Submitted:
12 May 2026
Posted:
13 May 2026
You are already at the latest version
Abstract
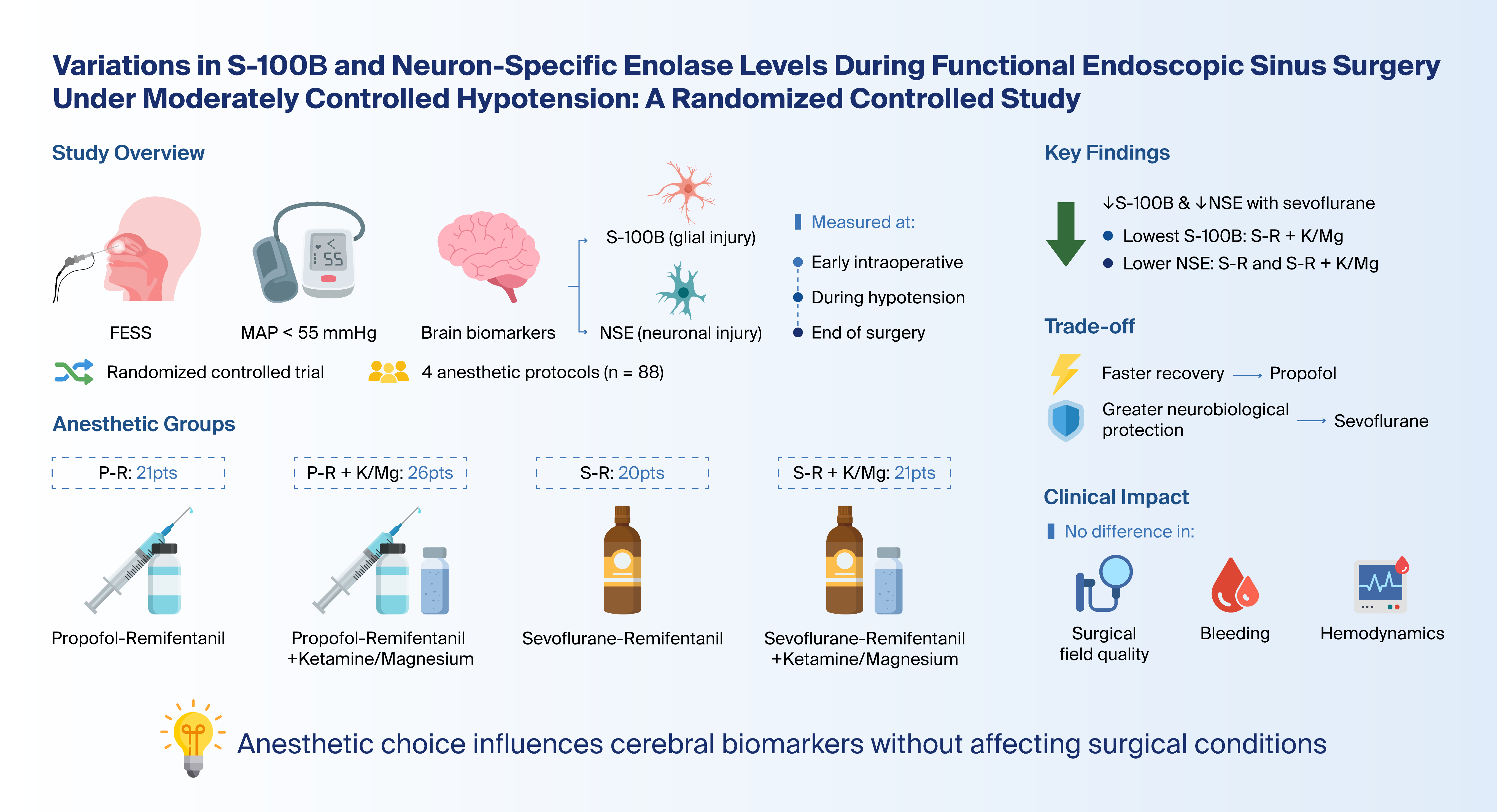
Background and Objectives: Controlled hypotension during functional endoscopic sinus surgery (FESS) improves surgical field visibility but may pose a risk of subclinical cerebral hypoperfusion. Serum S100Β and neuron‑specific enolase (NSE) are established biomarkers of glial and neuronal injury and may reflect perioperative neuroprotection associated with different anesthetic regimens. This study evaluated the effect of four anesthetic protocols on perioperative brain biomarker release during FESS. Materials and Methods: In this single‑center, randomized, controlled trial, 88 adult patients (ASA I–III) undergoing FESS under moderately controlled hypotension (mean arterial pressure <55 mmHg) were allocated to one of four groups: propofol–remifentanil, propofol–remifentanil with ketamine–magnesium, sevoflurane–remifentanil, or sevoflurane–remifentanil with ketamine–magnesium. Serum S100Β and NSE concentrations were measured at three timepoints: early intraoperatively, during hypotension, and at the end of surgery. Biomarker data were analyzed using nested ANOVA and linear mixed‑effects models adjusted for relevant covariates. Secondary outcomes included recovery characteristics, surgical field quality, bleeding scores, and perioperative hemodynamics. Results: Baseline demographic and perioperative characteristics were comparable across groups. The group receiving sevoflurane–remifentanil combined with ketamine–magnesium showed the lowest S100B levels (p=0.01 compared to the propofol–remifentanil group; p=0.04 compared to the sevoflurane–remifentanil group). Additionally, NSE concentrations were markedly lower in both sevoflurane groups (sevoflurane–remifentanil and sevoflurane–remifentanil plus ketamine–magnesium) compared to the propofol–remifentanil group (p=0.003 and p=0.007, respectively). No intergroup differences were observed at baseline and surgical field quality, bleeding, and hemodynamic parameters did not differ significantly among groups. Recovery and extubation times were shortest with propofol–remifentanil, whereas ketamine–magnesium prolonged emergence. Conclusions: Anesthetic technique significantly influences perioperative brain biomarker release during FESS. Sevoflurane‑based regimens, with or without ketamine–magnesium, demonstrate more favorable neurobiological profiles under controlled hypotension, although propofol‑based anesthesia offers faster recovery.
Keywords:
functional endoscopic sinus surgery
; controlled hypotension
; anesthesia techniques
; sevoflurane
; propofol
; ketamine
; magnesium sulfate
; S-100Β
; neuron-specific enolase
; neuroprotection
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



