Submitted:
03 April 2026
Posted:
07 April 2026
You are already at the latest version
Abstract
Background: Humanity faces an unprecedented crisis of suffering. Global mental health data reveal that mental disorders affect over 1 billion people worldwide, with depression, anxiety, and post-traumatic stress disorder (PTSD) representing the leading causes of disability. Conflict-affected populations experience PTSD prevalence rates exceeding 30%, while adverse childhood experiences (ACEs) create intergenerational cycles of trauma affecting billions. Despite advances in neuroscience, psychology, and contemplative traditions, these disciplines remain fragmented, limiting our capacity to address suffering at scale. Objective: This paper presents a comprehensive framework for understanding where and why people suffer globally, and establishes evidence-based protocols for transitioning from shadow states of consciousness to Fundamental Peace. Drawing on the Shadow-Gift-Essence (S-G-E) framework, Hawkins’ Map of Consciousness, Internal Family Systems (IFS), polyvagal theory, and global epidemiological data, we propose an integrative model that bridges ancient wisdom and modern science. Methods: We synthesized evidence from: (1) Global Burden of Disease (GBD) studies and WHO World Mental Health surveys documenting the epidemiology of suffering; (2) neuroscientific research on trauma, consciousness, and healing; (3) contemplative neuroscience examining meditation, hypnotherapy, and altered states of consciousness; (4) Prof. Gallardo’s published work on hypnosis, shadow work, consciousness elevation, and the Integrative Transformation Model (ITM). Framework: We present the Global Pain and Trauma Map (GPTM), an original seven-domain taxonomy of human suffering spanning Individual/Psychological, Relational/Social, Collective/Cultural, Structural/Systemic, Existential/Spiritual, Somatic/Biological, and Environmental/Planetary dimensions. Each domain is calibrated using Hawkins’ consciousness levels (20-1000 scale) and mapped to specific neurobiological mechanisms. We then detail evidence-based protocols for healing, including the S-G-E process, hypnotherapy and altered states of consciousness, the Meta Pets system, contemplative practices, community healing, and policy interventions. Conclusions: The global crisis of suffering is fundamentally a crisis of consciousness operating at shadow levels (shame-20 through pride-175 on Hawkins’ scale). Healing requires systematic elevation through courage (200), acceptance (350), and love (500) toward Fundamental Peace (600+). This transition is achievable through integrated protocols targeting seven shared neurobiological mechanisms: default mode network suppression, autonomic nervous system regulation, neuroplasticity enhancement, memory reconsolidation, interoceptive predictive coding, theta/alpha brainwave entrainment, and ego dissolution. Implementation requires coordinated action across individual, institutional, and planetary scales. We conclude with a research agenda for the next decade and a call for a global healing movement.
Keywords:
trauma
; consciousness
; shadow work
; fundamental peace
; global burden of disease
; PTSD
; hypnotherapy
; meditation
; Hawkins map of consciousness
; integrative transformation model
1. Introduction: The Global Crisis of Suffering
1.1. Why This Paper Is Needed Now
We stand at a critical juncture in human history. The World Health Organization estimates that mental disorders affect more than 1 billion people globally, with depression and anxiety alone accounting for over 300 million cases each (Ferrari et al., 2024). Post-traumatic stress disorder (PTSD) affects approximately 3.9% of the global population, with rates exceeding 30% in conflict-affected regions (Charlson et al., 2019; Hoppen et al., 2021). The Global Burden of Disease Study 2021 reveals that mental disorders constitute the leading cause of years lived with disability (YLDs) worldwide, surpassing cardiovascular disease and cancer (Fan et al., 2025).
Yet these statistics, staggering as they are, capture only the visible surface of human suffering. Beneath clinical diagnoses lies a vast ocean of unacknowledged pain: the shame that silences survivors of childhood sexual abuse, the grief of parents who have lost children to violence, the existential despair of those who have lost meaning and purpose, the intergenerational trauma carried in the bodies of descendants of genocide and slavery, and the collective anxiety of a species confronting ecological collapse (Liu et al., 2025; Benjet et al., 2016).
This paper argues that the fragmentation of our healing traditions—the separation of psychology from spirituality, neuroscience from contemplative practice, individual therapy from collective healing—has limited our capacity to address suffering at the scale and depth required. What is needed is an integrative framework that honors both the empirical rigor of modern science and the experiential wisdom of ancient traditions, that maps the full spectrum of human suffering across individual, relational, collective, and planetary dimensions, and that provides evidence-based protocols for systematic transformation (Gallardo & Chetri, 2026).
1.2. The Shadow-to-Peace Continuum
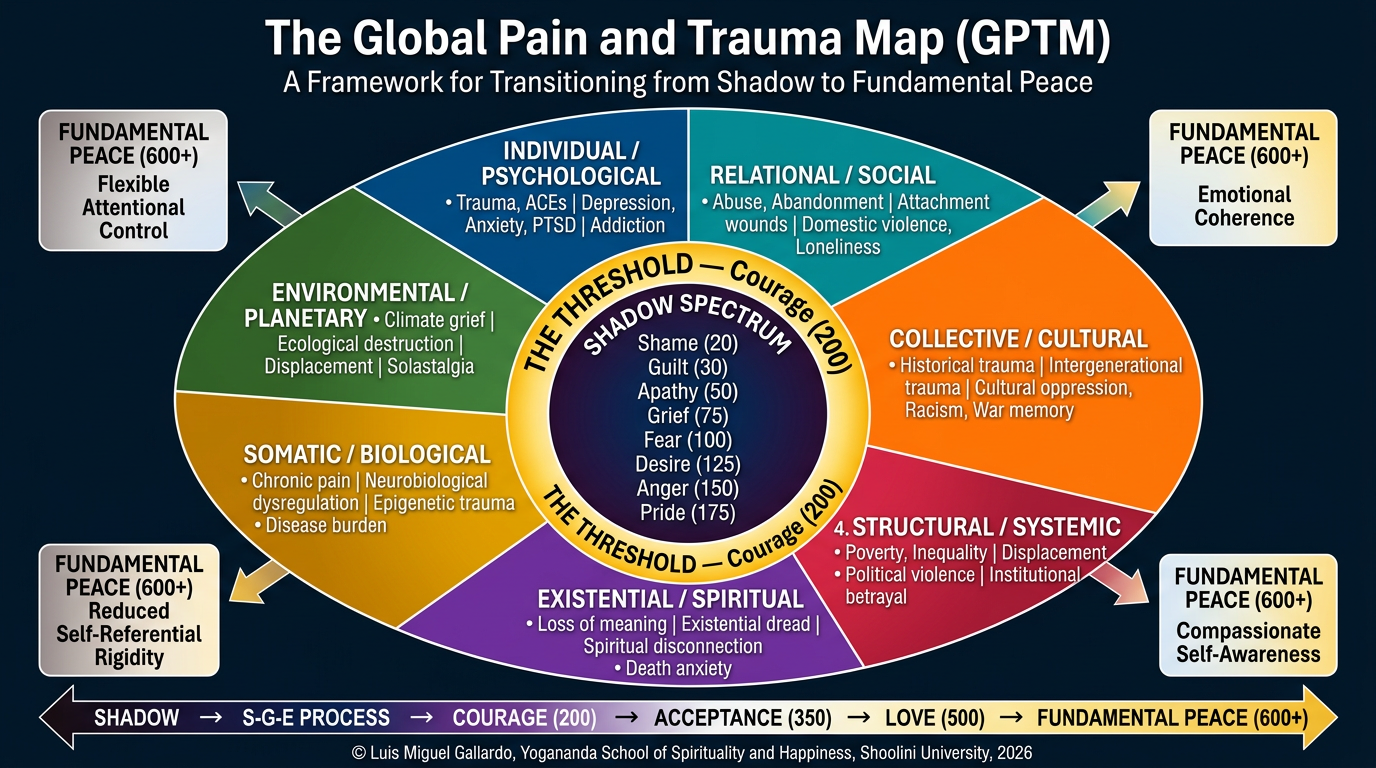
At the heart of this framework lies a simple yet profound insight: human suffering exists on a continuum of consciousness. Drawing on David Hawkins’ Map of Consciousness (Hawkins, 1995, 2012), we recognize that emotions and states of being can be calibrated on a logarithmic scale from 1 to 1,000. The lower levels—shame (20), guilt (30), apathy (50), grief (75), fear (100), desire (125), anger (150), and pride (175)—represent what we call the “shadow spectrum.” These are states characterized by contraction, separation, and suffering.
The critical threshold occurs at courage (200), where individuals begin to take responsibility for their experience and engage with life proactively rather than reactively. Above this level, consciousness expands through neutrality (250), willingness (310), acceptance (350), reason (400), love (500), joy (540), peace (600), and ultimately enlightenment (700-1000).
The journey from shadow to peace is not merely a philosophical aspiration—it is a neurobiologically grounded process that can be systematically cultivated through specific practices and interventions. This paper presents that roadmap.
1.3. Structure and Scope
This paper proceeds in nine sections. Section 2 maps the global epidemiology of pain and trauma using WHO and GBD data. Section 3 presents a seven-domain taxonomy of human suffering. Section 4 explores the architecture of the shadow, integrating Jungian psychology, IFS, trauma theory, and Hawkins’ consciousness levels. Section 5 introduces the Global Pain and Trauma Map (GPTM), an original framework by Prof. Gallardo. Section 6 details evidence-based protocols for healing, including the S-G-E process, hypnotherapy, the Meta Pets system, and contemplative practices. Section 7 defines Fundamental Peace scientifically, examining its neuroscience and cross-cultural dimensions. Section 8 outlines an implementation framework from individual to planetary scales. Section 9 proposes a research agenda for the next decade. Section 10 concludes with a call to action for a global healing movement.
2. Global Epidemiology of Pain and Trauma
2.1. The Mental Health Burden: Global Statistics
The Global Burden of Disease Study 2021 provides the most comprehensive assessment of mental health worldwide. Mental disorders affected 1.02 billion people in 2021, representing 13.1% of the global population (Fan et al., 2025). Depression alone affected 279.6 million people (3.8% prevalence), anxiety disorders 301.4 million (4.1%), and PTSD 71.3 million (0.9%). These conditions collectively accounted for 125.3 million disability-adjusted life years (DALYs), making mental disorders the fifth leading cause of disease burden globally (Ferrari et al., 2024).
The burden is not distributed equally. Low- and middle-income countries (LMICs) bear 75% of the global mental health burden but possess only 10% of mental health resources (Mubarak et al., 2024). Women experience depression at nearly twice the rate of men (5.1% vs. 2.8%), with the highest burden occurring during reproductive years (Cheng et al., 2025). Young people under 24 years face escalating rates of anxiety, depression, and self-harm, with projections suggesting continued increases through 2050 (Liu et al., 2025).
2.2. Trauma Exposure and PTSD: A Global Perspective
The WHO World Mental Health Surveys, spanning 24 countries and over 68,000 respondents, reveal that 70.4% of adults have experienced at least one traumatic event in their lifetime (Benjet et al., 2016; Kessler et al., 2017). The most common traumas include unexpected death of a loved one (31.4%), witnessing death or serious injury (22.8%), and experiencing life-threatening accidents (18.8%). Sexual violence affects 4.9% of women globally, with rates exceeding 10% in some regions (Benjet et al., 2016).
Conditional PTSD risk—the probability of developing PTSD following trauma exposure—varies dramatically by trauma type. Rape carries the highest risk (19.0% for women, 10.7% for men), followed by childhood physical abuse (12.2%), combat exposure (8.6%), and natural disasters (3.8%) (Kessler et al., 2017). These statistics underscore a critical insight: trauma is nearly universal, but PTSD develops when the nervous system becomes dysregulated and the traumatic memory fails to integrate (van der Kolk, 2014; Porges, 2011).
2.3. Conflict-Affected Populations: The Epicenter of Suffering
Armed conflict creates concentrated zones of extreme suffering. A meta-analysis of 129 studies across 39 conflict-affected countries found PTSD prevalence of 15.3% and major depression prevalence of 17.3%—rates three to four times higher than global averages (Charlson et al., 2019). In active war zones, rates exceed 30% (Hoppen et al., 2021).
Between 1989 and 2019, an estimated 1.45 billion people lived in conflict-affected countries. Of these, approximately 354 million adults experienced PTSD and 392 million experienced major depression (Hoppen et al., 2019). These numbers represent not just clinical diagnoses but shattered lives, disrupted childhoods, and communities torn apart by violence. The mental health consequences of conflict extend across generations through epigenetic mechanisms and intergenerational trauma transmission (Yehuda & Lehrner, 2018).
2.4. Adverse Childhood Experiences (ACEs): The Roots of Suffering
The Adverse Childhood Experiences (ACE) Study, one of the largest investigations of childhood abuse and neglect ever conducted, revealed that 64% of adults experienced at least one ACE, and 12.5% experienced four or more (Felitti et al., 1998). ACEs include physical, emotional, and sexual abuse; physical and emotional neglect; and household dysfunction (parental substance abuse, mental illness, domestic violence, incarceration, or separation/divorce).
The dose-response relationship between ACEs and adult health outcomes is striking. Individuals with four or more ACEs have a 4-12 fold increased risk of alcoholism, drug abuse, depression, and suicide attempts, a 2-4 fold increase in smoking, poor self-rated health, and sexually transmitted diseases, and a 1.4-1.6 fold increase in physical inactivity and severe obesity (Felitti et al., 1998). A recent cross-national analysis of 22 countries found that childhood adversity predicts adult suffering across cultures, with effects mediated by attachment insecurity, emotion dysregulation, and maladaptive coping (Cowden et al., 2025).
2.5. The Hidden Epidemics: Shame, Grief, and Existential Distress
Clinical epidemiology captures diagnosed disorders but misses vast domains of suffering that do not meet diagnostic thresholds. Shame—the feeling of being fundamentally flawed or unworthy—operates as a silent epidemic, particularly among survivors of sexual abuse, individuals with stigmatized identities, and those living in cultures emphasizing honor and face-saving (Brown, 2006). Shame calibrates at 20 on Hawkins’ scale, the lowest level of consciousness, and is associated with suicidality, addiction, and profound disconnection from self and others (Hawkins, 2012).
Grief, calibrating at 75, affects virtually every human being yet receives minimal attention in public health frameworks. The COVID-19 pandemic alone created over 10 million orphans globally, each carrying the weight of loss (Hillis et al., 2021). Complicated grief, where the bereaved cannot integrate the loss, affects 7-10% of mourners and is associated with increased mortality, substance abuse, and suicide (Shear, 2015).
Existential distress—the suffering that arises from confronting mortality, meaninglessness, isolation, and freedom—remains largely invisible to conventional mental health systems despite its profound impact on quality of life (Yalom, 1980). This form of suffering becomes particularly acute in late life, in the face of terminal illness, and during periods of rapid social change when traditional meaning-making structures collapse (Kissane, 2012).
2.6. Structural and Systemic Sources of Suffering
Suffering is not only individual but structural. Poverty, discrimination, oppression, and violence are embedded in social, economic, and political systems that systematically harm certain populations while privileging others (Sabariego et al., 2017). The social determinants of mental health—income inequality, educational access, employment conditions, housing stability, food security, and exposure to discrimination—account for a substantial portion of the global mental health burden (Lund et al., 2018).
Structural violence—the harm caused by social structures that prevent individuals from meeting their basic needs—operates invisibly yet lethally. An estimated 18 million people die annually from poverty-related causes, a death toll exceeding all wars, genocides, and homicides combined (Farmer, 2004). These deaths represent the shadow side of global economic systems that concentrate wealth and power while externalizing suffering onto the most vulnerable.
2.7. Environmental and Planetary Suffering
Finally, we must acknowledge a dimension of suffering that transcends individual and collective human experience: the suffering of the Earth itself and the psychological distress arising from ecological destruction. Climate anxiety, eco-grief, and solastalgia (distress caused by environmental change) are emerging as significant mental health concerns, particularly among young people (Hickman et al., 2021). The recognition that human activity is driving the sixth mass extinction and destabilizing planetary systems creates a form of existential dread that previous generations did not face (Albrecht, 2019).
This brief epidemiological overview reveals the scope and scale of global suffering. The question that follows is: how do we make sense of this vast landscape of pain? The next section presents a taxonomy that organizes suffering into seven domains, providing a framework for both understanding and intervention.
3. A Taxonomy of Human Suffering: Seven Domains
To address suffering systematically, we must first map its territory. This section presents a seven-domain taxonomy that organizes the sources and manifestations of human pain across individual, relational, collective, and planetary scales. This taxonomy forms the foundation of the Global Pain and Trauma Map (GPTM) presented in Section 5.
3.1. Domain 1: Individual/Psychological Suffering
Individual psychological suffering encompasses the internal experiences of distress that arise from thoughts, emotions, memories, and self-perceptions. This domain includes:
Clinical mental disorders: Depression, anxiety disorders, PTSD, obsessive-compulsive disorder (OCD), eating disorders, personality disorders, and psychotic disorders. These conditions involve dysregulation of mood, cognition, perception, and behavior that cause significant distress and functional impairment (American Psychiatric Association, 2013).
Trauma and traumatic memory: Unprocessed traumatic experiences stored in implicit memory systems, manifesting as intrusive thoughts, flashbacks, nightmares, hypervigilance, and emotional numbing (van der Kolk, 2014). Trauma fragments the self and disrupts the capacity for integration and coherence (Siegel, 2012).
Shadow material: In Jungian terms, the shadow consists of aspects of the self that have been disowned, repressed, or denied—typically because they were deemed unacceptable by family, culture, or society (Jung, 1959). Shadow material includes not only “negative” qualities (anger, jealousy, selfishness) but also positive potentials that were suppressed (creativity, assertiveness, sexuality). The shadow operates unconsciously, driving behavior through projection, reactivity, and self-sabotage (Gallardo, 2025a).
Shame and guilt: Shame (the belief “I am bad”) and guilt (the belief “I did something bad”) represent core wounds that undermine self-worth and generate chronic suffering (Brown, 2006). Shame calibrates at 20 on Hawkins’ scale and is associated with suicidality, addiction, and profound isolation (Hawkins, 2012).
Existential suffering: Anxiety arising from confronting the fundamental givens of existence—death, meaninglessness, isolation, and freedom (Yalom, 1980). This suffering intensifies during life transitions, loss, and when cultural meaning-making systems fail to provide adequate answers to existential questions (Frankl, 1959).
3.2. Domain 2: Relational/Social Suffering
Humans are fundamentally relational beings. Much of our suffering arises from disruptions in attachment, belonging, and connection. This domain includes:
Attachment trauma: Disruptions in early caregiver-child relationships that create insecure attachment patterns (anxious, avoidant, disorganized), leading to difficulties with trust, intimacy, and emotional regulation throughout life (Bowlby, 1988; Ainsworth et al., 1978). Disorganized attachment, arising from frightening or frightened caregivers, is particularly damaging and predicts dissociation, borderline personality features, and complex PTSD (Liotti, 2004).
Interpersonal violence: Physical, sexual, and emotional abuse within intimate relationships, affecting an estimated 1 in 3 women globally (WHO, 2021). Intimate partner violence creates a context of chronic fear, shame, and powerlessness that profoundly damages mental health (Campbell, 2002).
Betrayal and abandonment: The pain of broken trust, rejection, and loss of significant relationships. Betrayal trauma theory suggests that traumas perpetrated by those we depend on for survival (parents, partners, institutions) are particularly damaging because they violate the attachment system itself (Freyd, 1996).
Social isolation and loneliness: The subjective experience of inadequate social connection, which has been identified as a major public health crisis associated with increased mortality risk equivalent to smoking 15 cigarettes per day (Holt-Lunstad et al., 2015). Loneliness calibrates at grief (75) and apathy (50) levels and is epidemic in modern societies (Cacioppo & Patrick, 2008).
Bullying and social exclusion: Systematic harassment, humiliation, and exclusion, particularly during childhood and adolescence, which creates lasting psychological wounds and increases risk for depression, anxiety, and suicide (Liu et al., 2025).
3.3. Domain 3: Collective/Cultural Suffering
Suffering is not only individual but collective. Groups, communities, and entire cultures carry wounds that shape the experience of their members. This domain includes:
Collective trauma: Traumatic events that affect entire communities or populations—wars, genocides, natural disasters, pandemics, terrorist attacks—creating shared wounds that persist across generations (Hirschberger, 2018). Examples include the Holocaust, the transatlantic slave trade, the Rwandan genocide, and the COVID-19 pandemic.
Intergenerational trauma: The transmission of trauma effects from survivors to their descendants through biological (epigenetic), psychological (attachment and parenting), and social (cultural narratives) mechanisms (Yehuda & Lehrner, 2018). Studies of Holocaust survivors’ children and grandchildren demonstrate measurable effects on stress physiology, mental health, and worldview (Kellermann, 2013).
Cultural trauma: Events that shatter the collective identity and meaning-making systems of a group, requiring cultural reconstruction (Alexander, 2004). The colonization of indigenous peoples, for example, destroyed not only lives but entire ways of being, knowing, and relating to the world (Brave Heart & DeBruyn, 1998).
Historical trauma: The cumulative emotional and psychological wounding across generations resulting from massive group trauma experiences (Brave Heart, 2003). Native American communities, for instance, continue to experience elevated rates of substance abuse, suicide, and domestic violence as manifestations of unresolved historical trauma from genocide, forced relocation, and cultural destruction (Whitbeck et al., 2004).
Moral injury: The psychological distress resulting from actions, or the witnessing of actions, that violate one’s moral code (Litz et al., 2009). Common among combat veterans, healthcare workers, and others who face impossible moral dilemmas, moral injury involves guilt, shame, and a sense of betrayal by authorities or institutions (Shay, 1994).
3.4. Domain 4: Structural/Systemic Suffering
Suffering is embedded in social, economic, and political structures that systematically harm certain populations. This domain includes:
Poverty and economic inequality: Material deprivation and the chronic stress of financial insecurity, which are strongly associated with mental health problems across the lifespan (Lund et al., 2018). The relationship is bidirectional: poverty increases risk for mental disorders, and mental disorders increase risk for poverty, creating vicious cycles (Patel & Kleinman, 2003).
Discrimination and oppression: Systematic mistreatment based on race, ethnicity, gender, sexual orientation, religion, disability, or other marginalized identities. Discrimination operates as a chronic stressor that damages mental and physical health through multiple pathways, including direct victimization, vigilance and anticipation of discrimination, and internalized oppression (Williams & Mohammed, 2013).
Structural violence: The harm caused by social structures that prevent individuals from meeting their basic needs—hunger, preventable disease, lack of education, homelessness (Farmer, 2004). Structural violence is often invisible because it is normalized within existing systems, yet it causes immense suffering and premature death (Galtung, 1969).
Institutional betrayal: Harm perpetrated by trusted institutions (schools, churches, military, healthcare systems) through action or inaction, which compounds the trauma of the original harm and undermines trust in social systems (Smith & Freyd, 2014). Examples include institutional cover-ups of sexual abuse, medical experimentation on vulnerable populations, and denial of benefits to veterans.
Mass incarceration and criminal justice trauma: The United States incarcerates over 2 million people, disproportionately affecting Black and Latino communities. Incarceration causes profound psychological harm, disrupts families, and perpetuates cycles of poverty and trauma (Alexander, 2010). The criminal justice system itself often retraumatizes survivors of violence through adversarial processes that prioritize punishment over healing (Herman, 2005).
3.5. Domain 5: Existential/Spiritual Suffering
This domain addresses suffering that arises from confronting the ultimate concerns of human existence and from disconnection from meaning, purpose, and the sacred. It includes:
Existential anxiety: Dread arising from awareness of death, meaninglessness, isolation, and freedom (Yalom, 1980). While existential anxiety is a universal human experience, it becomes pathological when individuals lack resources to metabolize these concerns into wisdom and acceptance (Tillich, 1952).
Loss of meaning and purpose: The suffering that arises when life feels empty, pointless, or absurd. Viktor Frankl identified “existential vacuum” as a primary source of modern suffering, arguing that humans can endure almost any suffering if they can find meaning in it (Frankl, 1959). Loss of meaning calibrates at apathy (50) on Hawkins’ scale.
Spiritual crisis: Periods of profound questioning, doubt, or disillusionment with previously held beliefs, often triggered by trauma, loss, or mystical experiences that cannot be integrated (Grof & Grof, 1989). Spiritual emergencies, when handled skillfully, can lead to transformation, but when misunderstood or pathologized, they cause immense suffering (Lukoff, 1985).
Disconnection from the sacred: The loss of connection to something larger than oneself—whether conceived as God, nature, the cosmos, or the interconnected web of life. This disconnection, characteristic of modern secular societies, leaves individuals without access to transcendent sources of meaning, comfort, and guidance (Taylor, 2007).
Fear of death: Terror of annihilation and non-existence, which Becker (1973) argued is the primary driver of human behavior and culture. Death anxiety underlies much psychological suffering and motivates defensive strategies (denial, distraction, symbolic immortality projects) that create additional problems (Yalom, 2008).
3.6. Domain 6: Somatic/Biological Suffering
The body is not separate from the mind; suffering is embodied. This domain includes:
Chronic pain: Persistent pain lasting more than three months, affecting over 1.5 billion people globally (Goldberg & McGee, 2011). Chronic pain involves complex interactions between nociceptive signals, central sensitization, emotional distress, and meaning-making (Melzack & Wall, 1965). Pain and suffering, while related, are distinct: suffering arises when pain is perceived as meaningless, uncontrollable, or endless (Cassell, 1982).
Trauma stored in the body: Traumatic experiences are encoded not only in explicit memory but in the body’s sensorimotor systems, manifesting as chronic muscle tension, dysregulated breathing, digestive problems, and autonomic nervous system dysregulation (van der Kolk, 2014; Levine, 1997). Somatic approaches to trauma recognize that healing must include the body, not just the mind (Ogden et al., 2006).
Nervous system dysregulation: Chronic activation of the sympathetic nervous system (fight-or-flight) or dorsal vagal shutdown (freeze, collapse) in the absence of actual threat, characteristic of PTSD and complex trauma (Porges, 2011). Polyvagal theory explains how trauma disrupts the social engagement system and leaves individuals oscillating between hyperarousal and hypoarousal (Porges, 2017).
Chronic illness and disability: The suffering associated with living with persistent health conditions, pain, and functional limitations. Chronic illness often involves loss of identity, social roles, and future possibilities, creating existential as well as physical suffering (Charmaz, 1983).
Addiction and substance use disorders: Compulsive engagement with substances or behaviors despite negative consequences, often representing attempts to self-medicate underlying trauma, pain, or emptiness (Maté, 2008). Addiction calibrates at desire (125) and fear (100) levels and involves hijacking of the brain’s reward systems (Volkow et al., 2016).
3.7. Domain 7: Environmental/Planetary Suffering
Finally, we must acknowledge suffering that arises from our relationship with the natural world and the ecological crisis. This domain includes:
Climate anxiety and eco-grief: Psychological distress related to climate change, including worry about the future, grief over environmental losses, and feelings of helplessness (Hickman et al., 2021). A global survey of 10,000 young people found that 59% were very or extremely worried about climate change, and 45% said climate anxiety affected their daily functioning (Hickman et al., 2021).
Solastalgia: Distress caused by environmental change in one’s home environment, a form of homesickness experienced while still at home (Albrecht, 2019). Indigenous communities facing loss of traditional lands, farmers experiencing drought, and coastal residents watching sea-level rise all experience solastalgia.
Ecological grief: Mourning the loss of species, ecosystems, and ways of life due to environmental destruction (Cunsolo & Ellis, 2018). This grief is often disenfranchised—not socially recognized or validated—making it particularly difficult to process (Doka, 1989).
Disconnection from nature: The psychological and spiritual costs of living in built environments with minimal contact with the natural world. Nature deficit disorder, while not a clinical diagnosis, describes the constellation of problems (attention difficulties, depression, anxiety, reduced creativity) associated with lack of nature exposure (Louv, 2005).
Planetary-scale existential dread: The recognition that human activity is destabilizing Earth systems and driving the sixth mass extinction, creating a form of existential threat that previous generations did not face (Scranton, 2015). This awareness can lead to despair, nihilism, or, alternatively, to profound commitment to healing and transformation (Macy & Johnstone, 2012).
3.8. Interconnections Across Domains
These seven domains are not separate but deeply interconnected. Individual psychological suffering often has roots in relational trauma, which itself may be embedded in collective historical trauma and structural oppression. Somatic symptoms may express unprocessed emotional pain. Existential despair may arise from disconnection from both human community and the natural world. Environmental destruction creates collective trauma that manifests in individual anxiety and grief.
Understanding these interconnections is essential for effective intervention. Treating individual symptoms without addressing relational, collective, structural, and environmental contexts will produce limited and temporary results. Conversely, addressing only structural issues without supporting individual healing leaves people without the inner resources to sustain social change. The framework presented in this paper integrates across all seven domains, recognizing that healing must occur simultaneously at multiple scales.
4. The Shadow: Understanding the Architecture of Suffering
4.1. The Shadow in Jungian Psychology
Carl Jung introduced the concept of the shadow to describe the aspects of the self that have been repressed, denied, or disowned—typically because they were deemed unacceptable by family, culture, or society (Jung, 1959). The shadow is not inherently negative; it contains both destructive impulses and positive potentials that were suppressed. A child who was punished for expressing anger may repress that emotion, creating a shadow that later erupts in passive-aggressive behavior or explosive rage. A child whose creativity was dismissed may bury that gift, living a constricted life while the creative shadow seeks expression through symptoms or dreams.
Jung emphasized that the shadow operates unconsciously, influencing behavior through projection (seeing in others what we deny in ourselves), reactivity (being triggered by others who embody our shadow qualities), and self-sabotage (unconsciously undermining our own goals because success would require owning disowned aspects of self) (Jung, 1968). The path to wholeness, Jung argued, requires making the unconscious conscious—bringing shadow material into awareness where it can be integrated rather than acted out (Jung, 1959).
4.2. Internal Family Systems: Parts and the Self
Richard Schwartz’s Internal Family Systems (IFS) model provides a contemporary framework for understanding the shadow that is highly compatible with Jungian thought (Schwartz, 1995). IFS proposes that the psyche is naturally multiple, composed of “parts”—subpersonalities with their own perspectives, emotions, and agendas. These parts organize into three categories:
Exiles: Young, vulnerable parts that carry the pain of past trauma, abuse, or neglect. Exiles hold feelings of shame, fear, grief, and worthlessness. They are called exiles because other parts work hard to keep them locked away, fearing that if their pain were felt, it would be overwhelming (Schwartz, 2001).
Managers: Proactive protector parts that try to maintain control and prevent exiles from being triggered. Managers use strategies like perfectionism, intellectualization, caretaking, and hypervigilance to keep the system safe (Schwartz, 1995).
Firefighters: Reactive protector parts that spring into action when exiles are activated despite managers’ efforts. Firefighters use emergency measures—substance abuse, binge eating, self-harm, dissociation, rage—to extinguish the pain as quickly as possible (Schwartz, 2001).
In IFS, the shadow consists primarily of exiles and the extreme strategies of protectors. Healing occurs when the Self—the core of consciousness characterized by qualities like compassion, curiosity, calm, and clarity—leads the internal system, unburdening exiles and helping protectors relax their extreme roles (Schwartz, 2013). This process closely parallels the Shadow-Gift-Essence framework: the shadow (exiles and extreme protectors) is recognized, the gift (the positive intention and capacity within each part) is honored, and the essence (Self-led wholeness) emerges (Gallardo, 2025b).
4.3. Trauma Theory: The Fragmentation of Self
Trauma theory, particularly as articulated by Bessel van der Kolk, emphasizes that trauma fragments the self and disrupts integration (van der Kolk, 2014). Traumatic experiences overwhelm the brain’s capacity to process and integrate information, resulting in memories that are stored in implicit, sensorimotor, and emotional systems without being integrated into explicit, narrative memory (van der Kolk et al., 1996).
This fragmentation manifests in several ways:
Dissociation: A disconnection between thoughts, feelings, sensations, and sense of self, ranging from mild (spacing out) to severe (dissociative identity disorder). Dissociation is a survival mechanism that allows the person to escape unbearable experience, but it prevents integration and healing (Nijenhuis & van der Hart, 2011).
Intrusion and avoidance: Traumatic memories intrude involuntarily through flashbacks, nightmares, and triggered emotional states, while the person simultaneously avoids reminders of the trauma. This oscillation between intrusion and avoidance prevents processing (Horowitz, 1986).
Hyperarousal and hypoarousal: The autonomic nervous system becomes dysregulated, oscillating between sympathetic hyperactivation (hypervigilance, panic, rage) and dorsal vagal shutdown (numbness, collapse, dissociation) (Porges, 2011). This dysregulation is the somatic signature of unresolved trauma.
Loss of coherent narrative: Trauma disrupts the capacity to construct a coherent life story. The traumatic event exists as a disconnected fragment that cannot be integrated into the person’s sense of who they are (Herman, 1992).
Healing trauma, from this perspective, requires creating conditions of safety in which fragmented aspects of experience can be brought into awareness, processed, and integrated into a coherent whole (van der Kolk, 2014). This is precisely what the Shadow-Gift-Essence process facilitates.
4.4. Polyvagal Theory: The Neurobiology of Safety and Threat
Stephen Porges’ polyvagal theory provides a neurobiological framework for understanding how trauma disrupts the nervous system and how healing occurs (Porges, 2011). The theory identifies three hierarchical neural circuits that regulate physiological state:
Ventral vagal complex (social engagement system): The newest evolutionary system, mediated by myelinated vagal pathways to the heart and face, supports social engagement, communication, and feelings of safety. When this system is active, we feel calm, connected, and curious—the optimal state for learning, healing, and relationship (Porges, 2017).
Sympathetic nervous system (mobilization): The fight-or-flight system, which activates when the social engagement system fails to resolve threat. Sympathetic activation increases heart rate, blood pressure, and muscle tension, preparing the body for action. Chronic sympathetic activation manifests as anxiety, hypervigilance, and irritability (Porges, 2011).
Dorsal vagal complex (immobilization): The oldest evolutionary system, which produces shutdown, collapse, and dissociation when fight-or-flight is not possible. Dorsal vagal activation slows heart rate, lowers blood pressure, and produces feelings of numbness, hopelessness, and disconnection (Porges, 2011).
Trauma disrupts the social engagement system, leaving individuals oscillating between sympathetic hyperarousal and dorsal vagal shutdown. Healing requires restoring ventral vagal tone—the capacity to feel safe in one’s body and in relationship with others (Porges, 2017). This is why therapeutic presence, attunement, and co-regulation are essential elements of trauma treatment (Dana, 2018).
The shadow, in polyvagal terms, consists of the defensive states (fight, flight, freeze, collapse) that become chronic when the nervous system cannot return to safety. The gift is the adaptive capacity these states represent—the ability to mobilize energy or conserve resources when needed. The essence is the ventral vagal state of safety, connection, and presence (Gallardo, 2025b).
4.5. Hawkins’ Map of Consciousness: Calibrating the Shadow Spectrum
David Hawkins’ Map of Consciousness provides a precise calibration system for understanding levels of consciousness and their associated emotional states (Hawkins, 1995, 2012). The map uses a logarithmic scale from 1 to 1,000, where each level represents a tenfold increase in energetic power. The shadow spectrum occupies the lower levels:
Shame (20): The lowest level of consciousness, characterized by feelings of worthlessness, humiliation, and the desire to disappear. Shame is associated with suicidality, profound isolation, and the belief “I am bad.” Individuals at this level often experienced severe abuse, neglect, or trauma (Hawkins, 2012).
Guilt (30): Characterized by remorse, self-blame, and the belief “I did something bad.” While guilt can motivate reparative action, chronic guilt becomes self-punishing and paralyzing. Guilt is often weaponized by religious and cultural systems to control behavior (Hawkins, 2012).
Apathy (50): A state of hopelessness, helplessness, and despair. Individuals at this level feel powerless to change their circumstances and often give up. Apathy is common among the chronically poor, the homeless, and those with severe depression (Hawkins, 2012).
Grief (75): Characterized by sadness, loss, and regret. Grief is a natural response to loss, but when it becomes chronic or complicated, it can trap individuals in the past. Grief calibrates higher than apathy because it involves emotional engagement rather than numbness (Hawkins, 2012).
Fear (100): The world is perceived as dangerous and threatening. Fear drives hypervigilance, avoidance, and anxiety. While fear can be adaptive in the presence of real threat, chronic fear is exhausting and limiting (Hawkins, 2012).
Desire (125): Characterized by craving, wanting, and attachment. Desire drives much human behavior, from ambition to addiction. While desire can motivate achievement, it also creates suffering through constant striving and dissatisfaction (Hawkins, 2012).
Anger (150): Characterized by resentment, frustration, and hostility. Anger can be empowering compared to lower levels (it involves taking action rather than collapsing), but it is also destructive and separating. Anger often masks underlying fear or pain (Hawkins, 2012).
Pride (175): The highest level of the shadow spectrum, characterized by inflation, defensiveness, and the need to be right. Pride feels good compared to lower levels, but it is vulnerable (dependent on external validation) and separating (requires seeing others as inferior). Pride is the level of nationalism, religious fundamentalism, and narcissism (Hawkins, 2012).
The critical threshold occurs at courage (200), where individuals begin to take responsibility for their experience and engage with life proactively. Above 200, consciousness expands through neutrality (250), willingness (310), acceptance (350), reason (400), love (500), joy (540), peace (600), and enlightenment (700-1000) (Hawkins, 2012).
Hawkins’ map provides a precise diagnostic tool for assessing where individuals, groups, and even nations operate on the consciousness spectrum. It also provides a roadmap for transformation: healing requires systematic elevation from shadow levels through courage and acceptance toward love and peace.
4.6. The Shadow-Gift-Essence (S-G-E) Framework
Prof. Gallardo’s Shadow-Gift-Essence framework integrates these perspectives into a practical, transformative process (Gallardo, 2025b). The framework recognizes three dimensions of every emotional experience:
Shadow: The difficult, disowned, or painful emotion or part of self. This is the raw feeling—fear, anger, shame, grief—that we typically try to avoid or suppress. In IFS terms, this is the exile or the extreme strategy of a protector. In Hawkins’ terms, this is the consciousness level at which the emotion calibrates (Gallardo, 2025b).
Gift: The positive intention, adaptive capacity, or wisdom hidden within the shadow. Every emotion, no matter how painful, carries a message or serves a purpose. Fear wants to protect us. Anger wants to defend our boundaries. Shame wants us to belong. Grief honors what we have loved. The gift is the healthy expression of the need or capacity that the shadow represents (Gallardo, 2025b).
Essence: The integrated quality of being that emerges when the shadow is acknowledged and the gift is claimed. Essence represents the Self-led state in IFS terms, or the higher consciousness level in Hawkins’ terms. Examples of essence qualities include peace, wisdom, love, freedom, authenticity, and compassion (Gallardo, 2025b).
The S-G-E process involves three steps:
- Recognize and name the shadow: Bring the difficult emotion or part into awareness without judgment. “I notice fear present” or “There’s a part of me that feels ashamed.”
- Ask for the gift: Inquire into the positive intention or message. “What are you trying to tell me? What do you need? What capacity are you trying to develop?” This step transforms the relationship with the emotion from adversarial to collaborative.
- Embody the essence: Integrate the gift and experience the essence state. “When this need is met, who am I? How do I feel?” This step anchors the transformation (Gallardo, 2025b).
The S-G-E framework is compatible with multiple therapeutic modalities—IFS, Gestalt, Focusing, Hakomi, EMDR—and can be applied in individual therapy, group work, and self-practice. It is particularly powerful when combined with hypnotherapy, which creates the relaxed, receptive state in which shadow material can surface safely and gifts can be installed at the subconscious level (Gallardo & Chetri, 2026).
4.7. The Meta Pets System: Playful Shadow Integration
The Meta Pets system is Prof. Gallardo’s innovative application of the S-G-E framework using symbolic cosmic animals to represent internal parts (Gallardo, 2025a). Each Meta Pet embodies a shadow-gift-essence triad. For example:
- • Shadow: A frightened rabbit (fear, hypervigilance)
- • Gift: A wise owl (discernment, foresight)
- • Essence: A peaceful dove (trust, serenity)
By externalizing internal parts as playful, archetypal animals, the Meta Pets system bypasses ego defenses and engages the imagination. Clients can dialogue with their Meta Pets, color them, visualize them, and gradually transform them from shadow to essence forms. This approach is particularly effective with children, but adults also respond powerfully to the symbolic, imaginal dimension (Gallardo, 2025a).
The Meta Pets system draws on Jungian active imagination, IFS parts work, and hypnotic visualization techniques. It represents a unique contribution to the field of shadow integration, making deep psychological work accessible, engaging, and even joyful (Gallardo, 2025a).
5. The Global Pain and Trauma Map (GPTM)
5.1. Introduction to the GPTM
The Global Pain and Trauma Map (GPTM) is an original framework developed by Prof. Luis Miguel Gallardo that integrates the seven-domain taxonomy of suffering (Section 3) with Hawkins’ Map of Consciousness (Section 4.5) and neurobiological mechanisms of healing (Section 6). The GPTM provides a structured matrix for:
- Mapping sources of suffering across individual, relational, collective, structural, existential, somatic, and environmental domains
- Calibrating consciousness levels associated with each source of suffering using Hawkins’ scale
- Identifying neurobiological mechanisms involved in each type of suffering
- Prescribing evidence-based interventions tailored to each domain and consciousness level
The GPTM is designed to be used by clinicians, researchers, policymakers, and individuals seeking to understand and address suffering systematically. It represents a synthesis of global epidemiological data, consciousness research, neuroscience, and contemplative wisdom.
5.2. The GPTM Matrix: Structure and Components
The GPTM is organized as a seven-by-seven matrix, with the seven domains of suffering on one axis and seven key dimensions on the other:
Axis 1: Seven Domains of Suffering 1. Individual/Psychological 2. Relational/Social 3. Collective/Cultural 4. Structural/Systemic 5. Existential/Spiritual 6. Somatic/Biological 7. Environmental/Planetary
Axis 2: Seven Dimensions of Analysis 1. Primary manifestations: How suffering appears in this domain 2. Consciousness calibration: Hawkins’ levels associated with this suffering 3. Neurobiological correlates: Brain systems and mechanisms involved 4. Epidemiological data: Prevalence, incidence, burden 5. Shadow-Gift-Essence triad: The transformation pathway 6. Evidence-based interventions: Protocols with strongest evidence 7. Implementation scale: Individual, community, institutional, or planetary
Due to space constraints, we present here a condensed version of the GPTM focusing on three domains (Individual/Psychological, Collective/Cultural, and Existential/Spiritual) with all seven dimensions. The complete GPTM, including all seven domains, is available as a supplementary resource.
5.3. GPTM Domain 1: Individual/Psychological Suffering
Primary Manifestations: - Depression (persistent sadness, anhedonia, hopelessness) - Anxiety disorders (excessive worry, panic, phobias) - PTSD (intrusive memories, hyperarousal, avoidance) - Shame and guilt (self-condemnation, worthlessness) - Shadow material (repressed emotions, disowned parts)
Consciousness Calibration: - Depression: Apathy (50) to Grief (75) - Anxiety: Fear (100) - PTSD: Fear (100) to Anger (150) - Shame: Shame (20) - Guilt: Guilt (30) - Repressed anger: Anger (150) held unconsciously
Neurobiological Correlates: - Overactive default mode network (DMN) → rumination, self-referential thinking - Amygdala hyperactivity → threat detection, fear conditioning - Prefrontal cortex hypoactivity → impaired emotion regulation - Hippocampal volume reduction → memory consolidation deficits - HPA axis dysregulation → chronic cortisol elevation - Reduced BDNF → impaired neuroplasticity
Epidemiological Data: - Depression: 279.6 million globally (3.8% prevalence) - Anxiety: 301.4 million globally (4.1% prevalence) - PTSD: 71.3 million globally (0.9% prevalence) - Lifetime trauma exposure: 70.4% of adults - ACEs (4+): 12.5% of adults, predicting 4-12x increased risk for mental disorders
Shadow-Gift-Essence Triad: - Shadow: Depression (apathy, hopelessness), Anxiety (fear, hypervigilance), Shame (worthlessness) - Gift: Depression → Depth, introspection, sensitivity; Anxiety → Discernment, preparation; Shame → Humility, belonging - Essence: Peace, self-compassion, authentic presence
Evidence-Based Interventions: - Cognitive-behavioral therapy (CBT): Strong evidence for depression, anxiety - EMDR: Strong evidence for PTSD - Mindfulness-based interventions: Strong evidence for depression relapse prevention, anxiety - Hypnotherapy: Moderate-strong evidence for anxiety, PTSD, depression - IFS therapy: Emerging evidence for complex trauma - Psychedelic-assisted therapy: Strong emerging evidence (psilocybin for depression, MDMA for PTSD) - Shadow work practices: Clinical case series evidence
Implementation Scale: - Individual: Psychotherapy, medication, self-practice - Community: Support groups, peer counseling, community mental health centers - Institutional: Workplace mental health programs, school-based interventions - Planetary: Global mental health initiatives, WHO Mental Health Action Plan
5.4. GPTM Domain 3: Collective/Cultural Suffering
Primary Manifestations: - Collective trauma (war, genocide, natural disasters, pandemics) - Intergenerational trauma (transmitted across generations) - Historical trauma (cumulative wounding of marginalized groups) - Cultural trauma (shattering of collective identity) - Moral injury (violation of moral code in impossible situations)
Consciousness Calibration: - Collective trauma: Grief (75) to Fear (100) to Anger (150) - Intergenerational trauma: Apathy (50) to Grief (75) - Historical trauma: Shame (20) to Anger (150) - Moral injury: Guilt (30) to Shame (20)
Neurobiological Correlates: - Epigenetic modifications (DNA methylation, histone acetylation) transmitting stress vulnerability - Altered HPA axis function in descendants of trauma survivors - Amygdala sensitization across generations - Disrupted attachment systems affecting parenting and child development - Collective nervous system dysregulation in communities
Epidemiological Data: - 1.45 billion people in conflict-affected countries (1989-2019) - 354 million adults with PTSD in conflict zones - 392 million adults with depression in conflict zones - Elevated rates of substance abuse, suicide, domestic violence in historically traumatized communities (e.g., Native American communities: suicide rate 2.5x national average)
Shadow-Gift-Essence Triad: - Shadow: Collective grief, rage, shame, victimhood identity - Gift: Resilience, solidarity, cultural memory, moral clarity - Essence: Collective healing, reconciliation, shared wisdom, cultural renewal
Evidence-Based Interventions: - Trauma-informed community interventions: Moderate evidence - Truth and reconciliation processes: Case study evidence (South Africa, Rwanda) - Collective healing rituals: Traditional practice evidence - Narrative therapy for collective stories: Emerging evidence - Intergenerational dialogue programs: Pilot evidence - Community-based participatory research: Moderate evidence
Implementation Scale: - Individual: Family therapy addressing intergenerational patterns - Community: Community healing circles, cultural revitalization programs - Institutional: Truth commissions, reparations programs, memorial processes - Planetary: International justice mechanisms, global reconciliation initiatives
5.5. GPTM Domain 5: Existential/Spiritual Suffering
Primary Manifestations: - Existential anxiety (death, meaninglessness, isolation, freedom) - Loss of meaning and purpose (existential vacuum) - Spiritual crisis (dark night of the soul, spiritual emergency) - Disconnection from the sacred - Fear of death and annihilation
Consciousness Calibration: - Existential anxiety: Fear (100) - Loss of meaning: Apathy (50) - Spiritual crisis: Grief (75) to Fear (100) (during crisis); potential for breakthrough to Love (500+) - Fear of death: Fear (100)
Neurobiological Correlates: - DMN activity related to self-referential thinking and mortality salience - Anterior cingulate cortex activation in meaning-making - Insular cortex involvement in interoceptive awareness and existential feelings - Prefrontal-parietal networks supporting abstract reasoning about existence - Reduced DMN activity during mystical experiences correlating with ego dissolution
Epidemiological Data: - Existential distress: Difficult to quantify; elevated in terminal illness (40-60% of cancer patients), late life, and during social upheaval - Loss of meaning: Associated with depression, suicide risk - Spiritual crisis: Estimated 5-10% of population experiences significant spiritual emergency - Death anxiety: Universal but varies in intensity; elevated in anxiety disorders, PTSD
Shadow-Gift-Essence Triad: - Shadow: Existential dread, meaninglessness, isolation, death terror - Gift: Depth, authenticity, freedom, capacity for transcendence - Essence: Peace, meaning, connection to the sacred, acceptance of mortality
Evidence-Based Interventions: - Existential psychotherapy: Moderate evidence for existential distress - Meaning-centered therapy: Strong evidence for cancer patients (Breitbart et al.) - Psilocybin-assisted therapy: Strong evidence for existential distress in terminal illness - Contemplative practices (meditation, prayer): Strong evidence for meaning, peace - Life Between Lives (LBL) hypnotherapy: Clinical case series evidence for existential questions - Logotherapy: Moderate evidence for meaning-making
Implementation Scale: - Individual: Psychotherapy, spiritual direction, contemplative practice - Community: Spiritual communities, death cafes, meaning-making groups - Institutional: Chaplaincy programs, palliative care, educational curricula on meaning - Planetary: Global dialogue on meaning, purpose, and human flourishing
5.6. Using the GPTM: Clinical and Research Applications
The GPTM serves multiple functions:
For clinicians: The GPTM provides a comprehensive assessment framework. By identifying which domains of suffering are most active for a client and calibrating their consciousness level, clinicians can select interventions most likely to be effective. For example, a client operating at shame (20) requires different interventions than one at anger (150) or acceptance (350).
For researchers: The GPTM identifies gaps in evidence and suggests research priorities. Domains with strong epidemiological data but weak intervention evidence (e.g., structural suffering, environmental suffering) require urgent research attention. The GPTM also suggests cross-domain research questions: How does addressing individual trauma affect collective healing? How do structural interventions impact individual consciousness?
For policymakers: The GPTM reveals that addressing suffering requires multi-level intervention. Policies focused only on individual treatment will fail if structural, collective, and environmental sources of suffering remain unaddressed. The GPTM supports integrated policy approaches that address suffering across all seven domains simultaneously.
For individuals: The GPTM provides a map for self-understanding and personal growth. By identifying which domains are most active in one’s own experience and recognizing the consciousness level at which one is operating, individuals can choose practices and interventions to support their journey from shadow to essence.
6. Protocols for the Journey from Shadow to Fundamental Peace
This section presents evidence-based protocols for healing and consciousness elevation, organized by intervention type. Each protocol is grounded in neuroscience, supported by clinical evidence, and integrated with the S-G-E framework and Hawkins’ Map of Consciousness.
6.1. The Shadow-Gift-Essence (S-G-E) Process
The S-G-E process, detailed in Section 4.6, is the foundational protocol underlying all other interventions. It can be practiced independently or integrated into any therapeutic modality. The process involves:
Step 1: Recognize and name the shadow - Bring awareness to the difficult emotion, sensation, or part - Name it without judgment: “I notice fear” or “There’s a part that feels ashamed” - Locate it in the body if possible - Rate its intensity (0-10 scale)
Step 2: Ask for the gift - Approach the shadow with curiosity and compassion - Ask: “What are you trying to tell me? What do you need? What are you protecting?” - Listen for the answer (words, images, sensations, intuitions) - Identify the positive intention or adaptive capacity - Thank the shadow for its message
Step 3: Embody the essence - Imagine the need being met or the gift being claimed - Notice how you feel when this happens - Identify the essence quality (peace, freedom, love, authenticity, etc.) - Anchor this state with a word, image, gesture, or breath - Practice returning to this essence state
Clinical applications: - Individual therapy: Guide clients through S-G-E process for presenting problems - Group therapy: Facilitate shared S-G-E exploration of collective shadows - Self-practice: Daily S-G-E journaling or meditation - Crisis intervention: Rapid S-G-E process for acute distress
Evidence base: - Integrates evidence-based elements from IFS (Schwartz, 2013), Focusing (Gendlin, 1978), Gestalt (Perls, 1969), and emotion-focused therapy (Greenberg, 2015) - Clinical case series from Gallardo’s practice show significant improvements in depression, anxiety, and self-compassion (Gallardo, 2025b)
6.2. Hypnotherapy and Altered States of Consciousness
Hypnotherapy is a powerful tool for accessing and transforming shadow material because it creates a relaxed, receptive state in which the subconscious mind becomes accessible (Gallardo & Chetri, 2026). The neurobiological mechanisms include:
- • DMN suppression: Hypnotic trance reduces default mode network activity, quieting rumination and self-referential thinking
- • Theta/alpha entrainment: Trance states are characterized by theta (4-8 Hz) and alpha (8-13 Hz) brainwaves, which facilitate access to subconscious material
- • Enhanced suggestibility: Hypnosis increases responsiveness to therapeutic suggestions, enabling installation of new responses and beliefs
- • Memory reconsolidation: Hypnotic states may open reconsolidation windows for traumatic memories
- • Autonomic regulation: Hypnotic relaxation activates the parasympathetic nervous system, creating felt safety
Hypnotherapy protocols for shadow work:
Protocol 1: Hypnotic S-G-E Process 1. Induction: Progressive relaxation, breath focus, or imagery-based induction 2. Deepening: Counting down, descending stairs, or deepening imagery 3. Shadow exploration: “Allow an image, symbol, or feeling to emerge that represents what needs attention today” 4. Dialogue: “Ask this part what it wants you to know. Listen for its message” 5. Gift identification: “What gift or capacity does this part carry for you?” 6. Essence installation: “Imagine integrating this gift. Notice how you feel. Anchor this state” 7. Post-hypnotic suggestion: “Each time you [anchor], you’ll access this essence state” 8. Reorientation: Gradual return to alert consciousness
Protocol 2: Parts Negotiation - Used when internal parts are in conflict (e.g., a part that wants to succeed vs. a part that fears failure) - Hypnotic state facilitates dialogue between parts - Goal: Negotiate a solution that honors both parts’ needs - Outcome: Internal harmony, reduced self-sabotage
Protocol 3: Age Regression for Trauma Healing - Hypnotic regression to the time of traumatic event - Adult self provides comfort, protection, and new perspective to younger self - Facilitates memory reconsolidation and integration - Requires careful pacing and safety protocols
Evidence base: - Meta-analysis: Hypnotherapy effective for anxiety (d = 0.79), PTSD (d = 1.10), depression (d = 0.57) (Flammer & Alladin, 2007) - RCT: Hypnotherapy superior to CBT for IBS (Whorwell et al., 1984) - Neuroimaging: Hypnosis reduces DMN activity and increases executive-salience network coupling (Jiang et al., 2017) - Gallardo & Chetri (2026): Hypnosis as mechanism for emotion regulation and self-integration, with pathway to Fundamental Peace
6.3. The Integrative Transformation Model (ITM)
The Integrative Transformation Model (ITM) is Prof. Gallardo’s comprehensive framework for personal and collective transformation, integrating shadow work, consciousness elevation, and systemic change (Gallardo, 2026). The ITM operates at four levels:
Level 1: Individual Transformation - Shadow integration through S-G-E process - Consciousness elevation through contemplative practices - Neurobiological regulation through somatic practices - Meaning-making through narrative work
Level 2: Relational Transformation - Healing attachment wounds - Developing secure, authentic relationships - Practicing compassionate communication - Co-regulating nervous systems
Level 3: Collective Transformation - Addressing collective and intergenerational trauma - Cultural healing and revitalization - Building communities of practice - Collective consciousness elevation
Level 4: Systemic Transformation - Addressing structural sources of suffering - Creating trauma-informed institutions - Advocating for policy change - Planetary healing and regeneration
The ITM recognizes that transformation at any level supports transformation at all other levels. Individual healing creates capacity for relational healing. Relational healing enables collective healing. Collective healing generates momentum for systemic change. And systemic change creates conditions that support individual flourishing.
ITM Implementation: - Individual: Therapy, coaching, self-practice - Organizational: Workplace well-being programs, leadership development - Community: Community healing initiatives, cultural programs - Societal: Policy advocacy, institutional reform, global movements
6.4. The Meta Pets System
The Meta Pets system, introduced in Section 4.7, is a playful, imaginal approach to shadow integration particularly effective for children and adults who respond well to symbolic work (Gallardo, 2025a). The system includes:
Components: - Meta Pets cards: Deck of cards featuring cosmic animals representing shadow-gift-essence triads - Coloring book: Allows clients to color and personalize their Meta Pets - Guided visualizations: Hypnotic journeys to meet and dialogue with Meta Pets - Journaling prompts: Written exploration of Meta Pets’ messages
Protocol: 1. Selection: Client selects or is guided to a Meta Pet that represents their current shadow 2. Exploration: Client explores the Meta Pet’s shadow qualities (e.g., frightened rabbit = fear, hypervigilance) 3. Transformation: Through dialogue and visualization, the Meta Pet transforms to reveal its gift (e.g., wise owl = discernment, foresight) 4. Integration: Client embodies the essence quality (e.g., peaceful dove = trust, serenity) 5. Anchoring: Client creates a visual reminder (colored image, small figurine) to anchor the transformation
Evidence base: - Integrates evidence-based elements from play therapy, art therapy, and Jungian active imagination - Clinical case series show high engagement and positive outcomes, particularly with children and trauma survivors (Gallardo, 2025a)
6.5. Hawkins Consciousness Elevation Practices
David Hawkins’ Map of Consciousness provides a roadmap for systematic elevation from shadow levels to peace and enlightenment (Hawkins, 2012). Key practices include:
Practice 1: Letting Go - Hawkins’ core technique: When a negative emotion arises, feel it fully without resistance, then let it go - Repeat: Feel → Release → Feel → Release - Over time, emotional charge diminishes and consciousness elevates - Documented in “Letting Go: The Pathway of Surrender” (Hawkins, 2012)
Practice 2: Devotional Non-Duality - Surrender the personal will to a higher power or reality - Practice radical acceptance of “what is” - Cultivate humility, gratitude, and reverence - Leads to states of peace (600) and beyond
Practice 3: Consciousness Calibration - Use muscle testing (applied kinesiology) to calibrate consciousness levels of thoughts, beliefs, media, relationships - Consciously choose inputs that calibrate above 200 (courage) - Avoid inputs below 200 (shadow levels)
Practice 4: Contemplation of Truth - Study teachings that calibrate at high levels (e.g., spiritual texts, wisdom traditions) - Contemplate the nature of consciousness, self, and reality - Allow understanding to deepen through direct experience
Evidence base: - Hawkins’ work is based on 20+ years of muscle testing calibrations (250,000+ calibrations) - Controversial in mainstream science due to methodology - Phenomenological reports from practitioners describe profound shifts in consciousness and well-being - Aligns with contemplative neuroscience findings on meditation and consciousness (Lutz et al., 2015)
6.6. Contemplative Practices: Meditation, Yoga, Breathwork
Contemplative practices are among the most well-researched interventions for consciousness elevation and mental health. Key practices include:
Mindfulness Meditation: - Systematic training in present-moment awareness without judgment - Reduces DMN activity, enhances attention regulation, improves emotion regulation - Strong evidence for depression relapse prevention (MBCT), anxiety reduction (MBSR), stress reduction - Meta-analysis: Mindfulness interventions show moderate effects for anxiety (d = 0.63) and depression (d = 0.59) (Goldberg et al., 2018)
Loving-Kindness Meditation (Metta): - Cultivation of unconditional goodwill toward self and others - Increases positive emotions, social connection, vagal tone - Reduces self-criticism, increases self-compassion - RCT evidence for depression, PTSD, chronic pain (Hofmann et al., 2011)
Yoga: - Integration of physical postures, breath control, and meditation - Regulates autonomic nervous system, increases HRV, reduces inflammation - Strong evidence for anxiety, depression, PTSD - Meta-analysis: Yoga shows moderate-large effects for mental health (Cramer et al., 2013)
Breathwork (Pranayama): - Systematic manipulation of breath patterns to regulate nervous system - Slow breathing (4-6 breaths/min) activates parasympathetic nervous system - Alternate nostril breathing balances hemispheric activity - Evidence for anxiety, depression, PTSD (Brown & Gerbarg, 2012)
Contemplative Neuroscience Findings: - Long-term meditators show increased gray matter in prefrontal cortex, insula, hippocampus - Meditation reduces amygdala reactivity to emotional stimuli - Advanced meditators show sustained gamma oscillations associated with compassion - Meditation increases functional connectivity between attention networks - Reviews: Lutz et al. (2015), Tang et al. (2015)
6.7. Community and Collective Healing
Individual healing is necessary but insufficient. Collective healing addresses shared wounds and creates conditions for sustained well-being. Key approaches include:
Trauma-Informed Communities: - Communities organized around principles of safety, trustworthiness, peer support, collaboration, empowerment, and cultural humility - Recognize prevalence and impact of trauma - Avoid re-traumatization through policies and practices - Evidence: Trauma-informed approaches reduce symptoms, improve engagement (SAMHSA, 2014)
Healing Circles: - Structured group processes for sharing stories, witnessing pain, and collective meaning-making - Used in indigenous communities, restorative justice, and community healing - Evidence: Qualitative studies show increased connection, reduced isolation, cultural revitalization (Gone, 2013)
Truth and Reconciliation: - Formal processes for acknowledging historical harms, hearing testimony, and pursuing justice and healing - Examples: South Africa (post-apartheid), Canada (residential schools), Rwanda (post-genocide) - Evidence: Mixed; successful when combined with reparations, institutional reform, and ongoing dialogue (Hayner, 2010)
Collective Rituals: - Shared ceremonies marking transitions, losses, and healing - Examples: Memorial services, cultural celebrations, seasonal rituals - Function: Create shared meaning, facilitate collective processing, strengthen social bonds - Evidence: Anthropological and qualitative research (Turner, 1969)
6.8. Policy-Level Interventions
Addressing suffering at scale requires policy change. Key policy interventions include:
Universal Mental Health Coverage: - Integrate mental health into primary care - Train community health workers in mental health first aid - Provide evidence-based treatments at scale - WHO Mental Health Action Plan 2013-2030
Trauma-Informed Systems: - Education: Trauma-informed schools with social-emotional learning, restorative discipline - Criminal justice: Diversion programs, therapeutic courts, trauma-informed prisons - Child welfare: Prevention-focused, family-centered, culturally responsive - Healthcare: Screening for ACEs, trauma-informed care protocols
Social Determinants of Health: - Poverty reduction: Universal basic income, living wages, social safety nets - Housing: Housing first models for homelessness - Education: Universal access to quality education - Employment: Job training, worker protections, anti-discrimination enforcement
Reparations and Restorative Justice: - Acknowledge historical harms - Provide material reparations to descendants of enslaved, colonized, and genocided peoples - Institutional reform to prevent future harms - Examples: Germany (Holocaust), U.S. (Japanese internment), emerging movements for slavery reparations
Environmental Protection: - Climate action to prevent further ecological destruction - Protection of biodiversity and ecosystems - Support for indigenous land rights and environmental stewardship - Recognition of rights of nature
7. Fundamental Peace as the Target State
7.1. Defining Fundamental Peace
Fundamental Peace (FP) is the target state toward which all healing protocols aim. It is not merely the absence of suffering but a positive, stable, and integrated state of consciousness characterized by specific experiential and neurobiological features (Gallardo & Chetri, 2026). FP calibrates at 600 on Hawkins’ Map of Consciousness, representing a profound shift from shadow levels (20-175) through courage (200) and acceptance (350) to a state of transcendent peace.
Gallardo and Chetri (2026) define Fundamental Peace through four core components:
1. Flexible attentional control without effortful suppression - The capacity to direct attention with ease rather than strain - Attention is stable yet responsive, focused yet open - No need to forcefully suppress distractions or unwanted thoughts - Corresponds to mature mindfulness and effortless concentration
2. Emotional coherence across self-states - A sense of inner continuity even when emotions change - No dissociation or fragmentation of experience - All parts of self are acknowledged and integrated - Corresponds to IFS concept of Self-leadership and secure attachment
3. Reduced self-referential rigidity - Freedom from repetitive, ruminative loops of self-criticism and worry - Flexible sense of self that can adapt to changing contexts - Reduced identification with fixed self-concepts - Corresponds to reduced DMN activity and ego flexibility
4. Compassionate self-awareness - The capacity to observe one’s own experience with genuine kindness - Self-compassion as a natural expression of a settled mind, not a technique - Corresponds to activation of self-compassion networks and ventral vagal state
7.2. Neuroscience of Fundamental Peace
Fundamental Peace is not merely a subjective experience but corresponds to specific, measurable patterns of brain activity and connectivity (Gallardo & Chetri, 2026). Key neurobiological features include:
Default Mode Network (DMN) Reconfiguration: - Reduced activity in posterior cingulate cortex (PCC) and medial prefrontal cortex (mPFC) - Decreased self-referential processing and rumination - Maintained connectivity for adaptive self-reflection without rigid self-focus - Similar to patterns observed in experienced meditators (Brewer et al., 2011)
Executive Control Network (ECN) Enhancement: - Increased activity in dorsolateral prefrontal cortex (dlPFC) and posterior parietal cortex - Enhanced capacity for goal-directed attention and cognitive control - Flexible deployment of attention without rigidity - Corresponds to mature attentional control (Posner & Rothbart, 2007)
Salience Network (SaN) Optimization: - Balanced activity in anterior insula and anterior cingulate cortex (ACC) - Appropriate detection of salient stimuli without hypervigilance - Integration of interoceptive and exteroceptive information - Corresponds to embodied awareness and emotional intelligence (Craig, 2009)
Enhanced ECN-SaN Coupling: - Increased functional connectivity between executive control and salience networks - Coordinated processing of emotional salience and cognitive control - Enables emotional regulation without suppression - Observed in hypnotic states and advanced meditation (Jiang et al., 2017)
Autonomic Nervous System Balance: - High heart rate variability (HRV) indicating vagal tone - Flexible shifting between sympathetic and parasympathetic activation - Predominant ventral vagal state (social engagement system) - Corresponds to polyvagal theory’s state of safety and connection (Porges, 2017)
Neuroplasticity Markers: - Elevated brain-derived neurotrophic factor (BDNF) - Increased gray matter density in prefrontal cortex, insula, hippocampus - Enhanced synaptic plasticity and learning capacity - Observed in long-term meditators and after psychedelic experiences (Tang et al., 2015)
Brainwave Patterns: - Increased alpha (8-13 Hz) and theta (4-8 Hz) power during rest - Gamma (40+ Hz) oscillations during compassion and insight states - Coherence across brain regions indicating integration - Corresponds to states of relaxed alertness and flow (Lutz et al., 2004)
7.3. Phenomenology of Fundamental Peace
Beyond neurobiology, Fundamental Peace has a distinctive phenomenology—a characteristic quality of lived experience. Individuals who have accessed FP describe:
Pervasive sense of okayness: - A baseline feeling that “all is well” regardless of external circumstances - Not denial or spiritual bypassing, but a deep trust in the unfolding of life - Corresponds to Hawkins’ level of peace (600): “A sense of perfection of creation” (Hawkins, 2012)
Spaciousness: - Mental and emotional space to hold complexity without collapsing - Capacity to be with difficult emotions without being overwhelmed - Sense of inner vastness or expansiveness
Presence: - Grounded in the present moment without clinging or aversion - Fully engaged with life as it is - Corresponds to mindfulness and flow states
Compassion: - Natural arising of kindness toward self and others - Not forced or effortful, but spontaneous expression of FP - Includes both self-compassion and other-compassion
Clarity: - Clear perception of reality without distortion by fear, desire, or ego - Insight into the nature of self, others, and existence - Corresponds to wisdom traditions’ concept of prajna or gnosis
Connection: - Sense of belonging to something larger than individual self - Connection to others, nature, the cosmos, or the divine - Transcendence of isolation and separation
Freedom: - Liberation from compulsive patterns, addictions, and reactivity - Capacity to choose responses rather than react automatically - Corresponds to psychological flexibility and autonomy
7.4. Fundamental Peace vs. Related Constructs
Fundamental Peace is related to but distinct from other positive psychological constructs:
FP vs. Mindfulness: - Mindfulness emphasizes present-moment awareness - FP includes mindfulness but adds emotional coherence, self-compassion, and reduced self-referential rigidity - FP is a stable trait; mindfulness can be a state or trait
FP vs. Equanimity: - Equanimity emphasizes affective neutrality and non-reactivity - FP includes equanimity but also includes positive qualities like compassion and joy - FP is warmer and more engaged than pure equanimity
FP vs. Flow: - Flow is tied to challenging activity and optimal performance - FP is a baseline state independent of activity - Flow is temporary; FP is stable
FP vs. Psychological Well-Being: - Well-being is a broad evaluative judgment of life satisfaction - FP is a specific neuro-experiential state - Well-being can exist without FP (e.g., through external success); FP generates well-being from within
FP vs. Enlightenment: - Enlightenment (700-1000 on Hawkins’ scale) represents complete transcendence of ego and identification with pure consciousness - FP (600) is a profound state of peace but retains individual selfhood - FP is more accessible and sustainable for most people than full enlightenment
7.5. Cross-Cultural Dimensions of Fundamental Peace
While the neuroscience of FP appears universal, its cultural expression and pathways to attainment vary across traditions:
Buddhist Traditions: - FP corresponds to states of samadhi (concentration), vipassana (insight), and metta (loving-kindness) - Emphasis on cessation of suffering through understanding impermanence, non-self, and interdependence - Practices: Meditation, ethical conduct, wisdom cultivation
Hindu/Yogic Traditions: - FP corresponds to states of samadhi, sat-chit-ananda (being-consciousness-bliss), and atman realization - Emphasis on union with ultimate reality (Brahman) and transcendence of ego (ahamkara) - Practices: Yoga, meditation, devotion (bhakti), self-inquiry (jnana)
Christian Contemplative Traditions: - FP corresponds to “peace that surpasses understanding” (Philippians 4:7) and union with God - Emphasis on surrender, grace, and divine love - Practices: Contemplative prayer, centering prayer, lectio divina
Indigenous Traditions: - FP corresponds to harmony with nature, ancestors, and community - Emphasis on balance, reciprocity, and right relationship - Practices: Ceremony, ritual, connection to land
Secular/Psychological Frameworks: - FP corresponds to self-actualization (Maslow), psychological integration (Jung), Self-leadership (IFS) - Emphasis on personal growth, authenticity, and wholeness - Practices: Psychotherapy, self-reflection, creative expression
These diverse pathways suggest that FP is a universal human capacity that can be cultivated through multiple routes. The Integrative Transformation Model honors this diversity while identifying common mechanisms.
7.6. Measuring Fundamental Peace
To study FP scientifically, we need reliable and valid measurement tools. Gallardo and Chetri (2026) propose a multi-level measurement framework:
Level 1: Self-Report - Fundamental Peace Scale (FPS): Proposed 20-item questionnaire assessing the four components of FP - Items assess flexible attentional control, emotional coherence, reduced self-referential rigidity, and compassionate self-awareness - Psychometric validation needed
Level 2: Behavioral - Attention tasks: Sustained attention, attentional flexibility, distractor resistance - Emotion regulation tasks: Ability to modulate emotional responses without suppression - Social behavior: Compassionate responding, prosocial behavior
Level 3: Physiological - Heart rate variability (HRV): Marker of autonomic balance and vagal tone - Cortisol: Marker of HPA axis regulation - Inflammatory markers: C-reactive protein, IL-6 (chronic stress reduces inflammation)
Level 4: Neurobiological - fMRI: DMN activity, ECN-SaN connectivity, amygdala reactivity - EEG: Alpha/theta power, gamma oscillations, coherence - Structural MRI: Gray matter density in key regions
Level 5: Longitudinal - Stability of FP over time - Resilience to stressors - Generalization across contexts
Development and validation of the Fundamental Peace Scale is a priority for future research (see Section 9).
8. Implementation Framework: Individual to Planetary Healing
Healing suffering at scale requires coordinated action across multiple levels. This section outlines an implementation framework spanning individual, community, institutional, and planetary scales.
8.1. Individual Level: Personal Healing and Growth
Target: Individuals experiencing suffering across any of the seven domains
Interventions: - Psychotherapy (CBT, EMDR, IFS, psychodynamic, humanistic) - Hypnotherapy and altered states work - Contemplative practices (meditation, yoga, breathwork) - Shadow work and S-G-E process - Medication when appropriate - Peer support and self-help groups
Implementation: - Increase access to mental health services through insurance coverage, sliding scale fees, teletherapy - Train therapists in integrative, trauma-informed approaches - Develop self-help resources (apps, books, online courses) - Normalize help-seeking and reduce stigma
Metrics: - Symptom reduction (depression, anxiety, PTSD scales) - Functional improvement (work, relationships, daily activities) - Quality of life and well-being - Consciousness elevation (Hawkins calibration, FP scale)
8.2. Community Level: Collective Healing and Resilience
Target: Communities affected by collective trauma, historical trauma, or ongoing stressors
Interventions: - Community healing circles and dialogue processes - Cultural revitalization programs - Trauma-informed community organizing - Collective rituals and ceremonies - Community-based participatory research
Implementation: - Partner with community leaders, elders, and grassroots organizations - Provide resources and training for community facilitators - Create safe spaces for collective processing - Honor cultural traditions and indigenous healing practices
Metrics: - Community cohesion and social capital - Collective efficacy and empowerment - Reduction in community-level indicators (violence, substance abuse, suicide) - Cultural vitality and identity strength
8.3. Institutional Level: Trauma-Informed Systems
Target: Schools, workplaces, healthcare systems, criminal justice, child welfare, military
Interventions: - Trauma-informed organizational policies and practices - Staff training in trauma awareness and response - Environmental modifications to increase safety - Integration of healing practices into institutional culture
Implementation Examples:
Schools: - Social-emotional learning curricula - Restorative discipline practices - Mindfulness and yoga programs - Trauma-informed teacher training - School-based mental health services
Workplaces: - Employee assistance programs - Stress reduction and resilience training - Flexible work arrangements - Psychological safety and inclusive culture - Leadership development in emotional intelligence
Healthcare: - Universal ACEs screening - Trauma-informed care protocols - Integration of behavioral health into primary care - Provider self-care and burnout prevention
Criminal Justice: - Diversion programs for mental health and substance use - Therapeutic courts (drug court, mental health court) - Trauma-informed corrections - Restorative justice practices
Metrics: - Organizational climate surveys - Staff well-being and retention - Client/patient outcomes - Reduction in disciplinary incidents, recidivism, etc.
8.4. Societal Level: Policy and Structural Change
Target: Social, economic, and political structures that generate suffering
Interventions: - Mental health policy reform - Social determinants of health initiatives - Anti-discrimination and equity policies - Reparations and restorative justice - Environmental protection and climate action
Implementation: - Advocacy and policy campaigns - Coalition building across sectors - Research to document need and evaluate interventions - Public education to shift cultural narratives
Policy Priorities: - Universal mental health coverage - Living wages and poverty reduction - Affordable housing and homelessness prevention - Quality education for all - Criminal justice reform - Climate action and environmental justice - Reparations for historical harms
Metrics: - Population-level mental health indicators - Health equity measures - Social determinants of health indicators - Environmental health indicators - Public opinion and cultural shifts
8.5. Planetary Level: Global Healing Movement
Target: Humanity as a whole and the Earth system
Vision: A global movement for healing and consciousness elevation that transcends national, cultural, and ideological boundaries
Components:
1. Global Mental Health Initiative: - WHO Mental Health Action Plan implementation - Capacity building in LMICs - Research on culturally adapted interventions - Global mental health workforce development
2. Consciousness Elevation Movement: - Dissemination of contemplative practices globally - Integration of consciousness education into schools - Support for spiritual and wisdom traditions - Research on consciousness and healing
3. Truth, Reconciliation, and Healing: - Global truth-telling about historical harms (colonialism, slavery, genocide) - International reparations and restorative justice - Healing of collective and intergenerational trauma - Building cultures of peace and nonviolence
4. Ecological Healing: - Climate action to prevent further destruction - Ecosystem restoration and rewilding - Protection of biodiversity and indigenous lands - Shift to regenerative economic systems
5. New Paradigm of Human Flourishing: - Beyond GDP: Measures of well-being, happiness, and consciousness - Happytalism: Economic system prioritizing human and planetary well-being (Gallardo, 2021) - Education for wisdom, compassion, and ecological literacy - Governance based on long-term thinking and intergenerational responsibility
Implementation: - International cooperation and funding - Global networks of practitioners, researchers, and advocates - Media and cultural narratives promoting healing and transformation - Grassroots movements and local action
Metrics: - Global mental health burden (GBD data) - Consciousness levels (Hawkins calibration of nations, cultures) - Peace indices and conflict reduction - Environmental health indicators - Subjective well-being and happiness (World Happiness Report)
8.6. The Role of Institutions and Organizations
Specific institutions have critical roles to play:
Universities and Research Institutions: - Conduct research on suffering, healing, and consciousness - Train next generation of integrative practitioners - Develop and validate measurement tools - Disseminate knowledge through publications and education
Healthcare Systems: - Integrate mental health into primary care - Provide trauma-informed care - Support provider well-being - Advocate for universal coverage
Schools and Educational Institutions: - Implement social-emotional learning - Create trauma-informed school environments - Teach contemplative practices - Educate for wisdom and compassion
Spiritual and Religious Organizations: - Provide spiritual guidance and community - Offer contemplative practices and rituals - Engage in social justice and healing work - Bridge spiritual and scientific perspectives
Businesses and Corporations: - Prioritize employee well-being - Adopt stakeholder capitalism and B-Corp models - Support Happytalism principles - Use resources for social and environmental good
Governments and Policy Makers: - Enact policies addressing social determinants of health - Fund mental health services and research - Pursue restorative justice and reparations - Lead on climate action and environmental protection
NGOs and Civil Society: - Provide direct services to affected populations - Advocate for policy change - Build grassroots movements - Bridge communities and institutions
8.7. Integration Across Levels
The power of this framework lies in integration across levels. Individual healing creates capacity for community engagement. Community healing generates momentum for institutional change. Institutional change enables policy reform. Policy reform creates conditions for planetary healing. And planetary healing supports individual flourishing.
This is not a linear process but a dynamic, iterative cycle. Change at any level ripples through the system. A single individual achieving Fundamental Peace affects their family, workplace, and community. A trauma-informed school transforms the lives of thousands of children and their families. A policy change can shift the trajectory of millions.
The call is for coordinated, multi-level action guided by a shared vision: a world where every human being has the opportunity to heal from suffering and realize their full potential for peace, wisdom, and compassion.
9. Research Agenda: Ten Priority Questions
To advance this field, we propose ten priority research questions for the next decade:
9.1. Question 1: Validation of the Fundamental Peace Scale
Question: Can we develop and validate a reliable, culturally sensitive self-report measure of Fundamental Peace?
Rationale: Measurement is essential for research and clinical practice. The proposed Fundamental Peace Scale (FPS) needs psychometric validation across diverse populations.
Methods: Item generation, expert review, pilot testing, factor analysis, convergent/discriminant validity, test-retest reliability, cross-cultural validation
Impact: Enables research on FP predictors, outcomes, and interventions; provides clinical assessment tool
9.2. Question 2: Neuroimaging of Fundamental Peace
Question: What are the neural signatures of Fundamental Peace, and how do they differ from related states?
Rationale: Understanding the neurobiology of FP will clarify mechanisms and guide intervention development.
Methods: fMRI and EEG studies comparing individuals high vs. low in FP; longitudinal studies tracking neural changes as FP develops; comparison with mindfulness, flow, and other states
Impact: Identifies neural targets for intervention; validates FP as distinct construct
9.3. Question 3: Efficacy of Integrative Protocols
Question: What is the efficacy of integrative protocols (S-G-E, hypnotherapy, ITM, Meta Pets) for specific clinical populations?
Rationale: While clinical case series are promising, RCTs are needed to establish efficacy.
Methods: Randomized controlled trials comparing integrative protocols to standard treatments for PTSD, depression, anxiety, complex trauma; dismantling studies to identify active ingredients
Impact: Establishes evidence base for integrative approaches; informs clinical practice guidelines
9.4. Question 4: Mechanisms of Shadow Integration
Question: What are the psychological and neurobiological mechanisms through which shadow integration produces healing?
Rationale: Understanding mechanisms enables optimization of interventions.
Methods: Mediation analyses in RCTs; neuroimaging during shadow work; qualitative studies of transformation process; longitudinal studies tracking mechanism changes
Impact: Clarifies how shadow work works; guides intervention refinement
9.5. Question 5: Collective and Intergenerational Trauma
Question: How can we effectively address collective and intergenerational trauma at community and societal scales?
Rationale: Individual interventions are insufficient for collective wounds; we need evidence-based collective healing approaches.
Methods: Community-based participatory research; evaluation of truth and reconciliation processes; longitudinal studies of intergenerational trauma transmission and healing; epigenetic studies
Impact: Informs community healing initiatives, policy, and reparations programs
9.6. Question 6: Structural Interventions
Question: What is the impact of structural interventions (poverty reduction, housing, education, anti-discrimination) on mental health and consciousness?
Rationale: Addressing structural sources of suffering may be more effective than individual treatment alone.
Methods: Natural experiments and quasi-experimental designs evaluating policy changes; longitudinal cohort studies; economic modeling
Impact: Provides evidence for policy advocacy; clarifies relative importance of individual vs. structural interventions
9.7. Question 7: Consciousness Elevation Trajectories
Question: What are the typical trajectories of consciousness elevation, and what factors predict successful transition from shadow to peace?
Rationale: Understanding trajectories enables better support for individuals on the healing journey.
Methods: Longitudinal studies tracking consciousness levels over time; identification of predictors (personality, trauma history, social support, practice engagement); qualitative studies of transformation narratives
Impact: Informs personalized intervention planning; identifies high-risk periods requiring support
9.8. Question 8: Cross-Cultural Validity
Question: Are the constructs and interventions presented in this framework valid across diverse cultural contexts?
Rationale: Most psychological research is WEIRD (Western, Educated, Industrialized, Rich, Democratic); cross-cultural validation is essential.
Methods: Cross-cultural studies of FP, shadow work, and healing practices; adaptation and validation of interventions in diverse cultural contexts; collaboration with indigenous healers and wisdom keepers
Impact: Ensures cultural humility and relevance; enriches framework with diverse perspectives
9.9. Question 9: Epigenetic and Intergenerational Effects
Question: Can healing practices produce epigenetic changes that are transmitted to future generations?
Rationale: If trauma can be transmitted epigenetically, healing may be as well.
Methods: Epigenetic studies (DNA methylation, histone modification) before and after healing interventions; multi-generational studies; animal models
Impact: Reveals potential for healing to benefit future generations; motivates investment in healing work
9.10. Question 10: Planetary-Scale Implementation
Question: What are the most effective strategies for scaling healing interventions to reach billions of people?
Rationale: The global burden of suffering requires interventions that can reach planetary scale.
Methods: Implementation science studies; cost-effectiveness analyses; evaluation of digital interventions (apps, online courses); task-shifting models (training non-specialists); policy analysis
Impact: Enables global mental health initiatives; maximizes impact of limited resources
10. Conclusion: A Call for a Global Healing Movement
10.1. Summary of Key Findings
This paper has presented a comprehensive framework for understanding and addressing global suffering. We have shown that:
- The scale of suffering is immense: Over 1 billion people affected by mental disorders, 70% experiencing trauma, elevated rates in conflict zones, and vast hidden suffering from shame, grief, existential distress, and structural violence.
- Suffering is multi-dimensional: The seven-domain taxonomy (Individual/Psychological, Relational/Social, Collective/Cultural, Structural/Systemic, Existential/Spiritual, Somatic/Biological, Environmental/Planetary) reveals the complexity and interconnection of human pain.
- Suffering is a crisis of consciousness: Operating at shadow levels (shame-20 through pride-175 on Hawkins’ scale), characterized by contraction, separation, and reactivity.
- Healing is possible: Through evidence-based protocols targeting seven shared neurobiological mechanisms (DMN suppression, autonomic regulation, neuroplasticity enhancement, memory reconsolidation, interoceptive predictive coding, theta/alpha entrainment, ego dissolution).
- The target is Fundamental Peace: A stable, integrated state of consciousness (calibrating at 600) characterized by flexible attentional control, emotional coherence, reduced self-referential rigidity, and compassionate self-awareness.
- Implementation requires multi-level action: Individual therapy, community healing, institutional reform, policy change, and planetary transformation must occur simultaneously.
10.2. The Urgency of Now
We live in a time of unprecedented crisis and unprecedented opportunity. The mental health pandemic, ecological collapse, political polarization, and collective trauma of recent years have brought humanity to a breaking point. Yet this breaking point is also a breakthrough point—a moment when old paradigms are crumbling and new possibilities are emerging.
The fragmentation that has characterized our approach to suffering—the separation of mind from body, individual from collective, psychology from spirituality, science from wisdom—is no longer tenable. We need integrative frameworks that honor the full complexity of human experience and address suffering at all levels simultaneously.
This paper offers such a framework. It is grounded in rigorous science yet open to contemplative wisdom. It honors individual healing while recognizing collective and structural dimensions. It provides practical protocols while pointing toward transcendent possibilities.
10.3. A Vision for the Future
Imagine a world where:
- Every child grows up in an environment of safety, attunement, and belonging, with their emotional and spiritual needs met alongside their physical needs.
- Schools teach not only reading and mathematics but also emotional intelligence, contemplative practice, and the skills of shadow integration and consciousness elevation.
- Healthcare systems treat the whole person—body, mind, and spirit—with trauma-informed care as the standard, not the exception.
- Workplaces prioritize employee well-being, creating cultures of psychological safety, meaning, and purpose.
- Communities have spaces and practices for collective healing, where historical and ongoing traumas can be acknowledged, processed, and transformed.
- Governments enact policies that address the social determinants of health, pursue restorative justice, and protect the environment for future generations.
- Humanity recognizes its interconnection with all life and acts as stewards of the Earth rather than exploiters.
- Consciousness elevation is understood as a legitimate and essential dimension of human development, supported by education, culture, and institutions.
- Fundamental Peace is not a rare attainment of spiritual masters but an accessible state cultivated by millions, creating a critical mass that shifts collective consciousness.
This is not utopian fantasy. Every element of this vision is already being implemented somewhere in the world. The question is whether we have the collective will to scale these efforts and integrate them into a coherent global movement.
10.4. The Role of Shoolini University and the Yogananda School
Shoolini University, and particularly the Yogananda School of Spirituality and Happiness, is uniquely positioned to lead this movement. Located in India—a civilization with ancient wisdom traditions and modern scientific capacity—the university can serve as a bridge between East and West, tradition and innovation, spirituality and science.
The Yogananda School’s mission—to integrate spirituality and happiness into education and research—aligns perfectly with the framework presented in this paper. By training students in both contemplative practices and scientific methods, by conducting rigorous research on consciousness and healing, and by developing innovative interventions like the Meta Pets system and the Integrative Transformation Model, the school can become a global center for the study and practice of healing and transformation.
Specific initiatives could include:
- • Research Center for Consciousness and Healing: Conducting the research outlined in Section 9, particularly neuroimaging of Fundamental Peace, validation of the FP Scale, and efficacy trials of integrative protocols.
- • Training Programs: Offering certificates and degrees in integrative healing, trauma-informed practice, and consciousness studies, training the next generation of practitioners and researchers.
- • Community Outreach: Partnering with local communities to implement trauma-informed programs, collective healing initiatives, and consciousness elevation practices.
- • Global Collaborations: Building partnerships with universities, research centers, and organizations worldwide to advance the global healing movement.
- • Policy Advocacy: Engaging with government and international organizations to promote mental health policy, trauma-informed systems, and consciousness-based approaches.
10.5. A Call to Action
This paper is not merely an academic exercise. It is a call to action—for researchers, clinicians, educators, policymakers, spiritual leaders, and every individual who recognizes that the world’s suffering is unsustainable and that transformation is both necessary and possible.
For researchers: Pursue the questions outlined in Section 9. Develop rigorous methods for studying consciousness, healing, and transformation. Publish your findings and contribute to the evidence base.
For clinicians: Integrate shadow work, consciousness elevation, and trauma-informed approaches into your practice. Pursue training in hypnotherapy, IFS, EMDR, and contemplative practices. Measure outcomes and contribute to clinical knowledge.
For educators: Bring social-emotional learning, contemplative practices, and consciousness education into schools. Create trauma-informed learning environments. Teach students not only how to think but how to be.
For policymakers: Enact policies that address the social determinants of health, support mental health services, pursue restorative justice, and protect the environment. Use evidence to guide decisions and measure success by well-being, not just GDP.
For spiritual leaders: Bridge the gap between spirituality and science. Offer contemplative practices and wisdom teachings while honoring scientific inquiry. Support collective healing and social justice.
For individuals: Begin your own healing journey. Practice shadow integration, meditation, and self-compassion. Seek therapy or coaching if needed. As you heal, you contribute to collective healing. As you elevate your consciousness, you raise the consciousness of the whole.
10.6. The Power of One
David Hawkins’ research revealed a profound truth: consciousness is not additive but logarithmic. One individual at the level of Love (500) counterbalances 750,000 individuals below Courage (200). One individual at Peace (600) counterbalances 10 million below 200. One individual at Enlightenment (700+) counterbalances 70 million (Hawkins, 2012).
This means that your personal healing and consciousness elevation matter not only for you but for the entire world. Every moment of shadow integration, every practice of compassion, every choice to respond from peace rather than react from fear—these ripple out in ways we cannot fully measure but that are nonetheless real.
You are not separate from the global crisis of suffering. You are part of it. And you are also part of the solution. The journey from shadow to Fundamental Peace is not only your personal healing—it is your contribution to planetary healing.
10.7. Final Words
We began this paper by acknowledging the immensity of global suffering. We end by affirming the possibility of global healing. The frameworks, protocols, and evidence presented here demonstrate that transformation is not only possible but already occurring. The question is whether we will accelerate and scale these efforts to meet the magnitude of the crisis.
The world cannot be built on violence, as Prof. Gallardo has written (Gallardo, 2026). It cannot be built on fear, shame, or separation. It can only be built on peace—Fundamental Peace—arising from the integration of our shadows, the elevation of our consciousness, and the recognition of our profound interconnection with all life.
This is the work of our time. This is the calling of our generation. May we rise to meet it with courage, compassion, and unwavering commitment to the healing and flourishing of all beings.
References
- Ainsworth, M. D. S.; Blehar, M. C.; Waters, E.; Wall, S. Patterns of attachment: A psychological study of the strange situation; Lawrence Erlbaum, 1978. [Google Scholar]
- Albrecht, G. Earth emotions: New words for a new world; Cornell University Press, 2019. [Google Scholar]
- Alexander, J. C. Toward a theory of cultural trauma. In Cultural trauma and collective identity; Alexander, J. C., Eyerman, R., Giesen, B., Smelser, N. J., Sztompka, P., Eds.; University of California Press, 2004; pp. 1–30. [Google Scholar]
- Alexander, M. The new Jim Crow: Mass incarceration in the age of colorblindness; The New Press, 2010. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th ed.; American Psychiatric Publishing, 2013. [Google Scholar]
- Becker, E. The denial of death; Free Press, 1973. [Google Scholar]
- Benjet, C.; Bromet, E.; Karam, E. G.; Kessler, R. C.; McLaughlin, K. A.; Ruscio, A. M.; Koenen, K. C. The epidemiology of traumatic event exposure worldwide: Results from the World Mental Health Survey Consortium. Psychological Medicine 2016, 46, 327–343. [Google Scholar] [CrossRef]
- Bowlby, J. A secure base: Parent-child attachment and healthy human development; Basic Books, 1988. [Google Scholar]
- Brave Heart, M. Y. H. The historical trauma response among natives and its relationship with substance abuse: A Lakota illustration. Journal of Psychoactive Drugs 2003, 35, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Brave Heart, M. Y. H.; DeBruyn, L. M. The American Indian Holocaust: Healing historical unresolved grief. American Indian and Alaska Native Mental Health Research 1998, 8, 56–78. [Google Scholar] [CrossRef]
- Breitbart, W.; Rosenfeld, B.; Pessin, H.; Applebaum, A.; Kulikowski, J.; Lichtenthal, W. G. Meaning-centered group psychotherapy: An effective intervention for improving psychological well-being in patients with advanced cancer. Journal of Clinical Oncology 2015, 33, 749–754. [Google Scholar] [CrossRef]
- Brewer, J. A.; Worhunsky, P. D.; Gray, J. R.; Tang, Y. Y.; Weber, J.; Kober, H. Meditation experience is associated with differences in default mode network activity and connectivity. Proceedings of the National Academy of Sciences 2011, 108, 20254–20259. [Google Scholar] [CrossRef] [PubMed]
- Brown, B. Shame resilience theory: A grounded theory study on women and shame. Families in Society 2006, 87, 43–52. [Google Scholar] [CrossRef]
- Brown, R. P.; Gerbarg, P. L. The healing power of the breath: Simple techniques to reduce stress and anxiety, enhance concentration, and balance your emotions; Shambhala, 2012. [Google Scholar]
- Cacioppo, J. T.; Patrick, W. Loneliness: Human nature and the need for social connection; W. W. Norton, 2008. [Google Scholar]
- Campbell, J. C. Health consequences of intimate partner violence. The Lancet 2002, 359, 1331–1336. [Google Scholar] [CrossRef]
- Cassell, E. J. The nature of suffering and the goals of medicine. New England Journal of Medicine 1982, 306, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, K. Loss of self: A fundamental form of suffering in the chronically ill. Sociology of Health & Illness 1983, 5, 168–195. [Google Scholar] [CrossRef]
- Charlson, F.; van Ommeren, M.; Flaxman, A.; Cornett, J.; Whiteford, H.; Saxena, S. New WHO prevalence estimates of mental disorders in conflict settings: A systematic review and meta-analysis. The Lancet 2019, 394, 240–248. [Google Scholar] [CrossRef]
- Cheng, Y.; Li, X.; Lou, C.; Sonenstein, F. L.; Kalamar, A.; Jejeebhoy, S.; Santhya, K. G. Global, regional, and national burden of mental disorders among women of reproductive age, 1990–2021: A systematic analysis of the global burden of disease study 2021. BMC Public Health 2025, 25, 1–15. [Google Scholar] [CrossRef]
- Cowden, R. G.; Davis, E. B.; Van Tongeren, D. R.; Worthington, E. L.; Hook, J. N.; Aten, J. D.; Captari, L. E. Childhood predictors of suffering in adulthood: A cross-national analysis with 22 countries. 2025. [Google Scholar] [CrossRef]
- Craig, A. D. How do you feel—now? The anterior insula and human awareness. Nature Reviews Neuroscience 2009, 10, 59–70. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Langhorst, J.; Dobos, G. Yoga for depression: A systematic review and meta-analysis. Depression and Anxiety 2013, 30, 1068–1083. [Google Scholar] [CrossRef]
- Cunsolo, A.; Ellis, N. R. Ecological grief as a mental health response to climate change-related loss. Nature Climate Change 2018, 8, 275–281. [Google Scholar] [CrossRef]
- Dana, D. The polyvagal theory in therapy: Engaging the rhythm of regulation; W. W. Norton, 2018. [Google Scholar]
- Doka, K. J. Disenfranchised grief: Recognizing hidden sorrow; Lexington Books, 1989. [Google Scholar]
- Fan, M.; Liu, C.; Jiang, H.; Hu, J.; Lv, J.; Xu, J.; Zhang, X. Global burden of mental disorders in 204 countries and territories, 1990–2021: Results from the global burden of disease study 2021. BMC Psychiatry 2025, 25, 1–18. [Google Scholar] [CrossRef]
- Farmer, P. An anthropology of structural violence. Current Anthropology 2004, 45, 305–325. [Google Scholar] [CrossRef]
- Felitti, V. J.; Anda, R. F.; Nordenberg, D.; Williamson, D. F.; Spitz, A. M.; Edwards, V.; Marks, J. S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A. J.; Santomauro, D. F.; Aali, A.; Abate, Y. H.; Abbafati, C.; Abbastabar, H.; Vos, T. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. The Lancet 2024, 404, 1026–1049. [Google Scholar] [CrossRef]
- Flammer, E.; Alladin, A. The efficacy of hypnotherapy in the treatment of psychosomatic disorders: Meta-analytical evidence. International Journal of Clinical and Experimental Hypnosis 2007, 55, 251–274. [Google Scholar] [CrossRef] [PubMed]
- Frankl, V. E. Man’s search for meaning; Beacon Press, 1959. [Google Scholar]
- Freyd, J. J. Betrayal trauma: The logic of forgetting childhood abuse; Harvard University Press, 1996. [Google Scholar]
- Gallardo, L. M. Happytalism: How countries, cities, and companies are unlocking the secrets of happiness and well-being; World Happiness Foundation Press, 2021. [Google Scholar]
- Gallardo, L. M. Shadow work: Unlocking the hidden light. World Happiness Foundation. 2025a. Available online: https://worldhappiness.foundation/blog/consciousness/shadow-work-unlocking-the-hidden-light/.
- Gallardo, L. M. From shadow to essence: An integrative way to understand our emotions. World Happiness Foundation. 2025b. Available online: https://worldhappiness.foundation/blog/consciousness/from-shadow-to-essence-an-integrative-way-to-understand-our-emotions-and-how-it-compares-to-other-frameworks/.
- Gallardo, L. M. The road map to supraconsciousness: From the diagnosis of a world in crisis to the conscious evolution of humanity. World Happiness Foundation. 2026. Available online: https://worldhappiness.foundation/blog/consciousness/the-road-map-to-supraconsciousness-from-the-diagnosis-of-a-world-in-crisis-to-the-conscious-evolution-of-humanity/.
- Gallardo, L. M.; Chetri, S. Hypnosis as a mechanism of emotion regulation and self-integration: An integrative review of neural, cognitive, and experiential pathways to Fundamental Peace. Behavioral Sciences 2026, 16, 395. [Google Scholar] [CrossRef]
- Galtung, J. Violence, peace, and peace research. Journal of Peace Research 1969, 6, 167–191. [Google Scholar] [CrossRef]
- Gendlin, E. T. Focusing; Bantam Books, 1978. [Google Scholar]
- Goldberg, D. S.; McGee, S. J. Pain as a global public health priority. BMC Public Health 2011, 11, 1–5. [Google Scholar] [CrossRef]
- Goldberg, S. B.; Tucker, R. P.; Greene, P. A.; Davidson, R. J.; Wampold, B. E.; Kearney, D. J.; Simpson, T. L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clinical Psychology Review 2018, 59, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Gone, J. P. Redressing First Nations historical trauma: Theorizing mechanisms for indigenous culture as mental health treatment. Transcultural Psychiatry 2013, 50, 683–706. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, L. S. Emotion-focused therapy: Coaching clients to work through their feelings, 2nd ed.; American Psychological Association, 2015. [Google Scholar]
- Grof, S.; Grof, C. Spiritual emergency: When personal transformation becomes a crisis; Tarcher/Putnam, 1989. [Google Scholar]
- Hawkins, D. R. Power vs. force: The hidden determinants of human behavior; Hay House, 1995. [Google Scholar]
- Hawkins, D. R. Letting go: The pathway of surrender; Hay House, 2012. [Google Scholar]
- Hayner, P. B. Unspeakable truths: Transitional justice and the challenge of truth commissions, 2nd ed.; Routledge, 2010. [Google Scholar]
- Herman, J. L. Trauma and recovery: The aftermath of violence—from domestic abuse to political terror; Basic Books, 1992. [Google Scholar]
- Herman, J. L. Justice from the victim’s perspective. Violence Against Women 2005, 11, 571–602. [Google Scholar] [CrossRef]
- Hickman, C.; Marks, E.; Pihkala, P.; Clayton, S.; Lewandowski, R. E.; Mayall, E. E.; van Susteren, L. Climate anxiety in children and young people and their beliefs about government responses to climate change: A global survey. The Lancet Planetary Health 2021, 5, e863–e873. [Google Scholar] [CrossRef]
- Hillis, S. D.; Unwin, H. J. T.; Chen, Y.; Cluver, L.; Sherr, L.; Goldman, P. S.; Flaxman, S. Global minimum estimates of children affected by COVID-19-associated orphanhood and deaths of caregivers: A modelling study. The Lancet 2021, 398, 391–402. [Google Scholar] [CrossRef]
- Hirschberger, G. Collective trauma and the social construction of meaning. Frontiers in Psychology 2018, 9, 1441. [Google Scholar] [CrossRef]
- Hofmann, S. G.; Grossman, P.; Hinton, D. E. Loving-kindness and compassion meditation: Potential for psychological interventions. Clinical Psychology Review 2011, 31, 1126–1132. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T. B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspectives on Psychological Science 2015, 10, 227–237. [Google Scholar] [CrossRef]
- Hoppen, T. H.; Priebe, S.; Vetter, I.; Morina, N. The prevalence of PTSD and major depression in the global population of adult war survivors: A meta-analytically informed estimate in absolute numbers. European Journal of Psychotraumatology 2019, 10, 1578637. [Google Scholar] [CrossRef]
- Hoppen, T. H.; Priebe, S.; Vetter, I.; Morina, N. Global burden of post-traumatic stress disorder and major depression in countries affected by war between 1989 and 2019: A systematic review and meta-analysis. BMJ Global Health 2021, 6, e006303. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M. J. Stress response syndromes, 2nd ed.; Jason Aronson, 1986. [Google Scholar]
- Jiang, H.; White, M. P.; Greicius, M. D.; Waelde, L. C.; Spiegel, D. Brain activity and functional connectivity associated with hypnosis. Cerebral Cortex 2017, 27, 4083–4093. [Google Scholar] [CrossRef]
- Jung, C. G. The archetypes and the collective unconscious; Hull, R. F. C., Translator; Princeton University Press, 1959. [Google Scholar]
- Jung, C. G. Aion: Researches into the phenomenology of the self; Hull, R. F. C., Translator; Princeton University Press, 1968. [Google Scholar]
- Kellermann, N. P. F. Epigenetic transmission of Holocaust trauma: Can nightmares be inherited? Israel Journal of Psychiatry and Related Sciences 2013, 50, 33–39. [Google Scholar]
- Kessler, R. C.; Aguilar-Gaxiola, S.; Alonso, J.; Benjet, C.; Bromet, E. J.; Cardoso, G.; Koenen, K. C. Trauma and PTSD in the WHO World Mental Health Surveys. European Journal of Psychotraumatology 2017, 8(sup5), 1353383. [Google Scholar] [CrossRef]
- Kissane, D. W. The relief of existential suffering. Archives of Internal Medicine 2012, 172, 1501–1505. [Google Scholar] [CrossRef] [PubMed]
- Levine, P. A. Waking the tiger: Healing trauma; North Atlantic Books, 1997. [Google Scholar]
- Liotti, G. Trauma, dissociation, and disorganized attachment: Three strands of a single braid. Psychotherapy: Theory, Research, Practice, Training 2004, 41, 472–486. [Google Scholar] [CrossRef]
- Litz, B. T.; Stein, N.; Delaney, E.; Lebowitz, L.; Nash, W. P.; Silva, C.; Maguen, S. Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clinical Psychology Review 2009, 29, 695–706. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, Y.; Chen, S.; Zhang, J.; Wang, Z.; Lu, Q. The global burden of depression attributable to childhood sexual abuse, intimate partner violence, and bullying victimization from 1990 to 2021: An analysis based on the global burden of disease study. Annals of General Psychiatry 2025, 24, 1–12. [Google Scholar] [CrossRef]
- Louv, R. Last child in the woods: Saving our children from nature-deficit disorder; Algonquin Books, 2005. [Google Scholar]
- Lukoff, D. The diagnosis of mystical experiences with psychotic features. Journal of Transpersonal Psychology 1985, 17, 155–181. [Google Scholar]
- Lund, C.; Brooke-Sumner, C.; Baingana, F.; Baron, E. C.; Breuer, E.; Chandra, P.; Saxena, S. Social determinants of mental disorders and the Sustainable Development Goals: A systematic review of reviews. The Lancet Psychiatry 2018, 5, 357–369. [Google Scholar] [CrossRef]
- Lutz, A.; Greischar, L. L.; Rawlings, N. B.; Ricard, M.; Davidson, R. J. Long-term meditators self-induce high-amplitude gamma synchrony during mental practice. Proceedings of the National Academy of Sciences 2004, 101, 16369–16373. [Google Scholar] [CrossRef]
- Lutz, A.; Jha, A. P.; Dunne, J. D.; Saron, C. D. Investigating the phenomenological matrix of mindfulness-related practices from a neurocognitive perspective. American Psychologist 2015, 70, 632–658. [Google Scholar] [CrossRef]
- Macy, J.; Johnstone, C. Active hope: How to face the mess we’re in without going crazy; New World Library, 2012. [Google Scholar]
- Maté, G. the realm of hungry ghosts: Close encounters with addiction; Knopf Canada, 2008. [Google Scholar]
- Melzack, R.; Wall, P. D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Mubarak, A. R.; Bah, A. O.; Kargbo, A. T.; Barrie, M. S. Examining the tapestry of mental health crises in low- & middle-income countries: An intercontinental analysis of the contributing factors and instructive approaches. 2024. [Google Scholar] [CrossRef]
- Nijenhuis, E. R. S.; van der Hart, O. Dissociation in trauma: A new definition and comparison with previous formulations. Journal of Trauma & Dissociation 2011, 12, 416–445. [Google Scholar]
- Ogden, P.; Minton, K.; Pain, C. Trauma and the body: A sensorimotor approach to psychotherapy; W. W. Norton, 2006. [Google Scholar]
- Patel, V.; Kleinman, A. Poverty and common mental disorders in developing countries. Bulletin of the World Health Organization 2003, 81, 609–615. [Google Scholar]
- Perls, F. Gestalt therapy verbatim; Real People Press, 1969. [Google Scholar]
- Porges, S. W. The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation; W. W. Norton, 2011. [Google Scholar]
- Porges, S. W. The pocket guide to the polyvagal theory: The transformative power of feeling safe; W. W. Norton, 2017. [Google Scholar]
- Posner, M. I.; Rothbart, M. K. Research on attention networks as a model for the integration of psychological science. Annual Review of Psychology 2007, 58, 1–23. [Google Scholar] [CrossRef]
- Sabariego, C.; Oberhauser, C.; Posarac, A.; Bickenbach, J.; Kostanjsek, N.; Chatterji, S.; Cieza, A. Global mental health: Costs, poverty, violence, and socioeconomic determinants of health. In Handbook of disability and rehabilitation; Springer, 2017; pp. 371–388. [Google Scholar]
- SAMHSA. SAMHSA’s concept of trauma and guidance for a trauma-informed approach. In Substance Abuse and Mental Health Services Administration; 2014. [Google Scholar]
- Schwartz, R. C. Internal family systems therapy; Guilford Press, 1995. [Google Scholar]
- Schwartz, R. C. Introduction to the internal family systems model; Trailheads Publications, 2001. [Google Scholar]
- Schwartz, R. C. Moving from acceptance toward transformation with internal family systems therapy (IFS). Journal of Clinical Psychology 2013, 69, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Scranton, R. Learning to die in the Anthropocene: Reflections on the end of a civilization; City Lights Books, 2015. [Google Scholar]
- Shay, J. Achilles in Vietnam: Combat trauma and the undoing of character; Scribner, 1994. [Google Scholar]
- Shear, M. K. Complicated grief. New England Journal of Medicine 2015, 372, 153–160. [Google Scholar] [CrossRef]
- Siegel, D. J. The developing mind: How relationships and the brain interact to shape who we are, 2nd ed.; Guilford Press, 2012. [Google Scholar]
- Smith, C. P.; Freyd, J. J. Institutional betrayal. American Psychologist 2014, 69, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. SAMHSA’s concept of trauma and guidance for a trauma-informed approach 2014, HHS Publication No. (SMA), 14–4884.
- Tang, Y. Y.; Hölzel, B. K.; Posner, M. I. The neuroscience of mindfulness meditation. Nature Reviews Neuroscience 2015, 16, 213–225. [Google Scholar] [CrossRef]
- Taylor, C. A secular age; Harvard University Press, 2007. [Google Scholar]
- Tillich, P. The courage to be; Yale University Press, 1952. [Google Scholar]
- Turner, V. The ritual process: Structure and anti-structure; Aldine, 1969. [Google Scholar]
- van der Kolk, B. A. The body keeps the score: Brain, mind, and body in the healing of trauma; Viking, 2014. [Google Scholar]
- Traumatic stress: The effects of overwhelming experience on mind, body, and society; van der Kolk, B. A., McFarlane, A. C., Weisaeth, L., Eds.; Guilford Press, 1996. [Google Scholar]
- Volkow, N. D.; Koob, G. F.; McLellan, A. T. Neurobiologic advances from the brain disease model of addiction. New England Journal of Medicine 2016, 374, 363–371. [Google Scholar] [CrossRef]
- Whitbeck, L. B.; Adams, G. W.; Hoyt, D. R.; Chen, X. Conceptualizing and measuring historical trauma among American Indian people. American Journal of Community Psychology 2004, 33(3-4), 119–130. [Google Scholar] [CrossRef]
- WHO. Violence against women prevalence estimates, 2018; World Health Organization, 2021. [Google Scholar]
- Whorwell, P. J.; Prior, A.; Faragher, E. B. Controlled trial of hypnotherapy in the treatment of severe refractory irritable-bowel syndrome. The Lancet 1984, 324, 1232–1234. [Google Scholar] [CrossRef]
- Williams, D. R.; Mohammed, S. A. Racism and health I: Pathways and scientific evidence. American Behavioral Scientist 2013, 57, 1152–1173. [Google Scholar] [CrossRef]
- Yalom, I. D. Existential psychotherapy; Basic Books, 1980. [Google Scholar]
- Yalom, I. D. Staring at the sun: Overcoming the terror of death; Jossey-Bass, 2008. [Google Scholar]
- Yehuda, R.; Lehrner, A. Intergenerational transmission of trauma effects: Putative role of epigenetic mechanisms. World Psychiatry 2018, 17, 243–257. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



