Submitted:
04 April 2026
Posted:
06 April 2026
You are already at the latest version
Abstract
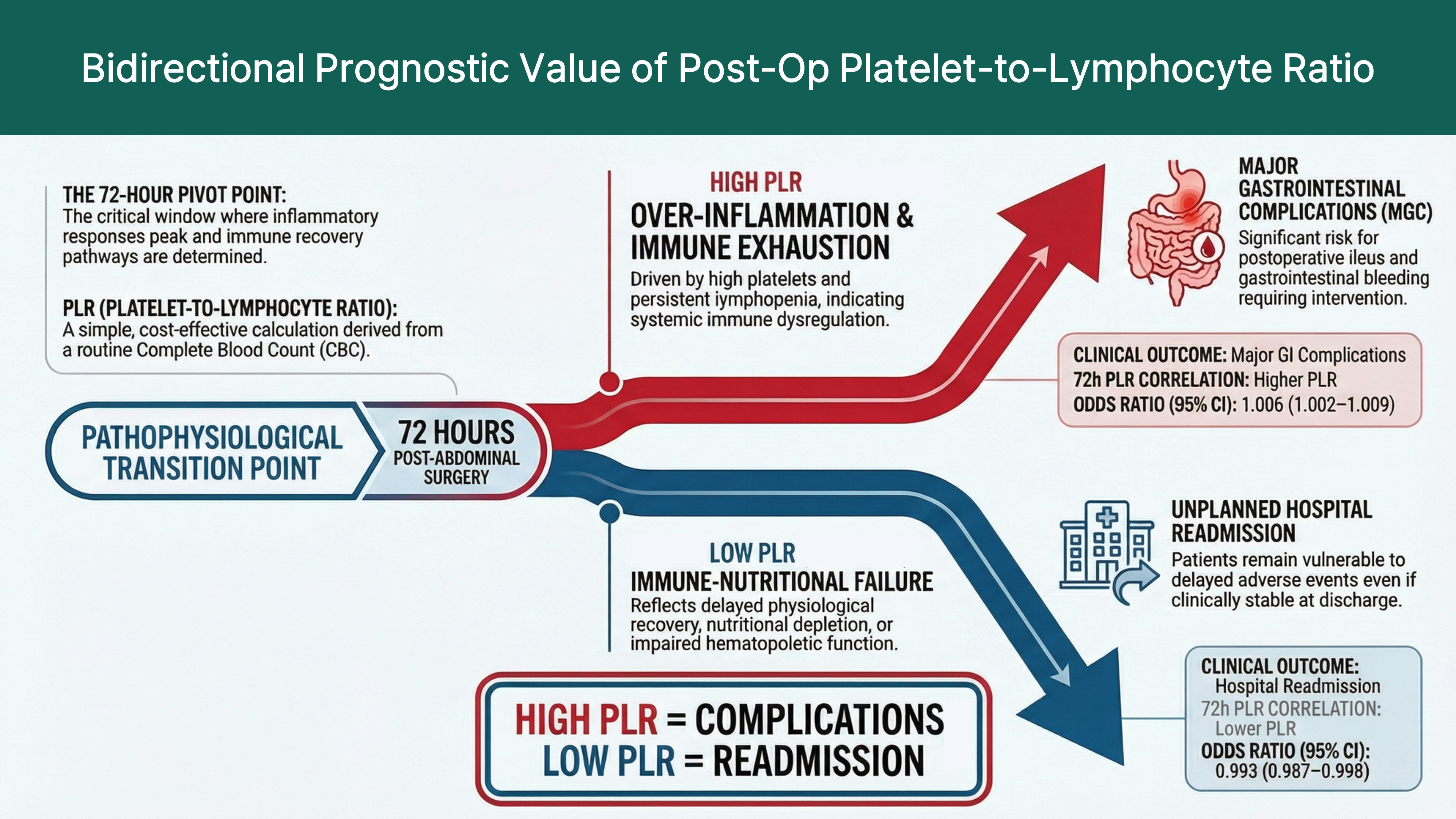
Background: Patients admitted to the intensive care unit (ICU) after major abdominal surgery are at high risk for gastrointestinal complications and unplanned hospital readmission. However, reliable and easily applicable biomarkers for early risk stratification are limited. This study evaluated the prognostic value of serial platelet-to-lymphocyte ratio (PLR) measurements in critically ill postoperative patients. Method: This retrospective observational study included adults admitted to the ICU after major abdominal surgery at a tertiary referral center between July 2020 and March 2025. The PLR was calculated from routine complete blood counts obtained at ICU admission and 24, 48, and 72 hours postoperatively. Multivariate logistic regression analysis was performed to identify the independent predictors of major gastrointestinal complications and hospital readmission rate. Results: Among 962 critically ill postoperative patients, nine (0.9%) developed major gastrointestinal complications. These patients had significantly higher disease severity scores and elevated PLRs at 72 hours postoperatively. In multivariate analysis, the PLR at 72 hours was an independent predictor of complications (odds ratio [OR] = 1.006; 95% confidence interval [CI]: 1.002–1.009). Conversely, a lower PLR at the same time point was independently associated with an increased risk of hospital readmission (OR = 0.993; 95% CI: 0.987–0.998). Conclusions: The postoperative PLR at 72 hours showed bidirectional prognostic value in critically ill patients after major abdominal surgery. Elevated PLRs were associated with major gastrointestinal complications, whereas lower PLRs were associated with hospital readmission. Thus, the PLR may serve as a practical biomarker for postoperative risk stratification and discharge decision-making in the ICU.
Keywords:
platelet-to-lymphocyte ratio
; critical illness
; Intensive care unit
; postoperative complications
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



