
Submitted:
25 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Background/Objectives: Survival rates after pediatric liver transplantation have improved substantially over recent decades, yet the psychiatric consequences for recipients remain a concern that warrants closer attention. We sought to map the psychiatric symptom burden across multiple domains in this population and to determine which symptom clusters carry the greatest impact on health-related quality of life (HRQOL).
Materials and Methods: Fifty liver transplant recipients between the ages of 8 and 16 were enrolled at a single center. Children and their parents completed four psychiatric measures—the CBCL, CDI, SCARED, and CRIES-13—alongside the parent-proxy PedsQL to capture HRQOL across physical, emotional, social, and school functioning domains. Correlations between instruments were calculated, and linear regression was used to determine which psychiatric variables independently predicted PedsQL Total scores.
Results: Across all psychiatric measures, higher symptom scores were associated with lower HRQOL, with emotional functioning emerging as the most consistently affected domain. CBCL Total (r=−0.607), SCARED Total (r=−0.557), and CRIES-13 Total (r=−0.548) scores all correlated meaningfully with overall HRQOL. When entered into multivariable analysis, anxiety symptoms measured by the SCARED (β=−0.295, p=0.032) and post-traumatic stress symptoms measured by the CRIES-13 (β=−0.400, p=0.004) stood out as the two independent predictors of worse PedsQL Total scores.
Conclusions: Even in medically stable recipients, anxiety and post-traumatic stress continue to weigh heavily on daily functioning and overall quality of life. These findings argue for integrating routine psychosocial screening and trauma-informed approaches into standard post-transplant care.
Keywords:
pediatric liver transplantation
; quality of life
; anxiety disorders
; post-traumatic stress
; child mental health
1. Introduction
Pediatric liver transplantation (PLT) has gradually become the standard treatment for children with end-stage liver disease, biliary atresia, and certain metabolic disorders. Data from recent studies indicate that PLT achieves high rates of therapeutic success and has low risks, with 5-year patient survival rates surpassing 85–90% and 20-year survival rates nearing 80% [1,2].
The psychosocial burden of PLT, however, is still a lesser-described aspect. Children and parents endure extended hospitalizations, recurrent invasive procedures, intensive care experiences, lifelong immunosuppression, and persistent anxiety regarding rejection or complications [3,4]. These stressors correlate with increased prevalence of psychiatric symptoms relative to healthy children, including elevated levels of depression (13–31%), anxiety (31–47%), posttraumatic stress disorder (PTSD) symptoms (44–48%), and behavioral challenges [3,5,6]. Parents also report high prevalence of internalizing issues, such as anxiety, depression, and withdrawal [7].
Health-related quality of life (HRQOL) is an essential outcome domain after PLT. Recipients of PLT exhibit significantly poorer quality of life –much like children with other chronic diseases, particularly in areas of school functioning, physical health, and overall health perceptions [8]. HRQOL is negatively correlated with psychiatric symptom burden. Elevated scores in depression, anxiety, and PTSD are indicative of diminished physical, emotional, social, and academic functioning [3,9]. Clinical factors, including time elapsed since transplantation, frequency of rejection episodes, hospitalization rates, and immunosuppressive burden, further influence both psychiatric symptoms and HRQOL [10].
The majority of current studies utilize parent-report screening tools, such as the Child Behavior Checklist (CBCL) and the Strengths and Difficulties Questionnaire. While useful, these tools lack Diagnostic and Statistical Manual of Mental Disorders (DSM)–level diagnostic accuracy. The Kiddie Schedule for Affective Disorders and Schizophrenia–Present and Lifetime Version and other semi-structured diagnostic interviews have not been used much in the transplant population, even though they can make accurate clinical diagnoses [11,12]. Based on the limitations of available data, there is a need to expand studies in this field by utilizing multiple tools to better understand the psychological impact of PLT. Comprehensive analysis of post-PLT psychiatric burden necessitates determination of (i) DSM-based psychiatric diagnoses, (ii) dimensional symptom severity across various domains (depression, anxiety, PTSD, behavioral issues), (iii) child- and parent-reported HRQOL, and (iv) correlations with essential clinical parameters [13].
The current cross-sectional study including PLT recipients was designed to examine the prevalence of psychiatric disorders (via K-SADS-PL), the severity of psychiatric symptoms, HRQOL, and the relationships between these variables and multiple clinical factors (time since transplantation, rejection episodes, hospitalization history). Our purpose was to address gaps in the literature by combining diagnostic interviews, multi-domain symptom assessments, and disease-specific HRQOL measurements.
2. Materials and Methods
2.1. Ethics, Design and Setting
Ethical approval was obtained from the Scientific Research and Publication Ethics Committee of Inonu University (Approval date: 02/12/2025, decision no: 2025/8901) based on the ethical standards described in the Declaration of Helsinki. Before enrolling, all of the children and their parents (or legal guardians) had to sign a written form to provide their consent. It was clearly indicated that participation was voluntary and that participants could leave the study and request data deletion at any time. To safeguard participant confidentiality, all personal identifiers were anonymized during data collection, with analysis and reporting performed on unidentifiable data.
This study utilized a single-center, cross-sectional design to assess psychiatric symptoms, clinical diagnoses, and HRQOL in pediatric liver transplant recipients. The research was conducted at the Liver Transplantation Institute, Inonu University, in Malatya, Türkiye. Data collection took place from January 2023 to December 2023, either during regular outpatient follow-up visits or through structured online interviews when in-person attendance was impractical.
2.2. Participants
The study population was planned to include children aged 8 to 16 years who had undergone PLT and attended ongoing follow-up at the participating institution. Participants were recruited through consecutive sampling from the outpatient clinic registry. The criteria for inclusion were: (1) being between the ages of 8 and 16 at the time of the assessment; (2) having had at least one successful liver transplant and being medically stable as confirmed by the treating physician; (3) being able to communicate in Turkish or Arabic; (4) having provided written informed consent; and (5) being willing to complete the required assessments either in person or online. Exclusion criteria were: (1) severe intellectual disability (intelligence quotient < 70, as established by prior clinical records or screening); (2) substantial neurological impairment that would prevent participation in interviews or self-report measures; (3) sensory deficits preventing the completion of assessments; and (4) acute medical instability or hospitalization at the time of recruitment. Fifty children met the requirements and were included.
2.3. Interviews and Data Collection
Data were gathered via structured clinical interviews, self-report questionnaires, parent-proxy reports, and medical record reviews. All tests were administered by specialist trained research staff, such as a child psychiatrist and a clinical psychologist, in a quiet, private space to reduce stress and improve accuracy. For in-person sessions, participants were evaluated during scheduled clinic visits, while online assessments were conducted through secure video conferencing platforms that adhered to data protection regulations. The process started with an explanation of the study’s goals and methods. After recording of sociodemographic and clinical data, psychiatric and quality-of-life assessments were performed. Each session lasted about 60 to 90 minutes, with breaks as needed, especially for younger kids. To ensure consistency, the contents of the items were kept the same and scale instructions were read aloud with each party confirming accurate comprehension. Positive screening results from initial tools were further assessed via structured diagnostic approaches and all data were entered into a secure electronic database immediately after collection to reduce transcription errors.
2.4. Demographic and Clinical Information
A custom-made form for sociodemographic and medical information was used to gather important data. This included age, sex, height, weight (from which body mass index was calculated), presence of comorbidities, immigrant status, school attendance, parental ages and education levels, family history of chronic diseases, age at transplantation, time since transplantation, donor type (living or deceased), immunosuppressive regimen (either tacrolimus or everolimus), history of transplantation complications, rejection episodes in the prior year, hospitalizations in the prior year, and liver function tests (aspartate aminotransferase [AST], alanine aminotransferase [ALT], total bilirubin, and gamma-glutamyl transferase [GGT]). Data were obtained from electronic medical records and corroborated with parents during the interview.
2.5. Instruments for Psychiatric Evaluation
Psychiatric evaluations included both diagnostic interviews and scales that focused on specific properties.
The Children’s Depression Inventory (CDI) [14] was used to measure the severity of symptoms more precisely. This 27-item self-report scale questions depressive symptoms over the past two weeks and yields scores from 0 to 54 points, with higher scores meaning more severe symptoms. The cutoffs were: <15 normal, 15–19 mild, 20–24 moderate, and ≥25 severe. The Screen for Child Anxiety Related Emotional Disorders (SCARED) [15] was filled out by both the child and the parent. It had 41 items across five subscales: panic/somatic, generalized anxiety, separation anxiety, social anxiety, and school avoidance. A total score of 25 or higher indicated clinical anxiety, and there were specific thresholds for each subscale to help with interpretation. The Children’s Revised Impact of Event Scale-13 (CRIES-13) [16] assessed PTSD symptoms associated with transplant experiences, comprising 13 items categorized into intrusion, avoidance, and arousal subscales (total scores ≥17 suggesting possible PTSD). Finally, the Child Behavior Checklist (CBCL/6-18) [17], a 113-item parent-report tool, was used to measure a wide range of behavioral and emotional issues. It yielded total, internalizing, and externalizing scores, with T-scores of 65 or higher being clinically significant.
2.6. Quality of Life
The Pediatric Quality of Life Inventory (PedsQL) 4.0 Generic Core Scales [18], parent-proxy version, was used to measure HRQOL. It has 23 items that cover physical, emotional, social, and school functioning areas. The scores for each subscale range from 0 to 100, with higher scores meaning better quality of life. The total score and psychosocial health summary score are found by averaging the scores for the relevant subscales. Parents filled out the form on their own based on how they thought their child had been doing over the past month. The scales employed in this study possess were based on Turkish reliability and validity studies.
2.7. Statistical Analysis
We used IBM SPSS version 27 (IBM Corp., Armonk, NY, USA) for statistical analyses. Statistical significance was defined as two-tailed p-values below 0.05. We used histograms and Q-Q plots to see if continuous variables were normally distributed. Mean ± standard deviation was used to describe normally distributed continuous variables, median (25th percentile - 75th percentile) was used to describe non-normally distributed continuous variables, and frequency (percentage) was used for categorical variables. The Pearson or Spearman correlation coefficients were calculated as appropriate to determine effect sizes. We used linear regression analyses to identify factors that were independently linked to the PedsQL Total score. Both univariable and multivariable linear regression analyses were performed, with the latter used to identify variables that were independently associated with the examined outcome. We used the stepwise selection method to avoid multicollinearity; however, we also calculated variance inflation factor (VIF) values to ascertain multicollinearity.
3. Results
The study comprised 50 participants (22 females) who underwent PLT, with a median age of 14 years (range 11–16). Demographic and clinical characteristics including family data are summarized in Table 1. Psychiatric measures and scale results, including CBCL, CDI, SCARED subscales, CRIES-13, and PedsQL, are described in Table 2.
There were strong negative correlations between CBCL Total scores and all PedsQL domains. These included Physical Health (p=0.003, r=−0.417), Emotional Functioning (p<0.001, r=−0.778), Social Functioning (p=0.003, r=−0.406), Psychosocial Health (p<0.001, r=−0.608), and Total PedsQL scores (p<0.001, r=−0.607). Likewise, CDI scores exhibited significant negative correlations with Physical Health (p=0.009, r=−0.365), Emotional Functioning (p<0.001, r=−0.688), Social Functioning (p=0.045, r=−0.284), Psychosocial Health (p=0.001, r=−0.467), and Total PedsQL scores (p=0.001, r=−0.446). The SCARED subscale and total scores exhibited a significant negative correlation with various PedsQL domains. Panic and somatic symptoms were linked to lower scores on the Emotional Functioning (p<0.001, r=−0.678), Psychosocial Health (p=0.005, r=−0.390), and Total PedsQL (p=0.004, r=−0.397) scales. Generalized Anxiety exhibited significant negative correlations with Emotional Functioning (p<0.001, r=−0.757), Psychosocial Health (p<0.001, r=−0.539), and Total scores (p=0.001, r=−0.439). Separation Anxiety exhibited a negative correlation with Emotional Functioning (p<0.001, r=−0.514), Psychosocial Health (p=0.008, r=−0.370), and Total PedsQL scores (p=0.025, r=−0.318). Social Anxiety correlated with diminished Physical Health (p<0.001, r=−0.511), Emotional Functioning (p<0.001, r=−0.516), Social Functioning (p=0.032, r=−0.304), Psychosocial Health (p<0.001, r=−0.480), and Total scores (p<0.001, r=−0.582). School Avoidance had a strong link to Physical Health (p=0.025, r=−0.373), Emotional Functioning (p<0.001, r=−0.595), Psychosocial Health (p=0.013, r=−0.409), and Total PedsQL scores (p=0.005, r=−0.457). The overall SCARED Total scores exhibited substantial negative correlations with Physical Health (p=0.004, r=−0.403), Emotional Functioning (p<0.001, r=−0.745), Social Functioning (p=0.028, r=−0.312), Psychosocial Health (p<0.001, r=−0.510), and Total scores (p<0.001, r=−0.557) (Figure 1). Post-traumatic stress symptoms evaluated by CRIES-13 exhibited significant negative correlations with multiple PedsQL domains. Intrusion scores were significantly correlated with diminished Emotional Functioning (p<0.001, r=−0.642), Social Functioning (p=0.023, r=−0.320), Psychosocial Health (p<0.001, r=−0.522), and Total PedsQL scores (p=0.004, r=−0.400). There was a negative correlation between avoidance scores and Emotional Functioning (p<0.001, r=−0.436), Social Functioning (p=0.007, r=−0.376), Psychosocial Health (p=0.001, r=−0.470), and Total scores (p=0.004, r=−0.396). Arousal exhibited significant negative correlations with Physical Health (p=0.002, r=−0.434), Emotional Functioning (p<0.001, r=−0.665), Psychosocial Health (p<0.001, r=−0.544), and Total PedsQL scores (p<0.001, r=−0.575). In the same way, CRIES-13 Total scores were significantly negatively correlated with Physical Health (p=0.017, r=−0.336), Emotional Functioning (p<0.001, r=−0.676), Social Functioning (p=0.016, r=−0.340), Psychosocial Health (p<0.001, r=−0.605), and Total PedsQL scores (p<0.001, r=−0.548) (Figure 2) (Table 3).
The results of multivariable linear regression analysis showed that a high SCARED Total score (b: -0.431, 95% CI: -0.824 - -0.038, p=0.032) and a high CRIES-13 Total score (b: -0.471, 95% CI: -0.787 - -0.154, p=0.004) were both linked to lower PedsQL Total scores. The VIF was determined to be 1.321, indicating the absence of multicollinearity in the final model (Table 4).
4. Discussion
The present study comprehensively evaluated the psychiatric symptoms experienced by PLT recipients, including emotional and behavioral challenges, anxiety, depression, and post-traumatic stress, which are negatively correlated with multiple aspects of HRQOL. Multiple correlations were found between examined parameters, with findings showing that behavioral issues were associated with diminished physical health, emotional functioning, social functioning, and overall psychosocial state. Depressive symptoms were linked to worse physical and mental health, while anxiety subscales, especially social and separation anxiety, were linked to worse emotional and psychosocial outcomes. PTSD characteristics, including intrusion, avoidance, and arousal, showed consistent negative correlations with emotional, social, and overall quality of life scores.
PLT is associated with increased rates of psychiatric symptoms and poorer HRQOL, and this inverse relationship is corroborated by the negative correlations between behavioral issues and various quality of life domains [3,6]. For example, Ünay and colleagues found in 50 PLT recipients that 30% to 60% had psychiatric diagnoses. Anxiety and depression symptoms were negatively correlated with PedsQL especially in the emotional and social functioning domains [3]. In a similar vein, Huang et al.’s propensity score-matched analysis of 741 children following living donor liver transplantation revealed heightened emotional issues and hyperactivity, which were associated with diminished psychosocial health, as assessed by the Strengths and Difficulties Questionnaire [6]. In our cohort, the total scores from the CBCL showed strong negative links to physical health (r = -0.417), emotional functioning (r = -0.778), and overall quality of life (r = -0.607), demonstrating that findings in this regard are confirmed by multiple studies.
Chronic immunosuppression may exert neurotoxic effects that disrupt neurotransmitter pathways, including serotonin and dopamine, which are fundamental to mood regulation and behavioral control [9]. Furthermore, pre-PLT nutritional deficiencies and the duration of the disease may impact neurodevelopment in children, leading to cognitive and emotional disruption [19]. Our results show that such impacts remain relevant in a cohort comprised of patients who had undergone successful PLT, suggesting that psychiatric symptoms diminish quality of life even after successful treatment. It appears that the CBCL may be useful to identify at-risk children, thereby potentially alleviating long-term psychosocial deterioration.
We incorporated DSM-based diagnostic interviews to allow accurate identification of clinical disorders [20]. This comprehensive evaluation indicates that internalizing issues, such as withdrawal and somatic complaints, are especially pronounced in PLT recipients. It can be hypothesized that these outcomes are associated with the cumulative burden of lifelong medical management, including recurrent hospitalizations and immunosuppression. These stressors may activate the hypothalamic-pituitary-adrenal axis, resulting in dysregulation of cortisol levels that sustain emotional dysregulation and behavioral problems [3,7,21]. Our findings indicate elevated rates of emotional issues among younger recipients, suggesting that an earlier transplant age exacerbates these risks. By quantifying these associations in adolescents, it may be possible to design interventions for domain-specific burdens, such as diminished academic performance that has been described in the long term among PLT recipients [22]. Indeed, cognitive-behavioral therapy and family support have been recommended to alleviate adverse psychiatric outcomes [23].
Anxiety and PTSD were identified as significantly harmful to emotional and psychosocial well-being in our sample, with various subscales demonstrating strong negative correlations with HRQOL domains, corroborating prior evidence [24]. Düken and Yayan identified elevated anxiety and post-traumatic stress in young PLT recipients and showed that they correlated with diminished HRQOL, as measured by the PedsQL [5]. Similarly, a single-center study involving 62 PLT recipients found that 9.67% had attention-deficit/hyperactivity disorder through clinical examination, with comorbid anxiety associated with inferior neurocognitive outcomes [7]. Our findings from the SCARED subscales and the total score from the CRIES-13 reveal the influence of anxiety on daily functioning –which are validated by studies involving children with medically-induced trauma (such as intensive care experience) [16].
Social isolation during recovery, as reported in a study of 84 adult survivors of PLT, increases the risk and extent of adverse outcomes. It was found that 26% of these patients experienced mental health disorders associated with early transplant age [23]. We find that anxiety impacts not only emotional functioning but also social integration. In a prospective cohort study conducted by Mohammad et al., the cessation of immunosuppression was linked to enhancements in disease-specific HRQOL. Notably, this improvement was mitigated in patients with persistence of anxiety symptoms [9]. In comparison, the elevated separation anxiety scores in our cohort may indicate the distinct stressors associated with parental dependency in younger transplant recipients. Indeed, Marshall and colleagues showed in adolescents that age at transplantation affected anxiety levels and HRQOL [25]. By integrating the SCARED score in our study [26], we demonstrate that somatic and panic symptoms further diminish physical health [9]. It is also important to note that cultural factors such as family-centric caregiving may increase separation anxiety, as suggested in adolescents [4], which is a crucial factor to consider with regard to the cultural family-centric characteristic of Turkish society. It may be feasible to recommend personalized treatments for such trauma, especially in the presence of comorbidities [7].
Depression and its correlation with impaired physical and emotional health in our cohort appear to be similar to those observed in chronic illness, where mood disorders and family dynamics can impact medical compliance. Among Turkish PLT recipients, depressive symptoms appear to persist even three years post-transplantation and our findings do not question this extensive impact [5]. These long-term influences are also observed in other populations, with younger age at transplantation increasing depressive symptoms later in life, as well as adversely affecting PedsQL domains such as appearance and social functioning [25]. Our findings, which indicate a negative correlation between depressive symptoms and physical and emotional health, are consistent with these observations. Notably, immunosuppressive agents can interfere with serotonin signaling and increase neuroinflammatory processes associated with depression [9]. Furthermore, parental mental health burdens can also cause increased risks for child depression [20]. In our sample, this is demonstrated by the correlations between depressive scores and family environment factors. Indeed, Huang et al. have shown that parental well-being is a predictor of child emotional health [6]. Our comprehensive evaluation reveals that depression disrupts both emotional and physical health, adding to prior research examining treatment non-adherent individuals [27]. We also show that even stable PLT recipients who adhere to treatments encounter these risks, which may appear to be in conflict to studies examining more acute states [19].
4.1. Limitations
The cross-sectional design inherently precludes causal inferences, as the examinations were performed at a single point in time without clarifying whether psychiatric issues precede or result from transplant experiences. The sample size of 50 participants from a single Turkish center is small, but similar to most literature in the field. However, since patient selection was based on attending follow-up, there is an apparent selection bias towards more compliant or medically-stable families / children. Using self-report and parent-proxy tools, like the PedsQL Inventory, can lead to systematic biases. For example, adolescents might downplay their symptoms to avoid stigma, or parents might inflate experiences due to concerns. These are well-known factors that apply to most transplant literature [8]. Unexamined confounders, including medication adherence, socioeconomic status, or family functioning may mediate the observed correlations but were excluded due to limitations of retrospective data. Moreover, all patients had stable graft function (0% recent rejections) which indicates that present results may not apply to high-risk cases or patients with worse condition [9]; however, this is also an advantage since the relationships established in this study indicate that even stable PLT patients experience great psychiatric burdens.
5. Conclusions
This study revealed the continuous psychiatric challenges faced by PLT recipients, with behavioral, depressive, anxiety, and post-traumatic symptoms associated with worse HRQOL, particularly in the physical, emotional, and social domains. Psychosocial screening accounting for personal and family characteristics appears to be essential in designing and planning post-transplant care. We also believe that utilizing instruments such as the CBCL and the SCARED may enable early detection and thus intervention. By addressing modifiable factors such as parental support and trauma processing, it may possible to increase resilience and improve HRQOL for these children.
Author Contributions
Conceptualization, A.B. and D.Y.B.; methodology, A.B., D.Y.B. and S.S.; validation, A.B., D.Y.B. and S.Y.; formal analysis, A.B. and I.T.; investigation, S.S., I.T. and D.Y.B.; resources, A.B. and D.Y.B.; data curation, S.S., I.T. and A.B.; writing—original draft preparation, A.B. and S.S.; writing—review and editing, A.B., D.Y.B. and S.Y.; visualization, A.B. and I.T.; supervision, S.Y. and A.B.; funding acquisition, D.Y.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval was obtained from the Scientific Research and Publication Ethics Committee of Inonu University (Approval date: 02/12/2025, decision no: 2025/8901) based on the ethical standards described in the Declaration of Helsinki.
Informed Consent Statement
Before enrolling, all of the children and their parents (or legal guardians) had to sign a written form to provide their consent. It was clearly indicated that participation was voluntary and that participants could leave the study and request data deletion at any time. To safeguard participant confidentiality, all personal identifiers were anonymized during data collection, with analysis and reporting performed on unidentifiable data.
Data Availability
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| CBCL | Child Behavior Checklist |
| CDI | Children’s Depression Inventory |
| SCARED | Screen for Child Anxiety Related Disorders |
| CRIES-13 | Screen |
| SCA | Children’s Revised Impact of Events Scale-13 |
| PedsQL | Pediatric Quality of Life Inventory |
| HRQOL | health-related quality of life |
| PLT | Pediatric liver transplantation |
| DSM | Diagnostic and Statistical Manual of Mental Disorders |
| AST | aspartate aminotransferase |
| ALT | alanine aminotransferase |
| GGT | gamma-glutamyl transferase |
References
- Kwong, A.J.; Ebel, N.H.; Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Schnellinger, E.M.; Handarova, D.; Weiss, S.; Cafarella, M. OPTN/SRTR 2021 annual data report: liver. Am. J. Transplant. 2023, 23, S178–S263. [Google Scholar] [CrossRef]
- Goss, J.A.; Shackleton, C.R.; Mcdiarmid, S.V.; Maggard, M.; Swenson, K.; Seu, P.; Vargas, J.; Martin, M.; Ament, M.; Brill, J. Long-term results of pediatric liver transplantation: an analysis of 569 transplants. Ann. Surg. 1998, 228, 411–420. [Google Scholar] [CrossRef]
- Ünay, M.; Önder, A.; Gizli Çoban, Ö.; Atalay, A.; Sürer Adanir, A.; Artan, R.; Özatalay, E. Psychopathology, quality of life, and related factors in pediatric liver transplantation candidates and recipients. Pediatr. Transplant. 2020, 24, e13633. [Google Scholar] [CrossRef]
- Taylor, R.; Franck, L.; Gibson, F.; Donaldson, N.; Dhawan, A. Study of the factors affecting health-related quality of life in adolescents after liver transplantation. Am. J. Transplant. 2009, 9, 1179–1188. [Google Scholar] [CrossRef]
- Düken, M.E.; Yayan, E.H. Psychosocial conditions of children after liver transplant: Post-traumatic stress, depression, and anxiety. J. Pediatr. Nurs. 2024, 75, e75–e80. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Hou, Y.; Li, W.; Wang, G.; Gu, G.; Xia, Q. Mental health in children with living donor liver transplantation: A propensity score-matched analysis. Child Adolesc. Psychiatry Ment. Health 2022, 16, 94. [Google Scholar] [CrossRef]
- Taş, B.Y.; Özbaran, B. Psychiatric comorbidities in pediatric organ transplantation: Current findings and clinical approaches. Eur. Transplant. Res. 2025, 1, 25–33. [Google Scholar]
- Parmar, A.; Vandriel, S.M.; Ng, V.L. Health-related quality of life after pediatric liver transplantation: a systematic review. Liver Transpl. 2017, 23, 361–374. [Google Scholar] [CrossRef]
- Mohammad, S.; Sundaram, S.S.; Mason, K.; Lobritto, S.; Martinez, M.; Turmelle, Y.P.; Bucuvalas, J.; Feng, S.; Alonso, E.M. Improvements in disease-specific health-related quality of life of pediatric liver transplant recipients during immunosuppression withdrawal. Liver Transpl. 2021, 27, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Hager, A.; Mager, D.; Robert, C.; Nicholas, D.; Gilmour, S. Health-related quality of life 10 years after liver transplantation: a longitudinal retrospective review. Diagnostics 2021, 11, 111. [Google Scholar] [CrossRef] [PubMed]
- Gritti, A.; Sicca, F.; Di Sarno, A.M.; Di Cosmo, N.; Vajro, S.; Vajro, P. Emotional and behavioral problems after pediatric liver transplantation: A quantitative assessment. Pediatr. Transplant. 2006, 10, 205–209. [Google Scholar] [CrossRef]
- Marangoz, Y.; Özçay, F.; Haberal, M. Association of Liver Transplant and Attention-Deficit Hyperactivity Disorder: A Single-Center Experience. Exp. Clin. Transplant. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Uçgun, T.; Koyuncu, İ.E.; Koç, E.; Kılınç, B.Ş.; Sarıdağ, K.N.K. Identification of Psychosocial Issues in Pediatric Patients Undergoing or Waiting for Organ Transplant: A Systematic Review. Exp. Clin. Transplant. 2024, 22, 132–138. [Google Scholar] [CrossRef]
- Kovacs, M. Children’s Depression Inventory (CDI and CDI 2); John Wiley & Sons, 2014. [Google Scholar]
- Monga, S.; Birmaher, B.; Chiappetta, L.; Brent, D.; Kaufman, J.; Bridge, J.; Cully, M. Screen for child anxiety-related emotional disorders (SCARED): Convergent and divergent validity. Depress. Anxiety 2000, 12, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Perrin, S.; Meiser-Stedman, R.; Smith, P. The Children’s Revised Impact of Event Scale (CRIES): Validity as a screening instrument for PTSD. Behav. Cogn. Psychother. 2005, 33, 487–498. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L. Child behavior checklist for ages 6-18; University of Vermont: Burlington, VT, 2001. [Google Scholar]
- Desai, A.D.; Zhou, C.; Stanford, S.; Haaland, W.; Varni, J.W.; Mangione-Smith, R.M. Validity and responsiveness of the pediatric quality of life inventory (PedsQL) 4.0 generic core scales in the pediatric inpatient setting. JAMA Pediatr. 2014, 168, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, L.G.; Neighbors, K.; Martz, K.; Zelko, F.; Bucuvalas, J.; Alonso, E.M. Cognitive and academic outcomes after pediatric liver transplantation: Functional Outcomes Group (FOG) results. Am. J. Transplant. 2011, 11, 303–311. [Google Scholar] [CrossRef]
- Cousino, M.K.; Hazen, R.A. Parenting stress among caregivers of children with chronic illness: a systematic review. J. Pediatr. Psychol. 2013, 38, 809–828. [Google Scholar] [CrossRef]
- Yalcinkaya, A.; Yalcinkaya, R.; Sardh, F.; Landegren, N. Immune dynamics throughout life in relation to sex hormones and perspectives gained from gender-affirming hormone therapy. Front. Immunol. 2025, 15, 1501364. [Google Scholar] [CrossRef]
- Ng, V.L.; Alonso, E.M.; Bucuvalas, J.C.; Cohen, G.; Limbers, C.A.; Varni, J.W.; Mazariegos, G.; Magee, J.; Mcdiarmid, S.V.; Anand, R. Health status of children alive 10 years after pediatric liver transplantation performed in the US and Canada: report of the studies of pediatric liver transplantation experience. J. Pediatr. 2012, 160, 820–826.e823. [Google Scholar] [CrossRef]
- Vimalesvaran, S.; Souza, L.N.; Deheragoda, M.; Samyn, M.; Day, J.; Verma, A.; Vilca-Melendez, H.; Rela, M.; Heaton, N.; Dhawan, A. Outcomes of adults who received liver transplant as young children. EClinicalMedicine 2021, 38, 100987. [Google Scholar] [CrossRef] [PubMed]
- Ala, S.; Ramos-Campos, F.; Relva, I.C. Symptoms of post-traumatic stress and mental health in a sample of university students: The mediating role of resilience and psychological well-being. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 2262–2281. [Google Scholar] [CrossRef]
- Marshall, A.F.; Mandac, C.; Qin, F.; Boothroyd, D.; Nasr, A.S. Effect of Age at Liver Transplant on Anxiety, Depression, and Quality of Life Among Adolescents. Prog. Transplant. 2024, 34, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Brent, D.A.; Chiappetta, L.; Bridge, J.; Monga, S.; Baugher, M. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Fredericks, E.M.; Magee, J.C.; Opipari-Arrigan, L.; Shieck, V.; Well, A.; Lopez, M.J. Adherence and health-related quality of life in adolescent liver transplant recipients. Pediatr. Transplant. 2008, 12, 289–299. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Scatter plot of Pediatric Quality of Life Inventory Total score and Screen for Child Anxiety Related Disorders Total score.
Figure 1.
Scatter plot of Pediatric Quality of Life Inventory Total score and Screen for Child Anxiety Related Disorders Total score.
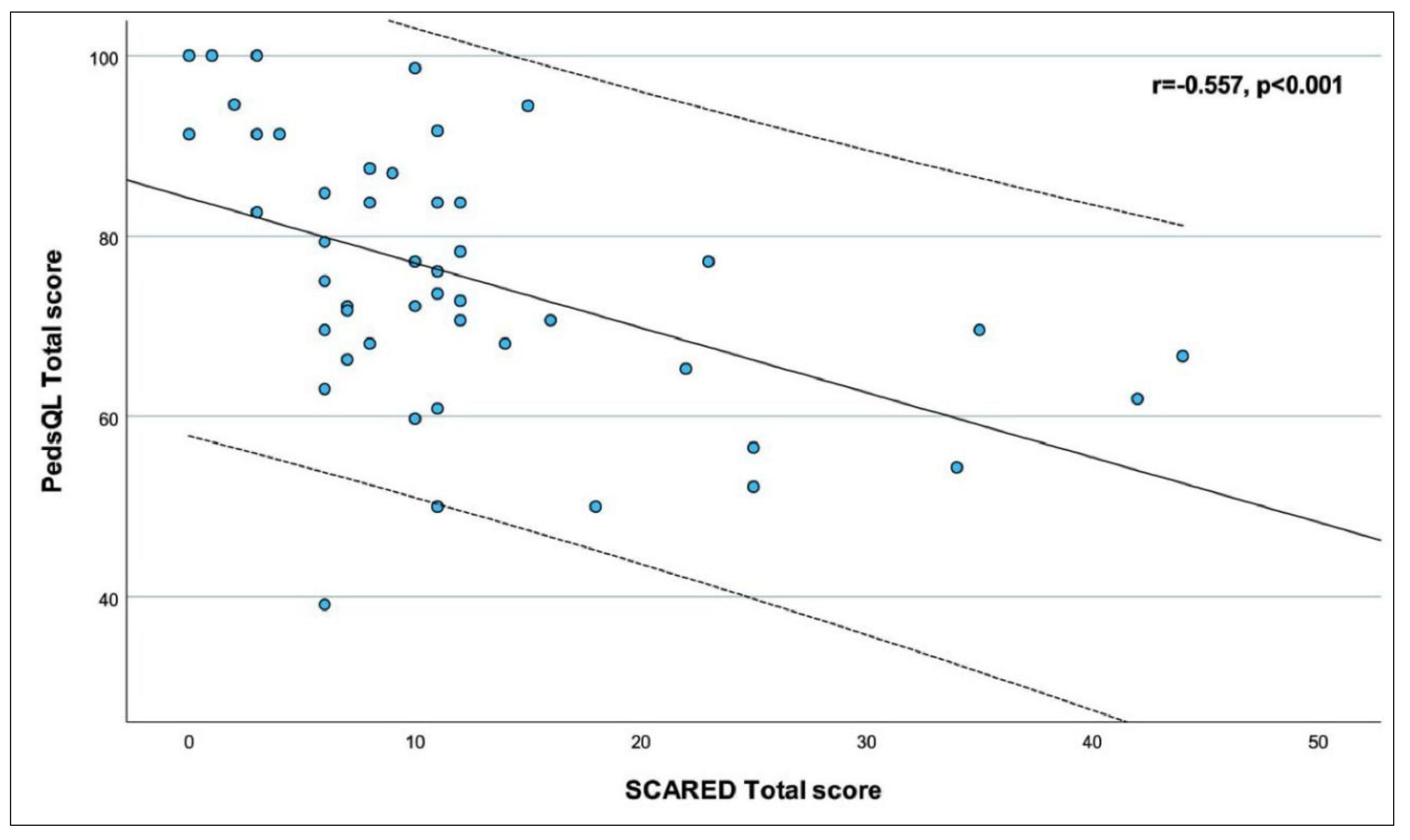
Figure 2.
Scatter plot of Pediatric Quality of Life Inventory Total score and Children’s Revised Impact of Events Scale 13-item Total score.
Figure 2.
Scatter plot of Pediatric Quality of Life Inventory Total score and Children’s Revised Impact of Events Scale 13-item Total score.
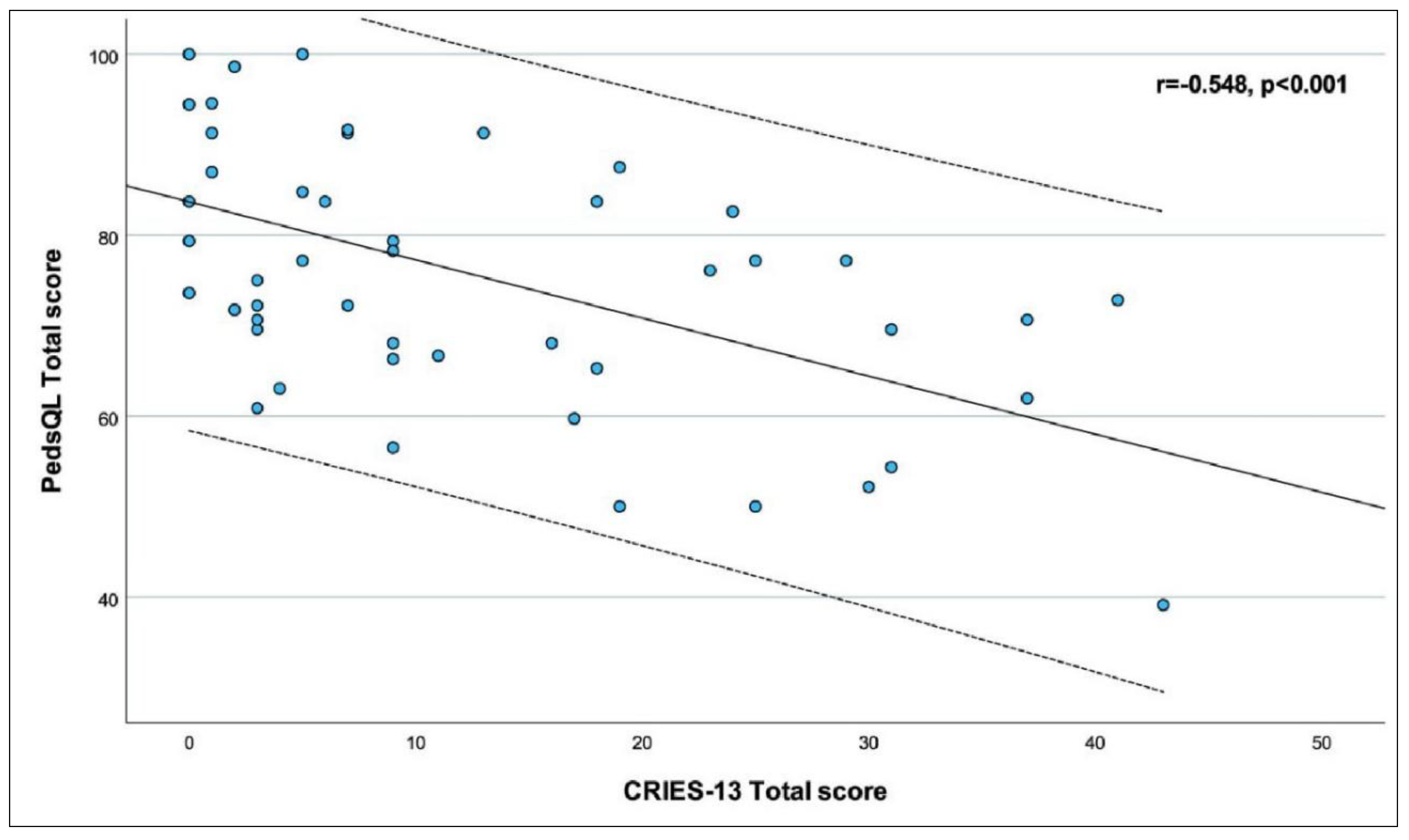

Table 1.
Demographic and Clinical Characteristics of the Study Population.
| Age of child, years | 14 (11 - 16) |
|---|---|
| Sex | |
| Male | 28 (56.0%) |
| Female | 22 (44.0%) |
| Height, cm | 155.5 (135 - 165) |
| Weight, kg | 45.10 ± 15.94 |
| Body mass index, kg/m2 | 19.38 ± 4.16 |
| Comorbidity | 2 (4.0%) |
| Immigrant | 7 (14.0%) |
| Going to school | 36 (72.0%) |
| Age of mother, years | 38.10 ± 5.98 |
| Education status of mother | |
| Literate | 17 (34.0%) |
| Primary school | 17 (34.0%) |
| Secondary school | 7 (14.0%) |
| High school | 5 (10.0%) |
| Associate degree | 3 (6.0%) |
| Bachelor degree | 1 (2.0%) |
| Age of father, years | 42.08 ± 6.03 |
| Education status of father | |
| Literate | 8 (16.0%) |
| Primary school | 13 (26.0%) |
| Secondary school | 17 (34.0%) |
| High school | 8 (16.0%) |
| Associate degree | 1 (2.0%) |
| Bachelor degree | 3 (6.0%) |
| Chronic disease in family | 10 (20.0%) |
| Age at transplantation, years | 5 (2 - 11) |
| Time since transplantation, years | 7.44 (2.25 - 11.67) |
| Type of donor | |
| Living | 44 (88.0%) |
| Deceased | 6 (12.0%) |
| Immunosuppressive drug | |
| Tacrolimus | 43 (86.0%) |
| Everolimus | 7 (14.0%) |
| Transplantation complication | 0 (0.0%) |
| Rejection attack, last year | 0 (0.0%) |
| Hospitalization, last year | 2 (4.0%) |
| AST, U/L | 32 (25 - 58) |
| ALT, U/L | 27 (16 - 71) |
| Total bilirubin, mg/dL | 0.60 (0.42 - 0.88) |
| GGT, U/L | 27.5 (17 - 93) |
Descriptive statistics are presented using mean ± standard deviation for normally distributed continuous variables, median (25th percentile - 75th percentile) for non-normally distributed continuous variables and frequency (percentage) for categorical variables. Abbreviations: ALT: Alanine aminotransferase, AST: Aspartate aminotransferase, GGT: Gamma-glutamyl transferaseDescriptive statistics are presented using mean ± standard deviation for normally distributed continuous variables, median (25th percentile - 75th percentile) for non-normally distributed continuous variables and frequency (percentage) for categorical variables. Abbreviations: ALT: Alanine aminotransferase, AST: Aspartate aminotransferase, GGT: Gamma-glutamyl transferase.
Table 2.
Psychological Assessment and Quality of Life Outcomes.
| Psychiatric follow-up | 1 (2.0%) |
|---|---|
| Psychiatric diagnosis | 0 (0.0%) |
| Type of interview | |
| Face to face | 30 (60.0%) |
| Online | 20 (40.0%) |
| CBCL Total score | 43.5 (36 - 57) |
| CDI score | 8.14 ± 5.47 |
| Normal (<15) | 42 (84.0%) |
| Mild depression (15-19) | 6 (12.0%) |
| Moderate depression (20-24) | 2 (4.0%) |
| Severe depression (≥25) | 0 (0.0%) |
| SCARED score | |
| Panic/Somatic | 1 (0 - 2) |
| ≥7 | 4 (8.0%) |
| Generalized Anxiety | 0 (0 - 2) |
| ≥9 | 4 (8.0%) |
| Separation Anxiety | 3 (1 - 5) |
| ≥5 | 15 (30.0%) |
| Social Anxiety | 4.40 ± 2.84 |
| ≥8 | 5 (10.0%) |
| School Avoidance | 0 (0 - 1) |
| ≥3 | 5 (13.9%) |
| Total | 10 (6 - 12) |
| ≥25 | 6 (12.0%) |
| CRIES-13 score | |
| Intrusion | 1.5 (0 - 5) |
| Avoidance | 2.5 (0 - 7) |
| Arousal | 3.5 (1 - 7) |
| Total | 8 (3 - 19) |
| PedsQL score | |
| Physical Health | 71.88 (53.13 - 93.75) |
| Emotional Functioning | 92.5 (85 - 100) |
| Social Functioning | 80 (65 - 100) |
| School Functioning | 63.29 ± 19.25 |
| Psychosocial Health | 78.90 ± 13.14 |
| Total | 75.71 ± 14.57 |
Descriptive statistics are presented using mean ± standard deviation for normally distributed continuous variables, median (25th percentile - 75th percentile) for non-normally distributed continuous variables and frequency (percentage) for categorical variables. Abbreviations; CBCL: Child Behavior Checklist, CDI: Children’s Depression Inventory, CRIES-13: Children’s Revised Impact of Events Scale 13-item, SCARED: Screen for Child Anxiety Related Disorders, PedsQL: Pediatric Quality of Life Inventory.
Table 3.
Correlations between PedsQL scores and CBCL, CDI, SCARED, CRIES-13 scores.
| PedsQL | |||||||
|---|---|---|---|---|---|---|---|
| Physical Health | Emotional Functioning | Social Functioning | School Functioning | Psychosocial Health | Total | ||
| CBCL Total | r | -0.417‡ | -0.778‡ | -0.406‡ | -0.140‡ | -0.608‡ | -0.607‡ |
| p | 0.003 | <0.001 | 0.003 | 0.422 | <0.001 | <0.001 | |
| CDI | r | -0.365‡ | -0.688‡ | -0.284‡ | -0.197† | -0.467† | -0.446† |
| p | 0.009 | <0.001 | 0.045 | 0.257 | 0.001 | 0.001 | |
| SCARED Panic/Somatic | r | -0.278‡ | -0.678‡ | -0.177‡ | 0.101‡ | -0.390‡ | -0.397‡ |
| p | 0.051 | <0.001 | 0.219 | 0.565 | 0.005 | 0.004 | |
| SCARED Generalized Anxiety | r | -0.275‡ | -0.757‡ | -0.211‡ | 0.084‡ | -0.539‡ | -0.439‡ |
| p | 0.053 | <0.001 | 0.142 | 0.630 | <0.001 | 0.001 | |
| SCARED Separation Anxiety | r | -0.147‡ | -0.514‡ | -0.213‡ | -0.110‡ | -0.370‡ | -0.318‡ |
| p | 0.310 | <0.001 | 0.137 | 0.529 | 0.008 | 0.025 | |
| SCARED Social Anxiety | r | -0.511‡ | -0.516‡ | -0.304‡ | -0.223† | -0.480† | -0.582† |
| p | <0.001 | <0.001 | 0.032 | 0.198 | <0.001 | <0.001 | |
| SCARED School Avoidance | r | -0.373‡ | -0.595‡ | -0.099‡ | -0.157‡ | -0.409‡ | -0.457‡ |
| p | 0.025 | <0.001 | 0.566 | 0.367 | 0.013 | 0.005 | |
| SCARED Total | r | -0.403‡ | -0.745‡ | -0.312‡ | -0.087‡ | -0.510‡ | -0.557‡ |
| p | 0.004 | <0.001 | 0.028 | 0.620 | <0.001 | <0.001 | |
| CRIES-13 Intrusion | r | -0.169‡ | -0.642‡ | -0.320‡ | -0.075‡ | -0.522‡ | -0.400‡ |
| p | 0.239 | <0.001 | 0.023 | 0.667 | <0.001 | 0.004 | |
| CRIES-13 Avoidance | r | -0.216‡ | -0.436‡ | -0.376‡ | -0.181‡ | -0.470‡ | -0.396‡ |
| p | 0.132 | <0.001 | 0.007 | 0.297 | 0.001 | 0.004 | |
| CRIES-13 Arousal | r | -0.434‡ | -0.665‡ | -0.225‡ | -0.165‡ | -0.544‡ | -0.575‡ |
| p | 0.002 | <0.001 | 0.117 | 0.342 | <0.001 | <0.001 | |
| CRIES-13 Total | r | -0.336‡ | -0.676‡ | -0.340‡ | -0.207‡ | -0.605‡ | -0.548‡ |
| p | 0.017 | <0.001 | 0.016 | 0.234 | <0.001 | <0.001 | |
† Pearson correlation coefficient, ‡ Spearman correlation coefficient. Statistically significant p values are shown in bold. Abbreviations: CBCL: Child Behavior Checklist, CDI: Children’s Depression Inventory, CRIES-13: Children’s Revised Impact of Events Scale 13-item, PedsQL: Pediatric Quality of Life Inventory, r: Correlation coefficient, SCARED: Screen for Child Anxiety Related DisordersCBCL: Child Behavior Checklist, CDI: Children’s Depression Inventory, SCARED: Screen for Child Anxiety Related Disorders, CRIES-13: Children’s Revised Impact of Events Scale 13-item, PedsQL: Pediatric Quality of Life Inventory.
Table 4.
Associations between PedsQL Total score, linear regression analysis results.
| Univariable | Multivariable (a) | |||||
|---|---|---|---|---|---|---|
| Unstandardized coefficients (95% CI) | Standardized coefficients | p | Unstandardized coefficients (95% CI) | Standardized coefficients | p | |
| Age of child, years | 1.400 (0.084 - 2.715) | 0.295 | 0.038 | 0.081 | ||
| Sex, Female | -4.719 (-13.042 - 3.604) | -0.162 | 0.260 | |||
| Body mass index, kg/m2 | 0.283 (-0.731 - 1.297) | 0.081 | 0.577 | |||
| Comorbidity, Yes | -11.494 (-32.598 - 9.610) | -0.156 | 0.279 | |||
| Immigrant, Yes | 0.670 (-11.395 - 12.735) | 0.016 | 0.912 | |||
| Going to school, Yes | -2.047 (-11.353 - 7.259) | -0.064 | 0.660 | |||
| Age of mother, years | 0.259 (-0.443 - 0.962) | 0.107 | 0.461 | |||
| Education status of mother | 0.114 (-3.123 - 3.352) | 0.010 | 0.944 | |||
| Age of father, years | -0.069 (-0.774 - 0.637) | -0.029 | 0.846 | |||
| Education status of father | -0.150 (-3.419 - 3.119) | -0.013 | 0.927 | |||
| Chronic disease in family, Yes | -10.134 (-20.180 - -0.088) | -0.281 | 0.048 | 0.072 | ||
| Age at transplantation, years | -0.197 (-1.060 - 0.667) | -0.066 | 0.649 | |||
| Time since transplantation, years | 0.777 (-0.049 - 1.603) | 0.263 | 0.065 | |||
| Type of donor, Deceased | -10.081 (-22.628 - 2.467) | -0.227 | 0.113 | |||
| Immunosuppressive drug, Everolimus | -1.406 (-13.466 - 10.654) | -0.034 | 0.816 | |||
| Hospitalization, last year | -19.421 (-40.031 - 1.189) | -0.264 | 0.064 | |||
| AST | 0.031 (-0.136 - 0.197) | 0.053 | 0.714 | |||
| ALT | 0.035 (-0.051 - 0.122) | 0.118 | 0.414 | |||
| Bilirubin | -0.320 (-1.602 - 0.961) | -0.072 | 0.618 | |||
| GGT | 0.007 (-0.046 - 0.061) | 0.040 | 0.783 | |||
| Psychiatric follow-up, Yes | -24.020 (-53.103 - 5.063) | -0.233 | 0.103 | |||
| Type of interview, Online | 7.661 (-0.591 - 15.914) | 0.260 | 0.068 | |||
| CBCL Total score | -0.408 (-0.611 - -0.206) | -0.505 | <0.001 | 0.279 | ||
| CDI score | -1.189 (-1.881 - -0.497) | -0.446 | 0.001 | 0.475 | ||
| SCARED Total score | -0.719 (-1.088 - -0.350) | -0.493 | <0.001 | -0.431 (-0.824 - -0.038) | -0.295 | 0.032 |
| CRIES-13 Total score | -0.642 (-0.928 - -0.356) | -0.546 | <0.001 | -0.471 (-0.787 - -0.154) | -0.400 | 0.004 |
| Adjusted R2 | - | 0.337 | ||||
| Regression model | - | F=13.436, p<0.001 | ||||
(a) Multivariable analysis was performed via stepwise selection method to avoid multicollinearity. Variance inflation factor (VIF) of the variables in the final model is 1.321. Statistically significant p values are shown in bold. Abbreviations: ALT: Alanine aminotransferase, AST: Aspartate aminotransferase, CBCL: Child Behavior Checklist, CDI: Children’s Depression Inventory, CI: Confidence interval, CRIES-13: Children’s Revised Impact of Events Scale 13-item, GGT: Gamma-glutamyl transferase, PedsQL: Pediatric Quality of Life Inventory, SCARED: Screen for Child Anxiety Related Disorders, VIF: Variance inflation factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



