
Submitted:
23 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Extra-medullary haematopoiesis (EMH) refers to haematopoietic proliferation outside the bone marrow, most often arising as a compensatory response to ineffective marrow function in chronic anaemias and myeloid neoplasms, particularly myelofibrosis and other myeloproliferative neoplasms. While the liver and spleen are typical sites, mass-forming EMH in non-reticuloendothelial organs is rare; renal involvement is particularly uncommon and may closely mimic infiltrative malignancy or infection on cross-sectional imaging. We report a 35-year-old woman who presented with asthenia, progressive weight loss and intermittent fever. Previous bone-marrow biopsy had demonstrated early myelofibrosis. Contrast-enhanced thoraco-abdominopelvic CT showed bilateral thoracic paravertebral and presacral soft-tissue masses and left peripelvic/pelvicalyceal infiltration, raising concern for malignancy or infection. Whole-body [18F]-FDG-PET/CT revealed only faint (low-grade) hypermetabolism within the paravertebral and presacral lesions, and no convincing focal hypermetabolism within the renal lesion, whose assessment was limited by urinary tracer activity. Given the haemorrhagic risk of renal biopsy in a cytopenic patient, technetium-99m sulphur colloid scintigraphy with SPECT/CT demonstrated tracer uptake within all lesions, confirming multifocal EMH. This case highlights renal peripelvic EMH as a rare malignancy mimic for which [18F]-FDG-PET/CT may be non-diagnostic, and supports sulphur colloid SPECT/CT as a robust, non-invasive alternative when tissue sampling is hazardous.
Keywords:
extramedullary haematopoiesis
; renal EMH
; myelofibrosis
; myeloproliferative neoplasm
; [18F]-FDG-PET/CT
; technetium-99m sulphur colloid
; SPECT/CT
; renal peripelvic infiltration
Figure 1.
Contrast-enhanced thoraco-abdominopelvic CT (CE-CT). (A). Coronal reconstruction showing massive hepatomegaly (red star) and splenomegaly (blue star), with left peripelvic/pelvicalyceal soft-tissue infiltration (red arrowheads) associated with renal pelvic dilatation. (B). Axial chest CT demonstrating bilateral thoracic paravertebral infiltrative soft-tissue masses (orange arrows). (C). Axial abdominal CT illustrating the left peripelvic/pelvicalyceal infiltrative abnormality (red arrow). (D). Axial pelvic CT showing a presacral infiltrative soft-tissue lesion (orange arrows). A 35-year-old woman was referred to the haematology department for evaluation of a persistent inflammatory syndrome with B symptoms, consisting of intermittent fever, profuse night sweats, and unintentional weight loss of approximately 5-6 kg over three months. The symptoms had been present for around six months, with progressive worsening. She also reported low back pain of insidious onset that had rapidly become constant and predominantly nocturnal. Two months earlier, she had consulted her general practitioner regarding similar symptoms. At that time, blood tests were largely unremarkable, except for microcytic hypochromic anaemia, with haemoglobin (Hb) at 9.4 g/dL, mean corpuscular volume (MCV) at 74 fL, and mean corpuscular haemoglobin concentration (MCHC) at 28 g/dL. Her medical history included iron deficiency anaemia on supplementation, poorly controlled type 2 diabetes mellitus, and well-controlled arterial hypertension. She had recently returned from a three-week trip to Senegal. Bearing in mind the patient condition, further investigations were carried out. Laboratory investigations revealed severe pancytopenia with aregenerative anaemia (Hb 7.1 g/dL; reticulocytes 18 × 109/L), leukopenia (WBC 1.2 × 109/L) with profound neutropenia (0.45 × 109/L), and thrombocytopenia (platelets 52 × 109/L), together with marked inflammation (CRP 156 mg/L; ferritin 3,400 µg/L). The peripheral blood smear showed 5% circulating blasts. Lactate dehydrogenase was moderately elevated (520 U/L), while renal and liver function were preserved (creatinine 0.92 mg/dL; AST 31 U/L; ALT 34 U/L). First-line infectious and parasitological investigations were negative, including blood cultures, HIV and hepatitis B/C serology, CMV and EBV IgM, and malaria testing (rapid antigen test and thick film). Given the cytopenia’s, bone marrow aspirate and trephine biopsy showed a hypercellular marrow with dysplastic features and megakaryocytic atypia, without CD34-defined blast excess; reticulin/Masson trichrome staining confirmed grade 2 myelofibrosis with focal collagen deposition.
Figure 1.
Contrast-enhanced thoraco-abdominopelvic CT (CE-CT). (A). Coronal reconstruction showing massive hepatomegaly (red star) and splenomegaly (blue star), with left peripelvic/pelvicalyceal soft-tissue infiltration (red arrowheads) associated with renal pelvic dilatation. (B). Axial chest CT demonstrating bilateral thoracic paravertebral infiltrative soft-tissue masses (orange arrows). (C). Axial abdominal CT illustrating the left peripelvic/pelvicalyceal infiltrative abnormality (red arrow). (D). Axial pelvic CT showing a presacral infiltrative soft-tissue lesion (orange arrows). A 35-year-old woman was referred to the haematology department for evaluation of a persistent inflammatory syndrome with B symptoms, consisting of intermittent fever, profuse night sweats, and unintentional weight loss of approximately 5-6 kg over three months. The symptoms had been present for around six months, with progressive worsening. She also reported low back pain of insidious onset that had rapidly become constant and predominantly nocturnal. Two months earlier, she had consulted her general practitioner regarding similar symptoms. At that time, blood tests were largely unremarkable, except for microcytic hypochromic anaemia, with haemoglobin (Hb) at 9.4 g/dL, mean corpuscular volume (MCV) at 74 fL, and mean corpuscular haemoglobin concentration (MCHC) at 28 g/dL. Her medical history included iron deficiency anaemia on supplementation, poorly controlled type 2 diabetes mellitus, and well-controlled arterial hypertension. She had recently returned from a three-week trip to Senegal. Bearing in mind the patient condition, further investigations were carried out. Laboratory investigations revealed severe pancytopenia with aregenerative anaemia (Hb 7.1 g/dL; reticulocytes 18 × 109/L), leukopenia (WBC 1.2 × 109/L) with profound neutropenia (0.45 × 109/L), and thrombocytopenia (platelets 52 × 109/L), together with marked inflammation (CRP 156 mg/L; ferritin 3,400 µg/L). The peripheral blood smear showed 5% circulating blasts. Lactate dehydrogenase was moderately elevated (520 U/L), while renal and liver function were preserved (creatinine 0.92 mg/dL; AST 31 U/L; ALT 34 U/L). First-line infectious and parasitological investigations were negative, including blood cultures, HIV and hepatitis B/C serology, CMV and EBV IgM, and malaria testing (rapid antigen test and thick film). Given the cytopenia’s, bone marrow aspirate and trephine biopsy showed a hypercellular marrow with dysplastic features and megakaryocytic atypia, without CD34-defined blast excess; reticulin/Masson trichrome staining confirmed grade 2 myelofibrosis with focal collagen deposition.

Figure 2.
Figure 2. [18F]-FDG-PET/CT of the patient: (A) Maximum intensity projection (MIP) demonstrates faint FDG uptake in the thoracic paravertebral regions and in the presacral area (black arrows), without other suspicious hypermetabolic foci; physiological urinary excretion is present. (B) Axial PET images show low-grade uptake corresponding to the bilateral thoracic paravertebral soft-tissue masses (orange arrows, upper panel) and to the presacral infiltrative lesion (orange arrow, lower panel). The left peripelvic/pelvicalyceal infiltrative abnormality shows no definite focal hypermetabolism; assessment is limited by urinary activity within the collecting system (red arrow, middle panel). (C) Corresponding axial low-dose CT images. (D) Fused PET/CT images confirm the subtle metabolic activity of the paravertebral and presacral lesions (orange arrows) and the indeterminate metabolic characterisation of the left renal peripelvic/pelvicalyceal infiltration (red arrow). To further characterise the CT abnormalities and assess metabolic activity, an [18F]-FDG-PET/CT was performed (Figure 2). This demonstrated diffuse, heterogeneous hypermetabolism throughout the skeleton, in keeping with extensive marrow involvement (Figure 2A, black arrows). Increased FDG uptake was also seen within the paravertebral thoracic and presacral soft tissue infiltrates (Figure 2B and 2D, orange arrows). Furthermore, a left sided infiltrative lesion centred on the pyelocaliceal system showed abnormal uptake (Figure 2B and 2D, red arrow), although evaluation was partly limited by physiological urinary tracer activity. This renal lesion raised a key diagnostic dilemma between a primary urothelial malignancy and extra-medullary involvement related to the underlying haematological disorder. Tissue sampling was not feasible because of an unacceptably high haemorrhagic risk. To support a marrow related aetiology, technetium-99m sulphur colloid scintigraphy with SPECT/CT was performed (Figure 3).
Figure 2.
Figure 2. [18F]-FDG-PET/CT of the patient: (A) Maximum intensity projection (MIP) demonstrates faint FDG uptake in the thoracic paravertebral regions and in the presacral area (black arrows), without other suspicious hypermetabolic foci; physiological urinary excretion is present. (B) Axial PET images show low-grade uptake corresponding to the bilateral thoracic paravertebral soft-tissue masses (orange arrows, upper panel) and to the presacral infiltrative lesion (orange arrow, lower panel). The left peripelvic/pelvicalyceal infiltrative abnormality shows no definite focal hypermetabolism; assessment is limited by urinary activity within the collecting system (red arrow, middle panel). (C) Corresponding axial low-dose CT images. (D) Fused PET/CT images confirm the subtle metabolic activity of the paravertebral and presacral lesions (orange arrows) and the indeterminate metabolic characterisation of the left renal peripelvic/pelvicalyceal infiltration (red arrow). To further characterise the CT abnormalities and assess metabolic activity, an [18F]-FDG-PET/CT was performed (Figure 2). This demonstrated diffuse, heterogeneous hypermetabolism throughout the skeleton, in keeping with extensive marrow involvement (Figure 2A, black arrows). Increased FDG uptake was also seen within the paravertebral thoracic and presacral soft tissue infiltrates (Figure 2B and 2D, orange arrows). Furthermore, a left sided infiltrative lesion centred on the pyelocaliceal system showed abnormal uptake (Figure 2B and 2D, red arrow), although evaluation was partly limited by physiological urinary tracer activity. This renal lesion raised a key diagnostic dilemma between a primary urothelial malignancy and extra-medullary involvement related to the underlying haematological disorder. Tissue sampling was not feasible because of an unacceptably high haemorrhagic risk. To support a marrow related aetiology, technetium-99m sulphur colloid scintigraphy with SPECT/CT was performed (Figure 3).
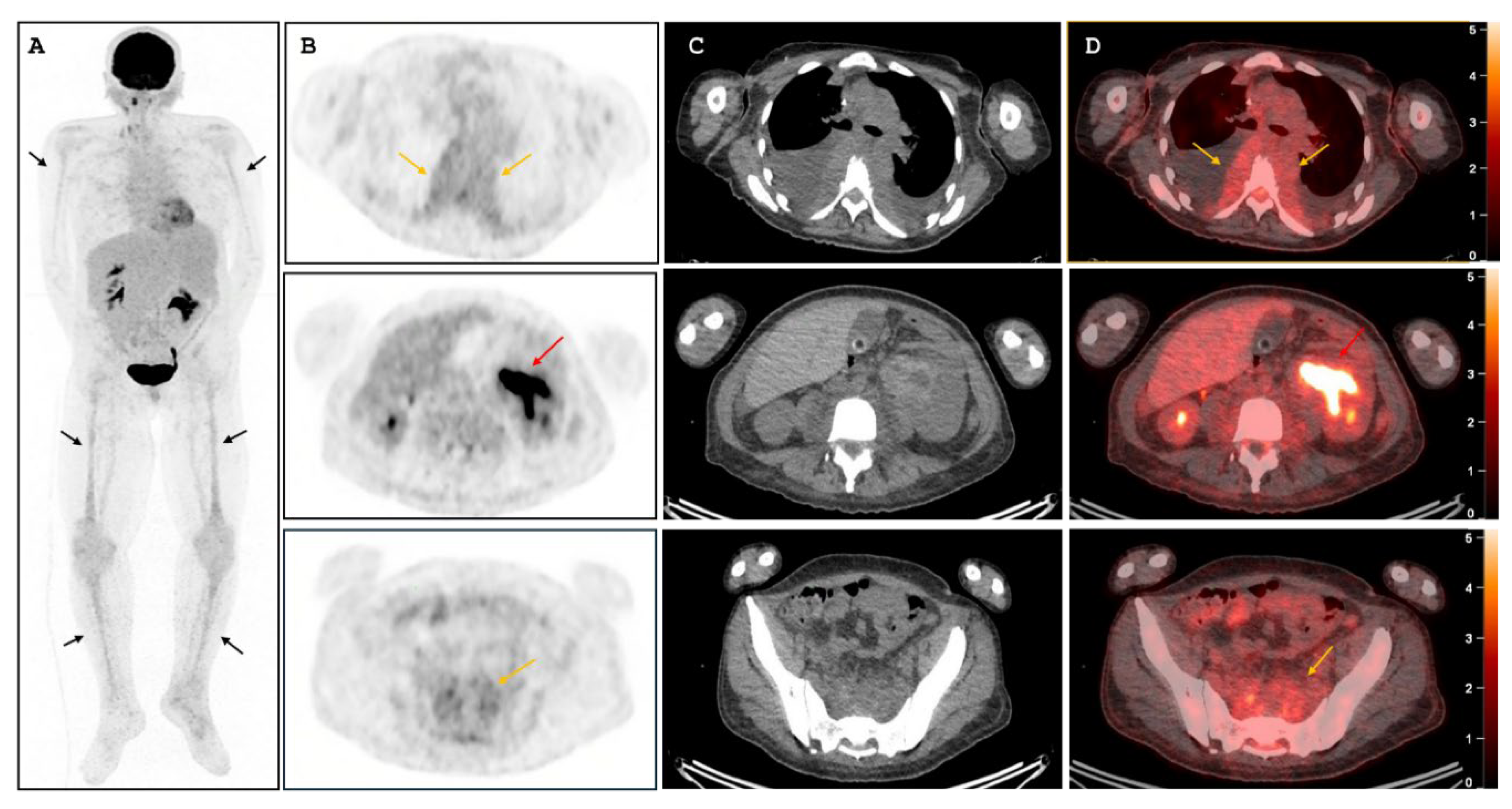
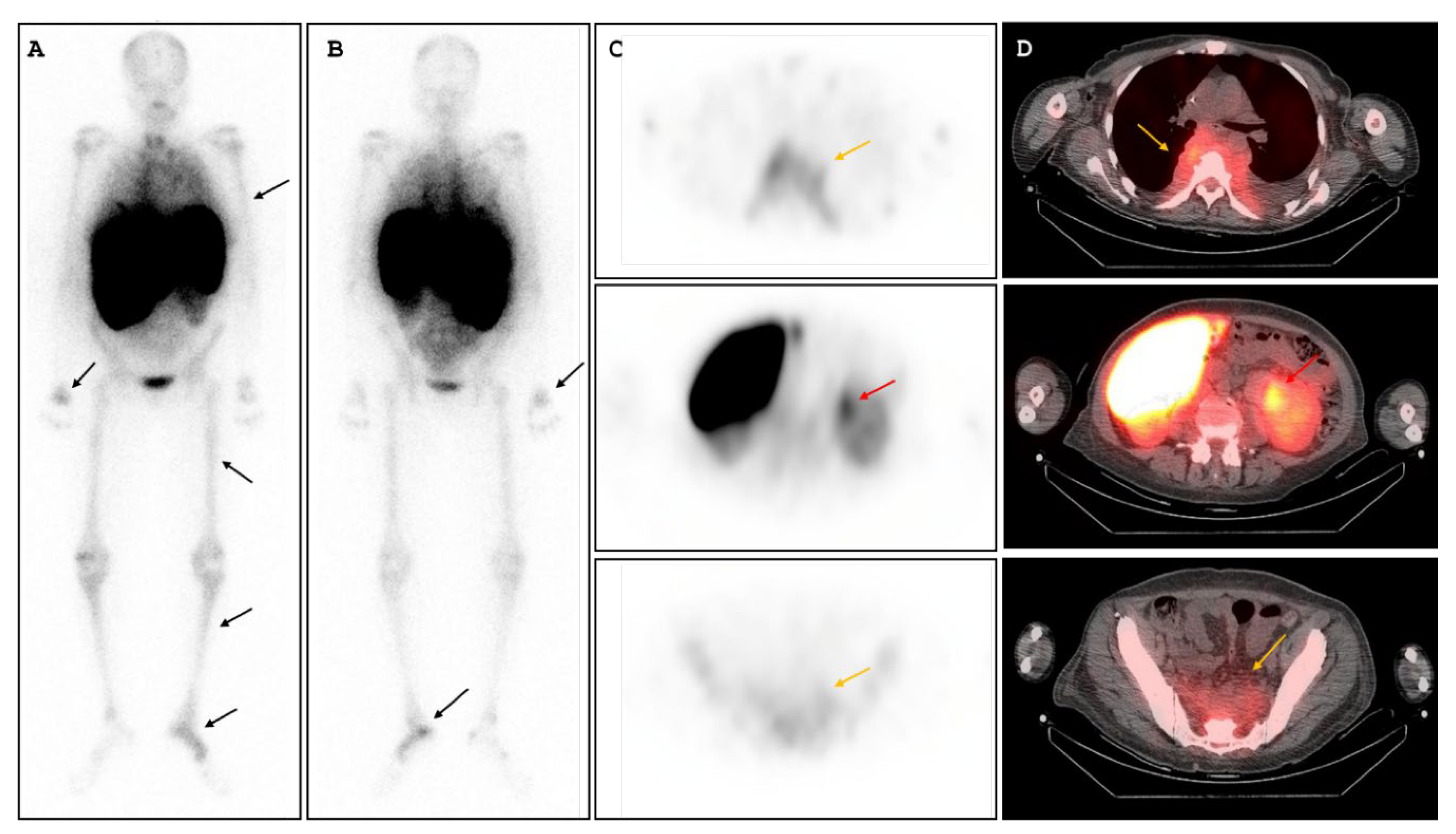
Figure 3.
[99mTc]-sulphur colloid scintigraphy with SPECT/CT. (A, B) Whole-body planar images (anterior/posterior) are displayed with intensity scaled to optimise skeletal activity; prominent hepatic and splenic uptake is seen in the context of hepatosplenomegaly. Diffuse, heterogeneous skeletal tracer distribution is consistent with extensive active marrow involvement (black arrows). (C) Axial SPECT images show tracer uptake within the thoracic paravertebral soft-tissue masses (orange arrow, upper panel), the left peripelvic/pelvicalyceal infiltrative lesion (red arrow, middle panel), and the presacral infiltrative lesion (orange arrow, lower panel). (D) Fused SPECT/CT images confirm concordant radiotracer uptake within the paravertebral and presacral soft-tissue infiltrates (orange arrows) and including the left peripelvic/pelvicalyceal lesion (red arrow). Overall, the concordant colloid uptake across all lesions supported multifocal EMH, providing a non-invasive alternative when tissue sampling is high risk. Given the left pelvicalyceal involvement with pelvic dilatation, a double-J ureteric stent was inserted. The patient required transfusion support and received anti-thymocyte globulin plus ciclosporin, with adjunct thrombopoietin-receptor agonists (romiplostim and eltrombopag), before proceeding to allogeneic haematopoietic stem-cell transplantation, with favourable clinical and haematological recovery. Extra-medullary haematopoiesis (EMH) is a recognised compensatory phenomenon in chronic anaemias and myeloid neoplasms, particularly primary myelofibrosis and related myeloproliferative neoplasms. However, clinically relevant mass-forming EMH at atypical sites remains uncommon and frequently mimics malignancy or infection on anatomical imaging [1,2]. The diagnostic challenge is further compounded when EMH occurs in non-reticuloendothelial organs, where tumour-like deposits may be misinterpreted as lymphoma, metastatic disease, inflammatory pseudo-tumour, or chronic infection, resulting in invasive procedures that can be hazardous for cytopenic patients [1,2]. Renal EMH is particularly rare and represents a key imaging pitfall. Reported patterns include perinephric plaques, renal hilar/perihilar masses, and infiltrative soft-tissue encasement of the renal sinus and pelvicalyceal system, sometimes extending to the proximal ureter and potentially causing obstruction or renal dysfunction [3,4,5]. Several reports have emphasised “pelvicalyceal encasement” as a suggestive pattern only in the appropriate haematological context, while acknowledging that it is non-specific outside that context [3,4]. In our case, the renal lesion showed infiltrative peripelvic involvement with pelvic dilatation, raising a high-stakes differential diagnosis, but biopsy was not feasible and carried an unacceptably high haemorrhagic risk in the setting of marked pancytopenia [3,4,5]. Imaging with [18F]fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography ([18F]-FDG-PET/CT) is frequently used to investigate occult infection, inflammatory disease, or malignancy, and it may be helpful to identify highly glycolytic tumours such as aggressive lymphoma [6,7]. However, FDG uptake in EMH is variable and non-specific [2,7,8]. In our patient, the thoracic paravertebral and presacral masses showed only faint uptake, while the renal peripelvic component remained metabolically indeterminate because urinary activity limited assessment, maintaining diagnostic uncertainty [2,7,8]. This “grey zone” is precisely where marrow- or reticuloendothelial-targeted tracers become valuable. Reticuloendothelial or marrow-targeting radiotracers can provide direct evidence of functioning haematopoietic tissue at ectopic sites. Technetium-99m-labelled colloids ([99m]Tc-sulphur colloid) are widely used and provide direct functional evidence of ectopic haematopoietic/reticuloendothelial tissue [2,9]. A contemporary radiology review highlights marrow and reticuloendothelial tracers as confirmatory tools for EMH, with hybrid SPECT/CT improving anatomical correlation and diagnostic confidence, particularly for deep lesions or those adjacent to physiological uptake [2,9]. In myelofibrosis, colloid SPECT/CT has been used to assess marrow distribution and support EMH when uptake is demonstrated at ectopic sites [10]. In our case, [99m]Tc-sulphur colloid SPECT/CT demonstrated concordant uptake with the paravertebral, presacral and renal lesions identified on the [18F]-FDG-PET/CT, confirming multifocal EMH. This multimodality approach is clinically relevant because biopsy is often unsafe: EMH lesions can be vascular, and thrombocytopenia or platelet dysfunction in myelofibrosis increases the haemorrhagic risk of sampling perihilar or peripelvic renal lesions [1,3,4,5]. Renal peripelvic involvement may also have immediate management implications through obstruction; ureteric stenting is a standard decompressive option when hydronephrosis/pelvic dilatation is present [11]. More broadly, treatment targets the underlying haematological disorder and may include transfusion support, immunosuppression and thrombopoietin-receptor agonists in immune-mediated marrow failure syndromes, with allogeneic HSCT reserved for selected patients and offering curative potential in myelofibrosis [12,13,14]. In conclusion, renal peripelvic EMH is an exceptional but important diagnostic pitfall that can closely resemble infiltrative malignancy on CT. In cytopenic patients in whom biopsy is high risk, [18F]-FDG-PET/CT and [99mTc]-sulphur colloid SPECT/CT offer robust non-invasive confirmation and can guide management.
Figure 3.
[99mTc]-sulphur colloid scintigraphy with SPECT/CT. (A, B) Whole-body planar images (anterior/posterior) are displayed with intensity scaled to optimise skeletal activity; prominent hepatic and splenic uptake is seen in the context of hepatosplenomegaly. Diffuse, heterogeneous skeletal tracer distribution is consistent with extensive active marrow involvement (black arrows). (C) Axial SPECT images show tracer uptake within the thoracic paravertebral soft-tissue masses (orange arrow, upper panel), the left peripelvic/pelvicalyceal infiltrative lesion (red arrow, middle panel), and the presacral infiltrative lesion (orange arrow, lower panel). (D) Fused SPECT/CT images confirm concordant radiotracer uptake within the paravertebral and presacral soft-tissue infiltrates (orange arrows) and including the left peripelvic/pelvicalyceal lesion (red arrow). Overall, the concordant colloid uptake across all lesions supported multifocal EMH, providing a non-invasive alternative when tissue sampling is high risk. Given the left pelvicalyceal involvement with pelvic dilatation, a double-J ureteric stent was inserted. The patient required transfusion support and received anti-thymocyte globulin plus ciclosporin, with adjunct thrombopoietin-receptor agonists (romiplostim and eltrombopag), before proceeding to allogeneic haematopoietic stem-cell transplantation, with favourable clinical and haematological recovery. Extra-medullary haematopoiesis (EMH) is a recognised compensatory phenomenon in chronic anaemias and myeloid neoplasms, particularly primary myelofibrosis and related myeloproliferative neoplasms. However, clinically relevant mass-forming EMH at atypical sites remains uncommon and frequently mimics malignancy or infection on anatomical imaging [1,2]. The diagnostic challenge is further compounded when EMH occurs in non-reticuloendothelial organs, where tumour-like deposits may be misinterpreted as lymphoma, metastatic disease, inflammatory pseudo-tumour, or chronic infection, resulting in invasive procedures that can be hazardous for cytopenic patients [1,2]. Renal EMH is particularly rare and represents a key imaging pitfall. Reported patterns include perinephric plaques, renal hilar/perihilar masses, and infiltrative soft-tissue encasement of the renal sinus and pelvicalyceal system, sometimes extending to the proximal ureter and potentially causing obstruction or renal dysfunction [3,4,5]. Several reports have emphasised “pelvicalyceal encasement” as a suggestive pattern only in the appropriate haematological context, while acknowledging that it is non-specific outside that context [3,4]. In our case, the renal lesion showed infiltrative peripelvic involvement with pelvic dilatation, raising a high-stakes differential diagnosis, but biopsy was not feasible and carried an unacceptably high haemorrhagic risk in the setting of marked pancytopenia [3,4,5]. Imaging with [18F]fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography ([18F]-FDG-PET/CT) is frequently used to investigate occult infection, inflammatory disease, or malignancy, and it may be helpful to identify highly glycolytic tumours such as aggressive lymphoma [6,7]. However, FDG uptake in EMH is variable and non-specific [2,7,8]. In our patient, the thoracic paravertebral and presacral masses showed only faint uptake, while the renal peripelvic component remained metabolically indeterminate because urinary activity limited assessment, maintaining diagnostic uncertainty [2,7,8]. This “grey zone” is precisely where marrow- or reticuloendothelial-targeted tracers become valuable. Reticuloendothelial or marrow-targeting radiotracers can provide direct evidence of functioning haematopoietic tissue at ectopic sites. Technetium-99m-labelled colloids ([99m]Tc-sulphur colloid) are widely used and provide direct functional evidence of ectopic haematopoietic/reticuloendothelial tissue [2,9]. A contemporary radiology review highlights marrow and reticuloendothelial tracers as confirmatory tools for EMH, with hybrid SPECT/CT improving anatomical correlation and diagnostic confidence, particularly for deep lesions or those adjacent to physiological uptake [2,9]. In myelofibrosis, colloid SPECT/CT has been used to assess marrow distribution and support EMH when uptake is demonstrated at ectopic sites [10]. In our case, [99m]Tc-sulphur colloid SPECT/CT demonstrated concordant uptake with the paravertebral, presacral and renal lesions identified on the [18F]-FDG-PET/CT, confirming multifocal EMH. This multimodality approach is clinically relevant because biopsy is often unsafe: EMH lesions can be vascular, and thrombocytopenia or platelet dysfunction in myelofibrosis increases the haemorrhagic risk of sampling perihilar or peripelvic renal lesions [1,3,4,5]. Renal peripelvic involvement may also have immediate management implications through obstruction; ureteric stenting is a standard decompressive option when hydronephrosis/pelvic dilatation is present [11]. More broadly, treatment targets the underlying haematological disorder and may include transfusion support, immunosuppression and thrombopoietin-receptor agonists in immune-mediated marrow failure syndromes, with allogeneic HSCT reserved for selected patients and offering curative potential in myelofibrosis [12,13,14]. In conclusion, renal peripelvic EMH is an exceptional but important diagnostic pitfall that can closely resemble infiltrative malignancy on CT. In cytopenic patients in whom biopsy is high risk, [18F]-FDG-PET/CT and [99mTc]-sulphur colloid SPECT/CT offer robust non-invasive confirmation and can guide management.
Author Contributions
Conceptualization: RS; methodology: RS and AJ; software; RS, AC, SZ, MZ and TS; validation: RS, TS and PF; formal analysis: AJ; investigation: RS, AJ, SZ ; resources: RS, AC and TS; writing-original draft preparation: RS and AJ; writing-review and editing; RS and AJ supervision: PF. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not receive ethical review and approval due to the nature of the research (Interesting Image).
Informed Consent Statement
Written informed consent was obtained from the patient. The consent form was obtained on 20 February 2026.
Data Availability Statement
The data used and analysed in this study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Malla S, Razik A, Das CJ, Naranje P, Kandasamy D, Kumar R. Marrow outside marrow: imaging of extramedullary haematopoiesis. Clin Radiol. 2020;75(8):565-578. [CrossRef]
- Roberts AS, Shetty AS, Mellnick VM, Pickhardt PJ, Bhalla S, Menias CO. Extramedullary haematopoiesis: radiological imaging features. Clin Radiol. 2016;71(9):807-814. [CrossRef]
- Gryspeerdt S, Oyen R, Van Hoe L, Baert AL, Boogaerts M. Extramedullary hematopoiesis encasing the pelvicalyceal system: CT findings. Ann Hematol. 1995;71(1):53-56. [CrossRef]
- La Fianza A, Torretta L, Spinazzola A. Extramedullary hematopoiesis in chronic myelofibrosis encasing the pelvicaliceal system and perirenal spaces: CT findings. Urol Int. 2005;75(3):281-284. [CrossRef]
- Galperin-Aizenberg M, Volchek Y, Even-Sapir E, Vasserman M, Maizlin ZV, Cohenpour M, et al. Renal extramedullary haematopoiesis mimicking renal lymphoma on computed tomography. Clin Radiol. 2006;61(10):896-898. [CrossRef]
- Boellaard R, Delgado-Bolton R, Oyen WJG, Giammarile F, Tatsch K, Eschner W, et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging. 2015;42(2):328-354. [CrossRef]
- Van Son PM, Evers D, Aarntzen EHJG. The value of FDG-PET CT scans to evaluate bone marrow in haemato-oncological conditions. Neth J Med. 2019;77(7):234-242.
- Dahlsgaard-Wallenius SE, Juul-Jensen K, Nielsen AL, Hildebrandt MG. Extramedullary hematopoiesis visualized on FDG-PET/CT in a patient with beta-thalassemia. Nucl Med Mol Imaging. 2022;56(6):328-330. [CrossRef]
- Yang M, Roarke M, Kelly J, et al. Diffuse pulmonary extramedullary hematopoiesis in myelofibrosis diagnosed with technetium-99m sulfur colloid bone marrow scintigraphy and single photon emission computerized tomography/CT. Am J Hematol. 2017;92(3):323-324. [CrossRef]
- Ojeda-Uribe M, Morel O, Ungureanu C, et al. Assessment of sites of marrow and extramedullary hematopoiesis by hybrid imaging in patients with primary myelofibrosis. Cancer Med. 2016;5(9):2378-2384. [CrossRef]
- Zul Khairul Azwadi I, Norhayati MN, Abdullah MS. Percutaneous nephrostomy versus retrograde ureteral stenting for acute upper obstructive uropathy: a systematic review and meta-analysis. Sci Rep. 2021 Mar 23;11(1):6613. [CrossRef]
- Townsley DM, Scheinberg P, Winkler T, et al. Eltrombopag added to standard immunosuppression for aplastic anemia. N Engl J Med. 2017 Apr 20;376(16):1540-1550. [CrossRef]
- Lee JW, Lee SE, Jung CW, et al. Romiplostim in patients with refractory aplastic anaemia previously treated with immunosuppressive therapy: a dose-finding and long-term treatment phase 2 trial. Lancet Haematol. 2019 Nov;6(11):e562-e572. [CrossRef]
- Kröger N, Bacigalupo A, Barbui T, et al. Indication and management of allogeneic haematopoietic stem-cell transplantation in myelofibrosis: updated recommendations by the EBMT/ELN International Working Group. Lancet Haematol. 2024 Jan;11(1):e62-e74. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



