Submitted:
27 March 2026
Posted:
31 March 2026
You are already at the latest version
Abstract
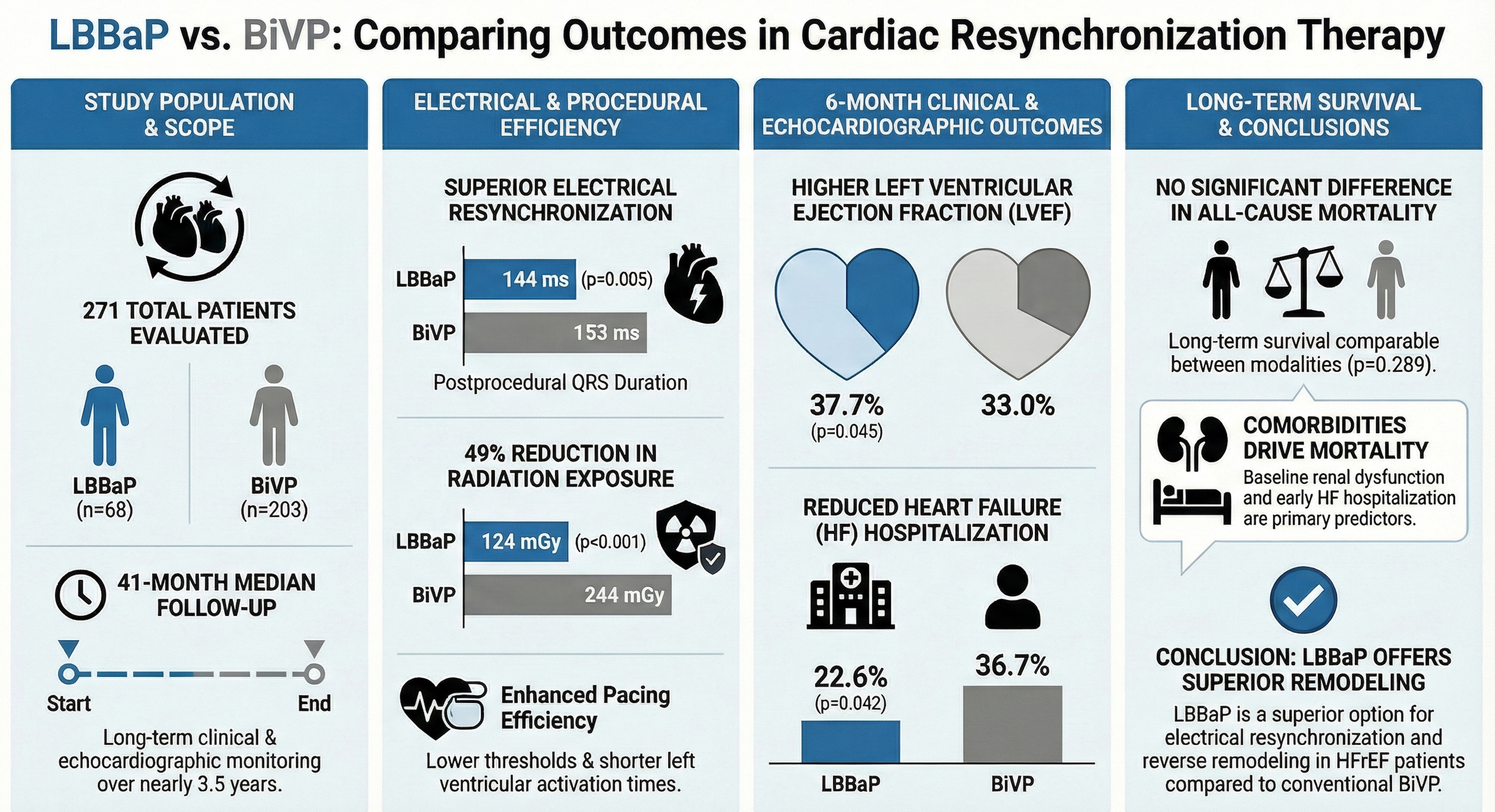
Background: Left bundle branch area pacing (LBBaP) has emerged as a physiological alternative to conventional biventricular pacing (BiVP) for cardiac resynchronization therapy (CRT). We aimed to compare long-term clinical, electrical, and echocardiographic outcomes of LBBaP versus BiVP in patients with heart failure with reduced ejection fraction (HFrEF).
Methods: In this single-center retrospective study, 271 consecutive patients undergoing CRT implantation were included (LBBaP, n = 68; BiVP, n = 203). Outcomes included electrical resynchronization parameters, echocardiographic reverse remodeling, heart failure hospitalization, and all-cause mortality during a median follow-up of 41 months.
Results: LBBaP achieved greater electrical resynchronization, with shorter postprocedural QRS duration (144 vs 153 ms; p = 0.005) and shorter left ventricular activation time compared with BiVP. LBBaP was associated with lower radiation exposure (124 vs 244 mGy; p < 0.001) and lower pacing thresholds. At 6 months, LVEF was higher in the LBBaP group (37.7% vs 33.0%; p = 0.005), and heart failure hospitalization occurred less frequently (22.6% vs 36.7%; p = 0.042). Long-term all-cause mortality did not differ between groups (p = 0.289). In multivariable analysis, baseline renal dysfunction and heart failure hospitalization within 6 months independently predicted mortality.
Conclusions: In patients with HFrEF undergoing CRT, LBBaP provides superior electrical resynchronization and greater reverse remodeling compared with BiVP. Although associated with improved short-term clinical outcomes, long-term survival appears primarily determined by comorbid conditions rather than pacing modality.
Keywords:
cardiac resynchronization therapy
; left bundle branch area pacing
; biventricular pacing
; heart failure with reduced ejection fraction
; conduction system pacing
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



