Submitted:
31 March 2026
Posted:
01 April 2026
You are already at the latest version
Abstract
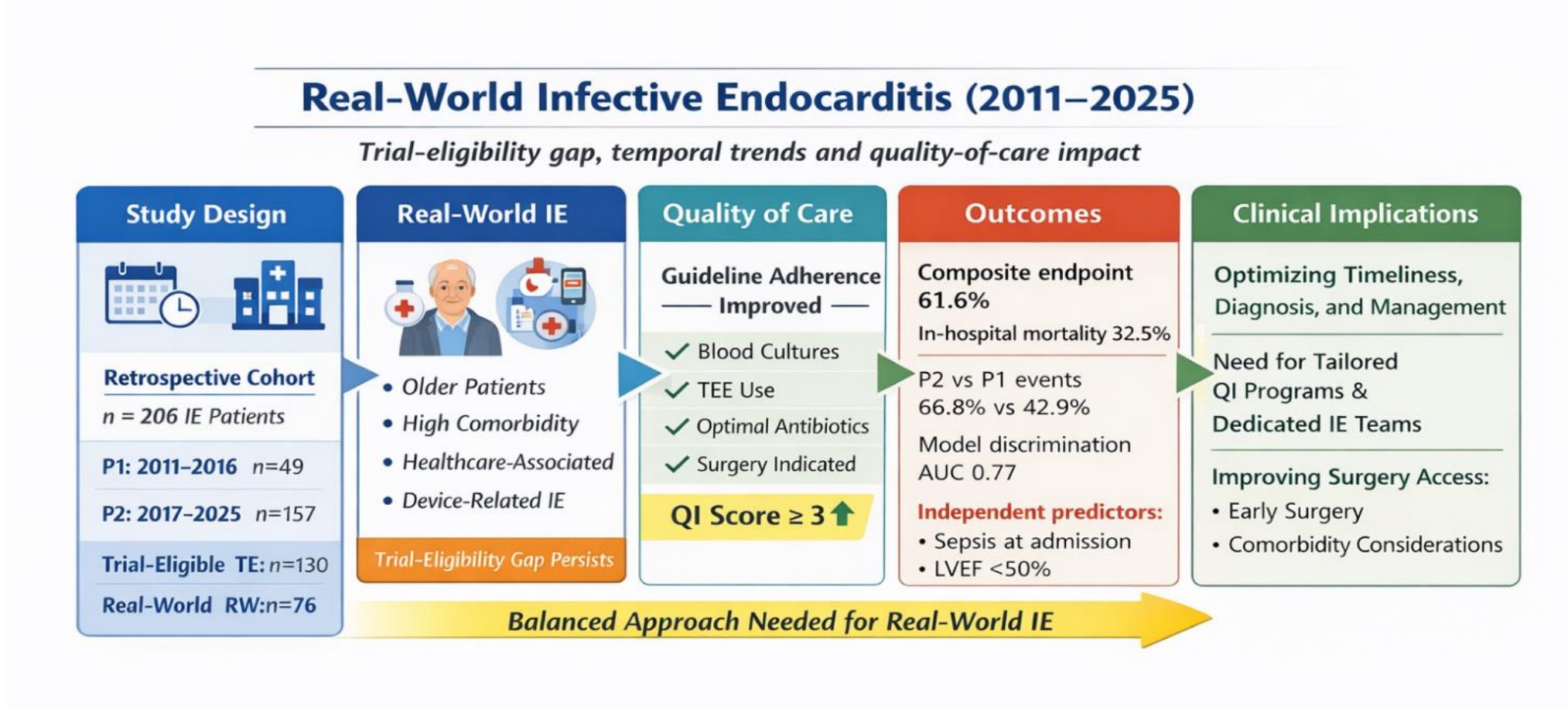
Background and Objectives: Infective endocarditis (IE) remains associated with high mortality, and real-world (RW) patients often differ from trial populations. We evaluated predictors of complications and mortality, the trial-eligibility gap, and temporal trends in guideline adherence across two periods (P1 2011–2016 vs P2 2017–2025) in a Romanian county hospital. Materials and Methods: We performed a retrospective analysis of consecutive adult patients with definite IE. Patients were categorized as trial-eligible (TE) or RW according to predefined criteria. The composite endpoint comprised acute heart failure, cardiogenic or septic shock, embolic events, infectious complications, need for renal replacement therapy, and in-hospital mortality. Guideline adherence was evaluated using a predefined quality indicator (QI) score ≥3. Independent predictors of outcome were identified using multivariable logistic regression. Results: Among 206 patients (mean age 63.0 ± 14.8 years; 70.4% male), blood cultures were positive in 64.1%, with Staphylococcus aureus accounting for 14.1%. Vegetations were documented in 72.8%, and cardiac surgery was performed in 26.2%. Overall, at least one event from the composite endpoint occurred in 61.6 %, and mortality was 32.5%. TE patients represented 63.1% of the cohort. Guideline adherence improved over time (QI ≥3: from 18.3% in P1 to 25.4% in P2 p=0.32). In the P2 period, the composite endpoint (66.8 % vs. 42.9%, p=0.002) and embolic events (31.8% vs. 8.2%, p< 0.001) were more frequent, whereas mortality remained unchanged (31.8% vs. 34.7%, p=0.844). Sepsis at admission and left ventricular ejection fraction < 50% independently predicted adverse outcomes; model discrimination was acceptable with an area under the curve (AUC) =0.77. Conclusions: Real-world IE showed high complication rates and a persistent trial gap; improved guideline adherence was counterbalanced by greater clinical severity.
Keywords:
infective endocarditis
; real-world evidence
; in-hospital mortality
; prognostic factors
; guideline adherence
; trial eligibility
; observational study
; microbiology
; complications
1. Introduction
Infective endocarditis (IE) remains a complex disease associated with substantial morbidity and mortality. Despite advancements in diagnostic techniques, microbiology, antimicrobial therapy, and cardiac surgery over recent decades, outcomes remain unsatisfactory. Contemporary data estimate an age-standardized incidence of approximately 10–15 cases per 100,000 person-years, with in-hospital mortality frequently exceeding 15–30% and one-year mortality approaching 40% in some studies [1,2]. The 2015 European society of Cardiology (ESC) guidelines marked a significant milestone by introducing structured quality indicators for blood culture acquisition, early multimodal imaging, multidisciplinary evaluation, and surgical timing, thereby facilitating better comparability of patient management [3]. The 2023 update reinforced the role of Endocarditis Teams, modern imaging, and optimized surgical pathways, while acknowledging that many recommendations still rely on limited-quality evidence [1,3,4]. In this context, observational studies are essential for documenting how IE is managed in routine practice. Large registries and national initiatives have highlighted important epidemiological shifts, including increased patient age, a higher burden of comorbidities, and a growing proportion of infections caused by Staphylococcus aureus, enterococci, and prosthetic valve/device-related pathogens [2,5,6,7]. Registry-based efforts, such as a nationwide consortium of endocarditis teams (ENDOCOR) in the Netherlands, illustrate attempts to integrate routine data collection and quality monitoring into clinical workflows [8](8). However, most published cohorts originate from tertiary centers, and certain regions of Europe, including Eastern Europe, remain underrepresented [2]. Differences between tertiary referral centers and regional hospitals, particularly in case mix, access to cardiac surgery, imaging resources, and multidisciplinary infrastructure—have also been noted [2,6]. Another area of increasing interest is the discrepancy between patients who could realistically enroll in randomized controlled trials (RCTs) and those treated in routine clinical practice. Only a minority of therapeutic questions in IE are informed by robust randomized evidence. Recent work on partial oral therapy illustrates this issue: pivotal trials enrolled highly selected patients, while analyses of routine practice populations suggest that many real-world (RW) cases would not have met eligibility criteria, despite demonstrating acceptable outcomes [9,10,11]. This “trial eligibility gap” largely reflects the exclusion of elderly, frail, or comorbid patients, as well as those with prosthetic valves, right-sided IE, or active drug use—groups commonly encountered in routine practice [6,9,12,13]. Recent Romanian studies have provided valuable insights. A retrospective cohort from Iași (2019–2024) reported a high proportion of positive blood cultures (84%) and a microbiological profile dominated by S. aureus, E. faecalis, and viridans streptococci, with in-hospital mortality around 5% [14]. A related analysis underscored challenges in identifying fastidious organisms [15]. A Bucharest cohort focusing on people who inject drugs (PWID) found major differences compared to non-PWID, including younger age, right-sided involvement, larger vegetations, S. aureus predominance, and higher one-year mortality [16]. Another series examining prosthetic valve IE documented high rates of late-onset infection, predominance of S. aureus/enterococci, relatively low surgical intervention rates, and in-hospital mortality exceeding one-third of cases [17]. Although these reports are valuable, they primarily originate from tertiary care settings and often target specific phenotypes [18]. Several knowledge gaps remain: international and Romanian cohorts rarely compare trial-eligible (TE) and RW patients, quantify the proportion meeting RCT criteria, or evaluate adherence to guideline-based quality indicators. Guideline documents consistently emphasize timely blood cultures, early echocardiography (both transthoracic and transesophageal), multidisciplinary evaluation, surgical decision-making, and appropriate antimicrobial therapy [1,3,4]. These aspects are particularly relevant for county hospitals, which often serve as first-contact facilities for complex cases and must coordinate care when cardiac surgery is not available on-site. Regional centers typically manage an unselected IE population, including older patients with multiple comorbidities, delayed presentations, or limited social support. Referral patterns, diagnostic delays, and surgical access may also differ from those in tertiary environments. The 2011–2025 period encompasses major changes in guideline recommendations, the establishment of Endocarditis Teams, wider use of advanced imaging, and the progressive acceptance of partial oral therapy [1,3,4,6]. Examining how these developments have been implemented in daily practice and their impact on outcomes at the county level is of both clinical and health system interest. The objectives of the present study are: (i) to describe the clinical, microbiological, and echocardiographic features of adults with definite IE treated at a Romanian county hospital from 2011 to 2025; (ii) to identify factors associated with a composite endpoint comprising acute heart failure, shock, major embolic events, severe infectious complications, renal replacement therapy, and/or in-hospital death; (iii) to distinguish between patients who meet contemporary RCT eligibility criteria and those representing RW practice; and (iv) to assess temporal changes in guideline-concordant management by comparing two time intervals (2011–2016 vs. 2017–2025). By contextualizing county-level data within guideline standards and RCT eligibility, this study aims to complement existing evidence and highlight practical considerations for improving IE care in similar settings.
2. Methods
2.1. Study Design
This retrospective, single-center observational cohort study involved adult patients diagnosed with definite IE. The research was conducted in the Department of Cardiology and Cardiovascular Intensive Care at the “Dr. Constantin Opriș” Emergency County Hospital in Baia Mare, Romania, a secondary/tertiary referral institution providing interventional cardiology services at the regional level. Two predefined intervals were analyzed: Period 1 (P1): 01.01.2011–31.12.2016 and Period 2 (P2): 01.01.2017–31.12.2025. Transesophageal echocardiography (TEE) was systematically implemented after 2016, and an on-site cardiac surgery program became operational in 2023. The study protocol was reviewed and approved on 02/02/2026 (decision 4979) by the Institutional Review Ethics Committee of “Dr. Constantin Opriș” Emergency County Hospital, Baia Mare. Given the retrospective design, the use of routinely collected clinical data, and anonymization prior to analysis, the requirement for individual informed consent was waived in accordance with national regulations and institutional policies. The study adhered to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines for cohort and observational studies [19].
2.2. Study Population
All consecutive adults (≥18 years) hospitalized with suspected IE during the study period were screened. Inclusion required fulfillment of definite IE according to the modified Duke criteria (ESC 2015) and the updated ESC 2023 definitions [1,3,20]. For individuals with multiple admissions, only the index episode was considered. Inclusion criteria were age ≥18 years, definite IE diagnosis, and availability of clinical, microbiological, and echocardiographic data. Exclusion criteria included possible or rejected IE diagnosis, transfer in/out within <24 hours with insufficient data, and isolated catheter-related right-sided infections lacking essential diagnostic information.
2.3. Variables and Data Sources
Data were abstracted from digital records, microbiology databases, echocardiography archives, and discharge documentation. Variable domains were grouped into predefined domains. Demographics and comorbidity burden included age, sex, and a global comorbidity burden defined as the cumulative number of major chronic conditions [hypertension (HTN), diabetes mellitus (DM), chronic heart failure (HF), chronic kidney disease (CKD), malignancy, liver cirrhosis, and coronary artery disease (CAD)]. Clinical presentation and severity variables encompassed symptom duration, fever, acute heart failure, sepsis at admission, requirement for vasopressors, and need for invasive mechanical ventilation. Microbiological variables included the number and timing of blood cultures, causative pathogens (with specific categorization of S. aureus, Enterococcus spp., and Streptococcus viridans), and culture-negative IE. Imaging and anatomical variables comprised the timing of transthoracic echocardiography (TTE) and TEE, valve involvement (native vs. prosthetic), right-sided involvement, vegetation size ≥10 mm, severe valvular regurgitation, perivalvular complications (abscess or fistula), and left ventricular ejection fraction (LVEF) <50%. Management variables included antimicrobial regimens, timing of surgery, patient transfers, and multidisciplinary evaluations. Outcome variables consisted of a composite endpoint, in-hospital mortality, renal replacement therapy, embolic events, and length of hospital stay. Case selection and data validation were performed by two independent investigators, with discrepancies adjudicated by a senior cardiologist.
2.4. Definitions and Endpoints
Cardiogenic shock (CS) was defined according to the Shock Academic Research Consortium (SHARC) expert panel criteria [21]. Septic shock was defined based on the Sepsis -3 criteria [22]. Sepsis at admission was defined according to the Sepsis-3 criteria as suspected or confirmed infection associated with acute organ dysfunction (increase in SOFA score ≥2 points) present at hospital presentation. In retrospective cases where complete SOFA variables were unavailable, clinically documented organ dysfunction (hypotension, acute kidney injury, respiratory insufficiency, altered mental status, thrombocytopenia, or elevated lactate) was considered consistent with sepsis [22]. The primary outcome was a composite in-hospital endpoint, defined as the occurrence of at least one of the following events: acute heart failure requiring intravenous therapy or ventilatory support, shock (cardiogenic and/or septic), embolic events symptomatic or confirmed by imaging or surgery, severe infectious complications (such as abscess, fistula, or metastatic infection), renal replacement therapy, and all-cause in-hospital mortality. Secondary outcomes included analysis of individual components and length of hospital stay.
2.5. Classification of Trial-Eligible vs. Real-World Patients
To evaluate the gap between RCT-eligible and routine-practice populations, patients were classified as TE if they fulfilled predefined clinical stability and selection criteria derived from contemporary IE trials and guideline-based frameworks [1,3,4,9]. Eligibility required the absence of the following conditions: age >80 years, persistent shock, prolonged invasive mechanical ventilation, active malignancy with an estimated life expectancy <1 year, end-stage renal disease (ESRD) and/or chronic dialysis, refractory heart failure, uncontrolled infection (such as perivalvular abscess or persistent bacteremia), or device-related IE requiring urgent extraction. All other patients were classified as RW patients.
2.6. Quality Indicators and Guidelines Adherence
Quality indicators were based on international guideline recommendations and included 4 indicators: 1) adequate blood culture (≥2 blood culture sets prior to antibiotics), 2) TEE performed when indicated in accordance with guideline-based diagnostic indications, 3) appropriate antimicrobial therapy (guideline-concordant initial antibiotics combined with adequate duration antimicrobial therapy according to microbiological data when available), 4) multidisciplinary evaluation (Heart Team) followed by cardiac surgery when indicated (Class I/IIa) or documented contraindication [1,3,4,23]. For each patient, a guideline adherence score (0–4) was computed as the sum of fulfilled indicators. We then calculated the number of fulfilled indicators (0–4) and defined overall guideline adherence as achieving a pre-specified threshold of ≥3 out of 4 indicators.
3. Statistical Analysis
Continuous variables were described as mean ± standard deviation (SD) or median (interquartile range), depending on their distribution. Group comparisons were performed using the Student’s t-test or the Mann–Whitney U test for continuous data, and the χ2 test or Fisher’s exact test for categorical data. Univariable analyses were conducted to identify factors associated with the composite outcome and in-hospital mortality. Variables with p<0.10, along with clinically relevant covariates, were included in multivariable logistic regression models. Results are presented as odds ratios with 95% confidence intervals. Model performance was assessed using the Hosmer–Lemeshow test and receiver operating characteristic (ROC) curves; collinearity was examined through variance inflation factors. Comparisons between TE and RW patients, as well as between the two-time intervals (P1: 2011–2016 vs. P2: 2017–2025), included baseline characteristics, quality indicators, and outcomes. For the composite endpoint and mortality, adjusted analyses were performed using logistic regression models that included age, sex, comorbidity burden, pathogen, and prosthetic/device-related status. All tests were two-sided, and p<0.05 was considered statistically significant. All statistical analyses were performed using R version 4.4.0 (2024-04-24 ucrt) – “Puppy Cup” [24].
4. Results
4.1. Study Population
Between 2011 and 2025, 221 patients were admitted with suspected IE. After diagnostic verification and the exclusion of non-definite cases, early transfers, and incomplete records, 206 adults with definite IE were included. Of these, 130 (63.1%) met predefined trial eligibility criteria and were classified as TE, while 76 (36.9%) represented RW patients. Temporal stratification identified 49 patients in Period 1 (2011–2016) and 157 in P2 (2017–2025). The study flow is illustrated in Figure 1.
4.2. Baseline Characteristics According to Trial Eligibility
Baseline characteristics are summarized in Table 1. RW patients were older than TE patients (68.3±12.1 vs. 59.9±15.4 years, p<0.001), representing an absolute difference of approximately eight years. Male sex predominated overall but was more frequent in the TE cohort (78.5% vs. 56.6%, p=0.002). The most common cardiovascular comorbidities were similarly distributed. HTN, DM, chronic HF, chronic obstructive pulmonary disease (COPD), and liver cirrhosis did not differ significantly between groups. CKD was more frequent in RW patients (34.2% vs. 18.5%, p=0.01), while malignancy occurred exclusively in RW patients, reflecting eligibility criteria. Infection location was predominantly left-sided in both groups (>95%). Device-related endocarditis showed a clear imbalance: cardiac implantable electronic device (CIED)-related IE was more common in RW patients (26.3% vs. 9.2%, p=0.001), and transcatheter aortic valve implantation (TAVI)-associated IE occurred only in this cohort. Microbiological patterns were broadly comparable, although Enterococcus spp. were more frequent in RW patients (21.1% vs. 7.7%, p=0.01). Culture-negative cases were similarly distributed. Echocardiographic findings were largely similar except for a higher rate of perivalvular abscess in TE patients (27.7% vs. 13.2%, p=0.02). Vegetation size and ventricular systolic function did not differ. Markers of acute severity were more prominent in RW patients. Sepsis at admission occurred twice as often (38.2% vs. 17.7%, p=0.002), and septic shock was markedly more frequent (19.7% vs. 1.5%, p<0.001). CS and acute heart failure showed no significant differences. Clinical outcomes were similar between groups for the composite endpoint and in-hospital mortality. However, major embolic events were more frequent in RW patients (35.5% vs. 20.8%, p=0.02). Length of stay did not differ significantly (12.6±11.1 vs. 13.5±10.2 days, p=0.331).
4.3. Temporal Trends Between Study Periods
Comparisons between study periods are presented in Table 2. The later cohort included a higher proportion of RW patients (p=0.002), indicating a shift toward more complex clinical profiles over time. Age and sex distribution remained stable. Device-related infections increased in P2, particularly CIED-associated cases. Diagnostic practices evolved substantially, with TEE used more frequently in the later period (p=0.01). Larger vegetations were documented more often in the earlier period and are concordant with more embolic events. Markers of clinical severity were more prevalent in P2, with higher rates of septic shock and CS. The composite endpoint increased (66.8% vs. 42.9%, p=0.002), mainly by septic complications and CS/acute HF. In-hospital mortality remained unchanged. Length of stay increased significantly in P2 (14.4±11.5 vs. 8.2±6.0 days, p=0.002).
4.4. Prediction of the Composite Endpoint
An univariable screening analysis identified markers of acute clinical severity, cardiac dysfunction, and structural complications as the strongest correlates of the composite in-hospital endpoint. Sepsis at admission, acute heart failure, CS, LVEF <50%, and perivalvular complications (abscesses) were each associated with higher event rates. The microbiological category also demonstrated prognostic relevance, whereas demographic variables showed weak or inconsistent associations – Table 3. Variables meeting statistical or clinical relevance criteria were entered into a multivariable logistic regression model. The final model confirmed sepsis at admission as the strongest independent predictor, followed by reduced LVEF < 50% and streptococcal infection, while prosthetic/device-related IE showed a protective trend - Table 4. Model discrimination was acceptable, with an AUC of 0.77, and calibration demonstrated agreement between predicted and observed outcomes (Figure 2 and Figure 3).
4.5. Quality Indicators and Outcome Linkage
Quality of care improved substantially over time. The proportion of patients achieving QI score ≥3 increased from 18.3% in P1 to 25.4% in P2 (OR 1.63, p=0.32), with a similar trend toward higher attainment in TE vs RW patients (26.9% vs 18.4%, OR 2.23, p=0.05). Marked improvements were observed for key diagnostic and therapeutic processes: adequate blood cultures increased from 34.7% to 73.2% (OR 5.14, p<0.001); TEE when indicated increased from 18.3% to 51.5% (OR 4.72, p=0.001); appropriate antimicrobial therapy increased from 32.7% to 73.9% (OR 5.86, p<0.001); surgery when indicated increased from 12.2% to 30.5% (OR 3.18, p=0.01). Differences between TE and RW patients were modest for individual indicators and not statistically significant - Table 5.
5. Discussion
To our knowledge, this is the first long-term study from Eastern Europe to jointly analyze real-world IE characteristics, RCT eligibility, guideline adherence and temporal outcome trends in a county hospital setting. Several key findings emerge, underscoring the utility and practical significance of our research. First, the cohort illustrates the increasing clinical complexity of IE, with a substantial proportion of patients presenting characteristics not typically represented in randomized trials. Second, adherence to guideline-based quality indicators improved significantly over time. Third, despite these improvements in process-of-care measures, the incidence of major in-hospital complications increased, reflecting a shift toward a more severe case mix rather than a decline in the quality-of-care delivery. The demographic and clinical differences between TE and RW patients resemble the patterns described in large observational registries, where aging populations, device-related infections, and comorbidity burden have reshaped IE epidemiology [6,7,25,26,27]. Only a subset of patients (63.1%) met predefined criteria approximating enrollment in contemporary randomized IE trials. This observation parallels analyses of trial cohorts such as The Partial Oral Treatment of Endocarditis (POET), where strict inclusion criteria systematically exclude older, unstable, or highly comorbid patients [9,10]. Similar discrepancies have been reported in registry comparisons, with RW populations demonstrating higher complication rates than trial cohorts [25,26,27,28,29].
The ESC- EURObservational Research Programme (EORP) European Endocarditis (EURO-ENDO) registry (ESC-EORP EURO-ENDO), a large prospective cohort comprising over 3,000 patients with IE from 156 centers across 40 countries, provides the most comprehensive contemporary data on epidemiology, management, and outcomes. In-hospital mortality was reported at approximately 17%, with notable representation of staphylococcal, enterococcal, prosthetic valve, and device-related infections [30,31,32]. In contrast, in-hospital mortality in our cohort (32.5%) appears higher than that reported in EURO-ENDO registry but remains within the range observed in contemporary high-severity RW series (approximately 25–30%) and is comparable to prior Romanian hospital cohorts reporting mortality approaching one-third of cases [16,17,18,26,30,31,32,33]. This difference is largely explained by case mix and clinical profile at presentation. A substantial proportion of our RW patients presented with sepsis or shock, conditions consistently identified as dominant short-term mortality drivers in IE [22,26,34,35]. Additionally, our cohort reflects the ongoing epidemiologic transition toward older, more comorbid populations with a higher burden of prosthetic or device-related infections—patterns associated with increased early clinical risk in observational studies [30,33]. Finally, regional system factors, particularly the timing and feasibility of surgery or device extraction (a cardiovascular surgery program initiated at our hospital in 2023)—may influence early outcomes, as observational data repeatedly demonstrate improved survival in high-risk subgroups when timely surgical management is achieved [36,37]. Our findings underscore the importance of interpreting outcome metrics within RW epidemiologic and organizational frameworks.
The temporal comparison between the P1 and P2 periods in our cohort reveals a pattern increasingly recognized in contemporary IE research: advances in structured care occur alongside a rising burden of clinical complexity. Patients in the later period (P2) demonstrated significantly higher adherence to quality indicators outlined in ESC guidelines, including broader use of TEE, routine microbiological sampling, and multidisciplinary evaluation. These improvements likely enhanced diagnostic precision and pathway consistency [23,30,33]. Simultaneously, the P2 group included a greater proportion of device-associated infections and septic presentations, both independently linked to more severe clinical courses and higher complication rates in registry analyses [30,33]. The observation that in-hospital mortality remained relatively stable despite an increase in serious complications suggests that improvements in care processes may have partially mitigated the impact of rising biological severity. This contrast highlights that adherence metrics primarily reflect the quality-of-care delivery, whereas short-term outcomes remain strongly influenced by baseline disease burden. Importantly, this temporal pattern mirrors differences observed between TE and RW populations: process adherence is necessary but insufficient to overcome the prognostic weight of acute severity markers. These longitudinal findings align with European registry data showing that coordinated diagnostic and management pathways are associated with improved process measures and more consistent early care [32,33].
Multivariable analysis identified sepsis at presentation, LVEF <50%, and streptococcal infection as independent predictors of the composite in-hospital endpoint. This pattern aligns with established prognostic frameworks in IE, where acute systemic inflammatory response and cardiac functional reserve are stronger determinants of early outcomes than baseline demographic characteristics. The persistence of microbiological category as an independent factor suggests that pathogen-specific virulence and tissue invasion significantly influence complication risk. In contrast, age and sex did not retain independent predictive value after adjustment, indicating that these variables primarily serve as background vulnerability markers rather than direct drivers of short-term events. Similarly, the apparent attenuation of risk associated with prosthetic or device-related infection and certain microbiological subtypes (such as staphylococcal infection in our study) should not be interpreted as biological protection. Rather, once dominant severity markers such as sepsis and ventricular dysfunction are accounted for, contextual characteristics lose independent statistical significance. This reflects model adjustment within a heterogeneous clinical population, not a reduction in clinical risk. Variables marked with dashes in Table 3—including CS, acute heart failure, and perivalvular abscess—were examined but not retained in the final model because they did not add independent predictive information after adjustment for overlapping severity indicators. Their exclusion represents statistical optimization rather than clinical irrelevance, as these features remain integral components of the composite endpoint and overall disease severity. Importantly, the multivariable findings align with descriptive cohort patterns. The same markers that differentiated TE from RW patients—particularly sepsis and impaired ventricular function—were those most strongly associated with adverse outcomes. From a practical perspective, the identified predictors are readily available at admission and therefore useful for early risk stratification. Recognition of sepsis and ventricular dysfunction should prompt intensified monitoring, rapid antimicrobial optimization, and early surgical assessment when appropriate. The model demonstrated acceptable discrimination (AUC=0.77), comparable to performance reported in observational IE prognostic studies, supporting its applicability to RW clinical decision-making rather than highly selected trial populations [38,39,40].
Our study demonstrates a substantial temporal improvement in key quality indicators of IE management, particularly regarding microbiological diagnosis, systematic use of TEE and implementation of guideline-directed antimicrobial therapy. These changes likely reflect increasing adherence to ESC recommendations and improved local diagnostic infrastructure, including broader access to TEE after 2016. Importantly, differences between TE and RW patients were limited, indicating that improvements in care delivery extended beyond selected lower-risk populations. The marked increase in blood culture adequacy and TEE utilization is clinically relevant, as both are strongly linked to diagnostic accuracy, embolic risk stratification and appropriate surgical referral. Similarly, the higher proportion of patients receiving appropriate antimicrobial therapy and surgery when indicated suggests improved integration of cardiology, infectious diseases and cardiac surgery teams. Taken together, these findings support a progressive alignment of real-world practice with guideline-recommended care pathways, while highlighting the persistent gap in achieving high composite QI scores in all patients.
Overall, this county-level cohort reflects the epidemiologic transition of IE described in contemporary registries, characterized by older patients with more comorbidities and an increasing prevalence of prosthetic and CIED related infections. While the microbiological patterns align with international data, the greater clinical severity observed in a regional hospital setting highlights the heterogeneity of RW IE beyond tertiary referral centers. These emphasize that regional cohorts provide essential complementary insights into disease burden, care delivery, and complication patterns. Therefore, interpreting outcomes within this broader clinical and organizational context is crucial when applying registry and trial data to everyday clinical practice.
6. Study Strengths and Limitations
This study has several strengths. Consecutive patient inclusion using standardized diagnostic criteria reduced selection bias and ensured internal consistency. The integration of clinical, microbiological, imaging and process-of-care variables allowed a comprehensive evaluation of IE, while the combined assessment of temporal trends, trial eligibility, guideline adherence and outcomes provided a multidimensional perspective. Independent case adjudication further supported data reliability. Limitations should also be considered. The retrospective single-center design exposes the analysis to potential information bias, residual confounding and limited external generalizability. Temporal differences may partly reflect changes in referral patterns and case mix. The prediction model was internally derived and not externally validated; therefore, results should be interpreted as exploratory associations rather than causal effects. Some clinically relevant variables were excluded from multivariable analysis due to collinearity or instability, and certain endpoints relied on routine clinical documentation, potentially introducing classification variability.
7. Future Directions
Future research should focus on multicenter validation of process-based quality indicators and prospective assessment of risk stratification in routine practice. Strengthening multidisciplinary care pathways and developing interoperable digital registries integrating imaging, microbiological and outcome data may improve clinical decision-making and benchmarking across centers. Particular attention should be given to underrepresented populations in clinical trials, especially older patients and those with device-related IE, to better align management strategies with real-world complexity.
8. Conclusions
Real-world IE is characterized by high complication burden and a persistent trial-eligibility gap. Although adherence to guideline-based care improved over time, increasing clinical severity likely attenuated potential gains in outcomes, underscoring the need for pragmatic, multidisciplinary management strategies adapted to real-world patient complexity.
Key Messages
- RW IE patients differ substantially from RCT populations.
- Guideline adherence improved markedly over time.
- Complication burden increased due to greater severity.
- Mortality remained stable despite higher clinical complexity.
- Early severity markers predict in-hospital outcomes.
- Structured care pathways support consistent management.
- ESC quality indicator adherence is achievable in regional hospitals.
- Regional registries complement tertiary sources of evidence.
Author Contributions
C.P wrote the first draft of the manuscript. C.P, L.L.P, LP and I.P. contributed to the critical revision of the manuscript for important intellectual content and confirmed the integrity of the work. CP, M.R.P, A.I.T, R.H and AMF contributed to the review & editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee (registration no. 4979; on 02/02/2026).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current outline of advances in our field of expertise.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Delgado, V.; Ajmone Marsan, N.; De Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the Management of Endocarditis. European Heart Journal 2023, 44, 3948–4042. [Google Scholar] [CrossRef]
- Ambrosioni, J.; Hernández-Meneses, M.; Durante-Mangoni, E.; Tattevin, P.; Olaison, L.; Freiberger, T.; Hurley, J.; Hannan, M.M.; Chu, V.; Hoen, B.; et al. Correction: Epidemiological Changes and Improvement in Outcomes of Infective Endocarditis in Europe in the Twenty-First Century: An International Collaboration on Endocarditis (ICE) Prospective Cohort Study (2000–2012). Infect. Dis. Ther. 2023, 12, 2819–2821. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the Management of Infective Endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC)Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015, 36, 3075–3128. [Google Scholar] [CrossRef]
- McDonald, E.G.; Aggrey, G.; Aslan, A.T.; Casias, M.; Cortes-Penfield, N.; Dong, M.Q.; Egbert, S.; Footer, B.; Isler, B.; King, M.; et al. Guidelines for Diagnosis and Management of Infective Endocarditis in Adults: A WikiGuidelines Group Consensus Statement. JAMA Netw Open 2023, 6, e2326366. [Google Scholar] [CrossRef]
- Pericàs, J.M.; Ambrosioni, J.; Muñoz, P.; De Alarcón, A.; Kestler, M.; Mari-Hualde, A.; Moreno, A.; Goenaga, M.Á; Fariñas, M.C.; Rodríguez-Álvarez, R.; et al. Prevalence of Colorectal Neoplasms Among Patients With Enterococcus Faecalis Endocarditis in the GAMES Cohort (2008–2017). Mayo Clinic Proceedings 2021, 96, 132–146. [Google Scholar] [CrossRef]
- Cimmino, G.; Bottino, R.; Formisano, T.; Orlandi, M.; Molinari, D.; Sperlongano, S.; Castaldo, P.; D’Elia, S.; Carbone, A.; Palladino, A.; et al. Current Views on Infective Endocarditis: Changing Epidemiology, Improving Diagnostic Tools and Centering the Patient for Up-to-Date Management. Life 2023, 13, 377. [Google Scholar] [CrossRef]
- Ha, K.E.; Kim, W.D.; Ko, K.-Y.; Kim, H.; Gwak, S.-Y.; Kim, K.; Lee, H.-J.; Shim, C.Y.; Hong, G.-R.; Ha, J.-W.; et al. Trends in Epidemiology, Clinical Characteristics, and Outcomes of Infective Endocarditis: A 16-Year Nationwide Cohort Study in Korea. J. Korean Med. Sci. 2025, 40, e183. [Google Scholar] [CrossRef] [PubMed]
- Peijster, A.J.L.; Heinen, F.J.; Douiyeb, S.; Van Der Stoel, M.D.; Selder, J.L.; Watson-de Lepper, A.G.W.; Houthuizen, P.; Meijs, M.F.L.; Kampschreur, L.M.; Schalla, S.; et al. ENDOCOR: A Nationwide Consortium of Endocarditis Teams—Initiating a Registry for Infective Endocarditis within the Netherlands Heart Registration. Neth Heart J 2025, 33, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Iversen, K.; Ihlemann, N.; Gill, S.U.; Madsen, T.; Elming, H.; Jensen, K.T.; Bruun, N.E.; Høfsten, D.E.; Fursted, K.; Christensen, J.J.; et al. Partial Oral versus Intravenous Antibiotic Treatment of Endocarditis. N Engl. J. Med. 2019, 380, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Freling, S.; Wald-Dickler, N.; Banerjee, J.; Canamar, C.P.; Tangpraphaphorn, S.; Bruce, D.; Davar, K.; Dominguez, F.; Norwitz, D.; Krishnamurthi, G.; et al. Real-World Application of Oral Therapy for Infective Endocarditis: A Multicenter, Retrospective, Cohort Study. Clin. Infect. Dis. 2023, 77, 672–679. [Google Scholar] [CrossRef]
- Rallet, B.; Pouy, R.; Coutureau, C.; Blot, M.; Bani-Sadr, F.; Sixt, T.; Moutel, M.; Piroth, L.; Hentzien, M. Should We Extend the Use of Oral Antibiotics in Infective Endocarditis? The ENDO-ORAL Study. Clin. Infect. Dis. 2025, ciaf452. [Google Scholar] [CrossRef]
- Moss, R.; Munt, B. Injection Drug Use and Right Sided Endocarditis. Heart 2003, 89, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Scheggi, V.; Menale, S.; Tonietti, B.; Giovacchini, J.; Del Pace, S.; Zoppetti, N.; Alterini, B.; Stefàno, P.L.; Marchionni, N. Infective Endocarditis in Octogenarians. A Retrospective Study in a Single, High-Volume Surgical Centre. BMC Geriatr 2023, 23, 659. [Google Scholar] [CrossRef] [PubMed]
- Loghin, I.I.; Surdu, A.E.; Rusu, Șerban A.; Cecan, I.; Dorobăț, V.D.; Mihăescu, A.A.; Dorobăţ, C.M. Etiological Aspects of Infectious Endocarditis in a Tertiary Hospital in Northeastern Romania. Medicina 2025, 61, 95. [Google Scholar] [CrossRef] [PubMed]
- “Grigore T. Popa” University of Medicine and Pharmacy Iasi, Romania; Buburuz, A.-M. Infective Endocarditis Etiologic Profile – Still a Classic Distribution of Microorganisms? MSJ 2022, 126, 25–32. [CrossRef]
- Nanu, A.-A.; Lazăr, D. Ștefan; Popescu, C.P.; Lazăr, M.-I.; Nica, M.; Florescu, S.A. Characteristics of Infective Endocarditis in Intravenous Drug Users vs. Non-Users: A Retrospective Study Conducted in Bucharest, Romania. Medicina 2025, 61, 1785. [Google Scholar] [CrossRef]
- Anton, C.-I.; Buzilă, C.A.; Stanciu, S.M.; Bucurică, S.; Anghel, D.; Ștefan, A.T.; Ștefan, I.; Streinu-Cercel, A. Prosthetic Valve Endocarditis: A Retrospective Cohort Study Conducted at “Dr. Carol Davila” Central Military Emergency University Hospital in Bucharest. Microorganisms 2024, 12, 1442. [Google Scholar] [CrossRef]
- Babeș, E.E.; Lucuța, D.A.; Petcheși, C.D.; Zaha, A.A.; Ilyes, C.; Jurca, A.D.; Vesa, C.M.; Zaha, D.C.; Babeș, V.V. Clinical Features and Outcome of Infective Endocarditis in a University Hospital in Romania. Medicina 2021, 57, 158. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. The Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef]
- Waksman, R.; Pahuja, M.; Van Diepen, S.; Proudfoot, A.G.; Morrow, D.; Spitzer, E.; Nichol, G.; Weisfeldt, M.L.; Moscucci, M.; Lawler, P.R.; et al. Standardized Definitions for Cardiogenic Shock Research and Mechanical Circulatory Support Devices: Scientific Expert Panel From the Shock Academic Research Consortium (SHARC). Circulation 2023, 148, 1113–1126. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801. [Google Scholar] [CrossRef]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 11 February 2026).
- Jordal, S.; Kommedal, Ø; Haaverstad, R.; Saeed, S.; Davidsen, E.S.; Salminen, P.-R.; Hufthammer, K.O.; Kittang, B.R. Epidemiological and Microbial Trends of Infective Endocarditis in Western Norway: A 7-Year Prospective Observational Study. BMC Infect Dis 2024, 24, 702. [Google Scholar] [CrossRef] [PubMed]
- Cresti, A.; Chiavarelli, M.; Scalese, M.; Nencioni, C.; Valentini, S.; Guerrini, F.; D’Aiello, I.; Picchi, A.; De Sensi, F.; Habib, G. Epidemiological and Mortality Trends in Infective Endocarditis, a 17-Year Population-Based Prospective Study. Cardiovasc. Diagn. Ther. 2017, 7, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Khardori, N. Changing Paradigms in Epidemiology, Microbiology, and Outcomes of Infective Endocarditis. Infect. Dis. Clin. Pract. 2024, 32, 1–3. [Google Scholar] [CrossRef]
- Camp, J.; Nüßle, K.; Deyhle, N.; Mathé, P.; Hornuss, D.; Grundmann, S.; Asmussen, A.; Zientara, A.; Bothe, W.; Schmidt-Hellerau, K.; et al. Partial Oral Treatment of Infective Endocarditis in Real-World Settings – an in-Depth Analysis of the Prospectively Evaluated German DERIVE Cohort. CMI Communications 2024, 1, 105032. [Google Scholar] [CrossRef]
- Pries-Heje, M.M.; Hjulmand, J.G.; Lenz, I.T.; Hasselbalch, R.B.; Povlsen, J.A.; Ihlemann, N.; Køber, N.; Tofterup, M.L.; Østergaard, L.; Dalsgaard, M.; et al. Clinical Implementation of Partial Oral Treatment in Infective Endocarditis: The Danish POETry Study. European Heart Journal 2023, 44, 5095–5106. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Erba, P.-A.; Sadeghpour, A.; Meshaal, M.; Sambola, A.; Furnaz, S.; Citro, R.; Ternacle, J.; Donal, E.; et al. The ESC-EORP EURO-ENDO (European Infective Endocarditis) Registry. Eur. Heart J. - Qual. Care Clin. Outcomes 2019, 5, 202–207. [Google Scholar] [CrossRef]
- Dobreva-Yatseva, B.; Nikolov, F.; Raycheva, R.; Tokmakova, M. Infective Endocarditis—Predictors of In-Hospital Mortality, 17 Years, Single-Center Experience in Bulgaria. Microorganisms 2024, 12, 1919. [Google Scholar] [CrossRef]
- Philip, M.; Dumonceau, R.G.; Citro, R.; Cosyns, B.; Donal, E.; Erba, P.A.; Gouriet, F.; Iung, B.; Kong, W.K.F.; Lancellotti, P.; et al. Clinical Characteristics, Management and Outcomes of Enterococcal Infective Endocarditis: An Ancillary Study from the ESC-EORP EURO-ENDO Registry. Eur. Heart J. - Qual. Care Clin. Outcomes 2025, qcaf145. [Google Scholar] [CrossRef]
- Becher, P.M.; Goßling, A.; Fluschnik, N.; Schrage, B.; Seiffert, M.; Schofer, N.; et al. Temporal trends in incidence, patient characteristics, microbiology and in-hospital mortality in patients with infective endocarditis: a contemporary analysis of 86,469 cases between 2007 and 2019. Clin. Res. Cardiol. 2024, 113, 205–215. [Google Scholar] [CrossRef]
- Murdoch, D.R. Clinical Presentation, Etiology, and Outcome of Infective Endocarditis in the 21st Century: The International Collaboration on Endocarditis–Prospective Cohort Study. Arch Intern Med 2009, 169, 463. [Google Scholar] [CrossRef]
- Wang, A.; Gaca, J.G.; Chu, V.H. Management Considerations in Infective Endocarditis: A Review. JAMA 2018, 320, 72. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-H.; Kim, Y.-J.; Kim, S.-H.; Sun, B.J.; Kim, D.-H.; Yun, S.-C.; Song, J.-M.; Choo, S.J.; Chung, C.-H.; Song, J.-K.; et al. Early Surgery versus Conventional Treatment for Infective Endocarditis. N Engl. J. Med. 2012, 366, 2466–2473. [Google Scholar] [CrossRef] [PubMed]
- Fowler, V.G.; Miro, J.M.; Hoen, B.; Cabell, C.H.; Abrutyn, E.; Rubinstein, E.; Corey, G.R.; Spelman, D.; Bradley, S.F.; Barsic, B.; et al. Staphylococcus Aureus Endocarditis: A Consequence of Medical Progress. JAMA 2005, 293, 3012. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Felix, B.M.; Barca, L.V.; Garcia-Esquinas, E.; Correa-Pérez, A.; Fernández-Hidalgo, N.; Muriel, A.; Lopez-Alcalde, J.; Álvarez-Diaz, N.; Pijoan, J.I.; Ribera, A.; et al. Prognostic Models for Mortality after Cardiac Surgery in Patients with Infective Endocarditis: A Systematic Review and Aggregation of Prediction Models. Clin. Microbiol. Infect. 2021, 27, 1422–1430. [Google Scholar] [CrossRef]
- Varela, L.; López-Menéndez, J.; Redondo, A.; Fajardo, E.R.; Miguelena, J.; Centella, T.; Martín, M.; Muñoz, R.; Navas, E.; Moya, J.L.; et al. Mortality Risk Prediction in Infective Endocarditis Surgery: Reliability Analysis of Specific Scores†. Eur. J. Cardio-Thorac. Surg. 2018, 53, 1049–1054. [Google Scholar] [CrossRef]
- Wang, Q.; Fu, B.; Hu, P.; Liao, X.; Guo, W.; Yu, D.; Wang, Z.; Wei, X. Clinical Evaluation of Sepsis-1 and Sepsis-3 in Infective Endocarditis. Int. J. Cardiol. 2023, 393, 131365. [Google Scholar] [CrossRef]
Figure 1.
Study selection process: Legend: IE – infective endocarditis, n- number, h- hours. P1-period 1, P2- period 2.
Figure 1.
Study selection process: Legend: IE – infective endocarditis, n- number, h- hours. P1-period 1, P2- period 2.

Figure 2.
Receiver operating characteristic curve for the prediction model. Legend: AUC = area under the curve, ROC - receiver operating characteristic curve.
Figure 2.
Receiver operating characteristic curve for the prediction model. Legend: AUC = area under the curve, ROC - receiver operating characteristic curve.

Figure 3.
Adjusted predictors of the composite in-hospital endpoint: multivariable logistic regression forest plot. Legend: LVEF = left ventricular ejection fraction, IE = infective endocarditis, OR = odds ratio, CI = confidence intervals, points indicate adjusted OR, horizontal lines show 95%, dashed vertical line denotes OR =1, NS - non significative.
Figure 3.
Adjusted predictors of the composite in-hospital endpoint: multivariable logistic regression forest plot. Legend: LVEF = left ventricular ejection fraction, IE = infective endocarditis, OR = odds ratio, CI = confidence intervals, points indicate adjusted OR, horizontal lines show 95%, dashed vertical line denotes OR =1, NS - non significative.


Table 1.
Baseline characteristics, management, and in-hospital outcomes of patients with definite infective endocarditis, stratified by trial eligibility.
Table 1.
Baseline characteristics, management, and in-hospital outcomes of patients with definite infective endocarditis, stratified by trial eligibility.
| Variable | Overall (n=206) | Trial-eligible (n=130) | Real World (n=76) | p-value (95% CI) |
|---|---|---|---|---|
| Demographics | ||||
| Age, years (median) | 63.0 ± 14.8 | 59.9 ± 15.4 | 68.3 ± 12.1 | < 0.001 (-12.2 to -4.6) |
| Male sex, n (%) | 145 (70.4%) | 102 (78.5%) | 43 (56.6%) | 0.002. (3.5% to 39.3%) |
| Comorbidities | ||||
| Hypertension, n (%) | 125 (60.7%) | 79 (60.8%) | 46 (60.5%) | 1.000 |
| Diabetes mellitus, n (%) | 37 (18.0%) | 24 (18.5%) | 13 (17.1%) | 0.955 |
| CKD (≥stage 3), n (%) | 47 (22.8%) | 21 (18.5%) | 26 (34.2%) | 0.01 (28.6% to 4.9%) |
| COPD, n (%) | 17 (8.3%) | 8 (6.2%) | 9 (11.8%) | 0.242 |
| IVDU, n (%) | 2 (1.0%) | 0 (0.0%) | 2 (2.6%) | 0.135 |
| Chronic HF, n (%) | 139 (67.5%) | 86 (66.2%) | 53 (69.7%) | 0.707 |
| Liver cirrhosis, n (%) | 5 (2.42%) | 2 (2.6%) | 3 (2.3%) | 1.000 |
| Malignancy, n (%) | 33 (16.0%) | 0 (0.0%) | 33 (43.4%) | 0.0001 (54.6% to 30.0%) |
| Infection location | ||||
| Left-sided IE, n (%) | 197 (95.6%) | 125 (96.2%) | 72 (94.7%) | 0.728 |
| Right-sided IE, n (%) | 9 (4.4%) | 5 (3.8%) | 4 (5.3%) | 0.718 |
| Prosthetic IE, n (%) | 81 (%) | 54 (41.5%) | 27 (35.5%) | 0.394 |
| CIED-related IE, n (%) | 32 (15.5%) | 12 (9.2%) | 20 (26.3%) | 0.001 (2.3 to 31.8) |
| TAVI-associated IE | 8 (3.8%) | 0 (0.0%) | 8 (10.5%) | <0.001 (2.6 to 19.4) |
| Microbiology | ||||
| S. aureus, n (%) | 29 (14.1%) | 22 (16.9%) | 7 (9.2%) | 0.184 |
| Enterococcus spp., n (%) | 26 (12.6%) | 10 (7.7%) | 16 (21.1%) | 0.010 (27.3% to 0.2%) |
| Viridans streptococci, n (%) | 20 (9.7%) | 18 (13.8%) | 2 (2.6%) | 0.009 (-20.1 to 0.2) |
| Culture-negative IE, n (%) | 74 (35.9%) | 45 (34.6%) | 29 (38.1%) | 0.480 |
| Echocardiography | ||||
| Vegetation present, n (%) | 150 (72.8%) | 93 (71.5%) | 57 (75.0%) | 0.590 |
| Vegetation >10 mm, n (%) | 95 (46.1%) | 60 (46.2%) | 35 (46.1%) | 0.989 |
| Perivalvular abscess, n (%) | 46 (22.3%) | 36 (27.7%) | 10 (13.2%) | 0.02 (1.8% to 28.6%) |
| Severe valvular regurgitation, n (%) | 79 (38.3) | 53 (40.8%) | 26 (34.2%) | 0.350 |
| LV EF <50%, n (%) | 93 (45.1%) | 61 (46.9%) | 32 (42.1%) | 0.599 |
| Clinical presentation / severity | ||||
| Acute HF on admission, n (%) | 25 (12.1%) | 12 (9.2%) | 13 (17.1%) | 0.147 |
| Sepsis at admission, n (%) | 52 (25.2%) | 23 (17.7%) | 29 (38.2%) | 0.002 (-37.3% to -2.9%) |
| Septic shock, n (%) | 17 (8.3%) | 2 (1.5%) | 15 (19.7%) | 0.0001 (−29.6% to −6.9%) |
| Cardiogenic shock, n (%) | 32 (15.5%) | 15 (11.5%) | 17 (22.4%) | 0.061 (25.8% to 3.7%) |
| Outcomes | ||||
| Composite endpoint, n (%)* | 126 (61.6%) | 75 (57.6%) | 51 (67.1%) | 0.218 |
| In-hospital mortality, n (%) | 67 (32.5%) | 37 (28.5%) | 30 (39.5%) | 0.141 |
| Renal replacement therapy (acute) | 8 (3.8%) | 6 (4.6%) | 2 (2.6%) | 0.713 |
| Any embolic event, n (%) ** | 54 (26.2%) | 27 (20.8%) | 27 (35.5%) | 0.02 (-2.8 to 32.1) |
| Length of stay, days | 13,05 ± 10,6 | 12.6 ± 11.1 | 13.5 ± 10.2 | 0.331 |
Legend: CKD = chronic kidney disease was defined as estimated glomerular filtration rate <60 mL/min/1.73 m2 (stage ≥3) or need for chronic dialysis, Chronic HF = existing heart failure documented before the index hospitalization, COPD = chronic obstructive pulmonary disease, IE = infective endocarditis, IVDU = intravenous drug use, CIED = cardiac implantable electronic device, TAVI = transcatheter aortic valve implantation, LVEF = left ventricular ejection fraction, Acute HF on admission = acute decompensated heart failure present at hospital admission, QI score = adherence score represents the number of fulfilled European Society of Cardiology (ESC) quality indicators (range 0–4), 95% CI = 95% confidence intervals, p-value <0.05 was considered statistically significant, * composite in-hospital endpoint = occurrence of at least one of the following events: acute heart failure requiring intravenous therapy or ventilatory support, shock (cardiogenic and/or septic), embolic events symptomatic or confirmed by imaging or surgery, severe infectious complications (such as abscess, fistula, or metastatic infection), renal replacement therapy, and all-cause in-hospital mortality. **cerebral asymptomatic imagistic detected or symptomatic, splenic, renal, hepatic, mesenteric, or limb arteries.
Table 2.
Comparison between study periods (P1: 2011–2016 vs P2: 2017–2025), including trial-eligibility distribution, quality indicators, and outcomes.
Table 2.
Comparison between study periods (P1: 2011–2016 vs P2: 2017–2025), including trial-eligibility distribution, quality indicators, and outcomes.
| Section / Variable | P1 (2011–2016) |
P2 (2017–2025) |
p-value 95% CI |
|---|---|---|---|
| Cohort composition | 49 | 157 | |
| Trial-eligible (TE) | 40 (81.6%) | 90 (57.3%) | 0.002 (-40.5 to -3.8) |
| Real-world (RW) | 9 (18.4%) | 67 (42.7%) | 0.002 (3.8 to 40.5) |
| Demographics | |||
| Age, years (mean) | 62.0 ± 13.3 | 63.4 ± 15.3 | 0.563 |
| Male sex, n % | 39 (79.6%) | 106 (67.5%) | 0.151 |
| Comorbidities | |||
| Hypertension | 34 (69.4%) | 91 (58.0%) | 0.153 |
| Diabetes mellitus | 7 (14.3%) | 30 (19.1%) | 0.443 |
| Coronary artery disease | 11 (22.4%) | 43 (27.4%) | 0.492 |
| Chronic HF, n % | 43 (87.8%) | 96 (61.1%) | <0.001 (-38.5 to -14.7) |
| Atrial fibrillation | 14 (28.6%) | 59 (37.6%) | 0.250 |
| CKD (≥stage 3), n (%) | 8 (16.3%) | 39 (24.8%) | 0.01 (12.6% to 28.9%) |
| Liver cirrhosis, n (%) | 1(2.1%) | 4(2.5%) | 0.983 |
| Malignancy, n % | 4 (8.2%) | 29 (18.5%) | 0.086 (-6.0 to 22.0) |
| IVDU | 0 (0.0%) | 2 (1.2) | 0.275 |
| Infection location | |||
| Prosthetic valve IE, n % | 21 (42.8%) | 60 (38.2) | 0.384 |
| CIED-related IE, n % | 1 (2.0%) | 31 (19.7%) | 0.003 (3.6 to 26.3) |
| TAVI-associated IE, n % | 0 (0.0%) | 8 (5.1%) | 0.202 |
| Microbiology | |||
| S. aureus, n (%) | 6 (12.2%) | 23 (14.6%) | 0.262 |
| Enterococcus spp., n (%) | 4 (8.1%) | 22 (14.01%) | 0.275 |
| Viridans streptococci, n (%) | 2 (4.08) | 18 (11.4%) | 0.126 |
| Culture-negative IE, n % | 32 (65.3%) | 42 (26.7%) | 0.001 (-43.1 to -12.4) |
| Echocardiography | |||
| TEE performed, n % | 9 (18.3%) | 81 (51.5%) | 0.01 (-1.1 to 38.9) |
| Vegetation >10 mm, n (%) | 42 (85.7%) | 53 (33.8%) | <0.001 (-66.1 to -31.9) |
| Perivalvular abscess, n % | 4/49 (8.2%) | 42 (26.8%) | 0.006 (8.3 to 28.9) |
| Severe regurgitation, n % | 25 (51.0%) | 54 (34.4%) | 0.05 (-32.5 to -0.8) |
| LVEF <50% | 30 (61.2%) | 63 (40.1%) | 0.010 (-40.8 to 0.7) |
| Clinical presentation / severity | |||
| Acute HF on admission, n (%) | 7 (14.2%) | 18 (11.4%) | 0.317. |
| Sepsis at admission, n (%) | 9 (18.3%) | 43 (27.3%) | 0.07 (15.8% to 37.7%) |
| Septic shock, n (%) | 2 (4.08%) | 15 (9.5%) | 0.02 (3.0 to 14.2) |
| Cardiogenic shock, n (%) | 3 (6.1%) | 29 (18.4%) | 0.01 (2.8% to 28.7%) |
| Outcomes | |||
| Composite endpoint, n (%)* | 21 (42.9%) | 105 (66.8%) | 0.002 (3.1 to 44.3) |
| In-hospital mortality, n % | 17 (34.7%) | 50 (31.8%) | 0.844 (-18.0 to 12.3) |
| Renal replacement therapy (acute), n % | 4 (8.2%) | 4 (2.5%) | 0.09 (-18.2 to 3.1) |
| Any embolic event, n % ** | 4 (8.2%) | 50 (31.8%) | <0.001 (5.9 to 36.3) |
| Length of stay, days | 8.2 ± 6.0 | 14.4 ± 11.5 | 0.002 (3.6 to 8.6) |
Legend: CKD = chronic kidney disease was defined as estimated glomerular filtration rate <60 mL/min/1.73 m2 (stage ≥3) or need for chronic dialysis, Chronic HF = existing heart failure documented before the index hospitalization, COPD = chronic obstructive pulmonary disease, IE = infective endocarditis, IVDU = intravenous drug use, CIED = cardiac implantable electronic device, TAVI = transcatheter aortic valve implantation, TEE= transesophageal echocardiography, LVEF = left ventricular ejection fraction, Acute HF on admission = acute decompensated heart failure present at hospital admission, QI score = adherence score represents the number of fulfilled European Society of Cardiology (ESC) quality indicators (range 0–4), 95% CI = 95% confidence intervals, p-value <0.05 was considered statistically significant, * composite in-hospital endpoint = occurrence of at least one of the following events: acute heart failure requiring intravenous therapy or ventilatory support, shock (cardiogenic and/or septic), embolic events symptomatic or confirmed by imaging or surgery, severe infectious complications (such as abscess, fistula, or metastatic infection), renal replacement therapy, and all-cause in-hospital mortality. ** cerebral asymptomatic imagistic detected or symptomatic, splenic, renal, hepatic, mesenteric, or limb arteries.
Table 3.
Univariable logistic regression for the composite in-hospital endpoint.
| Variable | Univariable OR | 95% CI | p-value |
|---|---|---|---|
| Sepsis at admission | 9.1 | 3.8–21.5 | <0.001 |
| Streptococcal infection | 5.8 | 1.4–24.0 | 0.014 |
| Cardiogenic shock | 3.9 | 1.8–8.4 | <0.001 |
| Acute heart failure | 2.7 | 1.4–5.0 | 0.002 |
| LVEF <50% | 2.6 | 1.3–5.2 | 0.006 |
| Perivalvular abscess | 2.2 | 1.0–4.9 | 0.048 |
| Staphylococcus aureus infection | 1.8 | 0.9–3.6 | 0.080 |
| Enterococcal infection | 1.4 | 0.7–2.9 | 0.320 |
| Age (per 10 years) | 1.02 | 0.99–1.04 | 0.160 |
| Male sex | 0.93 | 0.55–1.60 | 0.800 |
| Prosthetic/device-related IE | 0.70 | 0.40–1.20 | 0.190 |
Legend: OR = odds ratio; CI = confidence interval; IE = infective endocarditis; LVEF = left ventricular ejection fraction. Reference microbiological category: culture-negative IE. Values are OR with 95% CI obtained from univariable logistic regression assessing associations with the composite in-hospital endpoint (acute heart failure, cardiogenic shock, embolic events, renal replacement therapy, or in-hospital death). Variables with p<0.10 and clinically relevant factors were considered for multivariable modeling.
Table 4.
Multivariable logistic regression for the composite in-hospital endpoint.
| Predictor | Adjusted OR (95% CI) | p-value |
|---|---|---|
| Sepsis at admission | ≈8.4 (3.3–21.8) | <0.001 |
| LVEF <50% | ≈2.3 (1.1–5.0) | 0.032 |
| Streptococcal infection | ≈6.3 (1.3–30.6) | 0.024 |
| Prosthetic/device-related IE | ≈0.6 (0.4–1.1) | 0.080 |
| Age | ≈1.0 | NS |
| Sex | ≈1.0 | NS |
Legend: OR = odds ratio; CI = confidence interval; IE = infective endocarditis; LVEF = left ventricular ejection fraction. Reference microbiological category: culture-negative IE.
Table 5.
Extended quality-of-care indicators according to study period and trial eligibility.
| Variable | P1 n (%) |
P2 n (%) |
OR (95% CI) P2 vs P1 |
p | TE n (%) |
RW n (%) |
OR (95% CI) TE vs RW |
p |
|---|---|---|---|---|---|---|---|---|
| Overall patients (206), n | 49 | 157 | - | - | 130 | 76 | - | - |
| QI score ≥ 3 | 9 (18.3%) | 40 (25.4%) |
1.63 (0.62–4.27) |
0.32 | 35 (26.9%) |
14 (18.4%) |
2.23 (0.96–5.19) |
0.05 |
| Adequate blood cultures, n % * |
17 (34.7%) | 115 (73.2%) | 5.14 (2.47–10.7) |
<0.001 | 81 (62.3%) | 51 (67.1%) |
0.80 (0.44–1.46) |
0.588 |
| TEE performed when indicated, n % | 9 (18.3%) | 81 (51.5%) |
4.72 (2.10–10.6) |
0.001 | 52 (40.0%) |
38 (50.0%) |
0.67 (0.37–1.21) |
0.18 |
| Appropriate antimicrobial therapy, n % ** | 16 (32.7%) | 116 (73.9%) |
5.86 (2.85–12.0) |
<0.001 | 81 (62.3%) |
51 (67.1%) |
0.80 (0.44–1.46) |
0.588 |
| Surgery when indicated n % |
6 (12.2%) | 48 (30.5%) |
3.18 (1.2–8.2) |
0.01 | 35 (26.9%) |
19 (25.0%) | 1.10 (0.56–2.15) |
0.890 |
Legend IE = infective endocarditis; QI = quality indicator; P1 interval (2011–2016), P2 interval (2017-2025), TE = trial-eligible; RW = real-world; TEE = transesophageal echocardiography; OR = odds ratio; CI = confidence interval, n = numbers, p-value <0.05 was considered statistically significant, * ≥2 blood culture sets prior to antibiotics, ** guideline-concordant initial antibiotics combined with adequate duration antimicrobial therapy according to microbiological data when available.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



