Submitted:
22 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Objectives: Despite the widespread use of the leuprorelin 3-month depot in central precocious puberty (CPP), its clinical efficacy and patient follow-up remain unexplored. This study aimed to compare the clinical indicators of the leuprorelin 3-month depot and triptorelin 1-month depot following treatment in a CPP cohort to understand the therapeutic effect of the former.Methods: A retrospective analysis was performed on 60 children diagnosed with progressive idiopathic CPP or precocious puberty who received at least 24 months of treatment at the hospital. The treatment involved leuprorelin 3-month depot for 18 participants, triptorelin 1-month depot for 16 participants, and a combination of both drugs for 26 participants. Anthropometric, biochemical, and bone age (BA) data were examined before treatment and every 12 months during treatment.Results: Before treatment, no statistical differences were noted in the baseline levels of sex hormones (oestradiol (E2), luteinising hormone (LH), and follicle-stimulating hormone (FSH)) among the triptorelin 1-month depot, leuprorelin 3-month depot, and combination therapy groups (P>0.05). However, the serum testosterone levels among participants were statistically significant (P < 0.05). After 1 and 2 years of treatment, no statistically significant differences were noted in the baseline levels of sex hormones (E2, LH, and FSH) among the three groups (P>0.05). At baseline, no statistical differences were found in BA, height, or weight among the groups (P>0.05). After 1 and 2 years of treatment, no statistically significant differences were observed in the growth rate, maturity, or BA growth rate of the participants in all three groups (P>0.05).Conclusions: The therapeutic effects of the triptorelin 1-month and leuprorelin 3-month depots were equivalent. Furthermore, treatment with leuprorelin 3-month depot is cost-effective compared with the other options . It reduces the number of injections administered to paediatric patients, the time spent on medical visits, and improves compliance, leading to greater acceptance among patients.
Keywords:
central precocious puberty
; therapeutic effect
; comparative research
; leuprorelin 3-month depot
; triptorelin 1-month depot
1. Introduction
Central precocious puberty (CPP) is characterised by significant early puberty in children. Typically, girls experience CPP before 8 years and boys before 9 years [1,2]. If left untreated, children with CPP may experience accelerated growth and early bone maturation, which may result in shorter adult stature. Children with CPP often encounter psychological and social difficulties owing to their early physical maturation [3]. Furthermore, a link exists between CPP and increased risks of certain health complications later in life, such as metabolic syndromes and reproductive health concerns [4,5,6]
Analogues of gonadotropin-releasing hormone (GnRH) are the primary treatment for CPP. These medications inhibit sex hormone production, thereby delaying further development [7,8]. Treatment with GnRH agonists (GnRHa) leads to pubertal sign regression or stabilisation, growth velocity reduction, and a decrease in bone maturation rate. The outcomes of cohorts composed of patients with CPP treated with 1-month GnRHa formulations have been widely reported. Recent reports have described CPP treatment with long-acting GnRHa [7,9,10,11]. The advantages of these compounds over a 1-month GnRHa treatment have been recognised, such as a reduced number of injections, which improves compliance and convenience. Ramos et al. analysed the treatment outcomes in 24 girls before and after leuprorelin therapy. Their research results indicated that long-term anthropometric, metabolic, and reproductive follow-ups of patients with CPP treated with long-acting GnRHas have revealed safe, effective, and good results. However, few follow-up studies exist on the efficacy of leuprorelin 3-month depot in China. Therefore, we conducted a 24-month follow-up study in 60 children with CPP, assessing the clinical efficacy of the leuprorelin 3-month depot based on serum hormone levels and clinical manifestations in patients using leuprorelin 3-month depot alone, triptorelin 1-month depot alone, and a combination of the two drugs.
2. Materials and Methods
2.1. Patients and Treatment
We recruited 60 children (52 females, 8 males) diagnosed with CPP and treated at Longhua Branch of Shenzhen People’s Hospital Hospital between January 1, 2019 and December 31, 2022. Of these children, 16 (triptorelin 1-month depot group) were administered a 3.75 mg intramuscular injection of triptorelin 1-month depot every 28 d, 18 (leuprorelin 3-month depot group) received an 11.25 mg subcutaneous injection of leuprorelin 3-month depot every 84 d, and 26 (mixed group) received both the leuprorelin 3-month depot and the triptorelin 1-month depot. This study was approved by the Ethics Committee of Longhua Branch of Shenzhen People’s Hospital Hospital (LL-KY-2023096-02) and adhered to the Ethical Principles outlined in the Declaration of Helsinki. Participant inclusion criteria:(I) informed consent signed by the legal guardian of the child; (II) fulfilment of the diagnostic criteria of the ‘Guidelines for the Diagnosis and Treatment of Central (True) Precocious Puberty’; (III) bone age (BA) exceeds the actual age by > 1 year; (IV) no previous treatment history. The exclusion criteria were as follows:(I) diseases associated with reproductive development, including hypothyroidism, malnutrition, and genitourinary developmental abnormalities; (II) manifestation of secondary precocious puberty during childhood accompanied by multiple organ pathologies; and (III) poor adherence to treatment and inability to follow the doctor’s instructions. Injection precautions: (I) injection site: injections can be subcutaneously or intramuscularly administered either in the upper arm or buttock; (II) site rotation: each injection should be administered at a different site, and repeated injections should not be administered at the same location consecutively; (III) caution during injections: Healthcare providers should be careful during injections to avoid puncturing blood vessels and remind children to avoid touching or pressing on the injection site.
2.2. Evaluation and Laboratory Testing
All participants underwent a follow-up of up to 2 years. Baseline measurements were obtained at the start of the study, followed by measurements at 1 year and 2 years following treatment initiation. The covariates examined during this time included: (a) serum sex hormone oestradiol (E2), testosterone (TS ), luteinising hormone (LH), and follicle-stimulating hormone (FSH), which were measured using an immunoassay (UniCel DxI 800 Access, Beckman Coulter, Inc. Ireland). (b) Adrenocorticotropic hormone (ACTH) and 25-hydroxyvitamin D (25-OHD) levels were measured using a chemical luminescence method (iFlash 3000; Shenzhen YHLO Biotech Co., Ltd., China). (c) IGF-1 levels were measured using the chemical luminescence method (Maglumi 800, Snibe Co., Ltd., China). (d) BA was examined using the Greulich and Pyle method, and maturity (BA/actual age) and BA growth rate were calculated. (e) Body mass index (BMI) [weight (kg)/square of height (m]) was calculated using documented anthropometric measurements. Among children and adolescents (<18 years), BMI percentiles were used to define overweight (≥85th) and obesity (≥95th). The 7th edition of “Practical Pediatrics” was referred to determine the formula. These measurements were recorded to examine the effects of the treatment and track patient progress. (f) All patients underwent pituitary magnetic resonance imaging assessments without any abnormalities, and all girls underwent pelvic ultrasound examinations, which revealed characteristics consistent with adolescent development and no pathological abnormalities.
2.3. Statistical Analysis
Statistical analyses were performed using R (http://www.R-project.org/) and related R packages. Categorical variables included percentages, and comparisons were made using the chi-square test. Numerical data included medians with interquartile ranges, and comparisons between the means of numerical variables were calculated using the Wilcoxon rank sum test. Statistical significance was set at P < 0.05.
3. Results
3.1. Subsection
3.1.1. Comparative Analysis of the General Characteristics of the Three Groups
Most children were girls (52.87%), with an average age of 9 ± 1 years (Table 1). Before treatment, age, sex, birth weight, birth height, height, weight, BMI, serum levels of LH, FSH, E2, 25-OHD, calcium (Ca), thyroid-stimulating hormone (TSH), prolactin (PRL), ACTH, and BA were not significantly different among the three groups (P > 0.5); however, TS levels showed significant differences among the three groups (P = 0.04) (triptorelin 1-month depot: 0.58 (0.30, 1.12); leuprorelin 3-month depot: 1.32 (0.73, 2.28); mixed: 0.80 (0.40, 1.15)). Between the triptorelin 1-month depot and the leuprorelin 3-month depot groups, except for TS (triptorelin 1-month depot: 0.58 (0.30, 1.12); leuprorelin 3-month depot: 1.32 (0.73, 2.28); p = 0.049), most indicators were statistically insignificant (P > 0.05) (Supplementary Table 1).
3.1.2. Comparative Analysis of the Serum Sex Hormones and Growth Indexes in the Three Participant Groups After 1 Year
The comparative analysis results of the triptorelin 1-month depot, leuprorelin 3-month depot, and mixed group after 1–2 years of treatment revealed no significant differences in the sex hormone levels (E2, LH, FSH, and T S), height, weight, BMI, BA, growth rate, maturity, and BA growth rate (P > 0.05) (Table 2). During the first year of treatment, the LH levels in the three groups were < 0.83 μmol/L [triptorelin 1-month depot:0.29 (0.24, 0.36); leuprorelin 3-month depot: 0.38 (0.21, 0.79); mixed: 0.29 (0.19, 0.66)]. Additionally, no significant difference was noted among the three groups (p = 0.88). In the second year, an increase in weight led to an increase in LH levels in the three groups. However, the results of the triptorelin 1-month depot group were much lower than those of the other two groups (triptorelin 1-month depot: 0.43 (0.28); leuprorelin 3-month depot: 1.44 (1.66); mixed: 0.88 (1.04)). The differences between the three groups were statistically insignificant (p = 0.23). FSH levels revealed the same results.
3.1.3. Comparative Analysis of the Serum Sex Hormones and Growth Indexes in the Three Participant Groups After 2 Years
We calculated the differences between the serum sex hormones and growth indicators after 1 or 2 years of treatment and their respective baseline values to compare whether different drug usage caused a variance. The analysis of these discrepancies revealed no statistically significant differences (Table 3), suggesting equivalence in the usage methods.
3.1.4. Comparative Analysis of the Serum Sex Hormones
After administration of the medication, a significant reduction in the FSH, LH, and TS levels in all groups was evident (Figure 1), demonstrating the pronounced efficacy of the treatment. Figure 2 shows a significant increase in the growth and BA growth rates across all groups. Furthermore, no significant changes were noted in the maturity or BMI, confirming treatment efficacy.
4. Discussion
Precocious puberty is the early activation of the hypothalamic-pituitary-gonadal axis in children [12]. Female children typically demonstrate breast development, long pubic hair, and armpit hair, whereas male children often exhibit enlarged testicles and penises and long pubic hair. It often results in rapid increases in height and weight, as well as premature bone closure. Recently, the incidence of this disease has been increasing, posing a serious threat to the physical and mental health of children. This alarming trend has garnered the attention of medical professionals both domestically and internationally [10]. Factors contributing to its occurrence include the environment of intrauterine development during embryogenesis, exposure to endocrine disruptors in the external environment, and nutritional excess owing to recent improvements in living standards [13,14,15]. Leuprorelin is a type of GnRHa and is recognised as the most effective treatment for CPP, with good therapeutic effects in treating patients with precocious puberty [16]. Presently, 1-, 3-, 6-, and 12-month formulations are internationally available [7,11,17]. In China, a 1-month depot (3.75 mg) of leuprorelin acetate and triptorelin acetate is most commonly used. The 3-month depot (11.25 mg) of leuprorelin is more commonly used abroad and was introduced in China in 2019 [18]; however, large-scale clinical data are still unavailable.
This study involved 60 patients who were treated with a leuprorelin 3-month depot, triptorelin 1-month depot, and a combination of the two drugs for two consecutive years. We aimed to observe and compare the therapeutic effects of the two formulations and provide clinical evidence for the use of the 3-month long-acting formulation of leuprorelin acetate in China. Before treatment, the three groups of children were comparable in terms of age, sex, birth weight, birth height, height, weight, BMI, and blood indicators, including 25-OHD, Ca, TSH, PRL, ACTH, LH, FSH, and E2, as well as BA. Only serum TS levels in the mixed treatment group were lower than those in the other groups. After 1 and 2 years of treatment, the sex hormone levels (E2, LH, FSH, and TS) in all three groups were effectively controlled, and no significant differences were observed in the growth indicators (height, weight, BMI, BA, growth rate, maturity, and BA growth rate), consistent with the results of a previous study [19].
Additionally, as treatment progressed, the blood hormone levels (E2, LH, FSH, and TS) generally revealed a downward trend. The most significant decline occurred in the first year, with a slight increase in the second year, but they were still lower than before treatment. This result may be associated with the increase in body weight as children grow older, leading to a decrease in the drug concentration per unit body weight and a subsequent reduction in the inhibitory effect on the hypothalamic-pituitary-gonadal axis. Among these hormones, LH and FSH levels considerably decreased in the first year, whereas E2 levels substantially decreased for two consecutive years. Although T decreased, the change was not statistically significant. Overall, the long-term use of different formulations at the current treatment doses demonstrated an inhibitory effect on the sex hormone levels.
As treatment progressed, we noted an increase in height and a decrease in the rate of BA growth. The slowed BA growth aligns with the effects of GnRHa treatment in patients with CPP during the rapid growth phase. However, the decrease in the drug concentration per unit of body weight owing to weight gain may also contribute to the weakening effect on BA control. Nevertheless, we noted that bone maturity (the ratio of BA to chronological age) did not substantially increase, indicating the effectiveness of controlling BA growth. The accelerated rate of height growth was likely associated with the gradual combined use of growth hormone therapy in most children during treatment [20]. Additionally, no significant increase in BMI was noted in the patients during the 2 years before and after treatment, suggesting that neither the triptorelin 1-month depot nor the leuprorelin 3-month depot caused an increase in BMI or adverse effects such as overweight/obesity. This result differs from the findings reported by Soliman et al. [21]. A slight increase in BMI is considered normal during puberty.
Although using LH and FSH levels in the sex hormone stimulation test as comparison indicators would have been more accurate, we compared LH and FSH at baseline, which still gave certain reference values, owing to limited medical treatment during the epidemic and the high cost and poor compliance of some children and parents with the stimulation test. Owing to the pandemic, collecting data on paediatric pelvic ultrasound has been challenging. Therefore, we did not include this parameter in the present study. This issue should be addressed in future studies. The study needs to continue tracking the outcomes after children discontinue medication, such as the menarche timing, final height, and whether the target height has been achieved. However, the current findings provide a reference value by comparing the efficacy of the two drugs. In future studies, we will expand the sample size, particularly for patients receiving leuprorelin, extend the tracking time, and include more observational indicators.
In summary, the use of leuprorelin 3-month depot alone, a 1-month formulation of triptorelin 1-month depot alone, or a combination of the two drugs has comparable therapeutic effects [22,23]. They can effectively inhibit the HPGA axis and sex hormone levels in children with CPP, slow puberty progression, inhibit BA development, and increase predicted adult height [24]. Moreover, these treatments did not increase BMI, and their effectiveness and safety were consistent with those reported in domestic and international studies. Leuprorelin 3-month depot is injected quarterly; therefore, using this dosage form can effectively reduce the number of visits by the patient, lower treatment costs, and improve treatment compliance. It has economic advantages and is suitable for promotion and use in China. Overall, the leuprorelin 3-month depot may emerge as a prevailing treatment modality in the future.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Methodology, Writing- original draft, Project administration, Xuan Han; Investigation,Qiaorong Chen; Investigation, Changhua Yu; Data curation, Formal analysis, Qianqian Chen; :Investigation ,Wei Zhang; Validation, Supervision,Q in Zhang; Supervision (Investigation guidance) ,Duoqing Dong; Validation, Congliang Zhang.
Funding
This work was supported by grants from the Basic Project of Shenzhen Science and Technology Innovation Commission in 2021,”Discovery of Specific Intestinal Microflora and Intestinal Microecological Intervention for Early Sexual Maturity” (No. JCYJ20210324112804012).
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Due to privacy and hospital ethics management requirements, de-identified data can be requested via email: hanxuan415@126.com.
Acknowledgments
During the preparation of this manuscript, the author(s) used Language Editing Plus services provided by MDPI for the purpose of English language polishing. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Zevin, EL; Eugster, EA. Central precocious puberty: a review of diagnosis, treatment, and outcomes. Lancet Child Adolesc Health 2023, 7(12), 886–896. [Google Scholar] [CrossRef]
- Soriano-Guillén, L; Argente, J. Pubertad precoz central: aspectos epidemiológicos, etiológicos y diagnóstico-terapéuticos Central precocious puberty: epidemiology, etiology, diagnosis and treatment. Ann Paediatr (Barc);Spanish 2011, 74(5), 336.e1–336.e13. [Google Scholar] [CrossRef] [PubMed]
- Kim, EY; Lee, MI. Psychosocial aspects in girls with idiopathic precocious puberty. Psychiatry Investig. 2012, 9(1), 25–28. [Google Scholar] [CrossRef]
- Pasquino, AM; Pucarelli, I; Accardo, F; et al. Long-term observation of 87 girls with idiopathic central precocious puberty treated with gonadotropin-releasing hormone analogs: impact on adult height, body mass index, bone mineral content, and reproductive function. J Clin Endocrinol Metab. 2008, 93(1), 190–195. [Google Scholar] [CrossRef] [PubMed]
- Park, J; Kim, JH. Change in body mass index and insulin resistance after 1-year treatment with gonadotropin-releasing hormone agonists in girls with central precocious puberty. Ann Pediatr Endocrinol Metab 2017, 22(1), 27–35. [Google Scholar] [CrossRef]
- Poomthavorn, P; Suphasit, R; Mahachoklertwattana, P. Adult height, body mass index and time of menarche of girls with idiopathic central precocious puberty after gonadotropin releasing hormone analogue treatment. Gynecol Endocrinol 2011, 27(8), 524–528. [Google Scholar] [CrossRef] [PubMed]
- Klein, KO; Mauras, N; Nayak, S; et al. Efficacy and safety of leuprolide acetate 6-month depot for the treatment of central precocious puberty: a phase 3 study. J Endocr Soc. 2023, 7(7), bvad071. [Google Scholar] [CrossRef]
- Vatopoulou, A; Roos, E; Daniilidis, A; Dinas, K. Long-term effects of treatment of central precocious puberty with gonadotropin-releasing hormone analogs every three months. Gynecol Endocrinol 2020, 36(12), 1124–1126. [Google Scholar] [CrossRef]
- Popovic, J; Geffner, ME; Rogol, AD; et al. Gonadotropin-releasing hormone analog therapies for children with central precocious puberty in the United States. Front Pediatr 2022, 10, 968485. [Google Scholar] [CrossRef]
- Lin, WD; Wang, CH; Tsai, FJ. Genetic screening of the makorin ring finger 3 gene in girls with idiopathic central precocious puberty. Clin Chem Lab Med. 2016, 54(3), e93–e96. [Google Scholar] [CrossRef]
- Yoo, E; Kim, S; Jung, HL; et al. Impact of 6-month triptorelin formulation on predicted adult height and basal gonadotropin levels in patients with central precocious puberty. Front Endocrinol (Lausanne) 2023, 14, 1134977. [Google Scholar] [CrossRef]
- Micangeli, G; Paparella, R; Tarani, F; et al. Clinical management and therapy of precocious puberty in the Sapienza university pediatrics hospital of Rome, Italy. Children (Basel) 2023, 10(10), 1672. [Google Scholar] [CrossRef]
- Dong, Y; Dai, L; Dong, Y; et al. Analysis of risk factors of precocious puberty in children. BMC Pediatr 2023, 23(1), 456. [Google Scholar]
- Choe, Y; Cha, JH; Kim, YJ; et al. Rapid weight gain in early life is associated with central precocious puberty in girls, not in boys - a nationwide population-based study in Korea. Front Endocrinol (Lausanne) 2023, 14, 1210995. [Google Scholar] [CrossRef]
- Benedetto, M; Riveros, V; Eymann, A; Terrasa, S; Alonso, G. Analysis of the incidence of central precocious puberty treated with gonadotropin-releasing hormone analogs. Impact of the COVID-19 pandemic. Arch Argent Pediatr 2023, 121(3), e202202849. [Google Scholar] [PubMed]
- Jang, S; Kim, SJ; Lee, M; et al. Comparison of the effect of gonadotropin-releasing hormone agonist dosage in girls with central precocious puberty. Ann Pediatr Endocrinol Metab 2023, 28(4), 283–288. [Google Scholar] [CrossRef] [PubMed]
- Cipolla, C; Sodero, G; Pane, LC; et al. Auxological and metabolic parameters of children undergoing the gonadotropin-releasing hormone stimulation test: correlations with the final diagnosis of central precocious puberty in a single-center study. Biomedicines 2023, 11(6), 1678. [Google Scholar] [CrossRef] [PubMed]
- Bangalore Krishna, KK; Fuqua, JS; Rogol, AD; et al. Use of gonadotropin-releasing hormone analogs in children: update by an international consortium. Horm Res Paediatr. 2019, 91(6), 357–372. [Google Scholar] [CrossRef]
- Yang, J; Song, Q; Gao, S; et al. Efficacy of leuprorelin 3-month depot (11.25 mg) compared to 1-month depot (3.75 mg) for central precocious puberty in Chinese girls: A prospective cohort study. Int J Endocrinol 2022, 2022, 1043293. [Google Scholar] [CrossRef]
- Dotremont, H; France, A; Heinrichs, C; et al. Efficacy and safety of a 4-year combination therapy of growth hormone and gonadotropin-releasing hormone analogue in pubertal girls with short predicted adult height. Front Endocrinol (Lausanne) 2023, 14, 1113750. [Google Scholar] [CrossRef]
- Soliman, AT; Alaaraj, N; De Sanctis, V; et al. Long-term health consequences of central precocious/early puberty (CPP) and treatment with Gn-RH analogue: a short update. Acta Biomed. 2023, 94(6), e2023222. [Google Scholar] [PubMed]
- Valenzise, M; Nasso, C; Scarfone, A; et al. Leuprolide and triptorelin treatment in children with idiopathic central precocious puberty: an efficacy/tolerability comparison study. Front Pediatr 2023, 11, 1170025. [Google Scholar] [CrossRef] [PubMed]
- Yang, EH; Jo, HY; Park, SJ; et al. Effect of gonadotropin-releasing hormone agonist treatment on near final height in girls with central precocious puberty and early puberty. Ann Pediatr Endocrinol Metab 2023, 28(1), 49–53. [Google Scholar] [CrossRef] [PubMed]
- Luo, X; Zhang, C; Yang, Y; et al. Efficacy and safety of triptorelin 3-month formulation in Chinese children with central precocious puberty: A Phase 3, open-label, single-arm study. Adv Ther. 2023, 40(10), 4574–4588. [Google Scholar] [CrossRef]
Figure 1.
Comparative serum hormone levels in all group.
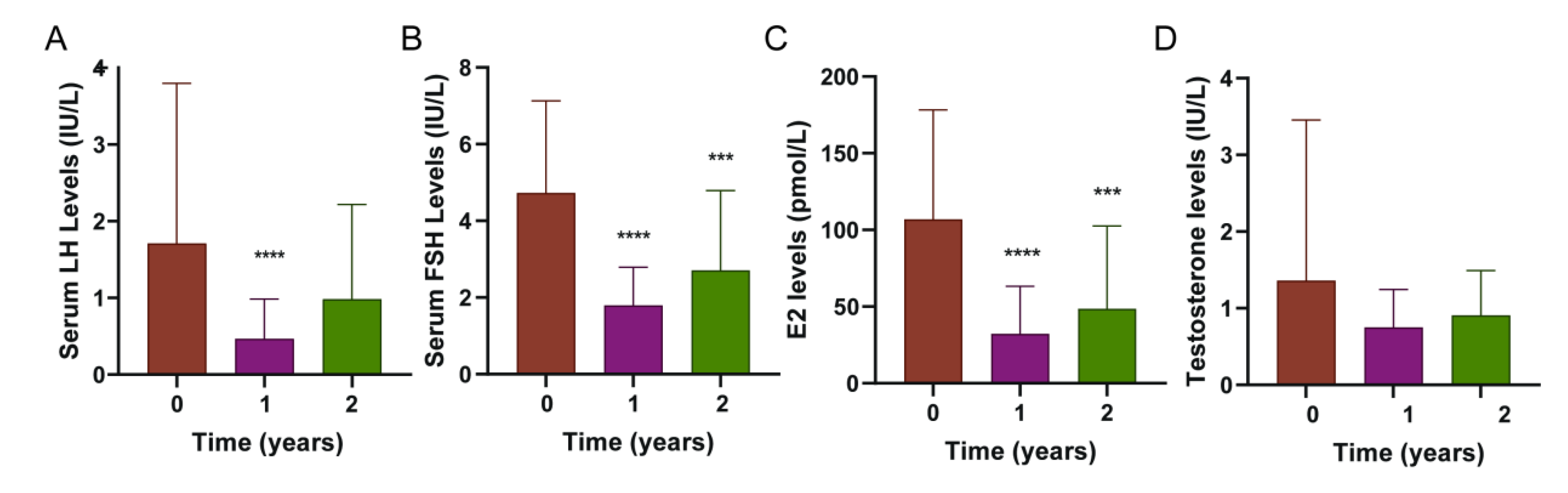
Figure 2.
Comparative growth indexes in all group.
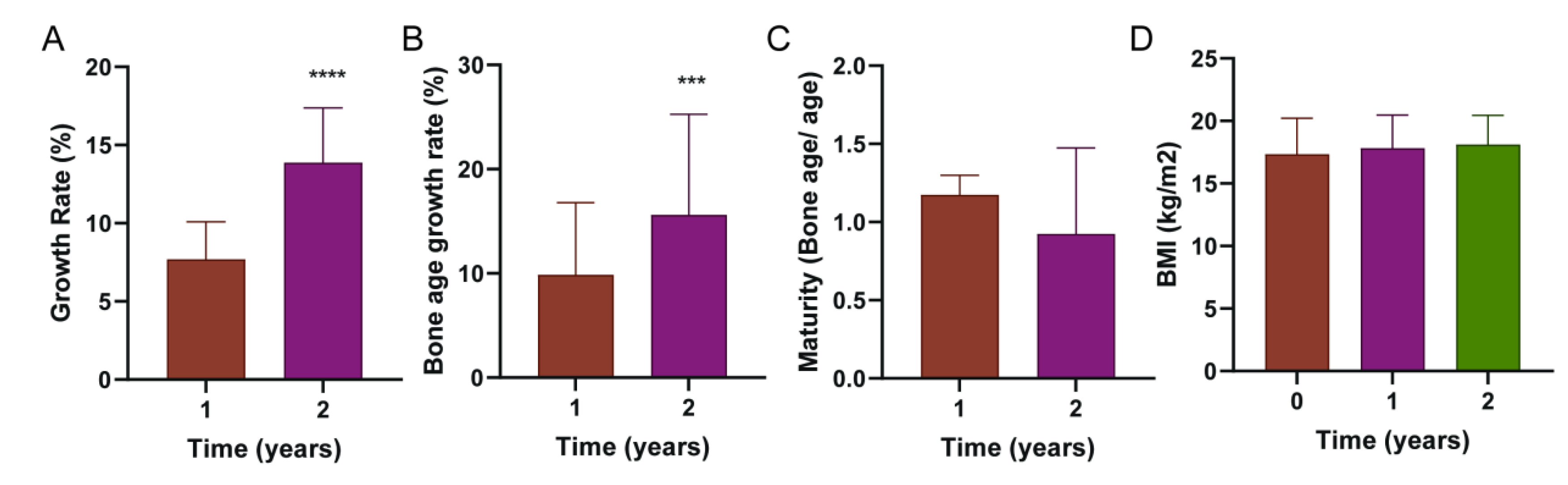

Table 1.
Comparative analysis of the general situation of three groups.
| Characteristic | N | Overall, N = 601 |
Triptorelingroup , N = 161 |
Leuprolide group, N = 181 | Mixed group, N = 261 |
p-value2 |
|---|---|---|---|---|---|---|
| Age | 60 | 9.00(8.00,10.00) | 8.50(8.00,10.00) | 10.00(8.00,10.75) | 9.00(8.00,9.75) | 0.39 |
| Sex | 60 | 0.34 | ||||
| Female | 52 (87%) | 14 (88%) | 14 (78%) | 24 (92%) | ||
| Male | 8 (13%) | 2 (13%) | 4 (22%) | 2 (7.7%) | ||
| Birth height | 60 | 50.00(49.00,50.00) | 50.00(49.75,50.00) | 50.00(49.25,50.00) | 50.00(49.25,50.00) | 0.89 |
| Birth weight | 60 | 3.25(2.95,3.46) | 3.20(2.94,3.33) | 3.15(2.85,3.43) | 3.35(3.00,3.50) | 0.37 |
| Height | 60 | 137(7) | 136(6) | 140(8) | 136(6) | 0.09 |
| Weight | 60 | 33(7) | 32(6) | 34(7) | 33(8) | 0.69 |
| BMI | 60 | 17.27(15.09,18.69) | 16.63(15.01,19.19) | 17.57(15.35,17.98) | 17.11(15.13,18.73) | 0.92 |
| BA | 60 | 10.57(1.32) | 10.30(1.61) | 11.04(1.35) | 10.42(1.04) | 0.20 |
| 25-OHD | 60 | 23.9(6.2) | 23.1(5.3) | 23.0(5.7) | 25.0(6.9) | 0.46 |
| Ca | 60 | 2.53(0.09) | 2.51(0.07) | 2.54(0.09) | 2.53(0.09) | 0.36 |
| TSH | 59 | 1.97(1.16,2.45) | 2.01(1.58,2.43) | 1.68(0.85,2.95) | 1.91(1.26,2.32) | 0.88 |
| T4 | 60 | 108(98,121) | 119(99,125) | 108(98,118) | 108(99,118) | 0.60 |
| ACTH | 60 | 11(8,18) | 15(7,19) | 11(10,21) | 10(8,15) | 0.68 |
| LH | 60 | 0.98(0.47,1.91) | 1.17(0.51,2.00) | 1.30(0.79,1.99) | 0.62(0.31,1.55) | 0.07 |
| Fsh | 60 | 4.42(2.83,6.31) | 5.17(4.12,5.66) | 4.25(2.86,6.53) | 4.17(2.71,6.13) | 0.58 |
| PRL | 60 | 168(134,235) | 166(132,215) | 195(136,271) | 164(135,236) | 0.59 |
| Testosterone | 57 | 0.80(0.41,1.50) | 0.58(0.30,1.12) | 1.32(0.73,2.28) | 0.80(0.40,1.15) | 0.04 |
| E2 | 57 | 86(52,135) | 104(74,132) | 87(53,183) | 74(39,124) | 0.26 |
1 Mean(SD); n (%); Median(25%,75%). 2 Kruskal-Wallis rank sum test; Fisher’s exact test Note:BA,bone age;BMI,body mass index; 25-OHD,25-HydroxyvitaminD; Ca,calcium; TSH,thyroid-stimulating hormone;T4,Thyroxine; ACTH,Adrenocorticotropic Hormone; LH,luteinizing hormone;FSH,follicle-stimulating hormone;PRL,Prolactin;E2,estradiol;.
Table 2.
Comparative analysis of serum sex hormones and growth indexes in three groups.
| Characteristic | N | Overall, N = 601 |
Triptorelin group, N = 161 |
Leuprolide group, N = 181 |
Mixed group, N = 261 |
p-value2 |
|---|---|---|---|---|---|---|
| LH- one year | 50 | 0.29(0.21,0.60) | 0.29(0.24,0.36) | 0.38(0.21,0.79) | 0.29(0.19,0.66) | 0.88 |
| LH- two year | 33 | 0.98(1.23) | 0.43(0.28) | 1.44(1.66) | 0.88(1.04) | 0.23 |
| Fsh- one year | 50 | 1.57(1.10,2.24) | 1.28(0.82,1.79) | 1.53(1.13,2.07) | 1.88(1.28,2.82) | 0.18 |
| Fsh- two year | 33 | 2.71(2.08) | 1.87(1.31) | 2.47(1.75) | 3.18(2.46) | 0.40 |
| Testosterone-one year | 48 | 0.76(0.42,1.15) | 0.65(0.37,1.18) | 0.85(0.55,1.13) | 0.73(0.25,1.10) | 0.61 |
| Testosterone- two year | 29 | 0.91(0.58) | 1.20(0.64) | 0.82(0.48) | 0.87(0.63) | 0.57 |
| E2-one year | 44 | 28(11,43) | 24(9,54) | 23(13,32) | 34(14,48) | 0.59 |
| E2- two year | 29 | 49(54) | 57(75) | 69(72) | 31(16) | 0.81 |
| Height -one year | 60 | 144.9(6.5) | 144.3(6.0) | 147.5(7.6) | 143.5(5.7) | 0.083 |
| Height- two year | 44 | 150(6) | 149(8) | 153(7) | 149(5) | 0.28 |
| Weight-one year | 60 | 38(7) | 37(7) | 39(7) | 37(8) | 0.73 |
| Weight- two year | 44 | 41(7) | 43(7) | 41(6) | 40(7) | 0.48 |
| BMI- one year | 60 | 17.82(2.65) | 17.91(2.87) | 17.61(2.09) | 17.92(2.94) | 0.89 |
| BMI- two year | 44 | 18.11(2.35) | 19.31(1.90) | 17.48(1.64) | 18.04(2.82) | 0.12 |
| BA-one year | 60 | 11.55(1.01) | 11.36(1.25) | 11.92(1.04) | 11.40(0.77) | 0.17 |
| BA- two year | 45 | 12.10(0.89) | 11.81(0.96) | 12.39(0.92) | 11.99(0.81) | 0.17 |
| Growth rate-one year | 60 | 7.20(6.28,9.13) | 7.15(6.48,9.25) | 7.40(6.55,8.30) | 6.65(6.00,9.18) | 0.63 |
| Growth rate- two year | 44 | 13.9(3.5) | 13.8(2.8) | 13.5(4.3) | 14.2(3.2) | 0.62 |
| Maturity3-one year | 60 | 1.18(1.08,1.26) | 1.13(1.08,1.29) | 1.17(1.10,1.21) | 1.20(1.06,1.26) | 0.96 |
| Maturity3- two year | 60 | 0.92(0.55) | 0.70(0.65) | 1.09(0.42) | 0.95(0.54) | 0.59 |
| GBA4-one year | 60 | 9(4,14) | 9(5,15) | 7(4,12) | 9(4,15) | 0.65 |
| GBA4- two year | 45 | 16(10) | 14(7) | 14(11) | 17(10) | 0.46 |
1 Mean(SD); Median(25%,75%) 2 Kruskal-Wallis rank sum test 3 Maturity means the ratio of bone age to living age 4 GBA means growth rate of bone age Note:BA,bone age;BMI,body mass index; hormone;LH,luteinizing hormone;FSH,follicle-stimulating hormone;E2,estradiol.
Table 3.
Comparative analysis of serum sex hormones and growth indexes in three groups.
| Characteristic | N | Overall, N = 601 |
Triptorelin group, N = 161 |
Leuprolide group, N = 181 |
Mixed,group, N = 261 |
p-value2 |
|---|---|---|---|---|---|---|
| LH- one year | 33 | -0.52(-1.25,-0.11) | -1.39(-2.59,-0.32) | -0.70(-1.18,-0.34) | -0.19(-0.74,-0.04) | 0.27 |
| LH- two year | 33 | -0.38(-0.90,0.60) | -1.42(-2.42,-0.42) | -0.20(-0.75,0.24) | -0.24(-0.65,0.71) | 0.28 |
| Fsh- one year | 33 | -2.17(-4.35,-0.83) | -2.30(-3.03,-2.00) | -3.04(-4.48,-0.48) | -1.53(-4.34,-0.82) | 0.91 |
| Fsh- two year | 33 | -1.67(-3.87,0.24) | -2.34(-3.13,-1.76) | -1.59(-3.84,0.32) | -1.57(-3.95,0.78) | 0.81 |
| Testosterone-one year | 28 | -0.07(-0.42,0.28) | 0.01(-0.02,0.27) | -0.28(-0.47,-0.18) | 0.09(-0.27,0.44) | 0.20 |
| Testosterone- two year | 28 | 0.23(-0.31,0.41) | 0.38(0.26,0.38) | -0.24(-0.80,0.01) | 0.30(-0.21,0.48) | 0.20 |
| E2- one year | 25 | -32(-85,-12) | -97(-118,-86) | -24(-77,-12) | -29(-71,-17) | 0.23 |
| E2- two year | 25 | -53(-91,26) | -115(-131,-84) | -14(-75,37) | -46(-59,-3) | 0.085 |
| Growth- one year | 60 | 7.20(6.28,9.13) | 7.15(6.48,9.25) | 7.40(6.55,8.30) | 6.65(6.00,9.18) | 0.63 |
| Growth- two year | 44 | 13.6(11.9,15.3) | 14.2(13.3,15.6) | 13.3(10.4,14.8) | 13.5(12.6,15.0) | 0.62 |
| Mature- one year | 60 | 1.18(1.08,1.26) | 1.13(1.08,1.29) | 1.17(1.10,1.21) | 1.20(1.06,1.26) | 0.96 |
| Mature- two year | 60 | 1.18(0.74,1.24) | 1.02(0.00,1.30) | 1.16(1.07,1.27) | 1.21(1.10,1.23) | 0.59 |
| BMI- one year | 44 | 0.43(-0.47,1.44) | 1.32(0.22,1.71) | 0.71(-0.16,1.26) | 0.02(-0.90,0.99) | 0.28 |
| BMI- two year | 44 | 0.82(-0.21,1.65) | 1.49(-0.14,1.71) | 0.68(-0.25,1.27) | 0.72(-0.01,1.32) | 0.81 |
1 Mean(SD); Median(25%,75%) 2 Kruskal-Wallis rank sum test Note:BA,bone age;BMI,body mass index; 25-OHD,25-HydroxyvitaminD; Ca,calcium; TSH,thyroid-stimulating hormone;T4,Thyroxine; ACTH,Adrenocorticotropic Hormone; LH,luteinizing hormone;FSH,follicle-stimulating hormone;PRL,Prolactin;E2,estradiol.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



