Submitted:
28 February 2026
Posted:
04 March 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Immune responses naturally decline with age in the elderly; this process is named immunosenescence. The risks for adverse events (AEs) can increase, decrease, or be uncorrelated with increasing age. Safety signals associated with vaccines can be detected within the Vaccine Adverse Event Reporting System (VAERS). Herein, VAERS was retrospectively examined for safety signals associated with the elderly. In general, common AEs include normal immune responses and also injection site-related AEs. For multiple COVID-19 vaccines, breakthrough infections and COVID-19-related AEs had unexpectedly high normalized frequencies. The normalized frequency for AE death was elevated for multiple vaccines, including COVID-19 vaccines; the associated risk appears to be additive for coadministered combinations of the COVID-19 Janssen vaccine with either the COVID-19 Pfizer-BioNTech BNT162b2 or the COVID-19 Moderna mRNA-1273 vaccine. Multiple manufacturing lots for the COVID-19 Janssen, COVID-19 Pfizer-BioNTech BNT162b2, and Moderna mRNA-1273 vaccines have high AE death normalized frequencies. These observations, combined with rapid AE death onset following vaccination, likely point to possible manufacturing contamination of specific manufacturing lots; endotoxins are a possible causative constituent. The sensitivity to these causative constituent(s) increases with age in the elderly.
Keywords:
death
; fall
; endotoxin
; mRNA vaccine
; COVID-19 vaccine
; breakthrough infection
1. Introduction
Aging-associated declines in immune system responses, a process named immunosenescence, result in weaker immune responses to new pathogens and vaccines. For improved protection against influenza, multiple high-dose vaccines are provided to the elderly. Immune responses to vaccines are reflected in associated adverse events. The Vaccine Adverse Event Reporting System (VAERS) collects population samples of adverse events (AEs) for the detection of associated safety signals. Safety signals specific to vaccine constituents can be detectable above expected background occurrence frequencies by comparing AE frequencies between different vaccines.
Characteristics of immunosenescence for antibody and T-cell responses have been observed in multiple studies for COVID-19 vaccines. Lower neutralization of SARS-CoV-2 infection was observed for IgA and IgG serum from elderly recipients, accompanied by lower T cell responses after the first dose of the Pfizer-BioNTech BNT162b2 vaccine [1]. Similar results were observed for 71 and 149 elderly COVID-19 Pfizer-BioNTech BNT162b2 vaccine recipients in two studies [2,3]. A study including 105 older long-term care facility residents found dramatically impaired humoral and cellular memory responses three months after the first COVID-19 Pfizer-BioNTech BNT162b2 mRNA vaccine dose [4]. A study of 138 nursing home residents found lower neutralization for residents receiving the COVID-19 Pfizer-BioNTech BNT163b2 vaccine (4-fold lower) and the COVID-19 Moderna mRNA-1273 vaccine (2-fold lower) [5]. A study of 165,755 nursing home residents in Sweden found higher mortality for unvaccinated residents and residents with no prior COVID-19 infection who had not received a COVID-19 vaccine or booster dose within the last 90 days [6]. Lower mortality is observed for COVID-19 vaccinated compared to unvaccinated individuals [7].
To detect possible safety signals in the elderly, AEs were retrospectively examined in VAERS for 10-year age groups for all vaccines. As anticipated, multiple AEs were observed with frequencies that correlate with increasing age, likely associated with immunosenescence. Unexpectedly, the AE death appears to have additive risks for coadministered vaccines with higher frequencies; this may indicate unknown causative constituents like manufacturing contaminants within specific vaccines. It is strongly recommended that COVID-19 vaccines not be coadministered with other vaccines without prior clinical trials of these vaccine combinations that include elderly individuals.
2. Materials and Methods
Materials
State all the materials used in the study, and include the manufacturer’s name, city and country of origin.
The VAERS database [8] was retrospectively examined for AEs with the Ruby program vaers_tally_age10.rb [9]; this program summarizes AEs by 10-year age groups. The download of VAERS data includes all AEs reported from 1990 to October 31, 2025. This program calculates the frequencies of reported AEs normalized to 100,000 VAERS reports: AE normalized frequency = (age group observed AEs/all vaccine AEs)*100,000 for each single administered vaccine or coadministered vaccines. For reference, the names of coadministered vaccines are joined with the plus symbol. Vaccines and vaccine combinations including the text “no brand name”, “foreign”, “unknown”, and “vaccine not specified” were excluded to avoid possible reporting biases due to the possibility of underrepresentation of less severe AEs resulting in increased normalized frequency estimates. This retrospective study examines the age groups 50-59, 60-69, 70-79, 80-89, 90-100, and 100-109. VAERS AE names and spelling have not been changed. The day of onset data was examined with the Ruby program vaers_slice5.rb [9]. Microsoft Excel was used for median calculations, data sorting, and creating figures.
3. Results
For the age group 80 to 89 and vaccines with at least 1,000 VAERS AEs, the top AEs are illustrated for five COVID-19 vaccines (Table 1A) and Influenza seasonal (Fluzone high-dose), Pneumo (Pneumovax), Pneumo (Prevnar13), Zoster (Shingrix), and Zoster live (Zostavax) (Table 1B); AEs selected were in the top 50 by normalized frequency for at least two vaccines. Multiple AEs in the COVID-19 AEs list (Table 1A) do not overlap with the top AE list for the other five vaccines; these AEs are illustrated in Table 2. Other top AEs for the five non-COVID-19 vaccines did not overlap the COVID-19 top list: back pain, blister, cellulitis, herpes zoster, hypoaesthesia, injected limb mobility decreased, injection site induration, injection site inflammation, injection site pruritus, injection site rash, injection site reaction, injection site warmth, mobility decreased, muscular weakness, musculoskeletal pain, neck pain, oedema peripheral, paraesthesia, rash erythematous, rash pruritic, skin warm, swelling, tenderness, tremor, and urticaria. The AE death normalized frequencies are illustrated in Figure 1, and AE fall in Figure 2 for multiple vaccines. The AE death normalized frequencies by manufacturing lot number are illustrated for selected lots for three COVID-19 vaccines (Figure 3). The day of onset for AE death is illustrated in Table 3.
4. Discussion
4.1. Frequent Adverse Events in the Age Group 80 to 89
Aging likely negatively impacts AEs following immunizations. The top AEs for vaccines with more than 1,000 VAERS reports are shown in Table 1. For COVID-19 vaccine recipients, COVID-19 infection and associated AEs are only seen associated with the COVID-19 vaccines (Table 1); age group comparisons for these AEs are illustrated in Table 2. For the age group 80 to 89 vaccine recipients of the COVID-19 Janssen vaccine, 1 in 3.3 (30.5%) reported COVID-19 infection, and 1 in 7.4 (13.6%) died (Table 1A). The normalized frequency for AE death for the COVID-19 vaccines was 1829 for the COVID-19 (Janssen), 1409 for the COVID-19 (Moderna), 646 for the COVID-19 (Moderna bivalent), 1260 for the COVID-19 (Moderna Mnexspike), 629 for the COVID-19 (Novavax), 1063 for the COVID-19 (Pfizer-BioNTech), and 887 for the COVID-19 (Pfizer-BioNTech bivalent). For all ages, higher numbers of deaths were reported following the second dose compared to the first dose of the COVID-19 Pfizer-BioNTech vaccine (3487 first dose and 4654 second dose) and the COVID-19 Moderna vaccine (2931 first dose and 3749 second dose). For the age group 80 to 89 vaccine recipients of the COVID-19 Pfizer-BioNTech vaccine, 1 in 4.9 (20.5%) reported COVID-19 infection, and 1 in 12.4 (8.1%) died (Table 1A). For the COVID-19 AEs illustrated in Table 2, the majority fit the pattern of increasing normalized frequency by increased age, except for chest pain and oropharyngeal pain. Note the chest pain AE may have associations with myocarditis and pericarditis AEs with inverse age risks following COVID-19 immunization for both genders [10].
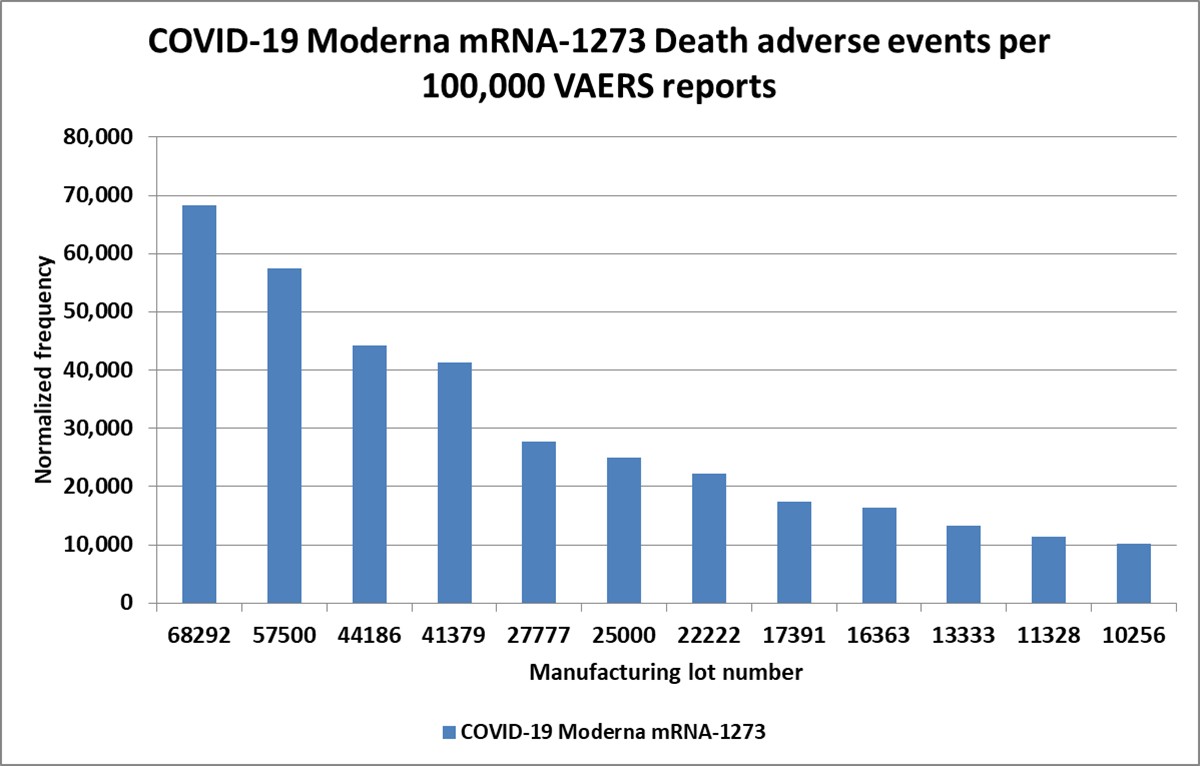
Multiple COVID-19 lots exhibit higher normalized frequencies than the overall average for all ages for the AE death (Figure 3 and Supplemental Table S1). For the COVID-19 Janssen lots 1805031 (4731), 1802070 (4676), and 212C21A (4651), plus 14 additional lots, were higher than the overall 1829 (Supplemental Table S1). A total of 175 COVID-19 Moderna lots with at least 4 death AEs exceed the overall 1260, including lots 207H23-2A (68,292), 3043159 (57,500), and 3046731 (44,186), with the normalized frequency for 12 lots higher than 10,000 (> 1 in 10) (Supplemental Table S1). Five COVID-19 Moderna bivalent lots had at least four AEs, including AS7184B (6756), AS7180B (4938), and 020H22A (3478), which were higher than the overall 646 (Supplemental Table S1). A total of 174 COVID-19 Pfizer-BioNTech lots exceed the overall AE death normalized frequency of 1063, including EK4238 (19,512), EK4242 (15,789), and E10140 (12,195) (Supplemental Table S1). While normal distributions are expected, the very high normalized frequencies for the COVID-19 Moderna, COVID-19 Moderna bivalent, COVID-19 Pfizer-BioNTech, and possibly COVID-19 Janssen vaccines are consistent with manufacturing contaminants as likely causative components [11].
Endotoxins are one possible manufacturing contaminant. Lipopolysaccharides (LPS), also known as endotoxins or pyrogens, are constituents of the outer membrane of gram-negative bacteria. Endotoxins are a common manufacturing contaminant of vaccines. Endotoxin levels can vary widely by vaccine [12,13]. To minimize endotoxin contaminants, nanoparticles should be manufactured under endotoxin-free conditions [14].
4.2. COVID-19 Breakthrough Infection
Individuals are getting the COVID-19 immunization to avoid COVID-19. It seems counterintuitive that the top AE associated with COVID-19 immunization (Table 1A) is COVID-19. The coronavirus family is well-known for infecting phagocytic immune cells using Fc receptor binding to infect additional host cells [15]. The process of antibody-dependent enhancement of disease (ADE) for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus has been proposed [16] and supported by clinical evidence [17]. The proposed ADE infection of immune cells has been demonstrated to be sensitive to the antibody titer level for the SARS-CoV-1 virus [18]. Hence, until COVID-19 vaccine recipients reach very high Spike protein antibody titer levels, the vaccine recipients have possibly higher infectivity potential than non-vaccinated individuals. Likewise, as the Spike antibody titers naturally decrease after several months, breakthrough infections of fully vaccinated and boosted individuals are being observed. The current recommendations for COVID-19 booster shots every six months should maintain ongoing very high levels of Spike protein antibodies.
4.3. Death Adverse Event
The risk of death increases with increased age. For comparison purposes, an upper limit for background AE death can be estimated roughly as 252 per 100,000 VAERS reports using the value for Zoster (Shingrix) (Table 1B); given this, the normalized frequency for COVID-19 Janssen is 81 times higher than this background rate (20,500 / 252), and COVID-19 Pfizer-BioNTech is 32 times higher than this background rate (8,089 / 252). The background deaths per 7 days per 100,000 individuals in the United States is 109 [19]. Normalized frequencies for AE death for age groups 50-59, 60-69, 70-79, and 80-89 for multiple vaccines and several coadministered vaccines are illustrated in Figure 1. The normalized frequencies for death appear additive for COVID-19 Janssen and COVID-19 Moderna (18.2%), COVID-19 Janssen and COVID-19 Pfizer-BioNTech (22.2%), and COVID-19 Pfizer-BioNTech bivalent + Influenza seasonal (Fluzone high-dose quadrivalent) (6.9%) (Figure 1). The normalized frequency for the COVID-19 Janssen vaccine is 1829 (1.8%), and the COVID-19 Pfizer-BioNTech vaccine is 1063 (1.1%). The normalized frequency for the COVID-19 Janssen vaccine age group 80 to 89 is 11.2 times higher than for all ages; the normalized frequency for ages 80 to 89 for the COVID-19 Pfizer-BioNTech vaccine is 7.6 times higher than for all ages. The majority of deaths AEs are reported with an onset of a few days (Table 3); it is well-known that as time increases, the likelihood of reporting AEs to VAERS decreases. The normalized frequencies for AE death for COVID-19 vaccine recipient age groups 70 to 79 and 80 to 89 represent multiple safety signals (Figure 1). The normalized frequencies for AE death for Pneumo (Pneumovax), Pneumo (Prevnar13), RSV (Abrysvo), and Zoster live (Zostavax) age group 80 to 89 may also represent safety signals (Figure 1). Top overlapping AEs with death that do not overlap the COVID-19 top AEs (Table 1A) include autopsy, cardiac arrest, cardio-respiratory arrest, endotracheal intubation, general physical health deterioration, hypotension, loss of consciousness, mechanical ventilation, mental status changes, myocardial infarction, oxygen saturation decreased, positive airway pressure therapy, pulse absent, respiratory arrest, respiratory distress, respiratory failure, resuscitation, septic shock, syncope, unresponsive to stimuli, and vaccination failure. Deaths have been linked with the COVID-19 Pfizer-BioNTech vaccine [20]. Excess deaths have been observed after repeated COVID-19 vaccination in Japan [21]. Florida residents who received the COVID-19 Pfizer-BioNTech BNT162b2 vaccine were observed with significantly higher risk for 12-month all-cause mortality compared to matched COVID-19 Moderna mRNA-1273 vaccine recipients [22].
Hypothesis 1:
Immunization with a COVID-19 vaccine correlates with SARS-CoV-2 infection in elderly individuals.
Multiple days are anticipated for a SARS-CoV-2 infection post-immunization, followed in some individuals by COVID-19-associated death, with COVID-19-associated death occurring multiple days after infection. Defining any individual receiving a COVID-19 vaccine as vaccinated, these cases all represent COVID-19 vaccine breakthrough infections; many cases in VAERS are reported after the first of two paired mRNA vaccine doses, but more cases follow the second dose. ADE may be contributing to the severity of COVID-19 in elderly individuals [16].
Hypothesis 2:
Novel safety signal detected is associated with multiple vaccines, including the COVID-19 Moderna, COVID-19 Pfizer-BioNTech, COVID-19 Moderna bivalent, and COVID-19 Janssen for AE death; elevated normalized frequencies associated with manufacturing lots are supportive of unknown manufacturing contamination as a likely causative component.
VAERS data indicate elevated additive risks for coadministration of two or more vaccines with elevated AE death normalized frequencies. VAERS data are consistent with a rapid onset in days for this safety signal. Deaths associated with the Hypothesis 2 model are likely independent of SARS-CoV-2 infection, but overlaps between these two independent etiology models can occur randomly. Note that both the COVID-19 Pfizer-BioNTech BNT162b2 and the COVID-19 Moderna Spikevax mRNA-1273 vaccines were found to have residual plasmid DNA and SV40 promoter-enhancer sequences in some vaccine batches [23]; while this is of major concern with regards to long-term expression of the Spike protein within vaccine recipient bacteria cells, any relationship to immediate-onset adverse event death is unknown. This does illustrate contamination of vaccine batches with unintended constituents.
4.4. Fall Adverse Event
The risk of falling following immunization has been previously identified [24]. The AE fall is in the top 50 ranked AEs for multiple vaccines (Table 1). This study demonstrates an undetected age risk factor for the fall AE (Figure 2). The normalized frequencies for the AE fall are much higher for COVID-19 vaccines and coadministered combinations including a COVID-19 vaccine than for non-COVID-19 vaccines (Figure 2). There may be some signature overlaps with the AE death signatures by vaccine and coadministered vaccines, pointing to possible overlapping etiologies worthy of further investigation. Immediate onset of fall AEs has been previously reported [24].
5. Conclusions
Informed consent considers risks versus benefits for vaccines and coadministered vaccines. This study identifies clear safety signals that increase with age for death associated with specific vaccines. Multiple safety signals associated with increased mortality risks were identified and are worthy of follow-up studies.
The risk of falling within two days post-immunization increases with age. Reiterating: “Avoidance of activities like driving, operating heavy machinery, with increased risks of falling, etc., for one to two days following immunization provides an opportunity to reduce the frequency of falls, injuries, and other rare accidents” [24].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, D.R.; Methodology, D.R.; Software, D.R.; Validation, D.R.; Formal Analysis, D.R..; Investigation, D.R..; Data Curation, D.R.; Writing – Original Draft Preparation, D.R.; Writing – Review & Editing, D.R.
Funding
This research received no external funding.
Data Availability Statement
Ricke, Darrell, 2025, "VAERS retrospective analysis by 10-year age groups", https://doi.org/10.7910/DVN/CKOV3E, Harvard Dataverse, V1.
Acknowledgments
None.
Conflicts of Interest
The author declares no conflict of interest.
Ethical approval
Not applicable.
References
- Collier, DA; Ferreira, IATM; Kotagiri, P; et al. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, T; Tober-Lau, P; Hillus, D; et al. Delayed Antibody and T-Cell Response to BNT162b2 Vaccination in the Elderly, Germany. Emerg Infect Dis J. 2021, 27, 2174. [Google Scholar] [CrossRef]
- Canaday, DH; Carias, L; Oyebanji, OA; et al. Reduced BNT162b2 Messenger RNA Vaccine Response in Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)–Naive Nursing Home Residents. Clin Infect Dis. 2021, 73, 2112–2115. [Google Scholar] [CrossRef] [PubMed]
- Demaret, J; Corroyer-Simovic, B; Alidjinou, EK; et al. Impaired Functional T-Cell Response to SARS-CoV-2 After Two Doses of BNT162b2 mRNA Vaccine in Older People. Front Immunol. 2021, 12-2021. Available online: https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2021.778679. [CrossRef]
- Breznik, JA; Zhang, A; Huynh, A; et al. Antibody Responses 3-5 Months Post-Vaccination with mRNA-1273 or BNT163b2 in Nursing Home Residents. J Am Med Dir Assoc. 2021, 22, 2512–2514. [Google Scholar] [CrossRef]
- Björk, J; Dietler, D; Bonander, C; et al. Vaccine protection against COVID-19 mortality in relation to time since last booster dose among nursing home residents in Sweden – A case-control study over 35 months. Vaccine 2026, 71, 128043. [Google Scholar] [CrossRef]
- Yang, XH; Bao, WJ; Zhang, H; Fu, SK; Jin, HM. The Efficacy of SARS-CoV-2 Vaccination in the Elderly: A Systemic Review and Meta-analysis. J Gen Intern Med. 2023. [Google Scholar] [CrossRef]
- VAERS. Vaccine Adverse Event Reporting System; U.S. Department of Health & Human Services, 2025. Available online: https://vaers.hhs.gov/data/datasets.html (accessed on 10 November 2025).
- Ricke, DO. VAERS-Tools. 2022. Available online: https://github.com/doricke/VAERS-Tools (accessed on 10 November 2025).
- Ricke, DO. Cardiac adverse events post-vaccination. Brain Heart 2025, 3, 1–15. [Google Scholar] [CrossRef]
- Ricke, DO. Menstrual adverse events post-COVID-19 and human papillomavirus immunization. Microbes Immun. 2025. [Google Scholar] [CrossRef]
- Geier, M R; Stanbro, H; Merril, C R. Endotoxins in commercial vaccines. Appl Environ Microbiol. 1978, 36, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Brito, LA; Singh, M. COMMENTARY: Acceptable Levels of Endotoxin in Vaccine Formulations During Preclinical Research. J Pharm Sci. 2011, 100, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Costa, JP; Jesus, S; Colaço, M; Duarte, A; Soares, E; Borges, O. Endotoxin contamination of nanoparticle formulations: A concern in vaccine adjuvant mechanistic studies. Vaccine 2023, 41, 3481–3485. [Google Scholar] [CrossRef] [PubMed]
- Jaume, M.; Yip, M.S.; Cheung, C.Y.; et al. Anti-Severe Acute Respiratory Syndrome Coronavirus Spike Antibodies Trigger Infection of Human Immune Cells via a pH- and Cysteine Protease-Independent FcγR Pathway. J Virol. 2011, 85, 10582–10597. [Google Scholar] [CrossRef]
- Ricke, DO. Two Different Antibody-Dependent Enhancement (ADE) Risks for SARS-CoV-2 Antibodies. Front Immunol. 2021, 12, 443. [Google Scholar] [CrossRef]
- Ricke, DO. Antibodies and infected monocytes and macrophages in COVID-19 patients. AIMS Allergy Immunol. 2022, 6, 64–70. [Google Scholar] [CrossRef]
- Wan, Y; Shang, J; Sun, S; et al. Molecular Mechanism for Antibody-Dependent Enhancement of Coronavirus Entry. J Virol. 2022, 94, e02015-19. [Google Scholar] [CrossRef]
- Liu, JY; Chen, TJ; Hou, MC. Does COVID-19 vaccination cause excess deaths? J Chin Med Assoc. 2021, 84. Available online: https://journals.lww.com/jcma/Fulltext/2021/09000/Does_COVID_19_vaccination_cause_excess_deaths_.2.aspx. [CrossRef]
- Torjesen, I. Covid-19: Pfizer-BioNTech vaccine is “likely” responsible for deaths of some elderly patients, Norwegian review finds. BMJ. 2021, 373, n1372. [Google Scholar] [CrossRef]
- Kakeya, H; Nitta, T; Kamijima, Y; Miyazawa, T. Significant Increase in Excess Deaths after Repeated COVID-19 Vaccination in Japan. JMA J. 2025, 8, 584–586. [Google Scholar] [CrossRef]
- Levi, R; Mansuri, F; Jordan, MM; Ladapo, JA. Twelve-Month All-Cause Mortality after Initial COVID-19 Vaccination with Pfizer-BioNTech or mRNA-1273 among Adults Living in Florida. medRxiv 2025. [Google Scholar] [CrossRef]
- Speicher, DJ; Rose, J; McKernan, K. Quantification of residual plasmid DNA and SV40 promoter-enhancer sequences in Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada. Autoimmunity 2025, 58, 2551517. [Google Scholar] [CrossRef] [PubMed]
- Ricke, DO. Rare dizziness, syncope, loss of consciousness, seizure, and risk of falling after vaccination. AIMS Allergy Immunol. 2023, 7, 164–175. [Google Scholar] [CrossRef]
Figure 1.
Death adverse event normalized frequencies by age group. A) COVID-19, Streptococcus pneumonia (Pneumo), Respiratory Syncytial virus (RSV), and Herpes Zoster vaccines; B) Influenza vaccines.
Figure 1.
Death adverse event normalized frequencies by age group. A) COVID-19, Streptococcus pneumonia (Pneumo), Respiratory Syncytial virus (RSV), and Herpes Zoster vaccines; B) Influenza vaccines.


Figure 2.
Fall adverse event normalized frequencies by age group. A) COVID-19, Streptococcus pneumonia (Pneumo), Respiratory Syncytial virus (RSV), and Herpes Zoster vaccines; B) Influenza vaccines.
Figure 2.
Fall adverse event normalized frequencies by age group. A) COVID-19, Streptococcus pneumonia (Pneumo), Respiratory Syncytial virus (RSV), and Herpes Zoster vaccines; B) Influenza vaccines.


Figure 3.
Death adverse event normalized frequency for selected manufacturing lots (A) COVID-19 Janssen, (B) COVID-19 Moderna mRNA-1273, and (C) COVID-19 Pfizer-BioNTech BNT162b2 vaccines.
Figure 3.
Death adverse event normalized frequency for selected manufacturing lots (A) COVID-19 Janssen, (B) COVID-19 Moderna mRNA-1273, and (C) COVID-19 Pfizer-BioNTech BNT162b2 vaccines.



Table 1.
Top 50 adverse events for vaccines with at least 1,000 VAERS adverse events for ages 80 to 89 (A) COVID-19 vaccines and (B) five other vaccines. The table is sorted by descending average mean value of the normalized frequencies. COVID-19 vaccines (A) top 50 list letter designators: J – COVID-19 (Janssen), m - COVID-19 (Moderna), M - COVID-19 (Moderna bivalent), p - COVID-19 (Pfizer-BioNTech), and P - COVID-19 (Pfizer-BioNTech bivalent). Additional vaccines (B) top 50 list letter designators: I – Influenza seasonal (Fluzone high-dose), O - Pneumo (Pneumovax), P - Pneumo (Prevnar13), S - Zoster (Shingrix), and Z - Zoster live (Zostavax).
Table 1.
Top 50 adverse events for vaccines with at least 1,000 VAERS adverse events for ages 80 to 89 (A) COVID-19 vaccines and (B) five other vaccines. The table is sorted by descending average mean value of the normalized frequencies. COVID-19 vaccines (A) top 50 list letter designators: J – COVID-19 (Janssen), m - COVID-19 (Moderna), M - COVID-19 (Moderna bivalent), p - COVID-19 (Pfizer-BioNTech), and P - COVID-19 (Pfizer-BioNTech bivalent). Additional vaccines (B) top 50 list letter designators: I – Influenza seasonal (Fluzone high-dose), O - Pneumo (Pneumovax), P - Pneumo (Prevnar13), S - Zoster (Shingrix), and Z - Zoster live (Zostavax).
| Adverse event | COVID-19 (Janssen) | COVID-19 (Moderna) | COVID-19 (Moderna bivalent) | COVID-19 (Pfizer-BioNTech) | COVID-19 (Pfizer-BioNTech bivalent) | Top 50 |
|---|---|---|---|---|---|---|
| COVID-19 | 30,540 | 15,462 | 15,502 | 20,500 | 18495 | JmMpP |
| SARS-CoV-2 test positive | 25,263 | 12,054 | 12,816 | 15,586 | 17651 | JmMpP |
| Dyspnoea | 13,588 | 6752 | 4834 | 9652 | 6680 | JmMpP |
| Fatigue | 8707 | 9157 | 8902 | 8036 | 4571 | JmMpP |
| Asthenia | 9234 | 7476 | 5679 | 7848 | 8509 | JmMpP |
| Pyrexia | 7387 | 8229 | 6983 | 8085 | 5555 | JmMpP |
| Death | 13,588 | 7147 | 1995 | 8089 | 3445 | JmMpP |
| Cough | 9036 | 4045 | 6753 | 5746 | 7383 | JmMpP |
| Expired product administered | 791 | 5410 | 11,588 | 1603 | 9845 | mM P |
| Product storage error | 1451 | 3903 | 4297 | 2342 | 13994 | mMpP |
| Headache | 4815 | 6305 | 5602 | 5334 | 2812 | JmMpP |
| Pain | 4617 | 4903 | 5909 | 4134 | 3445 | JmMpP |
| Pain in extremity | 4881 | 6088 | 5141 | 4615 | 2039 | JmMpP |
| Acute respiratory failure | 4089 | 2061 | 3146 | 2873 | 9704 | JmMpP |
| Dizziness | 4485 | 4638 | 3607 | 5142 | 2672 | JmMpP |
| Chills | 3891 | 5895 | 3146 | 4215 | 3305 | JmMpP |
| Nausea | 4485 | 4839 | 3530 | 4538 | 3023 | JmMpP |
| Malaise | 3759 | 2889 | 4758 | 4522 | 3305 | JmMpP |
| Hypoxia | 5343 | 2173 | 2686 | 2836 | 5977 | JmMpP |
| Condition aggravated | 4815 | 2647 | 2609 | 3224 | 4992 | JmMpP |
| Vaccine breakthrough infection | 5277 | 2539 | 2609 | 3048 | 2742 | JmMpP |
| Arthralgia | 2572 | 3549 | 3914 | 3273 | 1828 | JmMpP |
| Fall | 3627 | 2606 | 2302 | 3309 | 2953 | JmMpP |
| COVID-19 pneumonia | 5540 | 1961 | 1074 | 3485 | 2672 | Jm pP |
| Vomiting | 3166 | 3009 | 2455 | 3416 | 2531 | JmMpP |
| Diarrhoea | 3562 | 3180 | 2302 | 3428 | 1969 | JmMpP |
| Chest X-ray abnormal | 4485 | 1771 | 1688 | 2424 | 3375 | JmMpP |
| Extra dose administered | 1121 | 1334 | 4451 | 1285 | 4219 | M P |
| Myalgia | 1781 | 3419 | 2686 | 2489 | 1195 | mMp |
| Rash | 1385 | 3501 | 1611 | 2461 | 1969 | mMpP |
| Pneumonia | 3166 | 1879 | 1381 | 2718 | 1687 | Jm pP |
| Confusional state | 2770 | 1886 | 1534 | 2167 | 2461 | JmMpP |
| Decreased appetite | 2968 | 2382 | 1611 | 2767 | 984 | Jm pP |
| Atrial fibrillation | 2506 | 1659 | 1458 | 2424 | 2390 | JmMpP |
| Injection site pain | 1978 | 2457 | 1841 | 906 | 2109 | JmM P |
| Gait disturbance | 2044 | 1588 | 1841 | 1881 | 1687 | JmMpP |
| Peripheral swelling | 2440 | 2158 | 1995 | 1424 | 984 | JmM |
| Feeling abnormal | 1583 | 2102 | 2302 | 1816 | 1125 | mM |
| Pulmonary embolism | 2836 | 1107 | 997 | 1787 | 1898 | J P |
| Pruritus | 857 | 3818 | 1074 | 2028 | 843 | m p |
| Chest pain | 1715 | 1487 | 1841 | 1954 | 1336 | mMp |
| Cerebrovascular accident | 2440 | 1510 | 690 | 1848 | 1687 | Jm pP |
| Acute kidney injury | 2506 | 1017 | 920 | 1477 | 1969 | J P |
| Erythema | 1187 | 3143 | 1458 | 1461 | 632 | mM |
| Anticoagulant therapy | 2638 | 913 | 1151 | 1073 | 2039 | J P |
| Unevaluable event | 2968 | 1856 | 383 | 1885 | 703 | Jm p |
| Inappropriate schedule of product administration | 395 | 1935 | 1688 | 2301 | 1476 | mMp |
| Oropharyngeal pain | 1319 | 820 | 1918 | 1020 | 2672 | M P |
| Sepsis | 2308 | 816 | 1074 | 1048 | 2109 | J P |
| Injection site erythema | 263 | 3161 | 1841 | 624 | 914 | mM |
| Respiratory tract congestion | 791 | 678 | 1611 | 722 | 2039 | M |
| Injection site swelling | 329 | 1979 | 1688 | 453 | 1195 | mM |
| Adverse event | Influenza seasonal (Fluzone high-dose) | Pneumo (Pneumovax) | Pneumo (Prevnar13) | Zoster (Shingrix) | Zoster live (Zostavax) | Top 50 |
|---|---|---|---|---|---|---|
| Injection site erythema | 9978 | 25,530 | 28,231 | 13,499 | 12,782 | IOPSZ |
| Erythema | 7749 | 21,378 | 19,391 | 9769 | 8134 | IOPSZ |
| Injection site pain | 11,093 | 18,074 | 16,444 | 14,068 | 4770 | IOPSZ |
| Injection site swelling | 8439 | 21,472 | 17,395 | 9010 | 5932 | IOPSZ |
| Pain in extremity | 12,951 | 12,364 | 12,452 | 15,333 | 3363 | IOPSZ |
| Pain | 10,350 | 10,382 | 10,076 | 12,867 | 11,192 | IOPSZ |
| Pyrexia | 11,677 | 11,845 | 9410 | 9895 | 2568 | IOPSZ |
| Rash | 4299 | 3445 | 7889 | 10,907 | 15,902 | IOPSZ |
| Herpes zoster | 106 | 235 | 95 | 7556 | 32,782 | SZ |
| Pruritus | 3980 | 4907 | 9885 | 7714 | 10,275 | IOPSZ |
| Injection site warmth | 4989 | 10,335 | 11,501 | 5153 | 4036 | IOPSZ |
| Chills | 11,411 | 2642 | 5893 | 9326 | 1039 | IOPSZ |
| Peripheral swelling | 3237 | 9202 | 8935 | 5026 | 366 | IOPS |
| Headache | 6157 | 1793 | 4372 | 8409 | 3792 | IOPSZ |
| Fatigue | 5414 | 1840 | 4847 | 10,116 | 1834 | IOPSZ |
| Skin warm | 4299 | 6606 | 7414 | 3446 | 1896 | IOPSZ |
| Injection site pruritus | 2388 | 2501 | 8935 | 4331 | 4403 | IOPSZ |
| Asthenia | 5732 | 2737 | 3992 | 5501 | 2568 | IOPSZ |
| Swelling | 3078 | 6984 | 5513 | 3035 | 1651 | IOPSZ |
| Nausea | 5891 | 2548 | 3707 | 6165 | 1773 | IOPSZ |
| Dizziness | 4670 | 2595 | 3231 | 4552 | 3302 | IOPSZ |
| Malaise | 3397 | 3303 | 3326 | 4204 | 2385 | IOPSZ |
| Myalgia | 3343 | 2312 | 3897 | 5279 | 1590 | IOPSZ |
| Arthralgia | 2600 | 1604 | 3422 | 4805 | 1773 | IOPSZ |
| Mobility decreased | 3556 | 2878 | 2756 | 3793 | 733 | IOPS |
| Cellulitis | 636 | 7126 | 4182 | 885 | 550 | OP |
| Dyspnoea | 3927 | 2548 | 3802 | 1549 | 1345 | IOPSZ |
| Injection site rash | 1433 | 1179 | 4277 | 2402 | 3608 | I PSZ |
| Rash erythematous | 1804 | 1226 | 2756 | 2971 | 4036 | I PSZ |
| Vomiting | 5520 | 1321 | 1996 | 2307 | 856 | I PS |
| Urticaria | 2388 | 1038 | 2091 | 2655 | 2507 | I PSZ |
| Diarrhoea | 3450 | 566 | 2281 | 2845 | 978 | I PS |
| Tremor | 4989 | 943 | 855 | 2655 | 672 | I S |
| Injection site reaction | 1645 | 2925 | 1615 | 1517 | 2140 | IOP Z |
| Musculoskeletal pain | 3237 | 1793 | 1901 | 1738 | 1039 | IOPSZ |
| Injected limb mobility decreased | 2282 | 2831 | 2091 | 1896 | 122 | IOPS |
| Oedema peripheral | 796 | 6134 | 665 | 126 | 1406 | O Z |
| Extra dose administered | 3450 | 519 | 1235 | 2877 | 672 | I S |
| Tenderness | 1008 | 3445 | 1996 | 1201 | 978 | OP |
| Blister | 265 | 330 | 380 | 2023 | 5382 | SZ |
| Back pain | 1698 | 1274 | 1045 | 2023 | 2140 | I SZ |
| Rash pruritic | 1008 | 188 | 1330 | 2529 | 3058 | PSZ |
| Cough | 2813 | 1415 | 2376 | 758 | 550 | IOP |
| Pneumonia | 583 | 3916 | 2661 | 316 | 428 | OP |
| Decreased appetite | 1910 | 1179 | 2376 | 1802 | 550 | I PS |
| Muscular weakness | 1804 | 991 | 2091 | 1960 | 795 | I PS |
| Injection site induration | 690 | 1746 | 2756 | 695 | 1590 | OP Z |
| Neck pain | 1645 | 991 | 1996 | 1738 | 795 | I PS |
| Feeling abnormal | 1380 | 802 | 1235 | 2307 | 795 | I PS |
| Paraesthesia | 1433 | 519 | 570 | 1580 | 2262 | I SZ |
| Condition aggravated | 955 | 991 | 475 | 1580 | 1896 | SZ |
| Hypoaesthesia | 1857 | 849 | 570 | 1738 | 856 | I S |
| Gait disturbance | 1273 | 471 | 1520 | 1612 | 856 | PS |
| Death | 902 | 1746 | 1520 | 252 | 1039 | OP Z |
| Injection site inflammation | 424 | 1604 | 2186 | 663 | 489 | OP |
| Fall | 1645 | 755 | 380 | 1612 | 611 | I S |
Table 2.
COVID-19 selected adverse events normalized frequencies.
| Adverse event | Age group | COVID-19 (Janssen) | COVID-19 (Moderna) | COVID-19 (Moderna bivalent) | COVID-19 (Pfizer-BioNTech) | COVID-19 (Pfizer-BioNTech bivalent) |
|---|---|---|---|---|---|---|
| Acute kidney injury |
50-59 | 428 | 154 | 108 | 212 | 247 |
| 60-69 | 829 | 326 | 201 | 465 | 344 | |
| 70-79 | 1430 | 629 | 425 | 1045 | 789 | |
| 80-89 | 2506 | 1017 | 920 | 1477 | 1969 | |
| Acute respiratory failure |
50-59 | 714 | 200 | 325 | 379 | 949 |
| 60-69 | 1469 | 463 | 717 | 955 | 1895 | |
| 70-79 | 2861 | 957 | 1567 | 1862 | 3996 | |
| 80-89 | 4089 | 2061 | 3146 | 2873 | 9704 | |
| Atrial fibrillation |
50-59 | 436 | 407 | 595 | 508 | 289 |
| 60-69 | 965 | 746 | 1091 | 1017 | 1033 | |
| 70-79 | 1379 | 1223 | 1461 | 1726 | 1934 | |
| 80-89 | 2506 | 1659 | 1458 | 2424 | 2390 | |
| Cerebrovascular accident |
50-59 | 1045 | 463 | 325 | 601 | 371 |
| 60-69 | 1280 | 630 | 229 | 832 | 590 | |
| 70-79 | 1788 | 900 | 478 | 1224 | 1272 | |
| 80-89 | 2440 | 1510 | 690 | 1848 | 1687 | |
| Chest pain |
50-59 | 3683 | 2669 | 2329 | 3379 | 2105 |
| 60-69 | 3222 | 1880 | 1608 | 2680 | 1624 | |
| 70-79 | 3193 | 1554 | 1567 | 2254 | 1374 | |
| 80-89 | 1715 | 1487 | 1841 | 1954 | 1336 | |
| Chest X-ray abnormal |
50-59 | 729 | 257 | 270 | 393 | 660 |
| 60-69 | 1605 | 524 | 660 | 735 | 812 | |
| 70-79 | 2989 | 926 | 1036 | 1362 | 1960 | |
| 80-89 | 4485 | 1771 | 1688 | 2424 | 3375 | |
| Confusional state | 50-59 | 766 | 547 | 433 | 632 | 578 |
| 60-69 | 923 | 669 | 717 | 738 | 541 | |
| 70-79 | 1379 | 1085 | 744 | 1130 | 1069 | |
| 80-89 | 2770 | 1886 | 1534 | 2167 | 2461 | |
| COVID-19 |
50-59 | 7352 | 6030 | 12,026 | 7911 | 12,262 |
| 60-69 | 12,248 | 7494 | 20,017 | 11,670 | 19,374 | |
| 70-79 | 20,975 | 10,033 | 18,841 | 15,991 | 22,683 | |
| 80-89 | 30,540 | 15,462 | 15,502 | 20,500 | 18,495 | |
| COVID-19 pneumonia |
50-59 | 1075 | 232 | 108 | 432 | 165 |
| 60-69 | 1994 | 557 | 201 | 936 | 492 | |
| 70-79 | 3960 | 1045 | 451 | 2129 | 1145 | |
| 80-89 | 5540 | 1961 | 1074 | 3485 | 2672 | |
| Hypoxia |
50-59 | 781 | 214 | 54 | 405 | 743 |
| 60-69 | 1458 | 545 | 459 | 801 | 1452 | |
| 70-79 | 2938 | 970 | 876 | 1662 | 2316 | |
| 80-89 | 5343 | 2173 | 2686 | 2836 | 5977 | |
| Oropharyngeal pain |
50-59 | 1714 | 1673 | 4767 | 2216 | 4830 |
| 60-69 | 1700 | 1719 | 7495 | 2099 | 6794 | |
| 70-79 | 1303 | 1452 | 5793 | 1938 | 5804 | |
| 80-89 | 1319 | 820 | 1918 | 1020 | 2672 | |
| Pulmonary embolism |
50-59 | 1278 | 730 | 325 | 746 | 495 |
| 60-69 | 1731 | 859 | 373 | 977 | 861 | |
| 70-79 | 2120 | 916 | 558 | 1408 | 763 | |
| 80-89 | 2836 | 1107 | 997 | 1787 | 1898 | |
| Sepsis |
50-59 | 293 | 121 | 270 | 198 | 289 |
| 60-69 | 472 | 253 | 258 | 322 | 295 | |
| 70-79 | 919 | 456 | 558 | 733 | 992 | |
| 80-89 | 2308 | 816 | 1074 | 1048 | 2109 | |
| Unevaluable event |
50-59 | 699 | 740 | 812 | 731 | 1321 |
| 60-69 | 1143 | 946 | 459 | 1019 | 713 | |
| 70-79 | 1328 | 1259 | 558 | 1498 | 636 | |
| 80-89 | 2968 | 1856 | 383 | 1885 | 703 | |
| Vaccine breakthrough infection |
50-59 | 714 | 447 | 1083 | 559 | 660 |
| 60-69 | 1721 | 866 | 1062 | 1077 | 960 | |
| 70-79 | 2887 | 1228 | 1222 | 1851 | 2163 | |
| 80-89 | 5277 | 2539 | 2609 | 3048 | 2742 |
Table 3.
Death adverse event day of onset.
| Vaccine name | Day 0 | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 |
|---|---|---|---|---|---|---|---|---|
| COVID-19 (Janssen) | 62 | 73 | 32 | 34 | 20 | 16 | 20 | 23 |
| COVID-19 (Moderna) | 567 | 649 | 289 | 170 | 124 | 129 | 84 | 124 |
| COVID-19 (Moderna bivalent) | 11 | 19 | 9 | 2 | 2 | 4 | 3 | |
| COVID-19 (Pfizer-BioNTech) | 1022 | 795 | 404 | 287 | 216 | 201 | 138 | 131 |
| COVID-19 (Pfizer-BioNTech bivalent) | 15 | 30 | 11 | 7 | 3 | 4 | 5 | 2 |
| Pneumo (Pneumovax) | 56 | 19 | 15 | 11 | 5 | 4 | 3 | 2 |
| Pneumo (Prevnar13) | 138 | 189 | 67 | 49 | 34 | 9 | 13 | 11 |
| RSV (Abrysvo) | 4 | 2 | 3 | 1 | 1 | |||
| RSV (Arexvy) | 7 | 7 | 3 | 3 | 1 | 1 | ||
| Zoster (Shingrix) | 40 | 36 | 7 | 5 | 3 | 6 | 1 | 4 |
| Zoster live (Zostavax) | 13 | 7 | 10 | 2 | 1 | 2 | 4 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



