Submitted:
28 February 2026
Posted:
02 March 2026
You are already at the latest version
Abstract
Wild-boar–related trauma is uncommon but may result in severe injuries that pose di-agnostic and therapeutic challenges, particularly in wilderness or resource-limited en-vironments. Most literature consists of isolated case reports, regional series and foren-sic descriptions; clinical guidance is therefore fragmented. This guideline synthesizes two complementary evidence sources: a structured observational cohort documenting 101 injuries sustained by boar hunters during organized hunts in Germany, and a comprehensive systematic review of all globally published wild-boar– and feral-pig–related human injuries. The observational cohort provided internally consistent epi-demiologic information on who was injured, under what circumstances, how quickly assistance was obtained, and how injuries were treated and ultimately healed. The systematic review added detailed insight into injury morphology and severity across diverse settings, including reports of deep wound tracts, extensive soft-tissue disrup-tion, significant contamination and the risk of hemorrhage, neurovascular compromise or thoracoabdominal penetration. Integrating these sources enabled a field-oriented approach to assessment and management, emphasizing early hemorrhage control, broad-spectrum antibiotic therapy, appropriate use of imaging, thorough surgical ex-ploration when indicated and region-specific tetanus or rabies prophylaxis. Together, these findings support clinicians working in remote or austere environments who may encounter these rare but potentially serious injuries.
Keywords:
wild boar injury
; wilderness trauma
; penetrating extremity wounds
; austere environment medicine
; trauma management algorithm
1. Introduction
Wild boar (Sus scrofa) populations continue to rise across Europe and many other regions, driven by favorable climatic conditions, landscape fragmentation, agricultural food availability and reduced predator pressure [1,2,3,4]. As populations expand, human–wild boar contact has increased across rural, peri-urban and even urban areas, resulting in property damage, traffic collisions, zoonotic disease risks and, on occasion, traumatic injuries [1,4]. Wild-boar attacks are only a small proportion of wildlife-related trauma, but the resulting injuries can be severe. Solitary adult males are disproportionately associated with high-energy encounters given their size, behavior, and tusk morphology [5,6].
The published clinical and forensic literature contains numerous reports of penetrating or tearing wounds, most often affecting the lower extremities, groin or trunk and typically caused by close-range charges [5,7,8]. These accounts describe deep and irregular wound tracts, extensive soft-tissue disruption and heavy contamination with soil, vegetation, or organic material, sometimes accompanied by complex polymicrobial infection [4,9]. Tusk-inflicted injuries may involve sharp-force penetration with limited blunt components, with vascular or visceral injury even when the external wound appears deceptively small [7,8]. Inadequate debridement or delayed recognition of contamination has been associated with secondary systemic complications such as sepsis [10]. Together, these reports highlight the potential severity of wild-boar–related trauma across a diverse range of agricultural, wilderness and peri-urban contexts.
Despite these recurring patterns, the literature has remained fragmented, consisting predominantly of isolated case reports and small series without a unified clinical framework. This fragmentation complicates decision-making for prehospital providers, wilderness responders and clinicians who may encounter these rare injuries in remote or resource-limited settings.
Wild-boar–related trauma and explosion injuries share no common pathophysiology or injury mechanics, but both represent rare and potentially life-threatening events that many clinicians may encounter only once or a few times in an entire career. In this regard, the situation parallels recently published guidelines for the management of explosion trauma, which emphasize the importance of structured, evidence-based pathways for uncommon but high-stakes injury patterns [11,12]. These guidelines demonstrate how standardization can support rapid, high-quality decision-making when prior personal experience is inherently limited.
Comparable examples from the wilderness-medicine domain further underscore the value of formalized guidance for infrequent critical events. The Wilderness Medical Society has issued comprehensive clinical practice guidelines for scenarios such as drowning [13] and for the medical direction of search-and-rescue teams [14]. These documents highlight the essential role of structured recommendations in austere and prehospital environments, where limited resources, prolonged extraction times and variable provider experience may complicate clinical care. The present guideline follows the same conceptual rationale: to provide a consistent, field-oriented management framework for a rare but potentially severe injury mechanism.
To address long-standing gaps in the literature, the present guideline integrates two complementary sources of evidence originating from prior work [15]. The first was a structured observational cohort of hunters who sustained wild-boar–related injuries during organized hunting activities in Germany [15A]. The second was a comprehensive systematic review, summarizing all globally published clinical, forensic and epidemiologic accounts of injuries inflicted by wild boars and feral pigs [15B]. While the earlier study [15] focused on constructing and validating these datasets, the present guideline uses their combined insights to develop a practical, wilderness-oriented clinical framework aimed at improving assessment, management and prevention in austere environments.
2. Materials and Methods
This guideline was derived from two complementary evidence sources developed in previous work [15]. The first was a structured observational cohort of hunters who sustained wild-boar–related injuries during organized hunting activities in Germany [15A]. The second was a systematic review of the international literature on human injuries inflicted by wild boars or domestic swine [15B]. Together, these sources provided both consistent, context-specific data and a broader global perspective on the clinical characteristics and management of such injuries.
The observational cohort included 101 hunters who sustained wild-boar–related trauma in the context of licensed hunting activities [15A]. Data were collected through standardized, physician-led telephone interviews. For each participant, the interviews documented demographic characteristics, hunting experience, situational details of the incident, characteristics of the offending animal, the time to first help, the subsequent treatment setting, the use of operative or non-operative management, rehabilitation requirements, final healing outcomes, work absenteeism and post-injury behavioral adaptations. Injuries were categorized into three predefined groups: closed injuries, open injuries treated on an outpatient basis, and open injuries requiring inpatient care. This framework reflected treatment pathways and overall outcomes but did not capture detailed clinical descriptors such as wound morphology, imaging findings, or intraoperative observations.
Within this cohort, four participants provided substantially more detailed accounts of their injuries and clinical course. These narratives were obtained within the same interview framework and represent a more elaborated subset of the existing cohort rather than additional cases. Although they cannot be generalized to the full sample, they illustrate the range of complications that can occur after wild-boar–related trauma.
In the first case, a hunter younger than 40 years sustained an approximately 10 cm open wound on the medial aspect of the lower leg during a tracking operation. The wound extended to the muscle fascia, and the animal was killed at the scene. The patient reached hospital within one hour and underwent outpatient wound cleansing and primary closure without drainage; postoperative antibiotic therapy was not initiated. After seven days, wound-edge necrosis and a subcutaneous abscess developed beneath the suture line, necessitating inpatient revision with debridement, jet lavage, irrigation, negative-pressure wound therapy and a planned second-look procedure with further irrigation and secondary closure. The wound subsequently healed without long-term impairment.
The second case involved a hunter younger than 60 years who sustained an approximately 15 cm long laceration on the medial aspect of the lower leg, extending to the periosteum of the tibia, also during a tracking operation. Hospital presentation occurred within six hours after injury. Initial management consisted of wound irrigation and primary closure on an outpatient basis, again without systemic antibiotic therapy. Within two days, a deep wound infection developed, and the patient required inpatient revision surgery and open wound treatment. The clinical course was prolonged but ultimately resulted in complete healing.
In the third case, a hunter younger than 40 years suffered an extensive medial lower-leg wound extending from the ankle to the knee, with a reported depth “down to the bone,” during tracking. The patient presented to hospital within one hour and received outpatient wound irrigation and primary closure. In the following days, the clinical condition deteriorated with signs of sepsis, and inpatient surgical revision became necessary. The subsequent treatment included extensive debridement, fasciotomy for compartment syndrome, vascular repair and open wound management. The inpatient stay lasted 21 days, and the patient ultimately recovered fully.
The fourth case concerned a hunter younger than 40 years with an approximately 12 cm open lateral thigh wound reaching the femur, again incurred during a tracking operation. Hospital presentation took place within one hour. Initial management consisted of primary closure during a short inpatient stay. Six weeks later, persistent local inflammation prompted operative revision, during which a retained wooden foreign body was identified and removed from the wound base. After this procedure, the wound healed completely.
These four cases were not included in quantitative analyses but were used qualitatively to illustrate potential postoperative complications and the impact of initial management decisions, particularly in relation to primary closure and the recognition of deep contamination or retained foreign material.
The second evidence source was a systematic review [15B] conducted in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [16] and included all records indexed in PubMed and Ovid/Embase from inception through 12 February 2026. Titles, abstracts and full texts were screened, and after multistage screening, 41 studies [4,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56] were included. These reports originated from a broad range of settings, including agricultural, rural, peri-urban, wilderness and subsistence environments, and described a wide variety of injury mechanisms, anatomical patterns and management strategies. Table 1 provides an overview of the 41 included studies [4,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56] and the contextual literature [1,2,3,5,6,7,9] used to frame the international burden and variability of wild-boar–related injuries.
Relevant information was extracted and harmonized with the framework used in the observational hunters cohort [15A] to enable structured comparison between the two evidence sources.
A hierarchical synthesis approach was applied. The observational hunters cohort [15A] served as the primary empirical foundation because of its consistent methodology and internal coherence. The systematic review [15B] was then used to broaden the clinical perspective, provide additional context and highlight rare injury mechanisms or management challenges that could not be captured within the observational hunters cohort [15A] alone. Individual case reports identified through the systematic review [15B] were incorporated narratively when they complemented, but did not outweigh, the structured observational data. Because the observational hunters cohort [15A] did not include systematic information on wound morphology, imaging results, physiological responses or operative details, these aspects were informed either by the systematic review [15B] or by the four detailed case narratives.
The observational hunters cohort [15A] received approval from the Ethics Committee of Ludwig-Maximilians-University of Munich (Munich, Germany; reference 24-0377; approval date 05 June 2024). All procedures were conducted in accordance with the General Data Protection Regulation (GDPR), and written informed consent was obtained from all participants. The systematic review [15B] relied exclusively on previously published data and did not require additional ethical approval.
3. Results
3.1. Epidemiology
The observational hunters cohort [15A] included 101 injured hunters, all of whom sustained wild-boar–related trauma during organized hunting activities in Germany. Participants were experienced hunters with 24–31 years of hunting experience across injury categories. Most incidents occurred during tracking operations, which accounted for the majority of closed injuries (18 of 23; 78.3%), outpatient open injuries (42 of 46; 91.3%) and inpatient open injuries (24 of 32; 75.0%). Events took place predominantly in daylight, and male wild boar were responsible for most injuries, with their proportion increasing in the more severe injury categories. Injuries were concentrated in the autumn–winter hunting season, consistent with the timing of driven hunts. Because the dataset was limited to hunting situations, it cannot provide conclusions about risks in non-hunting environments. Qualitative remarks from participants described the encounters – particularly during tracking – as sudden and difficult to avoid. Many participants emphasized the importance of daylight tracking, cooperation within the hunting party, and the value of dogs and protective equipment. Notably, none of the hunters stopped hunting after the event. Overall, the cohort outlines a clear epidemiologic context: experienced hunters, mainly injured during daytime tracking of wild boar, most often by male animals and largely within the main hunting season [15A].
The systematic review [15B] added substantial global epidemiologic breadth to these structured observations, and demonstrated that comparable patterns arise in a wide range of environments far beyond recreational hunting. Numerous international reports described injuries among farmers tending crops, forest workers managing timber or underbrush, hikers traversing wooded paths, and individuals engaging in routine rural activities such as collecting firewood, searching for truffles or walking near water sources where boars may forage [38,39,40,41,42,43,44,45,46,47,48,49,50]. In several countries, particularly in parts of southern and eastern Asia, injuries occured when humans inadvertently entered the resting areas of boar sounders or disturbed lone males during feeding [30,37,38]. Reports from the Mediterranean region and Japan additionally highlighted peri-urban incidents in which expanding wild-boar populations moved into suburban gardens, parks and garbage-rich environments, increasing human exposure even among individuals without any direct wildlife-related occupation [4,34,37].
Seasonal variation is another important epidemiologic dimension. In the observational hunters cohort [15A], most injuries clustered during autumn and winter driven hunts, reflecting hunting calendars and seasonal shifts in boar behavior. In contrast, the systematic review [15B] described incidents occurring year-round, with peaks in spring and late summer linked to breeding behavior, juvenile dispersal and shifts in food availability. Male boars were overrepresented in injury causation in both evidence sources [15A,15B], which aligns with known behavioral ecology: adult males tend to defend themselves more aggressively, display less flight behavior when confronted and possess larger, sharper tusks capable of generating deeper wound tracts upon impact [15A,15B].
Population dynamics further affect exposure frequency. Rising wild-boar numbers in Europe, driven by abundant agricultural forage, warmer winters and reduced natural predation, have increased contact with humans [1,2,4]. Similar demographic expansion has occurred in Japan and parts of South Asia, where land-use change, depopulation of rural settlements and the abandonment of hillside farmland have drawn animals into previously low-exposure areas [30,34,37]. These ecological changes, combined with the adaptability and high reproductive rate of the species, indicate that wild-boar encounters may increase in frequency in coming years.
Although fatalities are rare relative to incidence, the systematic review [15B] documented several deaths resulting from catastrophic vascular injury, severe thoracoabdominal penetration or delayed recognition of internal damage. Such outcomes underscore that even though most encounters are survivable when managed promptly, the potential for life-threatening trauma is present in all settings where humans and wild boars interact. Together, the structured patterns identified in the observational hunters cohort [15A] and the globally diverse reports summarized in the systematic review [15B] form a coherent epidemiologic profile of a multifactorial and geographically widespread injury mechanism.
3.2. Clinical Presentation
The structured dataset of the observational hunters cohort [15A] contained only limited information about the acute clinical presentation of injuries. It distinguished cases by treatment pathway – closed injuries, open injuries treated on an outpatient basis and open injuries requiring inpatient care – but did not include systematic descriptions of wound appearance, severity, bleeding, pain, neurovascular status or physiological parameters. From the predefined treatment categories, it was evident that presentations ranged from minor closed trauma to open wounds requiring hospital admission and surgery. However, because the dataset did not record specific clinical findings at the time of presentation, these categories reflect treatment pathways rather than detailed injury morphology or physiological status.
A small subset of four participants provided more elaborate qualitative accounts describing delayed infections, wound necrosis, abscess formation, sepsis, compartment syndrome and, in one instance, the removal of a retained wooden foreign body at late revision surgery. These narratives illustrate the potential complexity of individual postoperative courses, but they cannot be extrapolated to the cohort as a whole. Overall, the dataset of the observational hunters cohort [15A] offered structured information on who was injured and how the injuries were managed, but only limited insight into the immediate clinical appearance or severity of the injuries at presentation.
The systematic review [15B] supported and expanded on these findings, demonstrating that similar clinical patterns appeared consistently across international case reports. Penetrating lower-extremity injuries were the hallmark presentation worldwide, often accompanied by extensive skin flaps, deep gashes and narrow subcutaneous tracts that extended far beyond the visible entry point [4,36,49]. In many cases, these tracts contained embedded debris such as soil, vegetation, hair or fragments of clothing, all of which significantly elevate the risk of infection [4,9,46]. Thoracic injuries described in the systematic review [15B] frequently presented with chest pain, dyspnea, subcutaneous emphysema or altered breath sounds [4,23,36]. Pneumothorax and hemothorax may be occult in the early stages but progress quickly and require urgent decompression. Abdominal injuries often exhibited localized tenderness, distension or guarding, but several case reports highlighted initial minimal symptoms despite significant internal damage including bowel perforation, mesenteric bleeding or diaphragmatic tears [34,42,50].
Upper-extremity and hand injuries, although less common in the observational hunters cohort [15A], were well described in the systematic review [15B]. These often involved defensive wounds sustained when victims attempted to push the animal away or shield themselves [4,37,44]. Such injuries included tendon lacerations, neurovascular compromise or deep-space involvement of the palm or forearm [4,24,29]. Head and neck injuries were rare but were associated with exceptionally high morbidity [4,5,29]. Case reports from multiple countries described facial lacerations, orbital penetration and blunt head trauma resulting from charges at close range or from individuals being knocked to the ground and trampled [5,50,52].
Pain severity was consistently reported across both evidence sources [15A,15B]. Many patients required significant analgesia early in their evaluation to allow adequate inspection of the wound [4,34,37]. The combination of pain, contamination and unpredictable wound geometry complicates initial clinical assessment, often limiting the ability to determine the full extent of injury until imaging or surgical exploration is performed. Contamination remained a defining clinical feature in both datasets [15A,15B]. The combination of environmental debris, organic matter and boar-associated oral microbiota contributed to a high risk of infection [4,34,55].
Physiological responses varied depending on the depth and location of injury. Tachycardia, hypotension and pallor are indicators of significant blood loss or evolving shock. Tachypnea may reflect pain, anxiety or subtle thoracic compromise. Visible bleeding ranges from profuse arterial hemorrhage to slow but persistent venous oozing from deep muscle wounds. The consistent picture presented by both the observational hunters cohort [15A] and the systematic review [15B] was that wild-boar injuries often appear deceptively benign at first glance, yet frequently conceal extensive and potentially life-threatening internal damage.
Table 2 summarizes injury patterns by anatomic region, drawing on data from the observational hunters cohort [15A] and the systematic review [15B].
3.3. Assessment and Initial Management
The structured dataset of the observational hunters cohort [15A] contained only limited information on early assessment or prehospital management. Apart from the time to first help, which varied substantially – from within the first hour for many participants to delays of up to six hours – no structured data were collected on first aid measures, initial clinical evaluation or transport logistics. Because “first help” included both lay assistance and medical contact, the cohort did not distinguish between care provided by hunting companions and interventions by emergency services. Details such as bleeding control, wound inspection, limb immobilization or early decision-making were not documented. The four supplementary qualitative cases described later complications rather than initial assessment, and therefore did not extend the insight of the dataset into early management. Overall, the observational hunters cohort [15A] provided an outline of how quickly help reached the injured hunters, but offered little information on the specific assessments or interventions performed in the early phase of care.
The systematic review [15B] provided more information. Multiple reports described individuals arriving at care in profound shock due to unrecognized vascular injury, especially involving the femoral or deep thigh vessels [29,34,50]. In some patients, uncontrolled prehospital bleeding contributed directly to fatal outcomes [5,34,50]. Early hemorrhage control is therefore a universal first principle of management. Furthermore, the systematic review [15B] highlighted challenges commonly faced in early assessment: poor lighting, difficult terrain, environmental stressors and the frequent inability to fully expose or irrigate the wound in the field [4,9,50]. Pain management is essential to allow adequate examination; however, field responders often lack sufficient analgesic resources. Immobility of the affected limb was frequently necessary to prevent further tissue damage, particularly when the depth or direction of wound tracts was unknown [9,34,40].
Assessment must also consider the mechanism of injury. The tusk-inflicted wounds documented in the observational hunters cohort [15A] typically followed an upward curving trajectory, which increased the likelihood of concealed involvement of deeper structures. This pattern suggests that any wound near a major vascular bundle, joint line or body cavity should be approached as potentially complex until proven otherwise. Both evidence sources [15A,15B] indicated that even superficial-appearing wounds may conceal deep muscular separation, joint capsule penetration or neurovascular disruption [4,29,34]. Given these possibilities, field assessment must err on the side of caution. Red-flag findings requiring immediate evacuation include uncontrolled bleeding, diminished distal pulses, altered sensation or motor function, chest deformity or pain, abdominal tenderness or any suspicion of penetrating thoracoabdominal injury.
The combined evidence [15A,15B] underscored the importance of early evacuation to a facility capable of advanced imaging and operative care. Long delays in transfer, as observed in several case reports in the systematic review [15B] from remote regions, correlated with development of infection, progression of compartment syndrome or delayed recognition of organ injury [4,34,45]. During transport, repeated assessment of bleeding, perfusion, respiratory status and level of consciousness is essential. Field responders should avoid deep probing of wounds and should refrain from attempting closure, as this may trap contaminants or compromise subsequent surgical evaluation.
Ultimately, the consistent message from both the observational hunters cohort [15A] and the systematic review [15B] was that early management must be systematic, cautious and oriented toward rapid identification of hidden injury. The combination of forceful penetration, contamination and unpredictable wound architecture makes wild-boar trauma a deceptively complex presentation requiring rigorous initial assessment [37,42,44].
Figure 1 presents a field-oriented management algorithm informed by evidence from both the observational hunters cohort [15A] and the systematic review [15B].
3.4. Diagnostic Imaging
The observational hunters cohort [15A] did not contain structured information on the use of diagnostic imaging. The dataset did not specify whether radiographs, ultrasound or CT were performed, nor did it provide imaging findings or described how imaging influenced management decisions. Because imaging was not captured as a variable, no conclusions could be drawn from the observational hunters cohort [15A] regarding typical diagnostic pathways or the frequency and relevance of imaging in wild-boar–related injuries.
The systematic review [15B] expanded on the essential role of imaging across a broader range of clinical presentations. In thoracic injuries, radiography and CT identified pneumothorax, hemothorax, pulmonary contusions and rib fractures [4,23,36]. Subtle chest findings on physical examination frequently masked profound internal compromise identified only after imaging [4,23,36]. In abdominal trauma, CT was indispensable to detect free air, organ lacerations, mesenteric injury or retroperitoneal involvement [4,34,50]. In several international cases, initial examination suggested only superficial injuries, yet imaging revealed deep visceral penetration requiring urgent laparotomy [4,34,45]. The systematic review [15B] also highlighted the value of ultrasound, particularly eFAST, in resource-limited environments [4,30,36]. Portable ultrasound enabled rapid identification of hemoperitoneum or pneumothorax in remote settings, guiding immediate management decisions while awaiting transfer [4,30,36].
Joint-related injuries also benefit from imaging. In reports of hand or lower-extremity wounds with suspected joint penetration, CT or radiography was critical in determining whether joint capsules were violated [4,24,44]. Tendon injuries require careful evaluation with ultrasound or MRI, though the latter is rarely performed acutely. Foreign body detection is another important imaging indication. Multiple cases in the systematic review [15B] described retained tusk fragments or embedded environmental debris that were only detected after imaging [4,23,45].
Across both evidence sources [15A,15B], imaging was consistently shown to reduce the risk of missed injury, refined operative planning and improved patient outcomes. The complexity and variability of tusk-inflicted wound trajectories make advanced imaging not just beneficial but often essential [30,36,45].
Table 3 presents the differential diagnosis and associated imaging indications, informed by data from the observational hunters cohort [15A] and the systematic review [15B].
3.5. Operative Management
Operative treatment in the observational hunters cohort [15A] was closely aligned with the predefined injury categories. All open injuries requiring inpatient care underwent surgery, whereas outpatient open injuries often received operative wound management without admission. Closed injuries were generally treated conservatively. The dataset did not include details about the surgical procedures themselves, such as the extent of debridement, wound exploration or closure strategy. Therefore, it was not possible to characterize typical operative findings or techniques based on the observational hunters cohort [15A] alone. Four participants provided qualitative descriptions of later complications that required revision surgery – such as infection, necrosis, sepsis, compartment syndrome or removal of a retained foreign body – but these narratives reflect individual cases and cannot be generalized. Overall, the observational hunters cohort [15A] documented whether surgery occurred, but not the specific operative approaches or intraoperative findings.
The systematic review [15B] highlighted the importance of aggressive and early operative management. Numerous international cases described severe infections and functional impairments arising when initial debridement was insufficient or when wound closure occurred prematurely [4,36,44]. Tendon injuries, nerve lacerations and vascular disruptions were frequently identified only during surgical exploration [4,24,29]. Thoracic injuries occasionally required chest tube placement, removal of foreign bodies or even thoracotomy [4,23,36]. Abdominal injuries mandated exploratory laparotomy, with several cases involving repair of bowel perforations, control of mesenteric bleeding or management of organ injury [4,40,45]. In partially healed or delayed-presenting cases, surgeons sometimes encountered necrotic tissue, abscess formation or advanced soft-tissue infection requiring extensive secondary debridement [4,44,45].
Complex extremity injuries often involved multiple staged procedures, particularly when large soft-tissue defects required flap coverage or grafting [4,34,44]. Joint involvement posed additional challenges, as penetrating joint trauma carries a high risk of septic arthritis. Washout, synovectomy and prolonged antibiotic therapy were frequently necessary [4,24,44]. The evidence also supports avoiding overly conservative surgical approaches. Minimal debridement or failure to explore the full wound tract increased the likelihood of complications and prolonged recovery [4,36,44].
Across the systematic review [15A], operative principles converged on several core themes: follow the wound tract to its deepest point; remove all devitalized and contaminated tissue; irrigate extensively; avoid early closure; reassess frequently; and coordinate multidisciplinary care when complex anatomical regions are involved [4,34,45].
3.6. Infection Prophylaxis and Antibiotic Management
The structured dataset of the observational hunters cohort [15A] did not include information on infection prophylaxis, antibiotic use or contamination characteristics. It therefore did not document whether antibiotics were administered routinely, which agents were used or how long therapy was continued. Among the four participants who provided extended qualitative accounts, postoperative infections and wound complications were described, and these cases required additional surgical management. While these narratives demonstrate that infections occurred in individual cases, they did not allow conclusions about the overall frequency of infection or typical prophylactic strategies in the observational hunters cohort [15A]. In summary, the dataset recorded treatment pathways and outcomes, but offered no systematic information on antibiotic management or infection prevention practices.
The systematic review [15B] documented a broad range of bacterial pathogens associated with wild-boar injuries. Identified organisms include Pasteurella species, Actinobacillus species, Streptococcus species, Staphylococcus species, anaerobes and various components of soil and environmental microbiota [4,34,36,40,44,45]. Several infections progressed to severe soft-tissue infection, septic arthritis or osteomyelitis [4,24,44]. Necrotizing soft-tissue infections were reported in patients in whom initial wound care was inadequate or of patients presented late [4,36,44]. Deep infections involving tendon sheaths or closed joint spaces required repeated surgical washouts and prolonged intravenous antibiotic therapy [4,24,44].
The systematic review [15B] also emphasized the need for antibiotic regimens that provide broad coverage of both aerobic and anaerobic bacteria. Amoxicillin–clavulanate was commonly used given its wide spectrum [4], but alternative regimens may be required based on allergy profiles or local resistance patterns. In severe or life-threatening cases, combinations of agents targeting Gram-negative rods, Gram-positive organisms and anaerobes are advisable. Duration of therapy varied based on wound severity, operative findings and contamination level [4,37,43]. In any case, aggressive antibiotic therapy significantly reduces the likelihood of infection-related complications.
3.7. Rabies and Tetanus Management
Rabies and tetanus prevention are integral parts of early management in wild-boar trauma. The observational hunters cohort [15A] did not collect data on rabies or tetanus prophylaxis. The systematic review [15B] presented a heterogeneous picture of the risk of rabies. In countries where wildlife rabies remains endemic, postexposure rabies prophylaxis was frequently administered after wild-boar injuries, particularly when deep wounds or bite-associated mechanisms were involved [4,44,45]. Several reports described administration of both rabies vaccine and rabies immunoglobulin when the rabies status of the wild boar could not be confirmed [4,36,44]. Conversely, in many European and East Asian regions where wild boars do not serve as rabies reservoirs, routine rabies prophylaxis was rarely indicated [4,7,23].
The consistent recommendation is that rabies prophylaxis should be determined by regional epidemiology rather than the species involved. In contrast, tetanus prophylaxis should be provided universally for all open wild-boar injuries given the high contamination burden and the severe consequences of tetanus infection.
3.8. Complications
Complications associated with wild-boar trauma are varied and may significantly impact recovery and long-term function. The dataset of the observational hunters cohort15A did not document specific medical complications such as infection rates, bleeding problems, neurovascular deficits or other acute or delayed sequelae. It reported only overall healing outcomes and whether persistent functional impairment remained after recovery. Complete healing without lasting impairment was common among participants with closed injuries (22 of 23; 95.7%) and outpatient open injuries (45 of 46; 97.8%), while 8 of 32 (25%) participants with inpatient open injuries reported persistent functional limitations. These residual limitations reflect the greater severity of injuries requiring hospital admission, although the dataset did not specify the underlying causes. Four participants provided extended qualitative accounts of postoperative complications – including delayed infections, wound necrosis, sepsis, compartment syndrome and a retained foreign body requiring removal. These examples illustrate the potential range of complications but cannot be generalized to the full observational hunters cohort [15A]. Overall, the structured data allowed conclusions only about final functional outcomes, not the specific complications that occurred along the treatment course.
The systematic review [15B] described a broad and often severe range of complications. Deep soft-tissue infections, necrotizing fasciitis, septic arthritis and osteomyelitis were well documented [4,24,45]. Vascular complications included pseudoaneurysms, delayed hemorrhage and thrombosis [4,34,49]. Nerve injuries ranged from transient palsies to complete transection requiring surgical repair [4,34,46]. In abdominal and thoracic injuries, delayed recognition of visceral damage led to peritonitis, empyema, overwhelming infection or systemic sepsis [4,23,45]. Several fatal cases resulted from massive hemorrhage, delayed presentations or missed internal injuries [41,45,50]. Chronic pain, limited joint mobility and functional impairment were common in survivors of complex extremity injuries [4,44,52]. Taken together, the evidence highlights that complications can arise even when initial presentation appears mild [9,35,37].
Both the observational hunters cohort [15A] and the systematic review [15B] emphasized that early, thorough management reduces but does not eliminate the risk of complications. Ongoing monitoring, multidisciplinary care and patient education regarding warning signs of infection or delayed vascular compromise are essential components of management.
4. Discussion
The combined evidence from the observational hunters cohort [15A] and the international literature summarized in the systematic review [15B] demonstrates that wild-boar–related trauma constitutes a distinct and often complex clinical challenge. Each evidence source contributed a different type of information. The structured observational hunters cohort [15A] provided consistent epidemiologic data on the circumstances of injury, the characteristics of affected hunters, the treatment settings and the overall healing outcomes. It established that most injuries occured during daytime tracking operations, predominantly involved experienced hunters and were frequently caused by male animals [15A]. The dataset also documented the time to first help and the subsequent treatment pathway, although it did not contain systematic information on wound morphology, contamination, imaging findings or intraoperative details.
The systematic review [15B] complemented these structured observations by providing detailed clinical and forensic descriptions across a wide range of environments, including agricultural, wilderness, peri-urban and subsistence contexts. Despite geographical and contextual heterogeneity, the reviewed cases revealed recurring clinical patterns: deep and unpredictable wound trajectories, extensive soft-tissue disruption, heavy environmental contamination and potentially severe neurovascular or visceral injury even when the external wound appears deceptively small. Thoracoabdominal injuries, although less common, were associated with disproportionate morbidity and mortality. These reports highlight the need for early imaging, aggressive debridement, staged wound management and broad-spectrum antibiotic therapy.
Several themes emerged when these two evidence streams [15A,15B] were integrated. First, the structured, observational hunters cohort [15A] defined who was injured and how injuries were managed, whereas the systematic review [15B] clarified how severe such injuries can be and what hidden risks must be anticipated. Second, the consistency of injury mechanisms across global case reports suggests that certain management principles – such as prioritizing hemorrhage control, maintaining a high index of suspicion for deep structural involvement and avoiding premature wound closure – are broadly applicable. Third, thoracoabdominal and major vascular injuries, though infrequent, require rapid escalation to advanced care. Fourth, the increasing wild-boar populations in many regions may increase opportunities for human–animal encounters, reinforcing the need for public-health measures and clinical preparedness.
Overall, integrating the structured data of the observational hunters cohort [15A] with the diverse international experience summarized in the systematic review [15B] enabled a comprehensive and practical approach to assessment and management, particularly in remote or resource-limited settings where these rare but potentially life-threatening injuries may occur.
5. Recommendations / Management Guideline
The development of clinical recommendations for wild-boar-related trauma relied on integrating the structured findings of the observational hunters cohort [15A] with the diverse international experiences summarized in the systematic review [15B]. Although the overall incidence of these injuries is low, their potential severity requires a systematic and well-defined management approach.
Early clinical priorities emphasize airway, breathing and circulation. Hemorrhage control is critical, as uncontrolled bleeding may be a major contributor to morbidity and mortality. Direct pressure should be applied immediately, followed by hemostatic dressings or tourniquets when necessary. These measures should be maintained during transport and reassessed periodically.
Imaging should be performed early and tailored to the suspected injury. Plain radiographs, ultrasound and CT are essential for evaluating wound trajectories, detecting fractures, identifying foreign bodies and assessing for thoracoabdominal involvement. In resource-limited settings, portable ultrasound may be the only available modality and can guide immediate management decisions.
Operative management should be proactive and extensive. Surgical exploration must follow the wound tract to its deepest point, exposing all areas of tissue injury. Wide debridement and thorough irrigation are essential because of the heavy contamination. Primary closure is rarely appropriate initially, and staged procedures with delayed closure or secondary intention healing are often required.
Infection prophylaxis must begin early, ideally at first clinical contact. Broad-spectrum antibiotics should target both aerobic and anaerobic organisms. Duration of therapy depends on wound severity, contamination level, operative findings and presence of infection or joint involvement. Tetanus prophylaxis is universally required considering the contamination burden. Rabies prophylaxis must be based on regional epidemiology rather than species-specific assumptions.
Evacuation decisions must prioritize early transfer for patients with suspected deep structural injury, neurovascular compromise, thoracoabdominal involvement or uncontrolled bleeding. Field responders should avoid deep probing of wounds or attempting closure. During transfer, continuous monitoring of airway, breathing and circulation is essential.
Together, these recommendations form a cohesive management framework based on consistent injury patterns and clinical needs demonstrated across structured observational and international evidence. Table 4 summarizes these key recommendations.
6. Conclusion
Wild-boar–related trauma represents a rare but clinically serious subset of wilderness and rural injuries that can result in deep contamination, complex soft-tissue damage and, in select cases, life-threatening complications. The combined use of a structured observational hunters cohort [15A] and a comprehensive systematic review [15B] provides, for the first time, an integrated evidence base from which to derive practical, field-oriented recommendations for assessment, early management and definitive care.
As seen in other uncommon but high-risk trauma scenarios – most notably explosion injuries, for which detailed clinical guidelines have recently been published [11,12] – the development of standardized guidance is particularly valuable when provider experience is inherently limited. Although the injury mechanisms differ completely, the comparison underscores a shared structural need: clinicians must be able to rely on reproducible, evidence-informed algorithms when confronted with rare events that nevertheless demand rapid, high-consequence decisions.
Similarly, existing guidelines from the Wilderness Medical Society – including those addressing drowning management [13] and the medical oversight of search-and-rescue operations [14] – illustrate the broader importance of formalized approaches to care in remote, resource-limited and operationally constrained environments. The present guideline aligns with this tradition by providing structured recommendations designed specifically for wild-boar–related trauma encountered in wilderness or austere contexts.
By synthesizing epidemiologic insights, detailed case descriptions and global clinical experience, this guideline aims to support clinicians, wilderness responders and prehospital providers who may face these rare but potentially severe injuries. Standardized, context-appropriate management principles may improve patient outcomes, reduce preventable complications and promote consistent clinical decision-making across diverse care environments.
Author Contributions
Conceptualization, M.M. and C.S..; methodology, M.M. and C.S.; validation, M.M. and C.S..; formal analysis, C.S.; investigation, M.M.; resources, M.M. and C.S.; data curation, M.M. and C.S.; writing—original draft preparation, C.S.; writing—review and editing, M.M., L.M, S.H. and N.M.; supervision, M.M.; project administration, M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Ludwig-Maximilians-University of Munich (Munich, Germany; reference 24-0377; date of approval 05 June 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The anonymized datasets generated and analyzed during this study are available from the corresponding author upon reasonable request and in compliance with institutional and data protection regulations.
Conflicts of Interest
None.
References
- Massei, G.; Kindberg, J.; Licoppe, A.; Gačić, D.; Šprem, N.; Kamler, J.; Baubet, E.; Hohmann, U.; Monaco, A.; Ozoliņš, J.; Cellina, S.; Podgórski, T.; Fonseca, C.; Markov, N.; Pokorny, B.; Rosell, C.; Náhlik, A. Wild boar populations up, numbers of hunters down? A review of trends and implications for Europe. Pest Manag. Sci. 2015, 71(4), 492–500. [CrossRef]
- Kamieniarz, R.; Jankowiak, Ł.; Fratczak, M.; Panek, M.; Wojtczak, J.; Tryjanowski, P. The relationship between hunting methods and the sex, age and body mass of wild boar Sus scrofa. Animals 2020, 10(12), 2345. [CrossRef]
- Vajas, P.; Von Essen, E.; Tickle, L.; Gamelon, M. Meeting the challenges of wild boar hunting in a modern society: The case of France. Ambio 2023, 52(8), 1359–1372. [CrossRef]
- Pujol, O.; Nuño, M.; Minguell, J.; Selga, J.; Tomás, J.; Rodríguez, D.; Martínez, X.; Mentaberre, G.; López-Olvera, J.R. Characterization and treatment protocol of injuries inflicted to humans by synurbic European wild boars (Sus scrofa). Eur. J. Trauma Emerg. Surg. 2024, 50(5), 2595–2604. [CrossRef]
- Mayer, J.J. Wild pig attacks on humans. In Proceedings of the 15th Wildlife Damage Management Conference; Armstrong, J.B., Gallagher, G.R., Eds.; 2013; pp. 17–35.
- Mayer, J.J.; Garabedian, J.E.; Kilgo, J.C. Human fatalities resulting from wild pig attacks worldwide: 2000–2019. Hum. Wildl. Interact. 2023, 17(1), 3–20. [CrossRef]
- Gudmannsson, P.; Berge, J. The forensic pathology of fatal attacks by the large mammals inhabiting the nordic wilderness-a literature review. J. Forensic Sci. 2019, 64(4), 976–981. [CrossRef]
- Bury, D.; Langlois, N.; Byard, R.W. Animal-related fatalities--part I: characteristic autopsy findings and variable causes of death associated with blunt and sharp trauma. J. Forensic Sci. 2012, 57(2), 370–374. [CrossRef]
- Freer, L. North American wild mammalian injuries. Emerg. Med. Clin. N. Am. 2004, 22(2), 445–473. [CrossRef]
- Bury, D.; Langlois, N.; Byard, R.W. Animal-related fatalities--part II: characteristic autopsy findings and variable causes of death associated with envenomation, poisoning, anaphylaxis, asphyxiation, and sepsis. J. Forensic Sci. 2012, 57(2), 375–380. [CrossRef]
- Hauer, T.; Grobert, S.; Wenniges, H.; Huschitt, N.; Willy, C. Explosionstrauma Teil 1: Physikalische Grundlagen und Pathophysiologie [Explosion trauma part 1 : Physical principles and pathophysiology]. Unfallchirurg. 2022, 125(2), 145-159. German. [CrossRef]
- Hauer, T.; Grobert, S.; Gaab, J.; Huschitt, N.; Willy, C. Explosionstrauma Teil 2: Medizinische Behandlungsprinzipien [Blast injuries part 2 : Principles of medical treatment]. Unfallchirurg. 2022, 125(3), 227-242. German. [CrossRef]
- Davis, C.A.; Schmidt, A.C.; Sempsrott, J.R.; Hawkins, S.C.; Arastu, A.S.; Giesbrecht, G.G.; Cushing, T.A. Wilderness Medical Society clinical practice guidelines for the treatment and prevention of drowning: 2024 update. Wilderness Environ Med. 2024, 35(1_suppl), 94S-111S. [CrossRef]
- Davis, C.A.; Lowry, C.; Billin, A.; Laskowski-Jones, L.; Sheets, A.; Fifer, D.; Hawkins, S.C. Wilderness Medical Society clinical practice guidelines for medical direction of search and rescue teams. Wilderness Environ Med. 2024, 35(3), 314-327. [CrossRef]
- Maier, M.; Maier, L.P.N., Hackl., S.; Eckermann, N.J.; Maffulli, N.; Barapatre, N.; Schmitz, C. At times, hunters should beware. Trauma from wild boar encounters during hunting: a nationwide survey in Germany with a systematic literature review. Preprint. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; Glanville, J.; Grimshaw, J.M.; Hróbjartsson, A.; Lalu, M.M.; Li, T.; Loder, E.W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L.A.; Stewart, L.A.; Thomas, J.; Tricco, A.C.; Welch, V.A.; Whiting, P.; Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [CrossRef]
- Ammann, L.M.; Barnum, M.; Cardin, S. Traumatic knee arthrotomy induced by wild boar tusk in a 15-year-old male: a case report. Wilderness Environ. Med. 2026, 37(1), 102–105. [CrossRef]
- Okamoto, N.; Nagasawa, H.; Miura, K.; Tanaka, N.; Maekawa, C.; Yanagawa, Y. Open digital fractures by boar bite. J. Emerg. Trauma Shock 2025, 18(3), 145–146. [CrossRef]
- Adhikari, J.N.; Bhattarai, B.P.; Thapa, T.B. Correlates and impacts of human-mammal conflict in the central part of Chitwan Annapurna Landscape, Nepal. Heliyon 2024, 10(4), e26386. [CrossRef]
- Iacoponi, N.; Bugelli, V.; Fico, R.; Giaconi, C.; Lorenzini, R.; Minervini, P.; Di Paolo, M. Boar hunt or Manhunt? fatality during a wild boar hunting expedition. Need for a multidisciplinary forensic approach. Leg. Med. 2024, 69, 102459. [CrossRef]
- Köroğlu, M.; Özdeş, H.U.; Acet, Ö.; Sarıbas, T.; Ergen, E.; Karakaplan, M.; Aslantürk, O. Common peroneal nerve injury caused by a wild boar attack. Wilderness Environ. Med. 2024, 35(1), 88–93. [CrossRef]
- Na, K.; Oh, B.H.; Lee, J.; Cho, M.J.; Lee, M.; Kim, H.R. Penetrating head injury resulting from wild boar attack in republic of korea: a case report. Korean J. Neurotrauma 2023, 19(4), 496–501. [CrossRef]
- Shimizu, Y.; Kubo, H. Foreign body in chest wall with traumatic pneumothorax caused by fang of wild boar. Kyobu Geka 2023, 76, 455–458. (In Japanese).
- Thalgaspitya, S.; Wijerathne, B.; Madusanka, M. The wild boar Sus scrofa cristatus attacks in Sri Lanka: a case series and review of literature. Anuradhapura Med. J. 2023, 17(3), 27–34. [CrossRef]
- Zaimoglu, M.; Mete, E.B.; Bayatli, E.; Guner, Y.E.; Ozdemir, A.; Buyuktepe, M.; Eroglu, U. A rare cause of foot drop: wild boar bites. J. Ankara Univ. Fac. Med. 2023, 76, 166–168.
- Ketenci, H.Ç.; Boz, H.; Kırcı, G.S.; Özer, E.; Beyhun, N.E.; Büyük, Y. An evaluation of traumatic deaths associated with animal attacks: A 10-year autopsy study. Ulus. Travma Acil Cerrahi Derg. 2022, 28(3), 254–261. [CrossRef]
- Özsoy, S.; Ketenci, H.C.; Askay, M. Fatal land hunting-related injuries in the Eastern Black Sea region-Turkey. Ulus. Travma Acil Cerrahi Derg. 2022, 28(10), 1494–1499. [CrossRef]
- Kiran, M.; Shetty, M.; Shetty, S. Exsanguinated to death: A case of death due to wild boar attack. J. Indian Acad. Forensic Med. 2021, 43(2), 191–193. [CrossRef]
- Quraishi, A.H.; Damdoo, A.; Srinivasan, S.; Umare, G.; Tongse, P. Mechanisms and patterns of animal-related injuries in patients admitted to a major trauma center in central India. J. Emerg. Trauma Shock 2021, 14(3), 190–191. [CrossRef]
- Singh, P.K.; Ali, S.M.; Radhakrishnan, R.V.; Mohanty, C.R.; Sahu, M.R.; Patro, B.P.; Ms, I.; Panda, S.K. Pattern of injuries due to wild animal attack among patients presenting to the emergency department: A retrospective observational study. Chin. J. Traumatol. 2021, 24(6), 383–388. [CrossRef]
- Ruda, A.; Kolejka, J.; Silwal, A.T. Spatial concentrations of wildlife attacks on humans in chitwan national park, nepal. Animals 2020, 10(1), 153. [CrossRef]
- Dokter, M.; Philipp, K.P.; Bockholdt, B. Der vermeidbare (?) Jagdunfall – tödliche Oberschenkelverletzung durch ein Wildschwein. Rechtsmedizin 2018, 28, 442–445. [CrossRef]
- Nagasawa, H.; Omori, K.; Takeuchi, I.; Fujiwara, K.; Uehara, H.; Jitsuiki, K.; Kondo, A.; Ohsaka, H.; Ishikawa, K.; Yanagawa, Y. A case of near-fatal drowning caused by an attack from a wild boar. Wilderness Environ. Med. 2018, 29(4), 549–551. [CrossRef]
- Okano, I.; Midorikawa, Y.; Kushima, N.; Watanabe, Y.; Sugiyama, T.; Mitachi, K.; Shinohara, K.; Sawada, T.; Inagaki, K. Penetrating anorectal injury caused by a wild boar attack: a case report. Wilderness Environ. Med. 2018, 29(3), 375–379. [CrossRef]
- Oliveira, S.V. de; Vargas, A.; Rocha, S.M.; Pereira, L.R.M.; Oliveira, C.G. de; Silva, V.S. The nature of attacks by wild boar (Sus scrofa) and wild boar/domestic pig hybrids (“Javaporcos”) and the conduct of anti-rabies care in Brazil. InterAm. J. Med. Health 2018, 1, e-201801001. [CrossRef]
- Singaravelu, K.P.; Pandit, V.; Saya, R.P.; Nagasubramanyam, V. Unusual cause of chest trauma: Case report of wild boar attack. J. Dr. NTR Univ. Health Sci. 2018, 7(4), 285. [CrossRef]
- Nagasawa, H.; Omori, K.; Maeda, H.; Takeuchi, I.; Kato, S.; Iso, T.; Jitsuiki, K.; Yoshizawa, T.; Ishikawa, K.; Ohsaka, H.; Yanagawa, Y. Bite wounds caused by a wild boar: a case report. Wilderness Environ. Med. 2017, 28(4), 313–317. [CrossRef]
- Silwal, T.; Kolejka, J.; Bhatta, B.P.; Rayamajhi, S.; Sharma, R.P.; Poudel, B.S. When, where and whom: assessing wildlife attacks on people in Chitwan National Park, Nepal. Oryx 2017, 51, 370–377. [CrossRef]
- Tumram, N.K.; Ambade, V.N.; Dixit, P.G. Human fatalities caused by animal attacks: A six-year autopsy study. Med. Leg. J. 2017, 85(4), 194–199. [CrossRef]
- Bhingare, P.D.; Shelke, U.R.; Bang, Y.A. A case of recto-vesico-cutaneous fistula following perineal injury by wild boar. J. Clin. Diagn. Res. 2016, 10(5), PD03–PD04. [CrossRef]
- Akhade, S.P.; Rohi, K.R.; Phad, L.G.; Dixit, P.G. Fatal penetrating lacerated wound by tusk of indian wild boar. J. Indian Acad. Forensic Med. 2015, 37(1), 100–102. [CrossRef]
- Tumram, N.K.; Dhawne, S.G.; Ambade, V.N.; Dixit, P.G. Fatal tusk injuries from a wild boar attack. Med. Leg. J. 2015, 83(1), 54–56. [CrossRef]
- Sprem, N.; Skavić, P.; Dezdek, D.; Keros, T. The wild boar attack--a case report of a wild boar inflicted injury and treatment. Coll. Antropol. 2014, 38(4), 1211–1212.
- Sprem, N.; Skavić, P.; Krupec, I.; Budor, I. Patterns of game animal attacks on hunters in Croatia over a 13-year period. Wilderness Environ. Med. 2013, 24(3), 267–272. [CrossRef]
- Attarde, H.; Badjate, S.; Shenoi, S.R. Wild boar inflicted human injury. J. Maxillofac. Oral Surg. 2011, 10(1), 77–79. [CrossRef]
- Kose, O.; Guler, F.; Baz, A.B.; Akalin, S.; Turan, A. Management of a wild boar wound: a case report. Wilderness Environ. Med. 2011, 22(3), 242–245. [CrossRef]
- Rajendra, K.R.; Chandru, K. Death—Who Caused It? Wild Boar or Doctor—Case Report. Anil Aggrawal’s Internet Journal of Forensic Medicine and Toxicology 2011, 11, No. 2. Available online: https://anil.aggrawal.org/ij/vol_012_no_002/papers/paper001.html (accessed on 16 February 2026).
- Shetty, M.; Menezes, R.G.; Kanchan, T.; Shetty, B.S.; Chauhan, A. Fatal craniocerebral injury from wild boar attack. Wilderness Environ. Med. 2008, 19(3), 222–223. [CrossRef]
- Gunduz, A.; Turedi, S.; Nuhoglu, I.; Kalkan, A.; Turkmen, S. Wild boar attacks. Wilderness Environ. Med. 2007, 18(2), 117–119. [CrossRef]
- Manipady, S.; Menezes, R.G.; Bastia, B.K. Death by attack from a wild boar. J. Clin. Forensic Med. 2006, 13(2), 89–91. [CrossRef]
- Escande, F.; Bailly, A.; Bone, S.; Lemozy, J. Actinobacillus suis infection after a pig bite. Lancet 1996, 348, 888. [CrossRef]
- Gubler, J.G.H. Septic arthritis of the knee induced by Pasteurella multocida and Bacteroides fragilis following an attack by a wild boar. J. Wilderness Med. 1992, 3(3), 288–291. [CrossRef]
- Van Demark, R.E., Sr.; Van Demark, R.E., Jr. Swine bites of the hand. J. Hand Surg. Am. 1991, 16(1), 136–138. [CrossRef]
- Goldstein, E.J.; Citron, D.M.; Merkin, T.E.; Pickett, M.J. Recovery of an unusual Flavobacterium group IIb-like isolate from a hand infection following pig bite. J. Clin. Microbiol. 1990, 28, 1079–1081. [CrossRef]
- Barnham, M. Pig bite injuries and infection: report of seven human cases. Epidemiol. Infect. 1988, 101(3), 641–645. [CrossRef]
- Barss, P.; Ennis, S. Injuries caused by pigs in Papua New Guinea. Med. J. Aust. 1988, 149, 649–656. [CrossRef]
Figure 1.
Field-oriented algorithm summarizing recommended assessment and management steps for wild-boar–related trauma.
Figure 1.
Field-oriented algorithm summarizing recommended assessment and management steps for wild-boar–related trauma.
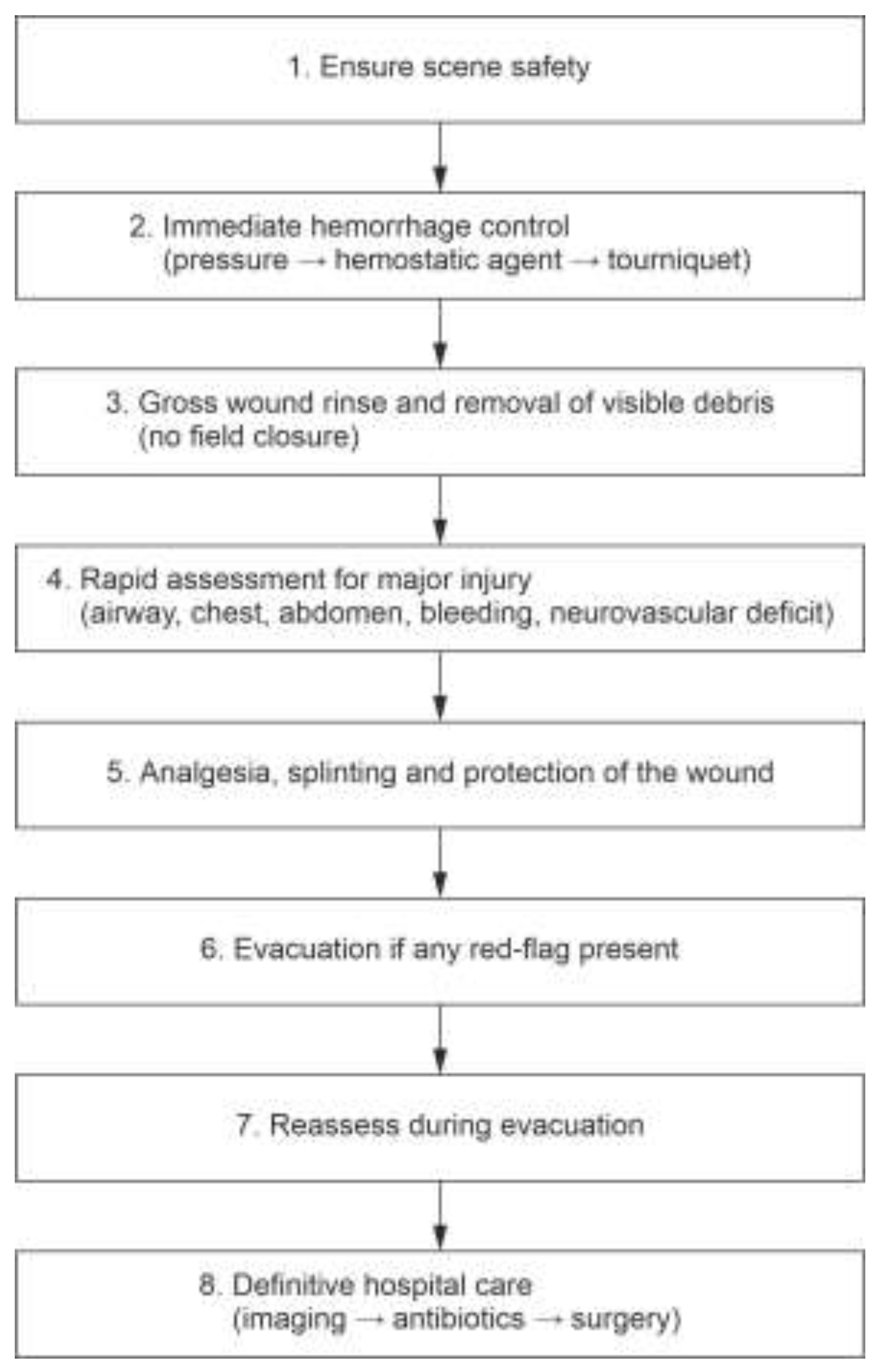

Table 1.
Overview of all studies included in the systematic review [15B] informing this guideline. Abbreviations: Y, Year of publication; C/R, country / region; N, number of human cases, WB, wild boar / wild pig (Sus scrofa); DP, domestic pig; WB/DP, wild–domestic hybrid (“javaporco” etc.).
Table 1.
Overview of all studies included in the systematic review [15B] informing this guideline. Abbreviations: Y, Year of publication; C/R, country / region; N, number of human cases, WB, wild boar / wild pig (Sus scrofa); DP, domestic pig; WB/DP, wild–domestic hybrid (“javaporco” etc.).
| Study | Y | C/R | Study type | N | Animal type | Main content / relevance |
| [17] | 2025 | USA (central Florida) | Case report | 1 | WB | Pediatric knee arthrotomy from WB tusk during hunting; intra-articular air on imaging; required urgent irrigation/debridement. Cultures grew Stenotrophomonas maltophilia and Aspergillus spp.; recovered fully after targeted therapy. |
| [18] | 2025 | Japan | Case report | 1 | WB | Penetrating thoracic injury with pneumothorax; CT-based diagnosis and chest tube placement; good recovery. |
| [19] | 2024 | Nepal | Case report | 1 | WB | Penetrating lower-extremity WB injury in a rural setting; deep soft-tissue laceration with significant contamination; treated with debridement, irrigation, and antibiotics; uneventful recovery. |
| [20] | 2024 | Japan | Case report | 1 | WB | Penetrating upper-body WB injury in suburban environment; deep soft-tissue trauma requiring surgical debridement; full recovery. |
| [21] | 2024 | Turkey | Case report | 1 | WB | Lower-extremity WB laceration with extensive contamination; operative irrigation/debridement and antibiotics; uncomplicated outcome. |
| [4] | 2024 | Spain | Case series / institutional protocol revision | Several | WB | Trauma service experience with WB extremity injuries; emphasizes standardized debridement protocol and broad-spectrum antibiotics. |
| [22] | 2023 | South Korea | Case report | 1 | WB | Lower-limb WB bite/laceration; surgically treated with irrigation/debridement and antibiotics; favorable recovery. |
| [23] | 2023 | Japan | Case report | 1 | WB | Chest/upper-body trauma from WB; emphasizes need for imaging and monitoring even in apparently stable patients. |
| [24] | 2023 | Sri Lanka | Case series | Several | WB | Series of WB attacks in agricultural workers; includes severe perineal, thigh, abdominal injuries with evisceration; describes surgery, tetanus and rabies prophylaxis. |
| [25] | 2023 | Turkey | Case report | 1 | WB | Peroneal nerve injury from deep calf laceration; required neurolysis; persistent foot drop; highlights neurovascular risk. |
| [26] | 2022 | Turkey | Case report | 1 | WB | Lower-extremity boar wound; illustrates management and need for surgical debridement and antibiotics. |
| [27] | 2022 | Turkey | Case report | 1 | WB | Knee joint–penetrating boar injury with joint involvement; orthopedic washout and infection prevention. |
| [28] | 2021 | India | Small series / retrospective | Several | WB/DP (mixed context) | Describes patterns of pig-related wounds (mostly lower-limb), mechanisms, and outcomes; provides additional Indian data on severity and contamination. |
| [29] | 2021 | Oman | Retrospective review of animal-related injuries | Subset | WB among other species | Describes patterns of wildlife trauma; WB cases characterized by lower-limb soft-tissue injuries requiring operative care. |
| [30] | 2021 | India | Animal-attack review | Subset | WB among others | Provides broader context of wildlife injuries in India; WB attacks form a small but severe portion. |
| [31] | 2020 | Europe | Spatial / epidemiologic study | N/A | Wildlife including WB | Spatial analysis of wildlife-related injuries and conflicts; relevant for prevention and risk mapping in regions with WB. |
| [32] | 2018 | Global | Review of wildlife trauma | Mixed | Various wild animals | Broad review of animal-related trauma; WB injuries are one component; used mainly for general trauma context, not specific case data. |
| [33] | 2018 | Japan | Case report | 1 | WB | Penetrating chest / rib fracture / pneumothorax; demonstrates thoracic risk even with small skin wounds. |
| [34] | 2018 | Japan | Case report (WEM) | 1 | WB | Complex attack: femoral artery and sciatic nerve injury, anorectal injury, pelvic fractures, open pneumothorax; prolonged, staged surgical management and complications. |
| [35] | 2018 | Brazil (national) | Retrospective analysis of human rabies treatment forms | 309 WB / WB–DP attacks | WB and WB/DP (“javaporcos”) | Nationwide Brazilian dataset: 309 attacks (271 WB, 38 hybrids); mainly deep single bites to lower limbs; anti-rabies serum+vaccine most commonly indicated; shows expanding WB invasion and health-system response. |
| [36] | 2018 | India | Case report | 1 | WB | Penetrating chest injury from WB with pneumothorax and subcutaneous emphysema; diagnosed via ultrasound and CT; treated with tube thoracostomy. |
| [37] | 2017 | Japan | Case report | 1 | WB | WB bite wounds to lower extremity; significant contamination; wound infection requiring re-debridement. |
| [38] | 2017 | Nepal (Chitwan NP) | 10-year wildlife conflict registry | 38 WB attacks | WB | Wildlife attacks on people in buffer zone; 38 WB-related events with pattern of lower-limb injuries and risk factors (time of day, activity). |
| [39] | 2017 | India | 6-year autopsy series of animal-attack deaths | Subset | Mixed including WB | Describes human fatalities caused by animal attacks; WB attacks are a subset, emphasizing that WB can be a cause of fatal trauma. |
| [40] | 2016 | India | Case report | 1 | WB | Perineal penetrating injury with recto-vesico-cutaneous fistula after WB attack; complex pelvic reconstruction and fistula repair. |
| [41] | 2015 | India | Forensic case report | 1 | WB | Fatal penetrating thigh wound from WB tusk with femoral vessel injury; illustrates exsanguinating potential of lower-limb tusk injuries. |
| [42] | 2015 | India | Forensic case report | 1 | WB | Fatal tusk injuries to thigh with transection of femoral vessels and nerve; provides detailed autopsy description of hemorrhagic death. |
| [43] | 2014 | Croatia | Case report | 1 | WB | Single WB-inflicted lower-extremity bite wounds in hunter; irrigation, debridement, primary closure; antibiotics; no complications. |
| [44] | 2013 | Croatia | Retrospective series of hunter injuries | Several | Mixed game including WB | Patterns of game-animal attacks on hunters; WB a prominent species; lower-limb soft-tissue injuries dominate; most require surgical management. |
| [45] | 2011 | India | Case report | 1 | WB | Facial/maxillofacial injury caused by WB; deep soft-tissue laceration; emphasizes need for surgical debridement and layered closure. |
| [46] | 2011 | Turkey | Case report | 1 | WB | Severe thigh laceration from WB attack; surgically treated; underscores contamination risk and need for broad-spectrum antibiotics. |
| [47] | 2010 | India | Case report | 1 | WB | Severe scrotal/testicular laceration by WB; highlights groin vulnerability and reconstructive issues. |
| [48] | 2008 | India | Case report | 1 | WB | Major thigh injury with significant hemorrhage during WB encounter; demonstrates risk of shock and need for emergency surgery. |
| [49] | 2007 | Turkey | Case series | 3 | WB | “Wild Boar Attacks” – 3 rural cases; significant soft-tissue trauma, mostly lower extremities; one case with upper abdomen/chest involvement. |
| [50] | 2006 | India | Forensic case report | 1 | WB | Fatal WB attack with deep groin and thigh penetration and major vascular injury; classic example of exsanguination mechanism. |
| [51] | 1996 | France | Single infected-bite case | 1 | DP | Actinobacillus suis infection after DP bite to knee; highlights unusual pathogens and confirms amoxicillin-clavulanate as good empiric choice. |
| [52] | 1992 | Switzerland (WEM) | Case report | 1 | WB | Septic arthritis of knee after WB attack; mixed Pasteurella multocida and Bacteroides fragilis infection; classic example of deep joint contamination. |
| [53] | 1991 | USA | Case report | 1 | Domestic boar | Severe hand wound with deep-space infection after domestic boar bite; emphasizes need for aggressive debridement and antibiotic therapy. |
| [54] | 1990 | USA | Case report (microbiology) | 1 | Pig (DP) | Hand infection following pig bite; recovery of unusual Flavobacterium group IIb-like organism; part of pathogen spectrum relevant to pig / WB wounds. |
| [55] | 1988 | United Kingdom (North Yorkshire) | Case series | 7 | Swine (DP / boar) | “Pig bite injuries and infection”; deep posterior-thigh lacerations and other wounds; mixed infections (streptococci, Pasteurella, Bacteroides etc.); argues for broad-spectrum antibiotics in severe pig bites. |
| [56] | 1988 | Papua New Guinea | 6-year hospital-based review | 15 pig-injury admissions | Mainly DP, some feral pigs | Med J Aust paper: injuries caused by pigs; mixture of abdominal, chest, limb, and scrotal wounds; includes “sucking” chest wound, bilateral pneumothoraces, open fractures, nerve and tendon injuries; demonstrates severity of pig gorings. |
| [6] | 2023 | Global | Extended/updated review | >400 attacks / fatalities | Wild pigs | Expanded analysis of world-wide wild-pig attacks and fatalities; confirms pattern of severe soft-tissue and blunt trauma, with majority of deaths due to hemorrhage. |
| [3] | 2023 | France / Europe | Socio-ecologic analysis | N/A | WB | Addresses synurbic WB and human–boar conflicts in peri-urban settings; directly relevant for prevention and public-health messaging. |
| [2] | 2020 | Poland / Europe | Ecologic / management paper | N/A | WB | Explores WB population management, hunting pressure, and landscape changes; informs risk reduction discussion. |
| [7] | 2019 | Nordic countries / literature-based | Forensic literature review of fatal attacks by large mammals in the Nordic wilderness | 3 fatal WB cases extracted from literature | WB (plus bear, moose, wolf) | Reviews species-specific injury patterns in fatal attacks by brown bear, moose, wild boar, and wolf; WB section synthesizes three Indian fatal boar cases (lower-body tusk penetration, exsanguination or craniocerebral injury) to help forensic differentiation. |
| [1] | 2015 | Europe (general) | Ecologic / population review | N/A | WB | Describes expanding WB populations and implications for human–boar interactions and conflicts; crucial for prevention context. |
| [5] | 2013 | Global | Narrative review | 412 attacks compiled | Wild pigs (WB + feral) | Comprehensive global review of wild-pig attacks; describes circumstances (hunting, non-hunting), injury patterns (single lacerations, puncture wounds, fractures), and causes of death (mostly exsanguination). |
| [9] | 2004 | North America (Yellowstone / US context) | Narrative review of wild mammalian injuries | Not specified (review) | Various wild mammals (not pig-specific) | “North American wild mammalian injuries” (Emerg Med Clin N Am 2004); covers general patterns of wild animal trauma, field care, wound management, antibiotic choices, rabies & tetanus guidance; used for general wilderness/animal-attack management principles, not WB case data. |
Table 2.
Summary of injury patterns by anatomic region based on the observational hunters cohort [15A] and the systematic review [15B].
Table 2.
Summary of injury patterns by anatomic region based on the observational hunters cohort [15A] and the systematic review [15B].
| Anatomic region | Primary evidence [15A] | Additional findings [15B] | Clinical implications |
|---|---|---|---|
| Lower extremities | Most common injury site; deep penetrating wounds; heavy contamination. | Consistently reported internationally with long wound tracts. | High hemorrhage risk; mandatory imaging and exploration. |
| Groin / pelvis | Injuries near femoral vessels; soft-tissue avulsion. | Additional reports of vascular penetration and genital trauma. | Rapid hemorrhage control; vascular assessment essential. |
| Abdomen | Occasional upward penetration. | Multiple reports of peritoneal violation and visceral injury. | Exploratory laparotomy often required. |
| Thorax | Rare in cohort. | Reports of pneumothorax, hemothorax, rib fractures. | Requires immediate imaging. |
| Upper extremities | Mainly defensive wounds. | Deep-space infections and tendon injuries. | High infection risk. |
| Head / neck | Rare. | Severe and fatal cases reported. | Airway priority; rapid transfer. |
| Neurovascular structures | Occasional involvement. | Cases of nerve palsy and arterial injury. | Full neurovascular examination essential. |
Table 3.
Differential diagnoses and corresponding imaging indications for common wild-boar–related injury presentations.
Table 3.
Differential diagnoses and corresponding imaging indications for common wild-boar–related injury presentations.
| Presentation | Differential diagnoses | Imaging |
|---|---|---|
| Lower-extremity wound | Vascular injury, occult fracture | Doppler US, X-ray, CT angiography |
| Groin injury | Femoral vessel penetration | CT angiography |
| Abdominal penetration | Bowel perforation, organ injury | CT with contrast |
| Chest symptoms | Pneumothorax, hemothorax | X-ray, eFAST, CT |
| Neurologic deficit | Nerve injury, compartment syndrome | MRI |
| Joint penetration | Septic arthritis | X-ray, CT, operative assessment |
Table 4.
Summary of key recommendations for the assessment and management of wild-boar–related trauma.
Table 4.
Summary of key recommendations for the assessment and management of wild-boar–related trauma.
| Domain | Recommendation |
|---|---|
| Early assessment | High suspicion for deep injury |
| Hemorrhage control | Direct pressure, hemostatic agents, tourniquet |
| Imaging | X-ray, ultrasound, CT |
| Surgical care | Thorough exploration, delayed closure |
| Antibiotics | Early broad-spectrum therapy |
| Tetanus/rabies | Universal tetanus; rabies per region |
| Disposition | Early evacuation for major injury |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



