Submitted:
07 March 2026
Posted:
10 March 2026
You are already at the latest version
Abstract
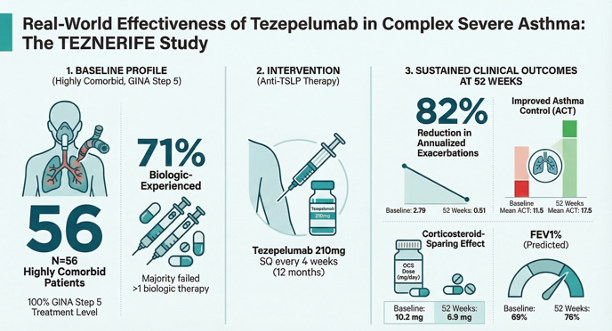
Background/Objectives: Severe asthma in routine practice often involves long-standing disease, multimorbidity, and prior biologic failure, settings underrepresented in pivotal tezepelumab trials. This study evaluated 52 week real world effectiveness and safety of tezepelumab in a highly comorbid, predominantly T2 high, biologic experienced severe asthma cohort from the Canary Islands. Methods: TEZNERIFE is a multicenter, retrospective phase IV study including consecutive adolescents and adults with GINA Step 5 severe uncontrolled asthma treated with tezepelumab 210 mg every 4 weeks for 12 months. Clinical outcomes, lung function, type 2 biomarkers, upper airway symptoms, and Biologics Asthma Response Score (BARS) were assessed at baseline, 26 weeks, and 52 weeks. Results: Fifty six patients (mean age 53.5 years, 71% female, mean asthma duration 30 years, 84% T2 high; 71% with ≥1 prior biologic) were analyzed. ACT improved from 11.5±3.7 to 15.9±4.7 at 26 weeks and 17.5±4.7 at 52 weeks (both p<0.0001), while annualized exacerbations declined from 2.79±2.0 to 0.50±0.72 and 0.51±0.89 (both p<0.0001). Maintenance oral corticosteroid dose fell from 10.2±8.3 to 6.9±2.4 mg/day at 52 weeks (p=0.014). FEV1% predicted increased from 69.3±19.2% to 75.3±17.7% and 76.2±20.6% (p=0.004 and p=0.001), and blood eosinophils decreased from 234±231 to 146±120 and 147±110 cells/µL (p=0.001 and p=0.013). At one year, 18.9% and 67.9% were classified as good and intermediate responders by BARS; 13.2% were insufficient responders. Two patients discontinued due to non serious adverse events while no treatment related serious events occurred. Conclusions: In this difficult to treat, multimorbid, biologic experienced population, tezepelumab achieved sustained improvements in asthma control, exacerbations, lung function, eosinophilic inflammation, and corticosteroid exposure over 52 weeks, supporting upstream alarmin inhibition as a versatile strategy in complex severe asthma.
Keywords:
severe uncontrolled asthma
; asthma phenotypes
; TSLP
; biologics
; tezepelumab
; precision medicine
1. Introduction
Severe asthma (SA) is a heterogeneous and potentially life-threatening condition in which symptoms persist despite optimized, guideline-directed therapy, including high-dose inhaled corticosteroids combined with additional controller medications such as long-acting bronchodilators. Although it affects a minority of individuals with asthma, SA accounts for a disproportionate burden of exacerbations, healthcare utilization, and impaired quality of life [1,2]. Patients frequently experience persistent dyspnea, nocturnal symptoms, and recurrent exacerbations requiring systemic corticosteroids or hospitalization. Pathophysiologically, SA is characterized by chronic airway inflammation, airway hyperresponsiveness, structural remodeling, and mucus hypersecretion, which may ultimately lead to fixed airflow limitation in a subset of patients [3]. Advances in asthma biology have demonstrated that severe asthma comprises multiple inflammatory phenotypes and endotypes rather than a single disease entity [4,5]. This paradigm shift has fostered precision medicine approaches and the development of biologic therapies targeting key type 2 (T2) mediators, including immunoglobulin E (IgE), interleukin (IL)-5, and the IL-4/IL-13 axis. [6]. These treatments have improved outcomes in selected populations; however, a substantial proportion of patients remain uncontrolled, partially responsive, or ineligible for currently available biologics that primarily target downstream T2 pathways [7,8,9,10].
Thymic stromal lymphopoietin (TSLP) has emerged as a pivotal epithelial-derived “alarmin” that links environmental triggers to both T2 and non-T2 airway inflammation. Released by airway epithelial and other structural cells in response to allergens, viral infections, pollutants, and mechanical injury, TSLP initiates and amplifies immune responses through activation of dendritic cells, type 2 innate lymphoid cells, mast cells, and other effector populations [11,12]. This cascade promotes T helper 2 (Th2) differentiation and the production of IL-4, IL-5, and IL-13. Elevated airway TSLP levels correlate with disease severity, persistent inflammation, and impaired lung function despite corticosteroid treatment. Importantly, accumulating evidence indicates that TSLP also contributes to non-allergic and T2-low inflammatory pathways, including Th1- and Th17-mediated responses and airway remodeling, positioning it as an upstream regulator across diverse SA endotypes [13,14].
Tezepelumab, a fully human monoclonal antibody targeting TSLP, inhibits its interaction with the TSLP receptor complex and thereby attenuates downstream inflammatory signaling. In pivotal randomized clinical trials involving patients with severe, uncontrolled asthma, tezepelumab significantly reduced exacerbation rates, improved lung function, and decreased biomarkers of airway inflammation—including fractional exhaled nitric oxide, blood eosinophils, and IgE—across a broad spectrum of baseline T2 biomarker levels [15]. These findings support the concept of TSLP inhibition as a broadly effective therapeutic strategy and expand the biologic armamentarium for severe asthma management [16,17,18,19]. Despite this robust clinical trial evidence, important uncertainties remain. Randomized controlled trials enroll selected populations under standardized conditions that may not fully reflect routine clinical practice. In real-world settings, patients often present with overlapping inflammatory endotypes, comorbidities, variable adherence, and distinct environmental exposures that may influence treatment response [20,21,22].
The Canary Islands represent such a setting, characterized by subtropical climatic conditions and the highest reported national prevalence of asthma and prescription rates of biologic therapies for SA in Spain [23]. Previous regional studies have described overlapping inflammatory subtypes in moderate and SA, reflecting a complex and heterogeneous inflammatory landscape [24,25,26]. However, data evaluating the real-world effectiveness of upstream TSLP inhibition in this population are currently lacking. Against this background, the present study aimed to assess the effectiveness and safety of monthly subcutaneous tezepelumab 210 mg at 26 and 52 weeks in patients with uncontrolled SA across different inflammatory endotypes in daily clinical practice.
2. Materials and Methods
2.1. Study Design and Setting
This phase IV, multicenter, retrospective, observational study (TEZNERIFE cohort) assessed the real-world effectiveness of upstream TSLP inhibition with tezepelumab in patients with uncontrolled SA. Participants received tezepelumab 210 mg administered subcutaneously every four weeks (q4w) for 12 consecutive months. Follow-up was conducted at the Severe Asthma Unit and Outpatient Allergy and Pneumology Clinic of Hospital Universitario de Canarias (Tenerife, Spain) and at the Severe Asthma Unit and Outpatient Pneumology Clinic of Hospital Universitario La Candelaria (Tenerife, Spain).
2.2. Participants
Eligible patients were adolescents and adults (>12 years) with clinician-confirmed severe refractory asthma according to the 2020 Global Initiative for Asthma (GINA) guidelines. Initiation of tezepelumab required uncontrolled disease, with no limitations on baseline biomarker levels, smoking status, or comorbidities, reflecting routine daily clinical practice. All patients underwent regular clinical follow-up every 3–6 months after biologic initiation. Pregnant or breastfeeding women were excluded. The study protocol was approved by the local Ethics Committee of CEIm Hospital Universitario de Canarias, Tenerife, Spain on October, 30 2025 (Acta 20/2025 Ordinaria VIRTUAL), and written informed consent was obtained from all participants or their legal guardians.
2.3. Data Collection and Clinical Outcomes
Data were retrospectively extracted from electronic medical records between January 2024 and January 2026. Collected variables included age, sex, age at asthma onset, atopy status, asthma-related comorbidities, exacerbation frequency, emergency department visits, hospitalizations, maintenance and burst oral corticosteroid (OCS) use, Asthma Control Test (ACT) score, spirometric parameters, fractional exhaled nitric oxide (FeNO), blood eosinophils, and serum IgE levels.
Clinically significant exacerbations were defined as worsening asthma requiring systemic corticosteroids for at least three days (or doubling the maintenance dose in patients on chronic OCS therapy) or leading to emergency department attendance or hospitalization [27]. Exacerbation rates during the 12 months before and after tezepelumab initiation were compared. Corticosteroid dependence was defined as daily OCS use for at least six consecutive months, and pulmonary function testing and FeNO measurements were performed according to global standards, and again compared at baseline, 6 months, and 12 months [28,29]. Both absolute and percent predicted values were evaluated, and only patients with paired measurements at each respective time point were included in longitudinal analyses.
2.4. Classification of Inflammatory Endotypes
Inflammatory endotype was determined at biologic initiation by the treating physician through an integrated assessment of clinical characteristics and available biomarkers, consistent with current recommendations [30,31]. In short, T2-high asthma was defined by the presence of at least one of the following: blood eosinophils ≥150 cells/μL at baseline or ≥300 cells/μL within the previous 12 months, FeNO ≥25 ppb, documented allergic sensitization with elevated total or specific IgE, or atopic comorbidities such as allergic rhinitis, nasal polyposis, or eczema. T2-low asthma was assigned when these features were consistently absent, defined by blood eosinophils <150 cells/μL, FeNO <25 ppb, and no evidence of allergic sensitization or atopic disease.
2.5. Laboratory and Serological Assessments
Peripheral blood samples were obtained from all participants, coded, stored at −40 °C, and analyzed using standardized laboratory procedures. Blood eosinophil counts were measured using automated hematological analysis. Total and specific IgE concentrations were determined using the Immulite 2000 Immunoassay System (Siemens Healthcare Diagnostics, Tarrytown, NY, USA). Sensitization to Dermatophagoides pteronyssinus and Dermatophagoides farinae was assessed. Total IgE was expressed in IU/mL and specific IgE in kUA/L, with values ≥0.35 kUA/L considered positive. Biomarker levels at 26 and 52 weeks were compared with baseline values.
2.6. Skin Prick Test
The skin prick test (SPT) was performed according to European Guidelines [32], enclosing a diagnostic panel (Inmunotek, Madrid, Spain) with standardized (Dermatophagoides pteronyssinus (D. pteronyssinus), and Dermatophagoides farinae (D. farinae) mite extracts. Histamine (10 mg/ml) and saline were used as positive and negative controls as usually. Following everyday practice, antihistamines were withdrawn a week prior to the SPT, and wheal diameters were immediately measured after 20 minutes and those greater than 3 mm were regarded as positive.
2.7. Definition of Treatment Response
Treatment response was evaluated at 6 and 12 months using the Biologics Asthma Response Score (BARS). The composite score incorporates reduction in exacerbation rate, reduction in daily OCS dose, and improvement in ACT score. Each criterion is scored as 2 (good), 1 (intermediate), or 0 (insufficient response), and the final score is calculated by dividing the total points by the number of applicable criteria. Thresholds for response classification were ≥1.5 for good, 0.5–1.33 for intermediate, and <0.5 for insufficient response [33]. An extended version additionally incorporated lung function improvement. FEV₁ normalization was defined as an increase of at least 100 mL and attainment of ≥80% predicted when baseline FEV₁ was <80% predicted. Criteria not applicable at baseline were excluded from the denominator, as elsewhere described [34].
2.8. Statistical Analysis
Continuous variables are presented as mean ± standard deviation or median (interquartile range), depending on distribution. Categorical variables are expressed as frequencies and percentages. Normality was assessed using the Kolmogorov–Smirnov test. Longitudinal changes in clinical and functional outcomes were analyzed using paired Student’s t-tests or Wilcoxon signed-rank tests, as appropriate. Effect sizes were calculated to estimate the magnitude of change. A two-sided p-value <0.05 was considered statistically significant. All statistical analyses were conducted using GraphPad Prism version 10.0.0 (GraphPad Software, La Jolla, California, USA).
3. Results
3.1. Demographic and Clinical Characteristics of Subjects at Baseline
A total of 62 patients with severe uncontrolled asthma receiving tezepelumab 210 mg q4w were screened for the study. Six subjects were subsequently excluded or discontinued: four were lost to follow-up, and two ceased tezepelumab therapy due to adverse events (AEs). Specifically, one patient withdrew at week 24 due to musculoskeletal and connective tissue disorders -arthromyalgias- while the second stopped at week 32 due to recurrent urinary tract infections (Figure 1). No serious adverse events (SAEs) related to the treatment were recorded during the study follow-up period.
Therefore, a total of 56 patients with severe uncontrolled asthma receiving biologic therapy were finally included in the study (Table 1). The mean age was 53.47 years (SD 13.3), with 3 patients (5.35%) aged <20 years and 53 (94.64%) aged ≥20 years. The majority were female (71.42%), while 28.58% were male. The mean body mass index (BMI) was 30.1 kg/m² (SD 6.53), indicating that, on average, the population was in the obese range. The mean duration of asthma was 29.98 years (SD 15.44), and 26 patients (46.42%) reported childhood-onset asthma. A family history of atopy was present in 41 patients (80.32%). Most patients exhibited a T2-high inflammatory phenotype (83.82%), whereas 16.08% were classified as T2-low. All patients (100%) were treated at Global Initiative for Asthma (GINA) Step 5, and 6 (10.74%) were receiving maintenance daily oral corticosteroids at baseline.
Regarding prior biologic exposure before initiation of tezepelumab, 16 patients (28.57%) were biologic-naïve. Eighteen (32.14%) had received one prior biologic, 14 (25.0%) had received two, 6 (10.71%) had received three, and 2 patients (3.56%) had received four or more prior biologics (one patient each with four and five previous agents). In terms of smoking status, 37 patients (66.07%) were never smokers, 16 (28.57%) were former smokers, and 3 (5.35%) were current smokers. Bronchiectasis confirmed by chest CT was present in 4 patients (7.1%). Sensitization to house dust mite (SPT+ HDM) was documented in 25 patients (44.64%). Comorbidities were common. Allergic rhinitis was reported in 27 patients (48.21%), atopic dermatitis in 4 (7.14%), chronic rhinosinusitis with nasal polyposis (CRSwNP) in 5 (8.09%), chronic rhinosinusitis without polyposis (CRSsNP) in 2 (3.57%), and nonsteroidal anti-inflammatory drug–exacerbated respiratory disease (NERD) in 2 (3.57%). Gastroesophageal reflux disease (GERD) was present in 15 patients (26.78%), depression in 9 (16.07%), and obstructive sleep apnea in 13 (23.21%). Overall, the cohort was characterized by long-standing, predominantly T2-high, severe asthma with a high burden of atopy and comorbid conditions.
3.2. Asthma Control and Exacerbations
Treatment with subcutaneous tezepelumab 210 mg every 4 weeks was associated with a rapid and sustained improvement in overall asthma control (Table 2).
Mean ACT scores increased from 11.52 ± 3.67 at baseline (Figure 2), consistent with poorly controlled disease, to 15.89 ± 4.73 at 26 weeks and 17.48 ± 4.73 at 52 weeks (both p < 0.0001 vs. baseline). The progressive rise in ACT values over time reflects a clinically meaningful shift toward better symptom control during follow-up. In parallel, exacerbation burden was markedly reduced. The annualized number of asthma exacerbations declined from 2.79 ± 2.0 at baseline to 0.50 ± 0.72 at 26 weeks and 0.51 ± 0.89 at 52 weeks (both p < 0.0001). This substantial and sustained reduction underscores the treatment’s effectiveness in preventing acute disease worsening over one year of observation.
3.3. Oral Corticosteroid Exposure
Baseline maintenance oral corticosteroid (OCS) use averaged 10.2 ± 8.3 mg/day. A numerical decrease was observed after 26 weeks (8.41 ± 6.2 mg/day; p = 0.1831), followed by a statistically significant reduction at 52 weeks to 6.9 ± 2.4 mg/day (p = 0.0140 vs. baseline). These findings indicate a delayed but meaningful corticosteroid-sparing effect emerging with longer treatment duration.
3.4. Lung Function
Pulmonary function parameters improved during tezepelumab therapy. Mean FVC increased from 2940 ± 992 mL at baseline to 3289 ± 1234 mL at 26 weeks (p = 0.0161) and remained elevated at 3214 ± 1148 mL at 52 weeks (p = 0.0125).
FEV₁ rose from 2061 ± 895 mL at baseline to 2206 ± 923 mL at 26 weeks (p = 0.0572) and further to 2316 ± 958 mL at 52 weeks (Figure 3), reaching statistical significance at one year (p = 0.0384). Consistently, FEV₁% predicted improved from 69.31 ± 19.2% to 75.32 ± 17.68% at 26 weeks (p = 0.0043) and 76.24 ± 20.63% at 52 weeks (p = 0.0012). Together, these data demonstrate early improvements in ventilatory capacity with sustained gains over 12 months.
3.5. Type 2 Inflammatory Biomarkers
Markers of type 2 inflammation showed differential patterns of response. Blood eosinophil counts declined significantly from 234 ± 231 cells/μL at baseline to 146 ± 120 cells/μL at 26 weeks (p = 0.0012) and 147 ± 110 cells/μL at 52 weeks (p = 0.0125), indicating durable suppression throughout follow-up.
FeNO decreased numerically from 29.17 ± 19.9 ppb to 23.93 ± 15.42 ppb at 26 weeks (p = 0.0889) and was 26.04 ± 16.87 ppb at 52 weeks (p = 0.1960), without statistical significance. Total IgE levels also declined from 354 ± 549 IU/mL at baseline to 240 ± 382 IU/mL at 26 weeks (p = 0.1324) and 234 ± 409 IU/mL at 52 weeks (p = 0.2356). Similarly, allergen specific IgE to D. pteronyssinus and D. farinae showed numerical reductions at 12 months (21.17 ± 33.0 to 17.15 ± 4.32 kUA/L, p = 0.1833; and 17.1 ± 30.21 to 13.58 ± 4.7 kUA/L, p = 0.1499, respectively), without reaching statistical significance.
3.6. Upper Airway Outcomes and Composite Response
Among patients with concomitant chronic rhinosinusitis with nasal polyps (n = 6), SNOT-22 scores decreased from 59.94 ± 19.36 at baseline to 55.67 ± 23.69 at 26 weeks (p = 0.5171) and to 46.76 ± 26.8 at 52 weeks (p = 0.373). Although statistical significance was not achieved, the reduction at one year exceeded the minimal clinically important difference (>8.9 points), suggesting potential symptomatic benefit in upper airway disease.
The combined Biologics Asthma Response Score (BARS) further characterized treatment response. Mean scores were 0.95 ± 0.53 at 26 weeks and 1.06 ± 0.55 at 52 weeks (p = 0.0501). At 26 weeks, 19.64% of patients were classified as good responders (≥1.5), 69.64% as intermediate responders (0.5–1.33), and 10.71% as insufficient responders (<0.5). At 52 weeks, corresponding proportions were 18.86%, 67.92%, and 13.2%, respectively, indicating a predominantly intermediate-to-good response profile maintained over time.
4. Discussion
This real-world longitudinal study assessed the effectiveness of tezepelumab in a highly complex population with severe uncontrolled asthma characterized by long-standing disease, substantial comorbidity burden, frequent prior biologic exposure, and universal GINA Step 5 treatment. The cohort reflects a difficult-to-treat phenotype typical of tertiary care settings, including obesity, overlapping upper and lower airway disease, psychiatric and sleep-related comorbidities, and considerable cumulative corticosteroid exposure—features often underrepresented in pivotal trials [15,17]. Within this challenging clinical context, tezepelumab was associated with clinically meaningful improvements across multiple domains over 52 weeks, consistent with emerging real-world data in similarly heterogeneous populations [35,36,37].
Asthma control improved markedly and was accompanied by a profound reduction in exacerbation frequency. At baseline, patients exhibited very poor symptom control (mean ACT 11.5) and frequent exacerbations (mean 2.79/year), reflecting substantial disease instability. Over 12 months, ACT scores increased progressively, while exacerbation rates declined by approximately 80%, with stability between 26 and 52 weeks. These findings are comparable to the 60–70% reductions reported in randomized trials and recent real-world studies [38,39,40]. Given that many patients had previously failed one or more biologic therapies, the magnitude and durability of exacerbation reduction are particularly noteworthy and align with evidence demonstrating benefit in biologic-experienced and low-eosinophil populations.
A corticosteroid-sparing effect further supports the clinical relevance of these outcomes. Although reduction in maintenance OCS dose did not reach statistical significance at 26 weeks, a significant decrease was observed at one year, likely reflecting cautious tapering in patients with long-standing steroid dependence and multimorbidity [18,41,42,43]. Even moderate reductions in chronic OCS exposure are clinically meaningful in this population, given the high prevalence of obesity, GERD, obstructive sleep apnea, and depression—conditions closely associated with cumulative corticosteroid toxicity and identified as dominant traits limiting remission [44,45]. The observed reduction therefore represents an important step toward limiting long-term treatment-related harm [46].
Lung function improved early and was sustained throughout follow-up. FVC increased significantly at both 26 and 52 weeks, while FEV₁ and FEV₁% predicted showed progressive gains reaching significance at one year. Considering the nearly three-decade mean disease duration and the presence of structural airway comorbidities in some patients, these changes are clinically relevant [47]. In long-standing asthma, airflow limitation may include a partially fixed component related to airway remodeling; thus, sustained functional improvement suggests that upstream TSLP inhibition may attenuate inflammatory mechanisms contributing to persistent airflow obstruction.
Biomarker analyses provide additional mechanistic insight. Blood eosinophil counts declined significantly and remained suppressed over 12 months, indicating sustained modulation of type 2 inflammation. In contrast, FeNO and total IgE showed only numerical, non-significant reductions. This dissociation between clinical improvement and certain biomarker changes likely reflects biological heterogeneity, including both T2-high and T2-low phenotypes as well as prior exposure to IL-5– or IgE-targeted therapies. Notably, clinical response was not dependent on marked reductions in all conventional type 2 biomarkers, supporting the broader upstream mechanism of TSLP inhibition [48]. In the subgroup with CRSwNP, SNOT-22 scores decreased beyond the minimal clinically important difference at 52 weeks. Although statistical significance was not reached—likely due to limited sample size—the magnitude and direction of change are clinically meaningful. The shared epithelial-driven inflammatory pathways underlying asthma and sinonasal disease provide a biological rationale for parallel improvement under TSLP inhibition, warranting confirmation in larger dedicated studies.
The composite BARS analysis showed that most patients achieved an intermediate or good response, with a stable distribution between 26 and 52 weeks. Nearly one-fifth fulfilled criteria for a good response despite extensive prior biologic exposure, while only a small proportion were classified as insufficient responders. These findings highlight the broad applicability of tezepelumab across heterogeneous phenotypes and suggest a durable rather than transient therapeutic effect [49]. Safety findings were consistent with established clinical experience [50,51]. Two patients discontinued therapy due to non-serious adverse events, and no treatment-related serious adverse events were reported. In a multimorbid population with high healthcare utilization, this tolerability profile supports the feasibility of long-term use in routine practice.
The study’s strengths include its real-world design and the inclusion of patients with multimorbidity, smoking history, structural lung disease, and prior biologic exposure, enhancing external validity. Predefined longitudinal assessments at 26 and 52 weeks allowed evaluation of both early and sustained treatment effects. However, the modest sample size, absence of a control group, and limited statistical power restrict the interpretation of subgroup analyses, particularly for upper airway outcomes and comparisons between biologic-experienced versus biologic-naïve patients and T2-high versus T2-low SA s phenotypes. Residual confounding related to concomitant therapies or comorbidity management cannot be excluded. Nevertheless, the consistent improvements observed across symptom control, exacerbation rates, lung function, and eosinophilic inflammation support the robustness of the findings and align with results from larger randomized and real-world studies.
5. Conclusions
In this difficult-to-treat, clinically heterogeneous severe asthma population with substantial prior biologic exposure and high comorbidity burden, tezepelumab was associated with sustained improvements in asthma control, exacerbation frequency, lung function, eosinophilic inflammation, and corticosteroid exposure over 52 weeks. These data extend randomized trial evidence into a complex real-world setting and support upstream epithelial alarmin inhibition as an effective and versatile strategy in SA management.
Author Contributions
Conceptualization, RG-P, PP-G and ID-G; methodology, RG-P, and PP-G; software, PP-G; validation and formal analysis, PP-G; investigation, RG-P, PP-G, ID-G, HI-F, HG-E and SG-G; resources, RG-P, and PP-G; data curation, PP-G, ID-G, HI-F, HG-E and SG-G; writing—original draft preparation, RG-P; writing—review and editing, RG-P and PP-G; project administration PP-G; funding acquisition RG-P, PP-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Fundación Canaria Instituto de Investigación Sanitaria de Canarias (FIISC), Servicio Canario de Salud, grant number OA17/042.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the local Institutional Ethics Committee CEIC Hospital Universitario de Canarias, Tenerife, Spain on October 30 2025 (Acta 20/2025 Ordinaria VIRTUAL) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from Servicio Canario de Salud but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Servicio Canario de Salud.
Acknowledgments
The authors acknowledge the use of OpenAI’s ChatGPT for refining the manuscript text and NotebookLM (Google, Mountain View, CA, USA) for the visual synthesis of study population characteristics and the development of the CONSORT-style flow diagram. All final analyses and interpretations were conducted and verified by the authors.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| SA | Severe Asthma |
| TSLP | Thymic stromal lymphopoietin |
| CRSwNP | Chronic Rinosinusitis with Nasal Polyposis |
| BARS | Biologics Asthma Response Score |
| OCS | Oral Corticosteroid |
| FeNO | Fractional exhaled Nitric Oxide |
References
- https://www.asthmaandlung.org.uk/conditions/severe-asthma/what-severe-asthma-how-it-diagnosed Last visited February 20, 2026.
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020 Oct 17;396(10258):1204-1222. Erratum in: Lancet. 2020 Nov 14;396(10262):1562. doi: 10.1016/S0140-6736(20)32226-1. [CrossRef]
- https://ginasthma.org/ Last visited February 4, 2026.
- Haldar, P; Pavord, ID; Shaw, DE; Berry, MA; Thomas, M; Brightling, CE; et al. Cluster analysis and clinical asthma phenotypes. Am J Respir Crit Care Med. 2008, 178(3), 218-24. [Google Scholar] [CrossRef]
- Moore, WC; Meyers, DA; Wenzel, SE; Teague, WG; Li, H; Li, X; et al. Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program. Am J Respir Crit Care Med. 2010, 181(4), 315-23. [Google Scholar] [CrossRef]
- Holguin, F; Cardet, JC; Chung, KF; Diver, S; Ferreira, DS; Fitzpatrick, A; et al. Management of severe asthma: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J 2020, 55(1), 1900588. [Google Scholar] [CrossRef] [PubMed]
- Gyawali, B; Georas, SN; Khurana, S. Biologics in severe asthma: a state-of-the-art review. Eur Respir Rev. 2025, 34(175), 240088. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Couillard, S; Jackson, DJ; Pavord, ID; Wechsler, ME. Choosing the Right Biologic for the Right Patient With Severe Asthma. Chest 2025, 167(2), 330–342. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Al-Shaikhly, T; Norris, MR; Dennis, EH; Liu, G; Craig, TJ. Comparative Impact of Asthma Biologics: A Nationwide US Claim-Based Analysis. J Allergy Clin Immunol Pract. 2024, 12(6), 1558–1567. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, BJ; Greig, R; Chan, R; Kuo, CR; Jackson, C. Head-To-Head Comparison of Biologic Efficacy in Asthma: What Have We Learned? Allergy 2025, 80(5), 1226–1241. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, Y; Wang, W; Lv, Z; Li, Y; Chen, Y; Huang, K; et al. Elevated Expression of IL-33 and TSLP in the Airways of Human Asthmatics In Vivo: A Potential Biomarker of Severe Refractory Disease. J Immunol. 2018, 200(7), 2253–2262. [Google Scholar] [CrossRef] [PubMed]
- Duchesne, M; Okoye, I; Lacy, P. Epithelial cell alarmin cytokines: Frontline mediators of the asthma inflammatory response. Front Immunol. 2022, 13, 975914. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Diver S, Khalfaoui L, Emson C, Wenzel SE, Menzies-pow A, Wechsler ME, et al. Effect of tezepelumab on airway inflammatory cells, remodelling, and hyperresponsiveness in patients with moderate-to-severe uncontrolled asthma (CASCADE): a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Respir Med. 2021 Nov;9(11):1299-1312. Epub 2021 Jul 10. Erratum in: Lancet Respir Med. 2021 Nov;9(11):e106. doi: 10.1016/S2213-2600(21)00446-X. [CrossRef] [PubMed]
- Menzies-Gow A, Wechsler ME, Brightling CE, Korn S, Corren J, Israel E, et al. Long-term safety and efficacy of tezepelumab in people with severe, uncontrolled asthma (DESTINATION): a randomised, placebocontrolled extension study. Lancet Respir Med. 2023 May;11(5):425-438. Epub 2023 Jan 23. Erratum in: Lancet Respir Med. 2023 Mar;11(3):e25. doi: 10.1016/S2213-2600(23)00048- 6. [CrossRef]
- Menzies-Gow, A; Colice, G; Griffiths, JM; Almqvist, G; Ponnarambil, S; Kaur, P; et al. NAVIGATOR: a phase 3 multicentre, randomized, double-blind, placebo-controlled, parallel-group trial to evaluate the efficacy and safety of tezepelumab in adults and adolescents with severe, uncontrolled asthma. Respir Res. 2020, 21(1), 266. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Menzies-Gow, A; Corren, J; Bourdin, A; et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N Engl J Med. 2021c, 384, 1800–1809. [Google Scholar] [CrossRef]
- Corren, J; Garcia Gil, E; Griffiths, JM; et al. Tezepelumab improves patient-reported outcomes in patients with severe, uncontrolled asthma in PATHWAY. Annual Allergy Asthma Immunol. 2021, 126, 187–193. [Google Scholar] [CrossRef]
- Wechsler, ME; Colice, G; Griffiths, JM; Almqvist, G; Skärby, T; Piechowiak, T; et al. SOURCE: a phase 3, multicentre, randomized, double-blind, placebo-controlled, parallel group trial to evaluate the efficacy and safety of tezepelumab in reducing oral corticosteroid use in adults with oral corticosteroid dependent asthma. Respir Res. 2020, 21(1), 264. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Edris, A; De Feyter, S; Maes, T; Joos, G; Lahousse, L. Monoclonal antibodies in type 2 asthma: a systematic review and network meta-analysis. Respir Res. 2019, 20(1), 179. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nagase, H; Suzukawa, M; Oishi, K; Matsunaga, K. Biologics for severe asthma: The real-world evidence, effectiveness of switching, and prediction factors for the efficacy. Allergol Int. 2023, 72(1), 11–23. [Google Scholar] [CrossRef] [PubMed]
- Casas Deza, D; Larrubia Domínguez, C; Pascual Oliver, A; Polo Cuadro, C; Yagüe; et al. Patients Included in Clinical Trials of Biological Drugs for Inflammatory Bowel Disease Do Not Represent the Real-World Population. Am J Gastroenterol 2025. [Google Scholar] [CrossRef] [PubMed]
- Pelaia, C; Giacalone, A; Ippolito, G; Pastore, D; Maglio, A; Piazzetta, GL; et al. Difficult-To-Treat and Severe Asthma: Can Real-World Studies On Effectiveness of Biological Treatments Change the Lives of Patients? Pragmat Obs Res 2024, 15, 45–51. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Casas-Maldonado, F; Álvarez-Gutiérrez, FJ; Blanco-Aparicio, M; Domingo-Ribas, C; Cisneros-Serrano, C; Soto-Campos, G; et al. Monoclonal antibody treatment for severe uncontrolled asthma in Spain: analytical map. J Asthma 2022, 59(10), 1997–2007. [Google Scholar] [CrossRef] [PubMed]
- González-Pérez, R; Poza-Guedes, P; Sánchez-Machín, I. Asma en Canarias: derivación centrada en el paciente [Asthma in the Canary Islands: Patient-Centered Derivation Criteria]. Open Respir Arch. 2024, 6(1), 100308, Spanish. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Martin-Gonzalez, E; Perez-Garcia, J; Martin-Almeida, M; Hernández-Pérez, JM; González-Pérez, R; Sardón, O; et al. Genome-wide Association Study of Asthma Exacerbations in the Spanish Population. Arch Bronconeumol 2025, 61(8), 490–494, English, Spanish. [Google Scholar] [CrossRef] [PubMed]
- González-Pérez, R; Poza-Guedes, P; Mederos-Luis, E; Sánchez-Machín, I. Real-Life Performance of Mepolizumab in T2-High Severe Refractory Asthma with the Overlapping Eosinophilic-Allergic Phenotype. Biomedicines 2022, 10(10), 2635. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bourdin, A; Bjermer, L; Brightling, C; Brusselle, GG; Chanez, P; Chung, KF; et al. ERS/EAACI statement on severe exacerbations in asthma in adults: facts, priorities and key research questions. Eur Respir J 2019, 54(3), 1900900. [Google Scholar] [CrossRef] [PubMed]
- Cooper, BG; Stocks, J; Hall, GL; Culver, B; Steenbruggen, I; Carter, KW; et al. The Global Lung Function Initiative (GLI) Network: bringing the world's respiratory reference values together. Breathe (Sheff) 2017, 13(3), e56–e64. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Graham, BL; Steenbruggen, I; Miller, MR; Barjaktarevic, IZ; Cooper, BG; Hall, GL; et al. H Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med 2019, 200(8), e70–e88. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sim, S; Choi, Y; Park, HS. Update on Inflammatory Biomarkers for Defining Asthma Phenotype. Allergy Asthma Immunol Res 2024, 16(5), 462–472. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bourdin, A; Brusselle, G; Couillard, S; Fajt, ML; Heaney, LG; Israel, E; et al. Phenotyping of Severe Asthma in the Era of Broad-Acting Anti-Asthma Biologics. J Allergy Clin Immunol Pract. 2024, 12(4), 809–823. [Google Scholar] [CrossRef] [PubMed]
- Heinzerling, L; Mari, A; Bergmann, KC; Bresciani, M; Burbach, G; Darsow, U; et al. The skin prick test - European standards. Clin Transl Allergy 2013, 3(1), 3. [Google Scholar] [CrossRef] [PubMed]
- Milger, K; Korn, S; Feder, C; Fuge, J; Mühle, A; Schütte, W; et al. Criteria for evaluation of response to biologics in severe asthma - the Biologics Asthma Response Score (BARS). Pneumologie 2025, 79(6), 439–451. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Milger, K; Suhling, H; Skowasch, D; Holtdirk, A; Kneidinger, N; Behr, J; et al. Response to Biologics and Clinical Remission in the Adult German Asthma Net Severe Asthma Registry Cohort. J Allergy Clin Immunol Pract. 2023, 11(9), 2701–2712.e2. [Google Scholar] [CrossRef] [PubMed]
- Pelaia, C; Greco, M; Iaccino, E; Crimi, C; Biafora, M; Dragone, F; et al. Short-term therapeutic effectiveness of tezepelumab in patients with severe asthma: A real-world study. Int Immunopharmacol. 2025, 162, 115185. [Google Scholar] [CrossRef] [PubMed]
- Miralles-López, JC; Bravo-Gutierrez, FJ; Andújar-Espinosa, R; Castilla-Martínez, M; Díaz-Chantar, C; Ramírez-Hernández, M; et al. RE-ASGRAMUR Group. Real-life effectiveness of tezepelumab in severe asthma. Allergol Immunopathol (Madr) 2025, 53(2), 163–173. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M; Buhl, R; Corren, J; Hanania, NA; Kim, H; Korn, S; et al. Tezepelumab in patients with allergic and eosinophilic asthma. Allergy 2024, 79(5), 1134–1145. [Google Scholar] [CrossRef] [PubMed]
- Aslam, MMS; Senn, R; Bagheri, A; Harwood, H; Troost, JP; Lugogo, NL; Mohan, A. Novel Real-World Insights Into Tezepelumab Effectiveness in Steroid-Dependent Asthma. J Asthma Allergy 2025, 18, 1835–1839. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Biener, L; Mümmler, C; Hinze, CA; Suhling, H; Korn, S; Fisser, C; Biener, A; Pizarro, C; Lenoir, A; Hackl, C; Skowasch, D; Milger, K. Real-World Data on Tezepelumab in Patients With Severe Asthma in Germany. J Allergy Clin Immunol Pract. 2024, 12(9), 2399–2407.e5. [Google Scholar] [CrossRef] [PubMed]
- Gates, J; Haris, F; Cefaloni, F; Khooshemehri, P; Green, L; Fernandes, M; Thomson, L; Roxas, C; Lam, J; d'Ancona, G; Nanzer, AM; Dhariwal, J; Jackson, DJ. Clinical and Biological Remission With Tezepelumab: The Real-World Response in Severe Uncontrolled Asthma. Allergy 2025, 80(6), 1669–1676. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Panettieri, R, Jr.; Lugogo, N; Corren, J; Ambrose, CS. Tezepelumab for Severe Asthma: One Drug Targeting Multiple Disease Pathways and Patient Types. J Asthma Allergy 2024, 17, 219–236. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hirai, K; Uehara, S; Shirai, T; Akamatsu, T; Itoh, K. Tezepelumab Targeting Thymic Stromal Lymphopoietin Enhances Steroid Sensitivity in Patients With Severe Asthma. Allergy 2026, 81(1), 277–280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pelaia, C; Greco, M; Iaccino, E; Crimi, C; Biafora, M; Dragone, F; et al. Short-term therapeutic effectiveness of tezepelumab in patients with severe asthma: A real-world study. Int Immunopharmacol. 2025, 162, 115185. [Google Scholar] [CrossRef] [PubMed]
- Mailhot-Larouche, S; Celis-Preciado, C; Heaney, LG; Couillard, S. Identifying super-responders: A review of the road to asthma remission. Ann Allergy Asthma Immunol 2025, 134(1), 31–45. [Google Scholar] [CrossRef] [PubMed]
- Shackleford, A; Heaney, LG; Redmond, C; McDowell, PJ; Busby, J. Clinical remission attainment, definitions, and correlates among patients with severe asthma treated with biologics: a systematic review and meta-analysis. Lancet Respir Med. 2025, 13(1), 23–34. [Google Scholar] [CrossRef] [PubMed]
- Furci, F; Scaramozzino, MU; Talesa, GR; Pelaia, C. Connections and Unmet Needs: Severe Asthma Biologics and Osteoporosis. Biomedicines 2025, 13(1), 197. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lupia, C; Battaglia, C; Pastore, D; Lee, Y; Piazzetta, GL; Chiarella, E; et al. Tezepelumab in severe asthma: chest computed tomography assessment of airway remodeling and clinical remission. Front Pharmacol. 2026, 17, 1757754. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Corren, J; Pham, TH; Garcia Gil, E; Sałapa, K; Ren, P; Parnes, JR; et al. Baseline type 2 biomarker levels and response to tezepelumab in severe asthma. Allergy 2022, 77(6), 1786–1796. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wechsler, ME; Brusselle, G; Virchow, JC; Bourdin, A; Kostikas, K; Llanos, JP; et al. Clinical response and on-treatment clinical remission with tezepelumab in a broad population of patients with severe, uncontrolled asthma: results over 2 years from the NAVIGATOR and DESTINATION studies. Eur Respir J 2024, 64(6), 2400316. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Boada-Fernández-Del-Campo, C; García-Sánchez-Colomer, M; Fernández-Quintana, E; Poza-Guedes, P; Rolingson-Landaeta, JL; Sánchez-Machín, I; et al. Real-World Safety Profile of Biologic Drugs for Severe Uncontrolled Asthma: A Descriptive Analysis from the Spanish Pharmacovigilance Database. J Clin Med. 2024, 13(14), 4192. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jappe, U; Bergmann, KC; Brinkmann, F; Faihs, V; Gülsen, A; Klimek, L; et al. Biologics in allergology and clinical immunology: Update on therapies for atopic diseases, urticaria, and angioedema and on safety aspects focusing on hypersensitivity reactions. Allergol Select 2024, 8, 365–406. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
CONSORT Flow diagram of the TEZNERIFE cohort. This diagram illustrates the patient selection process, beginning with 62 initially screened subjects with severe uncontrolled asthma. It details the reasons for exclusion, including four patients lost to follow-up and two patients who discontinued treatment due to specific non-serious adverse events (arthromyalgias and recurrent urinary tract infections), resulting in a final cohort of 56 patients for the 52-week longitudinal effectiveness analysis.
Figure 1.
CONSORT Flow diagram of the TEZNERIFE cohort. This diagram illustrates the patient selection process, beginning with 62 initially screened subjects with severe uncontrolled asthma. It details the reasons for exclusion, including four patients lost to follow-up and two patients who discontinued treatment due to specific non-serious adverse events (arthromyalgias and recurrent urinary tract infections), resulting in a final cohort of 56 patients for the 52-week longitudinal effectiveness analysis.

Figure 2.
Evolution of asthma control measured by the Asthma Control Test (ACT) in subjects with severe refractory asthma before and after 52-week treatment with tezepelumab 210 mg every 4 weeks. Asterisks indicate statistical significance (**** p < 0.001).
Figure 2.
Evolution of asthma control measured by the Asthma Control Test (ACT) in subjects with severe refractory asthma before and after 52-week treatment with tezepelumab 210 mg every 4 weeks. Asterisks indicate statistical significance (**** p < 0.001).

Figure 3.
Evolution of pulmonary function (FEV1 in mL) before and after 52-week treatment with tezepelumab 210 mg every 4 weeks. Asterisks indicate statistical significance (***p = 0.0384).
Figure 3.
Evolution of pulmonary function (FEV1 in mL) before and after 52-week treatment with tezepelumab 210 mg every 4 weeks. Asterisks indicate statistical significance (***p = 0.0384).


Table 1.
Demographic and clinical characteristics of patients prior to commencement of Tezepelumab 210 mg every 4-week.
Table 1.
Demographic and clinical characteristics of patients prior to commencement of Tezepelumab 210 mg every 4-week.
| Variable | Severe Uncontrolled Asthma |
|---|---|
| N (%) | 56 (100) |
| Age (y.o.) mean (SD) | 53.47 (±13.3) |
| <20 y.o. (%) | 3 (5.35) |
| ≥20 y.o. (%) | 53 (94.64) |
| Female Sex (%) | 40 (71.42) |
| BMI mean (SD) | 30.1 (±.53) |
| Duration of Asthma (y) mean (SD) | 29.98 (±15.44) |
| Asthma Onset at Childhood (%) | 26 (46.42) |
| Family History of Atopy (%) | 41 (80.32) |
| Asthma phenotype (T2 High/T2 Low,%) | 83,82/16,08 |
| GINA Step 5 Treatment Level (%) | 56 (100) |
| Daily Oral Corticosteroids (%) | 6 (10.74) |
| Former Use of Severe Asthma Biologics before Tezepelumab (%) | 40 (71.4) |
| None (%) | 16 (28.57) |
| One (%) | 18 (32.14) |
| Two (%) | 14 (25.0) |
| Three (%) | 6 (10.71) |
| Four (%) | 1 (1.78) |
| Five (%) | 1 (1.78) |
| Smoking | |
| Never smoker (%) | 37 (66.07) |
| Former smoker (%) | 16 (28.57) |
| Smoker (%) | 3 (5.35) |
| Bronchiectasis (Chest CT Scanner)(%) | 4 (7.1) |
| SPT+ HDM (%) | 25 (44.64) |
| Allergic Rhinitis (%) | 27 (48.21) |
| Atopic Dermatitis (%) | 4 (7.14) |
| Chronic Rinosinusitis with Nasal Polyposis (%) | 5 (8.09) |
| NERD (%) | 2 (3.57) |
| Chronic Rinosinusitis (%) | 2 (3.57) |
| GERD (%) | 15 (26.78) |
| Depression (%) | 9 (16.07) |
| Obstructive Sleep Apnea Syndrome (%) | 13 (23.21) |
SD: Standard deviation of the mean. SPT: Skin Prick Test. HDM: House dust mites (Dermatophagoides spp.) NERD: NSAID-exacerbated respiratory disease. GERD: Gastroesophageal reflux disease.
Table 2.
Longitudinal assessment of patients with severe uncontrolled asthma at baseline and after 26 and 52-week treatment with subcutaneous tezepelumab 210 mg every 4-week. SNOT-22 evaluation applies only for patients (n=6) afflicted with comorbid chronic rhinosinusitis with nasal polyps.
Table 2.
Longitudinal assessment of patients with severe uncontrolled asthma at baseline and after 26 and 52-week treatment with subcutaneous tezepelumab 210 mg every 4-week. SNOT-22 evaluation applies only for patients (n=6) afflicted with comorbid chronic rhinosinusitis with nasal polyps.
| Variables | Baseline | After 26-weeks of Tezepelumab (n=56) | p | After 52-weeks of Tezepelumab (n=53) | p |
|---|---|---|---|---|---|
| ACT | 11.52±3.67 | 15.89±4.73* | <0.0001 | 17.48±4.73* | <0.0001 |
| Number of annual AEs | 2.79±2.0 | 0.5±0.72* | <0.0001 | 0.51±0.89* | <0.0001 |
| Use of OCS (mg/day) | 10.2±.8.3 | 8,41±6.2 | 0.1831 | 6.9±2.4* | <0.0140 |
| FVC (mL) | 2940±992 | 3289±1234* | 0.0161 | 3214±1148* | 0.0125 |
| FEV1 (mL) | 2061±895 | 2206±923 | 0.0572 | 2316±958* | 0.0384 |
| FEV1% | 69.31±19.2 | 75.32±17.68* | 0.0043 | 76.24±20.63* | 0.0012 |
| FENO (ppb) | 29.17±19.9 | 23.93±15.42 | 0.0889 | 26.04±16.87 | 0.1960 |
| Blood Eosinophils/μL | 234±231 | 146±120* | 0.0012 | 147±110* | 0.0125 |
| Total IgE (IU/mL) | 354±549 | 240±382 | 0.1324 | 234±409 | 0.2356 |
| sIgE D. pteronyssinus (kUA/L) | 21.17±33.0 | N/A | N/A | 17.15±4.32 | 0.1833 |
| sIgE D. farinae (kUA/L) | 17.1±30.21 | N/A | N/A | 13.58±4.7 | 0.1499 |
| SNOT-22 | 59.94±19.36 | 55.67±23.69 | 0.5171 | 46.76±26.8 | 0.373 |
| Combined BARS | - | 0.95±0.53 | - | 1.06±0.55 | 0.0501 |
ACT: Asthma Control Test. AEs: Asthma exacerbations. OCS: Oral corticosteroids. FVC: Forced Ventilatory Capacity. FEV1: forced expiratory volume in the first second. SNOT-22: Sino-Nasal Outcome Test-22. FENO: Fractional exhaled nitric oxide. sIgE: Specific IgE. N/A: Not Assessed. BARS: Biologics Asthma Response Score. (*) Indicates statistical significance (p < 0.05). Mean values and standard deviation are shown.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



