Submitted:
22 March 2026
Posted:
23 March 2026
Read the latest preprint version here
Preprints on COVID-19 and SARS-CoV-2
Abstract
Tuberculosis (TB) and coronavirus disease 2019 (COVID-19) are among the most significant respiratory diseases, and their significant syndemic interaction in epidemiology during the pandemic period has raised severe global healthcare concerns. Disruption of TB control programs, potential co-infection and common risk factors underscore the need for a systematic assessment of the connection between these diseases. We summarize the current information regarding the relationship between tuberculosis (TB) and COVID-19 during and following the pandemic, including epidemiology; potential pathophysiological connections between SARS-CoV-2 infection and TB; clinical outcomes; and the implications for management. Global estimates of the burden of both diseases are reviewed, along with reported rates of TB–COVID-19 co-infection and associated mortality. The authors discuss mechanistic aspects of Mycobacterium tuberculosis and SARS-CoV-2 immune responses, including how these infections could modulate host immunity, thus impacting susceptibility and outcomes of disease upon co-infection. This review additionally discusses mutually shared risk factors and the broader implications of the COVID-19 pandemic on TB diagnosis, treatment sustainability and public health initiatives. The review also includes current therapeutic approaches and preventive strategies such as vaccination and integrated disease management. Overall, the evidence indicates that the overlap of TB and COVID-19 presents significant diagnostic, clinical and broader public health challenges, especially in settings of high burden. To reduce the combined burden of these infections and restore momentum towards global TB control targets, strengthening surveillance and respiratory disease management, as well as research on immune interactions and long-term outcomes will be the key.
Keywords:
tuberculosis
; SARS-CoV-2
; COVID-19
; coinfection
; mycobacterium
; immune
1. Introduction
The COVID-19 pandemic emerged from China, and its spread has strained the capacities of the healthcare system, which in turn has negatively affected the global economy. As we arrive at the beginning of 2026, the death count has risen to 7,097,789, highlighting the significance of our battle against the virus [1,2]. The RNA virus known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the primary cause of the illness. The symptoms of patients suffering from covid spans broad ranging from asymptomatic infection to life-threatening pneumonia [3].
On the other hand, Tuberculosis (TB) is one of the oldest and most common illnesses, caused by the bacteria Mycobacterium tuberculosis. It affects one-third of the world’s population and drives millions of deaths annually [4]. In 2022, it was reported that an estimated 10.6 million people fell ill with tuberculosis, including 5.8 million men, 3.5 million women, followed by 1.3 million deaths worldwide. [5,6].
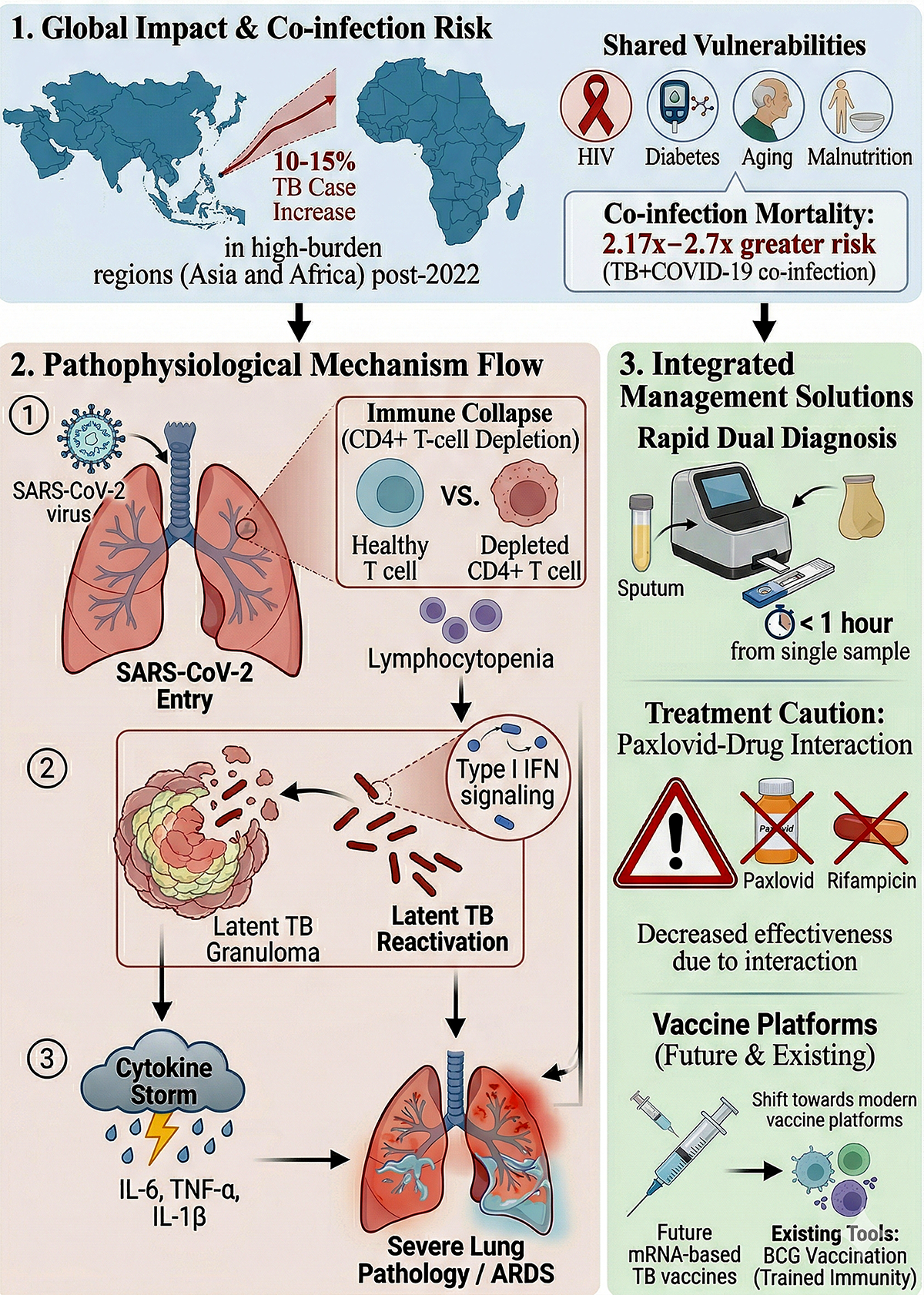
Both the disease TB and COVID-19 are transmitted via airborne particles and droplets and the lung is considered as their core target. Risk factors for these conditions are comparable and include COPD, HIV, diabetes, aging, and immunodeficiency. Co-infection of TB & COVID-19 worsens immune deregulation and paves the way for more severe disease manifestations. In the recent past, the emergence of the COVID-19 pandemic has impacted the TB care system significantly. Health facilities have been distracted from TB diagnosis and treatment from battling against the new threat by disrupting TB diagnosis [7,8]. The time it takes for clinical symptoms to appear is a significant factor in differentiating between these two illnesses; it is quicker for COVID-19 individuals but takes a longer period for Tuberculosis patients [8].
Numerous factors demonstrate that Tuberculosis can aid in the establishment of COVID-19. One of these variables is connected to TB-caused lung damage, which predisposes a person. Another cause is a TB individual’s immunological system, which might make them more susceptible to the COVID-19 outbreak, and resource limitations to monitor it continually in order to prevent the emergence of both illnesses at the same time [8]. Therefore, understanding the dynamics of this “deadly” co-infection is the need of the post-covid era.
This review highlights the interlinkage between TB and COVID-19 as a global burden and the urgent need to address the future risks. It begins with epidemiology and the impact of TB in the post-COVID era, followed by immunological response and long-term complications of both diseases, overlapping comorbidities in TB/COVID-19 cohort patients, as well as preventive measures such as vaccination and challenges in diagnosis and treatment in case of co-existing diseases. The importance of global collaborative efforts, identifying research gaps & possibilities, and legislative changes to improve disease management to mitigate the risks of the twin threat effectively were also discussed.
2. Epidemiology of Tuberculosis and COVID-19
2.1. Global Burden of Tuberculosis
Tuberculosis (TB) poses a significant global impact being one of the primary causes of mortality from an infectious disease. Although since the early 2000s, the number of cases has been decreasing due to improved TB control programs, better surveillance and improvements in socioeconomic status [9]. According to S. Silva et al. annually, TB deaths are decreasing by 2%, estimating 31.8 million TB deaths between 2020-2050, corresponding to an economic loss of around seventeen trillion US dollars [10]. In 2022, the global TB incidence rate was 133/100,000 population, and the global mortality rate was 16.1/100,000 population. Despite of the declining prevalence, multi (MDR) and extensively drug-resistant (XDR) TB continue to be a problem [11].
2.2. Global Burden of COVID-19
The COVID-19 pandemic, which originated from Wuhan, China, was finally deemed a public health emergency of international concern (PHEIC) by the World Health Organisation (WHO) on March 11, 2020. WHO has received reports of 776 million COVID-19 illnesses and 7.1 million fatalities as of July 10, 2024. Based on cumulative number of cases, USA (103 million), China (99.4 million), India (45 million), France (39 million) and Germany (38.4 million) contributing highest number of cases and stands in the top five countries worldwide and on basis of cumulative number of deaths, USA (1.2 million), Brazil (0.7 million), India (0.53 million), Russia (0.4 million) and Mexico (0.33 million) are the top five contributing countries
2.3. Co-infection Rates and Mortality
WHO has grouped the world regions into 7 categories: the African Region, the Region of the Americas, South-East Asia Region, the European Region, the Eastern Mediterranean Region, the Western Pacific Region, and the High TB burden countries. Among these, except the African Region, all the countries have shown an increase in TB incidence and death cases in 2020-2022 during the COVID-19 pandemic.
According to a prevalence study conducted by Daneshvar et al., 2018, among 5843 patients having COVID-19 and 101 patients having COVID-19 and TB both. It was found that 1.1% of patients with confirmed COVID-19 had a TB infection. This rate varies country-wise: 3.6% in Africa, 1.5% in Asia, and 1.1% in the Americas. Among those 1.1% co-infected patients, 20.83% patients died and 65.62% patients recovered. Compared to COVID-19 patients without TB, those with TB had a mortality risk that was 2.7 to 2.17 times greater [12]. Song et al., 2021 have included 36 studies and out of 89 co-infected patients, 19 died (80.90% were male and the majority had active TB – 88.76%). These cases included patients from India, China, and Italy and portrayed that the median age of survivors was less than non-survivors. The mortality rate among these co-infected patients was reported as 23.46%. Co-infected patients are twice as likely to die as compared to patients with COVID-19 but without TB, calculated by odds ratio [13]. Figure 1 illustrates an interesting influence of COVID-19 on TB incidence. The plot shows relatively stable TB incidence until 2019, followed by a downfall in 2020 coinciding with the onset of the COVID-19 pandemic. COVID-19 incidence sharply increased between 2020–2022, peaking in 2022 before declining in 2023, while TB incidence interestingly shown to be sharply increasing post 2020.
2.4. Incidence of Tuberculosis in the Post-COVID Era
The COVID-19 pandemic has severely affected the world’s leading cause of death by a single bacterial infection, Tuberculosis. Globally in 2021, 6.4 million people were diagnosed with TB. Of these, 83% had pulmonary TB, and 90% of total cases were from Asia and Africa. Since the previous two decades, TB incidence cases were annually declining by 2% but in between 2020 and 2021, it reversed to a 3.6% increase. Also, TB deaths were suddenly increased in 2020 (1.5 million), reversing the gradual decline of cases in between 2005-2019 and by 2021, the number of TB deaths were reverted to the same stage where 2017 was lying at that time (1.6 million, 4.5% increase from 2020). Between 2025 and 2020, a cumulative 13.5% drop in TB cases was seen, but in 2021, the cases were only 10% less than in 2015 [14]. According to a study conducted in Brazil, in the time duration 2013 to 2023, a decline of 18% in TB reported cases has been seen between 2019-2020 due the COVID-19 pandemic. Thereafter in 2021-2022, an 16% inclination of TB reported cases was observed [15]. A seven yearlong study from Kazakhstan has revealed that by 2024, TB incidence had declined by 30.5% (33.5 per 100,000) and mortality by 58.3% (1.0 per 100,000), indicating post-pandemic recovery. Globally, TB deaths decreased by about 5.3% from 1.32 million in 2022 to 1.25 million in 2023, suggesting improved global TB control measures [16]. WHO has reported an increase to approximately 10.8 million new TB cases in 2024 and an overall rise in TB incidence of approximately 3.9% between 2020 and 2024, reversing earlier annual declines. A moderate rise in TB incidence seen among pregnant women in the post-COVID era. Globally, women of reproductive age account for about one-third of TB cases, and in high-burden regions like Asia and Africa, TB incidences in pregnancy have increased by 10–15% since 2022. The trend shows that the pandemic has had a secondary effect on TB control [17].

Table 1.
Global evidence on TB–COVID-19 co-infection: prevalence, mortality, and risk estimates.
| Study (Year) | Region | Study design | COVID-19 cases | TB cases with COVID-19 | TB–COVID prevalence (%) | Mortality in co-infected (%) | Key findings |
|---|---|---|---|---|---|---|---|
| [12] | Global | Meta-analysis | 5843 | 101 | 1.1 | 20.8 | TB significantly increased COVID-19 mortality |
| [13] | Multi-country | Systematic review | — | 89 | — | 23.46 | Male predominance; survivors had less median age |
| [18] | Global | Meta-analysis | 2765 | 10-123 | 0.37–4.47 | — | TB associated with severe COVID-19 (OR 2.10); No statistically significant association in mortality (OR 1.40) |
| [19] | Multi-country | Cohort study | 1217 | 49 | — | 12.3 | Active TB worsened COVID outcomes |
| [20] | India | Retrospective cohort | 1073 | 22 | — | 27.3 | Higher ICU admission risk; Treated or Active-T patients both vulnerable to COVID-19 |
| [21] | 34 countries | Prospective cohort | — | 767 | — | 11.08 | Majority had pre-existing TB |
| [22] | Global | Systematic review | — | 146 | — | 13.0 | Co-infected patients had higher mortality than global average of COVID mortality |
| [23] | 31 countries | Longitudinal cohort | 788 | — | 10.8 | Predictors of mortality identified |
3. Pathophysiology of Tuberculosis and COVID-19 Association
3.1. Shared Risk Factors
Co-infection may aggravate immune dysregulation and clinical management. COVID-19 exhibits respiratory conditions analogous to TB, such as difficulty in breathing and cough. Due to convergent signs and symptoms, diagnosing co-infection can be complex and challenging (Cioboata et al., 2023b). Complications include low oxygen levels (hypoxia), respiratory failure, acute respiratory distress syndrome (ARDS), and abnormalities in glucose levels. Some patients require noninvasive ventilation, extended hospital stay, and superimposed bacterial infection (Mishra et al., 2020). The incubation period for TB (lasts two weeks to several years) is greater compared to COVID-19 (1-14 days) (Cioboata et al., 2023c). Stigmatisation of Tuberculosis is considered another significant issue; the overlapping symptoms of TB and COVID-19 create fear and confusion among common people and healthcare workers, leading to stigma. As a result, active TB patients avoid seeking medical treatment, exacerbating the situation (Togun et al., 2020).
A patient with both the disease TB and COVID-19, malnutrition, and a low body mass index (BMI) is at vital risk factor for early mortality. The high mortality rate of TB/COVID-19 cohort patients among older males and migrants is combined with comorbidities such as cardiovascular disease, liver disease, HIV, alcohol abuse, and smoking. Males died more compared to females by likely higher widespread presence of comorbidities and risk factors. Both TB & COVID-19 patients share a disparity of immune response.
Pregnant women with HIV are more likely to develop TB, which can negatively affect both the mother’s and the fetus’s health, pregnant women are one particular group of TB patients who require specialist treatment. Therefore, it is recommended that all pregnant women with HIV get evaluated for TB, even if they do not exhibit any clinical symptoms. To prevent treatment-related issues, pregnant women with TB who have had a COVID-19 infection should consult with cardiologists and have their D-dimer levels monitored (Starshinova et al., 2025b).
3.2. Immune Response in Co-Infection
The intersection of two major infectious disease TB and COVID collide in populations already facing a high burden of infectious disease. The impact of coinfection can range from TB reactivation to severe COVID-19 progression causing higher mortality. Management of tuberculosis (TB) and COVID-19 co-infection become a challenge due to overlapping clinical features. Both Tuberculosis and COVID-19 are associated with elevated Th1 and Th2 cell levels. Declination of Th17 cells takes place in TB, which may worsen with COVID-19. TB alone promote immune regulation by increase in Treg cells, whereas COVID-19 triggers a hyperinflammatory state. Accelerating CD4+ T cell depletion, COVID-19 worsen the latent TB infection which disrupts granuloma integrity.
The Type I IFN signalling pathway has an important function in boosting the development of tuberculosis among individuals coinfected with respiratory viruses and M. tuberculosis (Redford et al., 2014). According to research by L. Donovan et al., (2017) ex vivo data show that host cells that harbor M. tuberculosis bacilli, such as macrophages and myeloid DCs, are a source of type I IFN during infection (Donovan et al., 2017). IFN gamma is detectable in the initial phase of COVID-19 (Gadotti et al., 2020). As a consequence, COVID-19 poses a risk for tuberculosis activation, if already latent. (Musso et al., 2020) The amalgamated effect of COVID-19 and TB infection brings about Lymphocytopenia and a decline in CD4+ cell. This leads to exacerbation of pro-inflammatory cytokines, which results in a cytokine storm of active cells in the lungs, immunopathology, and an increased risk of morbidity and mortality (Luke et al., 2022). Figure 2 gives an illustrative idea on the immune response of the coinfection.
Granuloma plays a major role in latent TB infection; disintegration of granuloma leads to reactivation of infection from latent TB. COVID-19 can further exacerbate TB by triggering type I interferon signalling, accelerating the immune response. COVID-19 influence in reduction of mycobacterium specific CD4+ T cells and increased cytokines like TNF-α and IL-6, reduces the host’s ability to control latent or active TB [24]. Body shows signature immune response in TB-COVID-19 coinfection compared with COVID-19 by increase in TNF-α, macrophage inflammatory protein-1 β, and IL-9 secretion. Another signature where TNF-α, IL-1 β, IL-17A, IL-5, fibroblast growth factor-basic, and granulocyte macrophage colony-stimulating factor has seen to secrete more in coinfected patients compared with patients with TB. Coinfected patients exhibited significantly reduced immune responses specific to SARS-CoV-2 and Mycobacterium tuberculosis, affecting pro-inflammatory cytokines, anti-inflammatory cytokines, and growth factors [25]. The cytokine profile in co-infection is summarized in Figure 3.
3.3. Risk of Tuberculosis as a Long COVID Complication
Long COVID (LC) is the post-acute consequences of SARS-CoV-2 infection where the symptoms persists and new symptoms emerge after four weeks of initial infection [26]. There are several risk factors involved in development of Long Covid (LC) such as asthma, type 2 diabetes mellitus, pre-existing depression, hypothyroidism, and cases of hospitalized severe COVID-19 cases. If a patient feels shortness of breath, fatigue, headaches, myalgia during the acute illness or belongs to older age, female sex, socioeconomic deprivation that means the patient belongs to high-risk group for LC [27]. Patients who suffered severe acute COVID-19 or developed cytokine storm syndrome are more prone to LC due to prolonged inflammation and tissue damage [28].
There are two main ways that LC can make TB more likely to come back: (a) persistent T-cell depletion, which reduces the host’s ability to control latent Mycobacterium tuberculosis, and (b) ongoing inflammation or matricellular dysregulation such as elevated osteopontin (OPN) and galectin-9 (Gal-9) that makes granulomas less stable and changes the structure of lung tissue [29]. According to recent research, latent TB infection may play a role in TB reactivation as part of LC. Lymphopenia, and CD4+ T cell depletion caused by SARS-COV-2 may last into the convalescent phase. Immune surveillance systems that normally maintain TB latency may be compromised by this immune suppression event, which could result in TB reactivation [30]. According to studies, long COVID is characterized by increase in the levels of IL-6, TNF- and other pro-inflammatory cytokines. This persistent inflammation disrupts granuloma structure in latent TB patients leading to progression of active TB. Reduced pulmonary function, such as chronic dyspnea and interstitial lung abnormalities (e.g., fibrosis), can conceal TB symptoms, delaying diagnosis or underreporting cases. [31].
A recent cohort found prior SARS-CoV-2 exposure in newly diagnosed pulmonary TB patients was associated with reduced circulating elastase, a Neutrophil extracellular trap (NET) marker but normal levels of other inflammatory markers. The change in elastase levels was correlated with diabetes status and treatment outcome, suggesting altered neutrophil function after SARS-CoV-2 that could influence TB pathogenesis [32]. Cross-sectional data from LTBI cohorts show that prior SARS-CoV-2 seropositivity is associated with higher levels of several cytokines and chemokines that cause inflammation, such as IFN-γ, IL-2, TNF-α, IL-17, IL-6, and CXCL9/10, and lower levels of IL-10. At the same time, mitogen responses stay the same, which shows that the immune system is reprogramming itself to respond to the antigen [33].
In regions with high TB incidence, the combination of latent TB and long COVID presents a public health risk to immunocompromised and socioeconomically disadvantaged populations. Therefore, it is essential to keep an eye out for TB reactivation in patients recuperating from COVID-19, particularly in those who have underlying LTBI, lung injury, or persistent symptoms.
4. Impact of COVID-19 on Tuberculosis Control Programs
The COVID-19 pandemic has been seen to exacerbate worldwide vulnerability to TB, through terminating health care facilities, poverty, progression, and worsening treatment consequences among those with M. tuberculosis infection [34]. A qualitative study conducted by Garg et al., in Uttarakhand, India to assess impact of COVID-19 on National Tuberculosis Elimination Program (NTEP) highlighted a reduction in TB case report by 17%, an expansion in percentage of missing cases by 54%, and a fall in the treatment success ratio of new cases during pandemic by 45% [35]. In early 2020, due to the emergence and global spread of SARS-CoV-2, interventions executed by different countries to prevent the spread of the COVID-19 pandemic are directing people to reside at home, maintain social distancing, wear masks, etc., till the situation gets normalized. Alongside this initiative has multiple positive aspects in diminishing community wide spreading of COVID-19, similarly on same interval of time it also effected TB treatment and diagnostic facility in many ways: (1) Constraint of reaching the healthcare facility and regular health services; (2) healthcare workers encountered nervousness and panic, pivotal indication of error and grade of checkup; (3) media coverage and focus on pandemic operation with narrow oversight of TB management; (4) fear, anxiety and stigma of COVID-19 infection, demoralized common individuals from undergoing TB regime. All these components come up with the hindrance in the onset of treatment and delay in diagnosis (Alene et al., 2020; Sahu et al., 2022). Bacilli Calmette-Guerin (BCG) vaccination is considered a promising preventive measure towards TB treatment, have also been negatively affected by the COVID-19 pandemic [36].
Nigeria reported fewer TB diagnoses and cases in 2020 than in 2019, which may have been brought on by the COVID-19 pandemic and a lapse in TB diagnosis and treatment [37]. A modelling study undertaken by Cilloni et al.(2020) showed India would experience an additional 1.65 million TB cases and 438,000 TB deaths over the next 5 years as a result of the lockdown brought on by the COVID-19 pandemic [38].
Table 2.
Impact of the COVID-19 pandemic on TB control programs and outcomes.
| Indicator | Pre-COVID baseline | During COVID | Post-COVID trend | Region / Study | Reference |
|---|---|---|---|---|---|
| TB case notifications | Gradual decline | 15–35% reduction | Partial recovery | Global | [14] |
| TB mortality | Declining | Increased (2020–21) | Decreasing after 2022 | Global | [39] |
| Diagnostic delays | Routine diagnosis | Major delays | Improved but uneven | Global | [40] |
| DOTS access | Routine | Severely disrupted | Tele-DOTS adoption | India | [35] |
| Gene-Xpert use | TB diagnosis | Repurposed for COVID | Gradual restoration | Multi-country | [41] |
| Hospitalization rates | Baseline | Increased in co-infected | Stabilizing | Global cohort | [42] |
| Health system strain | Focused TB services | Resource diversion | Program rebuilding | Global | [39] |
| MDR/XDR TB risk | Baseline | Increased risk | Ongoing concern | Global model | [38] |
5. Management of Co-Infection
5.1. Therapeutic Strategies for Tuberculosis in Association with COVID-19
Across multiple studies we covered in our review, a finite number of studies provide information on the treatment of TB-COVID-19 co-infection. The pair of diseases, COVID-19 and TB, showed long-established effects on respiratory function and relative health. Since TB and COVID-19 share identical signs and symptoms, integrating and jointly screening symptoms of patients within existing TB services warrants early diagnosis and optimizing resource utilization [43]. In this review, we have highlighted three studies that emphasize the utilization of Intensive Care Units (ICUs) in the management of co-infection. The patients being admitted to the ICU varied from 1.3% to 31.8% [20,44,45]. Several chemotherapeutics such as hydroxychloroquine, azithromycin, lopinavir/ ritonavir, and darunavir/ cobicistat combination were employed to treat coinfection (Motta et al., 2020; Tadolini et al., 2020b). Some reports indicated the administration of anticoagulation (enoxaparin, parnaparin) as well (Tadolini et al., 2020c).
Wang Y. et al. (2022) reported consumption of Nirmatrelvir/ritonavir (an anti-viral remedial for COVID-19 treatment) a cytochrome P450 3A4 inhibitor and highlighted its contraindication in persons taking rifampicin (primary treatment for TB) because of drug interaction. Therefore, Nirmatrelvir/ritonavir was not considered an appropriate drug for treating persons with active TB-COVID co-infection receiving anti-TB treatment (ATT). Despite the severity of the infectious nature of the Omicron variant, persons with TB-COVID-19 co-infections do not show the expected severity of Omicron infection. [46].
A cross-sectional study conducted by Kabbur S et al. (2023) in India assessed that TB patients faced hindered access to DOTs treatment during the COVID-19 lockdown [47]. Telemedicine along with telemonitoring and teleconsultation has demonstrated efficacy in enabling remote patient management, guaranteeing access to medical services, and enhancing treatment protocol adherence. Future TB care can be strengthened by utilizing these technological advancements and digital health solutions. By eliminating the need for in-person visits and removing geographic restrictions, it can facilitate the distant diagnosis and follow-up of TB patients [48,49,50].
The study by Huang et al. (2023) reveals that there is a substantial transcriptome overlap between SARS-CoV-2 and TB, suggesting that there may be molecular interaction during co-infection. Three key hub genes—GAS6, OAS3, and PDCD1LG2—that control immunological dysregulation and interferon signaling pathways have been found, along with 124 common differentially expressed genes, using integrated bioinformatics and machine-learning analysis. This highlights that TB–COVID-19 co-infection is a mechanistically linked state rather than just a clinical cohabitation, necessitating more functional validation and investigation of host-directed treatment options.
5.2. Preventive Measures: Vaccination Programs
Bacillus Calmette-Guérin (BCG) is the only licensed vaccine developed and available for a long time that induces protection against Tuberculosis and has a non-specific (off-target) immune reaction that defends against a broad range of infections [51]. In some studies, the BCG vaccine is reported to reduce the severity of infection caused by a similar single-stranded positive-sense RNA virus like SARS-CoV-2. For instance, among Dutch volunteers, the BCG vaccination decreased viraemia caused by the yellow fever vaccine by 71% [52]. In two other studies, it significantly decreased the severity of mengovirus (encephalomyocarditis virus) infection in mice model. [53,54].
The BRACE trial (NCT04327206) Phase III, a randomized, double-blind study, aimed to investigate whether the BCG vaccine can protect healthcare workers against COVID-19 in several countries [51,55,56]. The result showed that the BCG vaccine, along with some live vaccine, prompts epigenetic and metabolic changes that boost the innate immune response to lower the risk of subsequent infection, a process called trained immunity [57]. One of the most favourable candidates, M72-AS01E, stepped into a phase III clinical trial to investigate the ability to slow down the severity of TB. Previously, the same candidate showed 54% protection against active pulmonary TB in a phase IIb preventive trial [58].
The dawn of mRNA vaccines marks a paradigm shift in the fight against TB. Its benefits include high efficiency, humoral and cellular immune activation, and safety (no genome integration). Antigen selection, however, is the primary bottleneck. A possible remedy is provided by rational design of multi antigen construction, such as BioNTech’s BNT164 (Ag85A, Esat, M72, VapB47, Rpf A/D) [59].
Researchers revealed neutralizing antibodies specific for the receptor binding domain (RBD) inside the Spike protein aimed at the angiotensin converting enzyme 2 (ACE-2) receptor diminish infection by preventing attachment to and entrance into host cells of SARS-CoV-2. There are no neutralizing antibodies against protective antigens in TB due to the intracellular habitat of M. tuberculosis, which is mostly found in macrophages. There is growing evidence that non-neutralizing antibodies play a part in protective immunity by activating several effector functions [60]. In recent times, several TB & COVID vaccines are in controlled clinical trials; however, there is no report of a unique vaccine that offers protection in case of the TB-COVID association. The focus is still directed at preventing the disease individually.
6. Challenges and Future Directions
6.1. Challenges in Diagnosis and Treatment
Bilateral ground glass opacities in CT scan were more frequent in COVID-19, and likewise, cavitary lesions in TB [7,21,61]
There are several traditional TB diagnostic methods available. One of them is smear microscopy, which is widely used but has a low sensitivity. TB culture takes 3-8 weeks to diagnose TB, leading to delayed treatment. However, TB detection has improved with the Gene-Xpert MTB/RIF assay, but its availability is limited in low-resource areas [41].
Before the occurrence of COVID-19, TB was the deadliest infection. The COVID-19 pandemic has significantly disrupted TB diagnosis worldwide. The reason behind the differential diagnosis of TB and COVID becomes so difficult is that both infections show similar respiratory symptoms like cough, difficulty in breathing, and fever. This can lead to underreporting or misinterpretation of TB cases. In 2020, during the pandemic, all the healthcare resource was allocated for COVID-19 management, which led to a decline of TB case detection by 20% compared to 2019. Europe was severely disrupted by the pandemic, and more than 56% of TB labs throughout Europe faced a shortage of healthcare staff, personal protective equipment (PPE). A study conducted in Malawi showed a 35.9% decrease in TB detection immediately after the start of COVID-19 [62]. The number of patients beginning TB preventive medications in 2020 decreased by 21% as a result of the pandemic-induced delay in the onset of TB therapy. Lockdown and transportation restrictions slowed down the supply chain of anti-TB drugs, leading to a shortage of resources. Fear of contracting COVID-19 restrained people from visiting health facilities [63]. Gene-Xpert machines were repurposed for COVID-19 testing, limiting TB diagnosis. Due to a lack of cost-effective, rapid diagnostic tools, it is going to be difficult to detect both TB and COVID-19 simultaneously. Overall, the healthcare system was prioritizing COVID-19 testing over TB case detection [41].
However, to address the diagnosis challenges, [64] introduced and evaluated the Truenat MTB Ultima/COVID-19 multiplex assay, a portable, chip-based real-time PCR platform capable of detecting both Mycobacterium tuberculosis and SARS-CoV-2 from a single sample within one hour. By utilizing different specimens like nasopharyngeal and tongue swabs, it reduces biosafety hazards and diagnostic wait times. The research demonstrated that combined molecular testing and comorbidity assessment facilitate early simultaneous identification and improved treatment of co-infected or high-risk individuals, providing an effective approach for TB–COVID diagnosis in settings with limited resources
6.2. Research Gaps and Opportunities
The topic, interaction between TB and COVID-19, has a lot of scope for research. Several research gaps need to be addressed to improve differential diagnosis and treatment of both or treatment when one is co-infected. There is limited understanding of the immunopathological interplay between Mycobacterium tuberculosis (Mtb) and SARS-CoV-2, how co-infection alters innate and adaptive immune responses, such as IFN and TNF signaling [65]. Limited data regarding the link between COVID and latent TB reactivation has been published. Limited availability of data on studies showing the drug interactions between these two. The long-term pulmonary consequences in a pre-existing TB patient coinfected with COVID-19 still remain porrly elucidated [66].
The cross-sectional studies mostly are with small samples, to find the cause, we need longitudinal and mechanistic tests, the timeline by which SARS-CoV-2 alters Mtb-specific immunity (and vice versa). There is also limited data on how HIV co-infection, anti-TB therapy, corticosteroids, and SARS-CoV-2 vaccination modify these interactions [67].
Moreover, underreporting and restricted monitoring in countries with a high burden of TB mask the actual prevalence and results of co-infection. The effects of co-infection on T-cell functionality, cytokine imbalance, and immune fatigue are still uncertain, emphasizing the necessity for thorough immunological and transcriptomic research. Also, BCG vaccination has not demonstrated a reliable protective effect against COVID-19 in extensive clinical trials, emphasizing the necessity for innovative vaccines or adjuvant strategies that can provide dual protection [65].
The translation challenge in drug-discovery for tuberculosis in complex disease settings was highlighted by a recent study where they reported a novel series of indazole derivatives with combined antiviral, anticancer, and anti-tuberculosis activities. One lead compound, 6-(1H-pyrazol-4-yl)-1H-indazole, demonstrated multi-target potency in vitro but also showed high in vivo toxicity. [68]
The pandemic has increased the risk of drug-resistant TB (MDR-TB and XDR-TB), which requires new treatment strategies. Innovative combined therapies that can effectively treat the twin threat of TB and COVID. There are lots of opportunities for future research. Development of mRNA-based TB vaccine and development of diagnostic multiplex platforms that can detect both simultaneously are among them. Following the recent advancements around the globe, AI & machine learning integration is also not remain a big task to integrate here [66,69].
7. Conclusions
The interconnection of TB and COVID-19 is an ongoing global health problem, like a twin threat. Before the pandemic, TB was the deadliest disease caused by a single bacterium. Since 2020, the COVID-19 pandemic has largely impacted the influence of TB control programs, also suppressing TB diagnosis and treatment.
One of the most serious concerns is the long-term consequences of COVID-19 on TB progression and immune response. These interactions at both the immunological and clinical levels are poorly understood and are crucial for improving patient health by taking proper patient care. The way the pandemic refuelled the surge of rapid vaccine development globally also brings up the urgency of advancement in mRNA-based TB vaccine development, which may become a future breakthrough. Scientists are trying to use artificial intelligence and machine learning to enhance diagnostics and epidemiological tracking in both TB and COVID-19 surveillance. Lastly, a global coordinated effort is needed to mitigate the effects of the pandemic on controlling TB. There are a few steps to be required to taken so that the TB epidemic can be eliminated by 2030, such as improvement in health infrastructure and fostering interdisciplinary research.
References
- Triggle, CR; Bansal, D; Ding, H; et al. A Comprehensive Review of Viral Characteristics, Transmission, Pathophysiology, Immune Response, and Management of SARS-CoV-2 and COVID-19 as a Basis for Controlling the Pandemic. Front Immunol 2021, 12, 631139. [Google Scholar] [CrossRef]
- WHO COVID-19 dashboard. 2025. Available online: https://data.who.int/dashboards/covid19/deaths?n=o.
- Bahceci, I; Yildiz, IE; Duran, OF; et al. Secondary Bacterial Infection Rates Among Patients With COVID-19. Cureus 2022, 14, e22363. [Google Scholar] [CrossRef]
- Natarajan, A; Beena, PM; Devnikar, AV; et al. A systemic review on tuberculosis. Indian J Tuberc 2020, 67, 295–311. [Google Scholar] [CrossRef]
- Stewart, GR; Robertson, BD; Young, DB. Tuberculosis: a problem with persistence. Nat Rev Microbiol 2003, 1, 97–105. [Google Scholar] [CrossRef]
- Tuberculosis WHO. 7 November 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis.
- Cioboata, R; Biciusca, V; Olteanu, M; et al. COVID-19 and Tuberculosis: Unveiling the Dual Threat and Shared Solutions Perspective. J Clin Med 2023, 12, 4784. [Google Scholar] [CrossRef] [PubMed]
- Koupaei, M; Naimi, A; Moafi, N; et al. Clinical Characteristics, Diagnosis, Treatment, and Mortality Rate of TB/COVID-19 Coinfectetd Patients: A Systematic Review. Front Med 2021, 8, 740593. [Google Scholar] [CrossRef]
- Glaziou, P; Sismanidis, C; Floyd, K; et al. Global Epidemiology of Tuberculosis. Cold Spring Harb Perspect Med 2015, 5, a017798–a017798. [Google Scholar] [CrossRef] [PubMed]
- Silva, S; Arinaminpathy, N; Atun, R; et al. Economic impact of tuberculosis mortality in 120 countries and the cost of not achieving the Sustainable Development Goals tuberculosis targets: a full-income analysis. Lancet Glob Health 2021, 9, e1372–e1379. [Google Scholar] [CrossRef] [PubMed]
- Shang, W; Cao, G; Jing, W; et al. Global Burden of Tuberculosis in Adolescents and Young Adults: 1990–2019. Pediatrics 2024, 153, e2023063910. [Google Scholar] [CrossRef]
- Daneshvar, P; Hajikhani, B; Sameni, F; et al. COVID-19 and tuberculosis coinfection: An overview of case reports/case series and meta-analysis of prevalence studies. Heliyon 2023, 9, e13637. [Google Scholar] [CrossRef]
- Song, W; Zhao, J; Zhang, Q; et al. COVID-19 and Tuberculosis Coinfection: An Overview of Case Reports/Case Series and Meta-Analysis. Front Med 2021, 8, 657006. [Google Scholar] [CrossRef] [PubMed]
- Falzon, D; Zignol, M; Bastard, M; et al. The impact of the COVID-19 pandemic on the global tuberculosis epidemic. Front Immunol 2023, 14, 1234785. [Google Scholar] [CrossRef]
- Do Bem Braga, RC; Meurer, IR; D’Carmo Sodré, MM; et al. Epidemiology of tuberculosis in Minas Gerais, Brazil, between 2013 and 2023 and the impact of the COVID-19 pandemic. Front Public Health 2025, 13, 1642015. [Google Scholar] [CrossRef] [PubMed]
- Bekshin, Z; Askarov, A; Abduraimov, Y; et al. Tuberculosis and Impact of COVID-19 on Spread of Epidemics in Kazakhstan. Pathogens 2025, 14, 559. [Google Scholar] [CrossRef]
- Starshinova, A; Belyaeva, E; Irtyuga, O; et al. Tuberculosis in Pregnant Women After COVID-19: Features of Prevention, Diagnosis, and Treatment (Narrative Review). J Clin Med 2025, 14, 5681. [Google Scholar] [CrossRef]
- Gao, Y; Liu, M; Chen, Y; et al. Association between tuberculosis and COVID-19 severity and mortality: A rapid systematic review and meta-analysis. J Med Virol 2021, 93, 194–196. [Google Scholar] [CrossRef]
- Tadolini, M; Codecasa, LR; García-García, J-M; et al. Active tuberculosis, sequelae and COVID-19 co-infection: first cohort of 49 cases. Eur Respir J 2020, 56, 2001398. [Google Scholar] [CrossRef]
- Gupta, N; Ish, P; Gupta, A; et al. A profile of a retrospective cohort of 22 patients with COVID-19 and active/treated tuberculosis. Eur Respir J 2020, 56, 2003408. [Google Scholar] [CrossRef]
- The TB/COVID-19 Global Study Group. Tuberculosis and COVID-19 co-infection: description of the global cohort. Eur Respir J 2022, 59, 2102538. [CrossRef]
- Koupaei, M; Naimi, A; Moafi, N; et al. Clinical Characteristics, Diagnosis, Treatment, and Mortality Rate of TB/COVID-19 Coinfectetd Patients: A Systematic Review. Front Med 2021, 8, 740593. [Google Scholar] [CrossRef] [PubMed]
- Casco, N; Jorge, AL; et al.; Global Tuberculosis Network and TB/COVID-19 Global Study Group Long-term outcomes of the global tuberculosis and COVID-19 co-infection cohort. Eur Respir J 2023, 62, 2300925. [Google Scholar] [PubMed]
- Starshinova, A; Kudryavtsev, I; Rubinstein, A; et al. Tuberculosis and COVID-19 Dually Affect Human Th17 Cell Immune Response. Biomedicines 2023, 11, 2123. [Google Scholar] [CrossRef]
- Najafi-Fard, S; Aiello, A; Navarra, A; et al. Characterization of the immune impairment of patients with tuberculosis and COVID-19 coinfection. Int J Infect Dis 2023, 130, S34–S42. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A; Sehgal, K; Gupta, A; et al. Post-acute COVID-19 syndrome. Nat Med 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Perumal, R; Shunmugam, L; Naidoo, K; et al. Long COVID: a review and proposed visualization of the complexity of long COVID. Front Immunol 2023, 14, 1117464. [Google Scholar] [CrossRef]
- Al-Aly, Z; Xie, Y; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef]
- Shete, A; Ghate, M; Iwasaki-Hozumi, H; et al. Association of SARS-CoV-2 Seropositivity with Persistent Immune Activation in HIV/Tuberculosis Co-Infected Patients. Y Rep 2024, 7, 61. [Google Scholar] [CrossRef]
- Aiello, A; Najafi-Fard, S; Goletti, D. Initial immune response after exposure to Mycobacterium tuberculosis or to SARS-COV-2: similarities and differences. Front Immunol 2023, 14, 1244556. [Google Scholar] [CrossRef] [PubMed]
- Proal, AD; VanElzakker, MB. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front Microbiol 2021, 12, 698169. [Google Scholar] [CrossRef]
- Joseph, NH; Natarajan, AP; Natarajan, S; et al. Previous COVID-19 infection significantly reduces elastase levels in newly diagnosed pulmonary tuberculosis patients. Front Immunol 2025, 16, 1586789. [Google Scholar] [CrossRef]
- Rajamanickam, A; Pavan Kumar, N; Chandrasekaran, P; et al. Effect of SARS-CoV-2 seropositivity on antigen – specific cytokine and chemokine responses in latent tuberculosis. Cytokine 2022, 150, 155785. [Google Scholar] [CrossRef] [PubMed]
- McQuaid, CF; Vassall, A; Cohen, T; et al. The impact of COVID-19 on TB: a review of the data. Int J Tuberc Lung Dis 2021, 25, 436–446. [Google Scholar] [CrossRef]
- Garg, K; Bahurupi, Y; Aggarwal, P; et al. Impact of COVID-19 on the National Tuberculosis Elimination Program in Uttarakhand, India: A Mixed-Methods Research Study. Infect Prev Pract 2023, 5, 100269. [Google Scholar] [CrossRef]
- McQuaid, CF; Vassall, A; Cohen, T; et al. The impact of COVID-19 on TB: a review of the data. Int J Tuberc Lung Dis 2021, 25, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Adewole, OO. Impact of COVID-19 on TB care: experiences of a treatment centre in Nigeria. Int J Tuberc Lung Dis 2020, 24, 981–982. [Google Scholar] [CrossRef] [PubMed]
- Cilloni, L; Fu, H; Vesga, JF; et al. The potential impact of the COVID-19 pandemic on the tuberculosis epidemic a modelling analysis. EClinicalMedicine 2020, 28, 100603. [Google Scholar] [CrossRef]
- WHO, CO; World health organization. Responding Community Spread COVID-19 Ref WHOCOVID-19CommunityTransmission20201.
- Semnani, K; Esmaeili, S. Nuances in the global impact of COVID-19 on tuberculosis control efforts: An updated review. Medicine (Baltimore) 2025, 104, e42195. [Google Scholar] [CrossRef]
- Kabir, S; Parash, MTH; Emran, NA; et al. Diagnostic challenges and Gene-Xpert utility in detecting Mycobacterium tuberculosis among suspected cases of Pulmonary tuberculosis. PLOS ONE 2021, 16, e0251858. [Google Scholar] [CrossRef]
- Dai, B; Chen, C; Shen, Y; et al. Hospitalizations trends and co-infection patterns for respiratory virus infections in children in central China 2015 to 2023: a longitudinal surveillance study. BMC Infect Dis 2025, 25, 1058. [Google Scholar] [CrossRef]
- Malik, AA; Hussain, H; Maniar, R; et al. Integrated Tuberculosis and COVID-19 Activities in Karachi and Tuberculosis Case Notifications. Trop Med Infect Dis 2022, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Otlu, B; Yakupoğullari, Y; Tanriverdi̇, ES; et al. Tüberküloz Hastalarında Gelişen COVID-19’un Klinik Özellikleri. In MİKROBİYOLOJİ Bül.
- Wang, Y; Chen, Y; Gu, L; et al. The clinical characteristics and risk factors for severe COVID-19 in patients with COVID-19 and tuberculosis coinfection. Front Microbiol 2022, 13, 1061879. [Google Scholar] [CrossRef]
- Wang, Y; Chen, Y; Gu, L; et al. The clinical characteristics and risk factors for severe COVID-19 in patients with COVID-19 and tuberculosis coinfection. Front Microbiol 2022, 13. [Google Scholar] [CrossRef]
- Kabbur, S; Patil, B; Angolkar, M; et al. Effect of pandemic on DOTS treatment during COVID-19 lockdown- A cross-sectional study. Indian J Tuberc 2023, 70, 324–328. [Google Scholar] [CrossRef]
- Anawade, PA; Sharma, D; Gahane, S. A Comprehensive Review on Exploring the Impact of Telemedicine on Healthcare Accessibility. Cureus 2024. [Google Scholar] [CrossRef]
- Bouabida, K; Lebouché, B; Pomey, M-P. Telehealth and COVID-19 Pandemic: An Overview of the Telehealth Use, Advantages, Challenges, and Opportunities during COVID-19 Pandemic. Healthcare 2022, 10, 2293. [Google Scholar] [CrossRef] [PubMed]
- Haleem, A; Javaid, M; Singh, RP; et al. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sens Int 2021, 2, 100117. [Google Scholar] [CrossRef] [PubMed]
- Curtis, N; Sparrow, A; Ghebreyesus, TA; et al. Considering BCG vaccination to reduce the impact of COVID-19. The Lancet 2020, 395, 1545–1546. [Google Scholar] [CrossRef]
- Arts, RJW; Moorlag, SJCFM; Novakovic, B; et al. BCG Vaccination Protects against Experimental Viral Infection in Humans through the Induction of Cytokines Associated with Trained Immunity. Cell Host Microbe 2018, 23, 89–100.e5. [Google Scholar] [CrossRef]
- Floc’h, F; Werner, GH. Increased resistance to virus infections of mice inoculated with BCG (Bacillus calmette-guérin). Ann Immunol 1976, 127, 173–186. [Google Scholar]
- Old, LJ; Benacerraf, B; Clarke, DA; et al. The role of the reticuloendothelial system in the host reaction to neoplasia. Cancer Res 1961, 21, 1281–1300. [Google Scholar]
- Pittet, LF; Messina, NL; Gardiner, K; et al. BCG vaccination to reduce the impact of COVID-19 in healthcare workers: Protocol for a randomised controlled trial (BRACE trial). BMJ Open 2021, 11, e052101. [Google Scholar] [CrossRef]
- Pittet, LF; Messina, NL; Orsini, F; et al. Randomized Trial of BCG Vaccine to Protect against Covid-19 in Health Care Workers. N Engl J Med 2023, 388, 1582–1596. [Google Scholar] [CrossRef] [PubMed]
- Netea, MG; Domínguez-Andrés, J; Barreiro, LB; et al. Defining trained immunity and its role in health and disease. Nat Rev Immunol 2020, 20, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Tait, DR; Hatherill, M; Van Der Meeren, O; et al. Final Analysis of a Trial of M72/AS01E Vaccine to Prevent Tuberculosis. N Engl J Med 2019, 381, 2429–2439. [Google Scholar] [CrossRef]
- Li, J; Liu, D; Li, X; et al. RNA vaccines: The dawn of a new age for tuberculosis? Hum Vaccines Immunother 2025, 21, 2469333. [Google Scholar] [CrossRef]
- Kaufmann, SHE. Vaccine development against tuberculosis before and after Covid-19. Front Immunol 2023, 14, 1273938. [Google Scholar] [CrossRef]
- Mishra, A; George, AA; Sahu, KK; et al. Tuberculosis and COVID-19 Co-infection: An Updated Review. Acta Bio-Medica Atenei Parm 2020, 92, e2021025. [Google Scholar]
- Soko, RN; Burke, RM; Feasey, HRA; et al. Effects of Coronavirus Disease Pandemic on Tuberculosis Notifications, Malawi. Emerg Infect Dis 2021, 27, 1831–1839. [Google Scholar] [CrossRef]
- Jeong, Y; Min, J. Impact of COVID-19 Pandemic on Tuberculosis Preventive Services and Their Post-Pandemic Recovery Strategies: A Rapid Review of Literature. J Korean Med Sci 2023, 38, e43. [Google Scholar] [CrossRef]
- Purohit, M; Ssengooba, W; Cox, H; et al. Performance evaluation of the Molbio diagnostics Truenat MTB Ultima/COVID-19 multiplex assay for TB and COVID-19 case detection among people with symptoms suggestive of tuberculosis—a study protocol for clinical trials. Front Public Health 2025, 13, 1620210. [Google Scholar] [CrossRef]
- Booysen, P; Wilkinson, KA; Sheerin, D; et al. Immune interaction between SARS-CoV-2 and Mycobacterium tuberculosis. Front Immunol 2023, 14, 1254206. [Google Scholar] [CrossRef]
- D’Souza, MP; Palin, AC; Calder, T; et al. Mind the gap from research laboratory to clinic: Challenges and opportunities for next-generation assays in human diseases. Vaccine 2021, 39, 5233–5239. [Google Scholar] [CrossRef] [PubMed]
- Flores-Lovon, K; Ortiz-Saavedra, B; Cueva-Chicaña, LA; et al. Immune responses in COVID-19 and tuberculosis coinfection: A scoping review. Front Immunol 2022, 13, 992743. [Google Scholar] [CrossRef] [PubMed]
- Anastasia, K; Evgenya, K; Vera, S; et al. New Indazole Derivatives as Potential Scaffolds for the Development of Anticancer, Antiviral, and Anti-tuberculosis Chemotherapeutic Compounds. Curr Med Chem 2025, 32. [Google Scholar] [CrossRef]
- Crisan-Dabija, R; Grigorescu, C; Pavel, C-A; et al. Tuberculosis and COVID-19: Lessons from the Past Viral Outbreaks and Possible Future Outcomes. Can Respir J 2020, 2020, 1–10. [Google Scholar] [CrossRef]
Figure 1.
Global incidence of Tuberculosis and COVID-19 in between 2015 & 2023. The yellow line represents TB incidence (in millions, left y-axis), while the blue line represents COVID-19 incidence (in millions, right y-axis).
Figure 1.
Global incidence of Tuberculosis and COVID-19 in between 2015 & 2023. The yellow line represents TB incidence (in millions, left y-axis), while the blue line represents COVID-19 incidence (in millions, right y-axis).

Figure 2.
Immunological responses involved in the synergistic effect of Tuberculosis and COVID-19 infection. This illustration showing the combined impact of SARS-CoV-2 and Mycobacterium tuberculosis on lung pathology. Co-infection is associated with lymphocytopenia, decline in CD4⁺ T cell populations in infected lungs compared to healthy lungs, and excessive immune activation leading to a cytokine storm mediated by macrophages.
Figure 2.
Immunological responses involved in the synergistic effect of Tuberculosis and COVID-19 infection. This illustration showing the combined impact of SARS-CoV-2 and Mycobacterium tuberculosis on lung pathology. Co-infection is associated with lymphocytopenia, decline in CD4⁺ T cell populations in infected lungs compared to healthy lungs, and excessive immune activation leading to a cytokine storm mediated by macrophages.

Figure 3.
Immunological outcomes of TB, COVID-19 co-infection. The Venn diagram highlights distinct and overlapping immune responses. TB is associated with reduced Th17 cells, diminished Mtb specific CD4⁺ cells, loss of granuloma integrity, and lymphocytopenia, whereas COVID-19 infection shows increased Type I interferons, TNF-α, IL-5, IL-6, IL-9, IL-10, IL-17A, and MIP-1β.
Figure 3.
Immunological outcomes of TB, COVID-19 co-infection. The Venn diagram highlights distinct and overlapping immune responses. TB is associated with reduced Th17 cells, diminished Mtb specific CD4⁺ cells, loss of granuloma integrity, and lymphocytopenia, whereas COVID-19 infection shows increased Type I interferons, TNF-α, IL-5, IL-6, IL-9, IL-10, IL-17A, and MIP-1β.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



