Submitted:
25 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Background/Objectives:
Erythroderma is a rare but potentially life-threatening dermatological emergency characterised by generalised erythema and scaling involving more than 80% of the total body surface area. Erythroderma is associated with significant morbidity and mortality due to systemic complications and diverse underlying aetiologies.
Methods:
In this narrative review PubMed and Google Scholar were searched up to February 2026. Studies were screened for relevance to emergency physicians, with emphasis on epidemiology, diagnostic approach and acute management. Non-English publications and conference abstracts were excluded. Fifty-seven sources were included in the final synthesis.
Results:
Erythroderma most commonly results from exacerbation of pre-existing inflammatory dermatoses, drug reactions, infections, or cutaneous T-cell lymphoma. Clinical presentation includes diffuse erythema and scaling affecting ≥80–90% of body surface area, often accompanied by pruritus, systemic symptoms, and signs of organ dysfunction. Systemic complications arise from cutaneous barrier failure and include fluid imbalance, thermoregulatory dysfunction, cardiovascular strain, protein loss, and secondary infection. Initial emergency department management prioritises supportive care, fluid and nutritional optimisation, restoration of skin barrier function, and assessment for organ dysfunction. While definitive aetiological diagnosis is not always immediately required, certain conditions—particularly severe drug reactions and infectious causes such as Staphylococcal Scalded Skin Syndrome—necessitate urgent targeted intervention.
Conclusions:
Erythroderma represents a syndromic emergency requiring systematic evaluation and early supportive management. Prompt recognition of high-risk aetiologies and timely dermatology referral are essential to optimise outcomes and reduce morbidity and mortality.
Keywords:
erythroderma
; emergency management
; dermatological emergency
; skin support
1. Introduction
Dermatological disease accounts for approximately 4–12% of emergency department (ED) visits [1,2,3]. Among these presentations, infectious conditions such as cellulitis and cutaneous abscesses constitute 46.73–65% of cases [2,4,5]. The majority of dermatological ED visits are non-emergent; up to 95% of patients younger than 30 years present with conditions that could be managed in primary care settings [6], thereby placing an avoidable strain on emergency services. Furthermore, many patients presenting with dermatological complaints have significant co-morbid disease. Of those requiring hospital admission, as few as 2.2% are admitted to a dedicated dermatology ward [7], reflecting both the systemic implications of severe cutaneous disease and limited access to specialised dermatology services.
Erythroderma is a clinical syndrome characterised by generalised erythema and scaling involving more than 90% of the total body surface area. In patients with skin of colour, erythema may be more subtle and fine scale may be a diagnostic clue (Figure 1). It is a rare condition, with an estimated incidence of 1–2 per 100,000 adults (0.001–0.002%) [8]. Erythroderma most commonly affects middle-aged males, with a mean age of onset ranging between 42 and 61 years [8,9,10]. Reported mortality rates vary considerably between studies, ranging from 3.73% to 9.1% [11,12], likely reflecting heterogeneity in underlying aetiology, patient comorbidities, and healthcare settings. Importantly, irrespective of the underlying cause, hospitalised patients with erythroderma demonstrate higher mortality rates per person-years compared to non-erythrodermic patients with the same dermatological disease as well as population controls [13].
Although erythroderma represents a small proportion of dermatological ED presentations, its potential for significant morbidity and mortality, combined with frequent admission to non-dermatological specialties, underscores the importance of early recognition and appropriate initial management by emergency physicians.
Figure 1.
The back of a darker toned skin erythrodermic patient: There is fine scale over the entire back with a central area of sparing that appears hyperpigmented.
Figure 1.
The back of a darker toned skin erythrodermic patient: There is fine scale over the entire back with a central area of sparing that appears hyperpigmented.

2. Materials and Methods
All elements assessed in the SANRA scale are included in this narrative review [14].
We aimed to provide an overview of erythroderma, evaluate the most common aetiologies and synthesize emergency management that should be initiated at patient presentation in emergency units.
A structured search of PubMed and Google Scholar for articles published up to February 2026 was conducted. No date restrictions were applied. A combination of keywords and Medical Subject Headings (MeSH) terms was used, including “erythroderma”, “emergency medicine”, “emergency department”, “management”, and “aetiology”. Specific guidelines for emergency management of different aetiologies of erythroderma were sought.
All study designs were included; including systematic reviews, narrative reviews, cohort studies, case-control studies, case series, and relevant observational studies. Non-English language publications and conference abstracts were excluded.
Titles and abstracts were screened for relevance prior to full-text review. Articles were selected based on their relevance to the emergency physician, with emphasis on epidemiology, diagnostic approach, acute management, and early referral considerations. Studies focusing exclusively on definitive long-term management of specific underlying aetiologies were excluded. A total of 57 sources were included in this narrative review.
The authors independently reviewed the literature and met on three occasions to synthesise the evidence and identify key clinical concepts relevant to the emergency management of erythroderma. Both authors contributed to manuscript drafting and approved the final version of the manuscript.
3. Results
3.1. Definition and Pathophysiology of Erythroderma
Erythroderma is defined as generalised erythema and scaling involving the majority of the body surface area. Historically, involvement of more than 90% of total body surface area (BSA) has been used as the diagnostic threshold. However, given the systemic complications associated with widespread cutaneous inflammation, more inclusive definitions of ≥80% BSA have been adopted [15].
Erythroderma remains incompletely understood and is considered a final common pathway of dysregulated cutaneous inflammation. In erythrodermic psoriasis, atopic dermatitis, drug reactions, and certain cutaneous malignancies, a predominance of T-helper 2 (Th2)–skewed inflammation has been described, characterised by increased levels of interleukin (IL)-4, IL-5, IL-10, and IL-13 [8]. Other studies have demonstrated prominent roles for IL-1, IL-8, tumour necrosis factor (TNF), and interferon-γ (IFN-γ) [16], suggesting heterogeneity in cytokine profiles depending on the underlying aetiology.
Despite differing upstream triggers, inflammatory pathways converge on increased endothelial expression of adhesion molecules, enhanced recruitment of inflammatory cells, and amplification of pro-inflammatory mediators within the dermis. This process accelerates epidermal mitotic activity and shortens keratinocyte transit time [8,16]. The resultant rapid epidermal turnover leads to excessive shedding of keratinocytes containing abnormal quantities of amino acids, proteins, and nucleic acids, clinically manifesting as diffuse scaling. Concurrent dysregulation of angiogenic factors and inflammatory mediators contributes to cutaneous vasodilatation and the characteristic diffuse erythema.
The natural history of erythroderma varies according to the underlying aetiology. Systemic complications are influenced both by the precipitating cause and by the duration of disease prior to presentation. Prolonged untreated erythroderma may impair physiological compensatory mechanisms and increase the risk of systemic sequelae.
3.2. Consequences of Erythroderma
Erythroderma represents a state of functional cutaneous failure, with disruption of barrier integrity, thermoregulation, and metabolic homeostasis. The major systemic consequences include:
1. Metabolic derangement and protein loss
Increased epidermal turnover results in substantial protein loss through exfoliative scaling. Compared with normal skin, protein loss may increase by approximately 15% in drug reactions and eczema, and up to 30% in psoriatic erythroderma [16,17]. This may lead to negative nitrogen balance, loss of muscle mass, peripheral oedema, hypalbuminaemia, and haemodilution [17].
2. Cardiovascular complications
Peripheral vasodilatation and cutaneous shunting may precipitate pedal oedema and high-output cardiac failure [18,19,20]. Cardiac arrhythmias have been reported in up to 11% of patients [21].
3. Thermoregulatory dysfunction
Increased heat loss through inflamed and barrier-disrupted skin may result in hypothermia [18].
4. Increased susceptibility to infection
Loss of barrier function facilitates colonisation, particularly by Staphylococcus aureus, and increases the risk of secondary cutaneous and systemic infection [8,16]. Some studies suggest that patients with abnormal liver function tests may have an increased susceptibility to infection [21].
5. Increased trans-epidermal water loss
Barrier disruption results in significant trans-epidermal water loss, predisposing patients to dehydration [22] .
These systemic consequences may account for the morbidity and mortality associated with erythroderma and underscore the need for early recognition and supportive management in the emergency setting.
3.3. Causes of Erythroderma
Erythroderma may be present at birth or develop during childhood and, most commonly, adulthood, with each age group demonstrating distinct underlying aetiologies [8]. Neonatal erythroderma is typically recognised within specialised neonatal units and is therefore beyond the scope of this review.
In adults, erythroderma most frequently arises from exacerbation of a pre-existing inflammatory dermatosis, particularly psoriasis, atopic dermatitis, or contact dermatitis. Other important and potentially life-threatening aetiologies include cutaneous T-cell lymphoma (CTCL) and severe drug reactions, including drug reaction with eosinophilia and systemic symptoms (DRESS) and Stevens–Johnson syndrome/toxic epidermal necrolysis (SJS/TEN). While SJS/TEN represents a distinct entity characterised by epidermal necrosis rather than classical erythroderma, early presentations may overlap clinically and warrant consideration in the differential diagnosis.
The mnemonic DELI (Drugs, Existing dermatoses, Lymphoma, Infections) provides a practical diagnostic framework for the common aetiologies in adult patients. In contrast, paediatric erythroderma more commonly results from infections or genodermatoses (inherited disorders of keratinisation and skin barrier function). The acronym DIET (Drugs, Infections, Existing dermatoses, Terrible genodermatoses) serves as a useful mnemonic in this population.Recognition of age-specific aetiologies is essential in the emergency setting, as it narrows the differential diagnosis and guides early investigation and referral. An overview of these causes, their reported prevalence in epidemiological studies, and key distinguishing clinical features is summarised in Table 1. Table 2 demonstrates the typical time onset of immunologically mediated drug reaction.
AGEP and DRESS are often accompanied by facial edema. AGEP presents with multiple pustules. DRESS is polymorphic and often progresses from a morbilliform eruption. Italics represent drug reaction that may present with erythroderma.
3.4. Clinical Presentation
Patients typically present with diffuse erythema and scaling affecting ≥80–90% of total body surface area (BSA). Standardised methods for estimating BSA involvement—commonly used in burn assessment—including the Rule of Nines, the Lund and Browder chart, and the Berkow formula may be utilised to quantify disease extent [47]. In addition, the patient’s palm including the fingers approximates 1% of BSA and may be used as a rapid bedside estimation tool in the emergency setting.
Pruritus and chills or rigors are the most frequently reported symptoms. Arthralgia, skin pain, and unintentional weight loss may also occur [21,24].
The onset of erythroderma may be acute or develop insidiously over weeks to months. A history of a preceding dermatosis, such as atopic dermatitis, psoriasis, or cutaneous T-cell lymphoma, may assist in narrowing the differential diagnosis. Careful elicitation of a recent drug exposure is essential. Underlying medical conditions may also provide diagnostic clues; for example, immunocompromised individuals- including those with human immunodeficiency virus infection- are at increased risk of infectious or drug-induced erythroderma.
Following convergence onto the inflammatory pathway characteristic of erythroderma, generalised erythema may precede visible exfoliation by approximately 2–6 days [16]. Progressive scaling subsequently develops. Periorbital oedema may result in ectropion. Specific examination findings that may assist with etiological differentiation include:
- Yellowish thickened palmoplantar skin
- “Islands of sparing” (patches of uninvolved skin within diffuse erythema)
- Nail abnormalities
- Character and morphology of scale (fine, lamellar, greasy, or bran-like)
Systemic inflammatory response may manifest as generalised lymphadenopathy and, less commonly, hepatosplenomegaly [9].
Systemic examination findings often reflect loss of skin barrier and thermoregulatory function, as well as cardiovascular compensation. Peripheral oedema, hypothermia or hyperthermia, and cardiac arrhythmias may be present.
3.5. Initial Evaluation and Investigations
Initial investigation should be guided by clinical examination and assessment of organ dysfunction. Given the recognised association between erythroderma and systemic complications, baseline laboratory investigations should include full blood count (FBC) with differential and peripheral smear, liver function tests, renal function tests (urea and creatinine), and serum amylase and lipase [16,21,48,49,50]. Blood cultures for microscopy, culture, and sensitivity are advisable, as secondary infection occurs in a significant proportion of patients; one case series reported secondary infections in 19.2% of cases [21]. Further organ-specific investigations should be directed by clinical suspicion and laboratory findings.
Skin biopsy can assist in determining the underlying aetiology. In adult patients, histopathological findings at the time of erythroderma correlate with the clinical and final diagnosis in approximately 72.4–85% of cases [12,24]. In neonates and infants (<1 year of age), histopathology is less specific, contributing to diagnostic confirmation in approximately 41.3% of cases [28]. This likely reflects broader etiological heterogeneity and overlapping histopathological features in genodermatoses.
Importantly, while histological evaluation is diagnostically valuable, it is urgent rather than emergent and should not delay initial stabilisation and supportive management.
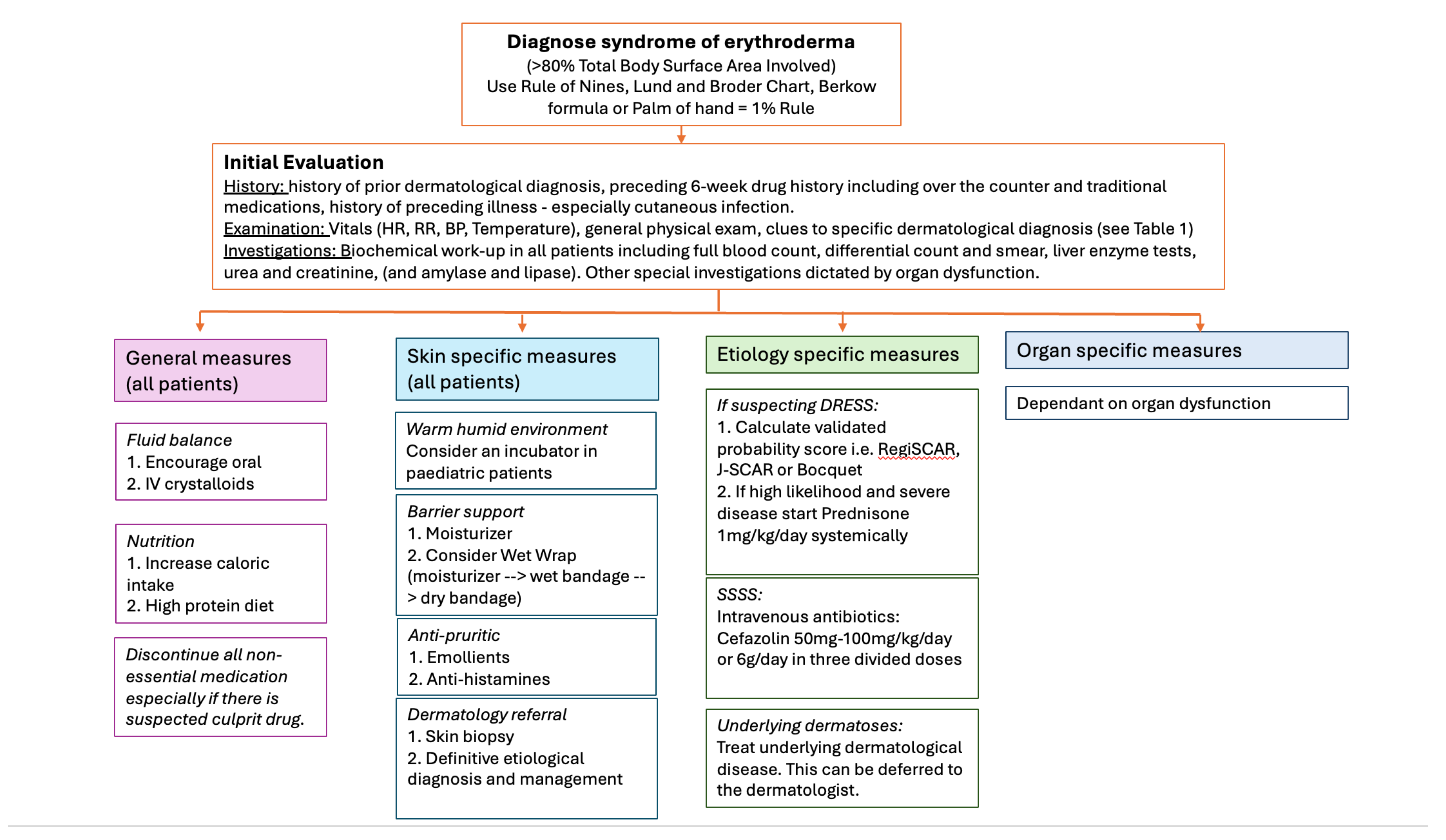
3.6. Management of Erythroderma in the Emergency Department
Initial management in the emergency department (ED) should prioritise general supportive care, restoration of skin barrier function, and identification and treatment of organ dysfunction. While efforts should be made to determine the underlying aetiology, definitive management of the primary disease is not the immediate priority in the acute setting- with specific exceptions such as severe drug reactions and infectious causes which are outlined below and summarised algorithmically in Figure 3.
3.6.1. General Measures
Fluid Management
Patients frequently experience increased trans-epidermal water loss and may have reduced oral intake, particularly when mucosal involvement is present. Adequate oral hydration should be encouraged. If intake is insufficient or there is evidence of dehydration, intravenous crystalloid replacement should be initiated [16,51].
Nutritional Support
Discontinuation of Non-Essential Medications
Drug reactions account for 7.3–67% of erythroderma cases [9,21,23,24,25,26,27,28,29,30,52]. All non-essential medications should be discontinued pending further evaluation. A detailed drug history covering at least the preceding six weeks—including prescription medications, over-the-counter preparations, traditional remedies and vaccines—must be obtained.
3.6.2. Skin Specific Measures
Environmental Modification
Partial Restoration of Skin Barrier Function
Regular application of emollients (e.g., Cetamacrogol-based moisturisers) or occlusive agents (e.g., liquid paraffin) helps reduce trans-epidermal water loss, minimise fissuring, and improve patient comfort [16,51].
Wet wrap therapy may be considered in selected cases. This involves application of a moisturiser to the skin followed by two layers of bandaging: a damp inner layer and a dry outer layer [53,54]. Wet wraps may be combined with topical corticosteroids in inflammatory dermatoses such as atopic dermatitis. However, topical corticosteroids under occlusion may increase systemic absorption and are associated with a non-significant increase in minor skin infections and potential hypothalamic–pituitary–adrenal axis suppression. These risks may be mitigated by using moisturisers alone and ensuring daily wrap changes. In outpatient settings, 100% cotton garments may serve as a practical alternative to bandaging [54].
Anti-Pruritic Measures
Management of Secondary infection
Secondary infection should be suspected in the presence of fever, purulent exudate, rapidly worsening erythema, or systemic instability. Appropriate microbiological sampling should be performed, and empiric antimicrobial therapy initiated in accordance with local guidelines when clinically indicated.
3.6.3. Definitive Diagnosis and Referral
Although identification of the precise aetiology is important, it is not the primary focus of acute ED management. Early referral to dermatology for ongoing investigation, skin biopsy (if indicated), and definitive treatment is essential for optimal long-term outcomes.
3.6.4. Organ Supportive Measures
Organ support should be guided by the presence and severity of dysfunction. Management should follow institutional protocols for cardiovascular instability, electrolyte imbalance, hepatic or renal impairment, and sepsis. Early involvement of appropriate specialty services (e.g., intensive care, infectious diseases, haematology/oncology) may be required depending on clinical presentation.
Mortality in erythroderma is more frequently related to systemic complications than to cutaneous inflammation itself; therefore, meticulous supportive care remains the cornerstone of emergency management.
3.6.5. Etiological Causes That Require Specific Management in the Emergency Department
While most cases of erythroderma are managed initially with supportive measures, certain aetiologies require urgent, targeted intervention in the emergency setting.
Drug Reactions
A high index of suspicion for drug-induced erythroderma is essential, as prompt discontinuation of all non-essential and potentially causative medications is critical. Drug reaction with eosinophilia and systemic symptoms (DRESS) represents a severe and potentially life-threatening hypersensitivity reaction in which early recognition significantly impacts management and prognosis [48,49,50].
Validated diagnostic criteria, including the Bocquet, Japanese Research Committee on Severe Cutaneous Adverse Reaction (J-SCAR), and RegiSCAR scoring systems, may be applied to assess the likelihood of DRESS prior to histopathological confirmation [55]. If DRESS is diagnosed or strongly suspected, additional investigations including quantitative polymerase chain reaction (PCR) testing for human herpesvirus 6 (HHV-6), HHV-7, Epstein–Barr virus (EBV), and cytomegalovirus (CMV) may be considered [48].
Management is stratified by severity. Mild to moderate cases may be managed with high-potency topical corticosteroids and close monitoring. Severe cases, particularly those with internal organ involvement, require systemic corticosteroids at a dose of 1–2 mg/kg/day of prednisone [48,49]. Escalation of care and multidisciplinary involvement may be necessary in cases of significant hepatic, renal, or pulmonary dysfunction.
Staphylococcal Scalded Skin Syndrome (SSSS)
Staphylococcal scalded skin syndrome (SSSS) primarily affects neonates and young children but may occur in immunocompromised adults; it is rare in immunocompetent adults [56]. A history of preceding impetigo or a localised skin infection may be elicited.
SSSS is a toxin-mediated disorder in which a localised focus of Staphylococcus aureus infection produces exfoliative toxins, particularly exfoliative toxin B (ET-B) [56,57] .These toxins disseminate haematogenously and cleave desmoglein 1, a keratinocyte adhesion molecule, leading to superficial epidermal splitting.
Diagnostic considerations include obtaining aerobic bacterial cultures from the primary infectious focus rather than from denuded skin, as cultures from intact infected sites yield higher positivity rates than blood cultures.
Management includes supportive care and prompt initiation of intravenous anti-staphylococcal antibiotics. First-generation cephalosporins are recommended, with cefazolin administered at 50–100 mg/kg/day in children and up to 6 g/day in adults, divided into three doses [56,57]. Antibiotic therapy should be adjusted according to culture results and local resistance patterns.
Crusted Scabies
Crusted scabies should be considered in immunocompromised or debilitated patients presenting with hyperkeratotic scale and widespread erythema. It represents a hyperinfestation with Sarcoptes scabiei var. hominis and is highly contagious. Early recognition is essential, as infection control measures, including patient isolation and contact precautions, must be instituted promptly. Management includes oral ivermectin (if available) in combination with topical scabicidal and keratolytic agents.
Stevens–Johnson Syndrome/Toxic Epidermal Necrolysis (SJS/TEN)
Although SJS/TEN represents a distinct entity characterised by epidermal necrosis rather than classical erythroderma, early presentations may overlap clinically. Rapid progression, mucosal involvement, skin pain disproportionate to clinical findings, and a positive Nikolsky sign should raise suspicion. Figure two demonstrates the classical clinical appearance of SJS. Immediate withdrawal of the offending drug, supportive care in a high-dependency or burn unit setting, and early specialist referral are critical.
Figure 2.
Erythematous macules coalescing into purple dusky patches representing epidermal necrosis.
Figure 2.
Erythematous macules coalescing into purple dusky patches representing epidermal necrosis.

Figure 3.
Figure showing emergency department management approach to the erythrodermic patient.
4. Discussion
Significant gaps remain in the understanding of the converging pathways in erythroderma and in evidence based emergency management. Much of the available literature is derived from retrospective cohort studies and single-centre case series, limiting generalisability. Prospective multicentre studies are needed to better define early predictors of organ dysfunction, stratify risk, and guide triage decisions in the emergency setting.
Standardised clinical pathways for the initial evaluation and management of erythroderma in emergency departments have not been widely established. Development and validation of structured assessment algorithms may improve early recognition of high-risk aetiologies such as severe drug reactions, cutaneous lymphoma, and toxin-mediated infections.
Emerging targeted immunomodulatory therapies have transformed the management of inflammatory dermatoses; however, their role in acute erythrodermic presentations requires further investigation. Additionally, improved biomarkers—clinical, laboratory, and molecular—may enhance early etiological differentiation and inform personalised treatment strategies.
Future research should prioritise integration of dermatology expertise within acute care pathways to optimise outcomes for patients presenting with this complex and potentially life-threatening condition.
5. Conclusions
Erythroderma represents a dermatological emergency and a syndromic presentation with diverse underlying aetiologies. Early recognition is critical, as widespread cutaneous inflammation may be associated with significant systemic complications, including fluid imbalance, thermoregulatory dysfunction, cardiovascular instability, and secondary infection.
Initial management in the emergency department should prioritise supportive care, restoration of skin barrier function, and identification and treatment of organ dysfunction. While definitive etiological diagnosis is not always immediately required, clinicians must maintain a high index of suspicion for conditions requiring urgent targeted intervention, including severe drug reactions such as DRESS and infectious causes such as staphylococcal scalded skin syndrome.
Timely referral to dermatology is essential to facilitate accurate diagnosis, guide definitive therapy, and optimise long-term outcomes. A structured, systematic approach to the patient with erythroderma can improve early management and potentially reduce morbidity and mortality.
Author Contributions
Conceptualization, HM and WV.; methodology, HM and WV.; data curation, HM and WV.; writing—original draft preparation, HM.; writing—review and editing, HM and WV; supervision, WV.; project administration, HM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent has been obtained from patients for clinical pictures included in this review.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ED | Emergency Department |
| SSSS | Staphylococcal scalded skin syndrome |
| DRESS | Drug reaction with eosinophilia and systemic symptoms |
| TEN | Toxic Epidermal Necrolysis |
| SJS | Steven Johnson Syndrome |
| AGEP | Acute Generalized Exanthomatous Pustulosis |
| AD | Atopic Dermatitis |
References
- Kilic, D.; Yigit, O.; Kilic, T.; Buyurgan, C.S.; Dicle, O. Epidemiologic Characteristics of Patients Admitted to Emergency Department with Dermatological Complaints; a Retrospective Cross sectional Study. Arch Acad Emerg Med 2019, 7, e47.
- Agarwal, A.; Verma, H.; Pathak, N.; Gulati, N. An update on dermatological trends among emergency department visits: a cross-sectional analysis, 2017–2021. Arch. Dermatol. Res. 2025, 317, 1–3. [CrossRef]
- Alegre-Sánchez, A.; de Perosanz-Lobo, D.; Pascual-Sánchez, A.; Pindado-Ortega, C.; Fonda-Pascual, P.; Moreno-Arrones, Ó.; Jaén-Olasolo, P. Impact on Quality of Life in Dermatology Patients Attending an Emergency Department. Actas Dermo-Sifiliogr. 2017, 108, 918–923. [CrossRef]
- Baibergenova, A.; Shear, N.H. Skin Conditions That Bring Patients to Emergency Departments. Arch. Dermatol. 2011, 147, 118–120. [CrossRef]
- Nadkarni, A.; Domeisen, N.; Hill, D.; Feldman, S.R. The most common dermatology diagnoses in the emergency department. J. Am. Acad. Dermatol. 2016, 75, 1261–1262. [CrossRef]
- Grillo, E.; Vañó-Galván, S.; Jiménez-Gómez, N.; Ballester, A.; Muñoz-Zato, E.; Jaén, P. Dermatologic Emergencies: Descriptive Analysis of 861 Patients in a Tertiary Care Teaching Hospital. Actas Dermo-Sifiliograficas 2013, 104, 316–324. [CrossRef]
- Okezie PU. Dermatologic Emergency And Rates Of Admission To The Hospital GlobalRPH. Global PxPh The Clinician’s Ultimate Reference 2024. https://globalrph.com/2024/08/dermatologic-emergency-admission-to-hospital/ (accessed January 30, 2026).
- Tso, S.; Satchwell, F.; Moiz, H.; Tushar, H.; Dhariwal, S.; Barlow, R.; Forbat, E.; Randeva, H.; Tan, Y.T.; Ilchyshyn, A.; et al. Erythroderma (exfoliative dermatitis). Part 1: underlying causes, clinical presentation and pathogenesis. Clin. Exp. Dermatol. 2021, 46, 1001–1010. [CrossRef]
- Harper-Kirksey, K. Erythroderma. Life-Threatening Rashes 2018:265. [CrossRef]
- Hulmani, M.; NandaKishore, B.; Bhat, M.; Sukumar, D.; Martis, J.; Kamath, G.; Srinath, M. Clinico-etiological study of 30 erythroderma cases from tertiary center in South India. Indian Dermatol. Online J. 2014, 5, 25–9. [CrossRef]
- Mistry, N.; Gupta, A.; Alavi, A.; Sibbald, R.G. A Review of the Diagnosis and Management of Erythroderma (Generalized Red Skin). Adv. Ski. Wound Care 2015, 28, 228–236. [CrossRef]
- Miyashiro, D.; Sanches, J.A. Erythroderma: a prospective study of 309 patients followed for 12 years in a tertiary center. Sci. Rep. 2020, 10, 1–13. [CrossRef]
- Egeberg, A.; Thyssen, J.; Gislason, G.; Skov, L. Prognosis after Hospitalization for Erythroderma. Acta Dermato-Venereologica 2016, 96, 959–962. [CrossRef]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—a scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 26, 5. [CrossRef]
- Whittaker S. Erythroderma. In: Bolognia JL, Schaffer J V, Cerroni L, editors. Dermatology , vol. 5, Elsevier ; 2024.
- Cuellar-Barboza, A.; Ocampo-Candiani, J.; Herz-Ruelas, M. A Practical Approach to the Diagnosis and Treatment of Adult Erythroderma. Actas Dermo-Sifiliograficas 2018, 109, 777–790. [CrossRef]
- Kanthraj, G.R.; Srinivas, C.R.; Devi, P.U.; Ganasoundari, A.; Shenoi, S.D.; Deshmukh, R.P.; Suresh, B.J.; Pai, S.B.; .; Pgdca Quantitative estimation and recommendations for supplementation of protein lost through scaling in exfoliative dermatitis. Int. J. Dermatol. 1999, 38, 91–95. [CrossRef]
- Sehgal, V.N.; Srivastava, G.; Sardana, K. Erythroderma/exfoliative dermatitis: a synopsis. Int. J. Dermatol. 2003, 43, 39–47. [CrossRef]
- Kurokawa, R.; Hagiwara, A.; Niijima, Y.; Kojima, K. Computed tomography imaging findings in erythrodermic psoriasis treated with infliximab: A case report. Radiol. Case Rep. 2018, 13, 460–463. [CrossRef]
- Shuster, S. HIGH-OUTPUT CARDIAC FAILURE FROM SKIN DISEASE. Lancet 1963, 281, 1338–1340. [CrossRef]
- Lu, L.-Y.; Yu, Y.-Z.; Wang, S.-H.; Zhang, J.; Fan, X.; Qi, Y.; Lin, B.-J. A Clinicopathological, Etiological Analysis of 136 Cases of Erythroderma: A Single-Center Retrospective Study. Int. J. Dermatol. Venereol. 2023, 7, 137–143. [CrossRef]
- Iqbal, M.; Tan, C.-H. Erythroderma and acute skin failure. Medicine 2025, 53, 512–516. [CrossRef]
- Holm, J.; Ren, Z.; McCarthy, M.; Pang, Y.; Nguyen, W.; Guitart, J.; Zhou, X. 64894 Retrospective analysis of demographic and clinical characteristics of erythroderma patients reveals potential risk factors. J. Am. Acad. Dermatol. 2025, 93, AB290. [CrossRef]
- Surekha, A.; Harikrishna, J.; Kushma, T. Aetiology and clinical profile of patients presenting with erythroderma. J. Clin. Sci. Res. 2025. [CrossRef]
- Vasconcellos C, Domingues PP, Aoki V, Miyake RK, Sauaia N, Martins EC. Erythroderma: analysis of 247 cases n.d.
- Avandi B, Ghahartar M, Kashkooli NM, Ahramiyanpour N, Parvizi MM. Epidemiological and clinical features of hospitalized erythroderma patients: a cross-sectional study. Iranian Journal of Dermatology 2022;25:60–5. [CrossRef]
- Sehgal, V.N.; Srivastava, G. Erythroderma/generalized exfoliative dermatitis in pediatric practice: An overview. Int. J. Dermatol. 2006, 45, 831–839. [CrossRef]
- Dhalimi, A.; A., M.A. Neonatal and infantile erythroderma: A clinical and follow-up study of 42 cases. J. Dermatol. 2007, 34, 302–307. [CrossRef]
- Kalsy, J.; Puri, K.J.P.S. Erythroderma in children: Clinico-etiological study from Punjab. Indian J. Paediatr. Dermatol. 2013, 14, 9. [CrossRef]
- Sarkar, R.; Garg, V.K. Erythroderma in children. Indian J. Dermatol. Venereol. Leprol. 2010, 76, 341–7. [CrossRef]
- Pruszkowski, A.; Bodemer, C.; Fraitag, S.; Teillac-Hamel, D.; Amoric, J.-C.; de Prost, Y. Neonatal and Infantile Erythrodermas. Arch. Dermatol. 2000, 136, 875–880. [CrossRef]
- Michalek IMaria, Loring Belinda, John SMalte. Global report on psoriasis 2016:44.
- Emanuel P, Cheng H. Eczema pathology. DermNet 2013:1. https://dermnetnz.org/topics/eczema-pathology (accessed February 7, 2026).
- Jeskey, J.; Kurien, C.; Blunk, H.; Sehmi, K.; Areti, S.; Nguyen, D.; Hostoffer, R. Atopic Dermatitis: A Review of Diagnosis and Treatment. J. Pediatr. Pharmacol. Ther. 2024, 29, 587–603. [CrossRef]
- Guttman-Yassky E, Renert-Yuval Y, Brunner PM. Atopic dermatitis. The Lancet 2025;405:583–96. [CrossRef]
- Joshi, T.P.; Duvic, M. Pityriasis Rubra Pilaris: An Updated Review of Clinical Presentation, Etiopathogenesis, and Treatment Options. Am. J. Clin. Dermatol. 2023, 25, 243–259. [CrossRef]
- Yuan, X.-Y.; Guo, J.-Y.; Dang, Y.-P.; Qiao, L.; Liu, W. Erythroderma: A clinical-etiological study of 82 cases. Eur. J. Dermatol. 2010, 20, 373–377. [CrossRef]
- Dummer, R.; Vermeer, M.H.; Scarisbrick, J.J.; Kim, Y.H.; Stonesifer, C.; Tensen, C.P.; Geskin, L.J.; Quaglino, P.; Ramelyte, E. Cutaneous T cell lymphoma. Nat. Rev. Dis. Prim. 2021, 7, 1–22. [CrossRef]
- Gutiérrez-Cerrajero, C.; Sprecher, E.; Paller, A.S.; Akiyama, M.; Mazereeuw-Hautier, J.; Hernández-Martín, A.; González-Sarmiento, R. Ichthyosis. Nat. Rev. Dis. Prim. 2023, 9, 1–23. [CrossRef]
- Vaillant AAJ, Qurie A. Immunodeficiency. StatPearls 2023.
- Qian, Q.; Shen, J.; Vinturache, A.; Ding, G. Staphylococcal scalded skin syndrome in a child. Lancet Infect. Dis. 2023, 23, 634–634. [CrossRef]
- Mishra, A.K.; Yadav, P.; Mishra, A. A Systemic Review on Staphylococcal Scalded Skin Syndrome (SSSS): A Rare and Critical Disease of Neonates. Open Microbiol. J. 2016, 10, 150–159. [CrossRef]
- Liy-Wong, C.; Pope, E.; Weinstein, M.; Lara-Corrales, I. Staphylococcal scalded skin syndrome: An epidemiological and clinical review of 84 cases. Pediatr. Dermatol. 2020, 38, 149–153. [CrossRef]
- Wang, X.-D.; Shen, H.; Liu, Z.-H. Contagious Erythroderma. J. Emerg. Med. 2016, 51, 180–181. [CrossRef]
- Devi, G.C.; Hazarika, N. Erythroderma secondary to crusted scabies. BMJ Case Rep. 2021, 14, e248000. [CrossRef]
- Talty, R.; Micevic, G.; Damsky, W.; King, B.A. Erythrodermic scabies in an immunocompetent patient. JAAD Case Rep. 2022, 29, 112–115. [CrossRef]
- Cox, S.; Kriho, K.; De Klerk, S.; van Dijk, M.; Rode, H. Total body and hand surface area: Measurements, calculations, and comparisons in ethnically diverse children in South Africa. Burns 2017, 43, 1567–1574. [CrossRef]
- Brüggen, M.-C.; Walsh, S.; Ameri, M.M.; Anasiewicz, N.; Maverakis, E.; French, L.E.; Ingen-Housz-Oro, S.; DRESS Delphi consensus group; Abe, R.; Ardern-Jones, M.; et al. Management of Adult Patients with Drug Reaction with Eosinophilia and Systemic Symptoms. JAMA Dermatol. 2024, 160, 37–44. [CrossRef]
- Wei, B.M.; Fox, L.P.; Kaffenberger, B.H.; Korman, A.M.; Micheletti, R.G.; Mostaghimi, A.; Noe, M.H.; Rosenbach, M.; Shinkai, K.; Kwah, J.H.; et al. Drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms. Part II diagnosis and management. J. Am. Acad. Dermatol. 2023, 90, 911–926. [CrossRef]
- Lee, E.Y.; Peter, J. Diagnosing and Managing Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Amidst Remaining Uncertainty. J. Allergy Clin. Immunol. Pr. 2025, 13, 979–988. [CrossRef]
- Mohapatra, L.; Singh, B.S.T.P.; Satapathy, S.; Samal, K. Pediatric erythroderma – A clinical and therapeutic review. Indian J. Ski. Allergy 2025, 4, 7–18. [CrossRef]
- Mistry, N.; Gupta, A.; Alavi, A.; Sibbald, R.G. A Review of the Diagnosis and Management of Erythroderma (Generalized Red Skin). Adv. Ski. Wound Care 2015, 28, 228–236. [CrossRef]
- González-López, G.; Ceballos-Rodríguez, R.; González-López, J.; Rodríguez, M.F.; Herranz-Pinto, P. Efficacy and safety of wet wrap therapy for patients with atopic dermatitis: a systematic review and meta-analysis. Br. J. Dermatol. 2016, 177, 688–695. [CrossRef]
- Andersen, R.; Thyssen, J.; Maibach, H. The Role of Wet Wrap Therapy in Skin Disorders – A Literature Review. Acta Dermato-Venereologica 2015, 95, 933–939. [CrossRef]
- Kim, D.-H.; Koh, Y.-I. Comparison of Diagnostic Criteria and Determination of Prognostic Factors for Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome. Allergy, Asthma Immunol. Res. 2014, 6, 216–21. [CrossRef]
- Brazel, M.; Desai, A.; Are, A.; Motaparthi, K. Staphylococcal Scalded Skin Syndrome and Bullous Impetigo. Medicina 2021, 57, 1157. [CrossRef]
- Gray, L.; Hansen, A.M.; Cipriano, S.D. Pediatric Staphylococcal Scalded Skin Syndrome: A Systematic Review of the Literature to Inform Work-Up and Management. Pediatr. Dermatol. 2025, 42, 978–984. [CrossRef]

Table 1.
Table of the aetiology of erythroderma, their respective prevalences and salient disease information.
Table 1.
Table of the aetiology of erythroderma, their respective prevalences and salient disease information.
| Etiology |
Adults (%) * [9,12,21,23,24,25,26] |
Children (%) *[27,28,29,30,31] |
Disease information |
| A. Exacerbation of diagnosed underlying dermatoses | 23 to 36.3 | 20 | In cases of exacerbation of a pre-existing dermatosis, a prior history of the underlying condition may be elicited. However, some patients may initially present with erythroderma as the first manifestation of their disease. |
| 1. Psoriasis | 14.5 to 45 | 18 | A multisystem immune-mediated inflammatory disease that classically presents with erythematous plaques and silvery scale, often with nail and joint involvement [32]. Nail findings such as irregular pitting, onycholysis, and “oil drop” discoloration are important diagnostic clues. |
| 2. Eczematous dermatoses | 8 to 33.9 | 14.3 to 20 | Eczema is a clinical term describing cutaneous inflammation that histologically manifests as intercellular oedema of the epidermis (spongiosis) [33]. Like erythroderma, it represents a syndrome with multiple etiologies. Common subtypes are outlined below. |
| 2.1 Atopic dermatitis (AD) | 8.7 to 21.8 | 12 | A chronic relapsing pruritic inflammatory dermatosis characterised by scaly patches on a background of xerosis. AD is part of the atopic spectrum, which includes allergic rhinitis, conjunctivitis, asthma, and food allergy [34,35]Fine scaling commonly accompanies erythrodermic transformation. |
| 2.2 Seborrheic dermatitis | Rare | 5 | Associated with overgrowth of Malassezia furfur, predominantly affecting sebaceous gland–rich areas. In immunocompromised individuals, including patients with HIV, the disease may generalise. The scale is typically greasy and yellowish with a bran-like appearance. |
| 3. Pityriasis Rubra Pilaris (PRP) | 1 | 2.4 | A rare papulosquamous disorder in which a trigger activates the IL-23/Th17 inflammatory pathway, leading to follicular hyperkeratosis and coalescence into widespread erythema [36]. PRP is subdivided into six clinical types, with types I, III, and VI potentially presenting with erythroderma. “Islands of sparing” and waxy palmoplantar keratoderma are characteristic clinical clues. |
| B. Drug reactions | 7.3 to 67 | 29 to 42.8 | Drug reactions may be immunologically or non-immunologically mediated. Temporal association with medication exposure is a key diagnostic clue as demonstrated in table 2. Acute generalized exanthematous pustulosis (AGEP), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS) may present with erythroderma [21,24]. Rapid onset of widespread erythema should raise suspicion for a drug-induced cause. A comprehensive medication history must include prescription drugs, over-the-counter preparations, and traditional remedies. In a Chinese cohort, traditional herbal medications were the most frequently implicated agents [37]. Among hospitalized erythroderma patients, anticonvulsants are commonly reported culprit drugs [21,24,26]. |
| C. Cutaneous T Cell Lymphoma (CTCL) | 4 to 21.8 | Rare | A group of non-Hodgkin lymphomas characterized by monoclonal T-cell infiltration of the skin without extracutaneous involvement at initial diagnosis [38]. Progressive pruritus, lymphadenopathy, and alopecia may be clinical clues. |
| D. Idiopathic | 4.4 to 30 | 30 | No identifiable underlying cause despite appropriate investigation. |
| E. Primary blistering diseases | Rare | Autoimmune or genetic disorders affecting adhesion molecules that maintain structural integrity between keratinocytes and between the epidermis and dermis. Autoantibodies or genetic mutations may disrupt these adhesion proteins, leading to widespread blistering and secondary erythroderma. | |
| F. Genodermatoses | Rare | 18 to 70 ^ | Genetic syndromes with prominent cutaneous manifestations involving skin, hair, and nails. |
| 1. Icthysiform disorders | Rare | 25 to 31.5 | Inherited disorders of keratinization characterized by abnormal epidermal differentiation and barrier dysfunction [39]. |
| 2. Immunodeficiency syndromes | Rare | 4.8 to 30 | Primary or secondary immune system defects that predispose patients to recurrent infections and inflammatory skin disease [40]. |
| G. Infections | 12 | 40 | |
| 1. Staphylococcal scalded skin syndrome | Rare | 7.4 to 18 | Caused by exfoliative toxins produced by Staphylococcus aureus, leading to superficial epidermal splitting [41,42,43]. Skin denudation typically begins on the central face and flexural areas (neck, axillae, groin). Radial fissuring around the mouth and eyes is a useful clinical clue. |
| 2. Crusted scabies | Rare | Occurs predominantly in immunocompromised or debilitated individuals with impaired sensory response [44,45,46]. In this hyper infestation state, millions of Sarcoptes scabiei var. hominis mites inhabit hyperkeratotic scale [46]. Prolonged duration and thick yellow crusted plaques are characteristic. Bedside scraping with potassium hydroxide microscopy is usually diagnostic. Importantly, crusted scabies is highly contagious [44]. | |
* Percentages cited are from collated from multiple sources. Ranges are shown so the total per column is greater than 100%. ^ Pediatric erythroderma can be further subdivided into neonatal, infantile and childhood erythroderma. Genodermatoses predominate etiologically in neonatal and infantile erythroderma.
Table 2.
Table showing the time of initial drug exposure and likely time of onset of immunologically mediated drug reactions.
Table 2.
Table showing the time of initial drug exposure and likely time of onset of immunologically mediated drug reactions.
| Day | 0 | D4-7 | D7 | D14 | D21 | D28 | D35 | D40 | |
| Urticaria Anaphylaxis |
AGEP | SJS/TEN | DRESS | ||||||
| Fixed drug reactions | |||||||||
AGEP: Acute generalized exanthematous pustulosis; SJS: Steven Johnson Syndrome; TEN: Toxic epidermal necrosis; DRESS: Drug reaction with eosinophilia and systemic symptoms.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



