Submitted:
10 March 2026
Posted:
10 March 2026
You are already at the latest version
Abstract
TBEV is a major cause of viral central nervous system infections in Europe, with heterogeneous geographical distribution and substantial underdiagnosis in low-incidence regions. This study aimed to evaluate the validity of regional TBE risk classification in Poland by combining surveillance-based incidence data with serological markers of TBEV exposure. Plasma samples from 5,541 blood donors residing in nine regions were tested by anti-TBEV IgG ELISA, followed by confirmatory VNT, IFA and anti-NS1 IgG ELISA to differentiate infection-induced from vaccine-induced antibodies. Regions were classified based on average TBE incidence from 2015–2019. Overall, anti-TBEV IgG screening reactivity was detected in 4.9% of donors, with significant regional variation (p < 0.001). The highest seroprevalence was observed in highly affected regions; however, unexpectedly elevated seroprevalence was also detected in regions classified as low affected. Markers consistent with TBEV infection (anti-NS1 IgG) were identified in only 2.6% of donors, whereas vaccine-induced immunity accounted for the majority of seropositive results. Male sex was independently associated with higher odds of seropositivity. Our findings suggest that passive surveillance data alone may insufficiently capture population-level exposure to TBEV, particularly in regions considered non-endemic. Integrating sero-epidemiological data with surveillance systems may improve risk assessment and inform targeted prevention strategies.
Keywords:
TBE
; TBEV
; surveillance
; blood donors
; Poland
; infection-induced vs vaccine-induced antibodies
1. Introduction
Tick-borne encephalitis virus (TBEV) is the leading cause of viral encephalitis (tick-borne encephalitis, TBE) and meningoencephalitis in the Polish population. The primary route of TBEV transmission to humans is through tick bites. Given that, as in many other European countries, Poland has experienced a recent increase in tick-borne diseases [1], a corresponding rise in the number of TBEV infections and human TBE cases can be anticipated. Occasional outbreaks have also been linked to the consumption of unpasteurized milk from infected sheep or goats [2,3]. In addition, TBEV transmission via transplanted organs has been documented in Poland [4], and sporadic cases of this transmission route have been reported in other countries [5,6].
The geographical distribution of TBEV-infected ticks in Poland is heterogeneous. Certain regions, particularly in the northeastern part of the country, have consistently reported the presence of TBEV-positive ticks, whereas other areas, notably in the northwest, have repeatedly tested negative [7]. However, no clear correlation has been observed between the regional distribution of TBEV in ticks and the incidence of reported TBE cases in humans [8,9]. Moreover, TBEV RNA has been detected in ticks collected from regions with low reported TBE incidence [8,10].
Most TBEV infections are asymptomatic or present with non-specific, mild symptoms; however, in approximately 10–15% of cases, central nervous system involvement occurs, often leading to long-term neurological sequelae. Diagnosis relies on laboratory testing; nevertheless, in regions where specific diagnostic assays are not routinely available, symptomatic TBE cases may remain undetected [11,12], as has been reported in several areas of Poland [8,13]. Vaccination remains the most effective strategy for the prevention of TBE [14,15,16,17].
In Poland, vaccination against TBE is recommended; however, the vaccine is not reimbursed through the public healthcare system. For individuals at occupational risk in highly affected areas, vaccination costs should be covered by employers in accordance with the Labour Code (Article 222) [18]. According to the current Immunization Program [19], vaccination is recommended for forest workers, soldiers, firefighters, border guards, and farmers. Nevertheless, the definition of “highly affected” areas remains ambiguous and allows for subjective interpretation. In contrast, several other countries have adopted more clearly defined and operational vaccination criteria [15]. The application of these recommendations could follow World Health Organization (WHO) guidance. The WHO recommends the implementation of vaccination in regions where the annual TBE incidence is ≥5 cases per 100,000 inhabitants. Based on national surveillance data, by 2023, only one region in Poland—Podlaskie voivodeship in the northeastern part of the country—met this criterion. In all other voivodeships, reported TBE incidence ranges from 0.0 to 1.0 per 100,000 inhabitants [7,20,21].
However, limited regional access to diagnostic testing may lead to underdiagnosis, calling into question the reliability of regional classification based solely on registered incidence rates. Furthermore, previous seroprevalence studies conducted in Poland [8,9,22] did not distinguish between vaccine-induced and post infection-acquired antibodies. Given increasing and regionally heterogeneous vaccination coverage, this limitation may bias interpretations of seroprevalence data and obscure the true epidemiological situation.
The aim of the presented study was to verify current classification of defined areas in Poland based on epidemiological surveillance data as highly, moderate and less affected with data from serological TBEV markers screening in blood donors.
2. Materials and Methods
2.1. Selection of Voivodeships
Due to the relatively small number of reported TBE cases and year-to-year variability in incidence, surveillance data were analyzed over a five-year period. Based on the mean annual incidence over five years (number of reported TBE cases per 100,000 population), voivodeships were classified as highly (≥1.0), moderately (≥0.1 to <1.0), or low affected (<0.1). For the purposes of this study, the World Health Organization (WHO) thresholds for defining exposure to TBEV were lowered to better reflect the epidemiological situation in Poland and to allow stratification of voivodeships into three exposure categories.
Using national surveillance data from 2015–2019 [Supplementary Data], voivodeships were classified as follows (Figure 1):
- Highly affected: Podlaskie, Warmińsko-Mazurskie (>1.0 per 100,000 population)
- Moderately affected: Dolnośląskie, Łódzkie, Mazowieckie, Lubelskie, Opolskie, Małopolskie, and Świętokrzyskie. In these regions, with a five-year TBE incidence ranging from sse population, TBE cases are reported annually, and virus has been sporadically detected in environmental studies [7]. One possible explanation is the presence of smaller administrative units within these voivodeships with higher local incidence, despite an overall voivodeship-level incidence above 1 per 100,000.
- Low affected: Zachodniopomorskie, Pomorskie, Kujawsko-Pomorskie, Lubuskie, Podkarpackie, Śląskie, and Wielkopolskie. In these regions, only sporadic TBE cases are reported, with a mean five-year incidence below 0.1 per 100,000 population; many of these cases are likely associated with travel to more highly affected areas.
2.2. Study Population and Design
The serum bank was established in 2021–2022 as part of the project “TBE seroprevalence in Poland” (TBEseroPL), conducted at the National Institute of Public Health – National Institute of Hygiene – National Research Institute (NIPH NIH–NRI). The study protocol was approved by the Ethics Committee of the NIPH NIH–NRI (approval no. 13/2021, 19 November 2021).
The sampling frame comprised blood donors registered at Regional Blood Transfusion Centers (RBTCs) located in nine of the sixteen Polish voivodeships: Dolnośląskie, Kujawsko-Pomorskie, Lubelskie, Łódzkie, Małopolskie, Podkarpackie, Podlaskie, Pomorskie, and Zachodniopomorskie. Each RBTC provided residual EDTA plasma samples from randomly selected adult donors (≥18 years) collected during routine mandatory screening for hepatitis C virus (HCV), hepatitis B virus (HBV), human immunodeficiency virus (HIV), and Treponema pallidum. All plasma samples were transported on dry ice and stored at −20°C until analysis.
2.3. Sample Size Calculation
Sample size was determined using a precision-based sample size calculation in STATA (version 18.0 SE; StataCorp LLC, College Station, TX, USA), assuming a two-sided significance level (α) of 0.05 and a statistical power of 0.80. Calculations were performed using the normal approximation to the binomial distribution and were conducted separately for highly affected, moderately affected, and low-affected areas.
A previous seroprevalence study by Stefanoff et al. [23] based on samples collected between 1996 and 2005, reported an anti-TBEV IgG seroprevalence of 4.3% in the endemic Podlaskie voivodeship using ELISA screening. The majority of positive samples (7/10) were confirmed as infection-induced by indirect immunofluorescence (IIF) and hemagglutination inhibition (HI) assays. In contrast, in non-endemic regions, the proportion of confirmed TBEV infections among ELISA-positive samples was lower (4/14 retested sera), indicating that similar ELISA seroprevalence rates may correspond to substantially different proportions of true infections.
Given evidence of TBE incidence in several moderate and low-affected areas that may remain undetected due to limited diagnostic testing, we assumed identical expected seroprevalence for moderately and low-affected regions for the purposes of sample size estimation.
The following assumptions were applied:
- Highly affected areas: expected seroprevalence of 4%, with an acceptable confidence interval width of 3% (e.g. 2.5%–5.5%), resulting in an estimated sample size of 688.
- Moderately and low-affected areas: expected seroprevalence of 1.5%, with an acceptable confidence interval width of 1% (e.g. 1.0%–2.0%), resulting in an estimated sample size of 2,346.
Accordingly, target sample sizes were set at approximately 700 samples for highly affected areas and 2,400 samples for both moderate and low-affected areas. The study included one highly affected voivodeship (Podlaskie), four moderately affected voivodeships (Dolnośląskie, Lubelskie, Łódzkie, and Małopolskie), and four low-affected voivodeships (Kujawsko-Pomorskie, Podkarpackie, Pomorskie, and Zachodniopomorskie), with an equal allocation of approximately 600 samples per voivodeship.
2.4. Screening Assays
As enzyme-linked immunosorbent assays (ELISAs) are the primary methods used for serological diagnosis of TBE, a commercially available anti-TBEV ELISA assay marketed in Poland was selected. All serum and plasma samples were tested using the Euroimmun anti-TBEV IgG ELISA (Anti-TBEV ELISA IgG, EI 2661-9601 G; Euroimmun, Germany) according to the manufacturer’s instructions. Results were expressed as the ratio of the optical density (OD) of the sample to that of the calibrator, with values >1.1 interpreted as positive, <0.8 as negative, and 0.8–1.09 as borderline.
2.5. Confirmatory Assays
Confirmatory testing was performed at the Bundeswehr Institute of Microbiology (Munich, Germany). Virus neutralization tests (VNTs) were conducted to verify the specificity of ELISA-positive results. To differentiate between vaccine-induced and infection-induced antibodies, an anti-NS1 IgG assay was applied as previously described [24].
Upon receipt, all selected sera were re-tested using the same ELISA screening assay to confirm reactivity. This step was necessary due to repeated freeze–thaw cycles, shipment conditions, and limited sample volumes, which may affect antibody stability.
Criteria for confirmatory testing included sera with repeated positive results (ratio ≥1.1), borderline results (ratio 0.8–1.1), or a marked decrease in antibody levels between tests. In total, 235 sera met these criteria and were subjected to confirmatory analysis using the following methods:
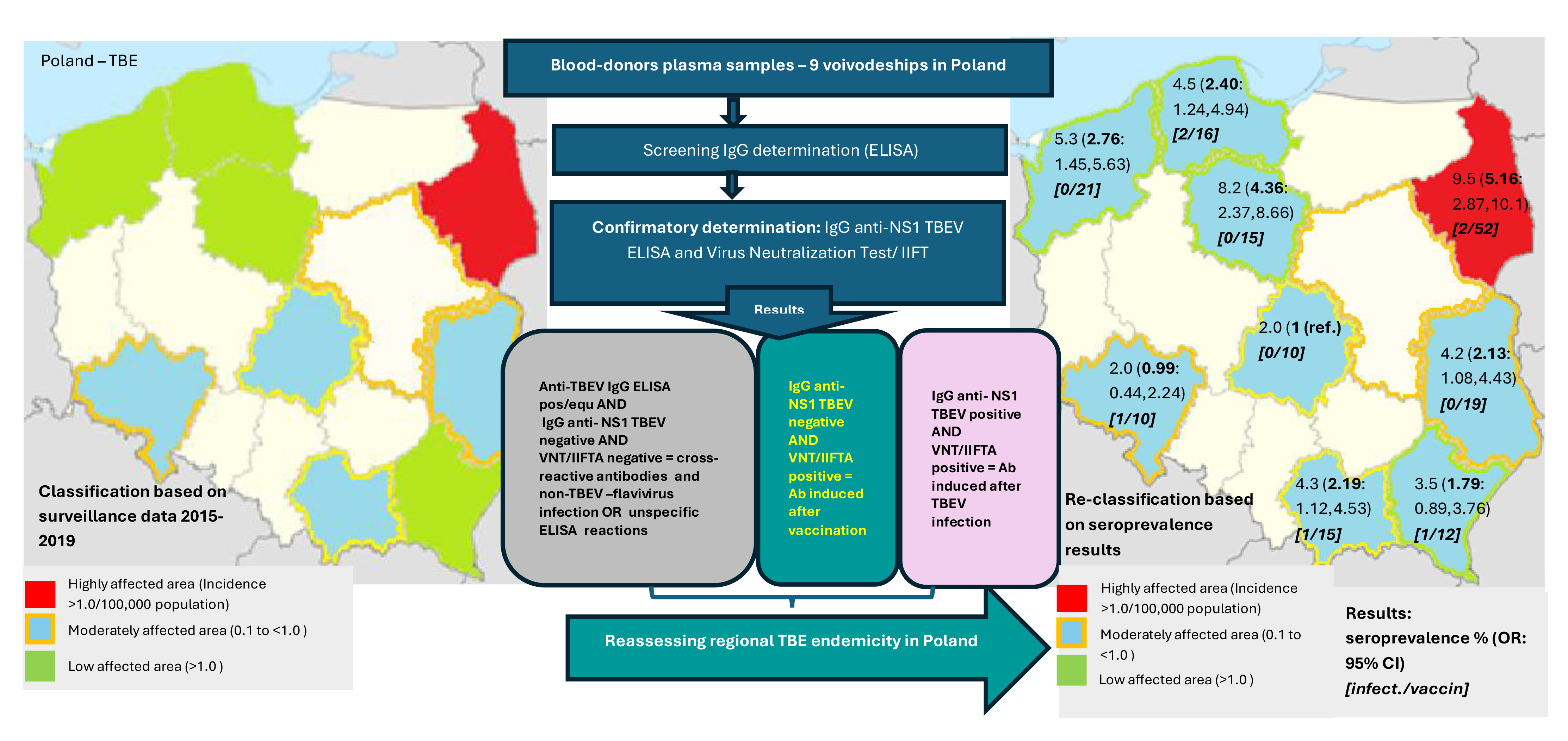
All assays were performed according to the diagnostic algorithm presented in Figure 2.
2.6. Statistical Analysis
Logistic regression was used to assess factors associated with immunological status. Results are presented as odds ratios (ORs) with corresponding 95% confidence intervals (CIs) and p-values. A two-sided significance level of α = 0.05 was applied in all analyses. Statistical analyses were conducted using R software version 3.4.1 [26].
3. Results
We analyzed results from 5,541 blood donor samples out of 5,544 collected and tested; results from three negative samples were excluded due to incomplete data. Donor age ranged from 18 to 66 years. Among the participants, 52.3% were ≤40 years old and 47.7% were older than 40 years. The median age was 40.0 years (interquartile range [IQR]: 30.0–46.0 years). The study population comprised 2,370 women (42.8%) and 3,171 men (57.2%). The majority of donors resided in urban areas (60.9%) (Table S1).
3.1. Screening IgG assays
Positive and equivocal anti-TBEV IgG screening results were detected in 205 (3.7%) and 67 (1.2%) serum samples, respectively. The distribution of results (positive + equivocal vs. negative) differed significantly between voivodeships (ranged 2.0%-9.5%), and difference of reactivity between less and highly affected regions was more than fivefold (p < 0.001) (Table 1). The highest seroprevalence (9.5%) was observed in the voivodeship previously classified as highly affected (Podlaskie). Notably, elevated seroprevalence was also detected in voivodeships classified as low affected: Kujawsko-Pomorskie (8.2%) and Zachodniopomorskie (5.3%).
A significant association between sex and seroprevalence was identified (p < 0.001). Overall, the odds of detecting anti-TBEV antibodies were 1.9 times higher in men than in women (OR = 1.86; 95% CI: 1.43–2.43; p < 0.001) (Table 1). No significant difference in anti-TBEV IgG positivity was observed with respect to age group (OR=0.86; 95% CI: 0.67, 1.09; p>0.05), and place of residence: 3.4% (74/2,170) among rural residents and 3.9% (132/3,371) among urban residents (OR=0,92; 95% CI: 0.72,1.18; p > 0.05).
3.2. Differentiation of Post-Vaccination and Post-Infection Immune Responses
Based on screening and confirmatory testing, immunological status was determined for 5,507 blood donors. Evidence of past TBEV infection was identified in 7 individuals (0.13%), vaccination-induced immunity in 170 individuals (3.1%), and no detectable TBEV antibodies in 5,330 individuals (96.8%). The distribution of immunological status differed significantly by voivodeship (p < 0.001) (Table 1). Immunological status could not be determined for 34 samples due to insufficient sample volume for confirmatory testing.
Analysis of anti-NS1 IgG antibodies indicated previous TBEV infection in seven blood donors from five voivodeships, representing 2.6% of samples with positive or borderline anti-TBEV IgG screening results (Table 1). Anti-NS1 IgG was detected in four men and three women. Two individuals resided in a highly affected region (Podlaskie), two in moderately affected regions, and three in regions classified as low affected. All but one individual (from Pomorskie voivodeship) lived in urban areas. Five of the seven individuals were older than 40 years (aged 45–52 years); the remaining two were under 40 years of age and also resided in urban areas.
Vaccination-induced immune responses were identified in 170 individuals (3.1% of all blood donors), predominantly among men (approximately 75%) (Figure 3). This male predominance was observed across all analyzed regions. However, vaccination coverage varied between voivodeships, ranging from 1.8% in Dolnośląskie to 7.4% in Podlaskie, with the highest proportion observed in the highly affected region. In some voivodeships (e.g. Łódzkie), vaccination was reported exclusively among men.
Sera yielded positive anti-TBEV IgG screening results but lacked confirmatory evidence of either infection-induced or vaccination-induced immunity - were categorized as “other.” Such results may reflect non-specific reactions or cross-reactivity with other Flaviviruses associated with prior vaccination or infection. Additionally, variation in the persistence of IgG antibodies against different viral epitopes may contribute to this finding. Overall, samples classified as “other” accounted for 1.7% of all tested samples, with proportions ranging from 0.2% to 5.7% across voivodeships; the highest proportion was observed in Kujawsko-Pomorskie.
No significant association was observed between place of residence (urban vs. rural) and immunological status (p > 0.05). Among 3,354 urban residents, vaccination-induced immunity was identified in 104 individuals (3.1%), and past infection in 6 individuals (0.2%). Among 2,153 rural residents, vaccination was detected in 66 individuals (3.1%), and past infection in only one individual (0.05%), residing in a voivodeship classified as low affected (Pomorskie).
3.3. Additional Analysis
Given the sporadic detection of anti-NS1 IgG across voivodeships, additional analyses were performed by aggregating data from highly affected regions, moderately affected regions (four voivodeships combined), and low affected regions (four voivodeships combined) (Table 2). A highly significant difference in anti-NS1 IgG seroprevalence was observed between highly affected and low affected regions when analyses excluded samples classified as “other” (OR = 2.8; 95% CI: 1.9–4.1; p < 0.001). A higher prevalence of reactions classified as “other” (non-TBEV infection, possible cross-reactivity, or non-specific reactions) was observed in low affected regions. Moreover, after exclusion of these “other” results, moderately affected regions exhibited seroprevalence levels comparable to those observed in low affected regions.
4. Discussion
Due to changes in the epidemiology of tick-borne encephalitis virus (TBEV) infections and the increasing number of detected and reported cases, tick-borne encephalitis (TBE) has become a major public health concern in Europe. Consequently, many countries have conducted seroprevalence studies to estimate the immune status of their populations resulting from both natural TBEV infection and vaccination, including Romania, Slovenia, Germany, Poland, the Czech Republic, Italy and Serbia [22,27,28,29,30,31,32,33]. More refined testing strategies that differentiate between immunity acquired through past infection and vaccination allow for a more accurate estimation of infection incidence and population susceptibility. Our study represents one of such enhanced approaches [25,27,34,35]. Despite several limitations discussed below, the use of blood donor samples in seroprevalence studies enables comparisons between countries. In most European countries, blood donors donate on a voluntary, non-commercial basis, and similar pre-donation screening procedures are applied, which supports the reliability and comparability of results. Comparable studies have recently been conducted in Romania, Germany, and Switzerland [25,29,34,36].
In our study conducted among Polish blood donors, the overall proportion of samples with positive or borderline anti-TBEV IgG ELISA screening results was 4.9% (3.7% positive and 1.2% borderline). However, substantial regional differences were observed between voivodeships, with prevalence ranging from 2.0% to 9.5%.
Overall, our findings are comparable to those reported in Romania [28], where 3.6% of 1,200 samples were positive or borderline in the TBEV IgG ELISA (2.3% positive and 1.3% borderline). In contrast, seroprevalence rates reported in Germany were markedly higher: positive IgG results were detected in 57% of 2,220 blood donors [25]. Importantly, that study focused on donors from a highly TBE-endemic region in southern Germany, where anti-TBE vaccination is highly recommended. In our study, although the overall prevalence was 4.9% among 5,541 donors, the highest regional prevalence—observed in a voivodeship classified as highly affected—reached 9.5% (67/703). A comparison of seroprevalence in two regions with high incidence rates (according to the WHO definition) in Poland (Podlaskie) and Germany shows significant differences, which may be the result of fewer infections and a likely lower vaccination rate in Poland. Data on TBE vaccination coverage in Poland are limited, as reporting of TBE vaccination is not mandatory. Estimates are therefore based on vaccine sales rather than medical records. Despite the absence of a national vaccination registry, an increasing trend in vaccination uptake has been noted in recent years. According to the report Tick-borne encephalitis in Poland and worldwide. Assessment of the epidemiological situation of TBE in Poland (28 February 2021) [37], approximately 90,000 individuals were vaccinated against TBE in 2019. Although vaccination coverage increased nearly threefold between 2015 and 2019, overall coverage remains low, at approximately 2.5–4% of the Polish population.
Our hypothesis regarding lower infection rates and vaccination coverage in the Podlaskie voivodeship than in South Germany, is supported by a study conducted by Bojkiewicz et al. in 2021 in the Podlaskie Province, which was severely affected by the virus [22]. The authors analyzed the seroprevalence of tick-borne encephalitis virus in two cohorts: 298 blood donors and 180 children (aged 2–17) hospitalized for viral gastroenteritis. They also assessed the attitudes of adult donors and parents of hospitalized children towards vaccination against tick-borne encephalitis. Based on survey data, only 13% of blood donors had been vaccinated against TBE prior to the study, with higher vaccination rates among men (15%) than women (7%), consistent with our findings. Vaccination coverage among parents of hospitalized children was even lower (9%), and none of the children had been vaccinated. Anti-TBEV IgG antibodies were detected in 10% of blood donors and 2% of children, which confirms the results obtained in our study in highly-affected area.
According to Polish national surveillance data, most TBE cases occur among unvaccinated individuals. Assessment of TBEV seroprevalence among unvaccinated individuals is particularly useful for estimating the frequency of asymptomatic infections. In the study by Bojkiewicz et al. [22], anti-TBEV IgG antibodies were detected in 5% of unvaccinated adults and 2% of children. These data support our findings from Podlaskie voivodeship, as well as results reported by Dobler et al. [25], indicating that asymptomatic or mild TBEV infections occur relatively frequently. The question remains whether antibodies produced during asymptomatic TBEV infection are as persistent as those produced during symptomatic infection, or whether they disappear more quickly.
Confirmatory testing in our study was performed to better estimate the risk of TBEV infection in selected regions. Detection of anti-NS1 TBEV antibodies indicates immune responses to virus infection, typically acquired through environmental exposure or consumption of unpasteurized dairy products. The prevalence of anti-NS1 TBEV IgG among anti-TBEV IgG-positive individuals was also higher in southwestern Germany than in our study (6% vs. 3.6%, respectively), although this difference was not statistically significant. Furthermore, in Bavaria, the frequency of IgG anti-NS1 was similar to that in our study, but with a significantly higher seroprevalence (86%). Notably, all mentioned studies used similar protocols, and all confirmatory testing was performed in the same reference laboratory in Munich, Germany [25,38].
Overall, the prevalence of anti-NS1 TBEV IgG was unexpectedly low (0.13% overall and 0.29% in highly affected regions) in our study. Also, the overall frequency of anti-TBEV IgG positivity (3.6%) was lower than anticipated based on literature data. Studies conducted in blood-donors in Sweden (2018–2019) and in highly endemic regions of southern Germany reported substantially higher seroprevalence rates: respectively: 9.7%–64% and 55%-84.8% [25,35,38]. Also study in general population in the Czech Republic (2001) indicated higher value (26.3%) than in our study [32]. The values obtained in our study are rather similar to the seroprevalence in Denmark [39]. A hypothesis that difference between the expected and determined seroprevalence due to lower vaccination rates or lower risk in Poland than in neighboring countries needs verification.
Bojkiewicz et al. [22] also assessed previous confirmed TBEV infections and vaccination responses among adults. Notably, four individuals with a documented history of TBE were seronegative at the time of testing, and only 68% of vaccinated individuals were anti-TBEV IgG positive. In contrast to these results, other studies conducted in Europe [40,41] indicate a rather stable and lasting up to 15 years response after vaccination. These findings highlight a key limitation of seroprevalence studies: protective antibody levels depend on time since vaccination or infection, individual health status and age, antibody persistence, and the presence of so-called natural boosters resulting from environmental exposure.
Furthermore, still insufficient information is available regarding the duration of anti-NS1 antibody persistence and potential differences between asymptomatic infections and cases with neurological symptoms. Research conducted in Latvia indicates that anti-NS1 antibodies are also detected in vaccinated individuals, probably as a result of asymptomatic or mild infections that remain unrecognized [37,42]. Girl et al. [38] study indicated unexpected high prevalence (>97%) of asymptomatic cases in highly-affected and with high level of anti-TBE vaccination coverage area in Germany. Repeated seroprevalence studies conducted at multi-year intervals could substantially improve understanding of TBE distribution, exposure levels, and inform public health strategies, including vaccination campaigns.
Interestingly, six of seven individuals with detectable anti-NS1 TBEV IgG resided in urban areas. This contrasts with surveillance analyses [37], which identify rural residence and prolonged exposure to forested or agricultural environments as major risk factors. One possible explanation is that urban residents—potentially tourists—may be exposed due to inadequate preventive measures, whereas repeated low-level exposure among rural residents may act as natural immune boosters. This hypothesis warrants further investigation.
High proportions of anti-TBEV IgG-positive blood donors were also observed in Kujawsko-Pomorskie and Zachodniopomorskie voivodeships (8.2% and 5.3%, respectively), regions classified as low-incidence areas based on surveillance data. No markers of recent or past infections were detected in these regions in our study. One possible explanation is the presence of military training grounds, with a higher proportion of vaccinated soldiers among donors. Additionally, Poland lacks routine environmental surveillance of Flaviviruses in ticks and mosquitoes, limiting verification of potential exposure. Although establishment of other Flaviviruses in these regions is unlikely, it cannot be excluded. Confirmation would require virus neutralization tests to assess potential cross-reactivity, which is well documented among flaviviruses [43].
In contrast, markers of past TBEV infection (anti-NS1 IgG) were detected in donors from Dolnośląskie, Małopolskie, Podkarpackie, and Pomorskie voivodeships. While the first two regions are classified as moderately affected, the latter two are considered low-incidence areas. This may reflect domestic travel patterns, particularly intensified during the COVID-19 pandemic, or underreporting of TBE cases in these regions. As shown by Paradowska-Stankiewicz et al. (2023) [20], comparison of surveillance data with Nationwide General Hospital Morbidity Study (NGHMS) records revealed substantial underestimation of TBE incidence, particularly in Podkarpackie and Pomorskie voivodeships.
This conclusion is supported by the study of Zajkowska et al.(2025) [13], who demonstrated that limited diagnostic capacity contributes to underreporting of TBE. By retrospectively testing patients initially diagnosed with other viral neurological conditions, they identified 124 previously unreported TBE cases among 766 patients across ten voivodeships. Similar studies conducted in Sweden detected only one such case (1/137) [44]. These findings support our conclusion that TBE incidence is underestimated in many regions of Poland and highlight the need to assess the risk of TBEV infection among blood donors in these areas.
5. Conclusions
In summary, our results suggest that surveillance effectiveness in Polish regions classified as non-endemic or low-incidence for TBEV is lower than in highly affected voivodeships. Limited awareness among healthcare providers and insufficient diagnostic capacity likely contribute to underdiagnosis, which in turn reduces vaccination uptake in the general population.
Our results also show that the variation in exposure to TBEV infection in Poland may be significantly lower than would be expected based on the TBE incidence. However, it should be emphasized that the highest risk of infection remains in highly affected regions in Poland—Podlaskie voivodeship and, most likely, the Warmińsko-Mazurskie (not studied in this work).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, K.P. and M.R.; methodology, K.P. M.R. ; software, NA.; validation, K.P., G.D.; formal analysis, D.R.., A.P.; investigation, A.K., G.D.; resources, A.K..; data curation, B.G., A.K..; writing—original draft preparation, K.P., P. G., M.R., G.D.; writing— review and editing, P.G., A.P., B.G.; visualization, B.G..; supervision, K.P., M.R..; project administration, K.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Pfizer (Pfizer Medical Grant, GMGS request #61773353 -Research Grant “TBE seroprevalence study in Poland) and partially by the NIPH NIH-NRI project: Assessment of the immune response against selected flaviviruses in a group of blood donors (2024–2026).
Institutional Review Board Statement
Sera from one biobank protocols were used. The protocol of the study was approved by the Ethics Committee at the NIPH NIH - NRI (no: 13/2021, 19th Nov 2021).
Informed Consent Statement
Patient consent was waived due to use anonymized blood sample residues remaining after routine testing were used for the research. Additional tests were performed on samples left at the disposal of the laboratory by blood-donors.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| TBEV | Tick-borne encephalitis virus |
| TBE | Tick-borne encephalitis |
| VNT | virus neutralization testing |
| WHO | World Health Organization |
| RBTCs | Regional Blood Transfusion Centers |
| IIF | indirect immunofluorescence |
| ELISAs | enzyme-linked immunosorbent assays |
| IIFT | Indirect immunofluorescence test |
References
- Mrozowska-Nyckowska, K.; Zbrzeźniak, J.; Paradowska-Stankiewicz, I. Meningitis and encephalitis in Poland in 2021. Przegl. Epidemiol. 2023, 77, 387–402. [Google Scholar] [CrossRef]
- Nagańska, A.; Garbacz-Łagożna, E.; Kowalski, J.; Cholewińska-Szymańska, G.; Chylak-Nowosielska, A.; Antosiewicz, M.; Szymański, R. The thick-borne encephalitis caused by alimentary transmission - case series report. Przegl. Epidemiol. 2023, 77, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Król, M.E.; Borawski, B.; Nowicka-Ciełuszecka, A.; Tarasiuk, J.; Zajkowska, J. Outbreak of alimentary tick-borne encephalitis in Podlaskie voivodeship, Poland. Przegl. Epidemiol. 2019, 73, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Lipowski, D.; Popiel, M.; Perlejewski, K.; Nakamura, S.; Bukowska-Osko, I.; Rzadkiewicz, E.; Dzieciatkowski, T.; Milecka, A.; Wenski, W.; Ciszek, M.; et al. Cluster of Fatal Tick-borne Encephalitis Virus Infection in Organ Transplant Setting. J. Infect. Dis. 2017, 215, 896–901. [Google Scholar] [CrossRef]
- Wahlberg, P.; Saikku, P.; Brummer-Korvenkontio, M. Tick-borne viral encephalitis in Finland. The clinical features of Kumlinge disease during 1959-1987. J. Intern. Med. 1989, 225, 173–177. [Google Scholar] [CrossRef]
- Mathys, S.; Gültekin, N.; Stanga, Z.; Ülgür, I.; Schlagenhauf, P. Seroprevalence of tick-borne infections in blood donors in Europe: a systematic review. New Microbes New Infect. 2025, 10, 65:101597. [Google Scholar] [CrossRef]
- 7. Pancer, K. TBE in Poland. In The TBE Book, 7th ed.; Dobler, G., Erber, W., Bröker, M., Chitimia-Dobler, L., Schmitt, H.J., Eds.; Global Health Press: Singapore, 2024; p. Chapter 13. [Google Scholar] [CrossRef]
- Stefanoff, P.; Pfeffer, M.; Hellenbrand, W.; Rogalska, J.; Rühe, F.; Makówka, A.; Michalik, J.; Wodecka, B.; Rymaszewska, A.; Kiewra, D.; et al. Virus detection in questing ticks is not a sensitive indicator for risk assessment of tick-borne encephalitis in humans. Zoonoses Public Health 2013, 60, 215–226. [Google Scholar] [CrossRef]
- Stefanoff, P.; Zielicka-Hardy, A.; Hlebowicz, M.; Konior, R.; Lipowski, D.; Szenborn, L.; Siennicka, J.; Orlikova, H. TBE enhanced surveillance working group. New endemic foci of tick-borne encephalitis (TBE) identified in districts where testing for TBE was not available before 2009 in Poland. Parasit. Vectors 2013, 6, 180. [Google Scholar] [CrossRef]
- Stefanoff, P.; Rubikowska, B.; Bratkowski, J.; Ustrnul, Z.; Vanwambeke, S.O.; Rosinska, M. A Predictive Model Has Identified Tick-Borne Encephalitis High-Risk Areas in Regions Where No Cases Were Reported Previously, Poland, 1999-2012. Int. J. Environ. Res. Public Health 2018, 15, 677. [Google Scholar] [CrossRef] [PubMed]
- Kunze, M.; Banović, P; Bogovič, P.; Briciu, V; Čivljak, R.; Dobler, G.; Hristea, A.; Kerlik, J.; Kuivanen, S.; Kynčl, J.; et al. Recommendations to Improve Tick-Borne Encephalitis Surveillance and Vaccine Uptake in Europe. Microorganisms 2022, 10, 1283. [Google Scholar] [CrossRef]
- Zielicka-Hardy, A.; Rosińska, M.; Kondrusik, M.; Hlebowicz, M.; Konior, R.; Stefanoff, P. Predictors for diagnosis of tick-borne encephalitis infection in Poland, 2009-2010. Infect. Dis. 2015, 47, 604–610. [Google Scholar] [CrossRef]
- Zajkowska, J.; Waluk, E.; Świerzbińska, R.; Dunaj, J.; Zajkowska, O.; Wawrzuta, D.; Niścigorska-Olsen, J.; Matukiewicz, M.; Oczko-Grzesik, B.; Veltze, D. The impact of serological testing implementation on tick-borne encephalitis detection in Poland. PLOS ONE 2025, 20, e0323022. [Google Scholar] [CrossRef] [PubMed]
- Caputo, M.; Stumpe, V.; Rübsamen, N.; Mikolajczyk, R.T.; Karch, A. Implementation of preventive measures against tick-borne infections in a non-endemic area for tick-borne encephalitis-Results from a population-based survey in Lower Saxony, Germany. Ticks Tick Borne Dis. 2019, 10, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Zavadska, D.; Anca, I.; André, F.; Bakir, M.; Chlibek, R.; Cižman, M.; Ivaskeviciene, I.; Mangarov, A.; Mészner, Z.; Pokorn, M.; et al. Recommendations for tick-borne encephalitis vaccination from the Central European Vaccination Awareness Group (CEVAG). Hum. Vaccin. Immunother. 2013, 9, 362–374. [Google Scholar] [CrossRef] [PubMed]
- Hertzell, K.B.; Pauksens, K.; Rombo, L.; Knight, A.; Vene, S.; Askling, H.H. Tick-borne encephalitis (TBE) vaccine to medically immunosuppressed patients with rheumatoid arthritis: A prospective, open-label, multi-centre study. Vaccine 2016, 34, 650–655. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Tick-borne encephalitis. Immunization offers the most effective protection [Internet]. Available from: https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases/tick-borne-encephalitis (accessed on 10 February 2026).
- Act of 26 June 1974 – Labour Code (consolidated text: Journal of Laws 2023, item 1465, as amended). Republic of Poland. Available online: https://isap.sejm.gov.pl/ (accessed on 10 February 2026).
- National Institute of Public Health NIH – National Research Institute. Program Szczepień Ochronnych dzieci i młodzieży w 2026 roku [Protective Vaccination Program for Children and Adolescents in 2026]. Szczepienia.info. 2026. Available online: https://szczepienia.pzh.gov.pl/kalendarz-szczepien-2026-2/ (accessed on 10 February 2026).
- Paradowska-Stankiewicz, I.; Pancer, K.; Poznańska, A.; Hordowicz, M.; Skibicka, M.; Słowiński, M.; Motak, G.; Falkiewicz, B. Tick-borne encephalitis epidemiology and surveillance in Poland, and comparison with selected European countries before and during the COVID-19 pandemic, 2008 to 2020. Euro Surveill. 2023, 28, 2200452. [Google Scholar] [CrossRef]
- Paradowska-Stankiewicz, I.; Piotrowska, A. Meningitis and encephalitis in Poland in 2015. Przegl. Epidemiol. 2017, 71, 493–500. [Google Scholar] [PubMed]
- Bojkiewicz, E.; Toczylowski, K.; Grygorczuk, S.; Zelazowska-Rutkowska, B.; Dunaj, J.; Zebrowska, A.; Czupryna, P.; Moniuszko-Malinowska, A.; Sulik, A. The Prevalence of Asymptomatic Infections with Tick-Borne Encephalitis Virus and Attitude towards Tick-Borne Encephalitis Vaccine in the Endemic Area of Northeastern Poland. Vaccines 2022, 10, 1294. [Google Scholar] [CrossRef]
- Stefanoff, P.; Siennicka, J.; Kaba, J.; Nowicki, M.; Ferenczi, E.; Gut, W. Identification of new endemic tick-borne encephalitis foci in Poland – a pilot seroprevalence study in selected regions. Int. J. Med. Microbiol. 2008, 298, 102–107. [Google Scholar] [CrossRef]
- Girl, P.; Bestehorn-Willmann, M.; Zange, S.; Borde, J.P.; Dobler, G.; von Buttlar, H. Tick-Borne Encephalitis Virus Nonstructural Protein 1 IgG Enzyme-Linked Immunosorbent Assay for Differentiating Infection versus Vaccination Antibody Responses. J. Clin. Microbiol. 2020, 58, e01783-19. [Google Scholar] [CrossRef]
- Dobler, G.; Euringer, K.; Kaier, K.; Borde, J.P. Serological Protection Rates against TBEV Infection in Blood Donors from a Highly Endemic Region in Southern Germany. Vaccines 2023, 11, 522. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing [Internet]; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/.
- Kelly, P.H.; Kwark, R.; Marick, H.M.; Davis, J.; Stark, J.H.; Madhava, H.; Dobler, G.; Moïsi, J.C. Different environmental factors predict the occurrence of tick-borne encephalitis virus (TBEV) and reveal new potential risk areas across Europe via geospatial models. Int J Health Geogr 2025, 24, 3. [Google Scholar] [CrossRef] [PubMed]
- Coroian, M.; Mihalca, A.D.; Dobler, G.; Euringer, K.; Girl, P.; Borșan, S.D.; Kalmár, Z.; Tincuța Briciu, V.; Flonta, M.; Topan, A.; et al. Seroprevalence Rates against West Nile, Usutu, and Tick-Borne Encephalitis Viruses in Blood-Donors from North-Western Romania. Int. J. Environ. Res. Public Health 2022, 19, 8182. [Google Scholar] [CrossRef] [PubMed]
- Panciu, A.M.; Cheran, C.A.; Militaru, E.D.; Rîciu, C.D.; Hristea, A. Serosurvey of Tick-Borne Encephalitis Virus Infection in Romania. Pathogens 2024, 13, 231. [Google Scholar] [CrossRef] [PubMed]
- Fafangel, M.; Cassini, A.; Colzani, E.; Klavs, I.; Grgič Vitek, M.; Učakar, V.; Muehlen, M.; Vudrag, M.; Kraigher, A. Estimating the annual burden of tick-borne encephalitis to inform vaccination policy, Slovenia, 2009 to 2013. Euro Surveill. 2017, 22, 30509. [Google Scholar] [CrossRef] [PubMed]
- Castagna, A.; Schiavon, S.; Mengozzi, G.; Baldovin, T.; Nozza, S.; Canetti, D.; Cocchio, S.; Montuori, E.A.; Iantomasi, R.; Baldo, V. Tick-borne encephalitis seroprevalence in northern Italy: a cross-sectional study on a randomly selected population. IJID Reg. 2024, 12, 100404. [Google Scholar] [CrossRef] [PubMed]
- Kriz, B.; Hubalek, Z.; Marek, M.; Daniel, M.; Strakova, P.; Betasova, L. Results of the Screening of Tick-Borne Encephalitis Virus Antibodies in Human Sera from Eight Districts Collected Two Decades Apart. Vector-Borne Zoonotic Dis. 2015, 15, 489–493. [Google Scholar] [CrossRef]
- Banović, P.; Obregón, D.; Mijatović, D.; Simin, V.; Stankov, S.; Budakov-Obradović, Z.; Bujandrić, N.; Grujić, J.; Sević, S.; Turkulov, V.; et al. Tick-Borne Encephalitis Virus Seropositivity among Tick Infested Individuals in Serbia. Pathogens 2021, 10, 301. [Google Scholar] [CrossRef]
- Euringer, K.; Girl, P.; Kaier, K.; Peilstöcker, J.; Schmidt, M.; Müller-Steinhardt, M.; Rauscher, B.; Bressau, E.; Kern, W.V.; Dobler, G.; et al. Tick-borne encephalitis virus IgG antibody surveillance: vaccination- and infection-induced seroprevalences, south-western Germany, 2021. Euro Surveill. 2023, 28, 2200408. [Google Scholar] [CrossRef]
- Albinsson, B.; Hoffman, T.; Kolstad, L.; Bergström, T.; Bogdanovic, G.; Heydecke, A.; Hägg, M.; Kjerstadius, T; Lindroth, Y; Petersson, A.; et al. Seroprevalence of tick-borne encephalitis virus and vaccination coverage of tick-borne encephalitis, Sweden, 2018 to 2019. Euro Surveill. 2024, 29, 2300221. [Google Scholar] [CrossRef]
- Ackermann-Gäumann, R.; Eyer, C.; Vock, M.; Gowland, P.; Tinguely, C.; Leib, S.L.; Bori, M.; Buser, A.; Fontana, S.; Thierbach, J.; et al. Prevalence of anti-tick-borne encephalitis virus (TBEV) antibodies in Swiss blood donors in 2014-2015. Blood Transfus. 2023, 21, 100–109. [Google Scholar] [CrossRef]
- Paradowska-Stankiewicz, I.; Zbrzeźniak, J. Kleszczowe zapalenie mózgu w Polsce i na świecie. Ocena sytuacji epidemiologicznej KZM w Polsce w latach 2015–2019 w oparciu o dane pochodzące z nadzoru epidemiologicznego [Tick-borne encephalitis in Poland and worldwide. Assessment of the epidemiological situation of TBE in Poland in 2015–2019 based on epidemiological surveillance data]. National Institute of Public Health NIH—National Research Institute: Warsaw, Poland, 2021. Available online: https://www.pzh.gov.pl/wp-content/uploads/2021/03/KleszczoweZapalenieMoz (accessed on 10 February 2026).
- Girl, P.; Schindler, A.; Martin, S.; Dobler, G.; Borde, J.P. Surveillance of Tick-Borne Encephalitis Virus-Comparison of Vaccination- and Infection-Induced Seroprevalences in Lower Bavaria, Germany. J. Med. Virol. 2025, 97, e70514. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.F.; Gynthersen, R.M.M.; Ocias, L.F.; Sørensen, C.A.; Jensen, B.A.; Erikstrup, C.; Holm, D.K.; Sækmose, S.G.; Harritshøj, L.H.; Kolstad, L.; et al. A serosurvey examining exposure to Borrelia burgdorferi sensu lato and tick-borne encephalitis virus in Danish blood donors, August 2022. IJID Reg. 2024, 12, 100414. [Google Scholar] [CrossRef]
- Costantini, M.; Callegaro, A.; Beran, J.; Berlaimont, V.; Galgani, I. Predicted long-term antibody persistence for a tick-borne encephalitis vaccine: results from a modeling study beyond 10 years after a booster dose following different primary vaccination schedules. Hum. Vaccin. Immunother. 2020, 16, 2274–2279. [Google Scholar] [CrossRef] [PubMed]
- Beran, J.; Lattanzi, M.; Costantini, M.; Pammolli, A.; Galgani, I. Sustained antibody persistence for at least 15 years after a booster vaccination against tick-borne encephalitis following different primary vaccination schedules: Third 5-year follow-up. Vaccine 2023, 41, 3518–3524. [Google Scholar] [CrossRef]
- Freimane, Z.; Dobler, G.; Karelis, G.; Chitimia-Dobler, L.; Savicka, O.; Zavadska, D. Seroprevalence of Tick-Borne Encephalitis Virus in Latvia Using Standard and Subtype-Specific NS1-Based ELISA Assays. Pathogens 2025, 14, 1115. [Google Scholar] [CrossRef]
- Chan, K.R.; Ismail, A.A.; Thergarajan, G.; Raju, C.S.; Yam, H.C.; Rishya, M.; Sekaran, S.D. Serological cross-reactivity among common flaviviruses. Front. Cell. Infect. Microbiol. 2022, 12, 975398. [Google Scholar] [CrossRef]
- Waldeck, M.; Winqvist, N.; Henriksson, G.; Dyrdak, R.; Settergren, B.; Lindgren, P.E. Surveillance of tick-borne encephalitis in emerging risk areas in southern Sweden: a retrospective case finding study. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 13–22. [Google Scholar] [CrossRef]
- Kubicka-Russel, D.; Kopacz, A.; Sulkowska, E.; Łętowska, M.; Grabarczyk, P. Demographic changes in the Polish blood donors eligible for blood donation and screened for transfusion-transmitted infections (2005–2018). J. Transfus. Med. Hemost. 2023, 16, 39–64. [Google Scholar] [CrossRef]
Figure 1.
Epidemiological situation of TBE in Poland based on epidemiological surveillance data: A. Number of TBE cases (incidence) reported in Poland in 2015-2019 by Voivodeship; B. Number of TBE cases (incidence) reported in Poland in 2022 by voivodeship.
Figure 1.
Epidemiological situation of TBE in Poland based on epidemiological surveillance data: A. Number of TBE cases (incidence) reported in Poland in 2015-2019 by Voivodeship; B. Number of TBE cases (incidence) reported in Poland in 2022 by voivodeship.

Figure 2.
Algorithm of the study.

Figure 3.
Distribution obtained values: anti-TBEV IgG in screening test (A) and determined immunological status examined blood-donors (B) by age group and gender (C)* (M=male aged 18-39 years; M>40y.o.= male aged ≥40 years; F<40y.o = female aged 18-39 years; F> female aged ≥40 years) * Differentiation of post-infection due to TBEV and post-vaccination response was performed in 85% or reactive sera (174/205) and 31% of sera with borderline result of screening IgG ELISA.
Figure 3.
Distribution obtained values: anti-TBEV IgG in screening test (A) and determined immunological status examined blood-donors (B) by age group and gender (C)* (M=male aged 18-39 years; M>40y.o.= male aged ≥40 years; F<40y.o = female aged 18-39 years; F> female aged ≥40 years) * Differentiation of post-infection due to TBEV and post-vaccination response was performed in 85% or reactive sera (174/205) and 31% of sera with borderline result of screening IgG ELISA.


Table 1.
Results of screening test (anti-TBEV IgG ELISA) and determined immunological status by voivodeship.
Table 1.
Results of screening test (anti-TBEV IgG ELISA) and determined immunological status by voivodeship.
| Voivodeship | Classification based on 5years TBE incidence/ 100 000 inhabitants |
Screening anti-TBEV IgG | OR1 | 95% CI1 | p-value2 | Gender % Pos+borderline |
Age % Pos+borderline |
Status3 N |
|||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of pos+borderline/N examined samples | % pos+ borderline |
Female % |
Male % |
<40 y.o. % |
>40 y.o. % |
Inf/vac /other | |||||
| Dolnośląskie | Moderately affect | 12/605 | 2.0 | 0.99 | 0.44, 2.24 | 0.977 | 1.8 | 2.1 | 1.9 | 2.1 | 1/10/1 |
| Kujawsko-pomorskie | Less affected | 49/600 | 8.2 | 4.36 | 2.37, 8.66 | <0.001 | 8.4 | 8.1 | 9.9 | 2.6 | 0/15/34 |
| Lubelskie | Moderately affect | 25/600 | 4.2 | 2.13 | 1.08, 4.43 | 0.034 | 2.6 | 5.5 | 5.4 | 2.8 | 0/19/6 |
| Łódzkie | Moderately affect | 12/600 | 2.0 | 14 | - | 0 | 3.92 | 2.3 | 1.6 | 0/10/2 | |
| Małopolskie | Moderately affect | 26/609 | 4.3 | 2.19 | 1.12, 4.53 | 0.027 | 2.3 | 6.32 | 4.5 | 3.1 | 1/15/10 |
| Podkarpackie | Less affected | 22/624 | 3.5 | 1.79 | 0.89, 3.76 | 0.110 | 1.6 | 5.42 | 3.5 | 3.8 | 1/12/9 |
| Podlaskie | Highly affected | 67/703 | 9.5 | 5.16 | 2.87, 10.1 | <0.001 | 8.3 | 10.5 | 7.3 | 12.2 | 2/52/13 |
| Pomorskie | Less affected | 27/600 | 4.5 | 2.40 | 1.24, 4.94 | 0.012 | 2.8 | 5.2 | 5.0 | 4.0 | 2/16/9 |
| Zachodniopomorskie | Less affected | 32/600 | 5.3 | 2.76 | 1.45, 5.63 | 0.003 | 5.0 | 5.7 | 7 | 3.7 | 0/21/11 |
| In total | 272/5541 | 4.9 | 3.5 | 6.12 | 5.2 | 4.5 | 7/170/95 | ||||
| N= 5541, OR1=1.86; 95% CI1 (1.43, 2.43), p<0.001 |
N= 5541, OR1=0.86; 95% CI1 (0.67, 1.09), p>0.05 |
N=272, p<0.001 | |||||||||
N=number; Pos=positive; 1OR = Odds Ratio, CI1 = Confidence Interval; 2p <0.05 (statistically significant); Status3 : other = cross-reactions among Flaviviruses or unspecific reactions/unknown; inf = TBEV infection = positive anti-NS1 TBEV ELISA result; vac = IgG induced by anti-TBE structural antigens in vaccine = VNT or IIFA positive result; 4 – reference Voivodeship.
Table 2.
Statistical analysis of obtained results by classification of regions.
| N positive+bordeline / N examined samples | Inf/vac/other1 | Seroprevalence (95% CI2) | Seroprevalece excl other (95% CI) | Seroprevalence, infection (95% CI) | OR3 vs Less affected (seroprev excl other) | OR vs Less affected (seroprev, inf) | |
|---|---|---|---|---|---|---|---|
| Highly affected | 67/703 | 2/52/13 | 9.5% (7.5% - 11.9%) | 7.7% (5.8%-9.9%) | 0.3% (0.03% - 1.0%) | 2.8 (1.9-4.1), p<0.001 | 2.3 (0.2-20.1) p=>0.05 |
| Moderately affect | 75/2414 | 2/54/19 | 3.1% (2.4%-3.9%) | 2.3% (1.8%-3.0%) | 0.08% (0.001%-0.3%) | 0.84 (0.58-1.22), p>0.05 | 0.67 (0.06-5.85) p=>0.05 |
| Less affected | 130/2424 | 3/64/63 | 5.4% (4.5%-6.3%) | 2.8% (2.1%-3.5%) | 0.1% (0.003% - 0.4%) | 1 (ref.) | 1 (ref.) |
other 1 = cross-reactions among Flaviviruses or unspecific reactions/unknown; inf = TBEV infection = positive anti-NS1 TBEV ELISA result; vac = IgG induced by anti-TBE structural antigens in vaccine = VNT or IIFA positive result; CI2 = Confidence Interval 2P-value <0.05 (statistically significant); 3OR = Odds Ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



