Submitted:
16 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Background: Type 2 diabetes mellitus (T2DM) is one of the most common non-communicable chronic diseases worldwide, with risk factors that can appear as early as adolescence. Socioeconomic status (SES), health behaviors, and health literacy determine health outcomes in the long term. Early identification of lifestyle, dietary habits, and diabetes risk in young people is crucial for prevention. The aim of this study was to explore the relationships between SES, T2DM risk, and diabetes-related knowledge among Hungarian high school students aged 16–20 years using the FINDRISC (Finnish Diabetes Risk Score) questionnaire adapted for adolescence. Method: A nationwide, cross-sectional questionnaire survey was conducted in Hungarian secondary schools (N=1,585). The SES status of respondents was determined using cluster analysis, and diabetes risk was assessed using a modified, age-adjusted FINDRISC score. Correlations were assessed through cross-tabulation and logistic regression analyses using SPSS version 27.0. Results: The prevalence of moderate to high diabetes risk was 7.3%. Students with low SES were significantly more likely to be classified into higher-risk categories (OR = 2.80; 95% CI: 1.35-5.81). A significant relationship was found between SES and FINDRISC-based risk categories (p<0.001). High-SES students had significantly higher levels of diabetes knowledge (OR = 2.44; p = 0.007). The proportion of correct responses to questions about insulin function and the effects of diet and exercise on blood glucose levels was significantly higher in the group with more favorable social status (p < 0.001). Conclusions: Social differences already influence diabetes risk and health knowledge in adolescence. The adapted FINDRISC is suitable for identifying risk groups. Schools can play a key role in prevention and promoting equal opportunities.
Keywords:
FINDRISC
; adolescents
; socioeconomic status
; nutritional knowledge
; health behavior
; type 2 diabetes
; health literacy
1. Introduction
Non-communicable diseases (NCDs) are among the leading causes of mortality and morbidity worldwide, with type 2 diabetes representing an especially rapidly growing public health challenge [1]. In recent years, a growing body of research has highlighted that risk factors for diabetes may already be present during adolescence, and that differences in health behaviors, particularly in nutrition and physical activity, can determine long-term health outcomes in adulthood [2,3].
Nutrition plays a key role in the prevention of T2DM, as confirmed by a systematic review conducted in 2025. Evidence from a study conducted across European Union member states indicates that plant-based diets, whole grains, and regular consumption of fiber-rich foods are associated with a lower risk of developing T2DM, while intake of ultra-processed foods, sugary drinks, and processed meats is linked to a higher risk [4].
Improving the quality of nutrition—particularly by increasing the consumption of whole grains—would be beneficial not only at the individual level but also from a health economic perspective, as supported by estimates from Finland [5].
The likelihood of developing diabetes is influenced not only by biological or lifestyle factors, but is also closely associated with socioeconomic status (SES) and cultural resources [6,7]. International research has consistently shown that obesity, physical inactivity, and unhealthy eating habits are more prevalent among young people with lower SES, all of which contribute to an increased risk of developing diabetes later in life [8,9].
International literature indicates that children and adolescents with lower SES generally have poorer diet quality, more unhealthy eating habits, and higher body mass index (BMI), which are closely linked to obesity and an increased risk of developing T2DM later in life [10]. A study examining dietary quality among Spanish adolescents found that poorer dietary quality is associated with lower SES and reduced physical activity, as well as other health-related factors [11].
Although numerous studies have documented the relationship between SES and unhealthy lifestyle behaviors among children and adolescents, few empirical, quantitative studies have specifically examined the relationship between SES background and risk factors for T2DM among adolescents [12]. An exception is a national study in Taiwan, which found that children and adolescents from low-income families had a significantly higher risk of developing T2DM compared to those from higher-income families [13]. Similarly, studies in Brazil have linked low SES to higher insulin resistance and unhealthy dietary patterns among adolescents, which may indirectly increase the risk of developing diabetes [14].
Available data on health behaviors of young people in Hungary indicate that social differences are reflected in lifestyle patterns and preventive health knowledge [15].
In multiple countries, questionnaire- and score-based tools are used to estimate the risk of type 2 diabetes mellitus (T2DM), as they are inexpensive, non-invasive, and suitable for screening large populations. The best-known of these tools is FINDRISC (Finnish Diabetes Risk Score) [16], which was developed by Lindström and Tuomilehto using a large adult sample in Finland to estimate the 10-year risk of T2DM. Key factors included in FINDRISC are age, body mass index (BMI), waist circumference, physical activity, vegetable and fruit consumption, history of blood pressure or blood glucose abnormalities, and family history of diabetes. This structure aligns with the approach we intended to use for assessing adolescent risk, combining lifestyle, body composition and family history.
An adapted version of the FINDRISC questionnaire allows for estimation of type 2 diabetes risk in adolescents as well [16], while taking into account lifestyle habits, body composition, and family history. [16].
FINDRISC can be conceptually applied to adolescents, as it is based on the same key risk dimensions (lifestyle, body composition, and family history). However, modification of the scoring is warranted because age—one of the strongest discriminating factors in the FINDRISC questionnaire (0 points under 25 years of age)—does not contribute to risk differentiation in adolescents. In this age group, the overall risk profile is primarily determined by factors related to body weight and health behaviors. Body composition, such as BMI and waist circumference, may warrant greater weighting, as they are most strongly associated with the emergence of early T2DM in adolescents. Previous studies highlight the importance of including family history, as hereditary and ethnic factors carry greater relative weight in juvenile T2DM compared to adult-onset T2DM [17,18,19]. Therefore, international literature has tested, rather than validated, the tool in young populations. Jordanian university students (average age: ~20 years) completed the classic FINDRISC and could be categorized into low-, medium-, and high-risk groups [20]. However, the authors noted that the sensitivity of the tool was lower in younger populations due to the age component. These findings support the conceptual approach described above, while indicating that the age scoring needs to be adjusted for adolescent use. A national survey conducted in Indonesia employed a modified FINDRISC and analyzed the younger (<35 years) age group separately. When a lower threshold was applied, the score proved to be an effective indicator of metabolic syndrome risk [21]. These findings support the notion that, by “rejuvenating” the scoring, the adult tool can be adapted for use in younger populations.
In other words, international examples do not claim the existence of an “adolescent FINDRISC,” but suggest that the underlying logic of FINDRISC can be extended to young people if age categories and thresholds are adjusted.
In Hungary, a study was conducted in 2010 that screened school-aged children and adolescents for type 2 diabetes based on risk factors (obesity, positive family history, and associated abnormalities) and identified those who required further examination [22]. The study followed the same logic as that of FINDRISC, creating a point-based risk score from easily obtainable data.
This is confirmed by screening conducted in Hungary through a network of health visitors, where adolescents at higher risk were identified in a school setting using a standardized questionnaire and anthropometry [23]. This shows that the principle of ,,adult logic applied to adolescents” is also acceptable in Hungarian practice, even if the tool is not called FINDRISC.
The aim of this study was to explore the relationships between the original and modified FINDRISC (Finnish Diabetes Risk Score) index, health behavior, and SES among Hungarian high school students aged 16-20 years. Our study fills a gap in the literature by seeking to determine the extent to which SES contributes to the risk of diabetes and health literacy among adolescents in Hungary. Our findings may contribute to understanding how social background influences health opportunities at a young age and may provide a basis for planning targeted interventions and school health promotion programs.
2. Materials and Methods
The study was conducted as a nationwide, cross-sectional, quantitative research project involving a survey of students aged 16-20 years attending Baptist secondary schools in Hungary (N = 1,585). The analyses were limited to this age group, for which 1,585 valid questionnaires were available.
Data collection was voluntary and anonymous using a paper-based, self-administered questionnaire across 16 different schools. Data were processed in aggregated and anonymous form, ensuring full protection of participant identity.
The questionnaire used in the study consisted of three main components, which measured SES, risk factors, and knowledge about diabetes.
SES status of students was characterized using multiple indicators of cultural and economic capital, including the highest level of parental education, occupation, number of books in the household, and frequency of travel abroad [24].
The FINDRISC questionnaire, a standardized tool for estimating the risk of type 2 diabetes, consists of eight items [16]. For this study, the research team modified and adapted it for use with adolescents.
Scoring was based on the following variables: body mass index (BMI), waist circumference, frequency of physical activity, consumption of vegetables and fruits, use of blood pressure medication, previously measured high blood glucose levels, and family history of diabetes. Age was not included as a risk factor as the study population was homogeneous in age. The assessment of physical activity was adapted to adolescent lifestyles, taking into account the frequency of intense physical activity lasting at least 60 minutes per day over the past week.”
Knowledge about diabetes was assessed using a 12-item questionnaire covering the pathophysiology of the disease, its main types, and fundamental knowledge of lifestyle and prevention. The questionnaire was based on the core elements of the Michigan Diabetes Knowledge Test (DKT) [25], a validated tool used in the literature to measure the knowledge about diabetes, and its Hungarian adaptation had previously been validated in the Hungarian population [26]. However, as the present study targeted a general, non-clinical population rather than individuals living with diabetes, a shortened version of the questionnaire included questions that asked about the most basic, publicly relevant information related to diabetes.
Data were processed using SPSS version 27.0, with multiple statistical procedures applied in sequence, each building on the results of the previous analysis.”
1. Descriptive statistics: SES characteristics (gender, age, place of residence, household size, parental education, and occupation) were described using descriptive statistics.
2. Cluster analysis:
TwoStep cluster analysis was used to group students by SES, incorporating variables such as parental education, occupation, number of books in the household, and frequency of travel abroad.
3. Cross-tabulation analyses: Cross-tabulation procedures were used to explore the relationships between SES, diabetes knowledge, and lifestyle factors.
4. Logistic regression: The relationship between SES and diabetes risk was examined using binary logistic regression. The dependent variable was the FINDRISC risk score, dichotomized into two categories (0 = low to moderate risk; 1 = moderate to high risk).
The research employed a quantitative, cross-sectional, questionnaire-based design to examine health knowledge and risk factors of high school students. The methodological approach allowed for the identification of subtle correlations between SES differences and health behaviors.
It provided a reliable basis for examining whether SES status was already reflected in adolescent health risk patterns and whether it played a decisive role in the acquisition of knowledge necessary for the prevention of chronic diseases.
3. Results
The sample was balanced in terms of gender (56.64% female, 43.36% male), with the majority of participants residing in urban areas. In terms of parental education, approximately one-third of the families had at least one parent with a higher education degree (father/stepfather: 35.10%; mother/stepmother: 43.20%), while a similar proportion had parents with a secondary education degree (father/stepfather: 29.60%; mother/stepmother: 33.55%). Approximately one quarter of respondents reported that their fathers or stepfathers had vocational school or vocational secondary school qualifications, whereas this proportion is notably lower for mothers or stepmothers (16.41%). The proportion of respondents whose parents had attained no more than a primary school education is below 10% for both parents (7.63% for fathers/stepfathers and 6.83% for mothers/stepmothers).
Three SES groups were identified using TwoStep cluster analysis (Table 1):
1. High-SES group (37.38%): parents with high educational attainment and greater financial and cultural capital (travel abroad, number of books).
2. Medium-SES group (19.97%): parents with average educational attainment and heterogeneous occupational and cultural background.
3. Low-SES group (42.65%): parents with lower educational attainment and limited cultural resources.
The risk of type 2 diabetes was estimated using an adapted version of the FINDRISC questionnaire. The majority of young people were in the low-risk category (70.87%), while 22.63% were classified as low risk and 6.50% were at medium or high risk.
The least favorable risk profiles were associated with physical inactivity, high blood glucose levels (16.2%), and family history of diabetes (46.8%) (Table 2).
There is a significant correlation between SES groups and categories based on FINDRISC scores (p<0.001; Cramer’s V=0.118) (Table 3).
The distributions show that respondents in the low-risk FINDRISC category are predominantly from the high-SES group (40.28%). In contrast, individuals from the low-SES group are significantly overrepresented in the high-risk category (81.82%). The medium-SES group exhibits a transitional pattern, with proportions across risk categories closely reflecting those of the total sample (Table 3).
The logistic regression model was designed to examine whether diabetes risk scores differed across social status groups. The dependent variable in the model was the FINDRISC risk, divided into two categories (0 = low to moderate, 1 = moderate to high), while the independent variable was the social status cluster (high, medium, low social status).
The results showed that the model was statistically significant (p = 0.002), although the explained variance was relatively low (R² = 0.027). Among the social clusters, individuals in the low-social-status group were significantly more likely to be classified in the medium- or high-risk group compared to the medium-status group (OR = 2.80, 95% CI = 1.35–5.81, p = 0.006).
Odds ratio in the high-status cluster group was 1.42, 95% CI = 0.65–3.13, p = 0.381).
Knowledge measurement variables
Diabetes knowledge clusters were derived from 12 items, with response options simplified to facilitate the analysis (Table 4).
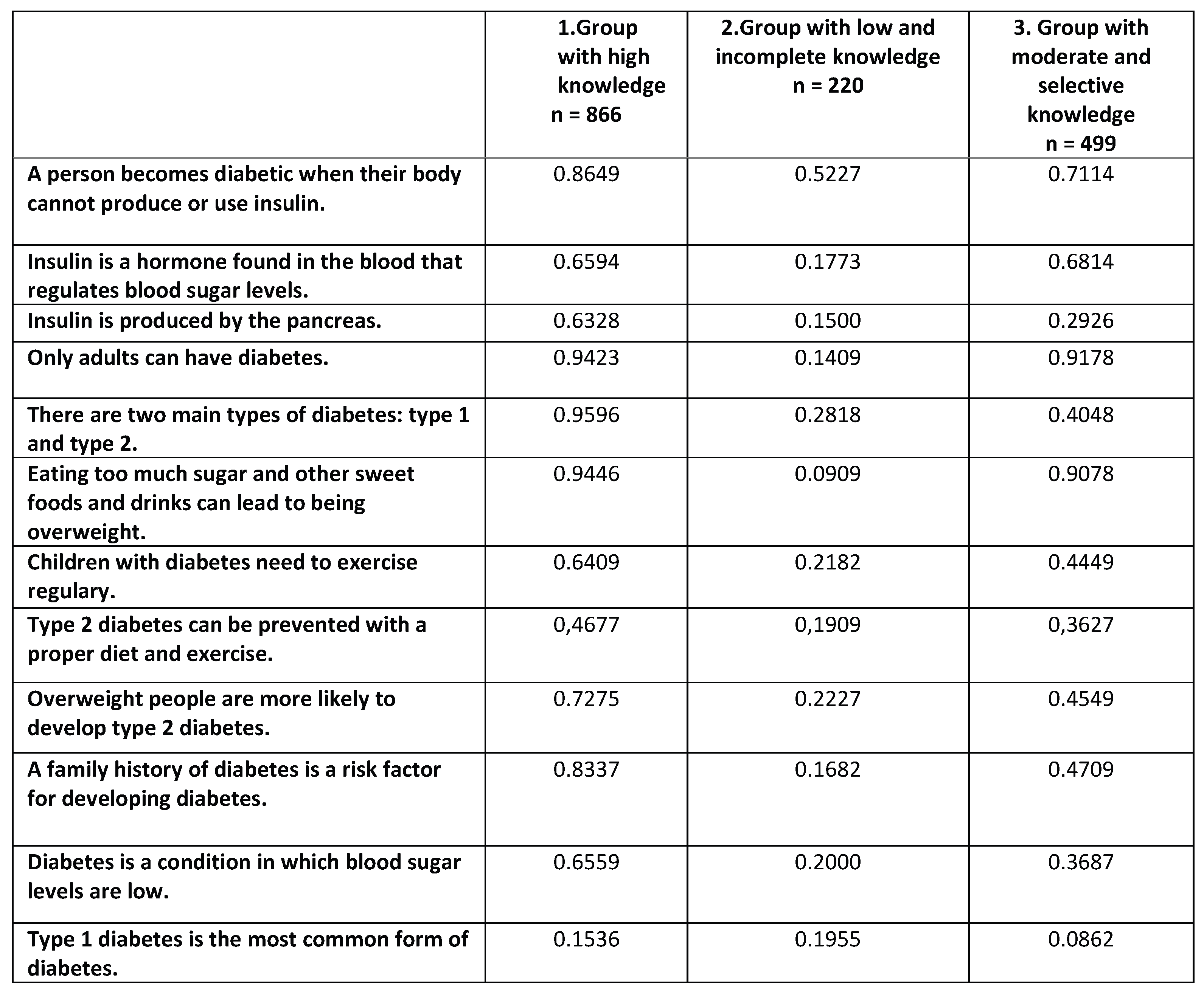
Cluster analysis was performed using 12 dichotomously coded diabetes knowledge items (0 = incorrect or “I do not know,” 1 = correct response), which identified three different knowledge profiles among respondents aged 16–20 years. The clusters were interpreted based on the average score for each item, with the averages representing the proportion of correct responses.
Cluster 1 – Group with high knowledge (n = 866)
Students in the first group responded to nearly all questions correctly at a very high rate. Students participating in the survey had a very high level of knowledge on questions concerning basic biological mechanisms. The majority correctly identified the definition of diabetes (M = 0.86), the main types of diabetes (M = 0.96), and the associations between obesity and sugar consumption (Overweight people are more likely to develop type 2 diabetes - M=0.73; Eating too much sugar and other sweet foods and drinks can lead to being overweight - M = 0.94).
They also achieved high average scores in the domains of lifestyle and prevention, including regular physical activity (M = 0.64) and awareness of family-related risk factors (M = 0.83). At the same time, some uncertainty was observed in relation to more complex or less emphasized knowledge: fewer respondents gave correct answers to questions concerning the preventability of type 2 diabetes (M = 0.47) and the prevalence of type 1 diabetes (M = 0.15).
This cluster represents a group with a high, balanced, and stable level of knowledge, with incorrect or uncertain responses mainly associated with less intuitive or more technical knowledge (Table 5).
Cluster 2 – Group with low and incomplete knowledge (n = 220)
The second group is clearly distinct from the first cluster, with consistently low percentages of correct responses across questions examined. The average number of correct responses is particularly low for basic biological concepts, such as the role of insulin (M = 0.18), its site of production (M = 0.15), and the different types of diabetes (M = 0.28).
Performance did not improve significantly for items related to lifestyle and prevention: only a small proportion of respondents correctly identified the risks associated with obesity (M = 0.22), the importance of regular physical activity (M = 0.22), and the influence of family history (M = 0.17).
The averages suggest that the response “I do not know” and incorrect responses predominate in this group, indicating a gap in foundational knowledge (Table 5).
Cluster 3 – Group with moderate and selective knowledge (n = 499)
The third group appears to function as a transitional cluster between the other two groups, characterized by a heterogeneous knowledge profile. For basic definitional items, the average number of correct responses is moderately high (e.g., definition of diabetes: M = 0.71; “only adults can have diabetes” - correct rejection of the statement M = 0.92).
However, greater uncertainty was observed for more complex or less straightforward items. In this group, only a small proportion of respondents correctly identified the site of insulin production (M = 0.29), the preventability of type 2 diabetes (M = 0.36), and the risks associated with being overweight (M = 0.46).
This group demonstrates predominantly selective knowledge: most students are familiar with basic, frequently emphasized concepts, yet substantial gaps remain in their understanding of more detailed biological and preventive factors (Table 5).
Based on the results of multinomial logistic regression, SES can be significantly correlated with diabetes knowledge group memberships (p=0.015), although the model demonstrated low explanatory power (R²=0.010).
Individuals with high SES were significantly more likely to belong to the group with high diabetes knowledge than to the group with low knowledge (OR=1.62; 95% CI: 1.03–2.57; p=0.039).
4. Discussion
Lifestyle and biological risk factors in adolescence
The primary objective of this study was to identify risk factors associated with type 2 diabetes among adolescents, with particular emphasis on lifestyle habits and health conditions that may influence disease risks at a young age.
Our results show that four-fifths of high school students aged 16–20 years were in the normal body mass index (BMI) range, while one-fifth were classified as overweight or obese according to the FINDRISC categories. The proportion of respondents consuming vegetables and fruit daily (two-thirds) can be considered favorable; however, the remaining one-third exhibited serious deficiencies. Data on physical activity are also noteworthy, as over one-third of respondents exercise less than two days per week.
Although most of the sample is currently classified as low-risk, obesity, a sedentary lifestyle, and insufficient fruit and vegetable consumption during adolescence reflect lifestyle behaviors that may increase the long-term risk of developing T2DM. These findings are consistent with international literature, which indicates that the early adoption of unhealthy lifestyles can lead to metabolic abnormalities [27,28].
Obesity and poor-quality carbohydrate intake are strongly associated with the risk of developing T2DM, which also affects younger age groups. Dietary patterns among adolescents and young adults are largely shaped by family habits and choices, which are in turn strongly influenced by socioeconomic status, underscoring the importance of considering SES in this context [29]. Indeed, diet quality, including nutrient density and sustainability, is closely associated with the socioeconomic environment, which also affects the dietary risks of adolescents. This is further supported by a study of British adolescents, which found that a suboptimal diet significantly impacts macro- and micronutrient intake, potentially contributing to the risk of metabolic diseases, including T2DM [30].
The role of socioeconomic background in FINDRISC risk
Our analysis of the FINDRISC questionnaire revealed clear social differences in diabetes risk. Members of the low-SES group were more than twice as likely as those of medium-SES to be classified into the medium- or high-risk category, whereas the odds ratio was not significant for the high-SES group. The three SES clusters exhibited clearly distinct health patterns, and the observed associations closely reflected social gradients reported in international studies [31,32]. A clear relationship emerged between socioeconomic status and FINDRISC-based risk categories: a more disadvantaged social position was associated with higher risk classification. Data presented in Table 3 further suggest that social resources (parental education, cultural background, and access to lifestyle opportunities) can serve as protective factors against diabetes risk even during adolescence. This finding is consistent with extensive research on social inequalities in adult populations, which indicates that lower SES is a major determinant of T2DM incidence [7,33].
This study also highlights that lower social status during adolescence is associated with health behaviors and characteristics that increase the long-term risk of developing T2DM.
Social disadvantages are already evident in adolescence. Consistent with previous studies, our findings show that poorer lifestyle indicators (physical activity, lower consumption of vegetables and fruit), unfavorable body composition, and a higher prevalence of high blood sugar levels were more common in the low-SES group [30].
Our results therefore suggest that social background is associated with diabetes risk even at a young age, with adolescents from lower socioeconomic groups more likely to exhibit an unfavorable risk profile according to the FINDRISC index.
Diabetes knowledge and social differences
An important finding of the study is the presence of a clear social gradient observed in the 12-item diabetes knowledge test. Students from high SES performed better across all areas. Most high-SES students correctly identified the basic mechanism of insulin function, whereas performance among low-SES students was more moderate, with nearly one-fifth selecting the option “I do not know”, reflecting significant uncertainty. Similar significant differences were observed in the recognition of conditions unrelated to diabetes, such as lung problems.
This knowledge gap aligns with existing literature on health literacy, which consistently indicates that young people from lower socioeconomic backgrounds have less access to structured health information and are more likely to rely on inaccurate, informal sources [34,35].
The greater confidence in diabetes knowledge observed among higher-SES students appears to result from both higher parental education and more favorable health behavior patterns. This is particularly important, as international evidence indicates, that knowledge about diabetes itself serves as a protective factor in early prevention and reducing engagement in risky behaviors [36].
The results indicate that socioeconomic background affects knowledge about disease, with misconceptions and gaps in understanding its basic biological processes being more common among disadvantaged students.
The applicability of FINDRISC in adolescence
FINDRISC was originally developed for adults, but several international studies have successfully adapted it for younger groups [20,21]. A similar logic has been applied in adolescent screenings in Hungary [22,23]. The results of the present study confirm that, with appropriate adjustments to age scales and threshold values, FINDRISC can effectively distinguish risk groups and reveal social inequalities among adolescents. This represents an important contribution to the Hungarian literature, as few studies have quantitatively examined the relationship between adolescent diabetes risk and social background.
The results of this study also highlight the significant role of family involvement in shaping diabetes risk profiles of adolescents. Among the risk factors assessed by FINDRISC, family history emerged as a key component, suggesting that hereditary predisposition can lead to higher risk scores even at a young age. The combined influence of genetic and lifestyle factors underscores the importance of early preventive interventions during adolescence.
Strengths and limitations
One of the main strengths of this gap-filling study is its large sample size (N = 1,585), which spans the entire country, as well as its use of socioeconomic status cluster analysis for classification. In addition, the standardized FINDRISC scoring and the knowledge assessment questionnaire allowed for complex and objective comparisons.
The primary limitation is the cross-sectional design, which prevents establishing clear causal relationships. Reliance on self-reported data may also introduce bias in reported lifestyle habits. Furthermore, as the sample was drawn from church schools, it cannot be considered representative of the entire Hungarian secondary school population. However, it is representative of a national network of church secondary schools, given the comprehensive nature of the survey.
5. Conclusions
The results of the study confirm that the FINDRISC questionnaire can be conceptually adapted for an adolescent population, provided that the age scale and risk thresholds are adjusted to reflect the characteristics of this younger group. The adapted tool was shown to be suitable for estimating diabetes risk among Hungarian high school students, while also sensitively capturing socioeconomic differences.
Our results indicate that social background is significantly associated with both diabetes risk and health literacy levels in adolescence. Unfavorable lifestyle patterns, higher FINDRISC scores, and lower levels of diabetes-related knowledge were more prevalent among students with low social status. A weak but significant correlation between social status and FINDRISC-based risk categories suggests that social resources may exert a protective effect even at a young age.
The distributions show that the proportion of adolescents in the low-risk category was highest among those with high social status, while higher risk categories were overrepresented in the low-status group. Students with medium status exhibited a profile closely aligning with the sample average. These findings are consistent with the social gradient described in the international literature on health behavior and health outcomes.
The findings highlight that health inequalities do not emerge only in adulthood but are rooted in the social and cultural environment of young people. Even moderate risks manifest earlier among adolescents with low social status, potentially contributing to unfavorable long-term health outcomes.
Our results indicate that social background is already reflected in health risk patterns during adolescence. Resources, knowledge, and lifestyle choices available to young people influence not only their current quality of life but also the trajectory of their future health outcomes.
Even moderate health risks emerge early among young adolescents with low social status, suggesting that health inequalities are not confined to adulthood but are rooted in the social and cultural environments of young people.
On the one hand, our findings suggest that adolescent health promotion can be an effective tool for reducing socially determined health inequalities. On the other hand, they help identify key points for intervention:
- Targeted school-based education for low-SES groups, with a focus on reinforcing basic metabolic concepts
- Expansion of sports and recreational opportunities, particularly in disadvantaged schools
- Practical, everyday nutrition education to compensate for limited family resources
- Identification of at-risk groups using simple, non-invasive tools (e.g., adapted version of FINDRISC)
As disadvantaged adolescents tend to have less favorable lifestyles, lower diabetes-related knowledge, and higher family risk factors, early interventions can be particularly effective in this population.
Preventive strategies should therefore target not only individual lifestyle changes but also broader efforts to reduce social inequalities. School-based health promotion, healthy lifestyle education, and targeted support for disadvantaged youth can be instrumental in preventing the early onset of chronic diseases, including diabetes, in the next generation.
Author Contributions
Concept, B.F. and H.J.F.; methodology, K.A.B.; formal analysis, B.F. and K.A.B.; investigation, B.F., H.J.F., and G.P.; data management, B.F.; writing of the original manuscript, B.F.; review and editing of the manuscript, B.F., H.J.F., P.G., A.H., and K.A.B.; supervision, H.J.F. and G.P.; project administration, H.J.F. All authors have read and approved the published version of the manuscript.
Funding
This project (No. 2023-2.1.2-KDP-2023-00016 was supported by the Ministry of Culture and Innovation of Hungary from the National Research, Development and Innovation Fund, within the framework of the KDP-2023 grant program. The sponsor had no role in study design, data collection, analysis, interpretation, manuscript preparation, or the decision to publish.
Institutional Review Board Statement
The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Scientific and Research Ethics Committee of the Health Sciences Council (ETT TUKEB) (approval number: BM/23061-3/2024, date of approval: October 15, 2024).
Informed Consent Statement
The study employed an anonymous, voluntary questionnaire. Participants provided consent by completing the questionnaire. All participants were informed about the purpose of the study and how their data would be used.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request. The data is not publicly available due to ethical reasons.
Acknowledgments
The authors are thankful to all the students, teachers and parents who participated in this study and to the management of the Hungarian Baptist Aid as the maintainer of the high schools involved in this research and to Eötvös Loránd University for permitting our questionnaires in a facilitated manner.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NCD | non-communicable chronic disease |
| T2DM | type 2 diabetes |
| SES | socioeconomic status |
| FINDRISC | diabetes risk assessment questionnaire |
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet 2024, 404, 2077–2093. [Google Scholar] [CrossRef]
- Viitasalo, A.; Lakka, T.A.; Laaksonen, D.E.; Savonen, K.; Lakka, H.M.; Hassinen, M.; Komulainen, P.; Tompuri, T.; Kurl, S.; Laukkanen, J.A.; et al. A 2-year physical activity and dietary intervention attenuate the increase in insulin resistance in a general population of children: the PANIC study. Diabetologia 2020, 63, 2270–2281. [Google Scholar] [CrossRef]
- Bel-Serrat, S.; Mouratidou, T.; Pala, V.; Huybrechts, I.; Börnhorst, C.; Fernández-Alvira, J.M.; Hadjigeorgiou, C.; Eiben, G.; Hebestreit, A.; Lissner, L.; et al. Lifestyle patterns and endocrine, metabolic, and immunological biomarkers in European adolescents: The HELENA study. Pediatr. Diabetes 2019, 20, 23–31. [Google Scholar] [CrossRef]
- Díaz-Benavides, D.A.; Muhlis, A.N.A.; Chamouni, G.; Charles, R.; Nigatu, D.T.; Ben Khadra, J.; Israel, F.E.A.; Shehab, B.; Tarek, G.L.; Sharshekeeva, A.; et al. Nutritional Determinants of Type 2 Diabetes Mellitus in the European Union: A Systematic Review. Nutrients 2025, 17, 3507. [Google Scholar] [CrossRef]
- Martikainen, J.; Jalkanen, K.; Heiskanen, J.; Lavikainen, P.; Peltonen, M.; Laatikainen, T.; Lindström, J. Type 2 Diabetes-Related Health Economic Impact Associated with Increased Whole Grains Consumption among Adults in Finland. Nutrients 2021, 13, 3583. [Google Scholar] [CrossRef]
- Agardh, E.; Allebeck, P.; Hallqvist, J.; Moradi, T.; Sidorchuk, A. Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. Int. J. Epidemiol. 2011, 40, 804–818. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, S.A.; Orr, C.J. Three Lessons About Diabetes and the Social Determinants of Health. Diabetes Care 2023, 46, 1587–1589. [Google Scholar] [CrossRef]
- Rutten, G.E.H.M.; Rauh, S.P.; Schram, M.T.; Stehouwer, C.D.A.; van der Kallen, C.J.H.; Koster, A.; Schaper, N.C.; Henry, R.M.A.; Köhler, S.; Wesselius, A.; et al. Socioeconomic position and type 2 diabetes: Examining the mediating role of social cohesion—The Maastricht Study. Diabetes Res. Clin. Pract. 2025, 219, 111925. [Google Scholar] [CrossRef]
- Lieb, D.C.; Snow, R.E.; DeBoer, M.D. Socioeconomic factors in the development of childhood obesity and diabetes. Clin. Sports Med. 2009, 28, 349–378. [Google Scholar] [CrossRef] [PubMed]
- González-Rodríguez, M.; Almazán-Catalán, J.; Redruello-Requejo, M.; Morais-Moreno, C.; Carretero-Krug, A.; Puga, A.M.; Montero-Bravo, A.; Samaniego-Vaesken, M.d.L.; Partearroyo, T.; Varela-Moreiras, G. Unhealthy and Unequal: Socioeconomic Vulnerability Shapes Dietary Quality in Children and Adolescents from Spain. Nutrients 2025, 17, 3635. [Google Scholar] [CrossRef]
- Colillas-Malet, E.; Bosque-Prous, M.; Esquius, L.; González-Casals, H.; Lafon-Guasch, A.; Fortes-Muñoz, P.; Espelt, A.; Aguilar-Martínez, A. Relationship between Diet Quality and Socioeconomic and Health-Related Factors in Adolescents by Gender. Nutrients 2024, 16, 139. [Google Scholar] [CrossRef]
- Thomas, C.; Nightingale, C.M.; Donin, A.S.; Rudnicka, A.R.; Owen, C.G.; Sattar, N.; Cook, D.G.; Whincup, P.H. Socio-Economic Position and Type 2 Diabetes Risk Factors: Patterns in UK Children of South Asian, Black African-Caribbean and White European Origin. PLoS ONE 2012, 7, e32619. [Google Scholar] [CrossRef] [PubMed]
- Yen, F.S.; Wei, J.C.C.; Liu, J.S.; Hwu, C.M.; Hsu, C.C. Parental Income Level and Risk of Developing Type 2 Diabetes in Youth. JAMA Netw. Open 2023, 6, e2345812. [Google Scholar] [CrossRef] [PubMed]
- Alves-Costa, S.; de Souza, B.F.; Rodrigues, F.A.; Ferraro, A.A.; Nascimento, G.G.; Leite, F.R.M.; Ladeira, L.L.C.; Batista, R.F.L.; Thomaz, E.B.A.F.; Alves, C.M.C.; et al. High free sugars, insulin resistance, and low socioeconomic indicators: the hubs in the complex network of non-communicable diseases in adolescents. Diabetol. Metab. Syndr. 2024, 16, 235. [Google Scholar] [CrossRef] [PubMed]
- Hajdú, T.; Kertesi, G. Social inequalities in children’s health in Hungary in the second decade of the 21st century. In Labour Market Mirror; Szabó-Morvai, Á., Pető, R., Eds.; Centre for Economic and Regional Studies, Institute of Economics, HUN-REN Hungarian Research Network (2023), 2022; pp. 45–71. [Google Scholar]
- Lindström, J.; Tuomilehto, J. The diabetes risk score: a practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, K.J.; Anderson, B.J.; Berg, E.G.; Chiang, J.L.; Chou, H.; Copeland, K.C.; Hannon, T.S.; Huang, T.T.; Lynch, J.L.; Powell, J.; et al. Youth-Onset Type 2 Diabetes Consensus Report: Current Status, Challenges, and Priorities. Diabetes Care 2016, 39, 1635–1642. [Google Scholar] [CrossRef]
- Perng, W.; Conway, R.; Mayer-Davis, E.; Dabelea, D. Youth-Onset Type 2 Diabetes: The Epidemiology of an Awakening Epidemic. Diabetes Care 2023, 46, 490–499. [Google Scholar] [CrossRef]
- Srinivasan, S.; Todd, J. The Genetics of Type 2 Diabetes in Youth: Where We Are and the Road Ahead. J. Pediatr. 2022, 247, 17–21. [Google Scholar] [CrossRef]
- Al-Shudifat, A.E.; Al-Shdaifat, A.; Al-Abdouh, A.A.; Aburoman, M.I.; Otoum, S.M.; Sweedan, A.G.; Khrais, I.; Abdel-Hafez, I.H.; Johannessen, A. Diabetes Risk Score in a Young Student Population in Jordan Using the Finnish Diabetes Risk Score (FINDRISC). Open Cardiovasc. Med. J. 2017, 11, 81–88. [Google Scholar] [CrossRef]
- Cahyaningsih, I.; Rokhman, M.R.; Sudikno; Postma, M.J.; van der Schans, J. Accuracy of the Modified Finnish Diabetes Risk Score (Modified FINDRISC) for detecting metabolic syndrome: Findings from the Indonesian national health survey. PLoS One 2025, 20, e0314824. [Google Scholar] [CrossRef]
- Barkai, L.; Madácsy, L. Kockázatalapú diabetesszűrés serdülők körében: az első hazai vizsgálat eredményei [Risk-stratified screening for diabetes in adolescents: results of the first investigation in Hungary]. Orv. Hetil. 2010, 151, 1742–1747. [Google Scholar] [CrossRef] [PubMed]
- Kiss-Tóth, E.; Lukács, A.; Csordás, Á.; Barkai, L. Serdülőkorú fiatalok 2-es típusú diabetes rizikó tényezőinek szűrése az iskolai egészségügyben dolgozó védőnők közreműködésével. [Screening of type 2 diabetes risk factors among adolescents with the involvement of school health nurses]. Védőnő 2013, 23, 33–34. [Google Scholar]
- Bourdieu, P. The forms of capital. In Handbook of Theory and Research for the Sociology of Education; Richardson, J.G., Ed.; Greenwood Press: Westport, CT, USA, 1986; pp. 241–258. [Google Scholar]
- Fitzgerald, J.T.; Funnell, M.M.; Anderson, R.M.; Nwankwo, R.; Stansfield, R.B.; Piatt, G.A. Validation of the Revised Brief Diabetes Knowledge Test (DKT2). Diabetes Educ. 2016, 42, 178–187. [Google Scholar] [CrossRef]
- Papp-Zipernovszky, O.; Klinovszky, A.; Buzás, N. Betegségismeret 2-es típusú diabetesszel élők körében: a Diabetes Knowledge Test magyar nyelvű validálása. [Disease knowledge among individuals living with type 2 diabetes: validation of the Hungarian version of the Diabetes Knowledge Test. Orv. Hetil. 2018, 159, 1965–1973. [Google Scholar] [CrossRef]
- Lakka, T.A.; Lintu, N.; Väistö, J.; Viitasalo, A.; Sallinen, T.; Haapala, E.A.; Tompuri, T.T.; Soininen, S.; Karjalainen, P.; Schnurr, T.M.; et al. A 2-year physical activity and dietary intervention attenuates the increase in insulin resistance in a general population of children: the PANIC study. Diabetologia 2020, 63, 2270–2281. [Google Scholar] [CrossRef]
- Agostinis-Sobrinho, C.; Gómez-Martínez, S.; Nova, E.; Hernandez, A.; Labayen, I.; Kafatos, A.; Gottand, F.; Molnár, D.; Ferrari, M.; Moreno, L.A.; et al. Lifestyle patterns and endocrine, metabolic, and immunological biomarkers in European adolescents: The HELENA study. Pediatr. Diabetes 2019, 20, 23–31. [Google Scholar] [CrossRef]
- Bonsembiante, L.; Targher, G.; Maffeis, C. Type 2 Diabetes and Dietary Carbohydrate Intake of Adolescents and Young Adults: What Is the Impact of Different Choices? Nutrients 2021, 13, 3344. [Google Scholar] [CrossRef]
- Ashraf, A.; Murphy, M.; Duff, R.; Adab, P.; Pallan, M. Sustainability of Diets Consumed by UK Adolescents and Associations Between Diet Sustainability and Meeting Nutritional Requirements. Nutrients 2025, 17, 2140. [Google Scholar] [CrossRef]
- Schmengler, H.; Peeters, M.; Stevens, G.W.J.M.; Kunst, A.E.; Delaruelle, K.; Dierckens, M.; Charrier, L.; Weinberg, D.; Oldehinkel, A.J.; Vollebergh, W.A.M. Socioeconomic inequalities in adolescent health behaviours across 32 different countries - The role of country-level social mobility. Soc. Sci. Med. 2022, 310, 115289. [Google Scholar] [CrossRef] [PubMed]
- Gautam, N.; Dessie, G.; Rahman, M.M.; Khanam, R. Socioeconomic status and health behavior in children and adolescents: a systematic literature review. Front. Public Health 2023, 11, 1228632. [Google Scholar] [CrossRef] [PubMed]
- Tatulashvili, S.; Fagherazzi, G.; Dow, C.; Cohen, R.; Fosse, S.; Bihan, H. Socioeconomic inequalities and type 2 diabetes complications: A systematic review. Diabetes Metab. 2020, 46, 89–99. [Google Scholar] [CrossRef]
- Fleary, S.A.; Joseph, P.; Pappagianopoulos, J.E. Adolescent health literacy and health behaviors: A systematic review. J. Adolesc. 2018, 62, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Balch-Crystal, E.; Manu, M.; Ruotsalainen, J.; Salminen, J.; Ulvinen, E.; Torppa, M. Health-literacy education drives empowerment and agency. Lancet 2023, 401, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Marciano, L.; Camerini, A.L.; Schulz, P.J. The Role of Health Literacy in Diabetes Knowledge, Self-Care, and Glycemic Control: a Meta-analysis. J. Gen. Intern. Med. 2019, 34, 1007–1017. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Standardized indicators of social status clusters (TwoStep cluster analysis) (N = 1,402).
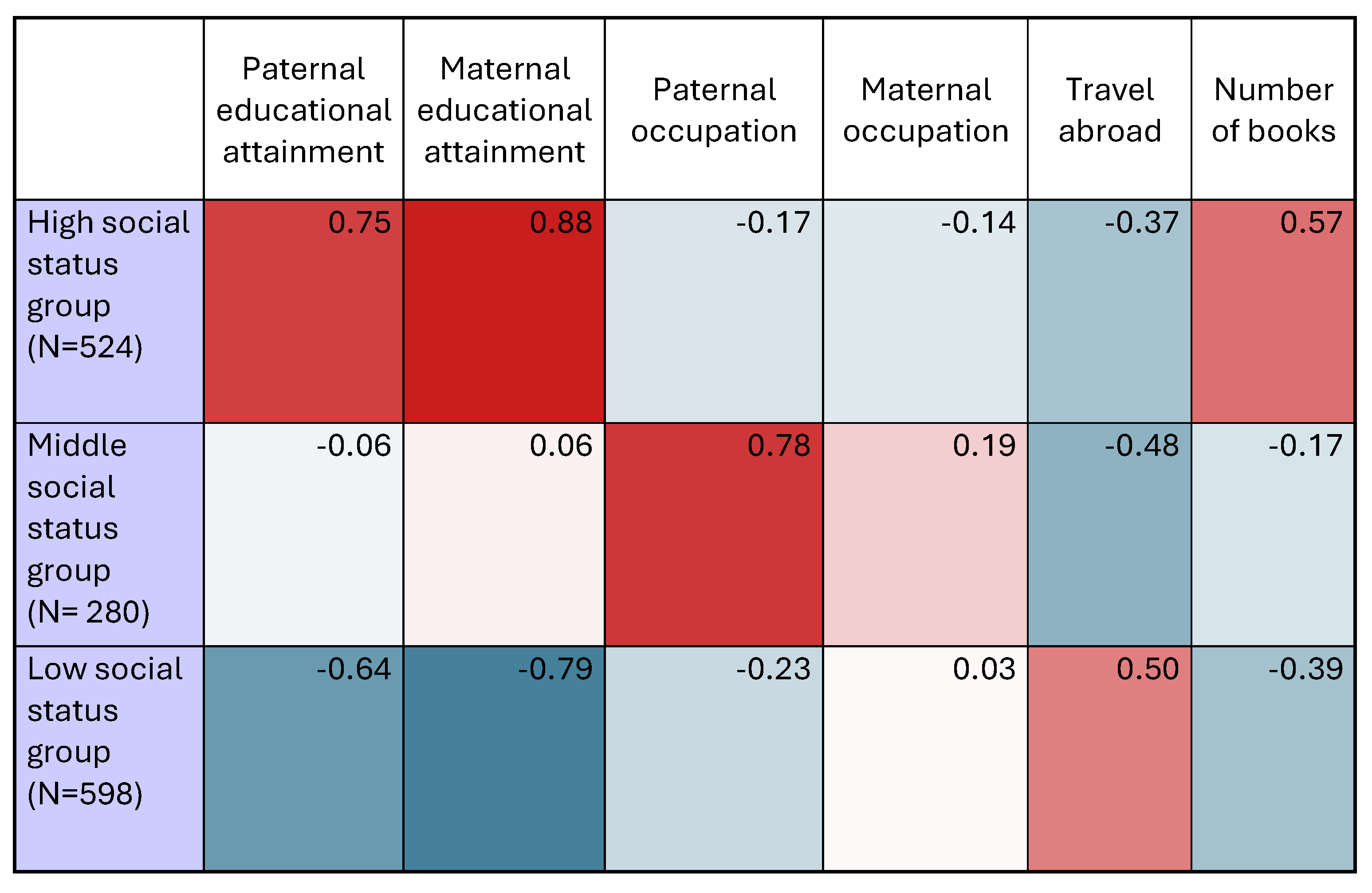 |
*blue = below average; white = sample average; red = above average.
Table 2.
Distribution of FINDRISC components among respondents aged 16-20 years (N = 1,585).
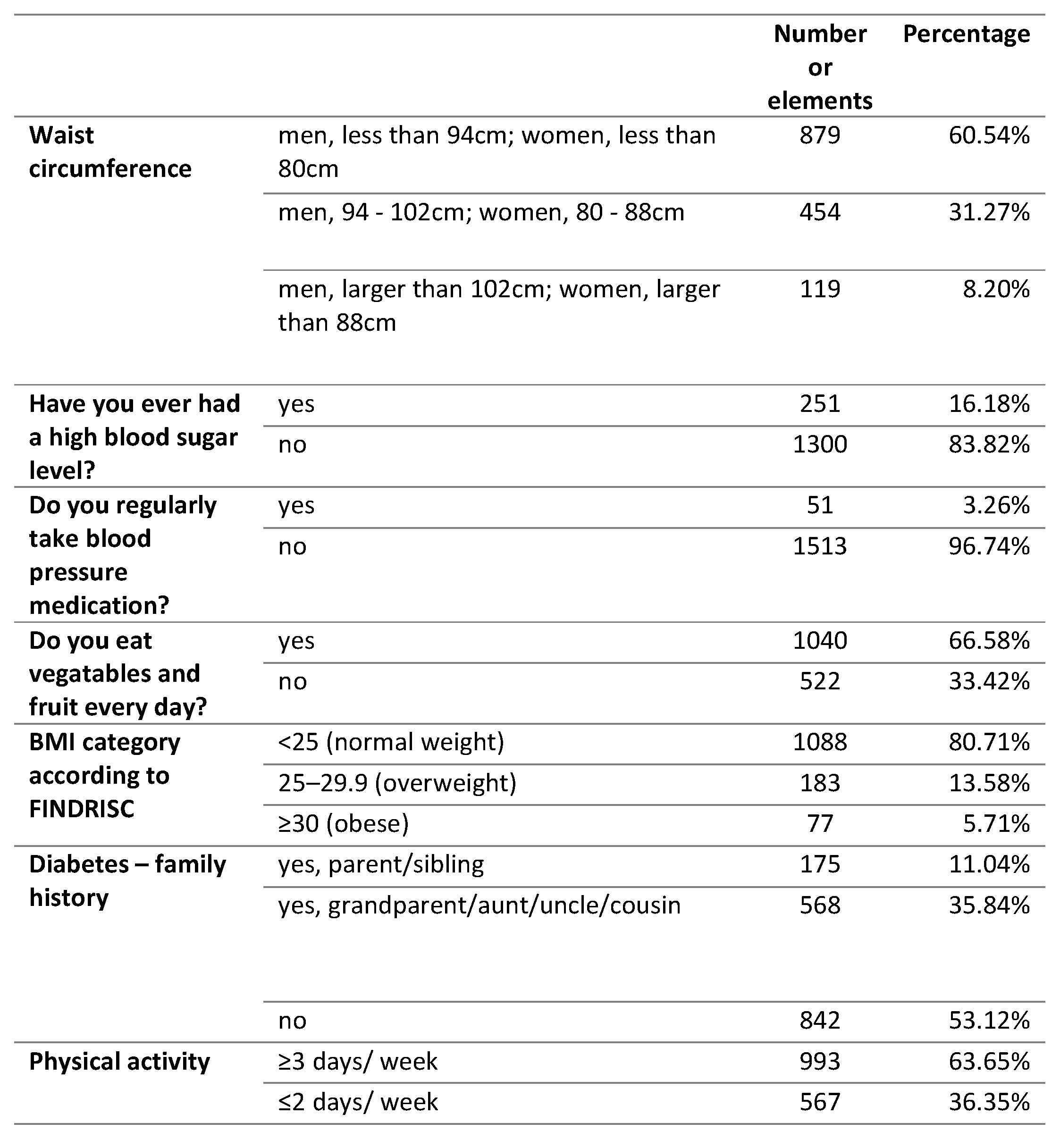 |
Table 3.
Distribution of FINDRISC risk categories by social status clusters (%).
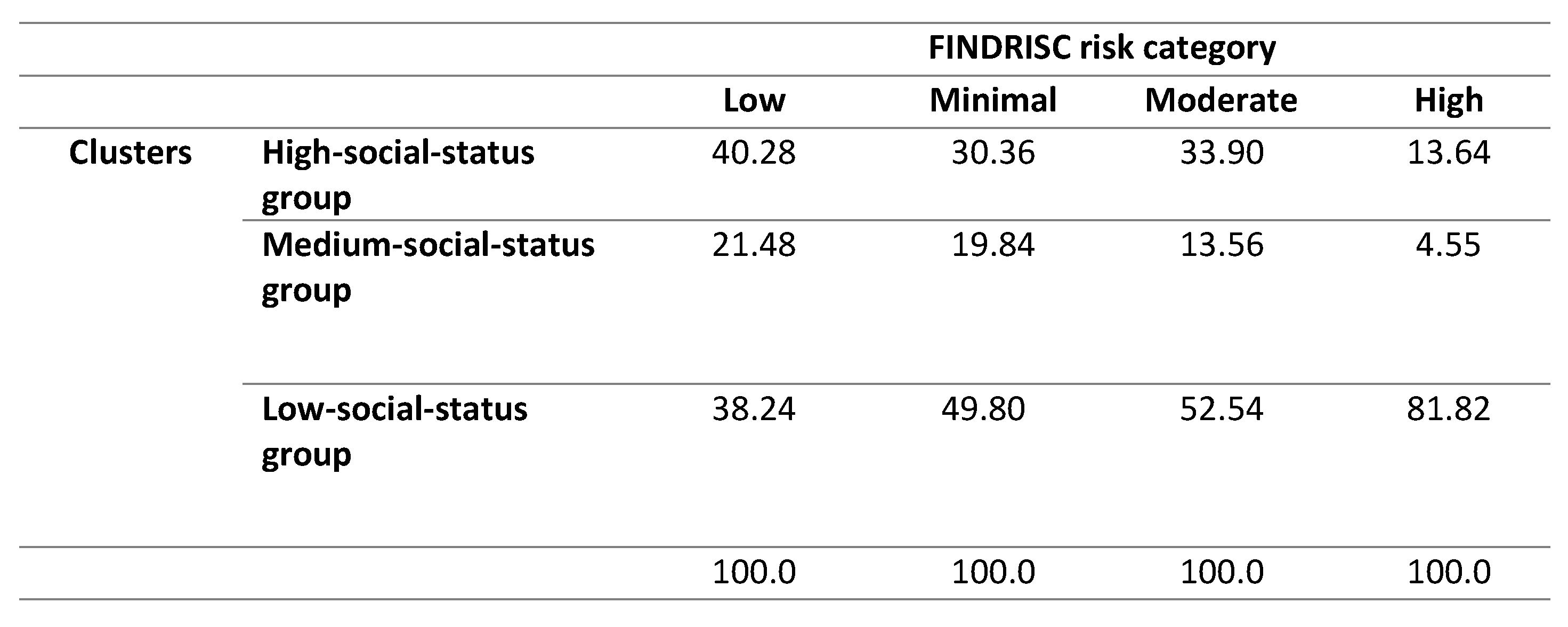 |
Table 4.
Distribution of responses to diabetes knowledge questions (N = 1,585).
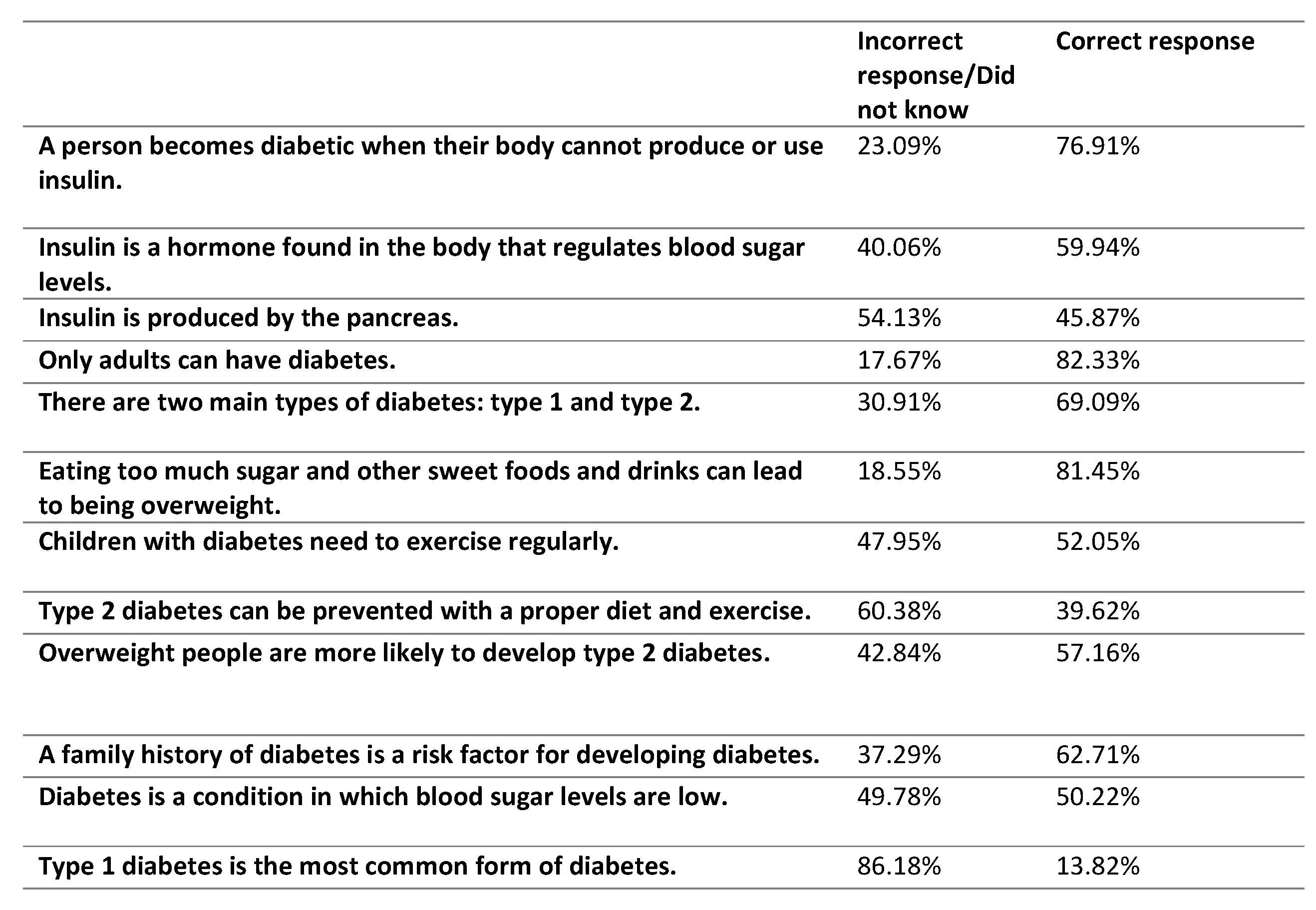 |
Table 5.
Average scores for diabetes-related knowledge items across knowledge clusters (N = 1,585).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



