Submitted:
09 April 2026
Posted:
10 April 2026
You are already at the latest version
Abstract
Cervical cancer remains a major public health challenge worldwide and in Poland, where mortality rates are among the highest in the European Union. Persistent infection with high-risk human papillomavirus (hrHPV), particularly genotype HPV16, plays a central role in cervical carcinogenesis. This study aimed to evaluate the regional variability of hrHPV prevalence and genotype distribution in Poland and to assess its potential implications for cervical cancer incidence and prevention strategies.
A systematic literature review was conducted using PubMed, Scopus, and Google Scholar to identify studies published up to May 2025 reporting hrHPV prevalence and genotypes among Polish women. Eligible studies included population-based cohorts, women undergoing screening, and patients with cervical lesions or cancer.
The analysis revealed substantial heterogeneity in hrHPV prevalence and genotype distribution across regions and study populations. Nationwide data indicate high overall HPV prevalence (up to 50.9%), with HPV16 consistently dominating, followed by HPV31, HPV51, HPV52, and HPV66. Regional differences were observed, including higher prevalence of HPV51 in southern Poland and HPV56 and HPV45 in central regions. Studies in women with abnormal cytology or cervical cancer showed markedly higher hrHPV prevalence (often >90%), with HPV16 predominating in high-grade lesions and invasive cancer.
These findings confirm the dominant oncogenic role of HPV16 while highlighting significant regional variability in other hrHPV genotypes. Such differences may influence the effectiveness of screening and vaccination programs. Strengthening standardized, regionally stratified HPV surveillance is essential to optimize cervical cancer prevention and tailor public health interventions in Poland.
Keywords:
HPV genotypes
; geographical variation
; Poland
Simple Summery
Cervical cancer is a significant health problem in Poland, largely caused by infection with high-risk types of human papillomavirus (hrHPV). This study summarizes current knowledge about how often different HPV types occur in Polish women and whether their distribution varies between regions. A review of published studies shows that HPV16 is the most common and most dangerous type across all groups of women, including those with normal cytology, precancerous lesions, and cervical cancer. However, other hrHPV types, such as HPV31, HPV51, HPV52, HPV56, and HPV66, also occur frequently and their distribution differs by region. For example, HPV51 is more common in southern Poland, while HPV56 and HPV45 are more often found in central regions. These regional differences may affect the effectiveness of screening and vaccination programs. Better, standardized monitoring of HPV types across Poland is needed to improve prevention and early detection of cervical cancer.
1. Introduction
Cervical cancer is nowdays the fourth most common cancer among women worldwide. In 2022, approximately 660,000 new cases were diagnosed globally, with around 350,000 deaths resulting from this disease [1]. According to data from the Polish National Cancer Registry in 2022 there were approximately 2,200 new cases of cervical cancer diagnosed, and nearly 1,500 deaths attributed to this type of cancer [2]. The standardized incidence rate is estimated at around 10 per 100,000 women, while the standardized mortality rate is approximately 5.5 per 100,000. These data place Poland among the countries with one of the higher cervical cancer mortality rates in the European Union. The discrepancy between incidence and mortality highlights a delay in diagnosis due to from the one side limited access to early detection methods and from other side low attendance of Polish women at screening program.
In the pathogenesis of cervical dysplasia and carcinoma central role plays Human papillomavirus (HPV) infection, particularly with high-risk genotypes. HPVs are a large group of DNA viruses, with over 200 identified genotypes, of which more than 40 can infect the anogenital tract. The International Agency for Research on Cancer (IARC) have classified HPV genotypes into categories based on their oncogenic potential, primarily with respect to their association with cervical and other anogenital cancers [3,4]. According to this classification, HPV genotypes are divided into the following risk categories: (1) group 1: carcinogenic to humans (high-risk HPV - hrHPV), including: HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59; (2) group 2A: probably carcinogenic to humans with limited evidence of carcinogenicity, but strong mechanistic and epidemiological support: HPV68; (3) group 2B: possibly carcinogenic to humans with limited and less consistent evidence: HPV26, 53, 66, 67, 70, 73, and 82; (4) group 3: not classifiable as to their carcinogenicity in humans and (5) low-risk HPV (lrHPV) types with genotypes not associated with cancer but are known to cause benign lesions [5].
HPV infection among women with normal cervical cytology constitutes a significant public health burden. Osmani et al. (2025), analyzing 73 studies with 41,745 women aged ≥50, reported a global prevalence of any HPV of 11.7% and high-risk HPV of 6.45% [6]. Earlier analyses found similar levels: Bruni et al. (2010) reviewed 194 studies including 1,016,719 women, reporting 11.7% [7], and de Sanjosé et al. (2007) found 10.4% among 157,879 women [8]. Thus, it seems that HPV prevalence remains fairly stable worldwide, but varies regionally, with highest in Sub-Saharan/Western Africa (16.5–32.2%), Central/South America (10.4–24.5%), and Eastern Europe (21.4–29.1%) [6,7,8,9], intermediate in Asia (3.3–14%), and lowest in Western Europe (3.7–6.6%) [6,7,9]. Globally, high-risk HPV16 dominates (1.2–19.7%), followed by HPV18, 31, 52, and 58, with other HR-HPVs showing regional patterns: HPV53/51 in North America, HPV58 in Asia/Latin America, HPV31/33 in Europe, and high genotype diversity in Africa [6,7,8,9]. In women with LSIL, HPV16 remains most prevalent (26.3%), followed by HPV31, 51, 53, and 56, with regional variation: HPV16 16.3–32.6%, HPV18 5.0–11.5%, and certain genotypes more frequent in specific regions (HPV31/33 in Europe, HPV58 in Asia) [10]. In CIN2/3 and ICC, HPV16 and HPV18 predominate, with combined attributable fractions of 71.9–83.2% across regions [11]. HPV16 prevalence in ICC ranges 52–79%, with regional contributions from other genotypes: HPV52/58 in East/Southeast Asia, HPV33/66 in Central/South America, HPV35 in Africa, and HPV45 frequently detected in adenocarcinomas [12,13,14,15,16,17]. In Europe, HPV16/18 remain the most common oncogenic types in ICC and HSIL, though their distribution varies by subregion due to behavioral, genetic, and public health factors [18]. Combined HPV16/18 prevalence in ICC is 74–77%, with hrHPVs 31, 33, and 45 showing regional variation. Eastern and Southeastern Europe exhibit higher HPV16/18 prevalence and broader HR-HPV diversity. Multicenter studies of cervical glandular neoplasia’s report HPV16 prevalence 15.8–75%, HPV18 25–68.4%, and HPV45 0–16.7% [19], while Tjalma et al. found HPV16 in 63% of ICC cases, HPV18 15.2%, and HPV45 5.3%, illustrating type-specific progression risks relevant for screening strategies [20].
There are also growing indications that the prevalence of hrHPV types may vary regionally within Poland. Observations from other European countries with similar demographic structures, such as Germany [21], Italy [22] or Spain [23], demonstrate that significant regional differences in the distribution of specific hrHPV genotypes are not uncommon. These variations have been attributed to multiple interrelated factors, including disparities in access to healthcare, differences in sexual behaviors and the average age of sexual debut, unequal coverage of HPV vaccination programs, and variable uptake of both cytological and molecular screening strategies. Poland exhibits substantial regional heterogeneity that could influence the distribution of hrHPV types. Differences in urbanization levels, economic development, the organization and accessibility of gynecological care, and health literacy across regions in Poland are also factors that may contribute to local variations in HPV epidemiology. Importantly, these disparities are also reflected in the incidence of cervical cancer. Epidemiological data show that the burden of cervical cancer in Poland is not uniformly distributed; rather, incidence rates vary significantly between voivodeships. The highest incidence rates have been reported in voivodeships such as Świętokrzyskie, Lubelskie, and Podkarpackie, where the burden of disease remains significantly elevated compared to the national average [2]. In contrast, voivodeships including Mazowieckie, Wielkopolskie, and Pomorskie consistently demonstrate some of the lowest incidence rates of cervical cancer. These variations suggest differences in regional risk factors, access to preventive services, screening coverage, and possibly socio-economic determinants that influence disease occurrence.
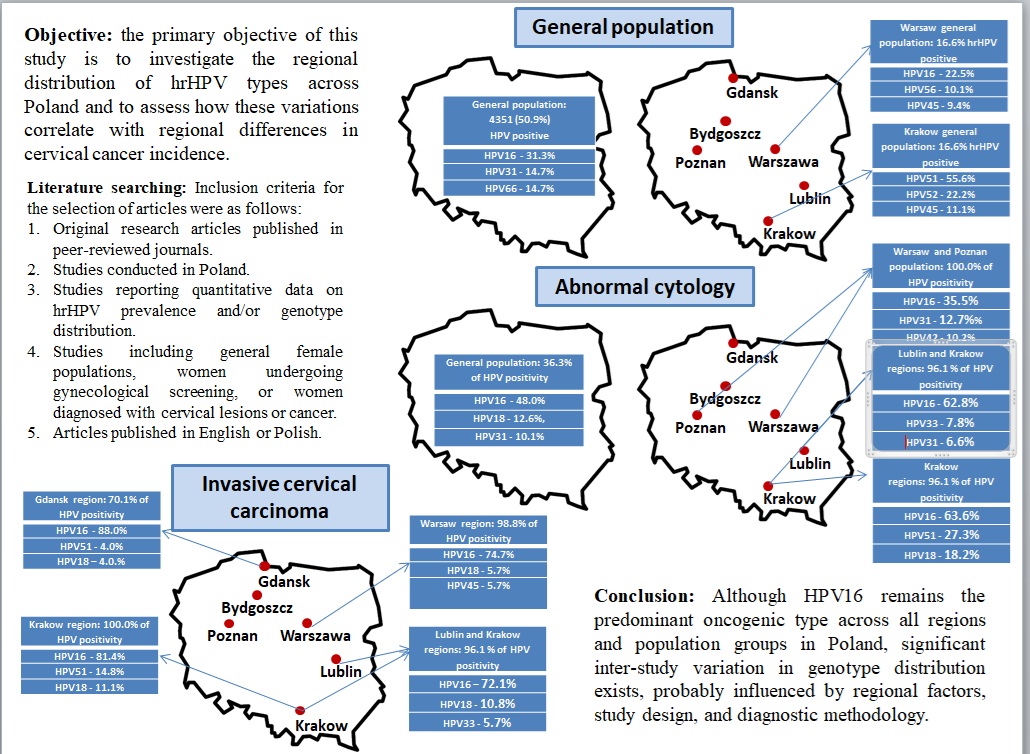
In light of the recent guidelines introducing molecular testing for carcinogenic types of human papillomavirus (cHPV) as a primary screening method in the cervical cancer prevention program in Poland [24], understanding the epidemiology of specific HPV genotypes within the local population has become crucial. In Poland, there is a lack of systematic analysis addressing whether significant geographic variation in the distribution of HPV genotypes exists within Poland. Such differences may affect the sensitivity and effectiveness of HPV-based screening tests, the design of region-specific public health strategies, the risk assessment for progression to HSIL/CIN2+, the justification for tailoring diagnostic tools to regional needs (e.g., locally adapted test panels). Therefore, the primary objective of this study is to investigate the regional distribution of hrHPV types across Poland and to assess how these variations correlate with regional differences in cervical cancer incidence. This research aims to fill the existing gap in nationwide, population-based data by providing representative, regionally stratified prevalence estimates. Additionally, the study seeks to identify regions with higher prevalence of specific hrHPV genotypes that may impact the effectiveness of current vaccination programs and screening strategies. Ultimately, the findings are intended to support the development of targeted, evidence-based public health interventions to optimize cervical cancer prevention and control in Poland.
2. Literature Search
A literature search was conducted to identify studies reporting the prevalence and genotype distribution of high-risk human papillomavirus (hrHPV) among women in Poland. The search aimed to include both population-based screening studies and studies focused on women with cytological abnormalities or cervical cancer.
The literature review was performed using the following electronic databases: PubMed, Scopus, and Google Scholar. The search included publications available up to May 2025 and used combinations of the following keywords and MeSH terms: “HPV”, “human papillomavirus”, “hrHPV”, “high-risk HPV”, “Poland”, “genotype”, “cervical cancer”, “cervical intraepithelial neoplasia”, “LSIL”, “HSIL”, “prevalence”, and “epidemiology”. Boolean operators such as AND, OR, and NOT were applied to refine the search.
Inclusion criteria for the selection of articles were as follows:
- Original research articles published in peer-reviewed journals.
- Studies conducted in Poland.
- Studies reporting quantitative data on hrHPV prevalence and/or genotype distribution.
- Studies including general female populations, women undergoing gynecological screening, or women diagnosed with cervical lesions or cancer.
- Articles published in English or Polish.
Exclusion criteria were:
- Review articles, conference abstracts, case reports, and editorials.
- Studies with insufficient data on HPV genotype distribution.
- Studies using outdated or non-specific HPV detection methods without genotype resolution.
3. Results
3.1. Human Papillomavirus Prevalence and Genotype Distribution in the General Female Population Across Different Regions of Poland
Table 1 presents data from six Polish studies assessing HPV prevalence and genotype distribution in the general female population and among women with cervical pathology or abnormal cytology. The studies span nearly two decades (2008–2024) and encompass a wide range of geographical regions of Poland and diagnostic methodologies, offering a comprehensive perspective on hrHPV epidemiology in Poland. The most geographically inclusive study by Glińska et al. [24] analyzed over 11,000 women from 556 sites across all 16 voivodeships of Poland. This large-scale, nationwide screening revealed a HPV prevalence of 50.9%, with HPV16 (31.3%), HPV31 (14.7%), HPV66 (14.7%), and HPV51 (13.0%) being the most common genotypes. The high genotype diversity identified in this cohort is likely attributable to the use of multiple advanced genotyping platforms, which allowed for broad HPV detection across the country. This study provides the most representative data for Poland and serves as a benchmark for regional comparison. However, in the earlier studies from 2008, the percentage of HPV prevalence was lower. In the studies including general population from Warsow region, Baradin et al have noticed percentage of cHPV infection in 16.6% woman with HPV16, HPV56, HPV45, HPV31 and HPV52 as the most frequent [25]. In turn, Szostek et al., analyzing population of woman with normal cytology from south-central Poland have noticed cHPV prevalence in 21.0% cases. In this study the most frequent HPV genotype were HPV51, HPV52, HPV45, HPV5 [26]6 and 11.1%. These results may reflect, from one side, increase on HPV infection among polish woman in the last years and on the other side, regional differences in distribution of particular cHPV genotypes.
3.2. Human Papillomavirus Prevalence and Genotype Distribution Among Women with Abnormal Cytology Across Different Regions of Poland
Studies among women with abnormal cytology indicate a high prevalence of hrHPV across Polish regions, with HPV16 consistently dominant (Table 2). Bebyn et al. [27] reported hrHPV RNA positivity in 36.3% of women from the Bydgoszcz region, with HPV16, HPV18, HPV31, HPV33, and HPV45 as the most common genotypes. Regional analyses by Kiwerska et al. [28] (Warsaw and Poznań) and Nowakowski et al. [29] (southeastern Poland) showed very high hrHPV prevalence in women with cervical abnormalities, particularly high-grade lesions, again dominated by HPV16. Szostek et al. [26] demonstrated genotype differences according to lesion severity in southern Poland, with HPV51 prevalent in LSIL and HPV16 dominating HSIL cases. Overall, these findings confirm the central role of HPV16 nationwide, while highlighting regional and lesion-specific variability in less common genotypes, influenced by geography, population characteristics, and diagnostic methodology.
Regarding woman with w abnormal cytology, study by Bebyn et al. [27] investigated the prevalence of high-risk HPV genotypes in cervical cytology samples from the Bydgoszcz region (Table 2). Among 1,840 women, most showed abnormal cytology, including LSIL, HSIL, ASC-US, ASC-H, and AGC. mRNA analysis using NucliSENS EasyQ HPV revealed that 36.3% (198 women) of the general population were HPV RNA positive. The most common genotypes were HPV16 (48.0%), HPV18 (12.6%), HPV31 (10.1%), HPV33 (8.6%), and HPV45 (4.5%), with 16.2% of women infected with more than one HPV type. Kiwerska et al [28], in 2019 have analyzed data from the Warsaw (central Poland) and Poznań (west Poland) regions. They found a 100% hrHPV positivity rate among this group, with HPV16 (35.5%) being the most prevalent, but also identifying genotypes such as HPV42, HPV39, HPV54, and HPV53, which were less commonly reported in nationwide data. In turn, Nowakowski et al. [29] in the analysis covering southeastern Poland (Lublin and Krakow), found high hrHPV prevalence in women with high-grade CIN (96.1%), with HPV16 (62.8%) and HPV33 (7.8%) being the most common. Although not a general population study, it supports regional data suggesting high HPV16 burden in the east of Poland. Szostek et al. (2008) provided a more nuanced analysis from southern Poland by separating women into cytological categories (LSIL, HSIL). The data showed significant differences in genotype profiles depending on the severity of cytological abnormalities. For example, HPV51 was the most common genotype in LSIL (30.2%) and also prominent in HSIL (27.3%) cases, whereas HPV16 was the leading type in HSIL (63.6%). This suggests both a biological gradient in genotype oncogenicity and potentially region-specific genotype distributions. Taken together, these studies illustrate the dominant role of HPV16 across all Polish regions, but also demonstrate meaningful regional variability in less common genotypes such as HPV51, HPV66, HPV52, and HPV45. Differences in prevalence and genotype spectrum are influenced not only by geography but also by population characteristics (screening vs. cytological abnormalities) and HPV detection methodology. These findings underscore the need for geographically sensitive public health strategies and highlight the importance of using broad-spectrum, high-sensitivity HPV detection tools in nationwide surveillance. As HPV vaccination continues to shift the landscape of prevalent genotypes, such detailed regional data will be essential to monitor genotype replacement and vaccine impact.
3.3. The prevalence and Genotype Distribution of Human Papillomavirus in Women with Invasive Cervical Cancer (ICC) Across Different Regions of Poland
Table 3 summarizes findings from four studies that examined the prevalence and genotype distribution of cHPV in women with invasive cervical cancer (ICC) across different regions of Poland, conducted between 1997 and 2008. While all studies consistently report a high prevalence of cHPV among cervical cancer cases (ranging from 70.1% to 100%), regional differences are evident in both detection rates and genotype distribution. HPV16 emerged as the predominant genotype in all regions, with the highest prevalence observed in the Gdańsk region (88.0%, Liss et al., 2002) and southern Poland (81.4%, Szostek et al., 2008). The prevalence of HPV18, the second most common oncogenic type, varied geographically—from 5.7% in the Warsaw region (Baradzin et al., 2008) to 11.1% in southern Poland (Szostek et al., 2008). Some regional differences may reflect methodological variability; however, they may also suggest genuine geographic heterogeneity in circulating HPV genotypes. In the Warsaw region, Baradzin et al. identified a relatively diverse hrHPV profile, detecting not only HPV16 and HPV18, but also HPV31, HPV45, HPV52, and HPV56. In contrast, the Lublin and Krakow regions (Nowakowski et al., 2014) showed a narrower spectrum, with HPV16, HPV18, HPV33, and HPV45 being most frequently detected. Similarly, in the Gdańsk cohort (Liss et al., 2002), only five hrHPV types were identified, and a significantly lower overall hrHPV positivity rate (70.1%) was reported—potentially due to earlier testing technologies and limited genotype panels. The southern Polish study by Szostek et al. (2008) revealed the highest hrHPV positivity (100%) and one of the broadest genotype spectrums, including HPV51, HPV66, and HPV68, suggesting possible regional differences in HPV ecology or sample characteristics. This variability highlights the importance of comprehensive HPV surveillance across diverse geographical regions to better understand the regional burden of different hrHPV types.
Taken together, these findings underscore the predominance of HPV16 and HPV18 in cervical cancer across Poland but also point to regional heterogeneity in less common hrHPV genotypes. Such geographic differences are important to consider when designing regionally tailored prevention strategies, including screening and vaccination programs, especially in the context of non-16/18 hrHPV types that may gain prominence as vaccination alters HPV type distribution.
4. Interpretation of Findings
Data from Polish studies demonstrate marked regional and population-related variability in hrHPV prevalence and genotype distribution, while consistently confirming the etiological dominance of HPV16 in cervical pathology. The nationwide study by Glińska et al. [24], based on samples from 556 sites across all 16 voivodeships, provides the most comprehensive overview of circulating hrHPV genotypes in the general population, although the lack of voivodeship-specific analyses limits regional interpretation. In contrast, other studies were regionally focused, covering central Poland (Warsaw and Bydgoszcz) [25,28], eastern regions [29], and southern Poland [26], and revealed distinct genotype patterns. Notably, HPV51 was highly prevalent in southern Poland, whereas HPV56 and HPV45 were more frequent in central regions. Higher proportions of HPV18 and HPV33 were observed in the Warsaw area, while HPV66 appeared more often in recent studies but was rare in earlier reports. These findings suggest true regional variation in hrHPV genotype circulation, potentially shaped by demographic, behavioral, and healthcare-related factors, and underline the need for region-specific prevention strategies, particularly where non-16/18 genotypes are common.
Comparisons across studies must also account for differences in population composition and study design. Population-based screening studies reported lower hrHPV prevalence (50.9% in the nationwide cohort [24]) than studies focusing on women with abnormal cytology or histologically confirmed lesions, where hrHPV prevalence ranged from over 90% to 100% [26,28]. Genotype distribution also varied with lesion severity: HPV51 and HPV52 predominated in LSIL, whereas HPV16 was dominant in HSIL and high-grade CIN, consistent with its higher oncogenic potential [26,29]. In low-risk populations, such as women with normal cytology, hrHPV prevalence was substantially lower, and HPV16 was rarely detected.
Inter-study variability is further influenced by substantial heterogeneity in HPV detection methods, including DNA-based PCR assays, hybrid capture techniques, mRNA-based tests, and multiplex genotyping platforms. Broad-spectrum PCR assays identified a wider range of hrHPV genotypes, including less common types, whereas mRNA-based assays detected transcriptionally active infections but may underestimate overall prevalence. Earlier studies using less sensitive methods likely underreported both prevalence and genotype diversity. Together, these methodological differences limit direct comparability and highlight the need for standardized, high-sensitivity HPV testing platforms in future surveillance to ensure reliable monitoring of regional trends and vaccination impact.
The compiled data from multiple Polish studies reveal a complex landscape of high-risk human papillomavirus (hrHPV) prevalence and genotype distribution among women in different regions and population groups. While all studies confirm the etiological dominance of HPV16 in cervical pathology, substantial differences in the frequency of other hrHPV types, as well as in overall prevalence, reflect underlying differences in population characteristics, study designs, and methodological approaches. The geographic scope of the studies also impacts the interpretation of HPV epidemiology. The study of Glińska et al. [24] is the only study to provide a nationwide perspective, drawing samples from 556 locations. Their findings likely offer the most comprehensive overview of circulating genotypes in the general population across Poland; however, it is regrettable that the authors did not present a separate analysis for each voivodeship, which could have provided more localized insights. Other studies had more localized scopes: Baradin et al. [25] and Kiwerska et al. [28] focused on central Poland (Warsaw and Bydgoszcz), Nowakowski et al. on Eastern regions [29] and Szostek et al. [26] on the South. Notably, genotype profiles differed across regions. In southern Poland [26], HPV51 was highly prevalent (up to 55.6% in women with normal cytology and 30.2% in LSIL), whereas in central Poland, HPV56 and HPV45 were more common [25]. The Warsaw region also showed relatively high frequencies of HPV18 and HPV33 [25], while HPV66 was frequent in both studies from 2024 [24] and 2019 [28] the but rare in older studies. These differences could reflect regional variation in HPV genotype circulation, potentially influenced by demographic, behavioral, or healthcare-related factors. They also highlight the need for regionally tailored prevention and vaccination strategies, especially in areas where non-16/18 types are more prevalent.
However, it should be noticed that comparing results of these studies attention must pay also on other factors influencing its results, such as: differences in study population, methodological differences in HPV presence assessment and genotyping. Variability in hrHPV prevalence across studies maybe related to the composition of the investigated population. Population-based screening studies, such as the large-scale nationwide project by Glińska et al. [24], which included over 11,000 women from all 16 Polish voivodeships, reported a 50.9% hrHPV positivity rate. In contrast, studies involving women with abnormal cytology or histologically confirmed lesions reported markedly higher hrHPV positivity rates. For example, Kiwerska et al. [28], analyzing women with cervical pathology from the Warsaw and Poznań regions, found a 100% hrHPV prevalence, with a similar dominance of HPV16 (35.5%), but also wide range of less common genotypes (e.g., HPV42, 53, 54, 66). Similarly, Szostek et al. [26] showed that among women with LSIL and HSIL, hrHPV prevalence reached 98.0% and 92.0%, respectively, with genotype distribution reflecting lesion severity-HPV51 and 52 were most common in LSIL, while HPV16 dominated in HSIL. Studies involving high-grade lesions or cancer, such as Nowakowski et al. [29], found HPV16 in 62.8% of women with HG-CIN, and HPV33 and HPV31 as the next most frequent types. This pattern supports the known progression risk associated with these genotypes and aligns with global trends. Conversely, in low-risk populations (e.g., women with normal cytology in study of Szostek et al. [26], hrHPV prevalence was significantly lower (21.0%), and the genotype profile differed, with HPV51 and 52 dominating, but HPV16 being almost absent (only 1 case).
Another major factor affecting inter-study comparability is the diversity in HPV detection techniques. Across the studies, there is significant heterogeneity in diagnostic platforms. The studies employed a variety of diagnostic platforms, ranging from PCR-based assays and hybrid capture techniques to mRNA analyses and multiplex genotyping systems (e.g., Anyplex II, INNO-LiPA, Linear Array, Alinity m). These methodological differences affect both sensitivity and the spectrum of detectable HPV genotypes. For instance, broad-spectrum, type-specific PCR assays, as used by Glińska et al. [24] and Kiwerska et al. [28], identified a more diverse high-risk HPV (hrHPV) profile, including less common genotypes such as HPV53, HPV42, and HPV68. Conversely, mRNA-based assays (e.g., NucliSENS EasyQ used by Bebyn et al., [27] target a limited number of genotypes but detect active viral transcription, potentially underestimating overall prevalence. Earlier studies (25, 29] relying on DNA hybridization or older PCR methods generally exhibited lower sensitivity and narrower genotype coverage. These methodological disparities likely contribute to variations in reported prevalence and bias genotype frequency estimates toward types detectable by the respective assays. Importantly, rarer genotypes may be underrepresented in older or less comprehensive studies. To improve comparability and reliability of HPV surveillance data globally, standardization of detection methods and assay platforms is critically needed in future research. Standardization of HPV testing platforms in future surveillance studies is essential to ensure consistency, reproducibility, and comparability of data across regions and over time.
Based on the current body of evidence and existing knowledge gaps, several critical priorities have been identified to advance our understanding and control of HPV-related disease in Poland. First, there is a pressing need for longitudinal, multicenter cohort studies that can track changes in HPV prevalence over time. Such studies are particularly important in the context of widespread vaccination programs, as they will help monitor vaccine impact and detect any shifts in genotype distribution, including the potential rise of non-vaccine HPV types in the post-vaccination era. Second, regional surveillance efforts must be reinforced to reflect the known geographic variability in the distribution of high-risk HPV genotypes. Strengthening these programs will facilitate tailored screening strategies and vaccination policies that are responsive to local epidemiological patterns. Third, the adoption of standardized genotyping protocols across national cervical cancer screening programs is essential. This standardization will ensure consistent and comparable data collection, improve data quality, and promote better integration with electronic health records and public health databases. Additionally, broader inclusion of diverse population groups in surveillance and research is crucial. Special attention should be given to underserved or high-risk populations, such as women living in rural areas, older women, and immunocompromised individuals, to ensure equitable access to prevention and care services. Finally, linking molecular HPV findings with clinical outcomes—including viral persistence, clearance rates, and progression of precancerous lesions—will enhance our understanding of the carcinogenic potential of less common high-risk HPV genotypes beyond types 16 and 18. This knowledge is vital for refining risk stratification and optimizing patient management in cervical cancer prevention programs.
Finally it should be underlie that the introduction in Poland of a primary cervical cancer screening model based on the detection of DNA from oncogenic human papillomavirus (HPV) types, implemented within a program funded by the Narodowy Fundusz Zdrowia, represents an important step toward modern, evidence-based secondary prevention. This strategy is consistent with current international recommendations and reflects the well-documented higher sensitivity of HPV testing compared with conventional cytology. At the same time, analysis of the epidemiological data presented in this study suggests that the performance of this model may be partially influenced by local biological factors and regional heterogeneity in circulating high-risk HPV (hrHPV) genotypes. Although HPV16 remains the dominant genotype across all regions of Poland and across all disease stages, the distribution of other hrHPV types shows meaningful geographic variation. In southern Poland, HPV51 has been reported relatively frequently, including in LSIL and HSIL lesions, whereas studies from central regions more often identified HPV56 and HPV45. In the Warsaw region, a comparatively higher contribution of HPV18 and HPV33 has been observed. More recent nationwide studies additionally indicate an increasing prevalence of HPV52 and HPV66, highlighting the dynamic nature of hrHPV epidemiology over time. In the context of an HPV-based primary screening algorithm with cytology performed only in HPV-positive women, this regional diversity of hrHPV genotypes underscores the importance of adequate test sensitivity, broad genotype coverage, and the quality of cytological triage. These observations do not challenge the rationale for the current screening model but rather suggest potential value in its continued optimization based on national and regional epidemiological data, which may further enhance the effectiveness and clinical safety of the program.
5. Conclusions
Although HPV16 remains the predominant oncogenic type across all regions and population groups in Poland, significant inter-study variation in genotype distribution exists, probably influenced by regional factors, study design, and diagnostic methodology. These findings underscore the importance of standardized, geographically comprehensive surveillance and the need for future studies that integrate epidemiological, molecular, and clinical data to inform effective and adaptive public health interventions, particularly in the era of HPV vaccination.
Author Contributions
Conceptualization, B.B. W.S methodology, B.B. A.M-M., A.K.W.S; writing—original draft preparation, B.B.; A.A.-M.; A.K., W.S. writing—review and editing, M.K. and R.T.; supervision, B.B.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024, 74(3), 229–263. [Google Scholar] [CrossRef]
- Didkowska, J.; Barańska, K.; Miklewska, M.J.; Wojciechowska, U. Cancer incidence and mortality in Poland in 2023. Nowotwory. Journal of Oncology 2024, 74(2), 75–93. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Biological agents. IARC Monogr Eval Carcinog Risks Hum. 2012, 100 Pt B, 1–441.
- Human Papillomaviruses. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, IARC. 2007, ISBN-13, 978-92-832-1290-4.
- Target product profiles for human papillomavirus screening tests to detect cervical precancer and cancer. Geneva: World Health Organization 2024, Licence: CC BY-NC-SA 3.0 IGO.
- Osmani, V.; Hörner, L.; Nkurunziza, T.; Rank, S.; Tanaka, L.F.; Klug, S.J. Global prevalence of cervical human papillomavirus in women aged 50 years and older with normal cytology: a systematic review and meta-analysis. Lancet Microbe 2025, 6(1), 100955. [Google Scholar] [CrossRef]
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F.X.; de Sanjosé, S. Cervical human papillomavirus prevalence in 5 continents: meta-analysis of 1 million women with normal cytological findings. J Infect Dis. 2010, 15;202(12), 1789–99. [Google Scholar] [CrossRef]
- de Sanjosé, S.; Diaz, M.; Castellsagué, X.; Clifford, G.; Bruni, L.; Muñoz, N.; Bosch, FX. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis. Lancet Infect Dis. 2007, 7(7), 453–9. [Google Scholar] [CrossRef]
- Clifford, G.M.; Gallus, S.; Herrero, R.; Muñoz, N.; Snijders, P.J.; Vaccarella, S.; Anh, P.T.; Ferreccio, C.; Hieu, N.T.; Matos, E.; Molano, M.; Rajkumar, R.; Ronco, G.; de Sanjosé, S.; Shin, H.R.; Sukvirach, S.; Thomas, J.O.; Tunsakul, S.; Meijer, C.J.; Franceschi, S. Worldwide distribution of human papillomavirus types in cytologically normal women in the International Agency for Research on Cancer HPV prevalence surveys: a pooled analysis. Lancet 2005, 366, 991–98. [Google Scholar] [CrossRef]
- Clifford, G.M.; Rana, R.K.; Franceschi, S.; Smith, J.S.; Gough, G.; Pimenta, J.M. Human papillomavirus genotype distribution in low-grade cervical lesions: comparison by geographic region and with cervical cancer. Cancer Epidemiol Biomarkers Prev. 2005, 14(5), 1157–64. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Georges, D.; Man, I.; Baussano, I.; Clifford, G.M. Causal attribution of human papillomavirus genotypes to invasive cervical cancer worldwide: a systematic analysis of the global literature. Lancet 2024, 404(10451), 43. [Google Scholar] [CrossRef] [PubMed]
- Guan, P.; Howell-Jones, R.; Li, N.; Bruni, L.; de Sanjosé, S.; Franceschi, S.; Franceschi, S.; Clifford, G.M. Human Papillomavirus Types in 115,789 HPV-Positive Women: A Meta-Analysis from Cervical Infection to Cancer. Int J Cancer 2012, 131, 2349–2359. [Google Scholar] [CrossRef]
- Li, N.; Franceschi, S.; Howell-Jones, R.; Snijders, P.J.; Clifford, G.M. Human papillomavirus type distribution in 30,848 invasive cervical cancers worldwide: Variation by geographical region, histological type and year of publication. Int J Cancer 2011, 128(4), 927–35. [Google Scholar] [CrossRef]
- de Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.R.; Vallejos, C.S.; de Ruiz, P.A.; Lima, M.A.; Guimera, N.; Clavero, O.; Alejo, M.; Llombart-Bosch, A.; Cheng-Yang, C.; Tatti, S.A.; Kasamatsu, E.; Iljazovic, E.; Odida, M.; Prado, R.; Seoud, M.; Grce, M.; Usubutun, A.; Jain, A.; Suarez, G.A.; Lombardi, L.E.; Banjo, A.; Menéndez, C.; Domingo, E.J.; Velasco, J.; Nessa, A.; Chichareon, S.C.; Qiao, Y.L.; Lerma, E.; Garland, S.M.; Sasagawa, T.; Ferrera, A.; Hammouda, D.; Mariani, L.; Pelayo, A.; Steiner, I.; Oliva, E.; Meijer, C.J.; Al-Jassar, W.F.; Cruz, E.; Wright, T.C.; Puras, A.; Llave, C.L.; Tzardi, M.; Agorastos, T.; Garcia-Barriola, V.; Clavel, C.; Ordi, J.; Andújar, M.; Castellsagué, X.; Sánchez, G.I.; Nowakowski, A.M.; Bornstein, J.; Muñoz, N.; Bosch, F.X. Retrospective International Survey and HPV Time Trends Study Group. Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 11(11), 1048–56. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Lindsay, L.; Hoots, B.; Keys, J.; Franceschi, S.; Winer, R.; Clifford, G.M. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer 2007, 121(3), 621–32. [Google Scholar] [CrossRef]
- Clifford, G.M.; Smith, J.S.; Aguado, T.; Franceschi, S. Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: a meta-analysis. Br J Cancer 2003, 89, 101–05. [Google Scholar] [CrossRef]
- Pinheiro, M.; Gage, J.C.; Clifford, G.M.; Demarco, M.; Cheung, L.C.; Chen, Z.; Yeager, M.; Cullen, M.; Boland, J.F.; Chen, X.; Raine-Bennett, T.; Steinberg, M.; Bass, S.; Befano, B.; Xiao, Y.; Tenet, V.; Walker, J.; Zuna, R.; Poitras, N.E.; Gold, M.A.; Dunn, T.; Yu, K.; \; Zhu, B.; Burdett, L.; Turan, S.; Lorey, T.; Castle, P.; Wentzensen, N.; Burk, R.; Schiffman, M.; Mirabello, L. Association of HPV35 with cervical carcinogenesis among women of African ancestry: Evidence of viral-host interaction with implications for disease intervention. Int J Cancer 2020, 147(10), 2677–2686. [Google Scholar] [CrossRef]
- Poljak, M.; Seme, K.; Maver, P.J.; Kocjan, B.; Cuschieri, K.S.; Rogovskaya, S.I.; Arbyn, M.; Syrjänen, S. Human papillomavirus prevalence and type-distribution, cervical cancer screening practices and current status of vaccination implementation in Central and Eastern Europe. Vaccine 2013, 31 Suppl 7, H59–70. [Google Scholar] [CrossRef]
- Reuschenbach, M.; Valente, S.; Takyar, J.; Dhawan, A.; Hall, A.; Agrawal, N.; Ghelardi, A.; Del Pino, M.; Nowakowski, A.; Sabale, U. Treatment characteristics, HPV genotype distribution and risk of subsequent disease among women with high-grade cervical intraepithelial neoplasia in Europe: A systematic literature review. Eur J Obstet Gynecol Reprod Biol. 2024, 300, 129–140. [Google Scholar] [CrossRef]
- Tjalma, W.A.; Fiander, A.; Reich, O.; Powell, N.; Nowakowski, A.M.; Kirschner, B.; Koiss, R.; O'Leary, J.; Joura, E.A.; Rosenlund, M.; Colau, B.; Schledermann, D.; Kukk, K.; Damaskou, V.; Repanti, M.; Vladareanu, R.; Kolomiets, L.; Savicheva, A.; Shipitsyna, E.; Ordi, J.; Molijn, A.; Quint, W.; Raillard, A.; Rosillon, D.; De Souza, S.C.; Jenkins, D.; Holl, K. HERACLES/SCALE Study Group. Differences in human papillomavirus type distribution in high-grade cervical intraepithelial neoplasia and invasive cervical cancer in Europe. Int J Cancer 2013, 132(4), 854–67. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.A.; Tanaka, L.F.; Radde, K.; Bussas, U.; Ikenberg, H.; Heideman, D.A.M.; Meijer, C.J.L.M.; Blettner, M.; Klug, S.J. Population-based age- and type-specific prevalence of human papillomavirus among non-vaccinated women aged 30 years and above in Germany. BMC Infect Dis. 2024, 24(1), 1008. [Google Scholar] [CrossRef] [PubMed]
- Cenci, M.; Rossi, F.; Pisani, T. Detection of 14 High-risk Human Papillomavirus (HPV) Genotypes Within the Italian Cervical Cancer Screening. In Vivo 2023, 37(5), 2161–2165. [Google Scholar] [CrossRef]
- López, N.; Torné, A.; Franco, A.; San-Martin, M.; Viayna, E.; Barrull, C.; Perulero, N. Epidemiologic and economic burden of HPV diseases in Spain: implication of additional 5 types from the 9-valent vaccine. Infect Agent Cancer 2018, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- Glińska, P.; Macios, A.; Jaworski, R.; Bobinski, M.; Pruski, D.; Przybylski, M.; Zielinska, A.; Sawicki, W.; Nowakowski, A. Baseline data on distribution of human papillomavirus (HPV) genotypes in cervical samples of gynecological patients before implementation of population-based HPV vaccination program in Poland. Ginekol Pol. 2024, 95(11), 870–878. [Google Scholar] [CrossRef]
- Bardin, A.; Vaccarella, S.; Clifford, G.M.; Lissowska, J.; Rekosz, M.; Bobkiewicz, P.; Kupryjańczyk, J.; Krynicki, R.; Jonska-Gmyrek, J.; Danska-Bidzinska, A.; Snijders, P.J.; Meijer, C.J.; Zatonski, W.; Franceschi, S. Human papillomavirus infection in women with and without cervical cancer in Warsaw, Poland. Eur J Cancer 2008, 44(4), 557–64. [Google Scholar] [CrossRef]
- Szostek, S.; Klimek, M.; Zawilinska, B.; Kosz-Vnenchak, M. Genotype-specific human papillomavirus detection in cervical smears. Acta Biochim Pol. 2008, 55(4), 687–92. [Google Scholar] [CrossRef]
- Bebyn, M.G.; Śledzińska, P.; Wojtysiak, J.; Jóźwicki, W.; Mierzwa, T.; Dziedzic, J.; Kowalewski, J.; Lewandowska, M. HPV RNA and DNA testing in Polish women screened for cervical cancer - A single oncological center study. Eur J Obstet Gynecol Reprod Biol. 2022, 268, 129–134. [Google Scholar] [CrossRef]
- Kiwerska, K.; Jozefiak, A.; Markowska, J.; Kedzia, W.; Jackowska, J.; Wierzbicka, M. Oral-genital human papillomavirus infection in Polish couples: frequent detection of HPV 42. BMC Infect Dis. 2019, 9(1), 122. [Google Scholar] [CrossRef] [PubMed]
- Nowakowski, A.; de Souza, S.C.; Jach, R.; Rosillon, D.; Książek, A.; Holl, K. HPV-type distribution and reproducibility of histological diagnosis in cervical neoplasia in Poland. Pathol Oncol Res. 2015, 21(3), 703–11. [Google Scholar] [CrossRef]
- Liss, J.; Łukaszuk, K.; Gulczyński, J.; Zwaliński, M.; Woźniak, I.; Emerich, J.; Wójcikowski, Cz. Występowanie DNA wirusa HPV u pacjentek z rakiem szyjki macicy w regionie gdańskim. Ginekol Pol. 2002, 73(9), 740–745. [Google Scholar] [PubMed]

Table 1.
Regional Distribution and Prevalence of High-Risk HPV Genotypes in the General Female Population Without Cervical Abnormalities in Poland.
Table 1.
Regional Distribution and Prevalence of High-Risk HPV Genotypes in the General Female Population Without Cervical Abnormalities in Poland.
| Authors [year of publication] | Cohort | Geagraphical region | Material |
Method of HPV detection |
hrHPV frequency |
|---|---|---|---|---|---|
| Glińska et al. [2024] [24] |
11 151 woman gynecological tested between 2018 - 2021 |
556 sites across Poland located all over the country in all 16 voivodeshipes | Cervical cytology material |
Amplisens HPV HCR genotype –titre FRT PCR KITand Alinity m HR HPV Assay/Abbot, BD OncoclarityLinear Array HPV Genotyping Test, Roche; Ampliquality HPV-type express v. 3.0, AB Analitica; Inno-LIPA Genotyping Extra II, Fuji Rebio |
General population: 4351 (50.9%) HPV positive: HPV16 - 31.3% HPV31 - 14.7% HPV66 - 14.7% HPV51 – 13.0%, HPV56 - 11.0% HPV52 - 10.1% HPV39 - 8.3% HPV18 - 7.4% HPV18 -7.4%, HPV58 - 7.2%, HPV59 - 6.8% HPV45 - 6.4% HPV33 - 6.0% HPV68 - 4.6% HPV35 - 2.6% |
| Baradin et al. [2008] [25] | 834 woman from general population |
Warsaw region |
Exfoliated cervical cells and cervical cancer biopsy |
HPV DNA Immunoassay with oligoprobe cocktails, detection of 44 HPV genotypes |
General population: 138 (16.6%) hrHPV positive HPV16 - 22.5% HPV56 - 10.1% HPV45 - 9.4% HPV31 - 8.7%, HPV52 - 8.7% HPV33 - 6.5% HPV58 - 5.1% HPV18 - 4.3%, HPV73 - 4.3%, HPV35 - 2.2% HPV39 - 2.2% HPV59 - 2.2% HPV68 - 2.2% HPV82 - 2.2% |
| Szostek et al. [2008] [26] | 42woman without abnormality in cytology |
Krakow region |
Cervical cytology material | INNO-LiPA HPV Genotyping |
Normal cytology population: 9 (21.0%) hrHPV: HPV51 - 55.6% HPV52 - 22.2% HPV45 - 11.1% HPV56 - 11.1% HPV66 - 11.1% |
Table 2.
Regional Distribution and Prevalence of High-Risk HPV Genotypes among women with abnormal cytology across different regions of Poland.
Table 2.
Regional Distribution and Prevalence of High-Risk HPV Genotypes among women with abnormal cytology across different regions of Poland.
|
Authors [year of publication] |
Cohort | Geagraphical region | Material |
Method of HPV detection |
hrHPV frequency |
|---|---|---|---|---|---|
| Bebyn et al. (2022) [27] |
1840 most with abnormal cytology LSIL, HSIL,ASC-US, ASC-H, AGC |
Bydgoszcz region |
Cervical cytology material |
mRNA analysis NucliSENS EasyQ HPV (detection of five HPV genotypes) |
General population: 198 (36.3%) HPV RNA positive HPV16 - 48.0% HPV18 - 12.6%, HPV31 - 10.1%, HPV33 - 8.6%, HPV45 - 4.5% More than one HPV type – 16.2% |
| Kiwerska et al. (2019) [28] |
197 females with cervical pathology, including cancer 2014-2016 |
Warsaw and Poznan regions |
Cervical cytology material | AnyplexTM IIHPV28 Detection system, Segene |
General population: 197 (100.0%) HPV positive: HPV16 - 35.5% HPV31 - 12.7% HPV42 – 10.2% HPV39 - 9.1% HPV54 – 8.1%, HPV18 - 7.1% HPV33 - 6.6% HPV53 - 6.6% HPV35 - 6.1% HPV66 - 5.1%, HPV56 - 4.7% HPV51 - 4.1% HPV68 - 4.1% HPV58 - 2.5% HPV59 - 2.5% HPV45 - 1.5% HPV52 – 0.5% |
| Nowakowski et al. (2014) [29] | 205 woman with HG-CIN and 193 ICC between 2001 - 2008 |
Lublin and Krakow regions |
FFPE | SPF10-DEIAliPA25-polymerase chain reaction (PCR) system |
HG-CIN poplutaion: : 197 (96.1%) hrHPV positive: HPV16 - 62.8% HPV33 - 7.8% HPV31 - 6.6% HPV52 - 3.7% HPV45 - 2.6% HPV58 - 2.6% |
| Szostek et al. (2008) [26] | 125 woman with LSIL (n=44), HSIL (n=12) |
Krakow region |
Cervical cytology material | INNO-LiPA HPV Genotyping |
L-SIL population: 43 (98.0%) hrHPV: HPV51 - 30.2% HPV52 - 25.6% HPV18 - 11.6% HPV31 - 11.6% HPV16 - 9.3% HPV33 – 7.0% HPV58 - 7.0% HPV66 – 7.0% HPV56 - 4.6% HPV35 - 2.3% HPV39 - 2.3% H-SIL population: 11 (92.0%) hrHPV: HPV16 - 63.6% HPV51 – 27.3% HPV18 - 18.2% HPV31 – 9.1% |
Table 3.
The prevalence and genotype distribution of Human papillomavirus in women with invasive cervical cancer across different regions of Poland.
Table 3.
The prevalence and genotype distribution of Human papillomavirus in women with invasive cervical cancer across different regions of Poland.
| Authors [year of publication] | Cohort | Geagraphical region | Material | Method of HPV detection | hrHPV frequency |
|---|---|---|---|---|---|
| Nowakowski et al. (2014) [29] |
193 pts with ICC 2001 - 2008 |
Lublin and Krakow regions |
FFPE | SPF10-DEIAliPA25-polymerase chain reaction (PCR) system |
176 (91.2%) hrHPV positive pts: HPV16 - 72.1% HPV18 - 10.8% HPV33 - 5.7% HPV45 - 3.4% |
| Baradin et al. [2008] [25] |
88 pts with ICC |
Warsaw region |
Exfoliated cervical cells and cervical cancer biopsy |
HPV DNA Immunoassay with oligoprobe cocktails, detection of 44 HPV genotypes |
87 (98.8%) hrHPV positive pts : HPV16 - 74.7% HPV18 - 5.7%, HPV45 - 5.7% HPV31 - 3.4%, HPV52 – 3.4% HPV56 – 3.4% |
| Szostek et al. [2008] [26] |
27 pts with ICC |
Southern Poland |
Cervical cytology material | INNO-LiPA HPV Genotyping |
27 (100.0%) hrHPV positive pts HPV16 - 81.4% HPV51 - 14.8% HPV18 - 11.1% HPV66 – 11.1% HPV45 – 2.2% HPV68 – 2.2% |
| Liss et al. (2002) [30] |
107 pts with ICC 1997 - 1998 |
Gdańsk region |
Cervical cytology material | DNA PCR |
75 (70.1%) hrHPV positive pts: HPV16 - 88.0% HPV31 - 4.0%, HPV33 - 4.0% HPV45 - 1.3%, HPV52 – 1.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



