Submitted:
27 March 2026
Posted:
31 March 2026
You are already at the latest version
Abstract
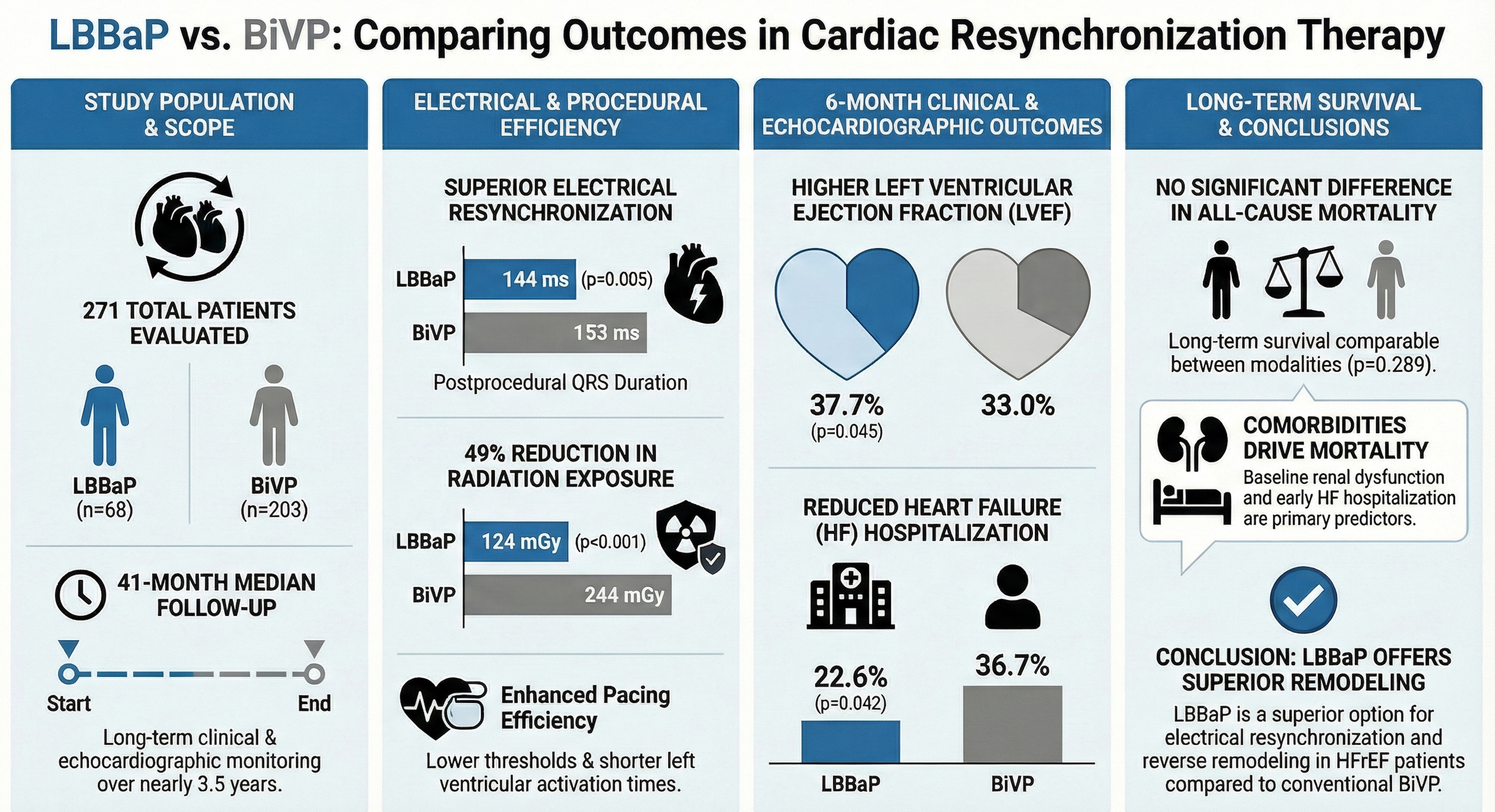
Background: Left bundle branch area pacing (LBBaP) has emerged as a physiological alternative to conventional biventricular pacing (BiVP) for cardiac resynchronization therapy (CRT). We aimed to compare long-term clinical, electrical, and echocardiographic outcomes of LBBaP versus BiVP in patients with heart failure with reduced ejection fraction (HFrEF).
Methods: In this single-center retrospective study, 271 consecutive patients undergoing CRT implantation were included (LBBaP, n = 68; BiVP, n = 203). Outcomes included electrical resynchronization parameters, echocardiographic reverse remodeling, heart failure hospitalization, and all-cause mortality during a median follow-up of 41 months.
Results: LBBaP achieved greater electrical resynchronization, with shorter postprocedural QRS duration (144 vs 153 ms; p = 0.005) and shorter left ventricular activation time compared with BiVP. LBBaP was associated with lower radiation exposure (124 vs 244 mGy; p < 0.001) and lower pacing thresholds. At 6 months, LVEF was higher in the LBBaP group (37.7% vs 33.0%; p = 0.005), and heart failure hospitalization occurred less frequently (22.6% vs 36.7%; p = 0.042). Long-term all-cause mortality did not differ between groups (p = 0.289). In multivariable analysis, baseline renal dysfunction and heart failure hospitalization within 6 months independently predicted mortality.
Conclusions: In patients with HFrEF undergoing CRT, LBBaP provides superior electrical resynchronization and greater reverse remodeling compared with BiVP. Although associated with improved short-term clinical outcomes, long-term survival appears primarily determined by comorbid conditions rather than pacing modality.
Keywords:
cardiac resynchronization therapy
; left bundle branch area pacing
; biventricular pacing
; heart failure with reduced ejection fraction
; conduction system pacing
Introduction
Heart failure with reduced ejection fraction (HFrEF) is a progressive clinical syndrome associated with substantial morbidity and mortality [1]. Cardiac resynchronization therapy (CRT) is an established treatment that improves symptoms, promotes reverse ventricular remodeling, and reduces mortality in appropriately selected patients [2]. Conventionally, CRT is delivered through biventricular pacing (BiVP); however, left bundle branch area pacing (LBBaP) has recently emerged as a physiologically based alternative with potential technical and clinical advantages [3].
Despite high implantation success rates, BiVP is limited by challenges including phrenic nerve stimulation, coronary sinus lead instability, and a nonresponse rate approaching 40% [4,5]. Conduction system pacing (CSP), particularly LBBaP, seeks to restore physiological ventricular activation and may overcome these limitations [6]. Although comparative evidence has rapidly expanded—including randomized and observational studies and recent meta-analyses—data on very long-term clinical outcomes and real-world durability of LBBaP/ LBBP compared with conventional BiVP remain comparatively less well defined [7]. Therefore, the present study aimed to compare the long-term clinical outcomes of LBBaP versus BiVP in patients with HFrEF.
Methods
Study Population
This single-center, retrospective observational study included patients who underwent cardiac resynchronization therapy (CRT) implantation at our institution between January 1, 2017, and July 31, 2024. A total of 455 consecutive patients undergoing CRT implantation were initially screened. Patients were stratified into two groups according to implantation strategy: left bundle branch area pacing CRT (LBBaP-CRT) and biventricular pacing CRT (BiVP-CRT). The pacing modality was selected at the operator’s discretion.
Patients were excluded if any of the following criteria were present: (1) failed transvenous CRT implantation; (2) age <18 years; (3) follow-up duration <6 months or unavailable follow-up data; (4) prior BiVP-CRT subsequently upgraded or converted to LBBaP-CRT; or (5) implantation of left bundle branch optimized CRT (LOT-CRT), defined as combined LBBaP and coronary sinus pacing. Based on these criteria, 184 patients were excluded, yielding a final study population of 271 patients.
Baseline demographic and clinical characteristics, including age, sex, comorbidities, electrocardiographic (ECG) and echocardiographic parameters, laboratory data, and preprocedural medical therapy, were retrieved from the institutional electronic medical records. Procedural characteristics, intracardiac electrograms (EGMs), peri-procedural complications, and device interrogation parameters were recorded. Long-term follow-up data, including device performance, ECG and echocardiographic changes, hospitalizations, and device-related complications, were obtained from hospital records and verified using the national health registry system.
The study protocol was approved by the Hacettepe University Health Sciences Ethics Committee (November 5, 2024; Decision No. 2024/19-09). The requirement for informed consent was waived due to the retrospective design. The study complied with the Declaration of Helsinki and its subsequent amendments.
Pre-Procedural Assessment
Standard 12-lead surface ECGs were obtained before implantation to evaluate intrinsic rhythm, QRS morphology and duration, left ventricular activation time (LVAT), and atrioventricular conduction status. ECG measurements were performed digitally using electronic calipers (EP Calipers, EP Studios, Inc.).
Transthoracic echocardiography was performed to assess left ventricular ejection fraction (LVEF), interventricular septal anatomy and thickness, left ventricular end-diastolic diameter (LVEDD), valvular disease, and cardiac chamber dimensions. LVEF was calculated using the modified Simpson method. Mitral valve area in stenotic lesions was calculated using the pressure half-time method, and aortic stenosis severity was assessed using the Bernoulli equation. Valvular regurgitation severity was visually graded as mild, moderate, or severe using color Doppler imaging [8].
Baseline laboratory evaluation included complete blood count, renal and liver function tests, B-type natriuretic peptide (BNP), and thyroid function tests.
For patients receiving warfarin, procedures were performed without interruption when the international normalized ratio (INR) was <2.5. Bridging with low-molecular-weight heparin was used when INR was <2.0, with the final dose withheld on the day of the procedure. Direct oral anticoagulants were discontinued 24–48 hours prior to implantation according to renal function. All patients received prophylactic intravenous cefazolin immediately before the procedure.
Procedural Technique
All procedures were performed under conscious sedation using intravenous midazolam and fentanyl. Local anesthesia was achieved with prilocaine infiltration in the left pectoral region. Venous access was obtained prior to device pocket creation. Procedures were performed under fluoroscopic guidance with continuous 12-lead ECG monitoring (Artis Zee Angiography System, Siemens Healthcare GmbH, Germany).
BiVP Implantation
Right atrial leads were positioned in the atrial appendage in patients with sinus rhythm, and right ventricular leads were positioned at the apex using standard techniques. The coronary sinus was cannulated using a pre-shaped diagnostic catheter within a long peel-away sheath, followed by coronary venography to define venous anatomy (Figure 1A).
A bipolar or quadripolar left ventricular lead was advanced over a 0.014-inch guidewire into a target branch, preferably the anterolateral or posterolateral vein. Adequate sensing and pacing thresholds were confirmed, and phrenic nerve stimulation was excluded prior to sheath removal (Figure 1B). Leads were secured to the pectoral muscle and connected to the pulse generator, and the pocket was closed in layers.
LBBaP Implantation
Right atrial and right ventricular leads were positioned using standard techniques. For LBBaP, a Selectra 3D delivery sheath (Biotronik, Germany) was advanced into the right ventricle over a 0.038-inch guidewire. The Solia S60 ventricular lead was prepared ex vivo by helix extension and inner coil pre-tensioning as previously described [9]. Lead deployment was guided by fluoroscopy, continuous ECG monitoring, and intracardiac electrograms recorded via a pacing system analyzer (Renamic Neo, Biotronik, Germany) [10]. The sheath was positioned against the interventricular septum in the right anterior oblique 30° view (Figure 2A). Contrast ventriculography was performed to delineate septal anatomy.
Optimal lead position was identified using unipolar pacing mapping targeting a “W” morphology in lead V1, aVL/aVR discordance, and greater R-wave amplitude in lead II than lead III. Lead depth was confirmed in the left anterior oblique projection (Figure 2B).
During septal penetration, impedance, fluoroscopic depth, and QRS morphology were continuously monitored. After development of a terminal r/R pattern in lead V1, the following parameters were assessed:
- V6 R-wave peak time (V6RWPT/LVAT)
- V6–V1 interpeak interval
- QRS transition during threshold testing
- Presence of left bundle or fascicular potentials
- Unipolar and bipolar pacing thresholds
Successful capture was defined according to EHRA consensus criteria for selective or nonselective left bundle branch pacing [11]. After confirmation, the sheath was removed and the lead connected to the LV port of the generator (Figure-2C). Postprocedural echocardiography was performed to confirm septal lead depth and exclude septal complications.
Post-Procedural Management and Follow-up
All patients underwent chest radiography, echocardiography, 12-lead ECG, and laboratory testing following implantation and were observed for at least 24 hours.
Follow-up visits were scheduled at 1 month, 6 months, and every 6 months thereafter. Each visit included clinical evaluation (NYHA functional class and congestion assessment), ECG, echocardiography, laboratory testing, and device interrogation to assess pacing thresholds, sensing amplitudes, and lead impedance.
CRT-related complications, hospitalizations, and all-cause mortality were recorded throughout follow-up.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics version 28.0 (IBM Corp., Armonk, NY). Continuous variables are presented as mean ± standard deviation or median (range) according to distribution. Categorical variables are expressed as frequencies and percentages.
Normality was assessed using visual inspection and Shapiro–Wilk or Kolmogorov–Smirnov tests. Between-group comparisons were performed using Student’s t test or Mann–Whitney U test for continuous variables and χ² or McNemar tests for categorical variables, as appropriate. Paired comparisons were analyzed using paired t tests or Wilcoxon signed-rank tests.
Overall survival was defined as the interval from CRT implantation to death from any cause. Survival curves were constructed using the Kaplan–Meier method and compared using the log-rank test. Predictors of survival were assessed using univariable and multivariable Cox proportional hazards regression analyses. Variables significant in univariable analysis were entered into multivariable models after assessment for multicollinearity. A 2-sided p value <0.05 was considered statistically significant.
Results
Patient Demographics
The study population consisted of 271 patients (mean age 63.6 ± 13.0 years; 69.4% male). CRT was delivered using biventricular pacing (BiVP) in 203 patients (74.9%) and left bundle branch area pacing (LBBaP) in 68 patients (25.1%).
Baseline demographic characteristics were comparable between groups, including age, sex, body mass index, NYHA functional class, prior cardiac implantable electronic device (CIED) implantation, and overall comorbidity burden. Ischemic cardiomyopathy was more prevalent in the BiVP group than in the LBBaP group (52.2% vs 33.8%, p = 0.009). Serum creatinine levels were lower in the LBBaP group (p = 0.032); however, estimated glomerular filtration rate (eGFR) categories did not differ significantly between groups (p = 0.123).
Guideline-directed medical therapy was widely used, including beta-blockers (86.0%), loop diuretics (68.6%), mineralocorticoid receptor antagonists (56.6%), angiotensin-converting enzyme inhibitors (44.3%), and angiotensin receptor blockers (27.7%), with no between-group differences. Sodium–glucose cotransporter-2 (SGLT2) inhibitor use was significantly higher in the LBBaP group (30.9% vs 8.9%, p < 0.001). Baseline characteristics are summarized in Table 1.
Baseline Electrocardiographic and Echocardiographic Characteristics
Persistent atrial fibrillation was present in 25.1% of patients, without differences between groups (p = 0.531). Baseline QRS duration was similar between BiVP and LBBaP groups (171 ± 29 ms vs 170 ± 30 ms; p = 0.706). Left bundle branch block was the predominant morphology (44.5%), with a trend toward lower prevalence in the LBBaP group (34.3% vs 48.1%; p = 0.051). Left anterior hemiblock (p = 0.015) and first-degree atrioventricular block (p = 0.038) were more frequent in the LBBaP group. Left ventricular activation time (LVAT) did not differ significantly; however, the LVAT/QRS ratio was lower in the LBBaP group (0.59 ± 0.07 vs 0.61 ± 0.07; p = 0.011).
Baseline echocardiographic parameters were comparable between groups, including left ventricular ejection fraction (LVEF) (29 ± 7.2%) and left ventricular end-diastolic diameter (LVEDD) (6.0 ± 0.8 cm) (p = 0.093 and p = 0.115, respectively). Moderate-to-severe mitral regurgitation was more common in the BiVP group (70.3% vs 55.9%; p = 0.029), whereas tricuspid and aortic regurgitation rates were similar.
Detailed electrocardiographic and echocardiographic data are presented in Table 2.
Procedural Outcomes and Complications
Median procedure duration (84 minutes) and fluoroscopy time (13.9 minutes) were similar between groups (p = 0.698 and p = 0.563, respectively). Radiation exposure was significantly lower in the LBBaP group (124 mGy vs 244 mGy; p < 0.001). LBBaP demonstrated superior electrical performance, including lower pacing thresholds (p < 0.001), lower lead impedance (p < 0.001), and absence of pulse width requirements >0.4 ms (0% vs 9.9%; p = 0.007). Crossover occurred in 4.8% of patients (p = 0.528). Eleven patients in the LBBaP group crossed over to BiVP due to septal perforation, inability to penetrate the septum, or suboptimal electrical parameters. Two BiVP cases crossed over to LBBaP because of unfavorable coronary venous anatomy.
Postprocedural QRS duration was shorter in the LBBaP group (144 ± 18 ms vs 153 ± 22 ms; p = 0.005), with greater QRS reduction (27 ms vs 17 ms; p = 0.017). LVAT was also shorter in the LBBaP group (81.3 ± 13.3 ms vs 93.4 ± 16.0 ms; p < 0.001).
The overall complication rate was 13.3%, without significant between-group differences. Acute complications requiring intervention within 24 hours occurred in 1.5% of patients, including pneumothorax, lead dislodgement, and asystole. An additional 2.6% were managed conservatively. During the first 6 months, device-related complications occurred in 9.2% of patients, most commonly pocket hematoma (4.1%) and lead dislodgement (4.4%), with no differences between groups.
Six-Month and Long-Term Clinical Outcomes
At 6 months, functional status improved more prominently in the LBBaP group, with a higher proportion of patients in NYHA class I (32.1% vs 12.5%) and fewer in class III (14.3% vs 27.1%) (p = 0.006). Electrical resynchronization remained superior with LBBaP. Paced QRS duration at 6 months was shorter (146 ± 19 ms vs 153 ± 19.3 ms; p = 0.017), and QRS reduction was greater (31 ms vs 19 ms; p = 0.036). LVAT and LVAT/QRS ratio were also lower (both p < 0.001). Echocardiographically, LVEF was higher in the LBBaP group (37.7 ± 10.8% vs 33.0 ± 10.6%; p = 0.005). A greater proportion achieved LVEF ≥40% (50.9% vs 28.4%; p = 0.003). LBBaP was also associated with reduced LVEDD (p = 0.025) and lower prevalence of moderate-to-severe mitral regurgitation (32.1% vs 54.3%; p = 0.005).
Pacing thresholds and impedance remained lower in the LBBaP group at 6 months (p < 0.001). Heart failure hospitalization within 6 months occurred less frequently in the LBBaP group (22.6% vs 36.7%; p = 0.042). Six-month all-cause mortality was also lower (2.9% vs 10.8%; p = 0.047).
Detailed outcomes are presented in Table 4.

Table 3.
Procedural outcomes, electrical parameters, and complications of the study population.
| Parameters | Total (n=271) | BiVP (n=203) | LBBaP (n=68) | P-value |
| Procedural Metrics | ||||
| Procedure Time, min [Median (min-max)] | 84 (40-208) | 83 (40-208) | 85 (40-166) | 0.698 |
| Fluoroscopy Time, min [Median (min-max)] | 13.9 (1.2-68.4) | 13.7 (4.8-68.4) | 14.8 (1.2-49.9) | 0.563 |
| Radiation Dose, Gy [Median (min-max)] | 188 (23-1217) | 244 (38-1217) | 124 (23-1063) | <0.001 |
| Crossover Rate, n (%) | 13 (4.8) | 11 (5.4) | 2 (2.9) | 0.528 |
| Electrical Parameters | ||||
| Pacing Threshold, V [Median (min-max)] | 0.85 (0.3-6) | 0.9 (0.3-6) | 0.7 (0.3-2.2) | <0.001 |
| Impedance, Ohm [Median (min-max)] | 596 (304-1790) | 640 (304-1790) | 507 (306-980) | <0.001 |
| Pulse Width >0.4 ms, n (%) | 20 (7.4) | 20 (9.9) | 0 (0.0) | 0.007 |
| ECG Outcomes | ||||
| Post-proc QRS Duration, ms (mean ± SD) | 151 ± 21 | 153 ± 22 | 144 ± 18 | 0.005 |
| ΔQRS (Reduction), ms [Median (min-max)] | 20 (-47 - 102) | 17 (-47 - 102) | 27 (-24 - 72) | 0.017 |
| Post-proc LVAT, ms (mean ± SD) | 90.3 ± 16.2 | 93.4 ± 16.0 | 81.3 ± 13.3 | <0.001 |
| Laboratory Safety | ||||
| Post-proc Hemoglobin, g/dL (mean ± SD) | 12.7 ± 1.9 | 12.8 ± 2.0 | 12.2 ± 1.8 | 0.031 |
| Post-proc Creatinine, mg/dL [Median (min-max)] | 0.96 (0.4-7.3) | 0.99 (0.4-7.3) | 0.91 (0.4-3.6) | 0.013 |
| Complications, n (%) | ||||
| Total Complications | 36 (13.3) | 28 (13.8) | 8 (11.8) | 0.670 |
| Acute (<24h) Requiring Intervention | 4 (1.5) | 3 (1.5) | 1 (1.5) | 1.000 |
| Subacute (24h-6mo) Device-Related | 25 (9.2) | 19 (9.4) | 6 (8.8) | 0.895 |
| Pocket Hematoma | 11 (4.1) | 7 (3.4) | 4 (5.9) | 0.476 |
| Lead Dislodgment | 12 (4.4) | 10 (4.9) | 2 (2.9) | 0.736 |
Values are presented as n (%), mean ± standard deviation, or median (minimum-maximum). BiVP: Biventricular Pacing; LBBaP: Left Bundle Branch Area Pacing; LVAT: Left Ventricular Activation Time; Gy: Gray.
Table 4.
Clinical, echocardiographic, and electrical outcomes at 6-month follow-up.
| Parameters | Total (n=271) | BiVP (n=203) | LBBaP (n=68) | P-value |
| NYHA Functional Class, n (%) | 0.006 | |||
| Class I | 36 (18.0) | 18 (12.5) | 18 (32.1) | |
| Class II | 115 (57.5) | 85 (59.0) | 30 (53.6) | |
| Class III | 47 (23.5) | 39 (27.1) | 8 (14.3) | |
| Class IV | 2 (1.0) | 2 (1.4) | 0 (0.0) | |
| Echocardiographic Outcomes | ||||
| LVEF, % (Mean ± SD) | 34.4 ± 10.8 | 33.0 ± 10.6 | 37.7 ± 10.8 | 0.005 |
| LVEF ≥40%, n (%) | 69 (34.8) | 40 (28.4) | 29 (50.9) | 0.003 |
| LVEDD, cm (Mean ± SD) | 5.8 ± 0.9 | 5.9 ± 0.8 | 5.6 ± 1.0 | 0.025 |
| Moderate-Severe MR, n (%) | 94 (48.0) | 76 (54.3) | 18 (32.1) | 0.005 |
| Electrical Outcomes | ||||
| QRS Duration, ms (Mean ± SD) | 151 ± 19.5 | 153 ± 19.3 | 146 ± 19 | 0.017 |
| ΔQRS, ms (Mean ± SD) | 22 | 19 | 31 | 0.036 |
| LVAT, ms (Mean ± SD) | 89.2 ± 14.3 | 92.0 ± 13.7 | 82.6 ± 13.6 | <0.001 |
| Pacing Threshold, V (Median) | 0.8 | 0.8 | 0.6 | <0.001 |
| Impedance, Ohm (Median) | 519 | 570 | 375 | <0.001 |
| Clinical Events | ||||
| Hospitalization (<6 mo), n (%) | 80 (33.1) | 66 (36.7) | 14 (22.6) | 0.042 |
| All-cause Mortality (<6 mo), n (%) | 24 (8.9) | 22 (10.8) | 2 (2.9) | 0.047 |
Values are presented as n (%), mean ± standard deviation, or median. BiVP: Biventricular Pacing; LBBaP: Left Bundle Branch Area Pacing; LVEF: Left Ventricular Ejection Fraction; MR: Mitral Regurgitation.
Long-Term Survival Analysis
During a median follow-up of 41 months (95% CI: 33.9–48.2), 95 patients (35.1%) died. Median overall survival was 73.4 months (95% CI: 60.8–85.9). Estimated survival rates were 82.8% at 2 years and 57.3% at 5 years (Figure 3A).
In univariable Cox regression analysis, predictors of mortality included age, ischemic cardiomyopathy, higher NYHA class, renal dysfunction, and hospitalization within the first 6 months. Pacing modality (LBBaP vs BiVP) was not independently associated with long-term mortality (HR 0.678; p = 0.289) (Figure 3B). Multivariable Cox regression identified baseline eGFR <60 mL/min/1.73 m² (HR 2.495; p < 0.001) and hospitalization within the first 6 months (HR 1.915; p = 0.010) as independent predictors of mortality (Figure 3C–D). Other variables, including age and baseline LVEF, were not independently associated with mortality after adjustment.
Dıscussıon
Main Findings
In this single-center retrospective study, we compared long-term clinical outcomes of left bundle branch area pacing (LBBaP)–CRT and biventricular pacing (BiVP)–CRT in patients with heart failure with reduced ejection fraction. The principal findings were: (1) LBBaP achieved superior electrical resynchronization, reflected by shorter QRS duration and left ventricular activation time (LVAT); (2) at 6 months, LBBaP was associated with greater improvement in left ventricular ejection fraction, fewer heart failure hospitalizations, and lower early mortality; (3) during long-term follow-up, pacing modality was not independently associated with all-cause mortality; and (4) baseline renal dysfunction and early heart failure hospitalization were the strongest predictors of long-term survival.
Physiological Pacing and Electrical Resynchronization
Limitations inherent to conventional BiVP have accelerated interest in physiological pacing strategies. By directly recruiting the His–Purkinje system, LBBaP enables near-native ventricular activation and avoids anatomical constraints associated with coronary sinus lead placement. Consistent with accumulating evidence, our findings demonstrate superior electrical resynchronization with LBBaP, characterized by narrower QRS complexes and shorter LVAT, together with stable and lower pacing thresholds [12].
Importantly, this study extends prior observations by demonstrating that these electrical advantages translate into sustained clinical and structural benefits during extended follow-up. Although further multicenter randomized studies are required, our results support conduction system pacing as a mechanistically sound alternative for CRT delivery.
Electrical Substrate and Patient Complexity
Our cohort exhibited longer baseline QRS duration (171 ± 21 ms) compared with pivotal studies such as I-CLAS (156 ± 29 ms) [13] and reports by Shroff et al. [14] and Vijayaraman et al. [15] (~160 ms), suggesting a population with more advanced electrical dyssynchrony. Additionally, the prevalence of left bundle branch block in the LBBaP group was relatively low (34.3%) compared with previously reported cohorts [13,15,16].
Despite a higher proportion of non-specific intraventricular conduction delay patterns, LBBaP achieved greater QRS narrowing and shorter LVAT than BiVP. These findings align with our previous work demonstrating preservation of ventricular depolarization and repolarization dynamics following LBBaP, supporting the concept that recruitment of the native conduction system enables more homogeneous ventricular activation independent of baseline conduction morphology.
Procedural Performance and Safety
Procedural duration was comparable between groups, consistent with prior studies [15,17]. Notably, radiation exposure was significantly lower with LBBaP. This difference likely reflects the technical complexity of coronary sinus cannulation and branch selection during BiVP implantation, which frequently requires prolonged fluoroscopic guidance.
Complication rates were similar between groups, corroborating existing safety data [13,18]. Physiological pacing may also contribute to electrical stability, as previously suggested by our observations regarding QTc behavior following LBBaP implantation [19], potentially explaining the low incidence of arrhythmic complications.
Reverse Remodeling and Clinical Outcomes
The superior electrical resynchronization achieved with LBBaP translated into greater reverse remodeling at 6 months, with a higher proportion of patients achieving LVEF ≥40%, and significant reductions in LVEDD and mitral regurgitation severity. Although the magnitude of LVEF improvement was modest compared with some reports, [20,21] this likely reflects the complexity of our cohort, characterized by wider baseline QRS duration and lower LBBB prevalence.
The higher use of SGLT2 inhibitors in the LBBaP group represents a potential confounder that may have contributed to improved outcomes. Nevertheless, the consistent association between electrical resynchronization parameters and structural improvement suggests that restoration of physiological activation remained the primary driver of remodeling.
Randomized data support the efficacy of LBBP for CRT. In the LBBP-RESYNC trial, LBBP-CRT achieved greater improvement in LV function compared with BiVP-CRT in patients with nonischemic cardiomyopathy and LBBB at 6 months [7]. In addition, a meta-analysis by Parlavecchio et al., including 10 studies and >1,000 patients reported that LBBP-CRT was associated with improved clinical and electrical/echocardiographic outcomes, including fewer heart-failure hospitalizations compared with BiVP-CRT [22]. These findings are consistent with our observed reductions in early heart-failure hospitalization and improved reverse remodeling, while our extended follow-up provides additional perspective on longer-term survival signals.
Determinants of Long-Term Survival
Despite favorable short-term outcomes, pacing modality was not independently associated with long-term mortality. Instead, renal dysfunction and early heart failure hospitalization emerged as dominant predictors of survival. This observation suggests that correction of electrical dyssynchrony alone may not fully modify long-term prognosis, which appears strongly influenced by systemic disease burden.
The prognostic impact of hospitalization within the first 6 months highlights this interval as a vulnerable phase following CRT implantation, consistent with previous CRT cohorts [15,18]. These findings emphasize the importance of intensified clinical surveillance, early optimization of guideline-directed medical therapy, and proactive device management during early follow-up.
Impact of Ischemic Etiology
The higher prevalence of ischemic cardiomyopathy in the BiVP group represents an important baseline imbalance. Myocardial scar burden is a well-recognized determinant of CRT response and may partly explain the lower degree of reverse remodeling and higher hospitalization rates observed in this group [23]. Nevertheless, comparable long-term survival between groups suggests that systemic comorbidities, particularly renal dysfunction, exert a greater influence on prognosis than pacing modality alone.
Limitations
This study has several limitations. First, its retrospective single-center design introduces potential selection bias and residual confounding related to operator-dependent device selection. Second, although adequately powered for primary analyses, subgroup analyses—particularly according to QRS morphology—may have been underpowered. Third, echocardiographic follow-up was standardized at 6 months and therefore may not fully capture long-term remodeling trajectories. Fourth, detailed electrophysiological characterization distinguishing selective from nonselective LBB capture and postimplant programming optimization were not systematically available. Finally, objective functional capacity assessments such as cardiopulmonary exercise testing or 6-minute walk testing were not routinely performed.
Conclusions
In patients with heart failure with reduced ejection fraction and wide QRS complexes, LBBaP provides superior electrical resynchronization, greater reverse remodeling, and lower radiation exposure compared with conventional BiVP. Although associated with improved short-term clinical outcomes, long-term survival was primarily determined by renal function and early clinical stability rather than pacing modality. LBBaP represents a safe and effective physiological alternative for delivery of cardiac resynchronization therapy.
Author Contributions
Conceptualization, FH, MD, KA, and UC; Methodology, FH, and UC; Validation, FH, MD, KA, and UC; Formal Analysis, FH, MD, and UC; Investigation, FH, and UC; Resources, FH, and UC; Data Curation, FH, and UC; Writing—Original Draft Preparation, FH, MD, and UC; Writing—Review & Editing, FH, MD, KA, and UC; Visualization, FH, MD, KA, and UC; Supervision, KA, and UC.
Funding
None.
Institutional Review Board Statement
Hacettepe University Health Sciences Ethics Committee on November 5, 2024 (Decision Number: 2024/19-09).
Data Availability Statement
Data available on request from the authors.
Conflicts of Interest
UC: Proctorship for Biotronik, Medtronic, and Spectranetics; KA: Proctorship for Boston Scientific, Medtronic, Biosense Webster, and Abbott; Other authors: None declared.
Use of Artificial Intelligence
This case report did not utilize artificial intelligence (AI)-assisted technologies.
Abbreviations
| AF | Atrial Fibrillation |
| AV | Atrioventricular |
| BiVP | Biventricular Pacing |
| BMI | Body Mass Index |
| BNP | B-type Natriuretic Peptide |
| CIED | Cardiac Implantable Electronic Device |
| CRT | Cardiac Resynchronization Therapy |
| CSP | Conduction System Pacing |
| HFrEF | Heart Failure with Reduced Ejection Fraction |
| LAHB | Left Anterior Hemiblock |
| LBBaP | Left Bundle Branch Area Pacing |
| LBBB | Left Bundle Branch Block |
| LOT-CRT | Left Bundle Branch Optimized |
| CRT LVAT | Left Ventricular Activation Time |
| LVEDD | Left Ventricular End-Diastolic Diameter |
| LVEF | Left Ventricular Ejection Fraction |
| NYHA | New York Heart Association |
| RBBB | Right Bundle Branch Block |
References
- Emmons-Bell, S.; Johnson, C.; Roth, G. Prevalence, incidence and survival of heart failure: a systematic review. Heart 2022, 108, 1351–1360. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Wu, S.; Su, L.; Vijayaraman, P.; Zheng, R.; Cai, M.; Xu, L.; Shi, R.; Huang, Z.; Whinnett, Z.I.; Huang, W. Left bundle branch pacing for cardiac resynchronization therapy: nonrandomized on-treatment comparison with His bundle pacing and biventricular pacing. Canadian Journal of Cardiology 2021, 37, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.S.; Wells, G.A.; Talajic, M.; Arnold, M.O.; Sheldon, R.; Connolly, S.; Hohnloser, S.H.; Nichol, G.; Birnie, D.H.; Sapp, J.L.; et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med 2010, 363, 2385–2395. [Google Scholar] [CrossRef] [PubMed]
- Bogale, N.; Priori, S.; Cleland, J.G.; Brugada, J.; Linde, C.; Auricchio, A.; van Veldhuisen, D.J.; Limbourg, T.; Gitt, A.; Gras, D.; et al. The European CRT Survey: 1 year (9-15 months) follow-up results. Eur J Heart Fail 2012, 14, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Padala, S.K.; Ellenbogen, K.A. Left bundle branch pacing is the best approach to physiological pacing. Heart Rhythm O2 2020, 1, 59–67. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, H.; Hou, X.; Wang, Z.; Zou, F.; Qian, Z.; Wei, Y.; Wang, X.; Zhang, L.; Li, X.; et al. Randomized Trial of Left Bundle Branch vs Biventricular Pacing for Cardiac Resynchronization Therapy. J Am Coll Cardiol 2022, 80, 1205–1216. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography 2019, 32, 1–64. [Google Scholar] [CrossRef]
- De Pooter, J.; Wauters, A.; Van Heuverswyn, F.; Le Polain de Waroux, J.-B. A guide to left bundle branch area pacing using stylet-driven pacing leads. Frontiers in Cardiovascular Medicine 2022, 9, 844152. [Google Scholar] [CrossRef]
- Canpolat, U.; Dogan, M.; Aytemir, K. Simplification of left bundle branch area pacing using a novel modified 3-lead pacing system analyzer electrocardiogram technique in the non-electrophysiology laboratory. Journal of Interventional Cardiac Electrophysiology 2025, 1–7. [CrossRef]
- Burri, H.; Jastrzebski, M.; Cano, Ó.; Čurila, K.; de Pooter, J.; Huang, W.; Israel, C.; Joza, J.; Romero, J.; Vernooy, K.; et al. EHRA clinical consensus statement on conduction system pacing implantation: endorsed by the Asia Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS), and Latin American Heart Rhythm Society (LAHRS). Europace 2023, 25, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A.; Saggu, D.; Bhandari, M. Left bundle branch pacing cardiac resynchronization therapy vs biventricular pacing cardiac resynchronization therapy-time to write a requiem for biventricular pacing-cardiac resynchronization therapy. World J Cardiol 2025, 17, 103356. [Google Scholar] [CrossRef] [PubMed]
- Morcos, R.; Vijayaraman, P.; Cano, Ó.; Zanon, F.; Ponnusamy, S.S.; Herweg, B.; Sharma, P.S.; Jastrzebski, M.; Molina-Lerma, M.; Whinnett, Z.I.; et al. Left bundle branch area pacing compared with biventricular pacing for cardiac resynchronization therapy in patients with left ventricular ejection fraction ≤50%: Results from the International Collaborative LBBAP Study (I-CLAS). Heart Rhythm 2025, 22, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Shroff, J.P.; Chandh Raja, D.; Tuan, L.Q.; Abhilash, S.P.; Mehta, A.; Abhayaratna, W.P.; Sanders, P.; Pathak, R.K. Efficacy of left bundle branch area pacing versus biventricular pacing in patients treated with cardiac resynchronization therapy: Select site - cohort study. Heart Rhythm 2024, 21, 893–900. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Sharma, P.S.; Cano, Ó.; Ponnusamy, S.S.; Herweg, B.; Zanon, F.; Jastrzebski, M.; Zou, J.; Chelu, M.G.; Vernooy, K.; et al. Comparison of Left Bundle Branch Area Pacing and Biventricular Pacing in Candidates for Resynchronization Therapy. J Am Coll Cardiol 2023, 82, 228–241. [Google Scholar] [CrossRef]
- Liang, Y.; Xiao, Z.; Liu, X.; Wang, J.; Yu, Z.; Gong, X.; Lu, H.; Yang, S.; Gu, M.; Zhang, L.; et al. Left Bundle Branch Area Pacing versus Biventricular Pacing for Cardiac Resynchronization Therapy on Morbidity and Mortality. Cardiovasc Drugs Ther 2024, 38, 471–481. [Google Scholar] [CrossRef]
- Diaz, J.C.; Tedrow, U.B.; Duque, M.; Aristizabal, J.; Braunstein, E.D.; Marin, J.; Niño, C.; Bastidas, O.; Lopez Cabanillas, N.; Koplan, B.A.; et al. Left Bundle Branch Pacing vs Left Ventricular Septal Pacing vs Biventricular Pacing for Cardiac Resynchronization Therapy. JACC Clin Electrophysiol 2024, 10, 295–305. [Google Scholar] [CrossRef]
- Diaz, J.C.; Sauer, W.H.; Duque, M.; Koplan, B.A.; Braunstein, E.D.; Marín, J.E.; Aristizabal, J.; Niño, C.D.; Bastidas, O.; Martinez, J.M.; et al. Left Bundle Branch Area Pacing Versus Biventricular Pacing as Initial Strategy for Cardiac Resynchronization. JACC Clin Electrophysiol 2023, 9, 1568–1581. [Google Scholar] [CrossRef]
- Doğan, M.; Canpolat, U.; Aytemir, K. A proposal for a novel formula for measurement of corrected QT interval in patients undergoing left bundle branch area pacing. Journal of Electrocardiology 2025, 91, 154030. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Ponnusamy, S.; Cano, Ó.; Sharma, P.S.; Naperkowski, A.; Subsposh, F.A.; Moskal, P.; Bednarek, A.; Dal Forno, A.R.; Young, W.; et al. Left Bundle Branch Area Pacing for Cardiac Resynchronization Therapy: Results From the International LBBAP Collaborative Study Group. JACC Clin Electrophysiol 2021, 7, 135–147. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Cano, O.; Ponnusamy, S.S.; Molina-Lerma, M.; Chan, J.Y.S.; Padala, S.K.; Sharma, P.S.; Whinnett, Z.I.; Herweg, B.; Upadhyay, G.A.; et al. Left bundle branch area pacing in patients with heart failure and right bundle branch block: Results from International LBBAP Collaborative-Study Group. Heart Rhythm O2 2022, 3, 358–367. [Google Scholar] [CrossRef]
- Parlavecchio, A.; Vetta, G.; Caminiti, R.; Coluccia, G.; Magnocavallo, M.; Ajello, M.; Pistelli, L.; Dattilo, G.; Foti, R.; Carerj, S.; et al. Left bundle branch pacing versus biventricular pacing for cardiac resynchronization therapy: A systematic review and meta-analysis. Pacing Clin Electrophysiol 2023, 46, 432–439. [Google Scholar] [CrossRef]
- Yokoshiki, H.; Mitsuyama, H.; Watanabe, M.; Mitsuhashi, T.; Shimizu, A. Cardiac resynchronization therapy in ischemic and non-ischemic cardiomyopathy. Journal of arrhythmia 2017, 33, 410–416. [Google Scholar] [CrossRef]
Figure 1.
Biventricular pacing (BiVP) implantation. (A) Coronary sinus venography demonstrating the coronary venous anatomy and identification of the target lateral branch (arrow) for left ventricular lead placement. (B) Final fluoroscopic image showing successful positioning of the right atrial, right ventricular, and coronary sinus left ventricular leads connected to the cardiac resynchronization therapy device following BiVP implantation.
Figure 1.
Biventricular pacing (BiVP) implantation. (A) Coronary sinus venography demonstrating the coronary venous anatomy and identification of the target lateral branch (arrow) for left ventricular lead placement. (B) Final fluoroscopic image showing successful positioning of the right atrial, right ventricular, and coronary sinus left ventricular leads connected to the cardiac resynchronization therapy device following BiVP implantation.

Figure 2.
Left bundle branch area pacing (LBBaP) implantation. (A) Fluoroscopic right anterior oblique projection demonstrating positioning of the delivery sheath against the interventricular septum and initial lead placement site (arrow). (B) Advancement of the pacing lead into the interventricular septum with progressive penetration toward the left bundle branch area (arrow). (C) Final fluoroscopic image confirming successful LBBaP lead deployment and connection to the CRT device with stable septal positioning.
Figure 2.
Left bundle branch area pacing (LBBaP) implantation. (A) Fluoroscopic right anterior oblique projection demonstrating positioning of the delivery sheath against the interventricular septum and initial lead placement site (arrow). (B) Advancement of the pacing lead into the interventricular septum with progressive penetration toward the left bundle branch area (arrow). (C) Final fluoroscopic image confirming successful LBBaP lead deployment and connection to the CRT device with stable septal positioning.

Figure 3.
Long-term survival analyses. (A) Kaplan–Meier curve showing overall survival of the entire study cohort during follow-up (median overall survival 73.4 months; 95% CI 60.8–85.9). (B) Kaplan–Meier survival comparison between patients receiving BiVP and LBBaP CRT, demonstrating no significant difference in long-term survival (log-rank p = 0.287). (C) Kaplan–Meier survival stratified by baseline renal function, showing significantly reduced survival in patients with estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m² (log-rank p < 0.001). (D) Kaplan–Meier survival according to heart failure hospitalization within the first 6 months after CRT implantation, demonstrating significantly worse survival among hospitalized patients (log-rank p < 0.001).
Figure 3.
Long-term survival analyses. (A) Kaplan–Meier curve showing overall survival of the entire study cohort during follow-up (median overall survival 73.4 months; 95% CI 60.8–85.9). (B) Kaplan–Meier survival comparison between patients receiving BiVP and LBBaP CRT, demonstrating no significant difference in long-term survival (log-rank p = 0.287). (C) Kaplan–Meier survival stratified by baseline renal function, showing significantly reduced survival in patients with estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m² (log-rank p < 0.001). (D) Kaplan–Meier survival according to heart failure hospitalization within the first 6 months after CRT implantation, demonstrating significantly worse survival among hospitalized patients (log-rank p < 0.001).

Table 1.
Baseline demographic, clinical, and laboratory characteristics of the study population.
| Characteristics | Total (n=271) | BiVP (n=203) | LBBaP (n=68) | P-value |
| Demographics | ||||
| Age, years (mean ± SD) | 63.6 ± 13.0 | 64.1 ± 13.1 | 62.4 ± 12.6 | 0.353 |
| Male Sex, n (%) | 188 (69.4) | 147 (72.4) | 41 (60.3) | 0.061 |
| BMI, kg/m² (mean ± SD) | 26.9 ± 4.7 | 26.9 ± 4.6 | 26.7 ± 4.8 | 0.692 |
| Clinical Characteristics | ||||
| Etiology, n (%) | 0.009 | |||
| Ischemic CMP | 129 (47.6) | 106 (52.2) | 23 (33.8) | |
| Non-ischemic CMP | 142 (52.4) | 97 (47.8) | 45 (66.2) | |
| NYHA Functional Class, n (%) | 0.149 | |||
| Class I-II | 133 (49.1) | 95 (46.8) | 38 (55.9) | |
| Class III-IV | 138 (50.9) | 108 (53.2) | 30 (44.1) | |
| Prior CIED History, n (%) | 90 (33.2) | 70 (34.5) | 20 (29.4) | 0.442 |
| Comorbidities, n (%) | ||||
| Hypertension | 201 (74.2) | 152 (74.9) | 49 (72.1) | 0.646 |
| Diabetes Mellitus | 158 (58.3) | 120 (59.1) | 38 (55.9) | 0.640 |
| Cerebrovascular Disease | 35 (12.9) | 29 (14.3) | 6 (8.8) | 0.245 |
| Renal Failure (Dialysis) | 6 (2.2) | 4 (2.0) | 2 (2.9) | 0.643 |
| Medical Therapy, n (%) | ||||
| Beta-blockers | 233 (86.0) | 175 (86.2) | 58 (85.3) | 0.851 |
| ACEI / ARB / ARNI | 219 (80.8) | 166 (81.8) | 53 (77.9) | 0.482 |
| MRA | 154 (56.6) | 109 (53.7) | 45 (66.2) | 0.072 |
| SGLT-2 Inhibitors | 39 (14.4) | 18 (8.9) | 21 (30.9) | <0.001 |
| Loop Diuretics | 186 (68.6) | 139 (68.5) | 47 (69.1) | 0.921 |
| DOAC / Warfarin | 90 (33.2) | 67 (33.0) | 23 (33.8) | 0.901 |
| Amiodarone | 31 (11.4) | 25 (12.3) | 6 (8.8) | 0.434 |
| Digoxin | 42 (15.5) | 33 (16.3) | 9 (13.2) | 0.551 |
| Laboratory Findings | ||||
| Hemoglobin, g/dL | 13.0 ± 1.9 | 13.0 ± 1.9 | 12.9 ± 1.8 | 0.491 |
| Serum creatinine, mg/dL* | 0.96 (0.4-6) | 0.97 (0.4-6) | 0.91 (0.5-3.5) | 0.032 |
| BNP, pg/mL* | 409 (10-7027) | 448 (10-7027) | 347 (10-6018) | 0.282 |
Angiotensin-converting enzyme inhibitor; ARB: Angiotensin receptor blocker; ARNI: Angiotensin receptor-neprilysin inhibitor; BiVP: Biventricular pacing; BMI: Body mass index; BNP: B-type natriuretic peptide; CIED: Cardiac implantable electronic device; CMP: Cardiomyopathy; DOAC: Direct oral anticoagulant; LBBaP: Left bundle branch area pacing; MRA: Mineralocorticoid receptor antagonist; NYHA: New York Heart Association; SD: Standard deviation; SGLT-2: Sodium-glucose cotransporter-2. *** Values are presented as median (minimum-maximum).**.
Table 2.
Baseline electrocardiographic and echocardiographic characteristics of the study population.
Table 2.
Baseline electrocardiographic and echocardiographic characteristics of the study population.
| Parameters | Total (n=271) | BiVP (n=203) | LBBaP (n=68) | P-value |
| Electrocardiographic Findings | ||||
| Rhythm, n (%) | ||||
| Persistent AF | 68 (25.1) | 49 (24.1) | 19 (27.9) | 0.531 |
| Paroxysmal AF | 10 (3.7) | 7 (3.4) | 3 (4.4) | 0.715 |
| Paced Rhythm | 49 (18.1) | 34 (16.7) | 15 (22.1) | 0.325 |
| QRS Duration, ms (mean±SD) | 171±29 | 171±29 | 170±30 | 0.706 |
| QRS Morphology, n (%) | ||||
| LBBB | 114 (44.5) | 91 (48.1) | 23 (34.3) | 0.051 |
| LAHB | 7 (2.7) | 2 (1.1) | 5 (7.5) | 0.015 |
| RBBB | 11 (4.3) | 7 (3.7) | 4 (6.0) | 0.485 |
| IVCD | 71 (27.7) | 53 (28.0) | 18 (26.9) | 0.853 |
| AV Conduction, n (%) | ||||
| 1st Degree AV Block | 20 (7.6) | 11 (5.6) | 9 (13.4) | 0.038 |
| 2nd Degree AV Block | 7 (2.7) | 5 (2.6) | 2 (3.0) | 1.000 |
| Complete AV Block | 53 (20.2) | 36 (18.5) | 17 (25.4) | 0.224 |
| Activation Intervals | ||||
| LVAT, ms (mean±SD) | 104±21.5 | 105±21 | 100±22 | 0.097 |
| LVAT / LVEDD ratio | 17.4±4.3 | 17.5±4.1 | 17.3±4.6 | 0.722 |
| LVAT / QRS Duration ratio | 0.61±0.07 | 0.61±0.07 | 0.59±0.07 | 0.011 |
| Echocardiographic Findings | ||||
| LVEF, % (mean±SD) | 29±7.2 | 29±7 | 30±7.5 | 0.093 |
| LVEDD, cm (mean±SD) | 6.0±0.8 | 6.1±0.7 | 5.9±0.9 | 0.115 |
| LA Diameter, cm (mean±SD) | 4.5±0.8 | 4.6±0.8 | 4.4±0.8 | 0.277 |
| Valvular Pathology (Mod-Severe), n (%) | ||||
| Mitral Regurgitation | 180 (66.7) | 142 (70.3) | 38 (55.9) | 0.029 |
| Tricuspid Regurgitation | 142 (52.6) | 107 (53.0) | 35 (51.5) | 0.830 |
| Aortic Regurgitation | 15 (5.6) | 11 (5.4) | 4 (5.9) | 1.000 |
Values are presented as n (%) or mean±standard deviation. AF: Atrial Fibrillation; LBBB: Left Bundle Branch Block; LAHB: Left Anterior Hemiblock; RBBB: Right Bundle Branch Block; IVCD: Intraventricular Conduction Delay; AV: Atrioventricular; LVAT: Left Ventricular Activation Time; LVEF: Left Ventricular Ejection Fraction; LVEDD: Left Ventricular End-Diastolic Diameter; LA: Left Atrium.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



