting mortality of patients with acute heart failure. PLoS One 2019, 14(7), e0219302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lima, E.M.; Ribeiro, A.H.; Paixão, G.M.M.; Ribeiro, M.H.; Pinto-Filho, M.M.; Gomes, P.R.; Oliveira, D.M.; Sabino, E.C.; Duncan, B.B.; Giatti, L.; Barreto, S.M.; Meira WJr Schön, T.B.; Ribeiro, A.L.P. Deep neural network-estimated electrocardiographic age as a mortality predictor. Nat Commun 2021, 12(1), 5117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Raghunath, S.; Ulloa Cerna, A.E.; Jing, L.; vanMaanen, D.P.; Stough, J.; Hartzel, D.N.; Leader, J.B.; Kirchner, H.L.; Stumpe, M.C.; Hafez, A.; Nemani, A.; Carbonati, T.; Johnson, K.W.; Young, K.; Good, C.W.; Pfeifer, J.M.; Patel, A.A.; Delisle, B.P.; Alsaid, A.; Beer, D.; Haggerty, C.M.; Fornwalt, B.K. Prediction of mortality from 12-lead ECG voltage data using a deep neural network. Nat Med. 2020, 26(6), 886–891. [Google Scholar] [CrossRef] [PubMed]
- Spatz, E.S.; Ginsburg, G.S.; Rumsfeld, J.S.; Turakhia, M.P. Wearable Digital Health Technologies for Monitoring in Cardiovascular Medicine. N Engl J Med. 2024, 390(4), 346–356. [Google Scholar] [CrossRef] [PubMed]
- Barrera, N.; Solorzano, M.; Jimenez, Y.; Kushnir, Y.; Gallegos-Koyner, F.; Dagostin de Carvalho, G. Accuracy of Smartwatches in the Detection of AF: A Systematic Review and Diagnostic Meta-Analysis. JACC Adv. 2025, 4 11 Pt 1, 102133. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Attia, Z.I.; Harmon, D.M.; Behr, E.R.; Friedman, P.A. Application of AI to the ECG. Eur Heart J 2021, 42(46), 4717–4730. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Krittanawong, C.; Zhang, H.; Wang, Z.; Aydar, M.; Kitai, T. AI in Precision Cardiovascular Medicine. J Am Coll Cardiol. 2017, 69(21), 2657–2664. [Google Scholar] [CrossRef] [PubMed]
- Dey, D.; Slomka, P.J.; Leeson, P.; Comaniciu, D.; Shrestha, S.; Sengupta, P.P.; Marwick, T.H. AI in Cardiovascular Imaging: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019, 73(11), 1317–1335. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moosavi, A.; Huang, S.; Vahabi, M.; Motamedivafa, B.; Tian, N.; Mahmood, R.; Liu, P.; Sun, C.L.F. Prospective Human Validation of AI Interventions in Cardiology: A Scoping Review. JACC Adv. 2024, 3(9), 101202. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quer, G.; Arnaout, R.; Henne, M.; Arnaout, R. Machine Learning and the Future of Cardiovascular Care: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021, 77(3), 300–313. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Karatzia, L.; Aung, N.; Aksentijevic, D. AI in cardiology: Hope for the future and power for the present. Front Cardiovasc Med. 2022, 9, 945726. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Armoundas, AA; Narayan, SM; Arnett, DK; Spector-Bagdady, K; Bennett, DA; Celi, LA; Friedman, PA; Gollob, MH; Hall, JL; Kwitek, AE; Lett, E; Menon, BK; Sheehan, KA; Al-Zaiti, SS. American Heart Association Institute for Precision Cardiovascular Medicine; Council on Cardiovascular and Stroke Nursing; Council on Lifelong Congenital Heart Disease and Heart Health in the Young; Council on Cardiovascular Radiology and Intervention; Council on Hypertension; Council on the Kidney in Cardiovascular Disease; and Stroke Council. Use of AI in Improving Outcomes in Heart Disease: A Scientific Statement From the American Heart Association. Circulation 2024, 149(14), e1028–e1050. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Table 1.
AI for AF detection and prediction.
| Study | Population | AI model | ECG type | Task | Main results | Clinical implication |
|---|---|---|---|---|---|---|
| Attia et al., 2019 [12] | 180,922 patients; 649,931 sinus-rhythm ECGs | Convolutional neural network (CNN) | Standard 10-s 12-lead ECG | Detection of AF during sinus rhythm | AUC 0.87 (single ECG); sensitivity 79.0%; specificity 79.5%; accuracy 79.4%. Using multiple ECGs: AUC 0.90, sensitivity 82.3%, specificity 83.4% | Enables identification of occult or future AF from a single routine ECG, supporting opportunistic screening and selection of patients for prolonged rhythm monitoring |
| Christopoulos et al., 2022 [13] | 59,212 patients; 957,816 ECGs before and after first AF episode | Convolutional neural network (CNN) | Standard 10-s 12-lead ECG | Temporal prediction of AF onset | AI-ECG probability progressively increased up to years before first AF episode (19.8% at 2–5 years prior → 34.0% within 3 months prior); mean interval between first positive AI-ECG and AF diagnosis: 5.4 years | Serial AI-ECG assessment may identify patients at increasing risk of AF years before clinical onset and guide targeted rhythm monitoring strategies |
| Raghunath et al., 2021 [14] | 1.6 million resting 12-lead ECGs from ~430,000 adult patients without prior atrial fibrillation (Geisinger health system cohort) | Deep neural network (convolutional deep learning model) | Standard 10-s 12-lead ECG | Prediction of new-onset AF within 1 year and identification of patients at risk of AF-related stroke | AUC 0.85 for prediction of incident AF within 1 year; sensitivity 69%, specificity 81% in simulated deployment scenario; hazard ratio 7.2 for long-term AF risk in high- vs low-risk groups; model identified 62% of patients who developed AF-related stroke within 3 years before stroke occurrence | Supports use of AI-ECG for early identification of patients at risk for incident AF and AF-related stroke, enabling targeted rhythm monitoring and preventive anticoagulation strategies in high-risk populations |
| Tison et al., 2018 [16] | 9,750 participants (Health eHeart cohort); external validation in 51 cardioversion patients; exploratory ambulatory cohort 1,617 subjects | Deep neural network | Smartwatch photoplethysmography (heart rate + step count data) | Passive detection of AF from wearable data | External validation vs 12-lead ECG: AUC 0.97, sensitivity 98.0%, specificity 90.2%; ambulatory detection: AUC 0.72, sensitivity 67.7%, specificity 67.6% | Demonstrates feasibility of passive large-scale AF detection using commercially available smartwatches, supporting wearable-based population screening strategies |
| Perez et al., 2019 (Apple Heart Study) [17] | 419,297 smartwatch users monitored for median 117 days | Irregular pulse detection algorithm (photoplethysmography-based) | Smartwatch PPG signal with confirmatory ECG patch | Large-scale population screening for AF | Irregular pulse notifications in 0.52% overall (3.14% ≥65 years); AF confirmed in 34% of participants returning ECG patch; notification PPV 0.84; tachogram PPV 0.71; 43% of notified participants reported new AF diagnosis vs 1.0% in non-notified | Demonstrates feasibility of large-scale digital AF screening using consumer wearable devices and supports integration of smartwatch-based alerts into diagnostic pathways |
Key studies evaluating AI–enabled electrocardiography (AI-ECG) for the detection and prediction of AF. AI-ECG models demonstrate high diagnostic accuracy for identifying occult or future AF from sinus-rhythm ECGs and support opportunistic screening strategies, targeted rhythm monitoring, and large-scale population detection through integration with wearable technologies. Abbreviations: AF: Atrial Fibrillation, AI: Artificial Intelligence, AI-ECG: Artificial Intelligence Electrocardiogram–based model output, AUC: Area Under the Curve, CNN: Convolutional Neural Network, ECG: Electrocardiogram, PPG: Photoplethysmography, PPV: Positive Predictive Value.
Table 2.
AI for LV systolic dysfunction detection.
| Study | Population | AI model | ECG type | Task | Main results | Clinical implication |
|---|---|---|---|---|---|---|
| Yao et al., 2021 (EAGLE trial) [20] | 22,641 adult patients from 120 primary care teams | Convolutional neural network (AI-ECG) | Standard 12-lead ECG | Detection of reduced left LVEF ≤50% in routine clinical practice | New diagnosis of low LVEF within 90 days: 2.1% vs 1.6% (AI vs usual care; OR 1.32); in AI-positive patients: 19.5% vs 14.5% (OR 1.43); echocardiography use higher in AI-positive group (49.6% vs 38.1%) | Demonstrates that integration of AI-ECG Demonstrates that integration of AI-ECG into clinical workflows improves early detection of asymptomatic LV dysfunction in real-world primary care settings |
| Attia et al., 2020 [21] | 27 COVID-19 patients with ECG and echocardiography within 14 days | Convolutional neural network (AI-ECG) | Standard 12-lead ECG | Detection of LV dysfunction (LVEF ≤40%) in COVID-19 patients | AUC 0.95 for identification of LVEF ≤40%; LV dysfunction detected in 3 patients (11.1%); algorithm identified myocarditis-related LVEF reduction with predicted probability 90.2% corresponding to echocardiographic LVEF 35% | Supports feasibility of AI-ECG as rapid bedside screening tool for ventricular dysfunction in COVID-19, potentially reducing need for immediate echocardiography in high-risk infectious settings |
| Attia et al., 2019 [22] | 97,829 patients with paired ECG–echocardiogram within 2 weeks (test set: 52,870) | Convolutional neural network (CNN) | Standard 12-lead ECG | Detection of asymptomatic LV systolic dysfunction (LVEF ≤35%) | AUC 0.93; sensitivity 86.3%; specificity 85.7%; accuracy 85.7%. Patients with positive AI-ECG but normal LVEF had 4-fold higher risk of developing future LV dysfunction (HR 4.1) | Demonstrates feasibility of AI-ECG as a population-level screening tool for asymptomatic LV dysfunction and early identification of subjects at risk for future heart failure |
| Kwon et al., 2019 [23] | 55,163 ECGs from 22,765 patients across 2 hospitals | Deep neural network | Standard 12-lead ECG + demographic features | Detection of HFrEF (LVEF ≤40%) and LVEF ≤50% | AUC 0.843 (internal) and 0.889 (external) for LVEF ≤40%; AUC 0.821 and 0.850 for LVEF ≤50%; performance superior to logistic regression and random forest (p<0.001) | Demonstrates feasibility of ECG-based deep-learning screening for heart failure using routine clinical parameters, enabling early identification of patients requiring echocardiographic evaluation |
| Demolder et al., 2024 [24] | 109,809 paired ECG–echocardiogram datasets (56,236 patients); validation cohort: 25,510 ECG–TTE pairs | Deep learning AI-ECG integrated with smartphone ECG digitization | Standard 12-lead ECG (smartphone-based acquisition/digitization) | Detection of reduced LVEF (≤40% and <50%) | For LVEF ≤40%: AUC 0.963, sensitivity 0.924, specificity 0.887, NPV 0.995; for LVEF <50%: AUC 0.952, sensitivity 0.899, specificity 0.875, NPV 0.99 | Demonstrates feasibility of smartphone-based AI-ECG screening for LV systolic dysfunction, enabling scalable point-of-care identification of patients requiring echocardiographic evaluation |
Key studies assessing the use of AI applied to electrocardiography for the identification of LV systolic dysfunction. AI-ECG algorithms enable early detection of reduced LV ejection fraction, including in asymptomatic individuals and primary care settings, supporting population-level screening strategies and guiding referral for confirmatory echocardiography. Abbreviations: AI: Artificial Intelligence, AI-ECG: Artificial Intelligence Electrocardiogram–based model output, CNN: Convolutional Neural Network, COVID-19: Coronavirus Disease 2019, ECG: Electrocardiogram, HR: Hazard Ratio, HFrEF: Heart Failure with Reduced Ejection Fraction, LV: Left Ventricle, LVEF: Left Ventricular Ejection Fraction, NPV: Negative Predictive Value, OR: Odds Ratio, TTE: Transthoracic Echocardiography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



