Submitted:
13 March 2026
Posted:
16 March 2026
You are already at the latest version
Abstract
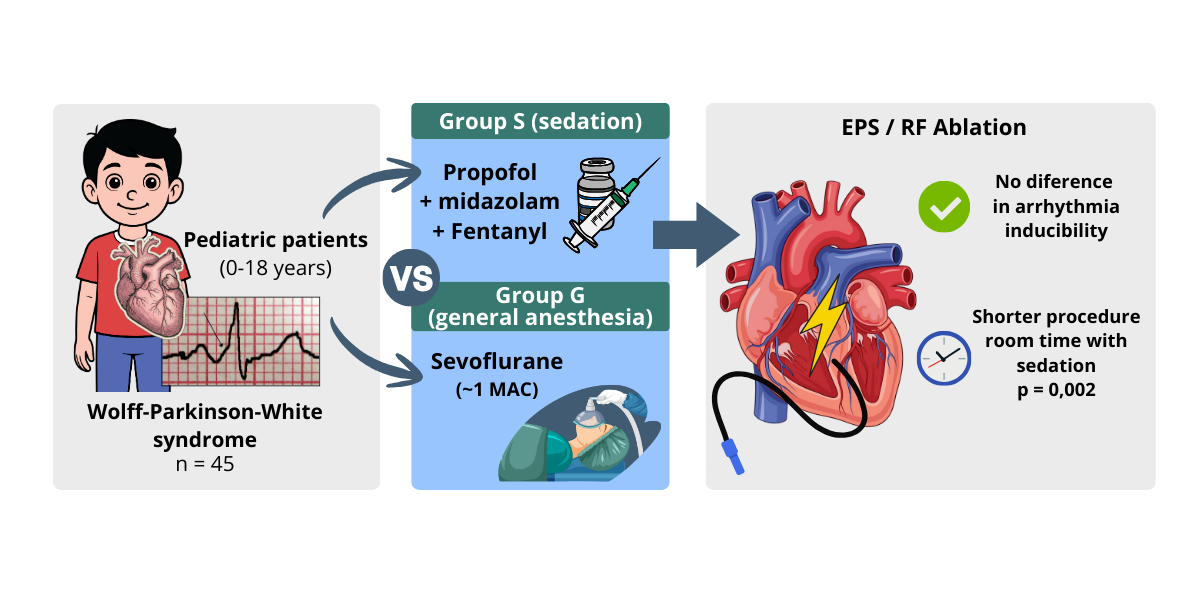
Introduction: Propofol is one of the most commonly used intravenous anesthetics worldwide and is considered safe for all age groups. However, there have been reports that propofol can induce severe atrioventricular block in humans, and several studies have shown that propofol hinders or prevents the inducibility of arrhythmias during electrophysiological studies (EPS) and radiofrequency (RF) ablation. Objectives: Verify whether propofol prevents or hinders the inducibility of arrhythmias during EPS and RF ablation procedures in children with Wolff-Parkinson-White Syndrome. Methods:We conducted a retrospective observational cohort study including 45 pediatric patients aged 0–18 years. Patients were identified through a review and analysis of a database of individuals with Wolff–Parkinson–White syndrome who were referred for electrophysiological study and/or radiofrequency ablation at the Electrophysiology Laboratory of the Institute of Cardiology (IC/FUC) in Porto Alegre over the past five years (2019-2024). Patients with prior ablation, structural heart disease, or ongoing antiarrhythmic therapy were excluded. The patients were divided into two groups and designated as group S (who received sedation) or group G (who received general anesthesia). Sedation (group S) was performed with midazolam (0.08–0.2 mg/kg), fentanyl (0.1–0.2 μcg/kg), and propofol 50–60 µg/kg/min in continuous infusion. General anesthesia (group G), in turn, was performed with sevoflurane at an average dose of 2% (1 MAC according to age). Results: From 4,874 invasive electrophysiology procedures performed during the study period, 45 involved pediatric patients with WPW. The sedation group (n=29) had significantly older patients (14.6±2.5 vs 10.3±2.8 years, p<0.001) with higher weight (65.9±16.3 vs 41.2±7.8 kg, p<0.001) compared to the general anesthesia group (n=16). Arrhythmia was successfully induced in 15/29 (51.7%) patients in the sedation group compared to 13/16 (81.2%) in the general anesthesia group (p=0.062, Fisher's exact test). Although this difference did not reach statistical significance, it represents a clinically relevant 29.5% lower induction rate in the sedation group. Post-hoc power analysis revealed the study was underpowered (49.8%), suggesting a possible Type II error. Analysis of the "procedure room time" revealed a longer duration in the general anesthesia group (97.8±36.7 vs 67.8±24.4 minutes), and this difference was statistically significant (p = 0.002). Conclusions: This study compared propofol-based sedation with sevoflurane-based general anesthesia in pediatric WPW patients. While sedation with propofol did not show a statistically significant reduction in arrhythmia inducibility, there was a concerning trend toward lower induction rates (29.5% difference) that may be clinically relevant. The study's limited statistical power (49.8%) suggests these findings should be interpreted cautiously, and larger prospective studies are needed to definitively establish whether propofol affects arrhythmia inducibility in this population. Propofol remains a viable option for these procedures, but clinicians should be aware of the potential for reduced inducibility, particularly in cases where arrhythmia induction is critical for diagnosis and treatment.
Keywords:
propofol
; pediatric anesthesia
; Wolff–Parkinson–White syndrome
; arrhythmia inducibility
; electrophysiological study
; radiofrequency ablation
1. Introduction
Accessory pathway (AP) ablation is one of the most frequently performed procedures in pediatric patients in the cardiac electrophysiology laboratory. In large-scale population studies involving children and adults, the prevalence of Wolff-Parkinson-White (WPW) Syndrome is estimated at 1 to 3 cases per 1,000 individuals (1).
Unlike adult patients, these procedures are performed under general anesthesia or deep sedation in most cases to ensure comfort and safety, owing to the limited patient cooperation(2). One of the most widely used and accepted anesthetic drugs for this purpose is propofol, an intravenous anesthetic agent broadly employed in general anesthesia or as a sedative in procedures for diagnostic and therapeutic examinations, such as electrophysiological studies (EPS) and radiofrequency (RF) ablation (3). This can be partly attributed to its favorable pharmacokinetic properties, among which we can mention the lack of cumulative effects and the ease of titration, which provides a rapid awakening without the residual sensation of hangover (4).
In patients under anesthetic effect, AP conduction usually increases due to the slower conduction properties of the atrioventricular node (AVN) during a parasympathetic phase. In some patients undergoing electrophysiological study, spontaneous disappearance of pre-excitation may be observed, characterized by loss of anterograde conduction through an accessory pathway during the introduction of sedation (1). In cases in which reentry is not inducible, mapping and ablation of the accessory pathway become significantly more difficult or may even be impossible.
Some case series have indicated a possibly negative side effect of propofol on AP conduction, suppressing it (4). Literature review studies mention rare proarrhythmic effects at clinically relevant concentrations of propofol (5). Moreover, reports of bradycardia and cessation of supraventricular tachycardia under the use of propofol are frequent in the literature (6) (7). In this regard, authors such as Wu et al. demonstrated that propofol appeared to interfere with arrhythmia inducibility, preventing treatment with ablation in some cases. These authors also observed that in pediatric patients with ectopic atrial tachycardia it was not possible to sustain the arrhythmia during EPS in four patients under the use of propofol, and they suggested a possible interference of this drug with the cardiac conduction system (CCS) in the group of patients with this arrhythmogenic substrate, concluding that this anesthetic agent should be used with caution in pediatric patients with ectopic atrial tachycardia undergoing EPS (8).
Similarly, Paech C et al., in a retrospective cohort study of patients with WPW, observed the occurrence of loss of pre-excitation in four patients after initiating sedation with propofol, demonstrating a possible suppression of the accessory pathway (1). In general, these authors reported that arrhythmia induction was not successful in all patients when propofol was included in the anesthetic plan, leading them to conclude that it may have negatively interfered with arrhythmia inducibility (1).
In this context, differing conclusions in the literature may be attributed, at least in part, to the use of different samples, concentrations, and experimental conditions (5). Thus, there is a need for additional studies to verify the possible interference of this drug with the inducibility of arrhythmias, which is of utmost importance for this group of patients, as it may determine whether or not this drug should be indicated in certain clinical situations.
Therefore, we proposed to investigate, through an observational study, whether propofol interfered with the inducibility of arrhythmias in a group of pediatric patients undergoing EPS and ablation of anomalous pathways at the Electrophysiology Laboratory of the Institute of Cardiology (IC/FUC) in Porto Alegre over the last 5 years.
2. Methods
2.1. Study Design and Patient Selection
This study was approved by the Research Ethics Committee of the Institute of Cardiology / University Foundation of Cardiology (IC/FUC) under protocol number: 1.696.303. As a retrospective observational study using de-identified data from an existing institutional database, the requirement for individual informed consent was waived by the ethics committee in accordance with Brazilian national regulations (Resolution CNS 466/2012) and the Declaration of Helsinki. All procedures were performed as part of standard clinical care.
This was a retrospective observational cohort study conducted at the Electrophysiology Laboratory of the Institute of Cardiology (IC/FUC) in Porto Alegre, Brazil. During the 5-year study period (2019-2024), 4,874 invasive electrophysiology procedures were performed at our institution. Of these, 52 procedures involved pediatric patients (aged 0-18 years) with Wolff-Parkinson-White syndrome. After excluding 7 patients due to missing anesthesia documentation or incomplete procedural data, 45 patients were included in the final analysis.
Inclusion criteria were: (1) age 0-18 years, (2) confirmed diagnosis of WPW syndrome, (3) undergoing EPS and/or RF ablation, and (4) complete anesthesia and procedural documentation.
Exclusion criteria were: (1) prior ablation procedures, (2) structural heart disease (except for simple congenital defects such as small atrial or ventricular septal defects that did not require intervention), (3) ongoing antiarrhythmic therapy at the time of the procedure, and (4) incomplete or missing data regarding anesthesia type or procedural outcomes.
2.2. Anesthetic Protocols
Patients were divided into two groups based on the anesthetic technique used: Group S (Sedation, n=29) and Group G (General Anesthesia, n=16). The choice of anesthetic technique was determined by the attending anesthesiologist based on patient age, cooperation ability, and clinical characteristics.
2.3. Sedation Protocol (Group S)
Patients received midazolam (0.08–0.2 mg/kg), fentanyl (0.1–0.2 μg/kg), and propofol administered by target-controlled infusion pump at 50–60 μg/kg/min, aiming at a target plasma concentration of 1–2 µg/mL or adjusted at clinical discretion to maintain adequate sedation and immobilization during the procedure. Spontaneous ventilation was maintained throughout the procedure with supplemental oxygen via nasal cannula or face mask. Sedation depth was monitored clinically by assessing patient response to verbal commands and procedural stimuli.
2.4. General Anesthesia Protocol (Group G)
Anesthesia was induced with propofol (1–2 mg/kg) and fentanyl (2 µg/kg). Rocuronium was administered as a neuromuscular blocker to facilitate endotracheal intubation. Maintenance of anesthesia was achieved with sevoflurane at an average dose of 2% (approximately 1 minimum alveolar concentration [MAC], adjusted for age). Mechanical ventilation was provided via endotracheal tube with parameters adjusted to maintain normocapnia. End-tidal sevoflurane concentration was continuously monitored.
2.5. Electrophysiological Study and Ablation Procedure
All EPS procedures were performed following standardized institutional protocols. Vascular access was obtained via the femoral veins using the Seldinger technique. Diagnostic catheters were positioned in the high right atrium, His bundle region, right ventricular apex, and coronary sinus.
Standard electrophysiological parameters were assessed, including baseline intervals (AH, HV, and accessory pathway conduction times when applicable), effective refractory periods, and arrhythmia inducibility. Programmed electrical stimulation was performed using standard protocols with burst pacing and programmed extrastimuli (up to three extrastimuli) from the atrium and ventricle.
Arrhythmia induction was defined as sustained (>30 seconds) or requiring termination due to hemodynamic compromise. The primary arrhythmia mechanisms recorded were atrioventricular reentrant tachycardia (AVRT) utilizing the accessory pathway and atrial fibrillation (AF). Cases where arrhythmia could not be induced despite standard stimulation protocols were classified as “not induced.”
Radiofrequency ablation was performed using a 4-mm tip ablation catheter with temperature-controlled energy delivery (target temperature 50-60 °C, power 25-35 W). Ablation success was defined as elimination of accessory pathway conduction (both anterograde and retrograde) with no inducible arrhythmia after a 30-minute waiting period and repeat stimulation.
In cases where arrhythmia induction was initially unsuccessful, isoproterenol (0.01-0.05 μg/kg/min) was administered to facilitate induction by enhancing accessory pathway conduction and increasing heart rate, as per standard institutional protocol.
3. Statistical Analysis
The data were entered into Microsoft Excel and subsequently exported to SPSS v. 20.0 (IBM Corp., Armonk, NY, USA) for statistical analysis. Categorical variables were described by frequencies and percentages and compared using the Chi-square test or Fisher’s exact test when expected cell counts were less than 5. Yates’ correction was applied in 2×2 tables where appropriate.
The normality of quantitative variables was assessed using the Kolmogorov–Smirnov test. When normality was confirmed, variables were expressed as mean ± standard deviation and compared between groups using Student’s t-test for independent samples. For non-normally distributed variables, the Mann-Whitney U test was used. A significance level of 5% (α = 0.05) was considered for all comparisons.
Post-hoc power analysis was performed to determine the statistical power of the study for detecting differences in arrhythmia induction rates between groups. Power was calculated using the observed effect size (difference in proportions), sample sizes, and alpha level of 0.05 (two-tailed). The power analysis was conducted using G*Power software version 3.1.9.7.
4. Results
The study included 45 pediatric patients from a total of 4,874 invasive electrophysiology procedures performed over the 5-year study period. The characteristics of the patients are shown in Table 1. The study cohort was predominantly male (27/45, 60.0%). Most patients were classified as ASA II (29/45, 64.4%).
Significant statistical differences were found in the comparison of anthropometric data between the two groups. The sedation group consisted of significantly older patients (14.6 ± 2.5 years) compared to the general anesthesia group (10.3 ± 2.8 years, p < 0.001). Similarly, patients in the sedation group had significantly higher weight (65.9 ± 16.3 kg vs 41.2 ± 7.8 kg, p < 0.001) and height (165.5 ± 11.9 cm vs 145.7 ± 12.9 cm, p < 0.001). These differences reflect the expected clinical practice pattern, where general anesthesia is preferentially indicated for younger pediatric patients with lower weight and height due to their limited ability to cooperate during the procedure.
Sex distribution did not differ significantly between groups (p = 0.949). ASA classification was similar between groups, with most patients classified as ASA II in both the sedation (62.1%) and general anesthesia (68.8%) groups.
Procedural Outcomes
The primary outcome of arrhythmia inducibility is presented in Table 2 and Figure 2. Arrhythmia was successfully induced in 15 out of 29 patients (51.7%) in the sedation group, compared to 13 out of 16 patients (81.2%) in the general anesthesia group. This difference approached but did not reach statistical significance (p = 0.062, Fisher’s exact test).
The types of induced arrhythmias differed between groups. In the sedation group, atrioventricular reentrant tachycardia (AVRT) was induced in 12 patients (41.4%), atrial fibrillation in 3 patients (10.3%), and arrhythmia could not be induced in 14 patients (48.3%). In the general anesthesia group, AVRT was induced in 11 patients (68.8%), atrial fibrillation in 2 patients (12.5%), and arrhythmia could not be induced in only 3 patients (18.8%).
Post-hoc power analysis revealed that with the observed effect size (29.5% difference in induction rates) and sample sizes (n=29 and n=16), the statistical power of this study was 49.8%. This indicates that the study was underpowered to detect a statistically significant difference, raising the possibility of a Type II error (false negative result).
Analysis of the secondary outcome, “procedure room time,” revealed a statistically significant difference between groups (Figure 1). The mean procedure time was significantly longer in the general anesthesia group (97.8 ± 36.7 minutes) compared to the sedation group (67.8 ± 24.4 minutes, p = 0.002).
The total propofol dose administered was similar between groups: sedation group received 134.1 ± 91.9 mg (for continuous sedation throughout the procedure) and general anesthesia group received 128.1 ± 100.7 mg (for induction only). In the general anesthesia group, sevoflurane consumption averaged 20.1 ± 10.4 mL.
We did not find a statistically significant difference in the outcome of arrhythmia induction, as shown in Table 2. However, when we analyzed the parameter “procedure room time,” it was greater in group “G” compared to group “S,” and this difference was statistically significant (p = 0.002). This can be seen in Table 2 and is represented in Figure 1
Figure 1.
Procedure room time according to anesthetic technique (sedation vs. general anesthesia) in pediatric patients with Wolff–Parkinson–White syndrome. A statistically significant difference was observed between groups (p = 0.002).
Figure 1.
Procedure room time according to anesthetic technique (sedation vs. general anesthesia) in pediatric patients with Wolff–Parkinson–White syndrome. A statistically significant difference was observed between groups (p = 0.002).

Figure 2.
compares arrhythmia induction success rates between sedation (n = 29) and general anesthesia (n = 16). Arrhythmia induction was achieved more frequently under general anesthesia (81.2%, n = 13) compared with sedation (51.7%, n = 15), while failure to induce arrhythmia was more common with sedation (48.3%, n = 14) than with general anesthesia (18.8%, n = 3). The difference showed a trend toward statistical significance (Fisher’s exact test, p = 0.0623).
Figure 2.
compares arrhythmia induction success rates between sedation (n = 29) and general anesthesia (n = 16). Arrhythmia induction was achieved more frequently under general anesthesia (81.2%, n = 13) compared with sedation (51.7%, n = 15), while failure to induce arrhythmia was more common with sedation (48.3%, n = 14) than with general anesthesia (18.8%, n = 3). The difference showed a trend toward statistical significance (Fisher’s exact test, p = 0.0623).

Figure 3.
Violin plots showing the age distribution of pediatric WPW patients according to anesthetic technique. Patients under sedation were older (mean 14.6 years) than those under general anesthesia (mean 10.2 years), with a statistically significant difference between groups (p < 0.001).
Figure 3.
Violin plots showing the age distribution of pediatric WPW patients according to anesthetic technique. Patients under sedation were older (mean 14.6 years) than those under general anesthesia (mean 10.2 years), with a statistically significant difference between groups (p < 0.001).

Figure 4.
CONSORT-style flow diagram illustrating patient selection and group allocation. From 4,874 EPS procedures, 45 pediatric WPW patients were included and divided into sedation (n = 29) and general anesthesia (n = 16) groups, with key anesthetic regimens, procedural outcomes, and statistical comparisons summarized.
Figure 4.
CONSORT-style flow diagram illustrating patient selection and group allocation. From 4,874 EPS procedures, 45 pediatric WPW patients were included and divided into sedation (n = 29) and general anesthesia (n = 16) groups, with key anesthetic regimens, procedural outcomes, and statistical comparisons summarized.

5. Discussion
Accessory pathway ablation is one of the most frequent procedures in pediatric electrophysiology, especially in patients with Wolff–Parkinson–White syndrome. Most of these procedures are performed with sedation or general anesthesia in children, due to limited patient cooperation and the need for adequate immobility during the electrophysiological study (9). However, the possibility of drug-induced arrhythmia suppression remains a relevant concern, as it may compromise both the performance of the EPS and the success of the ablation.
5.1. Primary Findings: Arrhythmia Inducibility
The central finding of our study is the observed trend toward lower arrhythmia inducibility in the sedation group (51.7%) compared to the general anesthesia group (81.2%), representing a 29.5% difference. Although this difference did not achieve statistical significance (p = 0.062), it approaches the conventional threshold and warrants careful consideration.
Critically, our post-hoc power analysis revealed that the study had only 49.8% statistical power to detect this observed difference. This low power substantially increases the risk of a Type II error—that is, failing to detect a true difference when one exists. Therefore, the lack of statistical significance should not be interpreted as definitive evidence of no effect. Rather, it suggests that a larger sample size would be necessary to conclusively determine whether propofol-based sedation genuinely reduces arrhythmia inducibility in this population.
From a clinical perspective, a 30% reduction in inducibility could have meaningful implications for procedural success. Inability to induce arrhythmia during EPS significantly complicates mapping and ablation, potentially leading to incomplete procedures, need for repeat interventions, or alternative management strategies. While our data cannot definitively establish causation, they raise important considerations for anesthesia selection in pediatric WPW ablation procedures.
5.2. Comparison with Existing Literature
Our findings align with several previous reports suggesting potential interference of propofol with arrhythmia inducibility, while also acknowledging contradictory evidence in the literature. Some authors suggest that propofol may influence parameters of the cardiac conduction system. Matsushima et al. studied the effect of propofol in pediatric patients during RF ablation and found that this drug significantly prolonged the HV interval but did not interfere with the Atrium–His interval or other intervals measured in the study; however, they observed that propofol directly suppresses parasympathetic activity as well as sympathetic activity, concluding that this result may help elucidate the mechanism by which lethal AV blocks are induced by propofol (10).
Similarly, Paech C et al., in their retrospective cohort study of patients with WPW, observed the occurrence of loss of pre-excitation in 4 patients after initiating sedation with propofol, demonstrating a possible suppression of the accessory pathway. These authors reported that they were not able to induce arrhythmia in all patients when propofol was used in the anesthetic regimen, concluding that propofol may have interfered negatively with the inducibility of the arrhythmias (1).
On the other hand, other studies attempted to demonstrate some effect of propofol on the CCS without success, such as that of Warpechowski et al., who evaluated the effects of propofol on the AV conduction system of patients with nodal reentrant tachycardia by analyzing the effective refractory periods of the slow pathway and the fast pathway of the AVN during EPS.The authors concluded that propofol did not cause significant alterations in the electrophysiological variables of the atrioventricular node (11). These findings were similar to those reported by Sharpe et al., who studied patients with Wolff–Parkinson–White syndrome; in both studies, the arrhythmia mechanism was reentry (12).Based on these studies and our findings, it appears that propofol’s effects may be substrate-dependent or dose-dependent, potentially explaining the conflicting results in the literature.
Perez et al. evaluated the electrophysiological effects in children with WPW undergoing RF ablation and found that the administration of sevoflurane produced a widening of the effective refractory period of the accessory pathway (APERP) (propofol-ERP 283 ± 22 ms; sevoflurane-ERP 298 ± 25 ms; p = 0.004), but it did not prevent its ablation, and no other significant change was found during the procedure (4).
Furthermore, the results we found are also aligned with the study by Hino et al. (2018), which demonstrated that propofol preserves the inducibility of supraventricular tachycardia in children with WPW, whereas desflurane, at concentrations of 0.5 MAC and 1.0 MAC, reduced this capability. In the study, the arrhythmia was induced in all children under propofol, but could not be induced in 1 child with 0.5 MAC and in 4 children with 1.0 MAC of desflurane. However, it is important to note that in the Hino study, propofol was used in isolation for sedation, whereas in our general anesthesia group, propofol was only used for induction followed by sevoflurane maintenance. This methodological difference may partly explain the divergent findings and highlights the challenge of attributing effects to specific agents in multi-drug anesthesia protocols.(13).
More recent data further support the potential neutrality of propofol with respect to arrhythmia inducibility. In a study by Zhang et al. (2025), which compared propofol with next-generation sedatives such as ciprofol and remimazolam in children undergoing electrophysiological study for supraventricular tachyarrhythmias, no significant differences were observed in arrhythmia induction rates among the three agents. These findings reinforce that, when compared with modern sedative agents, propofol maintains similar performance in preserving inducibility, though our study suggests this may not be the case when compared to volatile anesthetic-based general anesthesia.(14).
5.3. Procedural Time Differences
Regarding procedure duration, we observed significantly longer procedure times in the general anesthesia group (97.8 ± 36.7 minutes) compared to the sedation group (67.8 ± 24.4 minutes, p = 0.002). This 30-minute difference likely reflects multiple factors: (1) the time required for endotracheal intubation and airway management in the general anesthesia group, (2) the higher arrhythmia induction rate in the general anesthesia group potentially allowing more complete mapping and ablation procedures, and (3) possible differences in procedural complexity between the younger patients requiring general anesthesia and older patients managed with sedation.
Interestingly, the longer procedure time in the general anesthesia group occurred despite—or perhaps because of—the higher induction success rate. This paradoxical finding suggests that successful arrhythmia induction may lead to more comprehensive electrophysiological assessment and ablation, ultimately requiring more time but potentially resulting in more complete treatment.
5.4. Role of Isoproterenol
In this context, it is also important to note that, in situations of difficulty in inducing the arrhythmia during the electrophysiological study, especially in pediatric patients with WPW under general anesthesia, pharmacological strategies may assist in restoring conduction through the accessory pathway. In this context, the findings of Moore et al. (2011) are notably relevant: in a pediatric cohort, the authors demonstrated that the administration of isoproterenol significantly increased anterograde and retrograde conduction through the accessory pathways, facilitating the induction of reentrant tachyarrhythmias under general anesthesia. Thus, the use of isoproterenol emerges as a possible alternative to overcome induction difficulties potentially related to propofol sedation, allowing mapping and ablation to be completed safely and accurately. Future studies should systematically document the use of isoproterenol and other provocative agents to better understand their role in overcoming anesthesia-related suppression of arrhythmia inducibility.(15).
5.5. Methodological Considerations and Confounding Factors
A critical limitation of our study design is that propofol was not used in isolation in either group. In the sedation group, propofol was administered together with midazolam and fentanyl, while in the general anesthesia group it was combined with fentanyl, neuromuscular blockade, and sevoflurane. Consequently, any observed effects cannot be attributed solely to propofol. This polypharmacy approach, while reflecting real-world clinical practice, limits our ability to definitively isolate propofol’s specific contribution to the observed differences in arrhythmia inducibility.
Furthermore, the depth of sedation or anesthesia was not quantified using validated scales or monitoring tools such as Bispectral Index (BIS), Ramsay Sedation Scale, or Richmond Agitation-Sedation Scale (RASS). Given that autonomic tone and depth of anesthesia may influence accessory pathway conduction and arrhythmia inducibility, this represents an important methodological limitation that should be addressed in future prospective studies.
Additionally, we did not systematically document whether patients were receiving antiarrhythmic medications prior to the procedure, nor whether such medications were discontinued and for how long before the EPS. Antiarrhythmic drugs can significantly affect arrhythmia inducibility and should be carefully controlled in future studies.
An important mechanistic consideration is the role of autonomic tone in WPW arrhythmia inducibility. Young patients with WPW often exhibit heightened sympathetic activity and catecholamine prevalence, which can facilitate accessory pathway conduction and arrhythmia induction. Both sedation and general anesthesia suppress autonomic nervous system activity, though potentially through different mechanisms and to different degrees. Propofol has been shown to suppress both sympathetic and parasympathetic activity (10), while volatile anesthetics like sevoflurane have distinct autonomic effects. Therefore, any observed differences in arrhythmia inducibility between our groups may reflect differential autonomic suppression rather than direct electrophysiological effects on the cardiac conduction system. This autonomic confounding makes it impossible to isolate propofol’s direct cardiac effects in our study design.
5.6. Study Limitations
Several important limitations of our study must be acknowledged:
1. Small Sample Size and Statistical Power: The most significant limitation is the small number of patients (n=45), resulting in inadequate statistical power (49.8%) to detect the observed 29.5% difference in induction rates. This substantially increases the risk of Type II error and limits the generalizability of our findings.
2. Retrospective Design: As a retrospective observational study, our analysis is subject to selection bias and unmeasured confounding. The choice of anesthesia technique was not randomized but rather determined by clinical factors, particularly patient age and cooperation ability.
3. Lack of Detailed Electrophysiological Parameters: We did not evaluate specific intervals of the cardiac conduction system, such as the AH interval, HV interval, accessory pathway effective refractory periods, or other electrophysiological parameters that might provide mechanistic insights into propofol’s effects.
4. Absence of Drug Level Monitoring: Serum concentrations of propofol were not measured in the patients, limiting our ability to establish dose-response relationships.
5. Age Disparity Between Groups: The significant age difference between groups (14.6 vs 10.3 years) introduces potential confounding. Younger patients may have different electrophysiological properties, accessory pathway characteristics, or arrhythmia substrates compared to older children, independent of anesthesia type.
6. Wide Age Range: Our study included patients from 0 to 18 years, encompassing infants, children, and adolescents. The electrophysiological characteristics and responses to anesthetic agents may differ substantially across this developmental spectrum, and pooling such a heterogeneous age range may obscure age-specific effects.
7. Multi-Drug Protocols: Both anesthetic protocols involved multiple agents, making it impossible to attribute observed effects specifically to propofol versus other medications in the regimen.
8. Lack of Standardized Induction Protocols: Electrophysiological stimulation protocols, use of isoproterenol, and other procedural details were not standardized or systematically documented, introducing potential variability in arrhythmia induction attempts.
9. Autonomic Tone Confounding: We did not measure autonomic nervous system activity (e.g., heart rate variability, catecholamine levels) or control for baseline sympathetic tone. Given that both anesthetic techniques suppress autonomic activity—potentially the primary driver of WPW inducibility in young patients—we cannot distinguish between direct cardiac effects and indirect autonomic effects.
6. Clinical Implications
It is important to acknowledge the ethical constraints that limit our ability to definitively answer questions about anesthetic effects in pediatric electrophysiology. Performing EPS and ablation procedures in children without adequate sedation or anesthesia would be unethical, causing unnecessary suffering and compromising procedural safety through patient movement. This ethical imperative means that truly isolating the effects of any single anesthetic agent in this population is extraordinarily challenging. The ideal control group—awake, unsedated patients—is not ethically feasible in pediatric practice. Therefore, all studies in this field, including ours, must compare different anesthetic techniques rather than anesthetic versus no anesthetic. Given these ethical constraints, our study provides clinically relevant information about two commonly used anesthetic approaches in real-world practice. While we cannot definitively isolate propofol’s effects, we can inform clinicians about the relative performance of these two standard techniques.
Despite these limitations, our findings have several practical implications for clinical practice:
1. Propofol-based sedation remains a viable and commonly used option for pediatric EPS and ablation procedures, with no definitive evidence of harm or absolute contraindication.
2. Clinicians should be aware of the potential for reduced arrhythmia inducibility when using propofol-based sedation, particularly in cases where arrhythmia induction is critical for diagnosis and treatment planning.
3. In cases of initial difficulty with arrhythmia induction under propofol sedation, consideration should be given to pharmacological provocation with isoproterenol or, if clinically appropriate, adjusting the anesthetic depth or switching to alternative anesthetic techniques.
4. The significantly shorter procedure times associated with sedation (30 minutes less on average) may offer practical advantages in terms of laboratory efficiency and patient throughput, though this must be weighed against the potential for reduced inducibility.
7. Conclusions
This retrospective observational study compared propofol-based sedation with sevoflurane-based general anesthesia in 45 pediatric patients undergoing electrophysiological study and radiofrequency ablation for Wolff-Parkinson-White syndrome. While we did not identify a statistically significant difference in arrhythmia inducibility between the two anesthetic techniques (p = 0.062), a clinically relevant trend toward lower induction rates in the sedation group (51.7% vs 81.2%, representing a 29.5% difference) warrants consideration. Critically, our post-hoc power analysis revealed inadequate statistical power (49.8%), suggesting that the lack of statistical significance may reflect insufficient sample size rather than true equivalence between techniques.
The use of propofol for sedation was associated with significantly shorter procedure times (67.8 vs 97.8 minutes, p = 0.002), offering potential practical advantages. However, this benefit must be weighed against the possible reduction in arrhythmia inducibility, particularly in cases where successful induction is critical for procedural success.
Given the study’s limitations—including small sample size, retrospective design, significant age disparity between groups, use of multi-drug anesthetic protocols, and lack of detailed electrophysiological measurements—our findings should be interpreted cautiously. These results do not provide definitive evidence that propofol reduces arrhythmia inducibility, but they raise important questions that warrant further investigation.
Future prospective studies with larger sample sizes, age-matched cohorts, standardized anesthetic protocols, detailed electrophysiological parameter assessment, and systematic documentation of provocative agent use are essential to definitively establish whether propofol affects arrhythmia inducibility in pediatric WPW patients. Until such evidence is available, propofol remains a reasonable and widely used option for these procedures, with clinicians advised to maintain awareness of potential effects on inducibility and to utilize pharmacological provocation strategies when needed.
Author Contributions
Conceptualization, P.W.; Methodology, P.W. and T.L.L.; Formal Analysis, B.E.; Investigation, P.W., A.T.S., T.L.L. and G.G.L.; Data Curation, P.W., G.G.L.; Writing—Original Draft Preparation, P.W. and T.B.W.; Writing—Review & Editing, P.W., T.B.W. and B.E.; Supervision, A.T.S., T.B.W. and T.L.L.; Project Administration, P.W.; Funding Acquisition, none.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Research Ethics Committee of the Institute of Cardiology / University Foundation of Cardiology (IC/FUC), Porto Alegre, Brazil, under protocol number 1.696.303. All procedures were conducted in accordance with Brazilian national regulations (Resolution CNS 466/2012) and the Declaration of Helsinki.
Informed Consent Statement
As this was a retrospective observational study using de-identified data from an existing institutional database, the requirement for individual informed consent was waived by the Research Ethics Committee in accordance with Brazilian national regulations (Resolution CNS 466/2012). All clinical procedures included in the analysis had been performed as part of standard care.
Data Availability Statement
The data presented in this study are available in [Instituto de Cardiologia—Fundação Universitária de Cardiologia (IC-FUC)]at [https://cardiologia.org.br], reference number [reference number]. These data were derived from the following resources available in the public domain: [list resources and URLs
Conflicts of Interest
The authors declare no conflict of interest.
References
- Paech C, Wagner F, Strehlow V, Gebauer RA. Drug-induced loss of preexcitation in pediatric patients with WPW pattern during electrophysiologic study. Pediatr Cardiol. 2019;40(1):194–197. [CrossRef]
- Monaco F, D’Andria Ursoleo J, Lerose CC, Barucco G, Licheri M, Della Bella PE, et al. Anaesthetic management of paediatric patients undergoing electrophysiology study and ablation for supraventricular tachycardia: a focused narrative review. J Clin Anesth. 2024;93:111361. [CrossRef]
- Staikou C, Stamelos M, Stavroulakis E. Perioperative management of patients with pre-excitation syndromes. Rom J Anaesth Intensive Care. 2018;25(2):131–147. [CrossRef]
- Rodríguez Pérez E, Benito Bartolomé F, Sanabria Carretero P, Sánchez Fernández C, Jiménez Mateos E, Goldman Tarlovsky L. Electrophysiological effects of sevoflurane versus propofol in children with Wolff–Parkinson–White syndrome. Rev Esp Anestesiol Reanim. 2008;55(1):26–31. [CrossRef]
- Liu Q, Lai Y, Chen Q, Chi H, Wu S, Chen J, et al. Propofol and arrhythmias: two sides of the coin. Int J Clin Exp Med. 2011;4(3):180–185.
- Thomson SJ, Yate PM. Bradycardia after propofol infusion. Anaesthesia. 1987;42(4):430. [CrossRef]
- Terashima S, Muroya T, Ikegawa H, Kajino K, Sakuramoto K, Yui R, et al. Propofol suppresses ventricular arrhythmias: a case report of acute caffeine intoxication. Acute Med Surg. 2020;7(1):e514. [CrossRef]
- Wu MH, Lin JL, Lai LP, Young ML, Lu CW, Chang YC, et al. Radiofrequency catheter ablation of tachycardia in children with and without congenital heart disease: indications and limitations. Int J Cardiol. 2000;72(3):221–227. [CrossRef]
- Pappone C, Vicedomini G, Manguso F, Saviano M, Baldi M, Pappone A, et al. Radiofrequency ablation in children with asymptomatic Wolff–Parkinson–White syndrome. N Engl J Med. 2004;351(12):1197–1205. [CrossRef]
- Matsushima M, Kimura S, Kitaura A, Hamasaki S, Iwamoto T, Mino T, et al. Propofol suppresses His–ventricular conduction in paediatric patients. J Clin Pharm Ther. 2021;46(2):433–439. [CrossRef]
- Warpechowski P, Lima GG, Medeiros CM, Santos ATL, Kruse M, Migloransa MH, et al. Randomized study of the effects of propofol on the electrophysiological properties of the atrioventricular node in patients with atrioventricular nodal reentrant tachycardia. Pacing Clin Electrophysiol. 2006;29(12):1375–1382.
- Sharpe MD, Dobrkowski WB, Murkin JM. Propofol has no direct effect on sinoatrial node function or on normal atrioventricular and accessory pathway conduction in Wolff–Parkinson–White syndrome during alfentanil/midazolam anesthesia. Anesthesiology. 1995;82:888–895.
- Hino H, Nonaka A, Okubo N, Yanagi S, Hagiwara Y, Tsukada T, et al. Effects of desflurane and propofol on accessory pathway conduction and arrhythmia inducibility in children with Wolff–Parkinson–White syndrome. Acta Anaesthesiol Scand. 2018;62(10):1454–1461. [CrossRef]
- Zhang X, Yu L, Chen Y, Li J, Wang Z, Liu H, et al. Comparison of ciprofol, remimazolam, and propofol on arrhythmia inducibility in pediatric patients undergoing electrophysiological study for supraventricular tachycardia. Drug Des Devel Ther. 2025;19:41–50. [CrossRef]
- Moore JP, Kannankeril PJ, Fish FA. Isoproterenol administration during general anesthesia for the evaluation of children with ventricular preexcitation. Circ Arrhythm Electrophysiol. 2011;4(1):73–78. [CrossRef]

Table 1.
Baseline Characteristics of Pediatric Patients with WPW SyndromE.
| Variable | Sedation Group (n=29) | General Anesthesia Group (n=16) | p-value |
| Age (years) | 14.6 ± 2.5 | 10.3 ± 2.8 | <0.001*** |
| Weight (kg) | 65.9 ± 16.3 | 41.2 ± 7.8 | <0.001*** |
| Height (cm) | 165.5 ± 11.9 | 145.7 ± 12.9 | <0.001*** |
| Male sex, n (%) | 18 (62.1%) | 9 (56.2%) | 0.949 |
| ASA I, n (%) | 4 (13.8%) | 2 (12.5%) | |
| ASA II, n (%) | 18 (62.1%) | 11 (68.8%) | 0.874 |
| ASA III, n (%) | 7 (24.1%) | 3 (18.8%) |
Data presented as mean ± standard deviation or n (%). ***p < 0.001. ASA = American Society of Anesthesiologists physical status classification.
Table 2.
Procedural Outcomes and Arrhythmia Inducibility.
| Variable | Sedation Group (n=29) | General Anesthesia Group (n=16) | p-value |
| Arrhythmia induced, n (%) | 15 (51.7%) | 13 (81.2%) | 0.062 |
| AVRT, n (%) | 12 (41.4%) | 11 (68.8%) | |
| Atrial fibrillation, n (%) | 3 (10.3%) | 2 (12.5%) | |
| Not induced, n (%) | 14 (48.3%) | 3 (18.8%) | |
| Procedure time (min) | 67.8 ± 24.4 | 97.8 ± 36.7 | 0.002** |
| Propofol dose (mg)-*+ | 134.1 ± 91.9 | 128.1 ± 100.7 | 0.847 |
Data presented as mean ± standard deviation or n (%). **p < 0.01. AVRT = Atrioventricular reentrant tachycardia. Fisher’s exact test was used for arrhythmia induction comparison; Student’s t-test for continuous variables.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



