Submitted:
10 March 2026
Posted:
11 March 2026
You are already at the latest version
Abstract
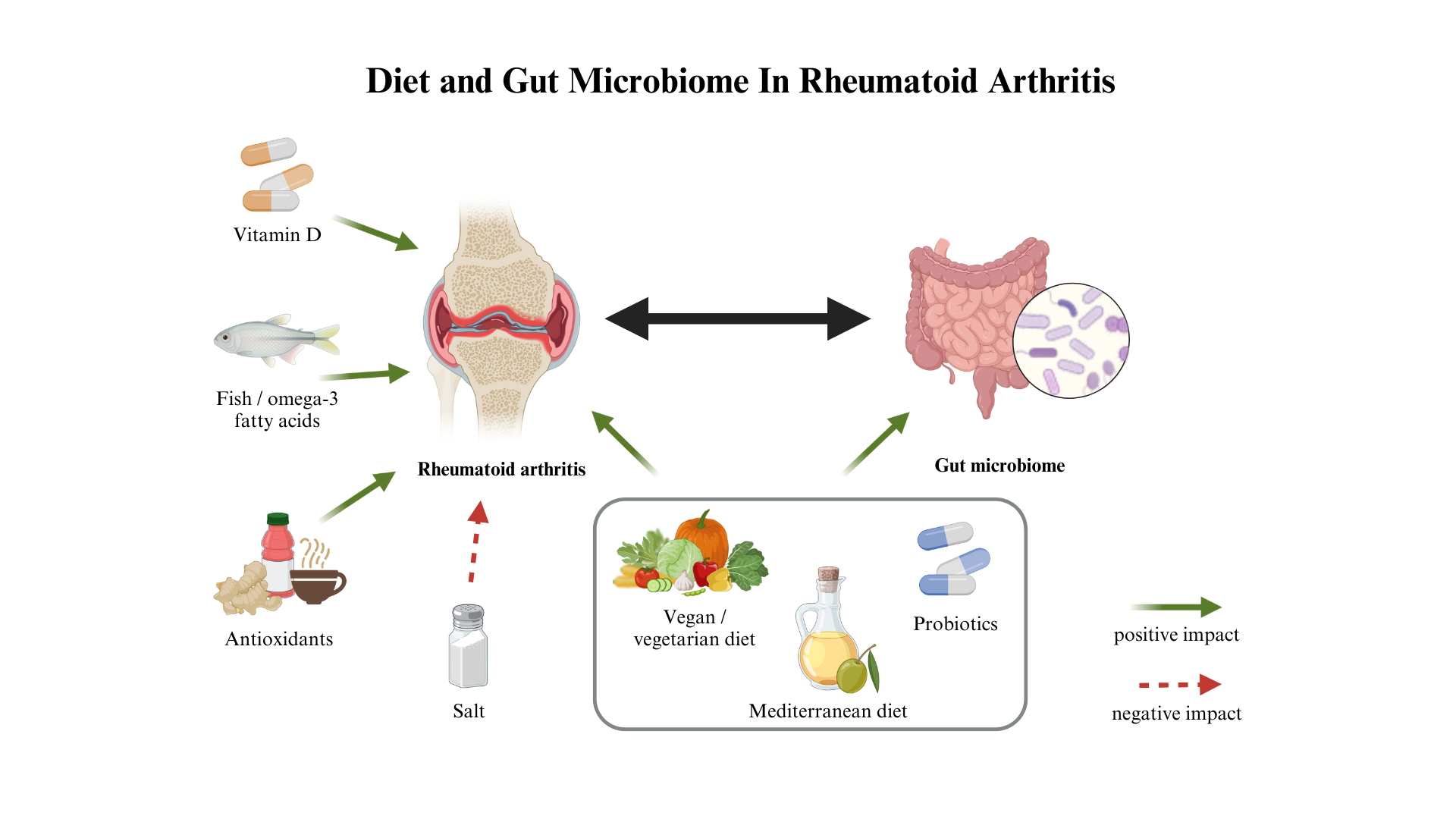
Rheumatoid arthritis (RA) is a chronic inflammatory disease of autoimmune background and unknown etiology. The importance of genetic factors in the RA development is well established. Environmental factors have also been extensively researched in relation to risk of RA and managing its symptoms. Smoking, physical activity, diet and gut microbiota are considered to be the most essential modifiable factors in RA. Among dietary interventions the most researched is Mediterranean diet, monounsaturated fatty acids, fish consumption and fish oil (EPA, eicosapentaenoic acid and DHA, docosahexaenoic acid). Others concerned gluten-free and vegan or vegetarian diet, salt intake, supplementation with vitamin D, antioxidants, prebiotics and probiotics. Diet modifications can alter the gut environment and the association between RA development or severity and composition of gut bacteria has already been shown. This review focuses on effectiveness and usefulness of various dietary approaches and supplements in RA prevention and management, including influence on disease activity and inflammatory status. Composition of gut microbiota and its changes in response to dietary factors are also considered. There is a great need for further research into mutual dependencies of diet, microbiome and RA activity. The current state of knowledge provides promising evidence for future nutrition and microbial therapies.
Keywords:
rheumatoid arthritis
; diet
; microbiome
; vitamin D
; Mediterranean diet
; EPA
; DHA
1. Introduction
Rheumatoid arthritis is a chronic inflammatory disease of unknown etiology. It is characterized by autoantibodies, synovial inflammation and associated joint destruction. The prevalence of disease is 0,5-1% in developed countries and it affects women more often than men (ratio 3:1) [1].
The genetic background of RA is well-investigated [2]. However, environmental factors play essential role in the disease development. Smoking is the most significant factor contributing to disease occurrence, worse prognosis and response to therapy. Symptoms occurring in the course of the disease significantly reduce quality of life.
Patients suffer from pain, fatigue, sleep disturbances and severe physical limitations. As a result their physical activity is predominantly insufficient which affects cardiovascular health [3]. RA is also associated with high risk of comorbidities such as hypertension, stroke, gastrointestinal disease, osteoporosis. Patients’ sedentary lifestyle often leads to obesity which is associated with poorer therapy effects and a higher prevalence of additional disorders [4]. Presumably systemic inflammation in obesity causes more severe RA and worse disease outcome.
Apart from reducing body mass and BMI other dietetic interventions and supplementation can help alleviate symptoms of RA. The most researched is Mediterranean diet and its’ elements such as monounsaturated fatty acids and fish oil (EPA, eicosapentaenoic acid and DHA, docosahexaenoic acid). Other tested interventions concerned gluten-free and vegan or vegetarian diet, salt intake, supplementation with vitamin D, antioxidants, prebiotics and probiotics.
There is also growing evidence that alterations in gut microbiome composition are closely linked to the development, activity and progression of rheumatoid arthritis. Multiple studies have demonstrated associations between specific bacterial taxa, reduced microbial diversity and markers of systemic inflammation, autoantibody production and joint damage. Since dietary patterns are among the strongest modulators of gut microbial composition and metabolic activity, nutritional interventions may directly influence disease-relevant immunological pathways through microbiome-mediated mechanisms. Therefore, the interaction between diet and gut microbiota is not merely associative but may play a meaningful role in modulating RA pathogenesis and clinical course.
2. Dietary Regimens and Supplements in Prophylaxis and Treatment of Rheumatoid Arthritis
Chronic inflammation in rheumatoid arthritis is sustained by dysregulation of immune pathways including NF-κB activation, the IL-23/IL-17 axis and NLRP3 inflammasome signaling, accompanied by increased oxidative stress and excessive production of reactive oxygen species (ROS). As emphasized in a recent comprehensive review by Kupczyk et al., redox imbalance not only amplifies cytokine production (TNF-α, IL-6, IL-1β) but also perpetuates synovial inflammation and tissue damage [5].
Diet has emerged as a modifiable factor capable of influencing these interconnected inflammatory and oxidative pathways. According to current evidence, nutritional patterns rich in omega-3 fatty acids, fiber, polyphenols and antioxidant vitamins may attenuate NF-κB activation, modulate Th17/Treg balance, and reduce oxidative stress markers. Importantly, many of these effects appear to be mediated indirectly through alterations in gut microbiota composition, short-chain fatty acid production and intestinal barrier integrity, thereby linking dietary exposure to systemic immune regulation.
Although mechanistic data are increasingly consistent, clinical studies remain heterogeneous and vary in methodological quality. Therefore, while dietary strategies cannot replace pharmacological therapy, they may represent a rational adjunct approach targeting immune and oxidative mechanisms involved in RA pathogenesis. The following sections summarize current evidence regarding specific dietary patterns and supplements investigated in RA prevention and treatment, with particular attention to their potential immunomodulatory and antioxidant effects.
2.1. Vitamin D
Vitamin D is a hormone produced in the skin from 7-dehydrocholesterol after sunlight exposure. Vitamin D is also present in food products such as fish, milk, cheese and eggs. However the amount in food is low so the skin synthesis remains the main source. Biologically active form 1,25-dihydroxyvitamin D is known for its’ role in calcium metabolism and bone homeostasis. Moreover it takes part in regulation of the immune system. It has been shown that vitamin D modulates B and T lymphocytes function, affects antigen presentation by dendritic cells, promotes monocytic differentiation to macrophages and regulates macrophage responses. It also indirectly affects interleukin production, e.g., inhibits the expression of the IL-6 protein, which stimulates T helper 17 (Th17) cells – crucial part of the autoimmune reaction. Therefore proper level of vitamin D may be essential in autoimmune diseases such as multiple sclerosis, diabetes mellitus and rheumatoid arthritis [6].
Vitamin D deficiency may be an environmental factor increasing the risk of RA. Studies considered in the meta-analysis from 2012 showed a significant association between vitamin D intake and incidence of rheumatoid arthritis. In the group with the highest total vitamin D intake the risk of RA was 24,2% lower than in the group with the lowest consumption. Separate analysis showed also significant association between vitamin D supplementation and RA incidence. Group with the highest vitamin D supplement intake had a 23,6% lower risk of developing RA compared to the group with the lowest supplement intake [7].
Some studies suggest correlation between vitamin D level and rheumatoid arthritis activity and progression. In a meta-analysis from 2015 Lee and Bae included fourteen studies. They found that serum vitamin D level was significantly lower in RA patients than in control group. The vitamin D deficiency was significantly more prevalent in the RA group than in control group (55,2% vs 33,2%). Vitamin D levels were also negatively correlated with 28 joint count Disease Activity Score (DAS28) in RA patients [8].
In 2016 Lin J. et al. analysed 24 reports involving 3489 patients. They confirmed results concerning lower vitamin D serum concentrations in RA patients than healthy controls and the negative correlation between vitamin D level and RA disease activity defined as DAS28 or CRP level. The negative correlation between 25(OH)D and DAS28 was even stronger in low-latitude regions and in developing countries when compared to developed ones. Authors hypothesize that the difference in low-latitude areas occurs due to humid climate. High humidity can cause greater arthritis pain and thus result in higher DAS28 score. As for the less wealthy countries, the stronger association between vitamin D level and RA activity score may stem from differences in diet, hygiene, medications and supplements intake. There is also higher risk of infections and exposure to environmental pollutants which can worsen the effect of vitamin D deficiency [9].
However the findings are inconsistent. Craig et al. found no statistically significant association between 25(OH)D concentration and DAS28 in African Americans with recent-onset RA [10]. In Baker’s et al. research there was also no correlation between vitamin D level and DAS28, serum inflammatory markers or van der Heijde-Sharp (vdHS) erosion scores [11]. Matsumoto et al. showed lower vitamin D level in RA patients than in healthy controls but failed to confirm correlation between 25(OH)D and disease activity [12].
Likewise, a 2017 study which included 35 female RA patients and 38 age- and gender-matched healthy controls demonstrated no statistically significant differences in levels of 25(OH)D between these two groups. Both groups consisted mostly of individuals with vitamin D deficiency (71.43% and 73.68%, respectively), which also indicates high prevalence of hypovitaminosis D among middle-aged women in Polish population. Authors also didn’t demonstrate correlation between vitamin D concentration and DAS28 or joint damage based on the Steinbrocker criteria. 25(OH)D positively correlated only with IL-6 concentration in RA patients [13]. Jelsness-Jørgensen et al. in a cross-sectional study analysed the association between fatigue and vitamin D status in 169 RA patients. Fatigue was assessed by the Chalder fatigue questionnaire (CFQ). However, no statistically significant correlation was found [14].
Improvement in disease activity was observed after supplementation in 59 RA patients with vitamin D deficiency (below 20 ng/mL), DAS28-CRP > 2.6 and treated with DMARDs. Supplementation lasted 12 weeks. Initially, the dose was 60 000 IU/week for 6 weeks. Subsequently patients received 60 000 IU/month. In result, amelioration of DAS28-CRP and DAS28-ESR was reported [15].
In another study 39 female patients with early RA were examined. 21 patients were randomly assigned to treatment with single dose of 300,000 IU of cholecalciferol and 18 to placebo. Simultaneously both groups received methotrexate (MTX) 15 mg/week and methylprednisolone (GC) per os 2-4 mg/day. Treatment with vitamin D improved global health, but had no significant effect on specific signs and symptoms of RA, CRP, VAS pain and DAS28 [16].
El-Banna and Gado demonstrated regulatory T cells (Tregs) elevation and significant DAS-28 score reduction due to vitamin D supplementation. Tregs take part in the maintenance of immunological tolerance and are decreased in the peripheral blood of RA patients in comparison to healthy controls. In this study 40 RA patients were divided into two groups. Both groups received methotrexate (MTX, subcutaneous injection of 20 mg/week) plus hydroxychloroquine (200 mg twice daily), whereas second group additionally supplemented weekly 50000 IU of Vitamin D2 (Ergocalciferol 1.25 mg tablet). After 3 months there were improvements in both groups, however in group receiving vitamin D there was more significant elevation of Tregs and more significant reduction in DAS-28 score [17].
Vitamin D supplementation may seem an important part of RA treatment. However establishing causality is difficult because severity of RA symptoms can limit patients’ mobility and result in restricted contact with UV light and decreased skin synthesis of vitamin D. More studies with larger sample sizes and placebo-controlled trials are needed to determine impact of vitamin D intake on RA activity. Scientists also underline significance of verifying the vitamin D level optimal for its therapeutic functions. Evidence regarding the association between serum vitamin D levels and RA activity is presented in Table 1, while data addressing the relationship between vitamin D status and the risk of developing RA are summarized in Table 2. Findings from interventional studies evaluating the effects of vitamin D supplementation on RA activity are outlined in Table 3.
2.2. Mediterranean Diet
The Mediterranean diet is derived from habits and traditional foods consumed in Mediterranean countries. It is characterized by a frequent consumption of olive oil, high proportion of plant foods such as vegetables, fruits, unrefined grains, legumes, nuts and seeds. It also includes many condiments and spices, moderate amounts of fish, meat, eggs, fermented dairy and modest red wine intake. This dietary pattern has high fat content (up to 40-50% of total daily calories) but restricted saturated fat (less than 8% of daily calories).
Due to anti-inflammatory potential Mediterranean diet is extensively researched in regard to many diseases and its prevention. This diet has been shown to have numerous beneficial health effects especially concerning cardiovascular diseases, various types of cancer, diabetes, obesity and metabolic syndrome [18].
Scientists also investigated impact of the Mediterranean diet on management and prevention of rheumatoid arthritis. However, evidence is heterogeneous and predominantly derived from female cohorts and short-term interventions.
In 2003 Sköldstam et al. published results of randomized controlled trial conducted in Sweden with only 51 patients. 26 patients were following a Cretan version of Mediterranean diet, whereas 25 control patients were eating regular Swedish food. After 12
weeks the Mediterranean diet group obtained a reduction in inflammatory activity measured as DAS28, improvement in physical function evaluated by Health Assessment Questionnaire (HAQ), and improvement in quality of life evaluated by Swedish version of the (SF-36). There was no difference in non-steroidal anti-inflammatory drugs intake. Also no significant change was observed in the control group. However, the study sample was small and comprised mostly women [19].
130 female patients took part in another study published in 2007. This controlled clinical trial lasted 6 months and the patients were divided into two groups. 75 participants in the intervention group were given written information about Mediterranean diet and additionally attended cooking classes once a week for 6 weeks. 55 control patients received written information about healthy eating in general. Over 3 months consumption of fruit, vegetables and legumes increased significantly and the ratio of monounsaturated: saturated fats improved in the Mediterranean diet group. There were also significant improvements in the intervention group in comparison to control group in several clinical parameters such as pain score at 3 and 6 months, morning stiffness at 6 months and Health Assessment Questionnaire score at 3 months. Authors concluded that Mediterranean diet may be beneficial for women with RA regarding disease progression and severity [20].
García-Morales et al. in a randomized clinical trial evaluated the impact of a dynamic exercise program (DEP) coupled with a Mediterranean diet (MD) on quality of life in female RA patients. Women were randomly assigned to 4 groups: diet and exercise (MD + DEP), exercise only (DEP), diet only (MD) or control. After 24 weeks the most significant improvement in health-related quality of life global punctuation assessed with 36-item Short Form Health Survey v2 was observed in groups MD + DEP and DEP. The MD group also showed some amelioration in comparison to control group, however smaller. Disability assessed with Health Assessment Questionnaire Disability Index also improved in 3 groups in comparison to control. The best results were obtained again in MD + DEP group [21].
In the 12-week randomized controlled MADEIRA trial including 40 women with rheumatoid arthritis, a personalized isocaloric Mediterranean diet combined with physical activity promotion led to significantly greater diet adherence and a reduction in disease activity (DAS28) compared with usual care. Improved adherence was associated with higher intake of monounsaturated fatty acids and dietary fiber, lower saturated fat intake, and favorable changes in body composition and glucose metabolism, suggesting modulation of immunometabolic pathways relevant to RA. Disease activity correlated negatively with Mediterranean diet adherence and positively with body mass index and total dietary fat intake; however, the lack of significant changes in CRP and the relatively small sample size warrant cautious interpretation of the underlying anti-inflammatory mechanisms [22].
In the 12-week telehealth-delivered MEDRA randomized controlled trial including 44 adults with rheumatoid arthritis (87.5% women; 40 completers), both a Mediterranean diet and adherence to national Healthy Eating Guidelines led to significant improvements in physical function and quality of life. Participants in the Mediterranean diet group reported significantly better HAQ-DI and RAQoL scores at 12 weeks compared
with the control group, alongside greater increases in physical activity and Mediterranean diet adherence. Improvements were also observed within both dietary arms, suggesting that enhanced overall diet quality under dietetic supervision may beneficially modulate patient-reported outcomes in RA [23].
In another 12-week randomized feeding trial including 154 overweight and obese patients with rheumatoid arthritis (58% women), the effects of a Mediterranean diet were compared with a low-fat high-carbohydrate diet and usual care. Despite comparable weight loss between the Mediterranean and low-fat diet groups, a significantly greater reduction in disease activity (DAS28) and erythrocyte sedimentation rate was observed in the Mediterranean diet arm. After adjustment for baseline variables, dietary pattern - but not weight loss - emerged as a significant determinant of DAS28 improvement, suggesting that diet composition may modulate inflammatory pathways independently of changes in body weight [24].
Two prospective studies evaluating the association between Mediterranean diet and risk of developing RA were published in 2015. Both failed to demonstrate any significant correlation.
In the first one Hu Y. et al. followed 83,245 participants from the Nurses’ Health Study (NHS; 1980–2008) and 91,393 participants from NHS II (1991–2009) for 28 years and 20 years, respectively. All participants were females, initially free of baseline connective tissue diseases. It is also important to mention that the study sample consisted of people with high health awareness so it may not reflect the general population [25].
Sundström et al. conducted nested case–control study comprising the Västerbotten Intervention Program (VIP) cohort. 386 pre-symptomatic individuals who subsequently developed RA and 1,866 matched controls were included in the analysis. Dietary patterns (including Meditteranean diet) and alcohol consumption were analysed and no significant associations were found [26].
Another similar study was published in 2021. Nguyen et al. assessed the risk of RA based on the E3N Study – a French prospective cohort including 98,995 women since 1990. No association between Mediterranean diet and risk of RA was found in the whole population. However, adherence to Mediterranean diet diminished the risk of RA among ever-smoking women [27].
The mechanism of anti-inflammatory action of Mediterranean diet is not known. Some scientists suggest the crucial role of monounsaturated fatty acids and polyphenols present in extra virgin olive oil. Hence, Matsumoto et al. evaluated impact of monounsaturated acids on rheumatoid arthritis activity [28]. 208 patients with RA and 205 age- and sex matched healthy controls took part in the research. The participants were Japanese and mostly elderly women, which is an important limitation of this study. The intake of components of the Mediterranean diet was assessed using the brief self-administered diet history questionnaire (BDHQ) only once, at the beginning of the TOMORROW study. There was a significant negative correlation between DAS28-ESR and the ratio of monounsaturated to saturated fatty acid (MUFA/SFA) intake. Also the group with high disease activity had low MUFA/SFA intake. Therefore authors concluded that monounsaturated fatty acids may be the component of Mediterranean diet responsible for suppression of RA activity.
A recent narrative review comprehensively summarized current evidence on the Mediterranean diet (MD) in rheumatoid arthritis, highlighting its potential anti-inflammatory and immunomodulatory effects [29]. The authors emphasized that MD, rich in fiber, polyphenols, unsaturated fatty acids and antioxidants, may modulate key inflammatory pathways involved in RA, including cytokine production (TNF-α, IL-6, IL-1β) and T-cell polarization. Several clinical trials reviewed demonstrated improvements in DAS28 scores, physical function and quality of life among RA patients adhering to MD, although heterogeneity in study design and duration limits definitive conclusions. Importantly, the review also underlined the role of MD in shaping gut microbiota composition, promoting short-chain fatty acid production and supporting redox balance, suggesting that microbiome-mediated and antioxidant mechanisms may partly explain the observed clinical benefits. The authors concluded that, while current evidence remains limited and further well-designed randomized controlled trials are required, the Mediterranean diet represents a promising complementary and cost-effective lifestyle approach in chronic autoimmune diseases, including RA, particularly when considered alongside pharmacological and other non-pharmacological strategies. Evidence concerning the association between adherence to the Mediterranean diet and the risk of RA development is summarized in Table 2, whereas studies evaluating its effects on disease activity are presented in Table 4.
2.3. Fish and Omega-3 Fatty Acids
Fatty fish are the main dietary source of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) – two types of polyunsaturated omega-3 fatty acids which downregulate proinflammatory cytokines. Their anti-inflammatory properties are well-known, thus their use is considered in various diseases including RA. EPA and DHA cannot be synthesized by humans so they have to be provided with food. However significant percentage of people in the developed countries don’t reach the recommended levels for fish and omega-3 intake [30]. The effective dose of EPA and DHA exceeds omega-3 content in one portion of fish. This suggests a need for using EPA and DHA supplements especially in inflammatory diseases such as RA.
There is also α-linolenic acid (ALA) which is a type of omega-3 fatty acid found in plant food such as flaxseed or walnuts. It can be converted into EPA and DHA but the efficacy of this process is very low (0,2% and 0,05% respectively) [31].
Another type of essential polyunsaturated fatty acids is omega-6. Ratio of omega 6s to omega 3s in diet is crucial since it influences the type of produced eicosanoids. Those derived from arachidonic acid (AA, type of omega-6) are involved in inflammation affecting joints and cartilage destruction in RA.
In a research from 2003 Adam O. et al. showed that low arachidonic acid (AA) diet improves effect of fish oil supplementation in RA. 60 patients were divided into two groups. One was on the anti-inflammatory diet (AID) with AA intake reduced to < 90 mg per day. It was a modified lactovegetarian diet without animal fat such as egg yolk and with dairy products with reduced fat content. Meat consumption was limited to a maximum of 2 portions of 120 g per week. Second group was on the western diet (WD) with regular meat products consumption, characteristic for developed countries. In each group patients were randomized for allocation to fish oil or placebo (corn oil). The fish oil supplementation provided 30 mg of n-3 fatty acids per kg of body weight. After 3 months there was a 2-month washout period and then patients crossed over to the other treatment (placebo or fish oil). In AID patients an impact of fish oil supplementation was more noticeable. Compared to WD patients receiving fish oil there was significant reduction in the numbers of tender (28% vs 11%) and swollen (34% vs 22%) joints [32].
Supplementation with n-3 fatty acids was already tested as an adjunctive therapy in RA. Majority of the research was conducted in the 90s. In a randomized, double-blind trial in 1992 Nielsen et al. observed an improvement in two out of six disease parameters – morning stiffness and joint tenderness in the group receiving n-3 supplementation. 51 patients with active rheumatoid arthritis took part. Study group received capsules of fish oil containing 2 g EPA and 1,2 g DHA every day for 12 weeks. Control group received capsules with a composition of fatty acids characteristic for Danish diet (mostly saturated and polyunsaturated but no n-3 fatty acids) [33].
In another double-blind controlled study from 1992 small anti-inflammatory effect in RA was observed. 43 patients completed the trial. Fish oil group participants were given 10g of fish oil for 6 months. After 3 and 6 months they reported significantly smaller intake of nonsteroidal anti-inflammatory drugs (NSAID) and an improvement of global arthritic activity after 3 months [34].
Reduction of NSAID requirement among mild RA patients was also shown in Lau C.S. et al. work in 1993. Patients in study group received 10 capsules with fish oil per day, each containing 171 mg EPA and 114 mg DHA. The double-blind placebo controlled trial lasted 12 months. First effect was observed after 3 months of supplementation and it lasted 3 more months after the end of trial. The most significant difference between study group and placebo was observed after 12 months. Patients receiving fish oil had average intake of NSAID reduced to 40,6% of the original dose compared to 84,1% in placebo group [35].
More recent randomized, double-blind controlled trial from 2013 showed the efficacy of fish oil supplementation as adjunctive therapy in modern treat-to-target drug treatment for recent onset RA. Proudman et al. observed higher rate of remission and decreased disease-modifying anti-rheumatic drugs (DMARDs) use among patients receiving 5,5 g EPA and DHA per day. There was no significant difference in methotrexate dose, modified Health Assessment Questionnaire (mHAQ) and Disease Activity Score in 28 Joints with erythrocyte sedimentation rate (DAS28-ESR) between groups.
However the control group also received EPA and DHA but 400 mg per day, which is insufficient to have an anti-inflammatory impact, according to the previous studies [36].
A meta-analysis of 17 randomized controlled trials demonstrated that omega-3 fatty acids supplementation is effective in improving pain outcomes. Significant results were obtained after 3 months with at least 2,7g per day of EPA and DHA. The improvement was observed particularly in duration of morning stiffness, number of painful and/or tender joints, patient assessed pain and NSAID intake. However the analysis included not only patients with RA, but also with joint pain secondary to inflammatory bowel disease and dysmenorrhea [37].
Another meta-analysis from 2012 which included 10 randomized controlled trials showed that supplementation with at least 2,7g of omega-3 fatty acids per day for minimum 3 months is effective for reducing NSAID dose among RA patients. However no significant improvement was found for other clinical outcomes such as tender joint count, swollen joint count, morning stiffness and physical function [38].
In more recent meta-analysis of 20 randomized controlled trials that involved 1288 patients Gioxari A. et al. also ascertained the beneficial impact of omega-3 fatty acids consumption on RA disease activity. However authors emphasized overall low quality of trials. The interventions lasted from 12 to 72 weeks. Patients were given daily dose of 0.30 to 9.60 g omega-3 fatty acids, either as a supplement or from food sources. In the majority of analyzed trials supplementation resulted in improved early morning stiffness, tender joint count, erythrocyte sedimentation rate and pain scale. Another statistically significant effects were the amelioration of blood triacylglycerol levels and the reduction of leukotriene B4 blood levels. There were no differences in the level of other inflammatory markers such as CRP, IL-6, IL-1 and TNF-α [39].
In contrast to marine-derived omega-3 fatty acids, evidence for plant-derived omega-3 fatty acids, primarily α-linolenic acid (ALA), in rheumatoid arthritis remains limited. In a 12-week randomized controlled trial including 120 patients with RA (111 women), supplementation with 30 g/day flaxseed - a rich dietary source of ALA - either alone or combined with an anti-inflammatory diet resulted in significant improvements in disease activity (DAS28), pain, morning stiffness, and quality of life compared with a control intervention. Notably, these clinical benefits occurred without significant changes in classical inflammatory markers, including CRP, ESR, rheumatoid factor, or anti-CCP antibodies. The findings suggest that plant-based omega-3 fatty acids may exert beneficial effects on RA-related symptoms through mechanisms not directly reflected by systemic inflammatory biomarkers, potentially related to neuromodulation, pain perception, or indirect immunometabolic pathways, while highlighting the limited conversion of ALA to long-chain omega-3 fatty acids as an important interpretative constraint [40] .
Importantly, evidence in rheumatoid arthritis extends beyond omega-3 supplementation and also includes studies assessing fish consumption as part of the habitual diet.
Tedeschi et al. assessed whether frequency of fish consumption is associated with disease activity in RA. In the cross-sectional analysis they evaluated Disease Activity Score in 28 Joints with CRP (DAS28-CRP) for 176 participants. Participants filled in a food-frequency questionnaire concerning their diet during past year. In the group with most frequent fish consumption there was longer disease duration and the highest percentage of smokers. Nevertheless those consuming fish ≥2 times per week had significantly lower DAS28-CRP than those with consumption lower than one serving per month. Also each additional portion of fish per week was associated with significantly lower DAS28-CRP [41].
Two complementary publications originating from the same randomized cross-over PIRA trial evaluated the acute effects of different protein sources, including fatty fish, on immunometabolic responses in rheumatoid arthritis. In this study including 25 patients with RA (predominantly women), isocaloric meals based on fatty fish, red meat, or soy protein did not differ in their postprandial effects on circulating IL-6, indicating that fatty fish did not elicit a distinct short-term anti-inflammatory response compared with other protein sources. However, metabolomic analyses from the same trial demonstrated that fatty fish meals induced a distinct postprandial lipid and metabolite profile, particularly affecting lipoprotein subclasses and fatty acid–related pathways, compared with red meat and soy. These findings suggest that while acute intake of fatty fish may not immediately modulate classical inflammatory markers in RA, it may influence immunometabolic pathways relevant to longer-term immune regulation and inflammatory processes [42,43].
Some studies concern the influence of omega-3 and fish consumption on the risk of developing RA. However available results are not consistent. A dose-response meta-analysis of 7 studies showed weak, non-statistically significant inverse correlation between fish consumption and risk of RA. According to analysed data, there is a decrease of RA risk for up to two servings of fish per week. Higher consumption (3 and 4 portions per week) was associated with a slightly increased risk of RA [44]. Authors explained the results with possible effect of polychlorinated biphenyls (PCBs). PCBs are contaminants often present in food, especially fatty fish, which are also the richest source of omega-3 acids. Exposure to PCBs was found to be positively associated with RA among women [45].
Di Giuseppe et al. published in 2013 a prospective cohort study of middle-aged and older women. Authors analysed data from food-frequency questionnaires and observed inverse association between long-term intake of dietary omega-3 and risk of developing RA . Regular intake of > 0,21 g omega-3 per day was associated with a 52% lower risk of RA. Such dose of omega-3 acids corresponded to at least one portion per week of fatty fish (e.g., salmon) or four portions per week of lean fish (e.g., cod). 29% decrease of risk was correlated with total consumption of fish at least once per week in comparison with less than one serving per week [46].
In a case-control study from 1996 it was reported that higher intake of omega-3 estimated from frequency of fish consumption was associated with reduced risk of RA among women. The strongest association was observed regarding to broiled or baked fish, but not other types e.g., fried. Authors also found a correlation with total protein and calorie intake. Increased protein content was associated with lower RA risk, whereas higher total caloric intake was associated with increased RA risk [47].
However in a recent prospective cohort study from 2018 which involved 166,013 women no protective impact of fish or omega-3 fatty acids consumption on RA risk was observed. Smoking-fish interaction for RA risk was also analysed. Authors found statistically significant difference in ever smokers with infrequent fish intake vs. ever smokers with frequent fish intake among women aged ≤55 years. RA risk was very elevated in the first subgroup (HR 2.59, 95%CI 1.65–4.06) and modestly increased in the second one ((HR 1.29, 95%CI 1.07–1.57;) in comparison with never smokers/frequent fish intake [48].
2.4. Vegan Diet, Gluten-Free Diet and Fasting
Some other dietary patterns were examined in order to assess impact on rheumatoid arthritis severity. Data is limited due to few studies with small groups of patients. Except for Mediterranean diet, the most extensively researched is vegan diet with various modifications. McDougall et al. studied impact of very low-fat vegan diet on moderate-to-severe rheumatoid arthritis. 24 patients for 4 weeks followed vegan diet consisting of only 10% of calories from fat. As a result scientists registered among patients a significant improvement of RA symptoms such as decrease in joint tenderness score, joint swelling score, degree of pain because of RA and improvement in severity of morning stiffness and limitation in ability to function. However, there were no significant differences in ESR, C-reactive protein, rheumatoid factor and duration of morning stiffness. Moreover, this study has many limitations; one of the most serious is lack of control group. The study fails to account for placebo effects and recurring changes in disease activity, therefore is less credible [49].
In the 16-week randomized controlled Plants for Joints trial including 83 patients with rheumatoid arthritis (92% women; 77 completers) and low–moderate disease activity, a multidisciplinary lifestyle program based on a whole-food plant-based diet, physical activity, and stress management led to a significantly greater reduction in DAS28 compared with usual care. The intervention resulted in a clinically meaningful improvement in disease activity (mean between-group difference −0.9 DAS28 points), accompanied by significant reductions in body weight, fat mass, waist circumference, HbA1c, and LDL cholesterol. Notably, improvements in disease activity occurred despite no significant between-group changes in CRP or ESR, suggesting that mechanisms beyond measurable systemic inflammation—potentially involving immunometabolic or lifestyle-related pathways - may contribute to the observed clinical effects. However, the combined nature of the intervention precludes attribution of the benefits to diet alone, and the short duration limits conclusions regarding long-term immune modulation [50].
More extreme raw version of vegan diet was examined by Hänninen and coworkers [51]. This diet, also called living food, consists of berries, fruits, vegetables and roots, nuts, germinated seeds and sprouts. Intervention lasted 3 months and 40 RA patients took part. They were divided into two groups (raw vegan and omnivorous/control) and received meals prepared in specialized kitchen. Patients on raw vegan diet reported subjective improvement in RA symptoms, which was confirmed by relative activity index (RAI), which highly correlates (r 0.92,P 0.0001) with DAS index. According to these results, raw vegan diet may be beneficial for RA patients.
However, in earlier study on raw vegan diet in RA published in 1993 Finnish scientists observed low availability of energy. Although 21 RA patients increased their energy intake on raw vegan diet, they lost 9% of their body weight [52].
Combination of plant-based diet with gluten-free regimen was also investigated. In a study from 2001 patients with active RA were to follow for 1 year either vegan diet free of gluten or a well-balanced non-vegan diet. 22 patients from the first group and 25 from the second completed 9 months or more of the recommended regimen. The improvement of symptoms was measured by the American College of Rheumatology response criteria (ACR20). Also joint destruction was assessed radiographically. Based on ACR20 vegan group obtained better improvement - 40,9% (22 patients) were classified as diet responders in comparison to 4% (1 patient) of the non-vegan group. However, there were no significant differences in radiographic progression between two groups. Researchers concluded that vegan diet free of gluten may reduce symptoms of RA but doesn’t protect against joint destruction [53].
Another study of vegan gluten-free diet aimed to investigate impact on blood lipids oxidized low-density lipoprotein (oxLDL) and natural atheroprotective antibodies against phosphorylcholine (anti-PCs). 66 patients with active rheumatoid arthritis were assigned to one of two groups. 38 patients in the first group were ordered to follow gluten-free vegan diet and second group consisted of 28 patients who were ordered to follow well-balanced non-vegan diet – both for 1 year. In the vegan group 30 patients completed at least 3 months of diet and ultimately only 22 patients in this group complied with recommendations for 12 months. Research primarily focused on parameters related to atherosclerosis and cardiovascular diseases. After 12 months of gluten-free vegan diet patients had significantly lower level of total cholesterol, LDL, BMI and higher level of anti-PC IgM in comparison with control group. Moreover vegan diet resulted in significantly lower DAS28 and HAQ score after 3 and 12 months compared to initial values. Also CRP was substantially lower but only after 12 months. Among non-vegan group there were no significant differences except for minor decrease of DAS28 after 3 months of diet. The results may support the use of gluten-free vegan diet in management of rheumatoid arthritis [54].
In a secondary analysis of the prospective multicentre BELIEVE cohort, which included patients with various chronic inflammatory diseases, the impact of habitual gluten intake was also assessed specifically in patients with rheumatoid arthritis (n = 37) initiating biological therapy. In the RA subgroup, no association was observed between high versus low-to-medium gluten intake and the likelihood of achieving clinical response to biologic treatment after 14–16 weeks, defined according to ACR20 criteria. Similarly, gluten intake was not associated with changes in disease activity or C-reactive protein levels during follow-up. These findings suggest that, in patients with RA starting biologic therapy, habitual gluten consumption does not appear to meaningfully influence short-term treatment response, although the limited sample size of the RA subgroup warrants cautious interpretation [55].
Another intensively researched dietary intervention in rheumatoid arthritis is fasting. Combination of fasting and vegan or vegetarian diet was analysed in numerous clinical trials [56]. The most commonly used research plan was 7-10 days of fasting, followed by 3,5 months of gluten-free vegan diet and subsequently lactovegetarian diet for up to a year.
Kjeldsen-Kragh et al. observed significant improvement among 27 patients after such intervention comprising 7-10 days of fast and then reintroducing “new” product every second day within gluten-free vegan diet. After 3,5 months the diet was extended to lactovegetarian. During the fast patients were allowed to consume vegetable broth, decoction of potatoes and parsley, herbal teas, garlic and carrot, beetroot or celery juice. After 4 weeks of the regimen patients exhibited decrease in number of tender and swollen joints, Ritchie articular index (RAI), pain, morning stiffness duration, grip strength, HAQ score, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and WBC count. The improvements were maintained throughout the year [57].
In other study scientists assessed impact of fasting and ketogenic diet on serum interleukin-6 (IL-6), dehydroepiandrosterone sulphate (DHEAS) and disease activity in RA patients. For 7 days 10 participants underwent subtotal fast with only vegetable juices allowed. Simultaneously 13 patients followed isocaloric ketogenic diet with less than 40 g of carbohydrates per day. Subsequently both groups underwent 2 weeks of re-feeding with lactovegetarian diet. Significant decrease in serum IL-6 and improvement in ESR, CRP and tender joint count were observed after 7-day-fasting, but not after ketogenic diet. However, serum DHEAS level was significantly increased after 7 days in both groups. Authors concluded that the reduction in serum IL-6 resulted from decreased IL-6 production in the synovium, which explains the correlation with disease activity improvement. However, fasting can be used only as a short-term intervention and rapidly after ending the fasting period RA symptoms return. Therefore authors do not consider intermittent fasting beneficial in managing rheumatoid arthritis [58].
In the exploratory NutriFast randomized controlled trial, 53 patients with rheumatoid arthritis were assigned either to a 7-day medically supervised fast (300–350 kcal/day) followed by an 11-week plant-based diet combined with time-restricted eating, or to a 12-week guideline-based anti-inflammatory diet according to the German Society for Nutrition. The primary endpoint (change in HAQ-DI at 12 weeks) did not differ significantly between groups. However, fasting induced a rapid improvement in functional status and disease activity within 7 days, which was sustained during the subsequent plant-based phase and maintained up to 6 months. Both dietary strategies led to significant reductions in DAS28, CDAI and SDAI scores by week 12, with a higher proportion of early ACR50 responses observed in the fasting group. Importantly, fasting followed by a plant-based diet resulted in greater weight loss and more pronounced improvements in cardiometabolic parameters, including reductions in atherogenic lipoproteins, while remaining safe and well tolerated. These findings suggest that short-term fasting combined with a plant-based dietary pattern may offer a rapid-acting, supportive non-pharmacological strategy in RA, particularly in the context of integrative management [59].
Two publications originating from the same randomized controlled trial evaluated the effects of intermittent fasting (16:8) in 44 overweight and obese postmenopausal women with rheumatoid arthritis. In this 8-week intervention, intermittent fasting led to significant improvements in disease activity indices (DAS28 and CDAI), physical function (HAQ-DI), body weight, and body mass index compared with a usual diet. However, no significant between-group changes were observed in systemic inflammatory markers (ESR, hs-CRP, IL-6) or oxidative stress parameters (TAC, TOS, OSI), despite improvements in clinical outcomes. Together, these findings suggest that short-term intermittent fasting in this population may improve RA disease activity and quality of life predominantly through weight-related or functional mechanisms rather than direct modulation of systemic inflammatory or oxidative pathways [60,61].
Evidence on effectiveness of various dietary patterns in rheumatoid arthritis suppression is promising, yet still insufficient. Moreover vegan and gluten-free diets can be difficult to sustain long term for many patients, whereas fasting provides only short-term effects. Further research is necessary in order to create proper recommendations. Research on impact of dietary regimens on RA activity is summarized in Table 4.
2.5. Antioxidants
Reactive oxygen and nitrogen species are produced in the course of inflammatory processes and are thought to play an important role in the aetiology of inflammatory diseases such as rheumatoid arthritis. Therefore antioxidants may be useful in preventing RA and managing symptoms. Effectiveness of various antioxidants was assessed in humans and animal models with conflicting results [62,63,64].
Few studies evaluated influence of supplements with combined several antioxidants on RA symptoms with promising results [65,66]. Jalili M et al. used capsules containing 50 μg selenium, 8 mg zinc, 400 μg vitamin A, 125 mg vitamin C, and 40 mg vitamin E. 40 female patients with RA received one capsule daily for 12 weeks. Supplementation resulted in significantly decreased DAS-28 score and serum hs-CRP. There were no differences in number of swollen and painful joints. Moreover erythrocyte antioxidant parameters such as catalase (CAT), glutathione peroxidase (GPX), superoxide dismutase (SOD) and total antioxidant capacity increased significantly after intervention [67].
Natural herbs, spices and plants with antioxidant properties have also been studied in regard to rheumatoid arthritis activity. Cranberry juice was recently used in a study conducted with 41 women with RA. 23 participants consumed daily 500 ml of low-calorie cranberry juice for 90 days, the remaining 18 patients maintained their usual diet. After the intervention there were no differences in the inflammatory biomarkers. There was a significant reduction in DAS28 and in anticyclic citrullinated peptide (anti-CCP) antibodies levels in the cranberry group. However, authors emphasized the broad interindividual response to cranberry juice. Not all of the patients in the experimental group noted a decrease in DAS28. 5 patients maintained the initial level and 5 other even increased DAS28 in response to the intervention. Authors hypothesize that many factors such as genetic polymorphisms, environmental influences or the composition of the gut microbiome may be responsible for this diversity [68].
Cranberry juice was also examined in adjunction to fish oil. RA patients were randomized into three groups. First group (21 patients) was a control, eating their usual diet. Second group (21 patients) received 3 g of omega-3 fatty acids daily. Third group (20 patients) consumed 3 g of omega-3 fatty acids and 500 mL of reduced-calorie cranberry juice daily. Fatel et al. showed additional beneficial effects of a combination of fish oil and cranberry juice on disease activity and inflammation level after 90 days of supplementation compared to fish oil: ESR, CRP, IL-6, DAS28-CRP and adiponectin were significantly decreased. Only the last two parameters were decreased in the fish oil group [69].
Turmeric (Curcuma longa) is a herb with anti-inflammatory properties, which has long been used in traditional Chinese and Ayurvedic medicines. Turmeric contains various bioactive compounds, out of which the most important and most frequently used is curcumin. Curcumin modifies NF-κB signalling, proinflammatory cytokines such as interleukin production and phospholipase A2, COX-2, and 5-LOX activities. The efficacy and safety of curcumin was assessed in 45 patients with active rheumatoid arthritis in a randomized clinical study. Patients were randomized into three groups, each of them received 500 mg curcumin, 50 mg diclofenac sodium or combination of both. After 8-week intervention all three groups showed significant decrease in DAS28 and improvement in ACR scores (ACR 20, 50 and 70). However, the results in the curcumin group were significantly better than in the diclofenac sodium group. Also a significant decrease in CRP level was observed only in the curcumin group [70].
In another study a novel, highly bioavailable form of curcumin in turmeric matrix was assessed for its impact on RA symptoms. For 90 days three groups, each comprising of 12 patients, received placebo, 250 or 500 mg of the curcumin product twice daily. At the end of the study significant improvement in DAS28, visual analog scale (VAS) and ACR scores was observed in both treatment groups. Patients receiving curcumin product showed also a significant decrease in ESR, CRP and RF values. In some cases the higher dose was slightly more effective [71].
Westerlind et al. examined the influence of tea, which is rich in antioxidants and therefore may reduce the risk of RA. Based on EIRA (Epidemiological Investigation of RA) study, a population-based case control study, the association between tea consumption and RA risk was assessed. The risk of RA was inversely correlated to high tea consumption in comparison to irregular consumption among smokers and in the ACPA-positive subset of RA [72].
Apart from individual dietary components, anti-inflammatory diet was studied as a whole. This type of diet was shown to reduce disease activity measured as DAS28-ESR in study published in 2020. However, the results were not statistically and clinically relevant. 47 RA patients completed at least one diet period, which lasted from 8 to 13 weeks. Diet contained fish (mostly salmon), vegetarian dishes with legumes, whole-grain cereals, vegetables, yoghurt for sauces, spices, fruits as snacks [73].
In another study published in 2021, dietary inflammatory index (DII®) and energy-adjusted DII (E-DII™) were calculated based on the brief-type self-administered diet history questionnaire (BDHQ) filled by 177 RA patients and 183 control subjects. Data was acquired from TOMORROW (Total management of risk factors in rheumatoid arthritis patients to lower morbidity and mortality) study. Matsumoto et al. demonstrated an association between anti-inflammatory change in E-DII and maintaining low disease activity (DAS28-ESR ≤ 3.2) [74].
2.6. Salt
Growing evidence suggests crucial impact of excessive salt and dietary sodium intake on autoimmune diseases development and possibly on severity of symptoms. High concentrations of sodium chloride have been shown to stimulate the differentiation of T helper (Th) lymphocytes into pro-inflammatory Th17 cells by salt-sensing serum glucocorticoid kinase 1 (SGK1) [75,76].
Two studies on association between salt intake and RA risk provided contradictory results. A Swedish nested case-control study failed to find significant association between sodium intake and RA development when compared 386 patients to 1886 matched controls. However, a separate analysis adjusted for smoking status revealed two times higher risk for RA among smokers and dose-dependent association. Smokers in the highest sodium intake tertile had higher risk for RA than those in the lowest tertile [77].
Another cross-sectional nested study included 18,555 individuals, 392 developed RA. Sodium intake was associated with RA risk and the effect was dose-dependent. Higher risk was observed in the highest quartile, among people consuming more than 4,55 grams of sodium per day. However, the association was stronger in nonsmokers, in contrast to previous study [78].
In order to assess sodium intake in RA patients 24-hour urinary sodium excretion was measured. Sodium excretion was significantly increased in 24 patients with untreated early RA in comparison with 24 matched healthy controls. It was found higher in patients with erosions than those without. However, there was no correlation between sodium excretion and disease activity [79].
Scrivo R. et al. in their research introduced dietary regimen based on modulation of sodium intake. Three weeks of low-sodium intake (< 5 g of sodium chloride/day) were followed by 2 weeks of normal-sodium dietary regimen (5 g of sodium chloride/day). 14 patients with rheumatoid arthritis completed the study protocol. A reduction in the percentage of Th17 cells after low-sodium intake period was observed and an increase after next 2 weeks of normal-sodium intake, whereas regulatory T cells (Treg) showed the opposite trend. However, the differences were not statistically significant. Also a reduction of TGFβ1 and IL-9 was observed at the end of the fifth week in comparison to the baseline. These are cytokines with a pro-inflammatory role in RA [80]. Data regarding the association between dietary salt intake and RA incidence as well as disease activity are presented in Table 2 and Table 3, respectively.
3. Gut Microbiome in Rheumatoid Arthritis
Particular parts of human body such as skin, gut, oral cavity, upper respiratory tract and female genital tract are abundant in commensal and symbiotic microorganisms, as a whole called microbiome. There is growing experimental and clinical evidence for essential impact of microbiome on human health. Especially gut microbiota seems to largely contribute to pathogenesis of inflammatory and autoimmune diseases, such as rheumatoid arthritis. Intestinal microbiota is largely responsible for maintaining homeostasis of the host immune system. Thus, any alteration in composition of microbiota may result in changes in the host immune response. Moreover it was shown that composition of gut microbiome can be modified by various factors, including infections, drugs, stress and most of all diet. Therefore it is possible that efficacy of dietary interventions in RA is connected with changes in gut microbiome.
Apart from gut microbial diversity scientists note the importance of permeability of the gut wall lumen in the inflammatory processes. Increased permeability leads to exposure of the immune system to microorganisms which normally wouldn’t cross the intestinal barrier. According to the gut-joint-axis hypothesis this causes immune response and subsequently via haematological spread, a local inflammatory process within the joints [81].
It was demonstrated that specific nutrients and compounds can influence gut permeability. Deterioration of intestinal barrier structure occurs after consumption of compounds characteristic of western diet, such as milk fat, fatty acids (particularly in high-fat diets), alcohol, gliadin and additives used in food industry, particularly salt, sugar, emulsifiers and surfactants, organic solvents, and microbial transglutaminase. Contrarily, many nutrients and compounds abundant in Mediterranean diet have been shown to decrease gut permeability. These are curcumin, polyphenols such as quercetin, myricetin and kaempferol, zinc, vitamin D and aminoacids – glutamine and tryptophan [82].
Gut microbiota comprises of numerous non-eukaryotic cells, most of which are bacterial. Despite huge diversity, gut bacteria belong to several dominating phyla, including Bacteroidetes, Actinobacteria, Proteobacteria, Firmicutes, Verrucomicrobia and Fusobacteria. Bacteroidetes and Firmicutes make up over 90% of intestinal bacteria. Arumugam M. et al. in their analysis distinguished three enterotypes in the human gut microbiome. Each was dominated by different genus: Bacteroides (enterotype 1), Prevotella (enterotype 2) or Ruminococcus (enterotype 3). They also display significant functional variation e.g., in enzymatic properties and vitamin biosynthesis [83]. Another research reduced the enterotypes to two clusters, one dominated by Bacteroides or Clostridiales, and the other dominated by Prevotella [84]. However, more recent study failed to distinguish distinct bacterial taxa and described rather gradients of both Bacteroides and Prevotella. Authors found the term “enterotypes” misleading and suggested using term “biomarker” instead to describe the dominant taxon [85].
Patients with rheumatoid arthritis display diminished gut microbial diversity and significantly different composition of gut and oral microbiome than healthy controls. Scientists observed relative enrichment of Gram-positive bacteria and depletion of Gram-negative bacteria such as some Proteobacteria and Gram-negative Firmicutes of the Veillonellaceae family in gut microbiome of RA patients. Particularly Haemophilus species were reduced and Lactobacillus salivarius was more abundant in RA patients. Modifications in gut microbiome make-up correlated with clinical measures such as such as CRP, anti-CCP and RF. Therefore it was suggested that chronic inflammation characteristic of rheumatoid arthritis might be exacerbated by deficiency of commensal bacteria or overabundance of pathogenic bacteria. The oral and gut dysbiosis was partially corrected after treatment with disease-modifying antirheumatic drugs (DMARDs) [86].
Vaahtovuo et al. demonstrated that patients with early RA have significantly less bifidobacteria and bacteria of the Bacteroides-Porphyromonas-Prevotella group, B. fragilis subgroup, and the E. rectale – C. coccoides group in comparison with fecal microbiota of patients with fibromyalgia (FM). Authors emphasize that there are two possible explanations for these results. Presumably patients with RA lack certain bacteria involved in immune homeostasis. However, it is also possible that those patients have greater diversity of bacteria that cannot be detected by chosen method and set of used oligonucleotide probes. Authors chose FM patients as controls, because just as RA patients they receive NSAID medication, and their age and sex distributions are similar, but FM is a noninflammatory disease [87].
In another experimental study diminished gut microbial diversity in RA patients correlated with disease duration and autoantibody levels. The diversity between microbiota of RA patients and healthy controls was displayed by differences in taxa, particularly the increase of rare bacterial lineages such as phylum Actinobacteria, along with its two genera, Eggerthella and Actinomyces in RA patients. Moreover, as it was shown in a humanized mouse model, Collinsella aerofaciens intensifies severity of arthritis. Collinsella also increases gut permeability, lowers the expression of TJ proteins and stimulates the epithelial production of IL-17A, so it may cause an increased inflammation and participate in RA pathogenesis [88].
In an observational study including 110 patients with established rheumatoid arthritis and 110 age- and sex-matched healthy controls, an increased abundance of the genus Collinsella was associated with cumulative inflammatory burden in RA. Higher levels of Collinsella were observed in patients with moderate to high disease activity and remained independently associated with long-term inflammatory activity alongside age, obesity, and impaired physical function. Alterations in gut microbiota composition, including Collinsella expansion, were accompanied by differences in predicted microbial metabolic pathways related to purine metabolism and short-chain fatty acid fermentation [89].
Li et al. also demonstrated significant alterations of gut microbiota in RA patients compared to healthy controls. Phylum Proteobacteria, which includes many pathogenic bacteria such as Enterobacter, was more abundant in RA patients, whereas Firmicutes was diminished. Moreover, the relative abundance of Blautia, Ruminococcus2, and Odoribacter was negatively correlated with T, B, CD4+T, and Tregs [90].
In a cross-sectional clinical study including 87 patients with moderate-to-severe rheumatoid arthritis, Kitamura et al. examined associations between intestinal bacterial load, bacterial-derived substances, and disease activity. Serum levels of lipopolysaccharide-binding protein (LBP) and fecal lipopolysaccharide (LPS) were positively correlated with multiple markers of disease activity and systemic inflammation, including DAS28, CRP, ESR, MMP-3, and IL-6, while total intestinal bacterial counts were inversely associated with circulating LPS levels. In addition, antibodies against Porphyromonas gingivalis–derived LPS were inversely correlated with pain and patient-reported disease activity, supporting the concept of an oral–gut microbiome axis in RA. Although the study design does not allow causal inference, the findings suggest that translocation of bacterial components and impaired endotoxin neutralization may contribute to inflammatory burden in established RA [91].
In a cross-sectional study including 94 patients with established rheumatoid arthritis treated with disease-modifying antirheumatic drugs (DMARDs) and 30 healthy controls, Koh et al. demonstrated that gut microbiome composition in RA differs from that of healthy individuals, despite comparable overall microbial richness and diversity. Microbiome profiles were influenced by age, with younger RA patients (<45 years) showing reduced diversity and a distinct microbial signature compared with older patients and controls, whereas disease activity, RF, and ACPA status were not associated with microbial composition. Most conventional synthetic DMARDs (csDMARDs; e.g., methotrexate, sulfasalazine) and biologic DMARDs (bDMARDs; targeted monoclonal antibodies or fusion proteins directed against specific immune pathways) showed limited impact on gut microbiota structure, although sulfasalazine was associated with reduced diversity and specific taxonomic shifts. Importantly, the relative abundance of selected genera, particularly Subdoligranulum and Fusicatenibacter, was associated with subsequent response to second-line csDMARD therapy, suggesting a potential link between gut microbiome composition and treatment outcomes in established RA [92] .
In a multicentre, longitudinal observational study of 144 DMARD-naive patients with newly diagnosed rheumatoid arthritis, Danckert et al. investigated whether baseline gut and oral microbiota could predict clinical response to DMARD therapy. Shotgun metagenomic sequencing revealed that patients who achieved a minimal clinically important improvement showed a progressive reduction in specific taxa, particularly Prevotella spp. at six weeks and Streptococcus spp. at twelve weeks of treatment. Importantly, baseline microbiome composition was indicative of future treatment response, suggesting that microbiota signatures precede and potentially modulate therapeutic outcomes. The authors noted that DMARD therapy was associated with a partial restoration of a more eubiotic microbiome profile, although causal relationships cannot be inferred from the observational design [93]. Together, these findings suggest that gut microbiome composition may not only reflect disease status, but also influence therapeutic trajectories in RA.
In another large cross-sectional study including 262 patients with rheumatoid arthritis and 475 healthy controls, Wang et al. demonstrated that gut microbiota profiles could be used to construct predictive models discriminating RA from healthy individuals. Using 16S rRNA sequencing and machine-learning approaches, the authors identified a set of seven genera that enabled moderate diagnostic performance across independent datasets. Although the study focused primarily on disease classification rather than therapeutic outcomes, several of the identified taxa (including Subdoligranulum and Fusicatenibacter) have previously been implicated in treatment response and inflammatory regulation in RA. The authors emphasized that microbiome-based prediction remains exploratory and requires validation in longitudinal and treatment-focused cohorts [94].
Growing evidence indicates that in rheumatoid arthritis microbiome alterations are not limited to compositional dysbiosis but involve significant disturbances in microbial metabolic activity that directly influence immune regulation and epithelial barrier function. Reduced levels of short-chain fatty acids, particularly butyrate, have been associated with impaired tight junction integrity, anti-CCP positivity and structural joint damage, while altered microbial tryptophan metabolism and dysregulated bile acid signaling may contribute to Th17 polarization, interferon-related pathways and persistent systemic inflammation. At the same time, specific microbial metabolites, including certain indole derivatives, exert barrier-protective and anti-inflammatory effects, underscoring the dual and context-dependent role of microbial metabolism in RA pathogenesis. Diet represents a major determinant of microbial functional output, whereas dietary fiber, polyphenol-rich patterns and microbiota-targeted strategies such as probiotics may partially restore immunometabolic balance. However, although mechanistic links between diet, microbial metabolites and immune pathways are increasingly supported by experimental data, clinical evidence remains heterogeneous and requires validation in longitudinal and interventional studies [95].
In a multi-omics cross-sectional study including 122 patients with rheumatoid arthritis and 67 healthy controls, Zhang et al. demonstrated that alterations in gut microbiota composition in RA are closely linked to changes in circulating and fecal microbial metabolites. Patients with RA exhibited a distinct metabolic signature characterized by reduced levels of short-chain fatty acids and tryptophan-derived metabolites, alongside enrichment of metabolites related to amino acid and bile acid metabolism. Integration of microbiome and metabolomic data revealed significant correlations between specific bacterial taxa and inflammatory metabolites associated with immune activation and disease activity. These findings suggest that functional metabolic outputs of the gut microbiome, rather than taxonomic composition alone, may play a key role in modulating immune dysregulation in RA, although the cross-sectional design precludes causal inference [96].
3.1. Segmented Filamentous Bacteria
Segmented filamentous bacteria (SFB) are spore-forming Gram-positive commensal bacteria most closely related to the genus Clostridium which colonize the ileum of the small intestine of numerous species, including humans [97]. It was shown that they are capable of inducing CD4+ T helper cells which results in upregulation of IL-17+Th17 cells in mice. Thus colonization with SFB may trigger inflammatory processes and contribute to pathogenesis of autoimmune diseases [98]. This mechanism was confirmed in the K/BxN mouse model of autoimmune arthritis, where emergence of SFB was enough to activate arthritis [99,100].
3.2. Prevotella
Prevotella species are anaerobic Gram-negative bacteria considered commensal due to their abundant colonization of healthy human body and their infrequent involvement in infection. However, increased prevalence of Prevotella species has been identified in many chronic inflammatory diseases, such as bacterial vaginosis, metabolic disorders, low-grade systemic inflammation and rheumatoid arthritis [101].
Prevotella copri has been shown to be increased in stool samples from patients with new-onset RA (NORA) in comparison with patients with chronic, treated RA (CRA), psoriatic arthritis, or healthy controls. Overgrowth of P. copri correlated with a reduction in Bacteroides and in beneficial microbes in NORA patients [102]. Scher et al. indicate that lower prevalence of Prevotella in CRA than NORA may be caused by decreased inflammation and disease activity. DAS28 was slightly lower in CRA patients but difference in CRP level was more significant. Thus, authors speculate on microbial modulating properties of CRP itself and emphasize the importance of future research on this subject.
Alpizar-Rodriguez et al. compared microbiome composition in 50 first-degree relatives (FDRs) of patients with RA (FDR controls) and 83 patients in pre-clinical RA stages. Significant differences were found, especially enrichment of Prevotella spp. in individuals at risk for RA compared with controls [103].
Immune relevance of Prevotella copri in patients with RA has been proved recently. 32% of RA patients were found to have serum IgA or IgG antibodies specific for P. copri, whereas in healthy controls and patients with other arthritic diseases these specific antibodies were almost absent. Moreover antibodies to the gut commensals Bacteroides fragilis and Escherichia coli were predominantly absent in all patients and healthy controls. The study demonstrates that the immune responses to P. copri may develop in RA patients and may be involved in disease pathogenesis or progression in some patients [104].
However, Marietta et al. showed that Prevotella histicola may have protective influence. HLA-DQ8 mice treated with P. histicola displayed significantly reduced incidence and severity of arthritis in comparison with controls. As a consequence of treatment with P. histicola increased expression of enzymes required to produce antimicrobial peptides and of tight junctions proteins (zonula occludens 1 and occludin) was observed, which resulted in lower gut permeability. Authors ascribed immunomodulating properties to this species and indicated that it can be further explored as a therapy for RA [105]. Prevotella consists of over 40 different species with high genetic diversity which presumably explains this conflicting data concerning RA.
3.3. Subdoligranulum
Recent evidence suggests a context-dependent role of Subdoligranulum in rheumatoid arthritis, spanning both potentially arthritogenic and immunoregulatory mechanisms. Using clonal IgA and IgG autoantibodies derived from individuals at risk for RA, one study identified a specific strain of Subdoligranulum that was selectively targeted by autoreactive antibodies and promoted inflammatory arthritis in gnotobiotic mouse models, supporting a possible role in early immune priming and loss of tolerance [106].
In contrast, a recent multi-omics Mendelian randomization study combined with in vitro validation demonstrated that Subdoligranulum variabile exerted anti-inflammatory effects by inducing tumor necrosis factor–stimulated gene 6 (TSG-6) expression in joint cells, leading to reduced TNF-α production and attenuation of inflammatory responses [107].
Together, these findings highlight marked strain-level heterogeneity within the genus Subdoligranulum and suggest that its role in RA may depend on microbial functional properties, host immune context, and disease stage rather than taxonomic presence alone.
3.4. Fusobacterium nucleatum
Experimental evidence implicates Fusobacterium nucleatum as a potential pro-inflammatory contributor to rheumatoid arthritis pathogenesis. In a mechanistic study combining human samples and murine models, F. nucleatum–derived outer membrane vesicles containing the adhesin FadA were shown to aggravate inflammatory arthritis by promoting macrophage activation and increasing the production of pro-inflammatory cytokines, including TNF-α and IL-6. FadA-mediated signaling enhanced intestinal permeability and facilitated systemic dissemination of inflammatory stimuli, thereby amplifying joint inflammation. Although primarily based on experimental models, these findings support a role for specific bacterial virulence factors, rather than overall bacterial abundance, in linking gut dysbiosis to immune activation in RA [108].
4. Probiotics in Rheumatoid Arthritis
Probiotics are viable microorganisms with great health potential and various beneficial effects on gut microbial balance, gut permeability, immune system and other human body function. Their efficacy has been assessed especially in inflammatory diseases and gastrointestinal disorders. Impact of probiotic supplementation has also been studied in RA. Lactobacillus supplementation was the most extensively examined. In one study patients with RA received Lactobacillus rhamnosus GG or placebo for 12 months. There were no significant differences in the activity of RA evaluated by clinical examination, HAQ index, and laboratory tests such as ESR, CRP, pro- and anti-inflammatory cytokines. However, more patients in the Lactobacillus group felt subjectively better. Also the reduction in the mean number of tender and swollen joints was greater in the Lactobacillus group (from 8.3 to 4.6) in comparison to the placebo group (from 5.5 to 4.8) [109].
Another study evaluated influence of Lactobacillus casei 01 supplementation on women with RA. For 8 weeks 22 patients in the first group received daily 108 colony forming units (CFU) of L. casei 01 and 24 patients in another group received placebo. Probiotic supplementation resulted in decrease of serum high-sensitivity C-reactive protein (hs-CRP) levels, tender and swollen joint counts, global health (GH) score and DAS28. Moreover, there were significant differences in IL-10, IL-12 and TNF-α level. The level of regulatory cytokine IL-10 was increased due to L. casei 01 supplementation, whereas levels of pro-inflammatory IL-12 and TNF-α were decreased [110].
Vaghef-Mehrabany E. et al. also assessed effects of Lactobacillus casei 01 supplementation in RA patients and received similar results. After 8 weeks of receiving probiotic capsules patients exhibited significant decrease in DAS28 and serum pro-inflammatory cytokines (IL-6, IL-12 and TNF-α), whereas IL-10 level raised when compared to placebo group [111].
Zamani et al. in their randomized, double-blind, placebo-controlled trial used capsules with mixture of three probiotic strains: Lactobacillus acidophilus, Lactobacillus casei and Bifidobacterium bifidum. 30 patients received probiotic capsules and other 30 received placebo for 8 weeks. After the intervention the probiotic group displayed improved DAS-28, decreased serum insulin levels and serum high-sensitivity C-reactive protein (hs-CRP) concentrations in comparison to the placebo group [112].
Three months of supplementation with Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 didn’t result in clinical improvement of RA as measured by the ACR20. Moreover, changes in cytokine levels were more beneficial in the placebo group [113].
Mixture containing (109 CFU/g) of each five strains Lactobacillus acidophilus LA-14, Lactobacillus casei LC-11, Lactococcus lactis LL-23, Bifidobacterium lactis BL-04 and Bifidobacterium bifidum BB-06 was taken for 60 days by RA patients in Cannarella et al. research. 21 patients supplemented probiotics, 21 were in placebo group. After 60 days white blood cell counts, tumor necrosis factor alpha (TNF-α), and interleukin 6 (IL-6) plasma levels were significantly reduced in the probiotic group. Also oxidative/nitrosative profile was improved - nitric oxide metabolites were lower, whereas sulfhydryl group and total radical-trapping antioxidant parameter were higher [114].
More recently, the potential role of probiotics as an adjunct to pharmacological treatment has been evaluated in patients with early rheumatoid arthritis. In a randomized, placebo-controlled trial including 100 patients with newly diagnosed RA, adjunctive supplementation with a multi-strain probiotic preparation (Lactobacillus casei BLn2401, Lactobacillus salivarius BL2201 and Bifidobacterium breve BL3406) in combination with conventional synthetic DMARDs resulted in faster and more sustained reductions in disease activity (DAS28), CRP, ESR, pain and functional disability over a 12-month follow-up compared with DMARD therapy alone. Probiotic supplementation was identified as an independent predictor of achieving remission or low disease activity, and was additionally associated with improved quality of life and reduced corticosteroid use. However, as gut microbiota composition was not directly assessed, the mechanistic link between probiotic intake and immunomodulation in RA remains to be elucidated [115].
5. Prebiotics and Synbiotics in Rheumatoid Arthritis
Beyond probiotics, increasing attention has been given to prebiotics and synbiotics as strategies aimed at modulating gut microbiota function rather than introducing exogenous bacterial strains. In a randomized, double-blind, placebo-controlled trial including 60 patients with rheumatoid arthritis, supplementation with a synbiotic preparation containing Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium bifidum and inulin for 8 weeks resulted in significant improvements in DAS28, serum hs-CRP, insulin resistance indices, and lipid profile compared with placebo [116].
Similarly, in a randomized controlled trial of 50 patients with RA, daily supplementation with inulin for 8 weeks led to significant reductions in disease activity, pain, morning stiffness, and serum inflammatory markers, alongside improvements in quality of life. Notably, both interventions exerted clinical and biochemical benefits despite the absence of direct microbiome sequencing, suggesting that enhancement of microbial metabolic activity - potentially via increased short-chain fatty acid production and improved gut barrier function - may contribute to immune modulation in RA. However, the relatively short intervention periods and limited mechanistic data warrant cautious interpretation of these findings and highlight the need for integrative studies combining clinical outcomes with microbiome and metabolomic analyses [117].
6. Diet and Gut Microbiome in Rheumatoid Arthritis
Microbiome composition depends on various factors, such as age, genetics and diet. Indeed, dietary patterns, consumed nutrients, amount and type of fat, fiber, food additives and many other have important influence on gut microbiota condition. Current evidence indicates that dietary patterns effective in alleviating RA symptoms are particularly beneficial for microbiota composition. Hence, modification of habitual diet may be an important part of RA treatment. Scientists are currently searching for particular relationship between gut bacteria, diet and health and trying to establish beneficial composition of microbiota. In one study long-term dietary pattern based on carbohydrates was associated with Prevotella, whereas higher consumption of protein and animal fat correlated with enterotype with predominance of Bacteroides [84].
6.1. Mediterranean Diet
Mediterranean diet abounds in high fibre foods such as vegetables, fruit, legumes and whole grains. Beneficial impact of this dietary pattern on gut microbiota can be attributed to the high carbohydrate, fibre, unsaturated fat and antioxidant content. Firmicutes and Bacteroidetes bacteria metabolize fiber into short chain fatty acids (SCFA) which have beneficial impact on intestinal barrier structure. Particularly the butyrate increases TJ protein expression and transepithelial electrical resistance (TER). This might explain amelioration of RA in patients implementing MD pattern.
Mitsou EK et al. described correlation of MD with gut microbiota composition, SCFA production and gastrointestinal symptoms in healthy individuals. Participants with higher adherence to MD displayed decreased Escherichia coli level, higher Bifidobacteria: E. coli ratio, increased levels and prevalence of Candida albicans. Bifidobacteria: E. coli ratio indicates gut microbiota equilibrium and overall health. Long-term diets abound in polysaccharides have been connected with reduction in Enterobacteriaceae (Shigella and Escherichia). The growth of E. coli strains may also be inhibited by dietary antioxidants. However, authors didn’t observe previously reported associations of MD or plant-based dietary patterns with Prevotella or Prevotella:Bacteroides ratio [118].
6.2. Vegan and Vegetarian Diets
Vegan and vegetarian diets as well as MD increase health and diminish disease risk by modulating microbiota. Zimmer et al. reported significant differences in the microbiota of long-term vegans, vegetarians and omnivores as controls. There were no differences in the total microbial counts between the groups. Vegans exhibited decreased counts of Bacteroides spp., Bifidobacterium spp., E. coli, and Enterobacteriaceae spp. However, it is worth noting, that the analyses were conducted with classical microbiological culture techniques. Since the majority of faecal bacteria cannot be cultured, these techniques don’t enable detecting all of them [119].
In more recent study subjects habitually following omnivore, vegetarian or vegan diets were compared, their adherence to MD, gut microbiota and metabolome were assessed. Diets rich in various vegetables were associated with faecal SCFA, and fibre degrading Firmicutes and Bacteroidetes. Lower adherence to MD resulted in higher urinary trimethylamine oxide (TMAO) levels, which is a potential risk factor for cardiovascular disease [120].
Few studies demonstrated changes in microbiota of RA patients after implementing plant-based diet. Shift from omnivorous to vegan diet resulted in alterations of microbiota detected by gas-liquid chromatography of bacterial cellular fatty acids. 53 patients with active RA were randomized into two groups. First group was subjected to 7-10 days of fast prior to 3,5 months of vegan diet and then 9 months of lactovegetarian diet. The control group continued the omnivorous diet. Significant differences in fatty acids profile were observed in the experimental group between the baseline samples and the samples from later time points and between samples from 1 month (vegan diet) and from samples taken at 7, 10, 13 months (lactovegetarian diet). Scientists also revealed association between intestinal bacteria and clinical improvement of RA [121].
Peltonen et al. further studied impact of raw vegan diet on microbiota of RA patients. Again, significant modifications of microbiota were observed in the vegan group after 1 month of intervention. Changes in faecal bacteria corresponded with improvement in RA activity [122].
6.3. Gluten-Free Diet
Gluten-free diet (GFD) is another dietary regimen which has been researched in terms of its impact on gut microbiota. It has been evaluated predominantly in patients with celiac disease and non-celiac gluten sensitivity. However, as it’s becoming more and more popular, a need for investigating it in healthy people emerged. There are no such studies conducted in patients with RA. The majority of studies demonstrated detrimental effect of GFD on composition of gut microbiota. After 1 month of GFD in 10 healthy subjects, a reduction in beneficial bacteria was observed. Particularly proportions of Bifidobacterium, Clostridium lituseburense and Faecalibacterium prausnitzii decreased, as analysed by fluorescence in situ hybridisation (FISH). qPCR analysis revealed reduction in Bifidobacterium, Lactobacillus and Bifidobacterium longum counts and increase in Enterobacteriaceae and Escherichia coli counts [123].
Similar study with 21 healthy individuals following GFD for 4 weeks also demonstrated moderate but significant differences in microbiota due to gluten elimination. The strongest effect was seen in the reduction of Veillonellaceae, family of bacteria which is considered proinflammatory. Ruminococcus bromii, and Roseburia faecis were also decreased, whereas Victivallaceae, Clostridiaceae, ML615J-28, Slackia, and Coriobacteriaceae increased on GFD. The Slackia genus, its family Coriobacteriaceae, and the family Clostridiaceae have been formerly associated with gastrointestinal diseases such as inflammatory bowel disease and celiac disease [124].
6.4. Dietary Timing
Recent evidence suggests that not only dietary composition, but also dietary timing, may influence gut microbiota–host interactions in rheumatoid arthritis. In an interventional study, time-restricted feeding was shown to modulate diurnal oscillations of gut microbiota and microbial metabolites, which were closely aligned with circadian rhythms of inflammatory markers in patients with RA. Disruption of normal feeding–fasting cycles was associated with blunted microbial rhythmicity and increased inflammatory activity, whereas restoration of regular meal timing partially normalized microbiota oscillations and inflammatory profiles. These findings indicate that dietary effects on the gut microbiome in RA may depend not only on nutrient quality, but also on temporal patterns of food intake, adding an additional layer of complexity to diet–microbiome interactions in inflammatory disease [125].
7. Conclusions
Dietary and lifestyle changes can be a powerful addition to conventional therapy and promising tools for preventing RA. Smoking, physical activity, diet and gut microbiota are listed among factors with the greatest impact on severity and risk of developing RA. Particularly diet and microbiome composition need extensive research since current evidence seems to be insufficient or contradictory. Recent studies further indicate that the gut microbiome may not only reflect disease status, but also influence inflammatory burden and response to treatment. It has been shown that specific compounds and supplements especially omega-3 fatty acids and vitamin D, as well as whole dietary regimens such as Meditterranean diet or vegan diet may be beneficial in managing RA symptoms. In several studies omega-3 supplementation resulted in decreased intake of NSAID or improvement in some symptoms such as morning stiffness and joint tenderness. It has also been shown that vitamin D level might be inversely associated with RA activity parameters, such as DAS28. Following Meditterranean diet or vegan diet might lead to reduction of inflammation and alleviate some symptoms of disease. However, there are only few studies, with small groups of patients, some of them consisting only of women or even without a control group, which limits the generalizability of the observed effects.
Available studies suggest that gut microbiota of RA patients changes in the course of disease and in response to treatment. RA patients display diminished gut microbial diversity, which might correlate with disease duration and autoantibody levels. Beyond taxonomic alterations, emerging evidence highlights the importance of functional features of the gut microbiome, including microbial metabolites, intestinal barrier integrity and translocation of bacterial components, which may contribute to immune activation in RA. According to current evidence there is an inseparable connection between diet composition and gut microbiota. Therefore, modification of gut microbiome through dietary interventions or probiotics supplementation may become an essential part of RA therapy. Beneficial impact of Meditterranean diet or plant-based diet on gut microbiome has already been demonstrated. Some studies also exhibited anti-inflammatory properties of probiotic supplementation in RA, particularly probiotics comprising Lactobacillus strains. Prebiotics and synbiotics have also shown modest but promising effects on disease activity and inflammatory markers in RA, although mechanistic data linking these interventions to specific microbiome changes remain limited. Furthermore, recent findings suggest that temporal aspects of diet, such as meal timing, may modulate gut microbial rhythmicity and inflammatory responses, adding another layer of complexity to diet–microbiome interactions in RA. Thus, mutual dependencies of diet, microbiome and RA activity or risk should be subjected to further comprehensive research..
Abbreviations.
The following abbreviations are used in this manuscript:
| AA ACPA ACR AID CAT CCP CDAI CRP DAS28 DHA DMARD EMS EPA ESR GPx HAQ HAQ-DI hs-CRP IFNα IL-1 IL-1β IL-6 IL-9 IL-12 IL-17 IL-23 LF-HC MD MDA mHAQ NSAID |
arachidonic acid anti-citrullinated protein autoantibody American College of Rheumatology response criteria anti-inflammatory diet catalase cyclic citrullinated peptide Clinical Disease Activity Indice C-reactive protein 28 joint count Disease Activity Score docosahexaenoic acid disease-modifying anti-rheumatic drugs early morning stiffness eicosapentaenoic acid erythrocyte sedimentation rate glutathione peroxidase Health Assessment Questionnaire Health Assessment Questionnaire Disability Index high-sensitivity C-reactive protein interferon α interleukin 1 interleukin 1β interleukin 6 interleukin 9 interleukin 12 interleukin 17 interleukin 23 low-fat high-carbohydrate Mediterranean diet malonedialdehyde modified Health Assessment Questionnaire nonsteroidal anti-inflammatory drugs |
| PCBs RA RAI RAI1 RF SDAI SF-36 SOD |
polychlorinated biphenyls rheumatoid arthritis Ritchie’s articular index relative activity index rheumatoid factor Simplified Disease Activity Indice short form-36 health survey superoxide dismutase |
| TGFβ1 Th17 t.i.d. TNF-α Treg |
transforming growth factor β1 T helper 17 three times a day tumor necrosis factor α regulatory T cells |
| VAS vdHS WBC |
visual analog scale van der Heijde-Sharp white blood cells |
Author Contributions
Conceptualization, E.B.; resources, A.R., E.B.; writing—original draft preparation, A.R.; writing—review and editing, A.R., E.B..; visualization, A.R.; supervision, E.B.; funding acquisition, E.B. All authors have read and agreed to the published version of the manuscript.
Funding
The present review was funded by Statutory Funds of the Medical University of Gdańsk nr 01-10026/0010451/01/262/0/2026.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.:.
References
- Scott, DL; Wolfe, F; Huizinga, TWJ. Rheumatoid arthritis. Lancet 2010, 376, 1094–108. [Google Scholar] [CrossRef]
- Van Der Woude, D; Houwing-Duistermaat, JJ; Toes, REM; et al. Quantitative heritability of anti-citrullinated protein antibody-positive and anti-citrullinated protein antibody-negative rheumatoid arthritis. Arthritis Rheum. 2009, 60, 916–923. [Google Scholar] [CrossRef]
- Sokka, T; Hakkinen, A; Kautiainen, H; et al. Physical inactivity in patients with rheumatoid arthritis: data from twenty-one countries in a cross-sectional, international study. Arthritis Rheum. 2008, 59, 42–50. [Google Scholar] [CrossRef]
- Ajeganova, S; Andersson, ML; Hafstrom, I. Association of obesity with worse disease severity in rheumatoid arthritis as well as with comorbidities: a long-term followup from disease onset. Arthritis Care Res. (Hoboken) 2013, 65, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Kupczyk, D; Bilski, R; Szeleszczuk, Ł; et al. The Role of Diet in Modulating Inflammation and Oxidative Stress in Rheumatoid Arthritis, Ankylosing Spondylitis, and Psoriatic Arthritis. Nutrients 2025, 17(9), 1603. [Google Scholar] [CrossRef]
- Arnson, Y; Amital, H; Shoenfeld, Y. Vitamin D and autoimmunity: new aetiological and therapeutic considerations. Ann. Rheum. Dis. 2007, 66, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Song, GG; Bae, S-C; Lee, YH. Association between vitamin D intake and the risk of rheumatoid arthritis: a meta-analysis. Clin. Rheumatol. 2012, 31, 1733–1739. [Google Scholar] [CrossRef] [PubMed]
- Lee, YH; Bae, S-C. Vitamin D level in rheumatoid arthritis and its correlation with the disease activity: a meta-analysis. Clin. Exp. Rheumatol. 2016, 34, 827–833. [Google Scholar]
- Lin, J; Liu, J; Davies, ML; et al. Serum Vitamin D Level and Rheumatoid Arthritis Disease Activity: Review and Meta-Analysis. PLoS One 2016, 11(1), e0146351. [Google Scholar] [CrossRef]
- Craig, SM; Yu, F; Curtis, JR; et al. Vitamin D status and its associations with disease activity and severity in African Americans with recent-onset rheumatoid arthritis. J. Rheumatol. 2010, 37, 275–281. [Google Scholar] [CrossRef]
- Baker, JF; Baker, DG; Toedter, G; et al. Associations between vitamin D, disease activity, and clinical response to therapy in rheumatoid arthritis. Clin. Exp. Rheumatol. 2012, 30, 658–664. [Google Scholar]
- Matsumoto, Y; Sugioka, Y; Tada, M; et al. Relationships between serum 25-hydroxycalciferol, vitamin D intake and disease activity in patients with rheumatoid arthritis--TOMORROW study. Mod. Rheumatol. 2015, 25, 246–250. [Google Scholar] [CrossRef]
- Polasik, K; Piotrowska, E; Lipinska, B; et al. Vitamin D status in patients with rheumatoid arthritis: a correlation analysis with disease activity and progression, as well as serum IL-6 levels. Acta Biochim. Pol. 2017, 64, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Jelsness-Jørgensen, LP; Grøvle, L; Haugen, AJ. Association between Vitamin D and fatigue in patients with rheumatoid arthritis: A cross-sectional study. BMJ Open 2020, 10, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekara, S; Patted, A. Role of vitamin D supplementation in improving disease activity in rheumatoid arthritis: An exploratory study. Int. J. Rheum. Dis. 2017, 20, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Buondonno, I; Rovera, G; Sassi, F; et al. Vitamin D and immunomodulation in early rheumatoid arthritis: A randomized doubleblind placebo-controlled study. PLoS One 2017, 12, 1–18. [Google Scholar] [CrossRef]
- El-Banna, HS; Gado, SE. Vitamin D: does it help Tregs in active rheumatoid arthritis patients. Expert Rev. Clin. Immunol. 2020, 16, 847–853. [Google Scholar] [CrossRef]
- Sofi, F; Macchi, C; Abbate, R; et al. Mediterranean diet and health. Biofactors 2013, 39, 335–342. [Google Scholar] [CrossRef]
- Sköldstam, L; Hagfors, L; Johansson, G. An experimental study of a Mediterranean diet intervention for patients with rheumatoid arthritis. Ann. Rheum. Dis. 2003, 62, 208–214. [Google Scholar] [CrossRef]
- McKellar, G; Morrison, E; McEntegart, A; et al. A pilot study of a Mediterranean-type diet intervention in female patients with rheumatoid arthritis living in areas of social deprivation in Glasgow. Ann. Rheum. Dis. 2007, 66, 1239–1243. [Google Scholar] [CrossRef] [PubMed]
- García-Morales, JM; Lozada-Mellado, M; Hinojosa-Azaola, A; et al. Effect of a Dynamic Exercise Program in Combination With Mediterranean Diet on Quality of Life in Women With Rheumatoid Arthritis. J. Clin. Rheumatol. 2020, 26, S116–S122. [Google Scholar] [CrossRef]
- Papandreou, P; Gioxari, A; Daskalou, E; et al. Mediterranean Diet and Physical Activity Nudges versus Usual Care in Women with Rheumatoid Arthritis: Results from the MADEIRA Randomized Controlled Trial. Nutrients 2023, 15(3), 676. [Google Scholar] [CrossRef]
- Raad, T; George, E; Griffin, A; et al. Effects of a telehealth-delivered Mediterranean diet intervention in adults with Rheumatoid Arthritis (MEDRA): a randomised controlled trial. BMC Musculoskelet. Disord. 2024, 25(1), 631. [Google Scholar] [CrossRef]
- Sadeghi, A; Tabatabaiee, M; Mousavi, MA; et al. Dietary Pattern or Weight Loss: Which One Is More Important to Reduce Disease Activity Score in Patients with Rheumatoid Arthritis? A Randomized Feeding Trial. Int. J. Clin. Pract. 2022, 6004916. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y; Costenbader, KH; Gao, X; et al. Mediterranean diet and incidence of rheumatoid arthritis in women. Arthritis Care Res. (Hoboken) 2015, 67, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Sundstrom, B; Johansson, I; Rantapaa-Dahlqvist, S. Diet and alcohol as risk factors for rheumatoid arthritis: a nested case-control study. Rheumatol. Int. 2015, 35, 533–539. [Google Scholar] [CrossRef]
- Nguyen, Y; Salliot, C; Gelot, A; et al. Mediterranean Diet and Risk of Rheumatoid Arthritis: Findings From the French E3N-EPIC Cohort Study. Arthritis and Rheumatology 2021, 73, 69–77. [Google Scholar] [CrossRef]
- Matsumoto, Y; Sugioka, Y; Tada, M; et al. Monounsaturated fatty acids might be key factors in the Mediterranean diet that suppress rheumatoid arthritis disease activity: The TOMORROW study. Clin. Nutr. 2018, 37, 675–680. [Google Scholar] [CrossRef]
- Barbalace, MC; Talotta, R; Rapisarda, F; et al. Unlocking the Power of the Mediterranean Diet: Two in One—Dual Benefits for Rheumatic and Thyroid Autoimmune Diseases. Nutrients 2025, 17(8), 1383. [Google Scholar] [CrossRef]
- Papanikolaou, Y; Brooks, J; Reider, C; et al. U.S. adults are not meeting recommended levels for fish and omega-3 fatty acid intake: results of an analysis using observational data from NHANES 2003-2008. Nutr. J. 2014, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Burdge, GC; Calder, PC. Conversion of alpha-linolenic acid to longer-chain polyunsaturated fatty acids in human adults. Reprod. Nutr. Dev. 2005, 45, 581–597. [Google Scholar] [CrossRef]
- Adam, O; Beringer, C; Kless, T; et al. Anti-inflammatory effects of a low arachidonic acid diet and fish oil in patients with rheumatoid arthritis. Rheumatol. Int. 2003, 23, 27–36. [Google Scholar] [CrossRef]
- Nielsen, GL; Faarvang, KL; Thomsen, BS; et al. The effects of dietary supplementation with n-3 polyunsaturated fatty acids in patients with rheumatoid arthritis: a randomized, double blind trial. Eur. J. Clin. Invest. 1992, 22, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Skoldstam, L; Borjesson, O; Kjallman, A; et al. Effect of six months of fish oil supplementation in stable rheumatoid arthritis. A double-blind, controlled study. Scand. J. Rheumatol. 1992, 21, 178–185. [Google Scholar] [CrossRef]
- Lau, CS; Morley, KD; Belch, JJ. Effects of fish oil supplementation on non-steroidal anti-inflammatory drug requirement in patients with mild rheumatoid arthritis--a double-blind placebo controlled study. Br. J. Rheumatol. 1993, 32, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Proudman, SM; James, MJ; Spargo, LD; et al. Fish oil in recent onset rheumatoid arthritis: a randomised, double-blind controlled trial within algorithm-based drug use. Ann. Rheum. Dis. 2015, 74, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, RJ; Katz, J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain 2007, 129, 210–223. [Google Scholar] [CrossRef]
- Lee, Y-H; Bae, S-C; Song, G-G. Omega-3 polyunsaturated fatty acids and the treatment of rheumatoid arthritis: a meta-analysis. Arch. Med. Res. 2012, 43, 356–362. [Google Scholar] [CrossRef]
- Gioxari, A; Kaliora, AC; Marantidou, F; et al. Intake of omega-3 polyunsaturated fatty acids in patients with rheumatoid arthritis: A systematic review and meta-analysis. Nutrition 2018, 45, 114–124.e4. [Google Scholar] [CrossRef]
- Ghaseminasab-Parizi, M; Nazarinia, MA; Akhlaghi, M. The effect of flaxseed with or without anti-inflammatory diet in patients with rheumatoid arthritis, a randomized controlled trial. Eur. J. Nutr. 2022, 61, 1377–1389. [Google Scholar] [CrossRef]
- Tedeschi, SK; Bathon, JM; Giles, JT; et al. Relationship Between Fish Consumption and Disease Activity in Rheumatoid Arthritis. Arthritis Care Res. (Hoboken) 2018, 70, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Hulander, E; Bärebring, L; Winkvist, A; et al. A randomized controlled cross-over trial investigating the acute inflammatory and metabolic response after meals based on red meat, fatty fish, or soy protein: the postprandial inflammation in rheumatoid arthritis (PIRA) trial. Eur. J. Nutr. 2024, 63, 2631–2642. [Google Scholar] [CrossRef]
- Lindqvist, HM; Hulander, E; Bärebring, L; et al. A randomized controlled cross-over trial of differences in acute effects on serum metabolites from isocaloric meals based on red meat, fatty fish, or soy protein. Eur. J. Nutr. 2025, 64(5), 187. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, D; Crippa, A; Orsini, N; et al. Fish consumption and risk of rheumatoid arthritis: a dose-response meta-analysis. Arthritis Res. Ther. 2014, 16, 446. [Google Scholar] [CrossRef]
- Lee, D-H; Steffes, M; Jacobs, DR. Positive associations of serum concentration of polychlorinated biphenyls or organochlorine pesticides with self-reported arthritis, especially rheumatoid type, in women. Environ. Health Perspect. 2007, 115, 883–888. [Google Scholar] [CrossRef]
- Di Giuseppe, D; Wallin, A; Bottai, M; et al. Long-term intake of dietary long-chain n-3 polyunsaturated fatty acids and risk of rheumatoid arthritis: a prospective cohort study of women. Ann. Rheum. Dis. 2014, 73, 1949–1953. [Google Scholar] [CrossRef]
- Shapiro, JA; Koepsell, TD; Voigt, LF; et al. Diet and rheumatoid arthritis in women: a possible protective effect of fish consumption. Epidemiology 1996, 7, 256–263. [Google Scholar] [CrossRef]
- Sparks, JA; O’Reilly, ÉJ; Barbhaiya, M; et al. Association of fish intake and smoking with risk of rheumatoid arthritis and age of onset: a prospective cohort study. BMC Musculoskelet. Disord. 2019, 20, 2. [Google Scholar] [CrossRef]
- McDougall, J; Bruce, B; Spiller, G; et al. Effects of a very low-fat, vegan diet in subjects with rheumatoid arthritis. J. Altern. Complement. Med. 2002, 8, 71–75. [Google Scholar] [CrossRef]
- Walrabenstein, W; Wagenaar, CA; Van Der Leeden, M; et al. A multidisciplinary lifestyle program for rheumatoid arthritis: The ‘Plants for Joints’ randomized controlled trial. Rheumatology 2023, 62, 2683–2691. [Google Scholar] [CrossRef] [PubMed]
- Hanninen; Kaartinen, K; Rauma, AL; et al. Antioxidants in vegan diet and rheumatic disorders. Toxicology 2000, 155, 45–53. [Google Scholar] [CrossRef]
- Rauma, AL; Nenonen, M; Helve, T; et al. Effect of a strict vegan diet on energy and nutrient intakes by Finnish rheumatoid patients. Eur. J. Clin. Nutr. 1993, 47, 747–749. [Google Scholar]
- Hafstrom, I; Ringertz, B; Spangberg, A; et al. A vegan diet free of gluten improves the signs and symptoms of rheumatoid arthritis: the effects on arthritis correlate with a reduction in antibodies to food antigens. Rheumatology (Oxford) 2001, 40, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Elkan, A-C; Sjoberg, B; Kolsrud, B; et al. Gluten-free vegan diet induces decreased LDL and oxidized LDL levels and raised atheroprotective natural antibodies against phosphorylcholine in patients with rheumatoid arthritis: a randomized study. Arthritis Res. Ther. 2008, 10, R34. [Google Scholar] [CrossRef]
- Gregersen, L; Jessen, PD; Lund, HW; et al. Impact of gluten intake on clinical outcomes in patients with chronic inflammatory diseases initiating biologics: Secondary analysis of the prospective multicentre BELIEVE cohort study. Scand. J. Immunol. 2024, 100(6), e13409. [Google Scholar] [CrossRef]
- Khanna, S; Jaiswal, KS; Gupta, B. Managing Rheumatoid Arthritis with Dietary Interventions. Front. Nutr. 2017, 4, 52. [Google Scholar] [CrossRef]
- Kjeldsen-Kragh, J; Haugen, M; Borchgrevink, CF; et al. Controlled trial of fasting and one-year vegetarian diet in rheumatoid arthritis. Lancet 1991, 338, 899–902. [Google Scholar] [CrossRef]
- Fraser, DA; Thoen, J; Djoseland, O; et al. Serum levels of interleukin-6 and dehydroepiandrosterone sulphate in response to either fasting or a ketogenic diet in rheumatoid arthritis patients. Clin. Exp. Rheumatol. 2000, 18, 357–362. [Google Scholar] [PubMed]
- Hartmann, AM; D’Urso, M; Dell’Oro, M; et al. Post Hoc Analysis of a Randomized Controlled Trial on Fasting and Plant-Based Diet in Rheumatoid Arthritis (NutriFast): Nutritional Supply and Impact on Dietary Behavior. Nutrients 2023, 15(4), 851. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, A; Akhgarjand, C; Ansar, H; et al. The effects of intermittent fasting on antioxidant and inflammatory markers and liver enzymes in postmenopausal, overweight and obese women with rheumatoid arthritis: a randomized controlled trial. Sci. Rep. 2025, 15(1), 2357. [Google Scholar] [CrossRef]
- Ranjbar, M; Shab-Bidar, S; Rostamian, A; et al. Effects of intermittent fasting diet in overweight and obese postmenopausal women with rheumatoid arthritis: A randomized controlled clinical trial. Complement. Ther. Med. 2025, 91, 103189. [Google Scholar] [CrossRef]
- Peretz, A; Siderova, V; Neve, J. Selenium supplementation in rheumatoid arthritis investigated in a double blind, placebo-controlled trial. Scand. J. Rheumatol. 2001, 30, 208–212. [Google Scholar] [CrossRef]
- Meki, A-RMA; Hamed, EA; Ezam, KA. Effect of green tea extract and vitamin C on oxidant or antioxidant status of rheumatoid arthritis rat model. Indian J. Clin. Biochem. 2009, 24, 280–287. [Google Scholar] [CrossRef]
- Karlson, EW; Shadick, NA; Cook, NR; et al. Vitamin E in the primary prevention of rheumatoid arthritis: the Women’s Health Study. Arthritis Rheum. 2008, 59, 1589–1595. [Google Scholar] [CrossRef] [PubMed]
- Helmy, M; Shohayeb, M; Helmy, MH; et al. Antioxidants as adjuvant therapy in rheumatoid disease. A preliminary study. Arzneimittelforschung 2001, 51, 293–298. [Google Scholar] [CrossRef] [PubMed]
- van Vugt, RM; Rijken, PJ; Rietveld, AG; et al. Antioxidant intervention in rheumatoid arthritis: results of an open pilot study. Clin. Rheumatol. 2008, 27, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Jalili, M; Kolahi, S; Aref-Hosseini, S-R; et al. Beneficial role of antioxidants on clinical outcomes and erythrocyte antioxidant parameters in rheumatoid arthritis patients. Int. J. Prev. Med. 2014, 5, 835–840. [Google Scholar]
- Thimoteo, NSB; Iryioda, TMV; Alfieri, DF; et al. Cranberry juice decreases disease activity in women with rheumatoid arthritis. Nutrition 2019, 60, 112–117. [Google Scholar] [CrossRef]
- Fatel, ECS; Rosa, FT; Alfieri, DF; et al. Beneficial effects of fish oil and cranberry juice on disease activity and inflammatory biomarkers in people with rheumatoid arthritis. Nutrition 2021, 86, 111183. [Google Scholar] [CrossRef]
- Chandran, B; Goel, A. A randomized, pilot study to assess the efficacy and safety of curcumin in patients with active rheumatoid arthritis. Phytother. Res. 2012, 26, 1719–1725. [Google Scholar] [CrossRef]
- Amalraj, A; Varma, K; Jacob, J; et al. A Novel Highly Bioavailable Curcumin Formulation Improves Symptoms and Diagnostic Indicators in Rheumatoid Arthritis Patients: A Randomized, Double-Blind, Placebo-Controlled, Two-Dose, Three-Arm, and Parallel-Group Study. J. Med. Food 2017, 20, 1022–1030. [Google Scholar] [CrossRef]
- Westerlind, H; Palmqvist, I; Saevarsdottir, S; et al. Is tea consumption associated with reduction of risk of rheumatoid arthritis? A Swedish case-control study. Arthritis Res. Ther. 2021, 23, 1–8. [Google Scholar] [CrossRef]
- Vadell, AKE; Bärebring, L; Hulander, E; et al. Anti-inflammatory Diet in Rheumatoid Arthritis (ADIRA) - A randomized, controlled crossover trial indicating effects on disease activity. American Journal of Clinical Nutrition 2020, 111, 1203–1213. [Google Scholar] [CrossRef]
- Matsumoto, Y; Shivappa, N; Sugioka, Y; et al. Change in dietary inflammatory index score is associated with control of long-term rheumatoid arthritis disease activity in a Japanese cohort: the TOMORROW study. Arthritis Res. Ther. 2021, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kleinewietfeld, M; Manzel, A; Titze, J; et al. Sodium chloride drives autoimmune disease by the induction of pathogenic TH17 cells. Nature 2013, 496, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Wu, C; Yosef, N; Thalhamer, T; et al. Induction of pathogenic TH17 cells by inducible salt-sensing kinase SGK1. Nature 2013, 496, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Sundstrom, B; Johansson, I; Rantapaa-Dahlqvist, S. Interaction between dietary sodium and smoking increases the risk for rheumatoid arthritis: results from a nested case-control study. Rheumatology (Oxford) 2015, 54, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Salgado, E; Bes-Rastrollo, M; de Irala, J; et al. High Sodium Intake Is Associated With Self-Reported Rheumatoid Arthritis: A Cross Sectional and Case Control Analysis Within the SUN Cohort. Medicine 2015, 94, e924. [Google Scholar] [CrossRef] [PubMed]
- Marouen, S; du Cailar, G; Audo, R; et al. Sodium excretion is higher in patients with rheumatoid arthritis than in matched controls. PLoS One 2017, 12, e0186157. [Google Scholar] [CrossRef]
- Scrivo, R; Massaro, L; Barbati, C; et al. The role of dietary sodium intake on the modulation of T helper 17 cells and regulatory T cells in patients with rheumatoid arthritis and systemic lupus erythematosus. PLoS One 2017, 12, e0184449. [Google Scholar] [CrossRef]
- Mortier, C; Govindarajan, S; Venken, K; et al. It Takes ‘Guts’ to Cause Joint Inflammation: Role of Innate-Like T Cells. Front. Immunol. 2018, 9, 1489. [Google Scholar] [CrossRef]
- Guerreiro, CS; Calado, A; Sousa, J; et al. Diet, Microbiota, and Gut Permeability-The Unknown Triad in Rheumatoid Arthritis. Front. Med. (Lausanne) 2018, 5, 349. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, M; Raes, J; Pelletier, E; et al. Enterotypes of the human gut microbiome. Nature 2011, 473, 174–180. [Google Scholar] [CrossRef]
- Wu, GD; Chen, J; Hoffmann, C; et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef]
- Gorvitovskaia, A; Holmes, SP; Huse, SM. Interpreting Prevotella and Bacteroides as biomarkers of diet and lifestyle. Microbiome 2016, 4, 15. [Google Scholar] [CrossRef]
- Zhang, X; Zhang, D; Jia, H; et al. The oral and gut microbiomes are perturbed in rheumatoid arthritis and partly normalized after treatment. Nat. Med. 2015, 21, 895–905. [Google Scholar] [CrossRef]
- Vaahtovuo, J; Munukka, E; Korkeamaki, M; et al. Fecal microbiota in early rheumatoid arthritis. J. Rheumatol. 2008, 35, 1500–1505. [Google Scholar] [PubMed]
- Chen, J; Wright, K; Davis, JM; et al. An expansion of rare lineage intestinal microbes characterizes rheumatoid arthritis. Genome Med. 2016, 8, 43. [Google Scholar] [CrossRef]
- Ruiz-Limón, P; Mena-Vázquez, N; Moreno-Indias, I; et al. Collinsella is associated with cumulative inflammatory burden in an established rheumatoid arthritis cohort. Biomedicine and Pharmacotherapy 2022, 153, 113518. [Google Scholar] [CrossRef] [PubMed]
- Li, Y; Zhang, SX; Yin, XF; et al. The Gut Microbiota and Its Relevance to Peripheral Lymphocyte Subpopulations and Cytokines in Patients with Rheumatoid Arthritis. J. Immunol. Res. 2021. [Google Scholar] [CrossRef]
- Kitamura, K; Shionoya, H; Suzuki, S; et al. Oral and Intestinal Bacterial Substances Associated with Disease Activities in Patients with Rheumatoid Arthritis: A Cross-Sectional Clinical Study. J. Immunol. Res. 2022. [Google Scholar] [CrossRef]
- Koh, JH; Lee, EH; Cha, KH; et al. Factors associated with the composition of the gut microbiome in patients with established rheumatoid arthritis and its value for predicting treatment responses. Arthritis Res. Ther. 2023, 25(1), 32. [Google Scholar] [CrossRef]
- Danckert, NP; Freidin, MB; Granville Smith, I; et al. Treatment response in rheumatoid arthritis is predicted by the microbiome: a large observational study in UK DMARD-naive patients. Rheumatology 2024, 63, 3486–3495. [Google Scholar] [CrossRef]
- Wang, Q; Li, CL; Yu, SY; et al. A predictive model based on the gut microbiota improves the diagnostic effect in patients with rheumatoid arthritis. Rheumatology 2025, 64, 4014–4021. [Google Scholar] [CrossRef]
- Zeng, L; Yang, Q; Luo, Y; et al. The Gut Microbiota: Emerging Evidence in Autoimmune and Inflammatory Diseases. Research 2025, 9, 1097. [Google Scholar] [CrossRef] [PubMed]
- Yu, D; Du, J; Pu, X; et al. The Gut Microbiome and Metabolites Are Altered and Interrelated in Patients With Rheumatoid Arthritis. Front. Cell. Infect. Microbiol. 2022, 11, 763507. [Google Scholar] [CrossRef]
- Klaasen, HL; Koopman, JP; Van den Brink, ME; et al. Intestinal, segmented, filamentous bacteria in a wide range of vertebrate species. Lab. Anim. 1993, 27, 141–150. [Google Scholar] [CrossRef]
- Ivanov, II; Atarashi, K; Manel, N; et al. Induction of intestinal Th17 cells by segmented filamentous bacteria. Cell 2009, 139, 485–498. [Google Scholar] [CrossRef] [PubMed]
- Wu, H-J; Ivanov, II; Darce, J; et al. Gut-residing segmented filamentous bacteria drive autoimmune arthritis via T helper 17 cells. Immunity 2010, 32, 815–827. [Google Scholar] [CrossRef] [PubMed]
- Teng, F; Klinger, CN; Felix, KM; et al. Gut Microbiota Drive Autoimmune Arthritis by Promoting Differentiation and Migration of Peyer’s Patch T Follicular Helper Cells. Immunity 2016, 44, 875–888. [Google Scholar] [CrossRef]
- Larsen, JM. The immune response to Prevotella bacteria in chronic inflammatory disease. Immunology 2017, 151, 363–374. [Google Scholar] [CrossRef]
- Scher, JU; Sczesnak, A; Longman, RS; et al. Expansion of intestinal Prevotella copri correlates with enhanced susceptibility to arthritis. Elife 2013, 2, e01202. [Google Scholar] [CrossRef]
- Alpizar-Rodriguez, D; Lesker, TR; Gronow, A; et al. Prevotella copri in individuals at risk for rheumatoid arthritis. Ann. Rheum. Dis. 2019, 78, 590–593. [Google Scholar] [CrossRef]
- Pianta, A; Arvikar, S; Strle, K; et al. Evidence of the Immune Relevance of Prevotella copri, a Gut Microbe, in Patients With Rheumatoid Arthritis. Arthritis Rheumatol. 2017, 69, 964–975. [Google Scholar] [CrossRef]
- Marietta, E V; Murray, JA; Luckey, DH; et al. Suppression of Inflammatory Arthritis by Human Gut-Derived Prevotella histicola in Humanized Mice. Arthritis Rheumatol. 2016, 68, 2878–2888. [Google Scholar] [CrossRef]
- Chriswell, ME; Lefferts, AR; Clay, MR; et al. Clonal IgA and IgG autoantibodies from individuals at risk for rheumatoid arthritis identify an arthritogenic strain of Subdoligranulum. Sci. Transl. Med. 2022, 14(668), eabn5166. [Google Scholar] [CrossRef] [PubMed]
- Li, H; Dai, J; Zhao, C; et al. Gut Subdoligranulum variabile ameliorates rheumatoid arthritis by promoting TSG-6 synthesis from joint cells. Front. Immunol. 2024, 15, 1418717. [Google Scholar] [CrossRef] [PubMed]
- Hong, M; Li, Z; Liu, H; et al. Fusobacterium nucleatum aggravates rheumatoid arthritis through FadA-containing outer membrane vesicles. Cell Host Microbe 2023, 31, 798–810.e7. [Google Scholar] [CrossRef] [PubMed]
- Hatakka, K; Martio, J; Korpela, M; et al. Effects of probiotic therapy on the activity and activation of mild rheumatoid arthritis--a pilot study. Scand. J. Rheumatol. 2003, 32, 211–215. [Google Scholar] [CrossRef]
- Alipour, B; Homayouni-Rad, A; Vaghef-Mehrabany, E; et al. Effects of Lactobacillus casei supplementation on disease activity and inflammatory cytokines in rheumatoid arthritis patients: a randomized double-blind clinical trial. Int. J. Rheum. Dis. 2014, 17, 519–527. [Google Scholar] [CrossRef]
- Vaghef-Mehrabany, E; Alipour, B; Homayouni-Rad, A; et al. Probiotic supplementation improves inflammatory status in patients with rheumatoid arthritis. Nutrition 2014, 30, 430–435. [Google Scholar] [CrossRef]
- Zamani, B; Golkar, HR; Farshbaf, S; et al. Clinical and metabolic response to probiotic supplementation in patients with rheumatoid arthritis: a randomized, double-blind, placebo-controlled trial. Int. J. Rheum. Dis. 2016, 19, 869–879. [Google Scholar] [CrossRef]
- Pineda M de, LA; Thompson, SF; Summers, K; et al. A randomized, double-blinded, placebo-controlled pilot study of probiotics in active rheumatoid arthritis. Med. Sci. Monit. 2011, 17, CR347–54. [Google Scholar] [CrossRef]
- Cannarella, LAT; Mari, NL; Alcântara, CC; et al. Mixture of probiotics reduces inflammatory biomarkers and improves the oxidative/nitrosative profile in people with rheumatoid arthritis. Nutrition 2021, 89, 111282. [Google Scholar] [CrossRef]
- Barac, B; Lukovic, S; Kojic, T; et al. Therapeutical efficacy of immunobiotics in patients with newly diagnosed rheumatoid arthritis. J. Infect. Dev. Ctries. 2025, 19, 1861–1868. [Google Scholar] [CrossRef]
- Zamani, B; Farshbaf, S; Golkar, HR; et al. Synbiotic supplementation and the effects on clinical and metabolic responses in patients with rheumatoid arthritis: A randomised, double-blind, placebo-controlled trial. British Journal of Nutrition 2017, 117, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaeyan, A; Grigorian, A; Salesi, M; et al. Inulin supplementation improves some inflammatory indices, clinical outcomes, and quality of life in rheumatoid arthritis patients. Sci. Rep. 2025, 15(1), 30732. [Google Scholar] [CrossRef]
- Mitsou, EK; Kakali, A; Antonopoulou, S; et al. Adherence to the Mediterranean diet is associated with the gut microbiota pattern and gastrointestinal characteristics in an adult population. Br. J. Nutr. 2017, 117, 1645–1655. [Google Scholar] [CrossRef]
- Zimmer, J; Lange, B; Frick, J-S; et al. A vegan or vegetarian diet substantially alters the human colonic faecal microbiota. Eur. J. Clin. Nutr. 2012, 66, 53–60. [Google Scholar] [CrossRef] [PubMed]
- De Filippis, F; Pellegrini, N; Vannini, L; et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut 2016, 65, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Peltonen, R; Kjeldsen-Kragh, J; Haugen, M; et al. Changes of faecal flora in rheumatoid arthritis during fasting and one-year vegetarian diet. Br. J. Rheumatol. 1994, 33, 638–643. [Google Scholar] [CrossRef]
- Peltonen, R; Nenonen, M; Helve, T; et al. Faecal microbial flora and disease activity in rheumatoid arthritis during a vegan diet. Br. J. Rheumatol. 1997, 36, 64–68. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G; Nadal, I; Collado, MC; et al. Effects of a gluten-free diet on gut microbiota and immune function in healthy adult human subjects. Br. J. Nutr. 2009, 102, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Bonder, MJ; Tigchelaar, EF; Cai, X; et al. The influence of a short-term gluten-free diet on the human gut microbiome. Genome Med. 2016, 8, 45. [Google Scholar] [CrossRef]
- Ma, F; Li, Z; Liu, H; et al. Dietary-timing-induced gut microbiota diurnal oscillations modulate inflammatory rhythms in rheumatoid arthritis. Cell Metab. 2024, 36, 2367–2382.e5. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Impact of vitamin D concentration on RA activity.
| Type of study | Participants | Evaluated parameters of disease activity | Results | Reference |
|---|---|---|---|---|
| Meta-analysis of 8 studies (6 cross-sectional studies, and 2 case–control studies) |
2,885 RA patients and 1,084 controls |
DAS28 | Seven of the eight studies showed that vitamin D levels are inversely associated with RA activity parameters, such as DAS28. |
[7] |
| Meta-analysis of 14 studies |
1,143 RA patients and 963 controls |
DAS28 | Serum vitamin D level significantly lower in RA patients. Negative correlation between vitamin D level and DAS28. |
[8] |
| Meta-analysis of 24 studies |
3489 patients | DAS28 CRP |
Negative correlation between vitamin D level and DAS28 or CRP level. |
[9] |
| Cross-sectional study |
266 African Americans with recent-onset RA | DAS28 | No statistically significant association between 25(OH)D concentration and DAS28. |
[10] |
| Cross-sectional study |
499 participants with active RA, age 18–85 |
DAS28-ESR, DAS28-CRP, ESR, CRP, HAQ Score, patient assessment on VAS, evaluator assessment on VAS, pain on VAS, van der Heidje erosion score, vdHS score, joint space narrowing, CCP | No correlation between vitamin D level and DAS28, serum inflammatory markers or van der Heijde-Sharp (vdHS) erosion scores. |
[11] |
| Cross-sectional study |
181 patients with RA and 186 controls | DAS28-ESR | No statistically significant association between 25(OH)D concentration and DAS28-ESR |
[12] |
| Cross-sectional study |
35 female RA patients and 38 age- and gender-matched healthy controls |
DAS28-ESR, joint damage based on the Steinbrocker criteria, serum IL-6 levels |
No statistically significant association between 25(OH)D concentration and DAS28 Positive correlation between 25(OH)D and IL-6 among RA patients |
[13] |
| Cross-sectional study | 169 patients with established RA |
DAS28- CRP, psychological distress, pain and sleep |
No statistically significant association between fatigue and serum concentrations of 25(OH)D. Fatigue was significantly associated with RA disease activity, psychological distress and pain, but not with serum 25(OH)D. |
[14] |
CCP, cyclic citrullinated peptide; CRP, C-reactive protein; DAS28, 28 joint count Disease Activity Score; ESR, erythrocyte sedimentation rate; HAQ, Health Assessment Questionnaire;; IL-6, interleukin 6; VAS, visual analog scale; vdHS, van der Heijde-Sharp.
Table 2.
Impact of dietary regimens and dietary factors on risk of RA incidence.
| Factor | Type of study | Study group | Results | Reference |
|---|---|---|---|---|
| Vitamin D | Meta-analysis of 3 cohort studies |
215,757 participants and 874 incident cases of RA |
Significant association between vitamin D intake or supplementation and incidence of RA. |
[7] |
| Mediterranean Diet | Prospective observational study |
83,245 participants from the Nurses’ Health Study (NHS; 1980–2008) and 91,393 participants from NHS II (1991–2009); females only |
No significant correlation. | [25] |
| Prospective observational study |
368 individuals in the Västerbotten Intervention Program (Sweden) who had developed RA and 1,886 controls |
No significant correlation. | [26] | |
| Prospective observational study |
62,629 women, 480 incident cases of RA |
No association between Mediterranean diet and risk of RA. However, adherence to Mediterranean diet diminished the risk of RA among ever-smoking women. |
[27] | |
| Fish and omega-3 consumption |
Meta-analysis of 7 studies | 174 701 participants | Non-statistically significant decrease of RA risk for up to two servings of fish per week; 3 and 4 portions per week associated with a slightly increased risk of RA. | [44] |
| Population-based prospective study |
32 232 middle-aged and older women from the Swedish Mammography Cohort; 205 RA cases |
Regular intake of > 0,21 g omega-3 per day was associated with a 52% lower risk of RA. Consistent long-term consumption of fish ≥1 serving per week compared with<1 was associated with a 29% decrease in RA risk. |
[46] | |
| Population-based case-control study |
324 incident RA cases, 1245 controls |
Higher intake of omega-3 estimated from Frequency of fish consumption was associated with reduced risk of RA. |
[47] | |
| Prospective cohort study |
166,013 women in two prospective cohorts, the Nurses’ Health Study (NHS, 1984–2014) And NHSII (1991–2015). |
No protective impact of fish or omega-3 fatty acids consumption on RA risk. |
[48] | |
| PCBs | Prospective observational study |
1,721 adults ≥ 20 years of age in the National Health and Nutrition Examination Survey 1999–2002 | Exposure to PCBs was positively Associated with RA risk in women. |
[45] |
| Tea | Population-based case control study |
2237 incident RA cases and 4661 matched controls | The risk of RA was inversely correlated to high tea consumption in comparison to irregular consumption among smokers and in the ACPA-positive subset of RA |
[72] |
| Salt | Nested case-control study | 386 RA patients and 1886 matched controls | No significant association between sodium intake and RA development |
[77] |
| Cross-sectional nested study | 18,555 individuals, 392 developed RA |
Sodium intake was associated with RA risk and the effect was dose-dependent. |
[78] |
ACPA, anti-citrullinated protein autoantibody; PCBs, polychlorinated biphenyls.
Table 3.
Impact of dietary factors and supplements on RA activity.
| Factor | Type of study | Dosage | Duration | Participants | Evaluated markers of disease activity | Effect | Reference |
|---|---|---|---|---|---|---|---|
| Vitamin D | Exploratory study | 60000 IU/week for 6 weeks, followed by 60000 IU/month | 12 weeks | 59 RA patients with vitamin D deficiency (below 20 ng/mL) |
DAS28-CRP, DAS28-ESR | Amelioration of DAS28-CRP and DAS28-ESR. |
[15] |
| Randomized double- blind placebo-controlled study |
300,000 IU (a single dose) |
3 months | 39 female patients with early RA: 21 patients assigned to treatment, 18 to placebo |
DAS 28, VAS Pain, HAQ, GH, ESR, CRP |
Treatment with vitamin D improved global health, but had no significant effect on specific signs and symptoms of RA, CRP, VAS pain and DAS28. |
[16] | |
| Randomized, non-blinded interventional study |
50000 IU of vitamin D2 weekly |
3 months | 40 RA patients | DAS-28, ESR, CRP, rheumatoid factor, anti-CCP antibodies | Regulatory T cells (Tregs) elevation and significant DAS-28 score reduction. |
[17] | |
| n-3 fatty acids + low arachidonic acid diet |
Randomized-controlled double-blind crossover study | Anti-inflammatory diet (modified lactovegetarian diet) with AA intake reduced to < 90 mg per day + 30 mg of n-3 fatty acids per kg of body weight per day or placebo (corn oil) |
8 months: 3 months of diet, 2-month washout period, crossover of supplementation, another 3 months of diet |
60 patients with RA; 30 in experimental group (anti-inflammatory diet), 30 in control group (western diet) |
Number of tender and swollen joints, patient’s global assessment, physician’s global assessment, patient’s assessment of pain (VAS) |
Greater reduction in the number of tender and swollen joints in the AID group. |
[32] |
| EPA and DHA/ fish oil supplementation |
Randomized, double-blind trial |
2 g EPA and 1,2 g DHA per day | 12 weeks | 51 patients with RA: 27 In intervention group, 24 in control group | grip strength, joint tenderness, joint swelling, morning stiffness, visual pain score, daily activity score, ESR, CRP | Improvement in: - morning stiffness, joint tenderness and CRP in experimental group, - joint tenderness in both groups. |
[33] |
| Double-blind, controlled study | 10 g of fish oil per day | 6 months | 43 patients with RA: 22 in intervention group, 21 in control group |
NSAID intake, global arthritis activity, pain (VAS), functional capacity (Fries index), grip strength, joint tenderness (Ritchie’s index), physician’s global assessment, ESR, CRP | Decreased intake of NSAID at 3 and 6 months; improvement of global arthritic activity at 3 months. |
[34] | |
| Double-blind placebo controlled study |
1,71 g EPA and 1,14 g DHA per day | 15 months (12 months of supplementation/ placebo, 3 months all patients on placebo) |
52 patients with mild RA: 29 in intervention group, 23 in control group | RAI, grip strength, morning stiffness, 100 mm VAS of joint pain severity as assessed by the patient; 100 mm VAS of joint pain severity as assessed by the metrologist, ESR, CRP |
Reduction of NSAID requirement at 3, 6, 9, 12, 15 months. | [35] | |
| Randomized, double-blind controlled trial |
5,5 g EPA and DHA per day (as adjunctive therapy in modern treat-to-target drug treatment) |
12 months | 121 patients with recent onset RA (<12 months’ duration): 75 in intervention group, 46 in control group |
rate of remission, DMARD use, methotrexate dose, mHAQ, DAS28-ESR |
Higher rate of remission and decreased DMARD use. | [36] | |
| Meta-analysis of 17 randomized controlled trials |
At least 2,7g per day of EPA and DHA | 3-4 months | 823 patients; with RA, but also with joint pain secondary to inflammatory bowel disease and dysmenorrhea |
patient assessed pain, physician assessed pain, duration of morning stiffness, number of painful and/or tender joints, RAI, nonselective NSAID consumption |
Improvement in duration of morning stiffness, number of painful and/or tender joints, patient assessed pain and NSAID intake. | [37] | |
| Meta-analysis of 10 randomized controlled trials |
At least 2,7g of omega-3 fatty acids | At least 3 months | 183 RA patients and 187 placebo-treated RA controls |
NSAID intake tender joint count, swollen joint count, morning stiffness and physical function |
Reduction of NSAID dose. | [38] | |
| Meta-analysis of 20 randomized controlled trials |
0.30 to 9.60 g omega-3 fatty acids (either as a supplement or from food sources) | 12 to 72 weeks | 717 patients with RA in the intervention group and 535 RA patients in the control group. | EMS, tender joint count, ESR and pain scale, CRP, IL-6, IL-1 and TNF-α |
Improved early morning stiffness, tender joint count, ESR and pain scale, reduction of leukotriene B4. | [39] | |
| Flaxseed + anti- inflammatory diet |
Randomized controlled trial for healthy eating | Three groups: flax-seed (30 g/day) plus anti-inflammatory diet (AIF group), flaxseed (30 g/day) plus regular diet (RF group), and roasted wheat (30 g/day) plus regular diet (RW group) |
12 weeks | 120 patients with RA (111 women) |
DAS28, HAQ, disability and pain, quality of life, ESR, CRP, rheumatoid factor, anti-CCP |
Flaxseed decreased DAS28 in RF group compared to RW. Pain severity, morning stiffness and disease feeling decreased significantly in AIF and RF groups. HAQ disability and quality of life measurements improved in all 3 groups, with a greater extent in AIF and RF groups compared to RW. Between-group differences were significant for DAS28, pain scores, and physical and mental health variables. ESR, CRP, anti-CCP, and rheumatoid factor were not different between groups. |
[40] |
| Meals based on red meat, fatty fish, or soy protein |
Randomized controlled cross-over trial |
Patients were assigned to eat isocaloric hamburger meals consisting of red meat (60% beef, 40% pork), fatty fish (salmon), or soy protein for breakfast. |
Blood samples were taken before meals and at intervals up to 5 h postprandial. | 25 patients with RA | IL-6 | Postprandial inflammation assessed by IL-6 did not indicate any significant differences between meals. |
[42,43] |
| Fish oil + cranberry juice |
Randomized, single-blind intervention study |
First group: control Second group: 3 g of omega-3 fatty acids daily Third group: 3 g of omega-3 fatty acids and 500 mL of reduced-calorie cranberry juice daily |
90 days | First group: 21 RA patients Second group: 21 RA patients Third group: 20 RA patients |
ESR, CRP, IL-6, DAS28-CRP, adiponectin, RF, leptin |
Decrease in ESR, CRP, DAS28-CRP, adiponectin and IL-6 in the cranberry juice group. Reduction in DAS28- CRP and adiponectin in the fish oil group. |
[69] |
| Double blind, placebo-controlled trial | 200 µg selenium-enriched yeast or a placebo |
90 days | 55 patients with moderate RA |
VAS, the Ritchie index, the number of swollen and painful joints, morning stiffness | No significant differences between groups. |
[62] | |
| Antioxidants | Randomized controlled study |
Group 1: a standard treatment of intramuscular methotrexate (12.5 mg/week), oral sulphasalazine (1g daily in 2 divided doses) and indomethacin (100 mg suppository at bed-time); Group 2: the standard treatment plus a combination of antioxidants (selenium 50 μg, medicinal yeast 105 mg, vitamin A acetate 5.54 mg, ascorbic acid 100 mg and vitamin E 30 mg); Group 3: standard treatment plus high dose of vitamin E (400 mg t.i.d.) |
2 months | 30 RA patients divided into 3 equal groups |
RAI, duration of morning stiffness, rheumatoid factor (Rose Waaler test), ESR, plasma levels of vitamin E and MDA, the activity of GPx |
Improvement in patients condition (RAI, morning stiffness, ESR) was reported after the first month in group 2 and 3. | [65] |
| Open pilot study | 20 g of antioxidant-enriched spread daily: mix of a-tocopherol (400 mg), lycopene (10 mg), palm oil carotenoids (5 mg; mainly α-carotene) and lutein (10 mg). + vitamin C (200 mg daily) as a supplement |
10 weeks + ‘wash-out’ period of 4 weeks. |
8 non-smoking female patients with rheumatoid factor + RA and DAS28 higher than 2.5 | morning stiffness, VAS pain, general health score and DAS28 (including pain, swelling of joints, ESR, general feeling of well-being) |
The number of swollen and painful joints were significantly decreased, and general health significantly increased at t=10 weeks. DAS was significantly decreased (−1.6) at 10 weeks. After the “wash-out period”, the DAS score was increased again by 0.6. |
[66] | |
| Pre-post clinical trial |
Capsules containing 50 μg selenium, 8 mg zinc, 400 μg vitamin A, 125 mg vitamin C, and 40 mg vitamin E | 12 weeks | 39 female patients with RA | DAS28, hs-CRP, number of swollen and painful joints, CAT, GP¬x, SOD, total antioxidant capacity | Significantly decreased DAS28 score and serum hs-CRP. No differences in number of swollen and painful joints. CAT, GP¬¬x, SOD and total antioxidant capacity increased significantly after intervention | [67] | |
| Randomized controlled study |
500 ml of low-calorie cranberry juice |
90 days | 38 women with RA, 20 in intervention group and 18 in control group |
DAS28, ESR, CRP, RF, anti-CCP antibodies | Significant reduction in DAS28 and anti-CCP antibodies levels | [68] | |
| Randomized, single-blinded clinical study | 500 mg curcumin, 50 mg diclofenac sodium or combination of both |
8 weeks | 38 patients with active RA: 14 in curcumin group, 12 in diclofenac sodium group, 12 in curcumin + diclofenac sodium group | DAS28, ESR, VAS, CRP, ACR20, ACR50, ACR70 |
Significant decrease in CRP level only in the curcumin group. Significant decrease in DAS28 and improvement in ACR scores (ACR 20, 50 and 70) in all groups. The results in the curcumin group were significantly better than in the diclofenac sodium group. | [70] | |
| Randomized, Double-Blind, Placebo-Controlled, Two-Dose, Three-Arm, and Parallel-Group Study | Placebo, 250 or 500mg of the curcumin product twice daily |
90 days | 36 RA patients, divided into 3 groups, 12 patients each |
ESR, CRP, RF, VAS, ACR20, tender joint count, swollen joint count, duration of morning stiffness | Significant improvement in DAS28, VAS and ACR scores, significant decrease in ESR, CRP and RF values. |
[71] | |
| Salt | Pre-post clinical trial |
Three weeks of low-sodium intake (< 5 grams of sodium chloride/day) followed by 2 weeks of normal-sodium dietary regimen (5 g of sodium chloride/day) | 5 weeks | 14 RA patients | Th17 and Treg cells , serum levels of IFNα, TGFβ1, IL-23, IL-1β, IL-6, IL-9, IL-12, IL-17, and TNF | Reduction in the percentage of Th17 cells after low-sodium intake period, increase after normal-sodium intake, Treg lymphocytes showed the opposite trend (not statistically significant); reduction of TGFβ and IL-9 |
[80] |
AA, arachidonic acid; ACR, American College of Rheumatology response criteria; AID, anti-inflammatory diet; CAT, catalase; CCP, cyclic citrullinated peptide; CRP, C-reactive protein; DAS28, 28 joint count Disease Activity Score; DHA, docosahexaenoic acid; DMARD, disease-modifying anti-rheumatic drugs; EMS, early morning stiffness; EPA, eicosapentaenoic acid; ESR, erythrocyte sedimentation rate; GPx, glutathione peroxidase; hs-CRP, high-sensitivity C-reactive protein; IFNα, interferon α; TGFβ1, transforming growth factor β1; IL-1, interleukin 1; IL-1β, interleukin 1β; IL-6, interleukin 6; IL-9, interleukin 9; IL-12, interleukin 12; IL-17, interleukin 17; IL-23, interleukin 23; NSAID, nonsteroidal anti-inflammatory drugs; MDA, malonedialdehyde; mHAQ, modified Health Assessment Questionnaire; RAI, Ritchie’s articular index; RF, rheumatoid factor; SOD, superoxide dismutase; Th17, T helper 17; t.i.d., three times a day; TNF-α, tumor necrosis factor α; Treg, regulatory T cells; VAS, visual analog scale.
Table 4.
Impact of dietary regimens on RA activity.
| Diet | Details of intervention | Duration | Participants | Evaluated markers of disease activity |
Effect | Reference |
|---|---|---|---|---|---|---|
| Mediterranean diet | Experimental group: Cretan version of Mediterranean diet Control group: regular Swedish food |
12 weeks | 51 patients with RA, mostly women; 26 in experimental group, 25 in control group | DAS28 HAQ SF-36 NSAID intake |
Improvement in DAS28, HAQ, SF-36. No difference in NSAID intake. | [19] |
| Intervention group: written information about Mediterranean Diet + cooking classes once a week for 6 weeks Control group: written information about healthy eating in general |
6 months | 130 female patients with RA; 75 in intervention group, 55 in control group |
Tender and swollen joint count, patient global VAS, pain score, EMS, DAS28, HAQ score, ESR, CRP, IL-6 |
Improvements after 3 months of diet in pain score and HAQ; after 6 months in patient global VAS, pain score, EMS | [20] | |
| Intervention group: personalized Mediterranean Diet plans and lifestyle consultation on improving physical activity levels, Control group: generic dietary and physical activity advice, based on the National Dietary Guidelines |
12 weeks | 40 adult women with RA on remission |
DAS28, anthropometric indices (BodPod), vitamin D concentrations, blood lipid profiles |
Participants in the intervention group exhibited lower DAS28, improvements in body weight and body composition, blood glucose and serum 1,25(OH)2D concentrations |
[22] | |
| Mediterranean dietary (MD) pattern and low-fat high-carbohydrate (LC-HF) diet Control group: regular diet |
12 weeks | 154 overweight and obese patients with rheumatoid arthritis |
DAS28 ESR VAS |
DAS 28 significantly decreased in MD compared to the LF-HC group and controls. Serum ESR level was significantly decreased in MD compared to the LF-HC and control groups. VAS was significantly de- creased in the LF-HC and MD groups compared to the controls; no significant difference between the MD and LF-HC groups |
[24] | |
| Vegan diet | Very low fat (10%), vegan diet No control group |
4 weeks | 24 RA patients | Joint swelling and joint tenderness score, degree of pain (VAS), limitation in ability of function, severity of morning stiffness, and duration of morning stiffness, ESR, CRP, RA factor |
Significant decrease in joint tenderness score, joint swelling score, degree of pain because of RA and improvement in severity of morning stiffness and limitation in ability to function. | [49] |
| Intervention: multidisciplinary lifestyle program based on a whole-food plant-based diet, physical activity, and stress management Control group: usual care |
16 weeks | 83 patients with RA | DAS28, Dutch-Flemish Patient Reported Outcomes Measurement Information System (PROMIS) |
Improvement of DAS28 in intervention group vs control group. All patient-reported outcome measures changed slightly (not statistically significantly) in favour of the intervention group |
[50] | |
| Intervention group: uncooked vegan diet (living food) Control group: omnivorous diet |
3 months | 40 RA patients | RAI1, joint stiffness, pain (VAS) | Significant subjective alleviation of symptoms, improvement in RAI1 | [51] | |
| Vegan gluten-free diet | Intervention group: vegan diet free of gluten Control group: well-balanced non-vegan diet |
At least 9 months (up to 1 year) | 47 RA patients: 22 in intervention group, 25 in control group | ACR20 response criteria, Radiographic assessment (Larsen score, number of erosions, joint count) |
Significant improvement in vegan diet patients in all measures contained within ACR response criteria, except CRP. No significant differences in radiographic progression between two groups. |
[53] |
| Intervention group: vegan diet free of gluten, started with 1-day low-energy fasting Control group: well-balanced non-vegan diet |
At least 3 months (up to 12 months) | 58 patients with active RA: 30 in intervention group, 28 in control group |
DAS28 ACR20 response HAQ score ESR, CRP |
Significantly lower DAS28 and HAQ score after 3 and 12 months, CRP after 12 months of vegan diet | [54] | |
| Gluten intake | Participants were stratified based on their habitual gluten intake: high and low- to- medium gluten intake. | 14-16 weeks | 37 RA patients | clinical response to biological treatment (ACR20), HrQoL, CRP |
No statistically significant differences were found between the groups |
[55] |
| Vegan diet and fasting | Intervention group: 7-10 days of fasting, 3,5 months of gluten-free vegan diet and subsequently lactovegetarian diet for up to a year Control group: ordinary mixed food |
13 months | 34 RA patients | number of tender and swollen joints, RAI, pain, morning stiffness duration, grip strength, HAQ score, ESR, CRP, WBC count | After 4 weeks improvement in vegan group in number of tender and swollen joints, RAI, pain, morning stiffness duration, grip strength, HAQ score, ESR, CRP and WBC count. Effects maintained throughout the year. | [57] |
| Fasting group: 7 days of subtotal fast, 2 weeks of re-feeding with lactovegetarian diet. Ketogenic group: isocaloric ketogenic diet, 2 weeks of re-feeding with lactovegetarian diet. |
21 days | 23 RA patients with active disease: 10 in fasting group, 13 in ketogenic group |
IL-6, CRP, ESR, tender joints |
Significant decrease in serum IL-6 and improvement in ESR, CRP and tender joint count after 7-day-fasting, but not after ketogenic diet. |
[58] | |
| Intervention group: 7-day fast followed by an 11-week whole-food plant-based diet combined with time-restricted eating (16:8) Control group: guideline-based anti-inflammatory diet following official German guidelines (German Nutrition Society, DGE) |
12 weeks | 41 women with RA | DAS28 HAQ-DI CDAI SDAI ACR20, ACR50, ACR70 VAS |
The intervention group achieved a HAQ-DI reduction at day 7 of the fast, which was sustained throughout the whole study period up until week 12 and even to the 6-month follow-up. In the control group a similar functional enhancement was seen from study week 6 on up to 6 months. Both dietary approaches had a positive effect on RA disease activity, no significant differences. |
[59] | |
| Intermittent fasting | Intervention group: 16:8 IF diet Control group: maintaining their usual diet + recommendations for healthy eating |
8 weeks | 44 overweight and obese postmenopausal women with RA |
HAQ-DI morning joint stiffness ESR, hs-CRP, IL-6, DAS28, CDAI |
The intervention diet significantly improved DAS-28, CDAI, and HAQ. No other significant differences. |
[60,61] |
| Anti-inflammatory Diet In Rheumatoid Arthritis (ADIRA) | Intervention diet: containing a portfolio of suggested anti-inflammatory foods Control diet: similar to the general dietary intake in Sweden |
10 weeks. After a 4-month washout period the participants switched diet | 47 RA patients | DAS28-ESR, tender and swollen joints, ESR, and visual analog scale for general health, DAS28-CRP | No significant difference between the intervention and control periods for DAS28-ESR. However, DAS28-ESR was significantly lower after the intervention period than before. |
[73] |
ACR, American College of Rheumatology response criteria; CDAI, Clinical Disease Activity Indice; CRP, C-reactive protein; DAS28, 28 joint count Disease Activity Score; EMS, early morning stiffness; ESR, erythrocyte sedimentation rate; HAQ, Health Assessment Questionnaire; HAQ-DI, Health Assessment Questionnaire Disability Index; IL-6, interleukin 6; LF-HC, low-fat high-carbohydrate diet; MD, Mediterranean diet; NSAID, nonsteroidal anti-inflammatory drugs; SDAI, Simplified Disease Activity Indice; SF-36, short form-36 health survey; RA, rheumatoid arthritis; RAI, Ritchie articular index; RAI1, relative activity index; ; VAS, visual analog scale; WBC, white blood cells;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



