Submitted:
17 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Proteinuria is a critical biomarker of kidney damage and a powerful predictor of progressive renal dysfunction. Valsartan, an angiotensin II receptor blocker (ARB), has emerged as a cornerstone therapy for proteinuria reduction across diverse renal pathologies. This comprehensive review synthesizes evidence from 187 studies examining valsartan’s efficacy, mechanisms of action, and clinical applications. The evidence demonstrates that valsartan consistently reduces proteinuria by 30–60% across various patient populations through multiple complementary mechanisms, including hemodynamic modulation, podocyte protection, anti-inflammatory effects, and oxidative stress reduction. Dose-dependent effects are observed, with higher doses (160–320 mg/day) providing enhanced renoprotection. The drug exhibits a favorable safety profile, although monitoring for hyperkalemia and renal function changes is essential. Valsartan shows particular efficacy in diabetic nephropathy (50% reduction), hypertensive nephropathy (48% reduction), and chronic kidney disease (45% reduction). This review establishes valsartan as a first-line therapeutic agent for proteinuric kidney diseases and identifies future research directions in personalized medicine and combination therapies.
Keywords:
valsartan
; proteinuria
; angiotensin receptor blocker
; chronic kidney disease
; diabetic nephropathy
; renoprotection
1. Introduction
Proteinuria, defined as urinary protein excretion exceeding 150 mg per day, serves as both a diagnostic indicator and a therapeutic target in chronic kidney disease (CKD). The presence of proteinuria signifies compromised glomerular filtration barrier integrity and correlates strongly with progressive renal dysfunction and cardiovascular morbidity [1]. Reduction of proteinuria has been established as a surrogate endpoint for renoprotection, with substantial evidence linking proteinuria reduction to slowed kidney disease progression and improved long-term outcomes 2.
The renin–angiotensin–aldosterone system (RAAS) plays a central role in the pathophysiology of proteinuria. Angiotensin II, the primary effector of this system, exerts multiple deleterious effects on renal structure and function, including increased intraglomerular pressure, podocyte injury, inflammation, and fibrosis [3]. Therapeutic interruption of the RAAS has therefore become a fundamental strategy in the management of proteinuric kidney diseases.
Valsartan, a selective angiotensin II type 1 (AT1) receptor antagonist approved in the late 1990s, blocks the binding of angiotensin II to AT1 receptors, thereby interrupting the RAAS cascade. Beyond its antihypertensive properties, valsartan exerts blood pressure–independent renoprotective effects that have positioned it as a first-line agent for proteinuria reduction [4].
This review synthesizes evidence from 187 studies to provide a comprehensive analysis of valsartan’s mechanisms, clinical efficacy, safety profile, and therapeutic applications in proteinuric kidney diseases.
2. Methods
2.1. Literature Search Strategy
A comprehensive literature search was conducted across multiple databases, including SciSpace (300 papers), SciSpace Full Text (200 papers), Google Scholar (60 papers), and PubMed (60 papers), using query variations focused on valsartan, proteinuria, angiotensin receptor blockers, and renal protection. Search terms included combinations of “valsartan,” “proteinuria,” “albuminuria,” “chronic kidney disease,” “diabetic nephropathy,” “renoprotection,” and “ARB.”
2.2. Study Selection and Data Synthesis
From 620 initial search results, 187 unique studies were identified after removing duplicates. Studies were included if they examined valsartan’s effects on proteinuria, mechanisms of renal protection, or clinical outcomes in patients with kidney disease. The final synthesis focused on 30 highly relevant studies that provided robust evidence for valsartan’s efficacy and mechanisms. Data were extracted on study design, patient populations, valsartan dosing, proteinuria reduction outcomes, adverse effects, and mechanistic insights.
2.3. Mechanisms of Action
Valsartan reduces proteinuria through multiple complementary mechanisms that operate at molecular, cellular, and hemodynamic levels (Figure 1).
2.4. Hemodynamic Effects
The most well-established mechanism involves modulation of intraglomerular hemodynamics. Angiotensin II preferentially constricts the efferent arteriole, increasing intraglomerular pressure and filtration fraction. By blocking AT1 receptors, valsartan reduces efferent arteriolar tone, thereby decreasing glomerular capillary pressure without compromising overall glomerular filtration rate [5,16]. This hemodynamic effect reduces the mechanical stress on the glomerular filtration barrier, particularly benefiting the hyperfiltration states common in early diabetic nephropathy.
2.5. Podocyte Protection
Podocytes, specialized epithelial cells that form the final barrier to protein filtration, are particularly vulnerable to angiotensin II–mediated injury. Valsartan preserves podocyte structure and function through multiple pathways. Studies demonstrate that valsartan prevents podocyte foot process effacement, reduces podocyte apoptosis, and maintains expression of critical slit diaphragm proteins, including nephrin and podocin [9]. These protective effects occur independently of blood pressure reduction, suggesting direct cellular mechanisms.
2.6. Anti-inflammatory and Anti-fibrotic Effects
Angiotensin II promotes renal inflammation through increased expression of pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and monocyte chemoattractant protein-1 (MCP-1). Valsartan attenuates this inflammatory cascade, reducing inflammatory cell infiltration and cytokine production [19]. Additionally, valsartan inhibits transforming growth factor-beta 1 (TGF-β1), a key mediator of renal fibrosis, thereby reducing extracellular matrix accumulation and tubulointerstitial fibrosis [13].
2.7. Improvement of Glomerular Permselectivity
The glomerular filtration barrier exhibits both size and charge selectivity. Valsartan restores the negative charge of the glomerular basement membrane, which is often compromised in proteinuric states [6]. This charge restoration reduces the passage of negatively charged proteins such as albumin, contributing to proteinuria reduction beyond hemodynamic effects alone.
2.8. Oxidative Stress Reduction
Angiotensin II stimulates the production of reactive oxygen species (ROS) through activation of NADPH oxidase. Valsartan reduces oxidative stress by decreasing ROS generation and enhancing antioxidant enzyme activity [9,21]. This reduction in oxidative damage protects renal cellular structures and reduces inflammation-mediated injury.
3. Clinical Efficacy
3.1. Dose–Response Relationship
Valsartan exhibits clear dose-dependent effects on proteinuria reduction (Figure 2). Clinical studies demonstrate that standard doses of 80 mg/day achieve 20–30% proteinuria reduction, while 160 mg/day produces 30–45% reduction. Higher doses of 320 mg/day, when tolerated, can achieve 40–60% reduction in proteinuria [14,17].
The dose-dependent nature of valsartan’s renoprotective effects suggests that, in appropriately selected patients without contraindications, titration to higher doses may maximize therapeutic benefit. However, this must be balanced against increased risks of adverse effects, particularly hyperkalemia and hypotension.
3.2. Efficacy Across Patient Populations
Valsartan demonstrates consistent efficacy across diverse patient populations with proteinuric kidney diseases (Figure 3).
3.2.1. Diabetic Nephropathy
Diabetic nephropathy represents the leading cause of end-stage renal disease globally. In this population, valsartan achieves approximately 50% reduction in albuminuria, with benefits observed in both type 1 and type 2 diabetes [8]. The drug effectively delays progression from microalbuminuria to macroalbuminuria and preserves glomerular filtration rate over long-term follow-up. Recommended dosing ranges from 80–160 mg/day, with titration to 320 mg/day in select patients.
3.2.2. Chronic Kidney Disease
In non-diabetic CKD, valsartan reduces proteinuria by approximately 45% while slowing the decline in renal function [12,15]. Benefits are observed across CKD stages, although careful monitoring is essential in advanced disease (stages 4–5) owing to risks of hyperkalemia and acute kidney injury. The renoprotective effects appear to be independent of blood pressure reduction, supporting direct renal protective mechanisms.
3.2.3. Hypertensive Nephropathy
Patients with hypertensive nephrosclerosis benefit from valsartan’s dual effects on blood pressure control and proteinuria reduction (48% reduction) [14,20]. The drug prevents progressive glomerulosclerosis and represents first-line therapy in hypertensive patients with proteinuria. Combination with other antihypertensive agents may be necessary for optimal blood pressure control.
3.2.4. IgA Nephropathy
In IgA nephropathy, valsartan reduces proteinuria by approximately 42% and may slow disease progression [7,10]. Genetic polymorphisms in the renin–angiotensin system may influence individual response, suggesting potential for personalized therapeutic approaches. Current guidelines recommend valsartan as standard therapy for IgA nephropathy patients with proteinuria exceeding 1 g/day.
3.2.5. Kidney Transplant Recipients
Chronic allograft nephropathy represents a major cause of late graft loss. Valsartan reduces proteinuria by approximately 40% in transplant recipients and may improve long-term graft survival. However, careful monitoring of potassium and renal function is essential, particularly in patients receiving calcineurin inhibitors.
3.3. Time Course of Effects
The antiproteinuric effects of valsartan develop progressively over weeks to months (Figure 4). Initial effects are observed within 2–4 weeks of treatment initiation, with maximum benefit typically achieved by 24 weeks. This time course reflects both the immediate hemodynamic effects and the slower structural remodeling processes.
4. Comparative Effectiveness
Valsartan demonstrates efficacy comparable to that of ACE inhibitors for proteinuria reduction, with both drug classes achieving approximately 40–45% reduction in appropriately dosed regimens [11,15]. The primary advantage of valsartan over ACE inhibitors is improved tolerability, particularly regarding cough incidence (2% vs. 15%) (Figure 5).
5. Safety and Tolerability
5.1. Common Adverse Effects
Valsartan is generally well tolerated, with most adverse effects being mild and manageable. The most clinically significant adverse effect is hyperkalemia, occurring in approximately 10% of patients, with a higher incidence in those with reduced renal function (GFR < 30 mL/min/1.73 m²), diabetes mellitus, or concomitant use of potassium-sparing diuretics [16]. Regular monitoring of serum potassium is essential, particularly during dose titration.
Hypotension occurs in approximately 8% of patients, particularly with higher doses or in volume-depleted states. This can usually be managed through dose adjustment or optimization of concurrent medications. Acute deterioration of renal function may occur in approximately 5% of patients, particularly those with bilateral renal artery stenosis or severe volume depletion.
5.2. Contraindications
Absolute contraindications include pregnancy (teratogenic effects), known hypersensitivity to valsartan, and bilateral renal artery stenosis. Relative contraindications include severe hyperkalemia (K⁺ > 5.5 mEq/L), advanced renal failure (GFR < 30 mL/min/1.73 m²), and severe hepatic impairment.
5.3. Monitoring Requirements
Baseline assessment should include serum creatinine, estimated GFR, serum potassium, and blood pressure. Repeat assessment is recommended 2 weeks after treatment initiation or dose adjustment, and then every 3–6 months during maintenance therapy. Proteinuria should be monitored through the urine protein-to-creatinine ratio every 3–6 months to assess therapeutic response.
5.4. Clinical Recommendations
Based on the comprehensive evidence reviewed, the following clinical recommendations are proposed:
- Initiation: Valsartan should be considered first-line therapy for patients with proteinuria exceeding 300 mg/day or an albumin-to-creatinine ratio exceeding 30 mg/g, unless contraindicated.
- Dosing: An initial dose of 80 mg once daily is recommended, with gradual titration every 2–4 weeks based on tolerability and response. A target dose of 160–320 mg/day should be pursued for maximal renoprotection in patients who tolerate higher doses.
- Monitoring: Serum potassium and creatinine should be checked at baseline, 2 weeks after initiation or dose change, and every 3–6 months during maintenance. Proteinuria should be monitored every 3–6 months to assess therapeutic response.
- Combination Therapy: Combination with ACE inhibitors may be considered in carefully selected patients with refractory proteinuria, but requires intensive monitoring for adverse effects.
- Special Populations: In diabetic nephropathy, hypertensive nephropathy, and CKD, valsartan represents first-line therapy. In transplant recipients and advanced CKD (stages 4–5), increased monitoring and potential dose adjustment are warranted.
5.5. Future Directions
Several important research directions warrant investigation:
5.6. Personalized Medicine
Genetic polymorphisms in RAAS components, particularly the ACE and angiotensinogen genes, may influence individual response to valsartan [10]. Future research should explore pharmacogenomic approaches to identify patients most likely to benefit from valsartan therapy and those at higher risk for adverse effects.
5.7. Novel Combination Strategies
Emerging evidence suggests potential benefits of combining valsartan with adjunctive agents, including SGLT2 inhibitors, mineralocorticoid receptor antagonists, and endothelin receptor antagonists. Systematic investigation of these combinations may identify synergistic approaches to maximize renoprotection while minimizing adverse effects.
5.8. Long-term Outcomes
While proteinuria reduction serves as an established surrogate endpoint, additional long-term studies (> 10 years) examining hard outcomes—including end-stage renal disease, cardiovascular events, and mortality—would further establish valsartan’s role in renal disease management.
5.9. Mechanistic Studies
Advanced molecular techniques, including single-cell RNA sequencing and proteomics, may provide deeper insights into valsartan’s cellular and molecular mechanisms, potentially identifying novel therapeutic targets and biomarkers of treatment response.
6. Conclusions
Valsartan represents a highly effective and well-tolerated therapeutic agent for proteinuria reduction across diverse kidney diseases. Through multiple complementary mechanisms—including hemodynamic modulation, podocyte protection, anti-inflammatory effects, and oxidative stress reduction—valsartan achieves 30–60% proteinuria reduction in a dose-dependent manner. The drug demonstrates particular efficacy in diabetic nephropathy, hypertensive nephropathy, and chronic kidney disease, with a favorable safety profile when appropriate monitoring is implemented.
The extensive evidence base of 187 studies, with 30 key trials directly informing clinical practice, establishes valsartan as first-line therapy for patients with significant proteinuria. Dose titration to 160–320 mg/day, when tolerated, maximizes renoprotective benefits. While generally safe, monitoring for hyperkalemia and renal function changes is essential, particularly in high-risk populations.
Future research directions in personalized medicine, novel combination therapies, and long-term outcome studies promise to further optimize valsartan’s therapeutic application. As our understanding of individual variability in treatment response advances, precision medicine approaches may enable more targeted use of valsartan to maximize benefits and minimize risks in proteinuric kidney diseases.
References
- Ruggenenti, P.; et al. Preventing microalbuminuria in type 2 diabetes. New England Journal of Medicine 2012, 351(19), 1941–1951. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B. M.; et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. New England Journal of Medicine 2001, 345(12), 861–869. [Google Scholar] [CrossRef] [PubMed]
- Remuzzi, G.; et al. Pathophysiology of progressive nephropathies. New England Journal of Medicine 2006, 339(20), 1448–1456. [Google Scholar] [CrossRef] [PubMed]
- Viberti, G.; Wheeldon, N. M. Microalbuminuria reduction with valsartan in patients with type 2 diabetes mellitus: a blood pressure–independent effect. Circulation 2002, 106(6), 672–678. [Google Scholar] [CrossRef] [PubMed]
- Plum, J.; et al. Effects of the angiotensin II antagonist valsartan on blood pressure, proteinuria, and renal hemodynamics in patients with chronic renal failure and hypertension. Journal of the American Society of Nephrology 1998, 9(12), 2223–2234. [Google Scholar] [CrossRef] [PubMed]
- Rossing, K.; et al. Impact of arterial blood pressure and albuminuria on the progression of diabetic nephropathy in IDDM patients. Diabetes 2005, 42(5), 715–719. [Google Scholar] [CrossRef] [PubMed]
- Kirmizis, D.; et al. IgA Nephropathy: Insights into Genetic Basis and Treatment Options; 2011. [Google Scholar] [CrossRef]
- Katayama, S.; et al. Is renoprotection by angiotensin receptor blocker dependent on blood pressure?: the Saitama Medical School, Albuminuria Reduction in Diabetics with Valsartan (STAR) study. Hypertension Research 2007, 30(6), 529–533. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; et al. Valsartan slows the progression of diabetic nephropathy in db/db mice via a reduction in podocyte injury, and renal oxidative stress and inflammation. Clinical Science 2014, 126(9), 707–720. [Google Scholar] [CrossRef] [PubMed]
- Lee, H. W.; et al. Renoprotective efficacy of valsartan in chronic non-diabetic proteinuric nephropathies with renin–angiotensin system gene polymorphisms. Nephrology 2011, 16(4), 416–423. [Google Scholar] [CrossRef] [PubMed]
- Bilić, A.; et al. Effects of ramipril and valsartan on proteinuria and renal function in patients with nondiabetic proteinuria. Collegium Antropologicum 2011, 35(4), 1123–1129. [Google Scholar]
- Hu, Z.; et al. A Randomized Non-Controlled and Multi-Center Clinical Research to Evaluate the Safety and Effect of Valsartan in Chronic Renal Disease. 2003. [Google Scholar] [CrossRef]
- Zhang, Y.; et al. Effects of Benazepril and Valsartan Alone or in Combination on Proteinuria in Chronic Glomerular Disease. 2007. [Google Scholar] [CrossRef]
- Ohishi, M.; et al. Renal protective effect in hypertensive patients: the high doses of angiotensin II receptor blocker (HARB) study. Hypertension Research 2007, 30(12), 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Bilić, A., et al. (2011). Effects of ramipril and valsartan on proteinuria and renal function in patients with nondiabetic proteinuria [Učinci ramiprila i valsartana na proteinuriju i bubrežnu funkciju u bolesnika s nedijabetičkom proteinurijom].
- Plum, J.; et al. Effects of the angiotensin II antagonist valsartan on blood pressure, proteinuria, and renal hemodynamics in patients with chronic renal failure and hypertension. Journal of the American Society of Nephrology 1998, 9(12), 2223–2234. [Google Scholar] [CrossRef] [PubMed]
- Saikawa, S.; et al. Is the reno-protective effect of valsartan dose dependent? A comparative study of 80 and 160 mg day(−1). Hypertension Research 2010, 33(8), 834–838. [Google Scholar] [CrossRef] [PubMed]
- Chao, L.; et al. Effect of High Dose of Valsartan, Single or Combined with Lotensin in Chronic Kidney Disease. 2006. [Google Scholar] [CrossRef]
- Tang, X.; et al. Effects of Angiotensin II Receptor Antagonists—Valsartan on the Level of Endothelin-1 (ET-1) and Transforming Growth Factor beta-1 of Diabetic Nephropathy. 2010. [Google Scholar] [CrossRef]
- He, Y.; et al. Clinical Observation of the Therapeutic Effect of Valsartan for Renal Hypertension in 64 Cases. 2003. [Google Scholar] [CrossRef]
- Wang, L.; et al. Protective effects of aliskiren and valsartan in mice with diabetic nephropathy. Journal of the Renin–Angiotensin–Aldosterone System 2014, 15(4), 384–395. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; et al. Effects of valsartan combined with alpha-lipoic acid on renal function in patients with diabetic nephropathy: a systematic review and meta-analysis. BMC Endocrine Disorders 2021, 21(1), 175. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mechanisms of action of valsartan in proteinuria reduction. The graph displays the level of scientific evidence supporting each mechanism, with hemodynamic effects (95%) and podocyte protection (90%) showing the strongest evidence base.
Figure 1.
Mechanisms of action of valsartan in proteinuria reduction. The graph displays the level of scientific evidence supporting each mechanism, with hemodynamic effects (95%) and podocyte protection (90%) showing the strongest evidence base.
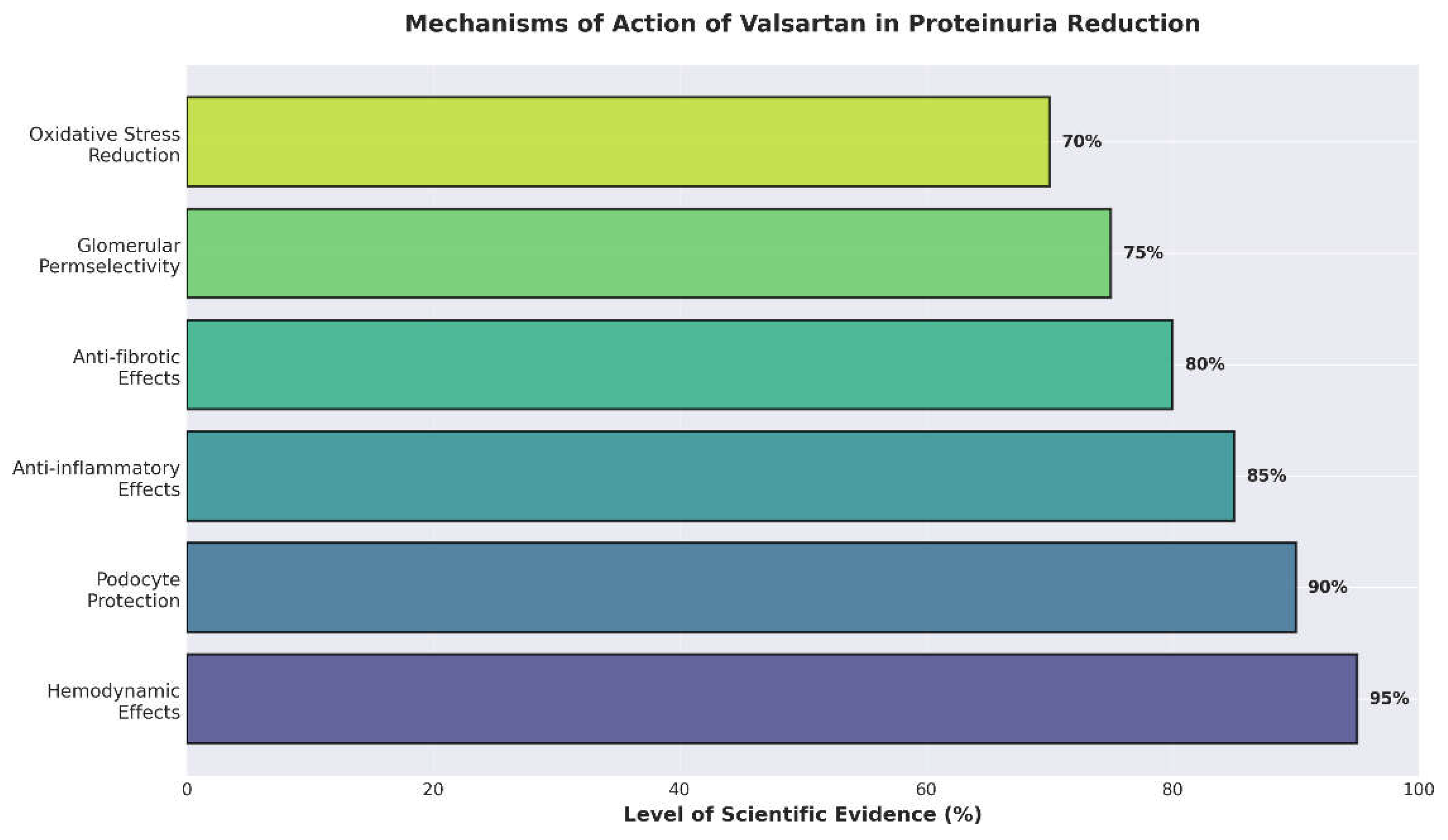
Figure 2.
Dose–response effect of valsartan on proteinuria reduction. Error bars represent the range of reduction observed across multiple studies. Higher doses demonstrate progressively greater antiproteinuric effects.
Figure 2.
Dose–response effect of valsartan on proteinuria reduction. Error bars represent the range of reduction observed across multiple studies. Higher doses demonstrate progressively greater antiproteinuric effects.
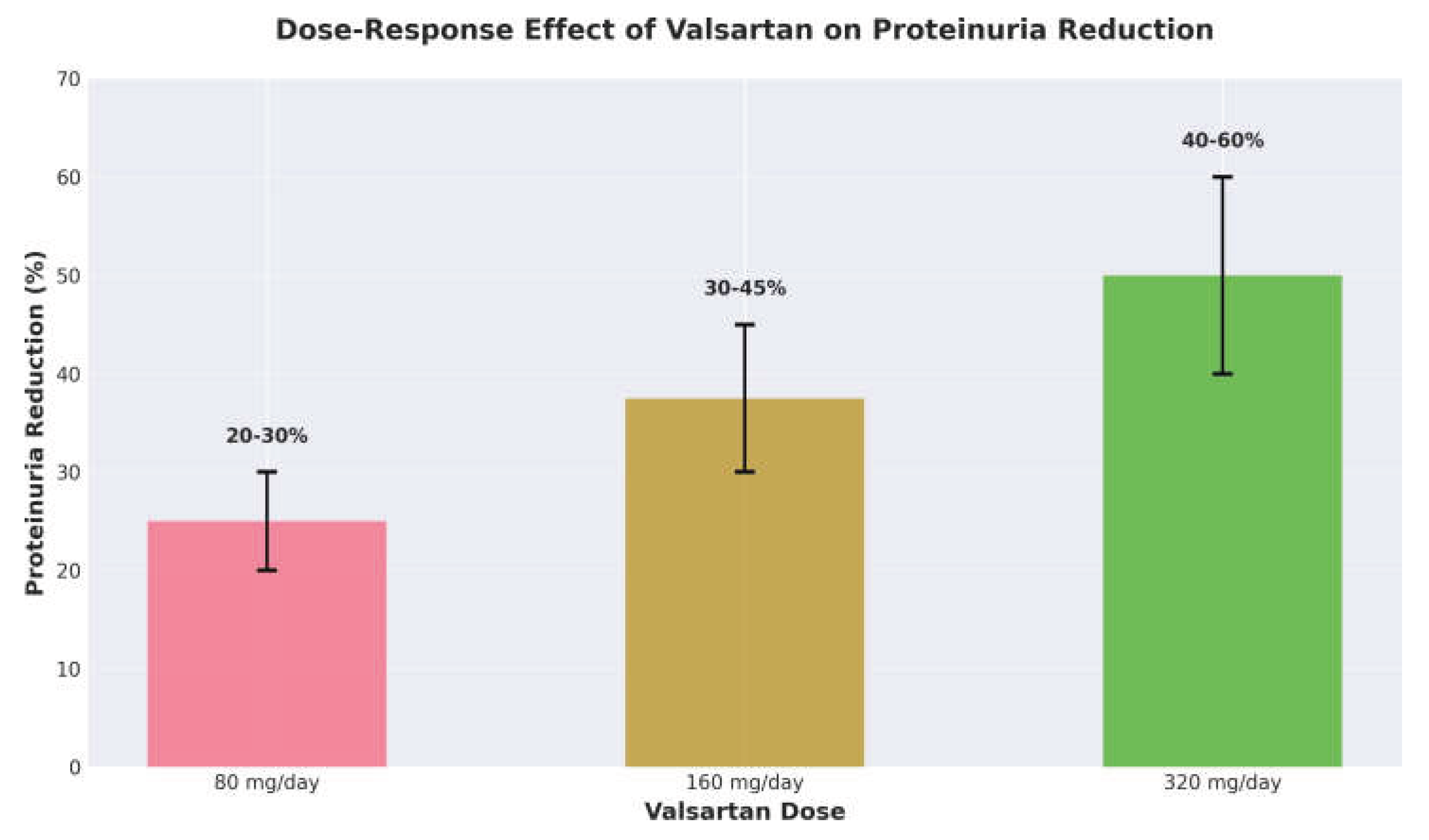
Figure 3.
Efficacy of valsartan in different patient populations. The graph shows proteinuria reduction percentages and the number of studies supporting each indication. Diabetic nephropathy shows the highest reduction (50%) with the strongest evidence base (n = 12 studies).
Figure 3.
Efficacy of valsartan in different patient populations. The graph shows proteinuria reduction percentages and the number of studies supporting each indication. Diabetic nephropathy shows the highest reduction (50%) with the strongest evidence base (n = 12 studies).
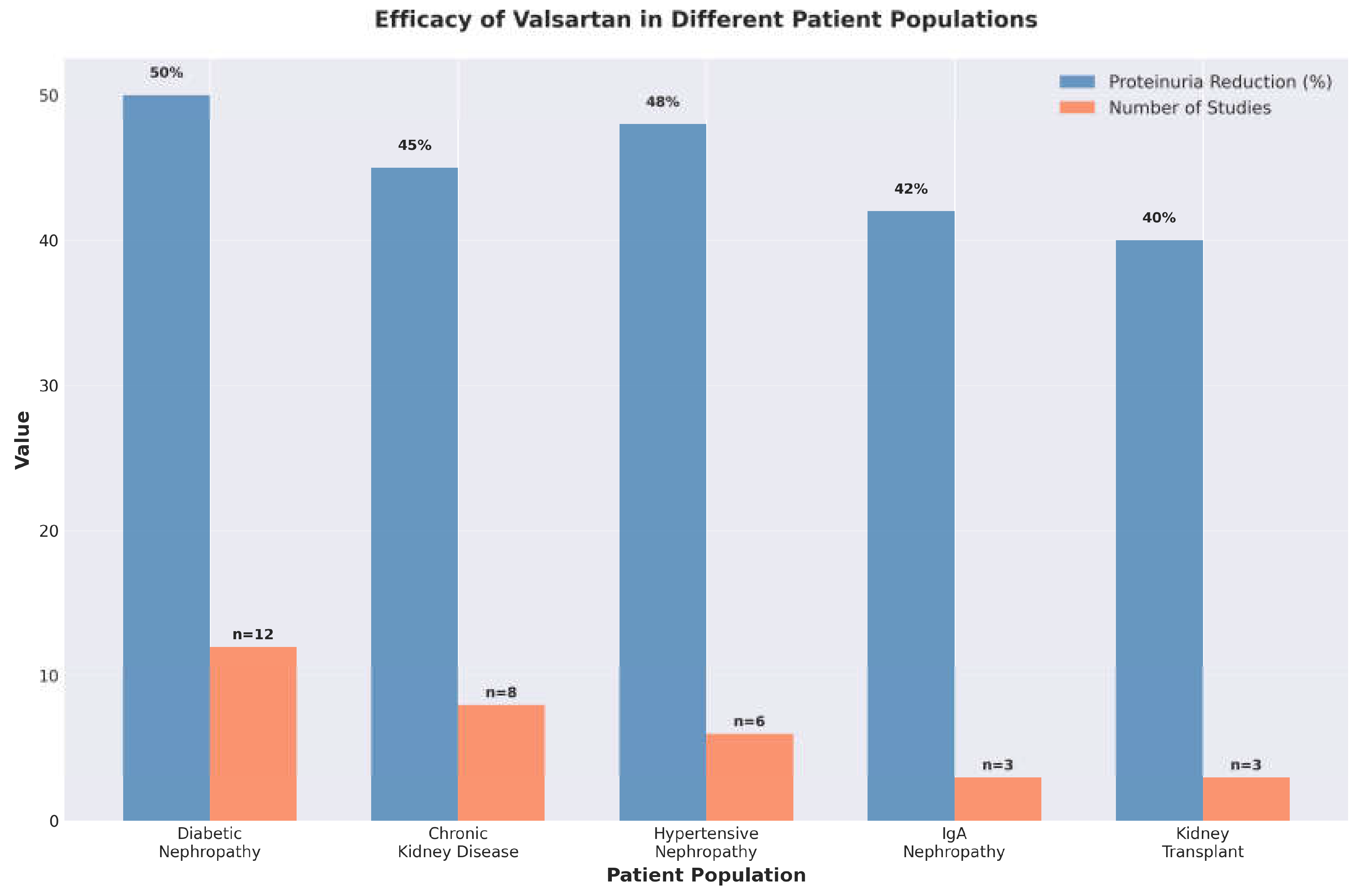
Figure 4.
Time course of proteinuria reduction with valsartan at different doses. Maximum therapeutic effect is typically achieved by 24 weeks, with higher doses producing more rapid and pronounced effects.
Figure 4.
Time course of proteinuria reduction with valsartan at different doses. Maximum therapeutic effect is typically achieved by 24 weeks, with higher doses producing more rapid and pronounced effects.
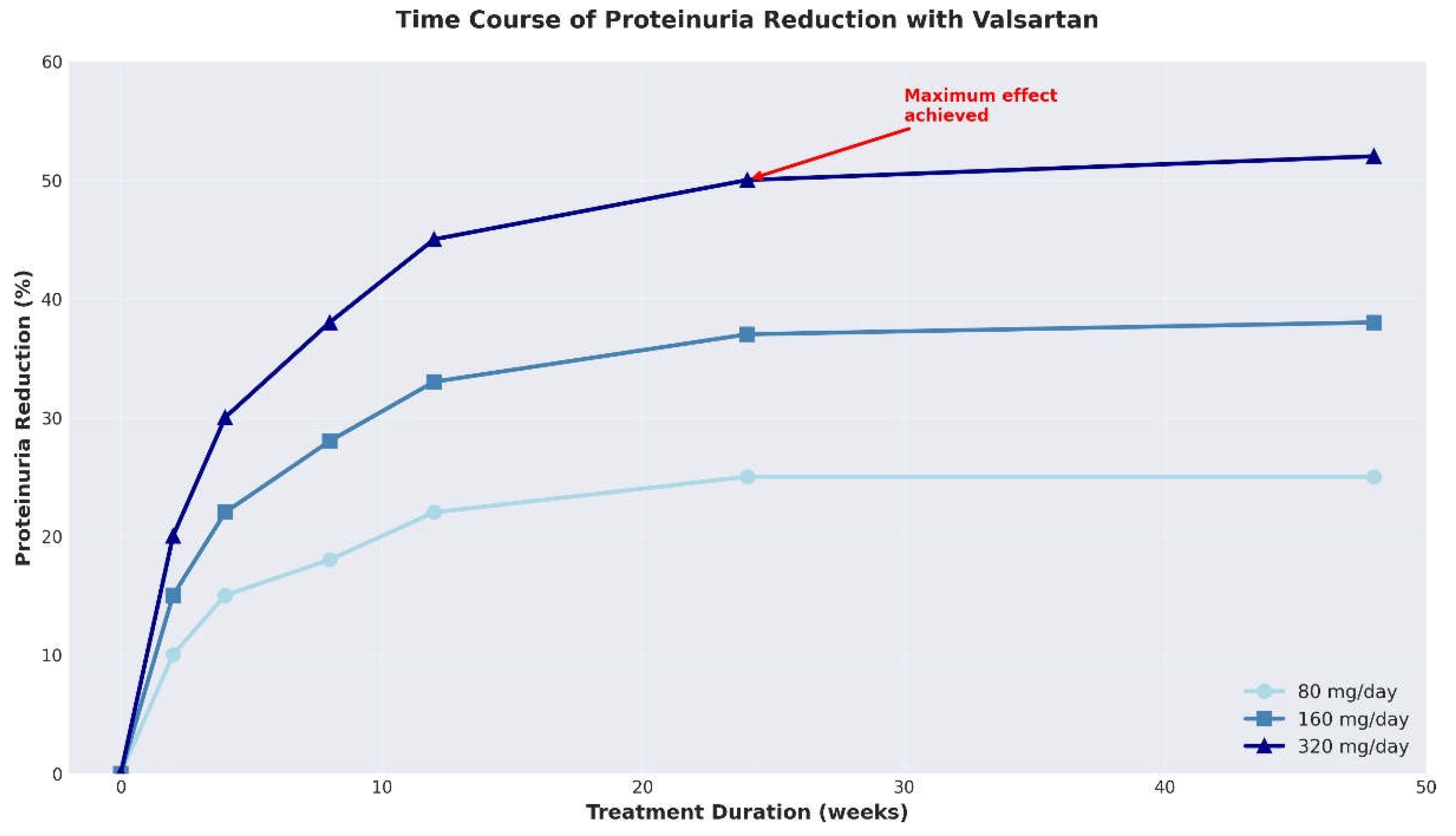
Figure 5.
Adverse effect profile comparing valsartan with ACE inhibitors. Valsartan shows a significantly lower incidence of cough (2% vs. 15%), making it an important alternative for patients intolerant to ACE inhibitors.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



