Submitted:
02 April 2026
Posted:
03 April 2026
You are already at the latest version
Abstract
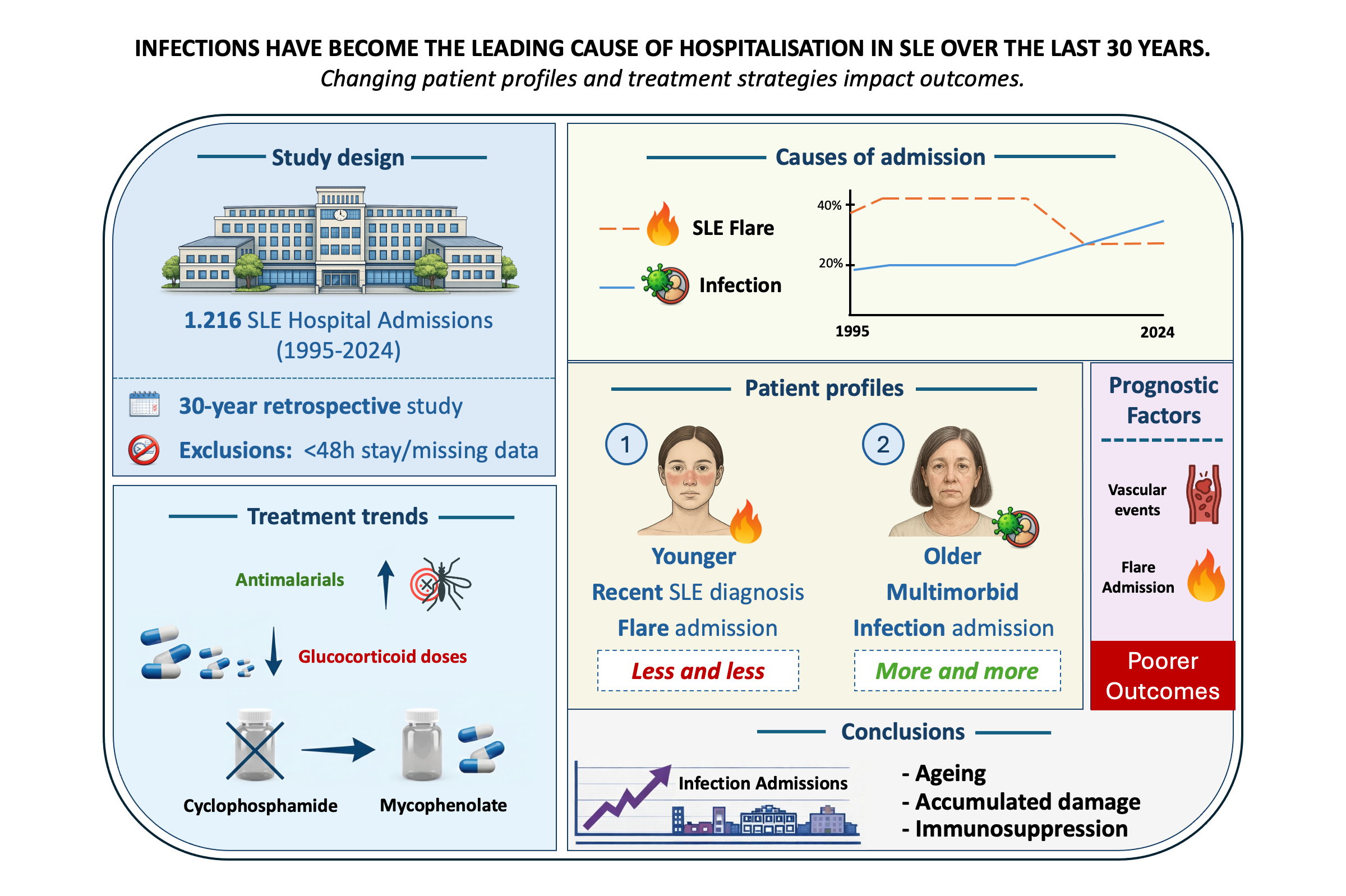
Background/Objectives: To analyse the causes, characteristics, and outcomes of hospital admissions in patients with systemic lupus erythematosus (SLE) over a 30-year period in a tertiary referral centre in Catalonia, and to evaluate temporal trends and prognostic factors associated with adverse outcomes. Methods: A retrospective observational study was conducted including all SLE patients admitted to the Department of Autoimmune Diseases at Hospital Clínic de Barcelona between June 1995 and December 2024. Admissions lasting less than 48 hours or lacking clinical documentation were excluded. Variables analysed included demographics, disease duration, comorbidities, cause of admission, treatments, and outcomes. A composite outcome was defined as intensive care unit (ICU) admission, 30-day readmission, or prolonged hospital stay. Statistical analyses included univariate and multivariate regression models. Results: Among the 1,216 hospital admissions, SLE flares and infections were the most frequent causes. Over the study period, admissions due to infections increased significantly and, in the last five years, exceeded those related to disease flares (33.7% vs. 26.1%). Patients hospitalized for flares were younger and had a shorter disease duration, whereas infection-related admissions were more common among older patients, those with overlap syndromes, and those with higher damage scores. Vascular events and SLE flares were independently associated with poorer outcomes. Although antimalarial use increased over time, it remained suboptimal, largely due to drug toxicity and newly diagnosed cases (from 45.2% to 69.7%; p< 0.001). Treatment strategies also evolved, with a shift toward lower gluco-corticoid doses (from 14.5% to 38.3%; p< 0.001), and mycophenolate mofetil replacing cyclophosphamide as the preferred immunosuppressive agent. Conclusions: Hospitalisation patterns in SLE have shifted over time, with infections emerging as the leading cause of admission. This trend reflects an evolving patient profile characterized by older age, greater accumulated damage, comorbidities, and increased exposure to immunosuppressive therapies. These findings underscore the need for optimized infection prevention strategies and individualized treatment approaches to improve outcomes in contemporary SLE care.
Keywords:
flare
; hospitalisation
; infection
; systemic lupus erythematosus
; trends
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



