Submitted:
19 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Hiatal hernia is a complex pathology, associated with gastroesophageal reflux disease, and whose management involves complex surgical treatment. Knowing the role of gastropexy in reducing postoperative recurrences, the current study aimed to highlight the intraoperative advantages and results of this surgical technique. Our study includes 29 patients, aged between 34 to 84 years. Regarding the mechanism of occurrence, two thirds of the patients presented with mixed hiatal hernias, 31.03% with sliding hiatal hernias and 3.45% with paraesophageal hiatal hernias. The hernia size played a decisive role in the choice of surgical procedure, for large hernias (with a diameter of over 7 cm) the Nissen procedure associated with gastropexy was preferred.For hernias with a diameter of less than 7 cm, the Nissen procedure associated with hernia orifice repair was performed. For hernias between 5 and 6 cm, gastropexy was also performed. The association of gastropexy does not increase hospitalization costs, but in the long term it has the advantage of reducing relapse.
Keywords:
hiatal hernia
; gastropexy
; minimally invasive repair
Introduction
The management of hiatal hernias, particularly para esophageal hernias, poses significant challenges, necessitating precise and often complex surgical interventions. Hiatal hernias occur when a portion of the stomach protrudes through the esophageal hiatus into the thoracic cavity, commonly leading to gastroesophageal reflux disease (GERD), dysphagia, and, in severe cases, gastric volvulus or obstruction (1; 2). Among various surgical approaches, gastropexy has emerged as a crucial technique for enhancing surgical repair outcomes, particularly in large or complicated hernias (3; 4).
The various types of hiatal hernias—types I to IV—differ in their anatomical characteristics and associated complications. Types III and IV are more prone to severe complications, which often necessitate surgical intervention to prevent potentially life-threatening scenarios (2; 5). The role of gastropexy in preventing recurrence and facilitating a more favorable recovery trajectory has garnered attention in recent research, emphasizing its importance as part of the surgical approach to managing hiatal hernias (3; 6).
Hiatal hernias are characterized by the abnormal displacement of stomach contents into the thoracic cavity, predominantly due to a weakening of the diaphragm and surrounding musculature. This condition is often closely associated with GERD, which can manifest as heartburn, regurgitation, and dysphagia (1; 7). In symptomatic cases, especially where complications arise, surgical intervention is often deemed necessary. Laparoscopic hiatal hernia repair is currently recognized as the gold standard due to its minimally invasive nature, which typically results in reduced postoperative pain and quicker recovery times compared to traditional open surgeries (8; 9).
The standard procedure for laparoscopic repair generally involves closing the hiatal defect, often accompanied by an antireflux procedure such as Nissen fundoplication (10). However, the effectiveness of these repairs can be significantly compromised if the stomach is not adequately secured postoperatively, leading to recurrence. This realization has highlighted the relevance of gastropexy, which involves surgically securing the stomach to the abdominal wall, thus maintaining its proper anatomical position and mitigating the risk of herniation .
Gastropexy presents a particular advantage for elderly patients or those with significant comorbidities who may present greater risks during extensive surgical maneuvers (6). By securing the stomach post-repair, gastropexy can contribute to reduced complications and enhanced recovery profiles for these patients (3; 4). Evidence increasingly indicates that employing anterior gastropexy significantly improves outcomes for high-risk patients, particularly in preventing the recurrence of large hiatal hernias (4).
Material and Methods
A retrospective observational study was conducted at a tertiary referral center for upper gastrointestinal surgery. All consecutive patients who underwent elective minimally invasive hiatal hernia repair between January 2019 and December 2023 were evaluated. The study was designed to assess the role of gastropexy as an adjunctive procedure in laparoscopic hiatal hernia repair, with particular emphasis on early recurrence and postoperative symptom persistence.
The study was conducted in accordance with the Declaration of Helsinki and institutional ethical standards. Due to the retrospective and non-interventional nature of the study, formal ethical committee approval was waived.
Patient Selection
Inclusion criteria:
- age ≥ 18 years
- symptomatic hiatal hernia confirmed by upper gastrointestinal endoscopy and/or computed tomography
- elective laparoscopic hiatal hernia repair
- complete perioperative and follow-up data
Exclusion criteria:
- previous esophageal or gastric surgery
- emergency procedures
- concomitant bariatric surgery
- follow-up shorter than six months
Data Collection
Clinical data were extracted from electronic medical records and operative reports. The following variables were analyzed:
- demographic data (age, sex)
- body mass index (BMI)
- comorbidities (obesity, diabetes mellitus, cardiovascular and pulmonary disease)
- duration and type of symptoms (heartburn, regurgitation, dysphagia, chest pain)
- type of hiatal hernia (sliding, mixed, paraesophageal)
- hiatal defect size measured intraoperatively (maximum transverse diameter)
- surgical technique employed
- operative time
- length of postoperative hospital stay
- postoperative complications
- early hernia recurrence
Surgical Technique
All procedures were performed laparoscopically by experienced upper gastrointestinal surgeons. After reduction of the hernia sac and mobilization of the distal esophagus, posterior crural closure was performed using non-absorbable sutures. A 360° Nissen fundoplication was completed in all cases.
Gastropexy was selectively performed based on intraoperative assessment, particularly in patients presenting with:
- hiatal defects ≥ 5 cm
- significant intrathoracic stomach migration
- esophageal shortening or increased tension at the hiatal repair
Anterior gastropexy consisted of fixation of the gastric fundus to the anterior abdominal wall using non-absorbable sutures, aiming to limit postoperative axial migration of the stomach and reduce tension on the hiatal closure.
Outcomes
The primary outcome was early hiatal hernia recurrence, defined as radiological or symptomatic evidence of herniation within six months postoperatively.
Secondary outcomes included:
- persistence of postoperative dysphagia
- operative time
- length of hospital stays
- perioperative complications
Statistical Analysis
Statistical analysis was performed using SPSS software. Continuous variables were expressed as mean ± standard deviation or median (range), depending on distribution. Comparisons between groups were performed using Student’s t-test or Mann–Whitney U test for continuous variables and chi-square or Fisher’s exact test for categorical variables.
Receiver operating characteristic (ROC) curve analysis was used to assess the predictive value of hiatal hernia size for persistent dysphagia. A p-value < 0.05 was considered statistically significant.
Results
Patient Demographics
A total of 29 patients were included in the analysis, with ages ranging from 34 to 84 years and a median age of 68 years. Female patients predominated (75.9%, n = 22), resulting in a female-to-male ratio of approximately 3:1. Half of the study population consisted of elderly patients (>68 years), reflecting the known age-related prevalence of hiatal hernia.
Figure 1.
age histogram.
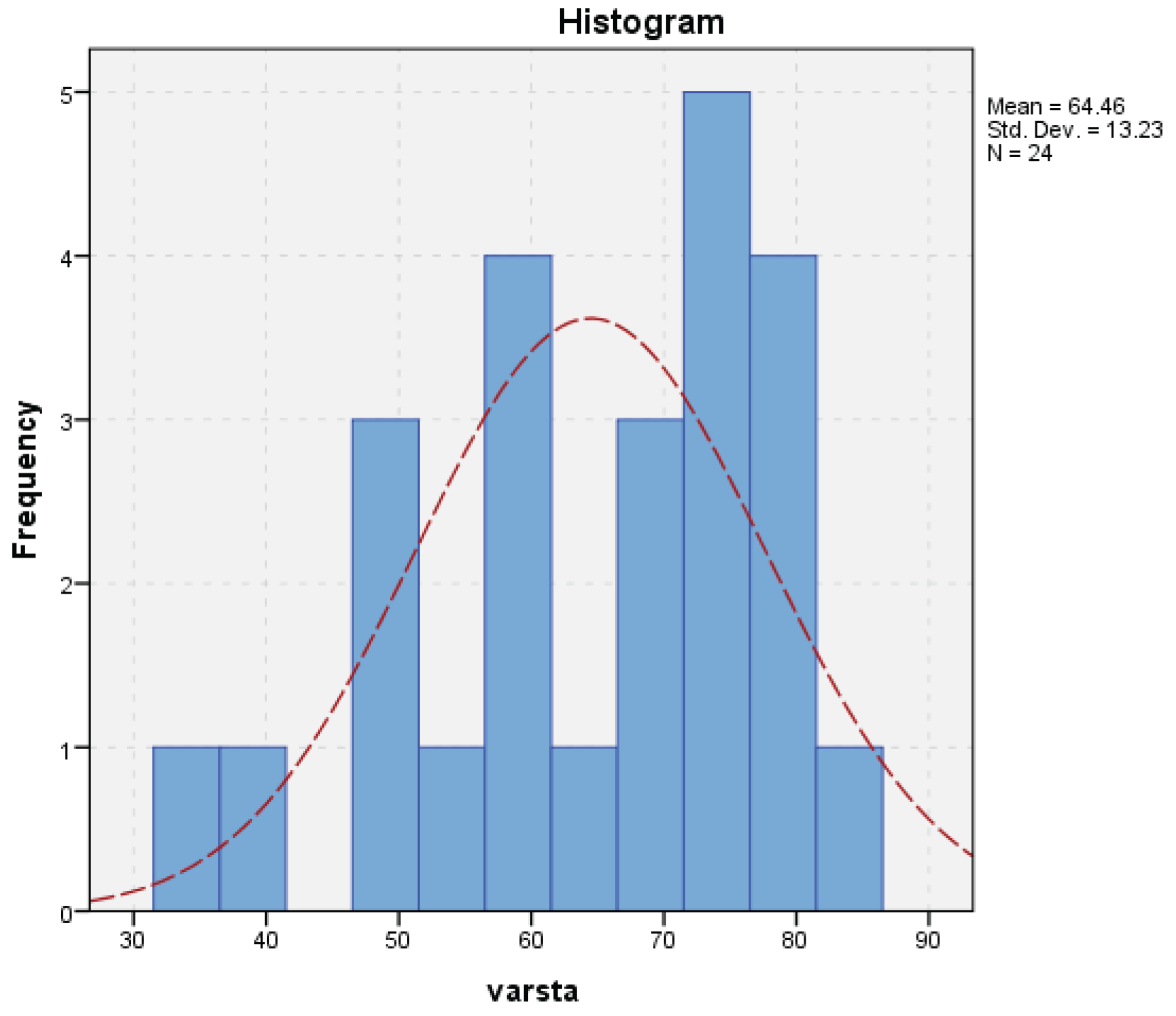
Gender-based analysis demonstrated a lower mean age among female patients compared to males, however, no statistically significant differences were observed regarding symptom duration or timing of surgical intervention between genders.

| Gender | Mean | N | Std. dev. | Median | Min | Max |
| F | 62.79 | 22 | 11.98 | 64 | 34 | 79 |
| M | 70.80 | 7 | 17.22 | 77 | 41 | 84 |
| Total | 64.46 | 29 | 13.23 | 68 | 34 | 84 |
This difference is not due to women presenting to the doctor earlier, but to the fact that this pathology occurs in men at an older age. This hypothesis is supported by the data in Table 2, which highlights the fact that there are no differences between women and men in terms of the duration between the onset of symptoms and the time of surgery.
Table 2.
gender distribution versus duration between symptom onset and surgery.
| Gender | Mean (onset of simpt) |
N | Std. dev. | Median | Min | Max |
|---|---|---|---|---|---|---|
| F | 9.55 | 22 | 3.113 | 10 | 4 | 15 |
| M | 11.50 | 7 | 4.087 | 10 | 8 | 18 |
| Total | 9.96 | 29 | 3.361 | 10 | 4 | 18 |
A majority of the individuals within this cohort exhibited a prolonged history of gastroesophageal reflux disease (GERD), with symptom durations ranging from 5 to 12 years, reflecting significant chronicity. The prevalent comorbidities included obesity (32% prevalence), diabetes (21%), cardiovascular diseases (28%), and pulmonary complications (18%). These comorbid factors are essential considerations, as they may profoundly impact surgical outcomes, as Almutairi et col and Arcerito et col noted (7; 11).
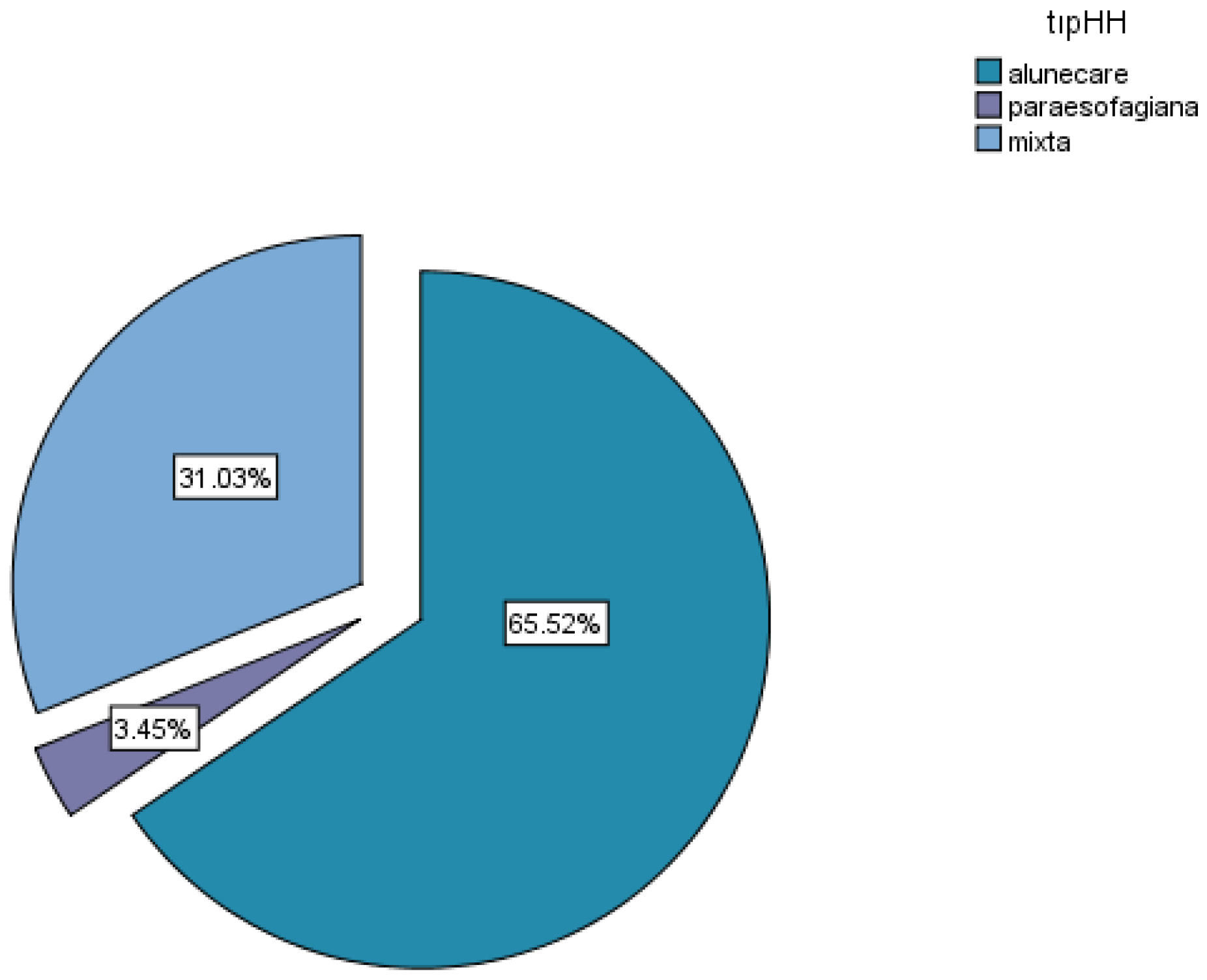
Regarding the mechanism of occurrence, two thirds of the patients presented with mixed hiatal hernias, 31.03% with sliding hiatal hernias and 3.45% with paraesophageal hiatal hernias (Fig2).
Figure 2.
types of hiatal hernias.
Hiatal hernia represents a widespread clinical condition that frequently necessitates surgical intervention. The dimensions of the hiatal defect can carry substantial clinical implications, influencing not just patient characteristics but also the severity of symptoms, the complexity of surgical procedures, and the outcomes post-surgery. This study aims to rigorously explore the interrelations between the size of the hiatal defect and a variety of factors, including patient demographic variables, comprehensive histories of gastroesophageal reflux disease (GERD), durations of symptoms, surgical time, length of hospitalization, and the utilization of surgical techniques.
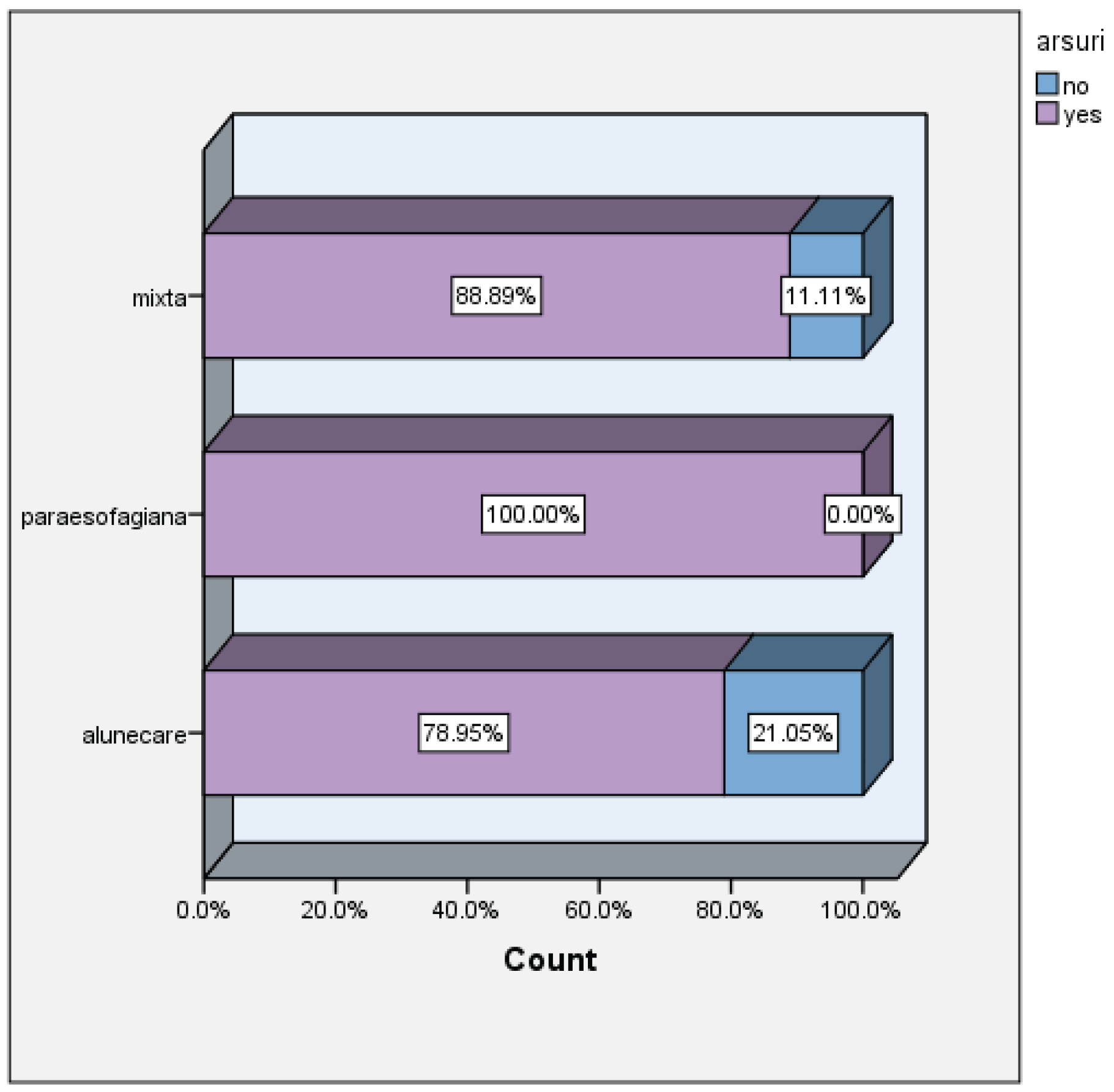
Heartburn was present in all patients with paraesophageal hiatal hernia, in 88.89% of patients with mixed hiatal hernia and in 78.95 of patients with sliding hernia, this being the predominant symptom.
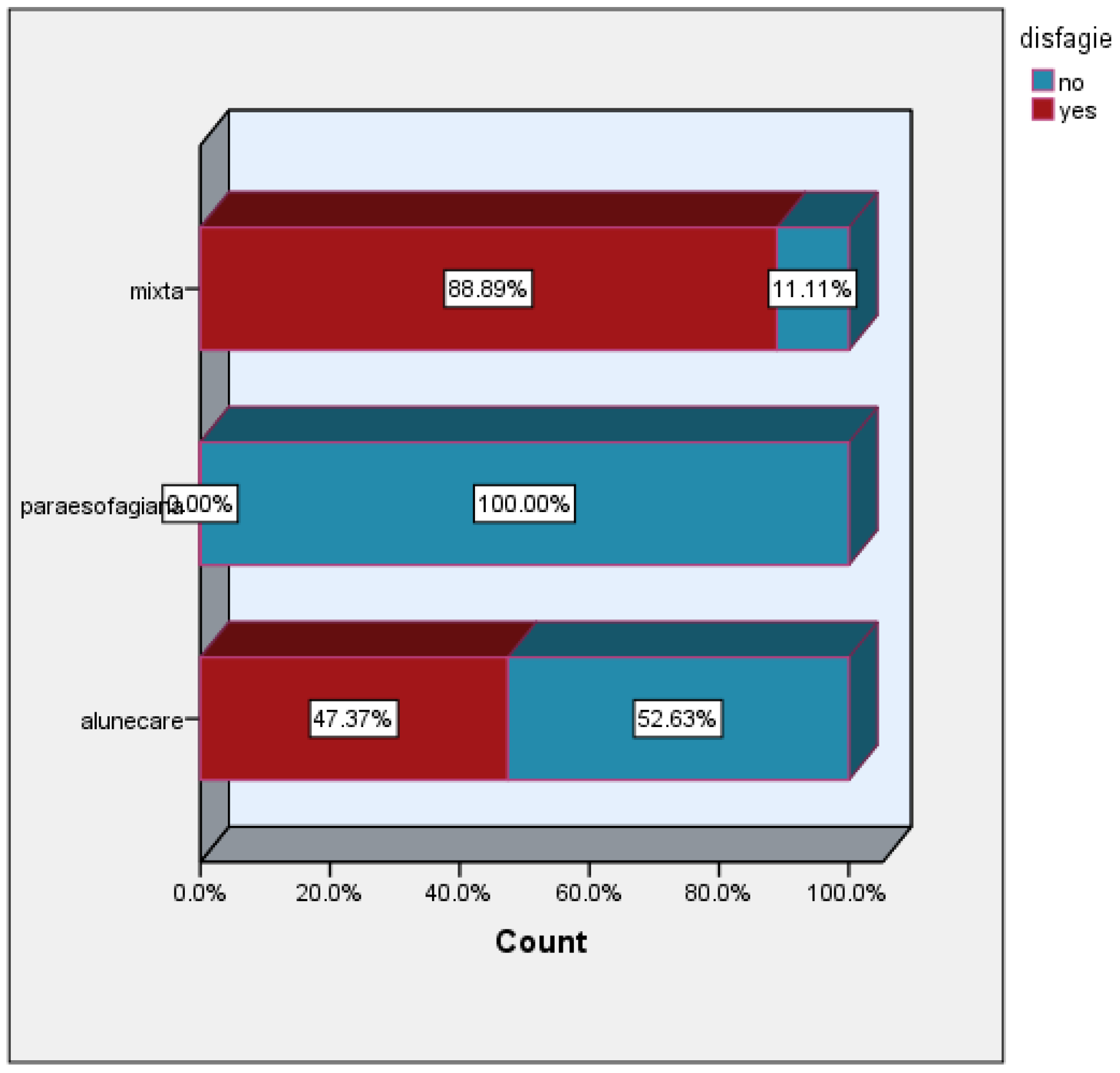
The incidence of dysphagia was 88.89% in the group of patients with mixed hiatal hernias, and 47.37% in the group of patients with sliding hiatal hernias. This symptom was absent in the group of patients with paraesophageal hiatal hernias.
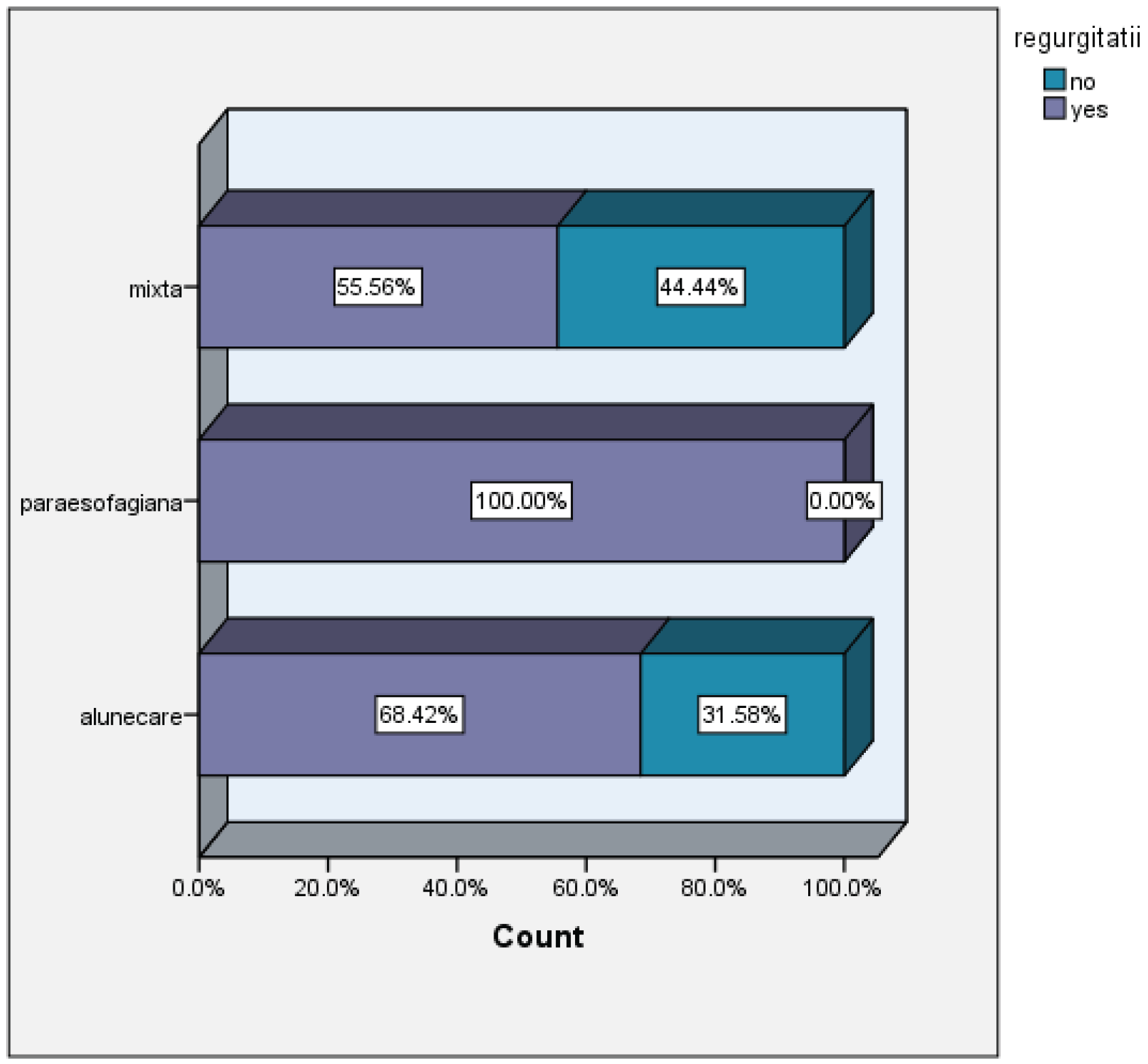
The incidence of regurgitation was approximately equivalent in the group of patients with mixed and sliding hiatal hernias (55.56%, 68.42%, respectively), unlike the group of patients with paraesophageal hernia, where all presented this symptom.
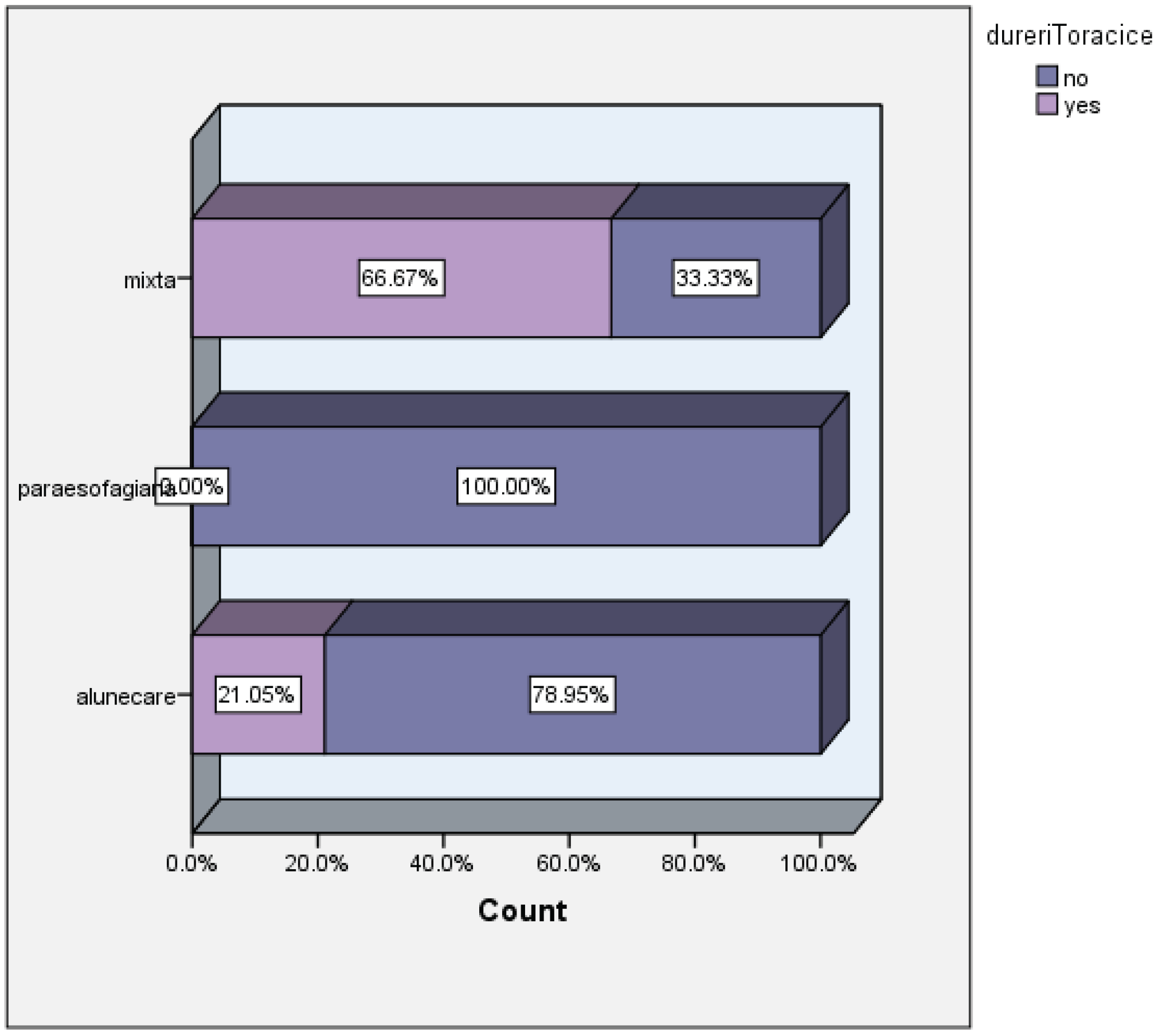
Two-thirds of patients with mixed hiatal hernias experienced chest pain, which was 3 times more than in the group of patients with sliding hernias.
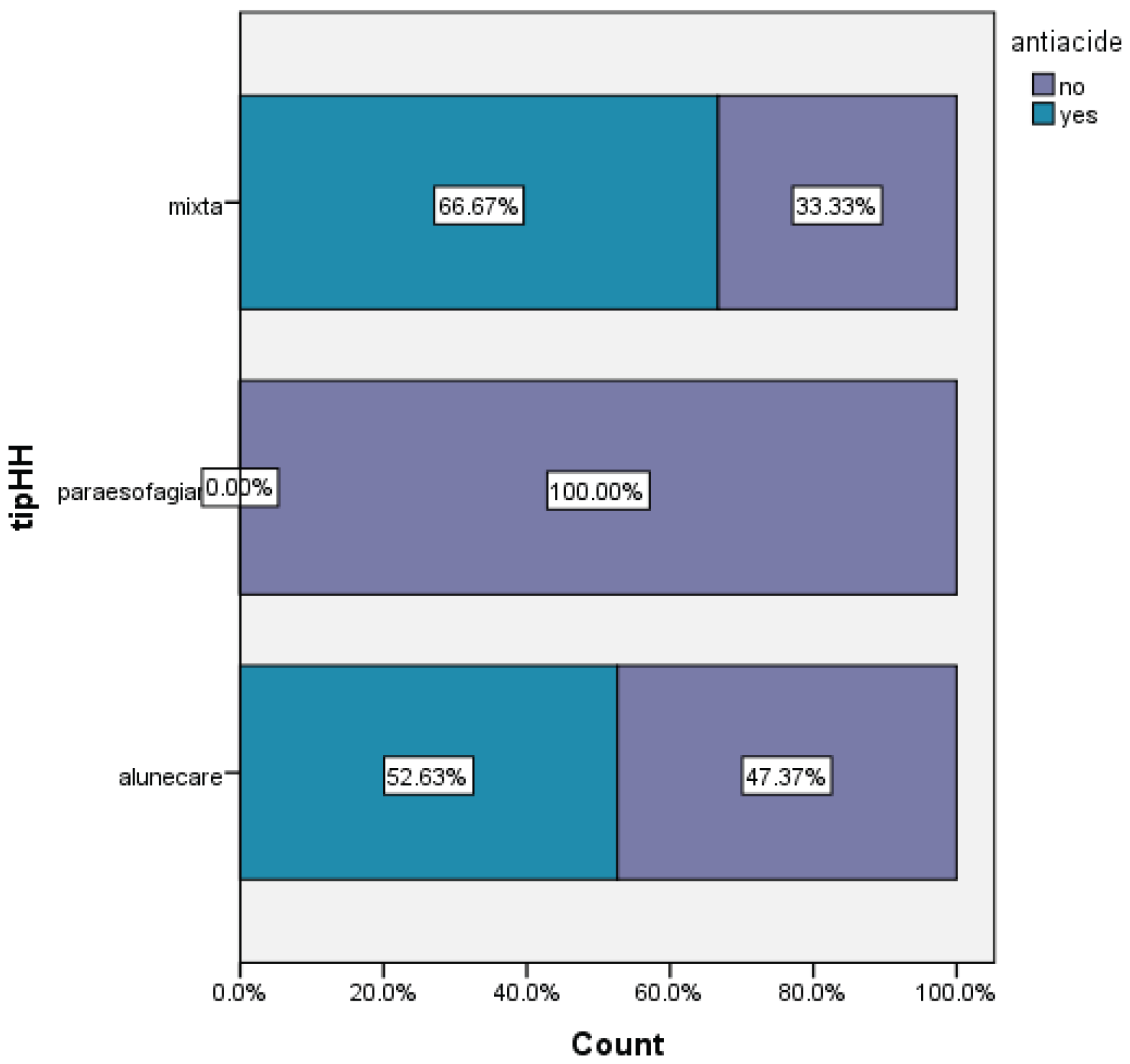
Preoperative treatment versus types of hiatal hernia
Two-thirds of patients with mixed hiatal hernias, respectively 52.63% of patients with sliding hiatal hernias, required treatment with antacids.
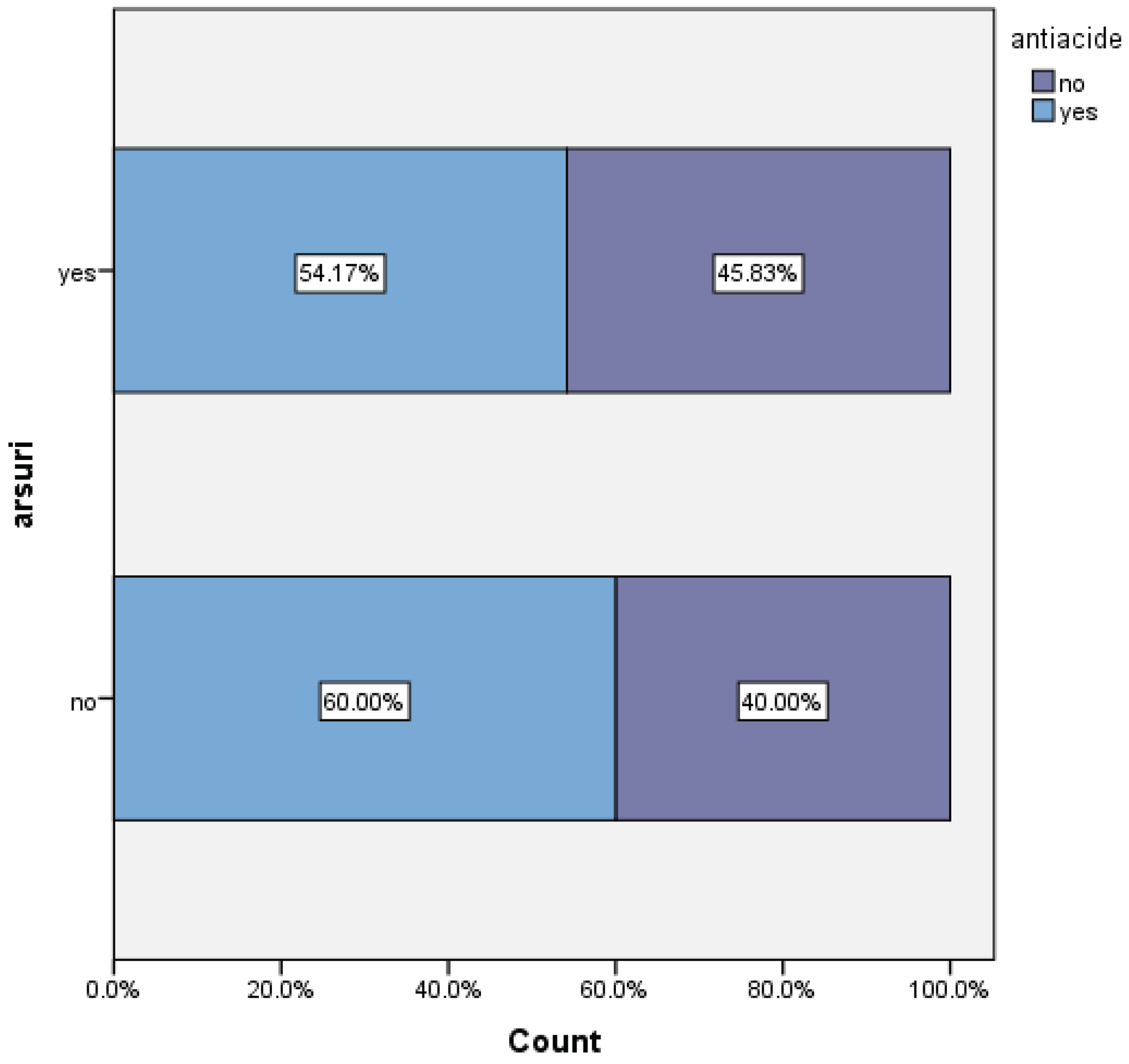
60% of patients who did not experience heartburn received antacid treatment, which may suggest that for these patients, the treatment was effective in controlling symptoms. Among patients with persistent heartburn, only 54.17% continued antacid therapy.
Hernia size versus presence of symptoms
No statistical correlations were found between hernia size and the presence of retrosternal heartburn, regurgitation, or chest pain.
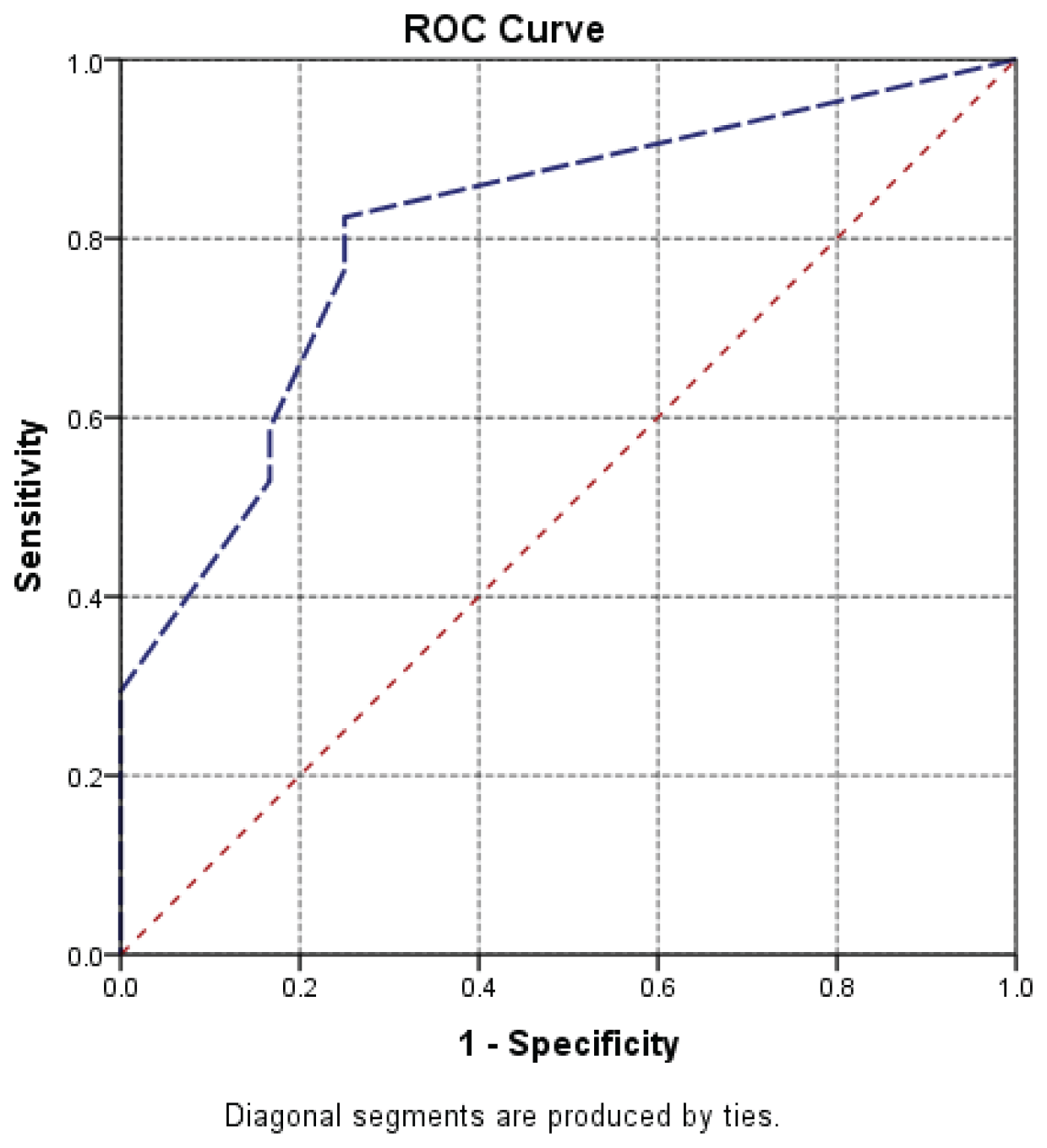
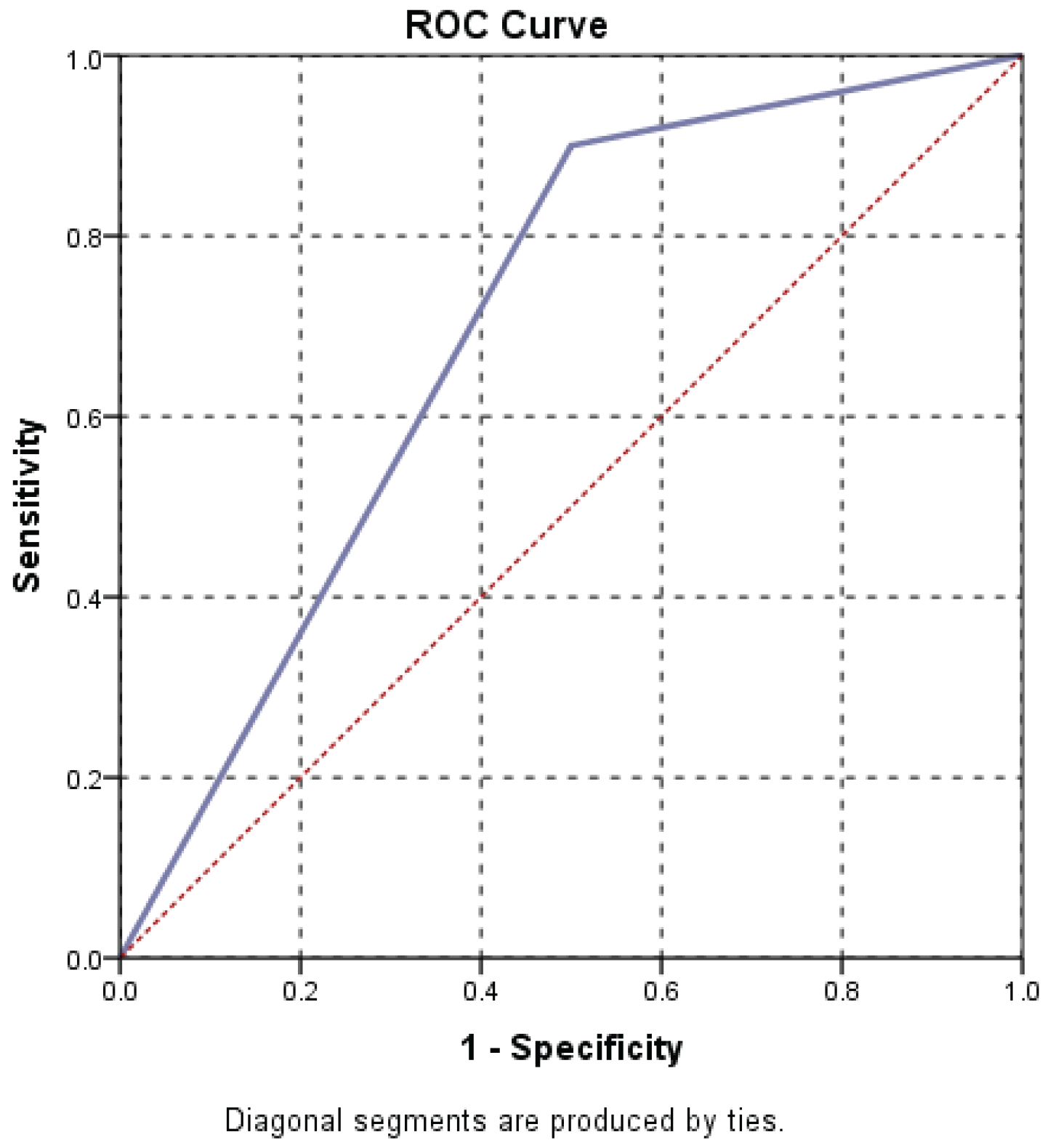
Statistical analysis identified a strong statistical correlation between hiatal hernia size and persistence of dysphagia ( p=0.004)
| Size of hiatal hernia versus dysphagia | |||||||
| Dysphagia | Mean | N | Std dev | Min | Max | Median | P value |
| No | 5.417 | 12 | .7930 | 5 | 7 | 5 | 0.004 |
| Yes | 6.853 | 17 | 1.4226 | 5 | 9 | 7 | |
| Total | 6.259 | 29 | 1.3863 | 5 | 9 | 6 | |
| F=9.970 | |||||||
Also, the analysis of the ROC curve and AUC= 809 indicates a high predictive power of hernia size on the persistence of dysphagia and lack of response to treatment.
Hernia size and choice of surgical intervention
Statistical analysis revealed a close correlation between the surgical procedure and the hernia size, with a p=0.005
As can be seen in the image below, the hernia size played a decisive role in the choice of surgical procedure, for large hernias (with a diameter of over 7 cm) the Nissen procedure associated with gastropexy was preferred.
For hernias with a diameter of less than 7 cm, the Nissen procedure associated with hernia orifice repair was performed. For hernias between 5 and 6 cm, gastropexy was also performed.
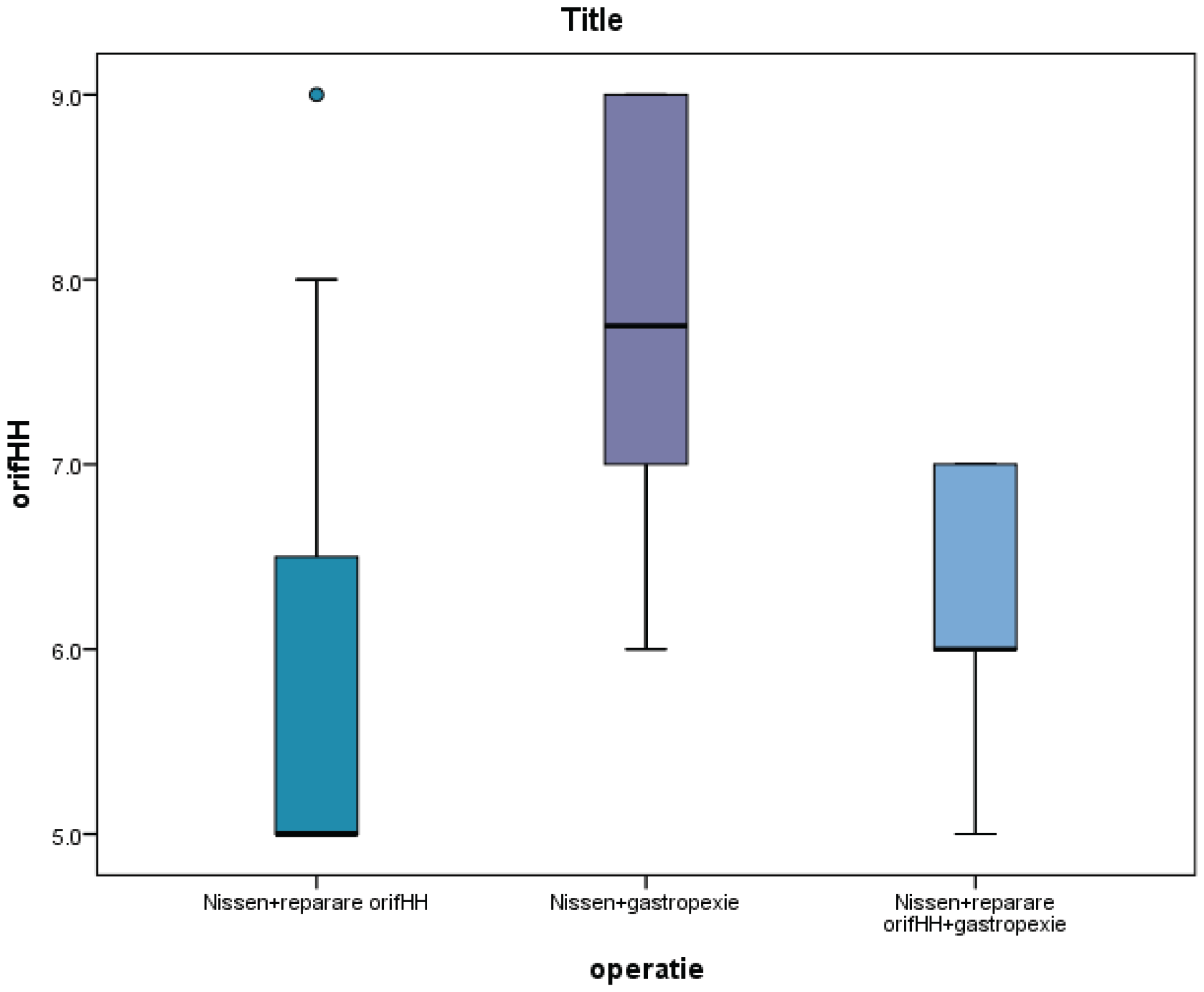
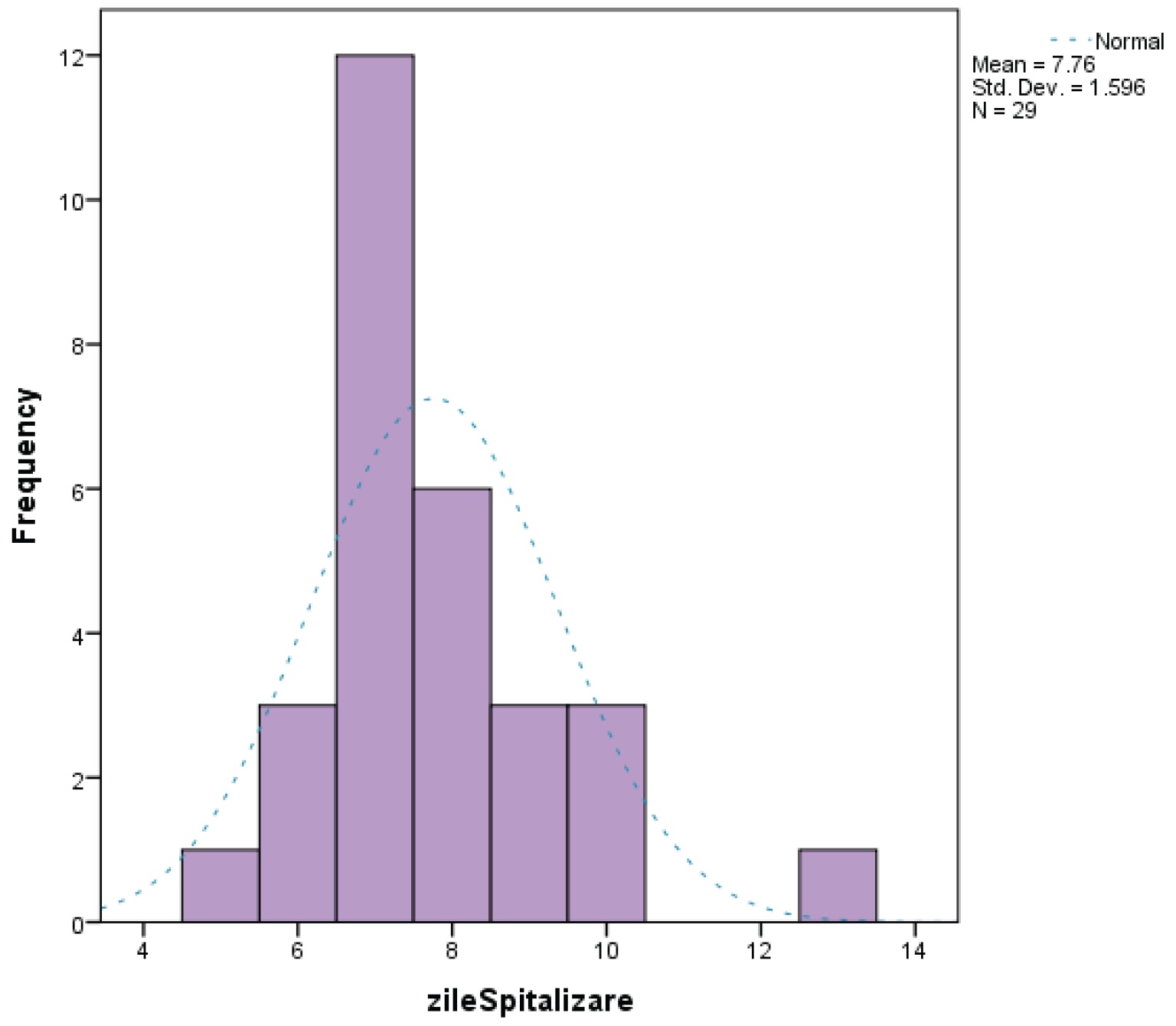
The choice of surgical procedure did not influence either the duration of the operation or the number of days of hospitalization, with no statistical associations between these variables. The duration of hospitalization ranged from 5 to 13 days, with a median of 7 days.
In these conditions, it is preferable to use gastropexy, considering that there is no significant increase in intraoperative time, nor in the number of days of hospitalization. The association of gastropexy does not increase hospitalization costs, but in the long term it has the advantage of reducing relapse.
The influence of obesity in study group
The patients' BMI ranged between 22.96 and 36.79, with a median of 27.49.
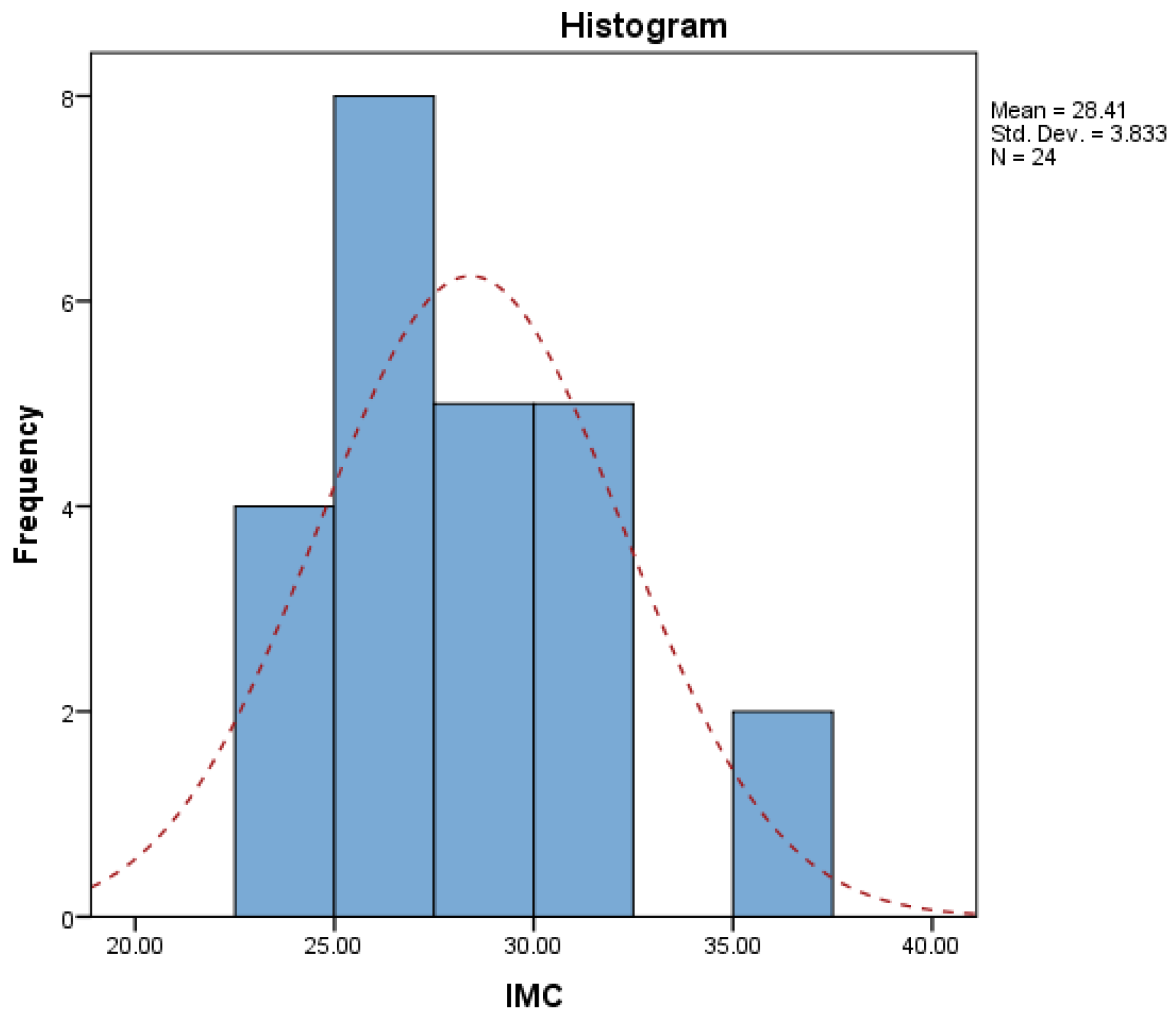
No statistically significant correlations were identified between BMI and hiatal hernia size.
ROC curve analysis revealed that a BMI>=25 has a high predictive value on the occurrence and persistence of retrosternal heartburn, with an AUC=700.
BMI does not influence and does not show statistical correlations with other symptoms.
Intraoperative section and surgical technique details:
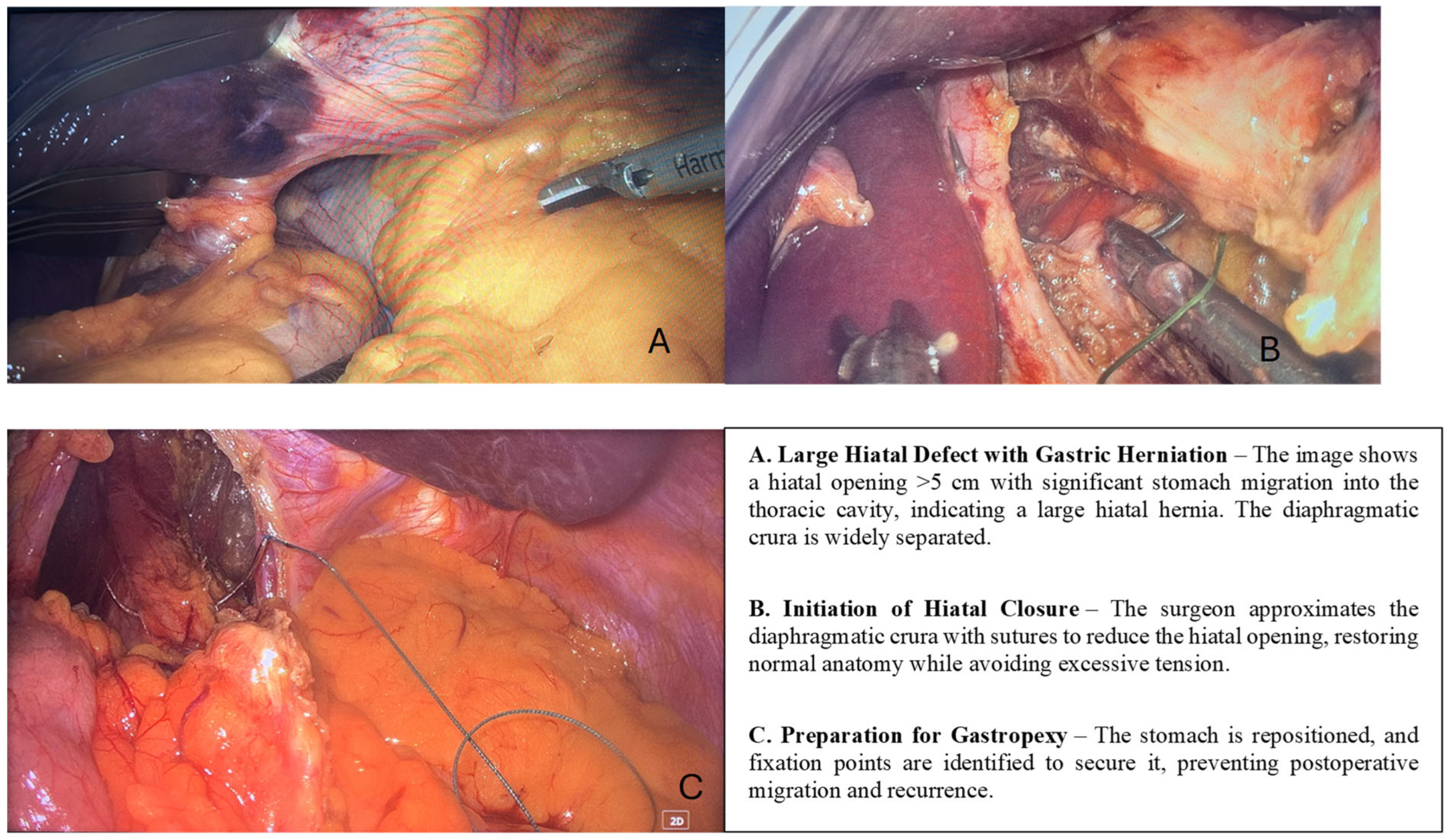
Surgical Techniques and Outcomes: All patients included in this robust study underwent laparoscopic hiatal hernia repair, with each individual receiving the widely recognized Nissen fundoplication procedure, which remains a standard technique for effectively addressing hiatal hernias. Within this carefully selected cohort, selective gastropexy was performed in approximately 40% of cases, specifically targeting patients with additional complications such as gastric volvulus, considerable intrathoracic stomach migration, or significant esophageal shortening.
Discussions
The Role of Gastropexy in Recurrence Prevention
The treatment of hiatal hernias was and remains a very controversial topic. There is important heterogeneity in studies and also in technique and technology employed. Although the first surgery was described in 1919 by Soresi (12), each new approach has been view with extreme enthusiasm only for most not to withstand scrutiny of time.
Traditional surgical methods have raised concerns regarding morbidity rates, with laparoscopic techniques demonstrating significantly lower complication rates compared to open repair strategies (13; 14). The lower complication rate comes in with a very high recurrence rate up to 50%. (15). A low percentage, 0.01 to 7% of these patients require revisional surgery but they exhibit a worse quality of life and increased symptoms of heartburn, early satiety, gas bloat, dysphagia (16; 17).
There are still a lot of controversies regarding the adequate surgical treatment of hiatal hernial, especially in regard to which procedure has the lowest recurrence rate as compared to crural sutures alone. Multiple concomitant procedures have been described, all very enthusiastically advocated at first, but without long term assessment. Such is the example of using tension free polyurethane mesh in addition to crural suture (18). A randomized clinical study aimed to asses long term (13 years) anatomical and functional outcomes in 103 patients, from the original 158 enrolled in the double blind study. Radiologically there was no significant difference between recurrence rates, 38% for mesh and 31% for suture alone. Worth mentioning are the mechanical complications. There were also significant higher dysphagia scores for solids in the mesh group. Other complications are mesh erosion, dense fibrosis leading to dysphagia, chronic pain or gastroparesis (19).
The next logical approach as the use of biosynthetic meshes alongside crural suture. Available studies have shown significant improvement and quality of life scores, despite extremely variable recurrence rates, varying from 0.9 to 25%. This can be attributed to the heterogeneity of the studies (20).
Another therapeutical approach which is currently being used in the treatment of Gastro esophageal reflux is the concomitant fundoplication. There is an absence of strong data to support the long term effects, although it is under the assumption that it can prevent or treat the reflux while fixing the stomach below the diaphragm and thus preventing recurrence (21). Available data shows that fundoplication can prevent postoperative reflux and subsequent esophagitis, especially in patients in which there is an incompetence of the lower esophageal sphincter due to extensive hiatal dissection during hernia repair. Another controversial topic is the type of fundoplication. Most studies did a total fundoplication(Niessen or Niessen- Rosetti) and the latest guidelines recommend that partial fundoplication (Toupet of Dor ) should be reserved for cases with significant impaired esophageal mobility (22).
Gastropexy without the repair of the hiatal hernia was first described in 1955 by Boerema and Germs. The hernia sac was not or was minimally dissected, the stomach was reintroduced into the peritoneal cavity, and the esophagus and stomach was put under tension through gastropexy of the lesser sac to the right of the laparotomy incision with multiple sutures (23). This method, although at first with promising results, has been abandoned for years because of the high recurrence rates> this can be attributed to the lack of vital techniques such as crural suture or the reduction of the hernia sac (24).
Different types of gastropexy have been described such as posterior gastropexy ( in which the stomach is sutured to the diaphragmatic crura), t- fastner percutaneous gastropexy (a T-fastener is placed into the gastric lumen and secured externally. Once the external sutures are cut, the T-fastener is able to migrate through the gastrointestinal tract and be expelled naturally) or using a percutaneous endoscopic gastrostomy tube as an anterior gastropexy in emergency setting has been proposed (25; 26; 24).
One study aimed to asses the relevance and late results of laparoscopic hernia repair without prosthetic reinforcement concluded that a factor significally linked with recurrence was the absence of gastropexy(50% as compared to 10.8 in the group with gastropexy) (27). These results have been confirmed by multiple other studies in smaller and non-comparative studies (28; 29; 30). The anatomical hypothesis is that anchoring the stomach to the anterior wall will prevent reherniation and avoid organoaxial rotation with the risk of strangulation.
To add more to this already controversial topic, a recent study has shown no advantage of fundoplication as compared to gastropexy alone. Only difference was the median operation time(108 minutes for fundoplication compared to 59 minutes) but comparable results regarding perioperative and postoperative events, reflux control or reccurence (31).
Anterior gastropexy is very appealing through the fact that it is easily performed laparoscopically, very low complication rate and easily reproductible. This is reflected in our study in which there were no complication reported and also there was no difference in hospitalization time.
Incorporating gastropexy into standard hiatal hernia repair has been demonstrated to provide several significant advantages such as optimization of surgical outcomes in high-risk patients. Our analysis reveals that larger hiatal defects correlate with extended surgical times (+0.30 correlation) and lengthier hospital stays (+0.40 correlation), suggesting a more intricate operative course. Incorporating gastropexy can act as a stabilizing adjunct in situations where conventional fundoplication alone may not suffice to deliver long-term support.
Although there is an increasing body of evidence advocating gastropexy, further studies are necessary to clarify its role in surgical practice. Key areas for future research should include:
- 1.
- Comparative studies evaluating long-term recurrence rates with versus without gastropexy in cases involving large hiatal hernias. While existing retrospective data suggest potential benefits, randomized controlled trials would generate more definitive conclusions.
- 2.
- Investigation into alternative fixation techniques, such as mesh-reinforced repairs, alongside gastropexy to discover the most effective treatment strategy for large or recurrent hiatal hernias.
- 3.
- Exploration of the role of gastropexy in individuals exhibiting altered esophageal motility, including those diagnosed with achalasia or ineffective peristalsis, to determine if additional gastric fixation contributes to improved symptom management.
In light of our findings and the current body of literature, we propose the following recommendations regarding the application of gastropexy in laparoscopic hiatal hernia repair:
- 1.
- Surgeons should contemplate the use of gastropexy for patients with extensive hiatal defects (greater than 5 cm), particularly in cases involving mixed-type hernias or increased intra-abdominal pressure.
- 2.
- Gastropexy should be embraced as a preventive strategy to diminish the chances of recurrence, particularly when high tension at the hiatal level exists or stability following fundoplication is uncertain.
- 3.
- Timely surgical intervention in patients presenting with large hiatuses may help mitigate prolonged symptomology and reduce the risk of severe complications such as gastric volvulus.
- 4.
- A tailored approach should be adopted, with preoperative evaluations assessing the severity of GERD, esophageal motility, and anatomical risk factors guiding the decision to incorporate gastropexy.
The average duration of postoperative hospital stays among the patient cohort was approximately 8.2 days, a statistic that was notably influenced by many variables, including each patient's preoperative health status, comorbid conditions, and the complexity of the surgical procedure performed. Importantly, throughout the study, no major complications—such as the formation of fistulas or significant postoperative bleeding—were documented within the studied population. However, minor complications emerged, with transient dysphagia occurring in 15% of patients and gas bloat syndrome being observed in 10% of patients. Of utmost significance, there were no documented cases of early hernia recurrences in the subgroup undergoing gastropexy, which starkly contrasts with the non-gastropexy group. In that group, three patients, comprising 5.8% of the cohort, experienced hernia recurrences within a six-month postoperative follow-up period.
The integration of gastropexy into laparoscopic hiatal hernia repair marks a significant advancement in the surgical management of complex hiatal defects. Although its routine utilization remains a point of contention, growing evidence supports its efficacy in lowering recurrence rates, enhancing symptom management, and improving surgical outcomes. As the field progresses, continuous research and extended follow-up studies will be vital in refining its indications and establishing standardized guidelines for its application.
Conclusions
Gastropexy represents a valuable adjunct in laparoscopic hiatal hernia repair, particularly in patients with large or mixed-type hernias. Hiatal hernia size plays a central role in symptom persistence and surgical decision-making, and larger defects may benefit from additional gastric fixation to enhance anatomical stability.
The selective use of gastropexy does not increase perioperative morbidity and may reduce early recurrence by limiting postoperative gastric migration and tension at the hiatal repair. These findings support a tailored surgical approach based on anatomical risk factors rather than routine application of a single technique.
Prospective, randomized studies with longer follow-up are required to further define the role of gastropexy and establish standardized indications for its use in minimally invasive hiatal hernia repair.
Reference
1. Minimally-invasive approach to paraoesophageal hernia in high surgical-risk patients“ . ho and et al. 2014, Surgical
Practice.
2. Robotic Repair of a Paraesophageal Hernia After an Open Nissen Fundoplication“. Hammar and et al. 2024, Cureus .
3. Laparoscopic anterior gastropexy for type III/IV hiatal hernia in elderly patients“. Higashi and et al. 2017, Surgical Case Reports .
4. Large paraesophageal hernia in elderly patients: Two case reports of laparoscopic posterior cruroplasty and anterior gastropexy“. Moussa and et al. 2019, International Journal of Surgery Case Reports.
5. Does concomitant laparoscopic sleeve gastrectomy and hiatal hernia repair increase morbidity?“. dincer and dogan. 2018, Archives of Medical Science .
6. Post-operative giant hiatal hernia“. felix and et al. 2019, Medicine .
7. Laparoscopic Posterior Cruroplasty and Anterior Gastropexy for Type IV Hiatal Hernia Repair in an Elderly Patient: A Case Report and Review of the Literature“. almutairi and et al. (2023), Cureus.
8. Laparoscopic Repair of Large Hiatal Hernia Without Prosthetic Reinforcement: Late Results and Relevance of Anterior Gastropexy“. poncet and et al. (2010, Journal of Gastrointestinal Surgery .
9. Comparing Open and Laparoscopic Techniques in Hiatal Hernia Repair“ . rogers and et al. (2021, JAMA Surgery .
10. Laparoscopic Approaches to Giant Hiatal Hernias“ . ceccareli and et al. (2019)., World Journal of Surgery .
11. Robotic Fundoplication for Large Paraesophageal Hiatal Hernias“ . arcerito and et al. (2020), Jsls journal of the society of laparoscopic & robotic surgeons.
12. The history of hiatal hernia surgery: from Bowditch to laparoscopy. Stylopoulos, N and rattner, D W. 1, s.l. : Ann Surg., 2005, Vol. 241.
13. Laparoscopic Approaches to Giant Hiatal Hernias. Ceccarelli and et al. s.l. : World Journal of surgery, 2019.
14. Sliding and Paraesophageal Hiatal Hernias are Distinct Diseasez: Surgeons are Responsible for Delineating the Differences. Herbella and et al. s.l. : Foregut the journal of the american foregut society, 2024.
15. Biologic prosthesis to prevent recurrence after laparoscopic paraesophageal hernia repair:long-term follow-up from a multicenter, prospective, randomized trial. Oelschlager, B K, et al. 4, s.l. : J Am Coll Surg, 2011, Vol. 213.
16. outcome for asymptomatic recurrence following laaproscopic repair of very large hiatus hernia. Wang, Z, et al. 8, s.l. : J Gastrointest Surd, 2015, Vol. 19.
17. Do recurrences after paraesophageal hernia repair matter?: ten-year follow-up after laaproscopic repair. White, B C, et al. 4, s.l. : Surg Endosc, 2008, Vol. 22.
18. Mesh in laparoscopic large hiatal hernia repair: a systematic review of the literature. Furnee, E and Hazebroek, E. s.l. : Surg Endosc, 2013, Vol. 27.
19. Mesh complications after prosthetic reinforcement of hiatal closure: a 28-case series. Stadlhuber, Rudolf, J and et al. s.l. : Surgical Endoscopy, 2009, Vol. 23.
20. Hiatal hernia repair with biosynthetic mesh reinforcement: a qualitative systematic review. Lima, D L and et al. 10, s.l. : Surg Endosc, 2023, Vol. 37.
21. Management of Paraesophageal Hernia- Still a Controversial Topic. Schlottmann, F, et al. 3, s.l. : JAMA Surg, 2025, Vol. 160.
22. Management of paraesophageal hernia review of clinical studies: timing to surgery, mesh use, fundoplication, gastropexy and other controversies. Dreifuss, N H, et al. 8, s.l. : Dis Esophagus, 2020, Vol. 33.
23. Gastropexia anterior geniculata wegen Hiatusbruch des Zwerchfells [Geniculate anterior gastropexy in hiatal hernia of the diafragm]. Boerema, I and Germs, R. 39, s.l. : Zentralbl Chir, 1955, Vol. 80.
24. The role of gastropexy in paraesophageal hernia repair: A scoping review of current evidence. kamran, H, et al. 1, s.l. : surgeon, 2025, Vol. 23.
25. Laparoscopic Nissen fundoplication combined with posterior gastropexy in surgical treatment of GERD. Tsimogiannis, E C, et al. 6, s.l. : Surg Endosc, 2010, Vol. 24.
26. Subcutaneous T-fastener gastropexy: a new technique. Black, M T, Hung, C A and Loh, C. 5, s.l. : AJR Am J Roentgenol, 2013, Vol. 200.
27. Laparoscopic repair of large hiatal hernia without prosthetic reinforcement: late results and relevance of anterior gastropexy. Ponget, G, et al. 12, s.l. : Gastrointest Surg, 2010, Vol. 14.
28. 360 degrees laparoscopic fundoplication with tension-free hiatoplasty in the treatment of symptomatic gastroesophageal reflux disease. Basso, N, et al. 2, s.l. : Surg Endosc, 2000, Vol. 14.
29. Laparoscopic paraesophageal hernia repair with mesh. Edelman, D S. 1, s.l. : Surg Laparosc Endosc, 1995, Vol. 5.
30. Mid term analysis of safety and quality of life after the laaproscopic repair of paraesophageal hiatal hernia. Targarona, E M, et al. 7, s.l. : Surg Endosc, 2004, Vol. 18.
31. No advantage of fundoplication in paraesophageal hernia repair: a retrospective multicenter study. Osterballe, L, et al. 3, s.l. : Dis Esophagus, 2025, Vol. 38.
32. Chronic Gastric Volvulus with Laparoscopic Gastropexy after Endoscopic Reduction: A Case Report“ . lee and et al. (2015), Journal of gastric cancer .
33. Upside-down stomach in paraesophageal hernia: A case report“ . zhu and et al. (2023)., Medicine .
34. Sliding and Paraesophageal Hiatal Hernias are Distinct Diseases: Surgeons are Responsible for Delineating the Differences“ . herbella and et al. (2024)., Foregut the journal of the american foregut society .
35. From Silent to Severe: Gastric Perforation Causing Spontaneous Hydropneumothorax Secondary to a Large Hiatal Hernia“ . gaddameedi and et al. (2024, Cureus .
36. Management and Outcomes in Gastric Volvulus: A Tiered Approach“ . askari and et al. (2022), Digestive disease interventions .
37. The impact of frailty on outcomes of paraesophageal hernia repair“ . chimukangara and et al. (2016)., Journal of surgical research .
38. The Pathophysiology of Gastroesophageal Reflux Disease. mittal and balaban. 2019, The American Journal of Medicine, , pp. 130(9), 965-977.
39. The Evolution of Hiatal Hernia Repair: From Nissen Fundoplication to Laparoscopic Techniques. Patti, M. G., Allaix, M. E., & Fisichella, P. M. 2016, . World Journal of Surgery, , pp. 40(6), 1451-1458.
40. Laparoscopic Hiatal Hernia Repair: Current Status and Future Directions. . soper and warson. 2017, Annals of Surgery, , pp. 265(5), 888-897.
Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



