Submitted:
20 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
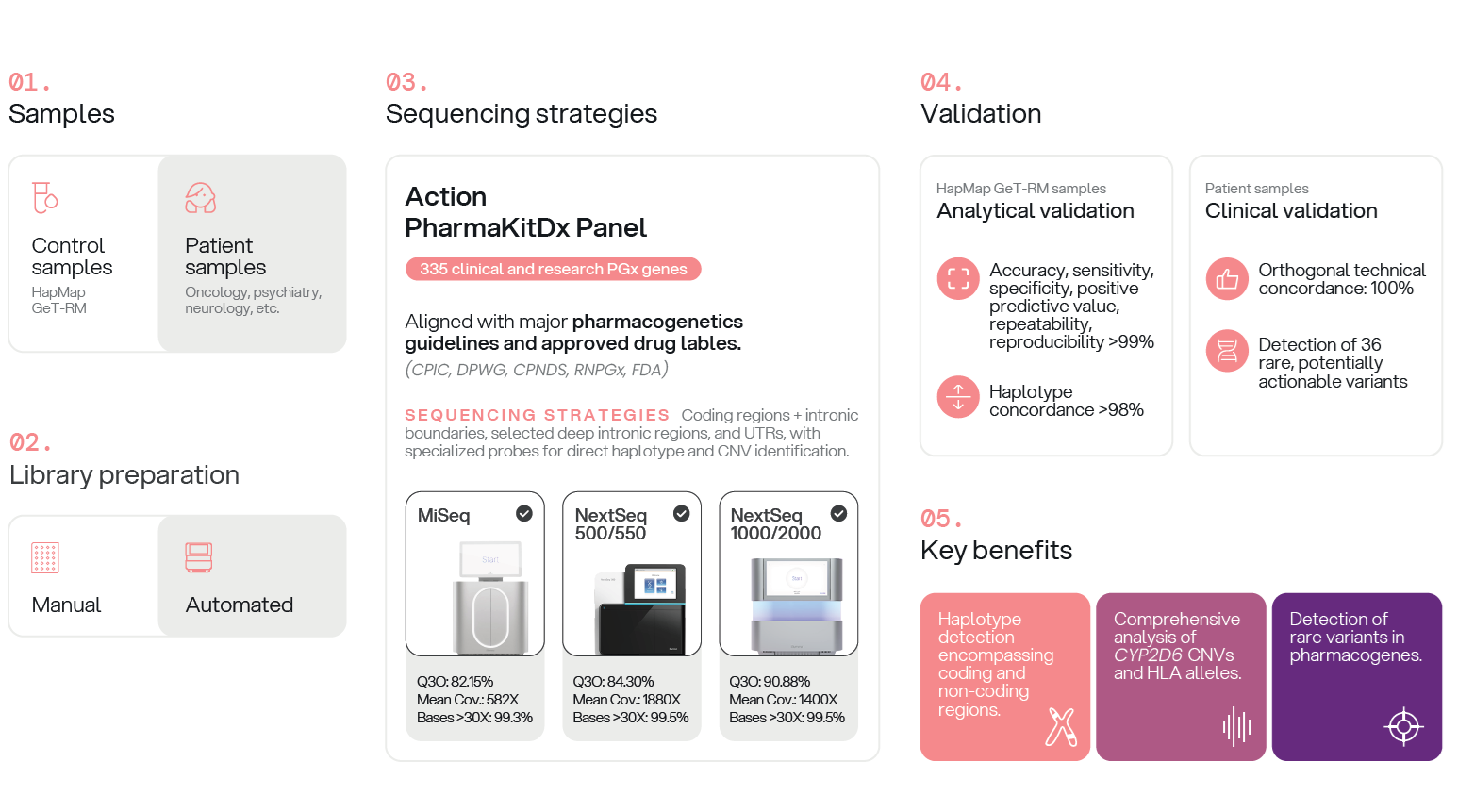
Background/Objectives: Pharmacogenomics (PGx) enables personalized therapy by identifying genetic variants that influence drug response. Despite the advantages of next-generation sequencing (NGS), few clinically validated, guideline-aligned panels comprehensively detect common, rare, and structurally complex pharmacogenetic variants. Methods: We developed and analytically validated Action PharmaKitDx, a targeted NGS panel covering 335 pharmacogenes, including all priority genes recommended by CPIC, DPWG, and CPNDS. Performance was assessed using Coriell HapMap and GeT-RM reference materials across multiple library preparation workflows and Illumina platforms. Clinical feasibility was evaluated in 41 patient samples from diverse specialties. Results were compared with established reference methods, including PCR-based assays, STR analysis, Sanger sequencing, and whole-exome sequencing. Results: More than 99% of target bases achieved ≥30× coverage. Analytical accuracy, sensitivity, specificity, and positive predictive value exceeded 99.3%, with repeatability and reproducibility >99.7%. Concordance with GeT-RM haplotypes reached 98% after star-allele harmonization. The panel accurately detected complex variants, including CYP2D6 copy-number changes and hybrid alleles. Full concordance with prior genotyping was observed in clinical samples. Beyond the initial testing indication, each sample harbored a mean of six actionable variants (range 2–10). Thirty-six rare (minor allele frequency <1%) potentially actionable variants were additionally identified. Conclusions: Action PharmaKitDx demonstrates high analytical performance and broad clinical applicability, supporting its implementation as a scalable solution for comprehensive pharmacogenetic testing and precision prescribing.
Keywords:
pharmacogenomics
; next-generation sequencing
; clinical pharmacogenetics
; drug metabolism
; precision medicine
; clinical validation
; analytical validation
; Cytochrome p-450 enzyme system
; copy number variation
1. Introduction
Pharmacogenomics (PGx) explores how genetic variation influences drug response and has become a key pillar of personalized medicine. By identifying variants that affect drug metabolism, transport, or targets, PGx enables clinicians to optimize therapies to maximize safety and efficacy [1]. Advances in genomic technologies—most notably next-generation sequencing (NGS)—have accelerated the integration of genomics into clinical practice by enabling comprehensive and cost-effective analysis of multiple drug-related genes simultaneously [2,3]. Unlike traditional genotyping methods such as PCR-based assays or microarrays, NGS allows for the detection of both common and rare variants with high sensitivity and specificity [4]. This is particularly relevant as recent evidence suggests that rare variants in pharmacogenes may be more prevalent than previously recognized and can have significant functional implications, impacting drug efficacy or toxicity in ways not captured by standard panels focused only on frequent alleles [5].
Importantly, NGS also enables the detection of complex structural variants and haplotypes in pharmacogenes with intricate genomic architectures, such as CYP2D6. The ability to characterize duplications, deletions, and hybrid alleles is essential for accurate genotype-to-phenotype translation in these loci [6,7,8]. By comparison, whole-exome sequencing (WES) is poorly suited to PGx applications because it often fails to cover key non-coding regulatory variants with known clinical relevance [9,10]. For instance, CYP2C19*17, located in the promoter region, increases gene transcription and leads to ultrarapid metabolism of drugs such as clopidogrel; missing this variant can result in inappropriate dosing and elevated bleeding risk. Similarly, UGT1A1*28 in the promoter affects bilirubin clearance and irinotecan toxicity, and VKORC1 intronic variants strongly influence warfarin sensitivity. These clinically actionable variants are typically outside the exonic regions targeted by WES, making exome-based approaches incomplete for comprehensive pharmacogenomic profiling. While whole-genome sequencing (WGS) may overcome these limitations by offering uniform coverage across the genome, its high cost and complex data interpretation currently limit its feasibility for routine clinical use. Overall, targeted NGS panels based on hybridization capture strike an optimal balance between analytical depth, clinical relevance, and cost-effectiveness, making them particularly well-suited for PGx testing in real-world settings [11,12].
Despite the technical benefits, there is a notable lack of clinically validated NGS kits specifically designed to meet the requirements of pharmacogenomics laboratories. Many commercial panels do not provide adequate coverage of guideline-recommended variants, lack structural variant detection, or are tailored to research rather than clinical diagnostics. This gap has hindered the broader implementation of PGx in healthcare, despite strong evidence supporting its clinical utility [13] Large cohort studies and clinical trials have shown that over 95% of individuals carry at least one actionable PGx variant, and that pharmacogenomic-guided prescribing reduces adverse drug reactions and healthcare costs [5,14,15]. There is thus an urgent need for scalable, robust, and clinically integrated PGx platforms that not only adhere to scientifically accepted guidelines but also align with national health authority frameworks and current clinical recommendations to ensure regulatory compliance and real-world applicability.
To address the need for a comprehensive NGS-based pharmacogenomics solution, the Action PharmaKitDx panel was carefully designed to encompass genetic variants relevant to drug response, including those recommended by major clinical guidelines—such as the Clinical Pharmacogenetics Implementation Consortium (CPIC) and the Dutch Pharmacogenetics Working Group (DPWG)—and FDA drug labels [16,17]. The development also ensures full alignment with current Spanish and European regulatory frameworks. It incorporates the pharmacogenomic biomarkers listed in the AEMPS’s official database, which reflects inclusion criteria from the National Health System’s genomic services portfolio approved in June 2023, and adheres to EMA’s Guideline on Good Pharmacogenomic Practice, which mandates robust methodology, validation, and clinical interpretation standards for germline genomic assays. The current version complies with the In Vitro Diagnostic Directive (IVDD) and is CE-marked under this framework, reinforcing analytical validity and regulatory robustness. The primary objective of this study was to validate the analytical performance of Action PharmaKitDx—including sensitivity, specificity, repeatability, and reproducibility—and to assess its clinical feasibility for implementation in routine pharmacogenetic testing, in line with these regulatory and clinical integration goals.
2. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
2.1. Sequencing Performance
Sequencing performance was assessed across four workflow configurations: manual library preparation on the MiSeq system, automated library preparation on the MiSeq system, and fully automated workflows using either the NextSeq 500/550Dx or the NextSeq 1000/2000 platforms. In all cases, library loading was optimized to ensure sufficient clusters passing filter, enabling coverage of more than 98% of bases at depths exceeding 30X.
In the manual MiSeq workflow, the mean Q30 score reached 82.15%, with an average coverage of 582x and 99.3% of bases covered at greater than 30x depth. The automated MiSeq workflow improved these metrics, yielding a mean Q30 of 93.4%, 89.1% of clusters passing filter, an average coverage of 926x, and 99.4% of bases exceeding 30x.
In the fully automated workflows, the NextSeq 500/550 system generated a mean Q30 of 84.3% and 89.4% clusters passing filter. On the NextSeq 1000/2000 system, sequencing performance included a mean Q30 of 90.9% and a total output of 41.3 Gb. Both NextSeq platforms achieved higher mean sequencing depths – 1880x on the NexSeq 500/550 and 1400x on the NextSeq 1000/2000- with more than 99.5% of bases covered at depths greater than 30x.
2.2. Analytical Performance
The analytical performance of the Action PharmaKit panel was evaluated using three well-characterized reference DNA samples (NA12878, NA12891, and NA12892) (Table 1).
Across all workflows, analytical specificity (NPA) and PPV were greater than 99.9%, demonstrating the absence of false-positive variant calls within the panel’s target regions. Analytical accuracy and sensitivity were consistently high, with mean values exceeding 99.3% for all workflows.
In the manual MiSeq workflow, mean analytical accuracy and sensitivity were 99.9% and 99.4%, respectively, with mean repeatability and reproducibility averaging 99.07%. The automated MiSeq workflow achieved optimal performance, achieving 100% across all metrics for all reference samples. In the NextSeq 500/550 platform, mean analytical accuracy and sensitivity were 99.9% and 99.8%, respectively, with repeatability and reproducibility of 99.8%. Similarly, the NextSeq 1000/2000 workflow yielded uniformly high performance across all metrics, with analytical accuracy, sensitivity, repeatability, and reproducibility each reaching 99.9%.
Observed differences in sensitivity and concordance were attributable to variant calls detected by the pipeline that did not meet predefined quality and/or coverage thresholds. Importantly, all pharmacogenetically relevant positions included in the panel were consistently detected across workflows and sequencing runs, supporting the robustness of the assay for clinical pharmacogenetic applications.
2.3. Pharmacogenetic Haplotypes
To evaluate the accuracy of pharmacogenetic haplotype and genotype calling, the 20 previously described Coriell GeT-RM reference samples were analyzed. Concordance was defined as the proportion of haplotypes identically assigned by the Action PharmaKitDx workflow and the GeT-RM reference dataset. This analysis was performed across 16 pharmacogenes included in the Action PharmaKitDx core panel and characterized by the GeT-RM program: CYP1A2, CYP2B6, CYP2C9, CYP2C19, CYP2D6, CYP3A4, CYP3A5, CYP4F2, DPYD, NAT2, SLCO1B1, TPMT, UGT1A1, VKORC1, HLA-A, and HLA-B.
Across 250 allele-level genotype calls, the initial concordance with the GeT-RM reference was 91.2%. Most discrepancies (6.8%) were attributable to differences in the star-allele definitions used by Action PharmaKitDx and the GeT-RM reference materials. Of these, 2.8% occurred because Action PharmaKitDx reported star alleles not defined or represented in the GeT-RM datasets, whereas 4.0% corresponded to alleles present in GeT-RM but not included in the allele database implemented by Action PharmaKitDx.
In cases where Action PharmaKitDx used narrower or incomplete allele definitions, manual review of the underlying variant calls allowed unclassified or partially defined alleles to be reassigned to the correct star allele. This reduced the discordance rate to 2% and increased the overall concordance to 98%.
Given the well-known complexity of the CYP2D6 locus due to frequent structural rearrangements—including gene whole gene deletions (CYP2D6*5), gene duplications (*1xN, *2xN, etc.), and hybrid alleles (CYP2D6/CYP2D7 and CYP2D7/CYP2D6 conversions) —an additional concordance analysis was performed using a graphical visualization tool that displays the relative depth of coverage for each CYP2D6 exon in the test sample compared to an internal control, supporting the identification and classification of duplications and deletions (Figure 1). All known duplications, deletions, and hybrid alleles present in the reference materials were correctly identified and annotated by the pipeline.
2.4. Clinical Feasibility
To further evaluate the clinical feasibility of Action PharmaKitDx, a retrospective analysis was performed on 41 patient samples obtained from several participating hospitals. These samples had been previously genotyped using established and validated clinical laboratory methodologies, including allelic discrimination PCR, fluorescent PCR for copy number analysis, short-tandem-repeat (STR) analysis, sanger sequencing, and whole-exome sequencing. The panel demonstrated complete concordance in allele-level distribution (100%) when compared with the reference genotypes generated using these methods. The results derived from this comparative analysis are summarized in Table 2.
Each of the clinical samples included in the study corresponded to a real diagnostic request intended to support therapeutic decision-making in diverse pharmacogenetic contexts, thereby providing a representative collection of use-cases reflective of routine clinical practice. The distribution of clinical indications and associated pharmacogenes is presented in Table 3.
The oncology group represented the largest clinical category (n = 16), encompassing patients treated with fluoropyrimidines, irinotecan, or tamoxifen. Action PharmaKitDx accurately identified clinically relevant variants in DPYD (rs3918290 (*2A), rs75017182+ rs56038477 (HapB3), rs67376798 (D949V), rs55886062 (*13)) and UGT1A1 (*28, *37, and c.1220_1221insG). These variants are strongly associated with severe toxicity or altered drug metabolism. For instance, samples 23U15557, 23S15558, 23U15560, 23T11744, and 23U11749 harbored actionable genotypes consistent with prior genotyping results. Additional samples from another hospital (24R11022, 24P11023, 24W11025) were analyzed as DPYD controls, confirming heterozygosity for key deleterious variants. Similarly, UGT1A1 testing in cases 24V11017, 24T11018, 24R11019, and 24V11020 validated the detection of *28, *37, and insertion alleles, demonstrating the panel’s capacity to detect structural and promoter variants. The panel also confirmed CYP2D6 alleles in a breast cancer patient receiving tamoxifen (23R15570). All findings were consistent with reference methods, confirming analytical reliability in oncopharmacogenetic applications.
The second most frequent indication was the optimization of psychotropic therapy in patients with affective or psychotic disorders (n = 10). In this group, variants in CYP2D6, CYP2C19, CYP2C9, CYP1A2, and CYP3A4 were analyzed to explain suboptimal response or adverse drug reactions to antidepressants and antipsychotics. Relevant genotypes included CYP2D6 poor or intermediate metabolizer alleles (*3, *4, *5, *6, *9, *10, *17, *41, and gene duplications), CYP2C19 alleles conferring reduced (*2) or increased (*17) activity, and regulatory variants in CYP1A2 (*1C, *1F). For example, samples 23V15555, 23Q15562, 23Z15563, and 23R15570 carried combinations of these alleles that explained altered metabolism of psychotropic drugs. All results were fully concordant with those obtained by conventional methods.
Within neurology (n = 7), samples from patients undergoing evaluation prior to siponimod therapy were analyzed for CYP2C9 genotype, which determines both dosage adjustment and eligibility for treatment. Action PharmaKitDx accurately identified CYP2C9 genotypes *1/*1, *1/*2, *1/*3, *2/*3, and *3/*3 across samples 23R11745, 23Z11738, 23Q11740, 23W11751, 24U11012, 24S11013, and 24X11016, showing complete concordance with Sanger sequencing.
In gastroenterology (n = 3), patients treated with thiopurines were genotyped for TPMT and NUDT15 to evaluate hematological toxicity risk. The panel identified clinically actionable variants such as TPMT *3B, *3C and *NUDT15*3 (samples 23T15566, 23R15567, 23Y15569), consistent with prior results.
The transplantation subgroup (n = 2) comprised heart transplant recipients under tacrolimus therapy. CYP3A5 expressor (*1) and non-expressor (*3, *7) alleles were detected with complete concordance with the reference assays (samples 23Q15559, 23V15565).
Finally, several individual cases addressed diverse clinical contexts. These included CYP2C19 analysis for omeprazole resistance (sample 23Y11750), CYP2C9 genotyping for NSAID hypersensitivity (sample 23Q11754), CYP2D6 testing for cardiovascular drug reactions (sample 23V11743), and detection of a pathogenic RYR1 nonsense variant (c.7858C>T, p.Gln2620*) in a patient with epilepsy treated with clobazam (sample 24S11027).
Beyond concordance with targeted clinical requests, analysis of these clinical samples with the NGS panel revealed additional actionable findings across other genes included in Action PharmaKitDx. On average, each sample carried 6 actionable variants (range: 2–10), suggesting a broader potential utility of comprehensive pharmacogenetic profiling compared with single-gene approaches. Moreover, a total of 36 rare potentially actionable variants were identified (. Variants were considered “rare” when presenting a minor allele frequency <1% across population databases (gnomAD, ExAC, 1000G, 5000G and dbSNP) and meeting quality thresholds (depth ≥30 and high base quality). Candidate variants were further restricted to those with predicted functional relevance, including non-synonymous coding changes, frameshift or truncating variants, and splicing alterations, supported when applicable by computational predictors (DANN, FATHMM, MutationTaster) or non-benign ClinVar annotations (Table S1). The complete filtering and prioritization strategy applied to identify these variants is described in detail in the Appendix A. This streamlined filtering demonstrates the panel’s ability not only to validate clinically expected variants but also to reveal additional rare alleles with potential clinical significance.
Overall, Action PharmaKitDx demonstrated full concordance with previously established methods across all 41 clinical samples, while simultaneously providing a richer spectrum of pharmacogenomic information. The ability to detect both common guideline-recommended variants and rare alleles underscores its reliability, comprehensiveness, and adds clinical value. These results support its applicability for pharmacogenetic testing across multiple therapeutic domains, including psychiatry, oncology, transplantation, gastroenterology, neurology, and cardiology, and point to its promise as a tool for more holistic pharmacogenomic implementation in clinical practice.
3. Discussion
Next-generation sequencing (NGS) has become a transformative technology for pharmacogenetic (PGx) testing, offering capabilities that extend far beyond the constraints of traditional single-nucleotide variant (SNV) genotyping panels. By enabling simultaneous detection of rare and clinically relevant variants, complex structural variants, hybrid alleles, gene deletions or duplications, and full haplotypes, NGS provides a level of genomic resolution that is essential for accurate phenotype prediction and therapeutic decision-making in PGx. This comprehensive variant detection is particularly impactful for pharmacogenes with highly polymorphic architectures—such as CYP2D6, CYP2B6, CYP2C19, and UGT1A1—where conventional methods often fail to resolve complex allele configurations or star-allele diplotypes (Gulilat et al., 2019; M. van der Lee et al., 2020).
In this study, the Action PharmaKitDx panel was validated as a targeted NGS solution specifically engineered to address the inherent complexities of pharmacogenomic analysis. The panel integrates broad genomic coverage with high analytical accuracy, enabling robust identification of SNVs, indels, copy-number alterations, gene conversions, and allele-level haplotypes. This design allows reconstruction of clinically actionable star-allele diplotypes across multiple pharmacogenes, ensuring reliable phenotype assignment and enhancing the clinical utility of PGx testing.
The following sections detail the panel’s design, sequencing performance, analytical validation, bioinformatic strategies for haplotype resolution, and the clinical implications of deploying a comprehensive NGS-based approach in routine pharmacogenomic practice, in comparison with previously reported NGS-enabled PGx assays.
Genomic Coverage and Design Strategies
Action PharmaKitDx provides extensive genomic coverage, encompassing 335 drug-related genes organized into 20 primary loci, 11 secondary loci, and 304 candidate loci. This scope exceeds that of most targeted PGx panels currently available, such as ClinPharmSeq (59 genes) and PGRNseq (84 genes, with 82 genes retained in the final analysis), and is comparable in breadth to the ADME panel described by Klein et al. (340 genes).(Bush et al., 2016; Klein et al., 2019; S. B. Lee et al., 2022). The design incorporates full coding regions, exon–intron boundaries, selected deep intronic regions, untranslated regions (UTRs), and clinically relevant hotspots across 307 genes. In addition, specialized probes enable direct haplotype identification in complex pharmacogenes such as CYP2D6 and HLA. This hybrid approach resembles that of ClinPharmSeq, which combines an exon-centered design with custom capture of highly polymorphic loci, and that of PGRNseq, which extends sequencing to upstream and downstream UTR regions. (Bush et al., 2016; S. B. Lee et al., 2022) Inclusion of pseudogenes and extragenic regulatory regions is essential, as functionally relevant variants—such as those in CYP2D6 or CYP2C19—can be missed by whole-exome sequencing (WES) (Chua et al., 2016; G. McInnes et al., 2020).
Sequencing Performance and Coverage
The panel demonstrated robust sequencing performance, with mean depths of 582× to 1880× depending on the Illumina platform, and >99% of targeted bases covered at ≥30×. These values are comparable or superior to other targeted approaches. ClinPharmSeq reported an average depth of 274× with 94.8% of bases covered ≥30×, while PGRNseq achieved 200× in the eMERGE-PGx dataset and 496× in HapMap96 samples.(Bush et al., 2016; Gordon et al., 2016; S. B. Lee et al., 2022) High and uniform coverage is critical for reliable detection of rare variants and SVs, which are increasingly recognized as clinically relevant in PGx.(Ingelman-Sundberg et al., 2018)
Analytical Accuracy and Validation
Validation of Action PharmaKitDx showed 100% sensitivity for SNVs and indels, with specificity ranging from 99.99% to 100%. Repeatability and reproducibility exceeded 99.7%. Concordance with GeT-RM reference materials was 98%. Notably, the panel correctly identified all known CYP2D6 duplications, deletions, and hybrids—a major challenge in PGx due to the locus’s structural complexity. Comparatively, ClinPharmSeq demonstrated 96.3% concordance with WGS data and >97% concordance with previously reported diplotypes, while Klein et al.’s ADME panel and PGRNseq both reported >99% concordance with independent datasets. (Bush et al., 2016; Gordon et al., 2016; Klein et al., 2019; S. B. Lee et al., 2022) High Collectively, these findings underscore the analytical robustness of targeted NGS for PGx.
Bioinformatics and Clinical Interpretation
The analytical strength of Action PharmaKitDx is further enhanced by its customized bioinformatics pipeline. This includes CYP2D6-specific filtering to distinguish pseudogene alignments (CYP2D7/8), depth normalization, and dedicated modules for HLA-B allele inference.(Nofziger et al., 2020; Wittig et al., 2015) Haplotypes are resolved through an in-house algorithm integrating allele–variant translation tables from PharmGKB and PharmVar.(Gaedigk et al., 2019; Whirl-Carrillo et al., 2021). Comparable pipelines, such as ClinPharmSeq’s use of PyPGx for star allele calling and SV detection, also highlight the importance of tailored bioinformatics in PGx, especially for loci with high structural complexity. (S. B. Lee et al., 2022)
Clinical Validation with Patient Samples
A major strength of this study is the validation of the panel using 41 clinical samples derived from real therapeutic contexts across psychiatry, oncology, transplantation, gastroenterology, neurology, and cardiology. Each sample had previously been genotyped using established methods (STR analysis of (TA)n promoter repeat; Sanger sequencing; whole-exome sequencing, allelic-discrimination assays and other PCR-based genotyping methods), enabling direct assessment of concordance. Action PharmaKitDx confirmed all reported genotypes, including clinically relevant star allele combinations and structural variants. Importantly, the panel proved its robustness across diverse clinical scenarios.
Detection of Rare and Additional Variants
Beyond confirming known variants, the panel revealed additional actionable findings beyond the scope of initial clinical requests. On average, each sample carried 6 actionable variants (range: 2–10), suggesting that a multigene approach may provide broader clinical insights than single-gene testing. This figure is higher than the mean of 3.7 non-typical response pharmacogene alleles per subject reported in the UK Biobank cohort (G. M. McInnes et al., 2021) which may reflect differences in panel design, allele classification criteria, and the clinical enrichment of our sample set. Moreover, 36 rare potentially actionable variants were identified in candidate genes, expanding the spectrum of PGx-relevant alleles. This supports previous observations that rare variants account for a substantial fraction of pharmacogenomic diversity and may have significant clinical consequences if functionally characterized. (Bush et al., 2016; Ingelman-Sundberg et al., 2018; Klein et al., 2019; M. van der Lee et al., 2020).
Clinical Implications and Future Perspectives
Prior studies estimate that >90% of individuals carry at least one clinically actionable PGx variant. (G. McInnes et al., 2020) Action PharmaKitDx consistently identified reported genotypes in diverse clinical samples—including complex star allele combinations and gene duplications—across therapeutic contexts such as psychiatry, oncology, and immunosuppression. This highlights its potential as a scalable tool for guiding individualized drug therapy.
Accurate detection of actionable variants is foundational for precision medicine. Action PharmaKitDx demonstrated not only 100% concordance with previously established methods across 41 clinical samples, but also an added ability to uncover additional and rare variants. This dual capacity underscores its reliability and broader clinical value compared to traditional genotyping. By consolidating multiple pharmacogenes into a single comprehensive assay, Action PharmaKitDx may streamline workflows, reduce costs, and improve the implementation of PGx-guided prescribing in routine practice.
Nevertheless, several challenges remain. Short-read NGS cannot phase variants separated by long genomic distances, and while CYP2D6 CNVs were validated, broader assessment of CNVs in other pharmacogenes is warranted.(Santos et al., 2018; Tremmel et al., 2020) The dynamic nature of allele nomenclature requires continuous alignment with PharmVar and CPIC updates.(Gaedigk et al., 2019) Moreover, long-read sequencing technologies (e.g., PacBio, Nanopore) may further improve haplotype resolution and structural variant detection in the future.(Graansma et al., 2023; Holt et al., 2024; Turner et al., 2023).
4. Materials and Methods
Panel Design
The panel was conceived to deliver a comprehensive pharmacogenetic assessment fully aligned with clinical practice. Its design integrates a broad set of genes implicated in drug response, integrating them into the standard framework used for pharmacogenetic evaluation. In addition to the primary actionable genes with the highest levels of evidence for predicting drug efficacy, toxicity, or optimal—those prioritized by leading pharmacogenetics guideline-issuing bodies such as the Clinical Pharmacogenetics Implementation Consortium (CPIC), the Dutch Pharmacogenetics Working Group (DPWG), and the Canadian Pharmacogenomics Network for Drug Safety (CPNDS) [16,17] —the panel also incorporates secondary and candidate genes. Although these genes are not yet fully integrated into formal recommendations, accumulating evidence suggests their potential contribution to pharmacokinetic and pharmacodynamic variability, adverse drug reactions, and dose optimization. Their inclusion ensures that the panel remains forward-looking and adaptable to the evolution of evidence in the field, while preserving methodological robustness and scientific validity.
The panel sequences more than 120,000 nucleotides and encompasses 335 genes organized into three evidence-based categories—priority, secondary, and candidate. Priority genes (21 in total), including ABCG2, CACNA1S, CYP2B6, CYP2C19, CYP2C9, CYP2D6, CYP3A4, CYP3A5, CYP4F2, DPYD, F5, G6PD, HLA-A, HLA-B, IFNL3, NUDT15, RYR1, SLCO1B1, TPMT, UGT1A1, and VKORC1, are consistently endorsed by major pharmacogenetic guidelines and represent the highest level of clinical evidence. Secondary genes (10 in total), such as ABCC3, CALU, COMT, CYP1A2, CYP2C18, GGCX, NAT2, RARG, SLC28A3, and UGT1A6, are supported by moderate evidence and hold relevance for specific drug-gene interactions. Finally, the candidate category a set of 304 genes currently under active investigation for their potential pharmacogenomic impact, ensuring the panel remains forward-looking and adaptable to emerging evidence.
To ensure comprehensive coverage, the panel combines three complementary sequencing strategies. First, it targets entire coding regions along with intronic boundaries, selected deep intronic segments, and untranslated regions (UTRs) to capture key non-coding variants. Second, it incorporates specialized probe sets for direct haplotype resolution in complex loci like CYP2D6 and the HLA gene family. Finally, it enriches genomic regions known to harbor clinically relevant variants documented in peer-reviewed literature and curated databases, reinforcing the panel’s clinical utility and evidence-based design. Detailed information on the capture strategies applied to each gene group, as well as the complete list of genes included in the panel, is provided in the Appendix A.
Sample Selection
A comprehensive dataset of 43 samples was analyzed, encompassing well-characterized reference materials and patient-derived specimens obtained from diverse DNA source matrices. Analytical performance evaluation focused on critical quality metrics, including sensitivity, specificity, off-target read assessment, and sequencing performance indicators such as coverage depth and uniformity. Repeatability and reproducibility were rigorously tested through multiple sequencing runs of reference materials—3 from the Coriell International HapMap Project and 20 from Coriell’s Pharmacogenetics Genetic Testing Reference Materials Coordination Program (GeT-RM)—under varying conditions. Clinical performance evaluation was assessed using 41 patient-derived samples from hospitals within the National Public Health System, selected to represent diverse DNA source matrices and sequencing platforms. This cohort also prioritized clinically relevant haplotypes associated with slow, rapid, and normal metabolizer phenotypes, ensuring real-world applicability. Together, these evaluations provide robust evidence of the panel’s accuracy, reliability, and suitability for routine pharmacogenetic testing.
the analytical validation of the panel, a total of 20 samples were analyzed. The dataset included 3 reference materials from the Coriell International HapMap Project and 20 reference materials from Coriell’s Pharmacogenetics Genetic Testing Reference Materials Coordination Program (GeT-RM). To ensure robust validation, some samples were sequenced multiple times.
DNA Extraction
Genomic DNA was isolated at each participating center using extraction workflows routinely implemented in their laboratories. Although the specific extraction methods varied across institutions, all procedures had been previously validated and were regularly employed in accordance with each center’s internal quality assurance and quality control standards. Prior to library preparation, the extracted DNA underwent quantitative assessment and purity evaluation to verify its integrity and ensure compliance with the quality requirements for downstream next-generation sequencing analyses.
Library Preparation and Next-Generation Sequencing
Between 50-100 ng of genomic DNA from each sample was processed following the Action PharmaKitDx instructions for use employing the SureSelect XT HS library preparation technology (Agilent Technologies, Santa Clara, CA, USA). The protocol included DNA fragmentation, end-repair, adenylation, and ligation of barcoded adapters. Libraries were purified using Agencourt AMPure XP beads (Beckman Coulter) and amplified by conventional PCR. The hybridization of the pre-amplified target regions was performed using custom biotinylated probes specifically designed for this study, followed by target capture with streptavidin-coated beads. The captured libraries were subsequently subjected to stringent wash conditions to remove nonspecific hybrids and then re-amplified by PCR to achieve sufficient enrichment. Library quality control included assessment of fragment size distribution between 200 and 250 base pairs, and quantification to confirm that both metrics met the required specifications for sequencing.
Library preparation was performed using both manual and automated workflows. Manual processing was carried out with the [18], whereas automated preparation was completed using the Magnis NGS Prep System (Agilent Technologies) with the CE-marked configuration Action PharmaKitDx (Health in Code). The automated platform is optimized for high-stringency, walk-away processing and enables parallel preparation of up to eight libraries per run, ensuring procedural consistency and reducing operator-dependent variability.
Sequencing was conducted across several Illumina platforms to accommodate different throughput needs. Runs were performed on the MiSeq System (Reagent Kit v2, 300 cycles) in batches of 8 samples, on the NextSeq 500/550Dx System (Mid Output v2.5, 300 cycles) in batches of 32 samples, and on the NextSeq 1000/2000 using the P2 XLEAP-SBS Reagent Kit (300 cycles), also in batches of 32 samples. Library denaturation and loading procedures were carried out strictly following the manufacturer’s recommendations to ensure optimal cluster generation and sequencing performance.
Bioinformatic Pipeline
Bioinformatic analysis was carried out using a custom pipeline that performs samples demultiplexing and integrates multiple software tools, including NovoAling, GATK (Genome Analysis Toolkit), SAMtools, and BCFtoolds for variant calling and genotyping. Initially, raw NGS reads underwent quality-control filtering to remove low-quality sequences. High-quality reads were then aligned to the GRCh37 reference genome. Haplotype inference was performed using a proprietary algorithm that uses variant-allele translation tables, variant files (vcf format), and coverage data (cov format) obtained from each sample [19]. Variant-allele translation tables were assigned using the PharmGKB and PharmVar databases [20,21]. Appendix A describe the pharmacogenetic alleles supported by the panel, and the complete list of automatically inferred haplotypes.
CYP2D6 analysis was performed using a custom-developed module based on the approaches described in [22,23]. This module filters out alignments originating from CYP2D7 and CYP2D8 to avoid artifacts in coverage plots caused by miss-mapped reads from highly homologous regions. Following this filtering step, read-depth values are normalized using the control sample NA17254, which reduces biases related to copy-number variation (CNV) events in other samples processed within the same sequencing run.
HLA-B allele inference was conducted with a dedicated module implementing the methodology described by Wittig et al. [24], ensuring accurate and reliable HLA-B allele assignment for downstream analysis.
5. Conclusions
In summary, Action PharmaKitDx delivers a step-change in clinical pharmacogenomics by uniting exceptional genomic breadth with deep, uniform sequencing and purpose-built analytics. Covering 335 drug-related genes with targeted capture of complex loci, the panel reliably detects SNVs, indels, copy-number changes, gene conversions, and allele-level haplotypes, resolving challenging architectures such as CYP2D6 with a level of fidelity that conventional genotyping and WES routinely miss. Its analytical performance—including 100% sensitivity for SNVs/indels, near-perfect specificity and reproducibility and 98% concordance with reference materials—coupled with accurate calling of CYP2D6 duplications, deletions, and hybrids, underpins confident genotype-to-phenotype translation. In real-world clinical samples across multiple specialties, Action PharmaKitDx not only confirmed previously reported diplotypes but also revealed additional actionable variants (on average ~6 per case), expanding therapeutic options and informing safer, more individualized pharmacotherapy. Supported by a custom bioinformatics pipeline (CYP2D6-aware alignment and depth normalization, HLA-B inference, and PharmGKB/PharmVar-anchored haplotyping), the platform delivers end-to-end interpretability aligned with contemporary PGx guidance. Compared with legacy panels and WES—and without the cost and operational burden of WGS—Action PharmaKitDx offers immediate clinical and operational value: it streamlines multigene PGx testing into a single, scalable assay, shortens time-to-insight, reduces downstream costs, and differentiates in the pharmacogenetics market through superior coverage of structural and rare variation. Taken together, these attributes position Action PharmaKitDx as a best-in-class, implementation-ready solution for broad deployment of PGx in routine care.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Filtered rare variants.
Author Contributions
Conceptualization, LRC. and MIG.; writing—review and editing, LRC. and MIG.; control sample analysis, MDS. and VCP.; clinical sample analysis, SBN., PRA., ALL., LTJ., VJA., IML, AOH., MM, and MAMP.; supervision, G.C.A. and J.P.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the program for the Promotion of R&D&I Projects aimed at Public Procurement of Innovation of the Agència Valenciana de la Innovació.
Institutional Review Board Statement
The present study was approved by the Galician Committee on Ethics in Medicines Research (Comité de ética de la investigación con medicamentos de Galicia) (CEIm-G ID 2021/149) and complies with the Declaration of Helsinki and its subsequent revisions.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors LRC, MIG, MDS, VCP, GCA, JPP are Health In Code group employees. The other authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADME | Absorption, Distribution, Metabolism, and Excretion |
| AEMPS | Agencia Española de Medicamentos y Productos Sanitarios |
| CNV | Copy Number Variation |
| CPNDS | Canadian Pharmacogenomics Network for Drug Safety |
| CPIC | Clinical Pharmacogenetics Implementation Consortium |
| DPWG | Dutch Pharmacogenetics Working Group |
| EMA | European Medicines Agency |
| FDA | U.S. Food and Drug Administration |
| GeT-RM | Genetic Testing Reference Materials Coordination Program |
| HLA | Human Leukocyte Antigen |
| IVDD | In Vitro Diagnostic Directive |
| NGS | Next-Generation Sequencing |
| NPA | Negative Percent Agreement |
| PCR | Polymerase Chain Reaction |
| PGx | Pharmacogenomics |
| PPA | Positive Percent Agreement |
| PPV | Positive Predictive Value |
| Q30 | Phred Quality Score ≥30 |
| SNV | Single Nucleotide Variant |
| STR | Short Tandem Repeat |
| SV | Structural Variant |
| UTR | Untranslated Region |
| WES | Whole-Exome Sequencing |
| WGS | Whole-Genome Sequencing |
Appendix A. Supplementary Methods
Appendix A.1. Target Enrichment and Capture Design
To balance comprehensive pharmacogenomic coverage with sequencing efficiency, the Action PharmaKitDx assay uses a mixed capture strategy combining three complementary approaches. This design ensures high-resolution analysis in core genes while enabling the detection of targeted variants across an extended pharmacogenomic landscape.
Appendix A.1.1. Full Coding Regions with Extended Intronic and Regulatory Coverage (23 Genes)
- All coding exons
- ±50 bp of flanking intronic sequence
- Selected deep intronic regions containing known pathogenic variants
- Relevant 5′ and 3′ untranslated regions (UTRs)
This strategy maximizes detection of both common and rare functional variants. Genes captured under this strategy include ABCB1, CACNA1S, CYP1A2, CYP2B6, CYP2C19, CYP2C8, CYP2C9, CYP3A4, DPYD, NUDT15, RYR1, SLCO1B1, TPMT, UGT1A1, and additional UGT family members, as well as VKORC1.
Appendix A.1.2. Direct Haplotype Capture for Highly Polymorphic Genes (6 Genes)
For genes where haplotype or allele-level resolution is essential but SNV-based reconstruction is unreliable, the panel uses direct haplotype capture with custom probe sets. This strategy allows accurate classification without relying on individual SNV annotation.
Genes analyzed with this approach:
- CYP2D6
- HLA-B, HLA-C, HLA-DRB1, HLA-E, HLA-G
This ensures reliable detection of copy-number variations, hybrid alleles, and highly polymorphic HLA haplotypes.
Appendix A.1.3. Targeted Capture of Clinically Relevant Loci (307 Genes)
For an additional 307 pharmacogenes, the panel selectively captures:
- Coding exons and selected noncoding regions containing well-established pharmacogenetic variants
- Specific loci documented in curated databases or medical literature
This approach focuses sequencing depth on variants with known or potential clinical relevance while maintaining broad genomic scope.
Appendix A.1.4. Total Gene Content
In total, the panel evaluates 335 pharmacogenes, encompassing drug-metabolizing enzymes, transporters, receptors, immune response genes, and genes associated with adverse drug reactions. The complete list of genes included in the panel is provided in list A1.
ABCB1, ABCB11, ABCB4, ABCB7, ABCC1, ABCC2, ABCC3, ABCC4, ABCC5,
ABCC6, ABCC8, ABCC9, ABCG1, ABCG2, ACE, ACKR1, ACYP2, ADA,
ADD1, ADGRB3, ADGRL2, ADH1A, ADH1B, ADH1C, ADORA2A, ADRB1,
ADRB2, AFF3, AHR, AKR1E2, ALDH1A1, ALDH2, ALOX5, ALPL, AMPD1,
ANKK1, APOA5, APOE, ARL14, ATIC, ATP7A, BDNF, BMP2, BMP7,
BRINP1, BTG1, C11orf65, C1orf167, C8orf34, CACNA1S, CADM2, CALU,
CARD8, CBR3, CCDC179, CCHCR1, CCR5, CD2, CD226, CD69, CD80, CD84,
CD86, CDA, CEP72, CES1, CES2, CETP, CHRNA3, CHRNB2, CHST7,
CHUK, CLEC2D, CLSTN2, CNTN5, COL22A1, COMT, COQ2, CREB1,
CRHR1, CRHR2, CRP, CSMD1, CSMD3, CUL1, CYP17A1, CYP19A1,
CYP1A1, CYP1A2, CYP1B1, CYP2A13, CYP2A6, CYP2B6, CYP2C18,
CYP2C19, CYP2C8, CYP2C9, CYP2D6, CYP2E1, CYP2F1, CYP2J2, CYP2S1,
CYP3A4, CYP3A43, CYP3A5, CYP3A7, CYP4B1, CYP4F2, DCK, DHFR,
DHODH, DLG2, DOCK1, DPP6, DPYD, DRD1, DRD2, DRD3, DRD4,
DYNC2H1, EGF, EGLN3, EMCN, ENOX1, EPHX1, ERCC1, ESR1, ESR2,
ETV1, EYA4, F5, FAAH, FAR1, FCGR2A, FCGR2B, FCGR3A, FDPS, FKBP5,
FLT3, FMO2, FMO3, FOXP3, FPGS, FTO, G6PD, GABBR2, GALNT18,
GATM, GFRA1, GFRA2, GGCX, GGH, GNB3, GP1BA, GRIK4, GSTM1,
GSTP1, GSTT1, HAS3, HLA-A, HLA-B, HLA-C, HLA-DRB1, HLA-E, HLA-G,
HMGCR, HTR1A, HTR2A, HTR2C, HTR3A, IFNG, IFNGR2, IFNL3, IFNL4,
IGHM, IKBKB, IL10, IL12B, IL17A, IL17F, IL18, IL1B, IL1R1, IL2, IL4R, IL6,
IL6R, IRAK3, ITGB7, ITPA, KCNE1, KCNH2, KCNIP1, KCNJ11, KIAA0391,
KIF6, KLRC1, KLRD1, LMO3, LMX1A, LPA, LRPAP1, LRRC55, LTC4S,
MAP2K6, MAP3K1, MAP3K14, MAP3K7, MAPK14, MAPKAPK2, MAPT,
MC4R, MED15, MICA, MMP20, MRPL36, MS4A1, MTHFD1, MTHFR,
MTR, MTRR, MYD88, NAT1, NAT2, NAV2, NEBL, NEDD4L, NFIB,
NFKBIA, NFKBIB, NFKBIE, NLRP3, NQO1, NR1I2, NR2F2, NR3C1, NT5C2,
NTRK2, NUBPL, NUDT15, OPRD1, OPRM1, OR2B11, OSR1, P2RY1,
P2RY12, PDZD2, PLA2G4A, PNPLA3, PRELID3B, PRKCA, PRSS53, PTGFR,
PTGIS, PTGS1, PTGS2, PTPRC, PTPRM, QKI, RAD51B, RHOBTB1,
RPS6KA5, RYR1, SCN1A, SCN5A, SCNN1A, SEMA3C, SHMT1, SLC15A1,
SLC15A2, SLC16A7, SLC19A1, SLC22A1, SLC22A11, SLC22A2, SLC22A6,
SLC28A3, SLC46A1, SLC6A4, SLC9A7, SLCO1A2, SLCO1B1, SLCO1B3,
SLCO1C1, SLCO2B1, SOD2, SP3, SRY, STAT4, STRBP, SULT1A1, SULT1A2,
SYNM, TANC1, TBXAS1, TCF7L2, TEC, TGFB1, TGFBR2, TLR1, TLR10,
TLR2, TLR4, TLR5, TNF, TNFAIP3, TNFRSF1A, TNFRSF1B, TNFSF13B,
TP53, TPMT, TRAF1, TUBB2A, TYMS, UGT1A1, UGT1A10, UGT1A3,
UGT1A4, UGT1A5, UGT1A6, UGT1A7, UGT1A8, UGT1A9, UGT2B10,
UGT2B15, UGT2B17, UGT2B7, UMPS, VDR, VKORC1, WDR27, XPC,
XRCC1, YEATS4, ZNF595.
ABCC6, ABCC8, ABCC9, ABCG1, ABCG2, ACE, ACKR1, ACYP2, ADA,
ADD1, ADGRB3, ADGRL2, ADH1A, ADH1B, ADH1C, ADORA2A, ADRB1,
ADRB2, AFF3, AHR, AKR1E2, ALDH1A1, ALDH2, ALOX5, ALPL, AMPD1,
ANKK1, APOA5, APOE, ARL14, ATIC, ATP7A, BDNF, BMP2, BMP7,
BRINP1, BTG1, C11orf65, C1orf167, C8orf34, CACNA1S, CADM2, CALU,
CARD8, CBR3, CCDC179, CCHCR1, CCR5, CD2, CD226, CD69, CD80, CD84,
CD86, CDA, CEP72, CES1, CES2, CETP, CHRNA3, CHRNB2, CHST7,
CHUK, CLEC2D, CLSTN2, CNTN5, COL22A1, COMT, COQ2, CREB1,
CRHR1, CRHR2, CRP, CSMD1, CSMD3, CUL1, CYP17A1, CYP19A1,
CYP1A1, CYP1A2, CYP1B1, CYP2A13, CYP2A6, CYP2B6, CYP2C18,
CYP2C19, CYP2C8, CYP2C9, CYP2D6, CYP2E1, CYP2F1, CYP2J2, CYP2S1,
CYP3A4, CYP3A43, CYP3A5, CYP3A7, CYP4B1, CYP4F2, DCK, DHFR,
DHODH, DLG2, DOCK1, DPP6, DPYD, DRD1, DRD2, DRD3, DRD4,
DYNC2H1, EGF, EGLN3, EMCN, ENOX1, EPHX1, ERCC1, ESR1, ESR2,
ETV1, EYA4, F5, FAAH, FAR1, FCGR2A, FCGR2B, FCGR3A, FDPS, FKBP5,
FLT3, FMO2, FMO3, FOXP3, FPGS, FTO, G6PD, GABBR2, GALNT18,
GATM, GFRA1, GFRA2, GGCX, GGH, GNB3, GP1BA, GRIK4, GSTM1,
GSTP1, GSTT1, HAS3, HLA-A, HLA-B, HLA-C, HLA-DRB1, HLA-E, HLA-G,
HMGCR, HTR1A, HTR2A, HTR2C, HTR3A, IFNG, IFNGR2, IFNL3, IFNL4,
IGHM, IKBKB, IL10, IL12B, IL17A, IL17F, IL18, IL1B, IL1R1, IL2, IL4R, IL6,
IL6R, IRAK3, ITGB7, ITPA, KCNE1, KCNH2, KCNIP1, KCNJ11, KIAA0391,
KIF6, KLRC1, KLRD1, LMO3, LMX1A, LPA, LRPAP1, LRRC55, LTC4S,
MAP2K6, MAP3K1, MAP3K14, MAP3K7, MAPK14, MAPKAPK2, MAPT,
MC4R, MED15, MICA, MMP20, MRPL36, MS4A1, MTHFD1, MTHFR,
MTR, MTRR, MYD88, NAT1, NAT2, NAV2, NEBL, NEDD4L, NFIB,
NFKBIA, NFKBIB, NFKBIE, NLRP3, NQO1, NR1I2, NR2F2, NR3C1, NT5C2,
NTRK2, NUBPL, NUDT15, OPRD1, OPRM1, OR2B11, OSR1, P2RY1,
P2RY12, PDZD2, PLA2G4A, PNPLA3, PRELID3B, PRKCA, PRSS53, PTGFR,
PTGIS, PTGS1, PTGS2, PTPRC, PTPRM, QKI, RAD51B, RHOBTB1,
RPS6KA5, RYR1, SCN1A, SCN5A, SCNN1A, SEMA3C, SHMT1, SLC15A1,
SLC15A2, SLC16A7, SLC19A1, SLC22A1, SLC22A11, SLC22A2, SLC22A6,
SLC28A3, SLC46A1, SLC6A4, SLC9A7, SLCO1A2, SLCO1B1, SLCO1B3,
SLCO1C1, SLCO2B1, SOD2, SP3, SRY, STAT4, STRBP, SULT1A1, SULT1A2,
SYNM, TANC1, TBXAS1, TCF7L2, TEC, TGFB1, TGFBR2, TLR1, TLR10,
TLR2, TLR4, TLR5, TNF, TNFAIP3, TNFRSF1A, TNFRSF1B, TNFSF13B,
TP53, TPMT, TRAF1, TUBB2A, TYMS, UGT1A1, UGT1A10, UGT1A3,
UGT1A4, UGT1A5, UGT1A6, UGT1A7, UGT1A8, UGT1A9, UGT2B10,
UGT2B15, UGT2B17, UGT2B7, UMPS, VDR, VKORC1, WDR27, XPC,
XRCC1, YEATS4, ZNF595.
Appendix A.2. Pharmacogenetic Alleles Included in the Panel
The Action PharmaKitDx platform incorporates a curated set of pharmacogenetically relevant alleles and haplotypes that are automatically inferred by a dedicated bioinformatic algorithm. Variant interpretation relies on a periodically updated allele database maintained by the clinical team at Health in Code, integrating information from international pharmacogenetic consortia, peer-reviewed literature, and population databases.
For each sample, the algorithm evaluates the detected SNVs, indels, and—in selected loci—structural or copy-number changes, assigning haplotypes according to established star allele nomenclatures. The system provides automated diplotype calls for a broad range of clinically relevant pharmacogenes, including but not limited to genes involved in drug metabolism (e.g., CYP family), drug transport (e.g., ABC transporters, SLCO1B1), immune-mediated toxicity (e.g., HLA alleles), and pharmacodynamic mechanisms (e.g., RYR1).
A list of alleles that can be automatically inferred by the algorithm is provided in list A2:
ABCC3 [rs1051640]
ABCG2 [rs2231142]
CACNA1S [c.1589G>A/p.Arg530His, c.1598G>A/p.Arg533His]
CALU [c.606+133A>G (rs339097)]
COMT [c.615+310C>T (rs4646316)]
CYP1A2 [*1A, *1C, *1D, *1F, *1K, *1L, *2, *3, *4, *5, *6, *7, *8, *11, *15, *16]
CYP2B6 [*2, *3, *4, *5, *6, *7, *8, *9, *11, *12, *13, *14, *15, *16, *18, *19, *20,
*21, *22, *26, *27, *28]
CYP2C18 [rs12777823]
CYP2C19 [*2A, *2B, *3, *4, *5, *6, *7, *8, *9, *10, *12, *13, *14, *15, *17]
CYP2C9 [*2, *3, *4, *5, *6, *9, *10, *11, *12, *13, *15, *16, *25]
CYP2D6 [*2, *3, *4, *5, *6, *7, *8, *9, *10A, *11, *12, *14A, *14B, *15, *17, *18,
*19, *20, *21A, *29, *38, *40, *41, *42, *44, *56A, *56B, *64, x2, xN, hyb]
CYP3A4 [*1B, *2, *3, *4, *5, *6, *7, *8, *10, *11, *12, *13, *14, *15A, *15B, *16,
*17, *18, *19, *20, *22]
CYP3A5 [*1A, *2, *3B, *3C, *3D, *3F, *3G, *3K, *3L, *4, *5, *6, *7, *8, *9]
CYP4F2 [*1, *2, *3]
DPYD [c.1024G>A (rs183385770), c.1057C>T (rs143154602), c.1129-5923C>G,
c.1236G>A (HapB3), c.1156G>T (*12), c.1314T>G (rs186169810),
c.1484A>G (rs111858276), c.1679T>G (*13), c.1774C>T (rs59086055),
c.1775G>A (rs138616379), c.1777G>A (rs145773863), c.1898delC (*3),
c.1905+1G>A (*2A), c.2021G>A (rs137999090), c.2279C>T (rs112766203),
c.2639G>T (rs55674432), c.2656C>T (rs147545709), c.2846A>T (rs67376798),
c.2872A>G (rs141044036), c.2933A>G (rs72547601), c.295_298delTCAT (*7),
c.2983G>T (*10), c.557A>G (rs115232898), c.601A>C (rs72549308),
c.61C>T (rs72549310), c.632A>G (rs72549307), c.703C>T (*8),
c.868A>G (rs146356975)]
F5 [Factor V Leiden]
G6PD [202G>A_376A>G_1264C>G, A, A- 202A_376G, Aachen, Abeno,
Acrokorinthos, Alhambra, Amazonia, Amiens, Amsterdam, Anadia, Ananindeua,
Andalus, Arakawa, Asahi, Asahikawa, Aures, Aveiro, B (wildtype),
Bajo Maumere, Bangkok, Bangkok Noi, Bao Loc, Bari, Belem, Beverly Hills,
Genova, Iwate, Niigata, Yamaguchi, Brighton, Buenos Aires, Cairo,
Calvo Mackenna, Campinas, Canton, Taiwan-Hakka, Gifu-like, Agrigento-like,
Cassano, Chatham, Chikugo, Chinese-1, Chinese-5, Cincinnati, Cleveland Corum,
Clinic, Coimbra Shunde, Cosenza, Costanzo, Covao do Lobo, Crispim, Dagua,
Durham, Farroupilha, Figuera da Foz, Flores, Fukaya, Fushan,
G6PD A- 680T_376G, G6PD A- 968C_376G, G6PDNice, Gaohe, Georgia, Gidra,
Gond, Guadalajara, Guangzhou, Haikou, Hammersmith, Harilaou, Harima,
Hartford, Hechi, Hermoupolis, Honiara, Ierapetra, Ilesha, Insuli, Iowa,
Walter Reed, Springfield, Iwatsuki, Japan, Shinagawa, Kaiping, Anant, Dhon,
Sapporo-like, Wosera, Kalyan-Kerala, Jamnaga, Rohini, Kambos, Kamiube,
Keelung, Kamogawa, Kawasaki, Kozukata, Krakow, La Jolla, Lages, Lagosanto,
Laibin, Lille, Liuzhou, Loma Linda, Ludhiana, Lynwood, Madrid, Mahidol,
Malaga, Manhattan, Mediterranean Haplotype, Mediterranean, Dallas, Panama‚
Sassari, Cagliari, Birmingham, Metaponto, Mexico City, Miaoli, Minnesota,
Marion, Gastonia, LeJeune, Mira d’Aire, Mizushima, Montalbano, Montpellier,
Mt Sinai, Munich, Murcia Oristano, Musashino, Namouru, Nankang, Nanning,
Naone, Nara, Nashville, Anaheim, Portici, Neapolis, Nilgiri, No name,
North Dallas, Olomouc, Omiya, Orissa, Osaka, Palestrina, Papua, Partenope,
Pawnee, Pedoplis-Ckaro, Piotrkow, Plymouth, Praha, Puerto Limon, Quing Yan,
Radlowo, Rehevot, Rignano, Riley, Riverside, Roubaix, S. Antioco,
Salerno Pyrgos, Santa Maria, Santiago, Santiago de Cuba, Morioka, Sao Borja,
Seattle, Lodi, Modena, Ferrara II, Athens-like, Seoul, Serres, Shenzen, Shinshu,
Sibari, Sierra Leone, Sinnai, Songklanagarind, Split, Stonybrook, Sugao, Sumare,
Sunderland, Surabaya, Suwalki, Swansea, Taipei‚ Chinese-3, Telti/Kobe,
Tenri, Tokyo, Fukushima, Toledo, Tomah, Tondela, Torun, Tsukui, Ube Konan,
Union, Maewo, Chinese-2, Kalo, Urayasu, Utrecht, Valladolid, Vancouver,
Vanua Lava, Viangchan, Jammu, Villeurbanne, Volendam, Wayne, West Virginia,
Wexham, Wisconsin, Yunan]
GGCX [c.2084+45G>C (rs11676382))]
HLA-A [c.*66A>T (rs1061235-T) (*31:01)]
HLA-B [base de datos IMGT/HLA v 3.12 compuesta 2932 alelos]
IFNL4 [c.151-152G>A (rs12979860)]
NAT1 [*4, *5, *11, *11C, *14, *15, *17, *19A, *19B, *22, *23, *27, *30]
NAT2 [*4, *5A, *5E, *6A, *6J, *7A, *7D, *10, *12D, *14A, *14D, *14F, *17, *18, *19]
NUDT15 [*2, *3, *4, *5, *6, *7, *8, *9, *10, *11, *12, *13, *14, *15, *16, *17, *18, *19]
RYR1 [p.Ala2350Thr, p.Ala2428Thr, p.Arg163Cys, p.Arg163Leu, p.Arg2163Cys,
p.Arg2163His, p.Arg2336His, p.Arg2355Trp, p.Arg2435His, p.Arg2452Trp,
p.Arg2454Cys, p.Arg2454His, p.Arg2458Cys, p.Arg2458Leu, p.Arg2508Cys,
p.Arg2508Gly, p.Arg2508His, p.Arg328Trp, p.Arg401Gly, p.Arg44Cys,
p.Arg4861His, p.Arg530His, p.Arg533His, p.Arg533Ser, p.Arg552Trp,
p.Arg614Cys, p.Arg614Leu, p.Glu2348del, p.Glu3104Lys, p.Gly2375Ala,
p.Gly2434Arg, p.Gly248Arg, p.Gly341Arg, p.Gly3990Val, p.His4833Tyr,
p.Ile403Met, p.Ile4898Thr, p.Leu4838Val, p.Thr2206Arg, p.Thr2206Met,
p.Thr4826Ile, p.Tyr4796Cys, p.Tyr522Ser, p.Val2168Met, p.Val4849Ile]
SLC28A3 [c.1381C>T, (rs7853758)]
SLCO1B1 [*1B, *2, *3, *4, *5, *6, *7, *8, *9, *11, *13, *14, *15, *16, *17, *18, *21, *31]
TPMT [*1, *2, *3A, *3B, *3C, *3D, *4, *8, *24]
UGT1A1 [*1, *27, *28, *36, *37, *6, *60, *93]
UGT1A6 [*1, *2, *3A, *4A, *4b, *5]
VKORC1 [c.-1639G>A (rs9923231)].
ABCG2 [rs2231142]
CACNA1S [c.1589G>A/p.Arg530His, c.1598G>A/p.Arg533His]
CALU [c.606+133A>G (rs339097)]
COMT [c.615+310C>T (rs4646316)]
CYP1A2 [*1A, *1C, *1D, *1F, *1K, *1L, *2, *3, *4, *5, *6, *7, *8, *11, *15, *16]
CYP2B6 [*2, *3, *4, *5, *6, *7, *8, *9, *11, *12, *13, *14, *15, *16, *18, *19, *20,
*21, *22, *26, *27, *28]
CYP2C18 [rs12777823]
CYP2C19 [*2A, *2B, *3, *4, *5, *6, *7, *8, *9, *10, *12, *13, *14, *15, *17]
CYP2C9 [*2, *3, *4, *5, *6, *9, *10, *11, *12, *13, *15, *16, *25]
CYP2D6 [*2, *3, *4, *5, *6, *7, *8, *9, *10A, *11, *12, *14A, *14B, *15, *17, *18,
*19, *20, *21A, *29, *38, *40, *41, *42, *44, *56A, *56B, *64, x2, xN, hyb]
CYP3A4 [*1B, *2, *3, *4, *5, *6, *7, *8, *10, *11, *12, *13, *14, *15A, *15B, *16,
*17, *18, *19, *20, *22]
CYP3A5 [*1A, *2, *3B, *3C, *3D, *3F, *3G, *3K, *3L, *4, *5, *6, *7, *8, *9]
CYP4F2 [*1, *2, *3]
DPYD [c.1024G>A (rs183385770), c.1057C>T (rs143154602), c.1129-5923C>G,
c.1236G>A (HapB3), c.1156G>T (*12), c.1314T>G (rs186169810),
c.1484A>G (rs111858276), c.1679T>G (*13), c.1774C>T (rs59086055),
c.1775G>A (rs138616379), c.1777G>A (rs145773863), c.1898delC (*3),
c.1905+1G>A (*2A), c.2021G>A (rs137999090), c.2279C>T (rs112766203),
c.2639G>T (rs55674432), c.2656C>T (rs147545709), c.2846A>T (rs67376798),
c.2872A>G (rs141044036), c.2933A>G (rs72547601), c.295_298delTCAT (*7),
c.2983G>T (*10), c.557A>G (rs115232898), c.601A>C (rs72549308),
c.61C>T (rs72549310), c.632A>G (rs72549307), c.703C>T (*8),
c.868A>G (rs146356975)]
F5 [Factor V Leiden]
G6PD [202G>A_376A>G_1264C>G, A, A- 202A_376G, Aachen, Abeno,
Acrokorinthos, Alhambra, Amazonia, Amiens, Amsterdam, Anadia, Ananindeua,
Andalus, Arakawa, Asahi, Asahikawa, Aures, Aveiro, B (wildtype),
Bajo Maumere, Bangkok, Bangkok Noi, Bao Loc, Bari, Belem, Beverly Hills,
Genova, Iwate, Niigata, Yamaguchi, Brighton, Buenos Aires, Cairo,
Calvo Mackenna, Campinas, Canton, Taiwan-Hakka, Gifu-like, Agrigento-like,
Cassano, Chatham, Chikugo, Chinese-1, Chinese-5, Cincinnati, Cleveland Corum,
Clinic, Coimbra Shunde, Cosenza, Costanzo, Covao do Lobo, Crispim, Dagua,
Durham, Farroupilha, Figuera da Foz, Flores, Fukaya, Fushan,
G6PD A- 680T_376G, G6PD A- 968C_376G, G6PDNice, Gaohe, Georgia, Gidra,
Gond, Guadalajara, Guangzhou, Haikou, Hammersmith, Harilaou, Harima,
Hartford, Hechi, Hermoupolis, Honiara, Ierapetra, Ilesha, Insuli, Iowa,
Walter Reed, Springfield, Iwatsuki, Japan, Shinagawa, Kaiping, Anant, Dhon,
Sapporo-like, Wosera, Kalyan-Kerala, Jamnaga, Rohini, Kambos, Kamiube,
Keelung, Kamogawa, Kawasaki, Kozukata, Krakow, La Jolla, Lages, Lagosanto,
Laibin, Lille, Liuzhou, Loma Linda, Ludhiana, Lynwood, Madrid, Mahidol,
Malaga, Manhattan, Mediterranean Haplotype, Mediterranean, Dallas, Panama‚
Sassari, Cagliari, Birmingham, Metaponto, Mexico City, Miaoli, Minnesota,
Marion, Gastonia, LeJeune, Mira d’Aire, Mizushima, Montalbano, Montpellier,
Mt Sinai, Munich, Murcia Oristano, Musashino, Namouru, Nankang, Nanning,
Naone, Nara, Nashville, Anaheim, Portici, Neapolis, Nilgiri, No name,
North Dallas, Olomouc, Omiya, Orissa, Osaka, Palestrina, Papua, Partenope,
Pawnee, Pedoplis-Ckaro, Piotrkow, Plymouth, Praha, Puerto Limon, Quing Yan,
Radlowo, Rehevot, Rignano, Riley, Riverside, Roubaix, S. Antioco,
Salerno Pyrgos, Santa Maria, Santiago, Santiago de Cuba, Morioka, Sao Borja,
Seattle, Lodi, Modena, Ferrara II, Athens-like, Seoul, Serres, Shenzen, Shinshu,
Sibari, Sierra Leone, Sinnai, Songklanagarind, Split, Stonybrook, Sugao, Sumare,
Sunderland, Surabaya, Suwalki, Swansea, Taipei‚ Chinese-3, Telti/Kobe,
Tenri, Tokyo, Fukushima, Toledo, Tomah, Tondela, Torun, Tsukui, Ube Konan,
Union, Maewo, Chinese-2, Kalo, Urayasu, Utrecht, Valladolid, Vancouver,
Vanua Lava, Viangchan, Jammu, Villeurbanne, Volendam, Wayne, West Virginia,
Wexham, Wisconsin, Yunan]
GGCX [c.2084+45G>C (rs11676382))]
HLA-A [c.*66A>T (rs1061235-T) (*31:01)]
HLA-B [base de datos IMGT/HLA v 3.12 compuesta 2932 alelos]
IFNL4 [c.151-152G>A (rs12979860)]
NAT1 [*4, *5, *11, *11C, *14, *15, *17, *19A, *19B, *22, *23, *27, *30]
NAT2 [*4, *5A, *5E, *6A, *6J, *7A, *7D, *10, *12D, *14A, *14D, *14F, *17, *18, *19]
NUDT15 [*2, *3, *4, *5, *6, *7, *8, *9, *10, *11, *12, *13, *14, *15, *16, *17, *18, *19]
RYR1 [p.Ala2350Thr, p.Ala2428Thr, p.Arg163Cys, p.Arg163Leu, p.Arg2163Cys,
p.Arg2163His, p.Arg2336His, p.Arg2355Trp, p.Arg2435His, p.Arg2452Trp,
p.Arg2454Cys, p.Arg2454His, p.Arg2458Cys, p.Arg2458Leu, p.Arg2508Cys,
p.Arg2508Gly, p.Arg2508His, p.Arg328Trp, p.Arg401Gly, p.Arg44Cys,
p.Arg4861His, p.Arg530His, p.Arg533His, p.Arg533Ser, p.Arg552Trp,
p.Arg614Cys, p.Arg614Leu, p.Glu2348del, p.Glu3104Lys, p.Gly2375Ala,
p.Gly2434Arg, p.Gly248Arg, p.Gly341Arg, p.Gly3990Val, p.His4833Tyr,
p.Ile403Met, p.Ile4898Thr, p.Leu4838Val, p.Thr2206Arg, p.Thr2206Met,
p.Thr4826Ile, p.Tyr4796Cys, p.Tyr522Ser, p.Val2168Met, p.Val4849Ile]
SLC28A3 [c.1381C>T, (rs7853758)]
SLCO1B1 [*1B, *2, *3, *4, *5, *6, *7, *8, *9, *11, *13, *14, *15, *16, *17, *18, *21, *31]
TPMT [*1, *2, *3A, *3B, *3C, *3D, *4, *8, *24]
UGT1A1 [*1, *27, *28, *36, *37, *6, *60, *93]
UGT1A6 [*1, *2, *3A, *4A, *4b, *5]
VKORC1 [c.-1639G>A (rs9923231)].
Appendix A.3. Analytical Performance Metrics
The analytical performance of the Action PharmaKitDx panel was evaluated using standard metrics for genotyping assays. Below are the definitions and formulas applied:
Analytical accuracy: proportion of correctly identified genotypes compared to reference materials.
Analytical sensitivity (positive percent agreement, PPA): proportion of true positive variants correctly detected.
Analytical specificity (negative percent agreement, NPA): proportion of true negative positions correctly identified.
Precision (positive predictive value, PPV): proportion of variant calls that are true positives.
Repeatability, reproducibility and robustness: consistency of results within the same sequencing run (repeatability), across different sequencing runs (reproducibility), and across different sequencing instruments.
Appendix A.4. Rare Variant Filtering and Prioritization Workflow
A multi-step filtering pipeline was applied to the full set of annotated variants to identify high-confidence rare variants of potential clinical relevance. The workflow integrated quality metrics, population allele frequencies, genomic context, in silico predictions, and ClinVar classifications. All filtering steps were implemented programmatically to ensure reproducibility.
Appendix A.4.1. Quality-Based Filtering
Variants were first required to meet minimal sequencing quality standards:
- Depth of coverage ≥ 30
- Base quality ≥ 100
-
Allele fraction thresholds adapted to zygosity:
- a.
- Heterozygous variants ≥ 0.25
- b.
- Homozygous variants ≥ 0.80
- c.
- Variants with undefined zygosity were conservatively required to meet ≥ 0.25
Variants failing any of these conditions were excluded from downstream evaluation.
Appendix A.4.2. Population Frequency Filtering
To retain only rare or ultra-rare alleles, population allele frequencies were examined across the following databases:
- gnomAD
- ExAC
- 1000 Genomes
- 5000 Exomes
- dbSNP frequency annotations
Variants were retained only when all available population frequency values were <1%, or when no population frequency data were available (classified as ultra-rare).
Appendix A.4.3. Functional Annotation Filtering
Variants were then evaluated for their genomic context and potential functional impact. Variants were kept if they fulfilled at least one of the following criteria:
- Located in coding regions or exons
- Caused a non-synonymous amino acid change, including missense, nonsense, frameshift, indels, or disruptions affecting the reading frame
-
Annotated as splicing-relevant, either through:
- d.
- Explicit splicing flags in the annotation, or
- e.
- NNSPLICE predictions indicating ≥10% reduction in splice-site strength
Synonymous variants were excluded unless supported by splicing predictions.
Appendix A.4.4. Pathogenicity Predictor Filtering
To prioritize variants with in silico evidence of deleteriousness, at least one of the following had to apply:
- DANN score ≥ 0.9
- FATHMM coding-group classification containing “damaging” or “deleterious”
- MutationTaster prediction = “D” (disease causing)
Variants lacking predictor data were not excluded unless previously removed in an earlier step.
Appendix A.4.5. ClinVar-Based Filtering
ClinVar annotations were used to integrate clinical evidence:
- Variants classified as pathogenic, likely pathogenic, conflicting, or VUS were retained.
- Variants labelled benign or likely benign were excluded unless at least one in silico predictor suggested deleteriousness (as defined above).
- Variants with no ClinVar annotation passed this step by default.
Appendix A.4.6. Final Variant Set
Only variants passing all filtering stages were included in the final prioritized list.
Across the full dataset, this workflow identified 36 rare variants with potential functional and clinical relevance.
References
- Kabbani, D.; Akika, R.; Wahid, A.; Daly, A.K.; Cascorbi, I.; Zgheib, N.K. Pharmacogenomics in Practice: A Review and Implementation Guide. Front. Pharmacol. 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Russell, L.; Zhou, Y.; Almousa, A.A.; Sodhi, J.K.; Nwabufo, C.K.; Lauschke, V.M. Pharmacogenomics in the Era of next Generation Sequencing – from Byte to Bedside. Drug Metab. Rev. 2021, 53, 253–278. [Google Scholar] [CrossRef]
- Schwarz, U.I.; Gulilat, M.; Kim, R.B. The Role of Next-Generation Sequencing in Pharmacogenetics and Pharmacogenomics. Cold Spring Harb. Perspect. Med. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Klein, K.; Tremmel, R.; Winter, S.; Fehr, S.; Battke, F.; Scheurenbrand, T.; Schaeffeler, E.; Biskup, S.; Schwab, M.; Zanger, U.M. A New Panel-Based Next-Generation Sequencing Method for ADME Genes Reveals Novel Associations of Common and Rare Variants With Expression in a Human Liver Cohort. Front. Genet. 2019, 10. [Google Scholar] [CrossRef]
- McInnes, G.; Lavertu, A.; Sangkuhl, K.; Klein, T.E.; Whirl-Carrillo, M.; Altman, R.B. Pharmacogenetics at Scale: An Analysis of the UK Biobank. Clin. Pharmacol. Ther. 2020, 109, 1528–1537. [Google Scholar] [CrossRef]
- Chen, X.; Shen, F.; Gonzaludo, N.; Malhotra, A.; Rogert, C.; Taft, R.J.; Bentley, D.; Eberle, M.A. Cyrius: Accurate CYP2D6 Genotyping Using Whole-Genome Sequencing Data. Pharmacogenomics J. 2021, 21, 251–261. [Google Scholar] [CrossRef]
- Luo, S.; Jiang, R.; Grzymski, J.J.; Lee, W.; Lu, J.T.; Washington, N.L. Comprehensive Allele Genotyping in Critical Pharmacogenes Reduces Residual Clinical Risk in Diverse Populations. Clin. Pharmacol. Ther. 2021, 110, 759–767. [Google Scholar] [CrossRef]
- Turner, A.; Derezinski, A.D.; Gaedigk, A.; Berres, M.E.; Gregornik, D.; Brown, K.; Broeckel, U.; Scharer, G. Characterization of Complex Structural Variation in the CYP2D6-CYP2D7-CYP2D8 Gene Loci Using Single-Molecule Long-Read Sequencing. Front. Pharmacol. 2023, 14. [Google Scholar] [CrossRef]
- Caspar, S.M.; Schneider, T.; Meienberg, J.; Matyas, G. Added Value of Clinical Sequencing: WGS-Based Profiling of Pharmacogenes. Int. J. Mol. Sci. 2020, 21. [Google Scholar] [CrossRef]
- Caspar, S.M.; Schneider, T.; Stoll, P.; Meienberg, J.; Mátyás, G. Potential of Whole-Genome Sequencing-Based Pharmacogenetic Profiling. Pharmacogenomics 2021, 22, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Gulilat, M.; Lamb, T.; Teft, W.A.; Wang, J.; Dron, J.S.; Robinson, J.F.; Tirona, R.G.; Hegele, R.A.; Kim, R.B.; Schwarz, U.I. Targeted next Generation Sequencing as a Tool for Precision Medicine. BMC Med. Genomics 2019, 12, 81. [Google Scholar] [CrossRef]
- Lee, S.B.; Shin, J.Y.; Kwon, N.J.; Kim, C.; Seo, J.S. ClinPharmSeq: A Targeted Sequencing Panel for Clinical Pharmacogenetics Implementation. PLoS ONE 2022, 17. [Google Scholar] [CrossRef]
- van der Lee, M.; Kriek, M.; Guchelaar, H.-J.; Swen, J.J. Technologies for Pharmacogenomics: A Review. Genes 2020, 11, 1456. [Google Scholar] [CrossRef]
- David, V.; Fylan, B.; Bryant, E.; Smith, H.; Sagoo, G.S.; Rattray, M. An Analysis of Pharmacogenomic-Guided Pathways and Their Effect on Medication Changes and Hospital Admissions: A Systematic Review and Meta-Analysis. Front. Genet. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.A.; Alsaidi, A.T.; Verbyla, A.; Cruz, A.; Macfarlane, C.; Bauer, J.; Patel, J.N. Cost Effectiveness of Pharmacogenetic Testing for Drugs with Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines: A Systematic Review. Clin. Pharmacol. Ther. 2022, 112, 1318–1328. [Google Scholar] [CrossRef]
- Abdullah-Koolmees, H.; van Keulen, A.M.; Nijenhuis, M.; Deneer, V.H.M. Pharmacogenetics Guidelines: Overview and Comparison of the DPWG, CPIC, CPNDS, and RNPGx Guidelines. Front. Pharmacol. 2020, 11, 595219. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, D.; Patel, J.N.; Stephens, L.E.; McLeod, H.L. Comparison of FDA Table of Pharmacogenetic Associations and Clinical Pharmacogenetics Implementation Consortium Guidelines. Am. J. Health-Syst. Pharm. AJHP Off. J. Am. Soc. Health-Syst. Pharm. 2022, 79, 993–1005. [Google Scholar] [CrossRef]
- Action PharmaKit Manual-RUO. Health Code.
- Ramudo-Cela, L.; López-Martí, J.M.; Colmeiro-Echeberría, D.; De-Uña-Iglesias, D.; Santomé-Collazo, J.L.; Monserrat-Iglesias, L. Development and Validation of a Next-Generation Sequencing Panel for Clinical Pharmacogenetics. Farm. Hosp. Organo Of. Expresion Cient. Soc. Espanola Farm. Hosp. 2020, 44, 243–253. [Google Scholar] [CrossRef]
- Gaedigk, A.; Sangkuhl, K.; Whirl-Carrillo, M.; Twist, G.P.; Klein, T.E.; Miller, N.A. The Evolution of PharmVar. Clin. Pharmacol. Ther. 2019, 105, 29–32. [Google Scholar] [CrossRef]
- Whirl-Carrillo, M.; Huddart, R.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Whaley, R.; Klein, T.E. An Evidence-Based Framework for Evaluating Pharmacogenomics Knowledge for Personalized Medicine. Clin. Pharmacol. Ther. 2021, 110, 563–572. [Google Scholar] [CrossRef] [PubMed]
- De-Uña, D. System and Method to Detect Structural Genetic Variants 2019.
- Ramudo-Cela, L.; López-Martí, J.M.; Colmeiro-Echeberría, D.; De-Uña-Iglesias, D.; Santomé-Collazo, J.L.; Monserrat-Iglesias, L. Development and Validation of a Next-Generation Sequencing Panel for Clinical Pharmacogenetics. Farm. Hosp. Organo Of. Expresion Cient. Soc. Espanola Farm. Hosp. 2020, 44, 243–253. [Google Scholar] [CrossRef]
- Wittig, M.; Anmarkrud, J.A.; Kassens, J.C.; Koch, S.; Forster, M.; Ellinghaus, E.; Hov, J.R.; Sauer, S.; Schimmler, M.; Ziemann, M.; et al. Development of a High-Resolution NGS-Based HLA-Typing and Analysis Pipeline. Nucleic Acids Res. 2015, 43, e70. [Google Scholar] [CrossRef]
Figure 1.
Strand-aware coverage analysis of the CYP2D6 locus and homologous regions in five GeT-RM reference samples. Orientation and conventions: The x-axis shows genomic coordinates that increase 5′→3′ along the reference plus (forward) strand. CYP2D6 is encoded on the reverse (minus) strand, so its transcription proceeds right-to-left in the plot. Blue boxes depict the CYP2D6 gene structure (thick = exons, thin = introns); arrowheads indicate the gene’s transcriptional direction. Panels and lines. For each sample—NA12892 (a), NA12878 (b), HG00276 (c), HG01190 (d), HG00436 (e)—the top panel shows absolute read depth (coverage), and the bottom panel shows normalized coverage (adjusted for probe hybridization efficiency). Red lines correspond to the sample under analysis; grey lines are other samples in the sequencing pool; the blue line in the top panel is the internal control (NA17254). Genomic context. Adjacent high-homology blocks (e.g., CYP2D7-derived segments) are included on the x-axis to resolve hybrid and tandem configurations. Sample interpretations (copy-number logic: ~50% decrease = heterozygous loss; ~50% increase = single extra copy): (a) NA12892: No deviations in coverage; consistent with diploid CYP2D6 (two copies; no CNVs). (b) NA12878: A focal ~50% coverage gain at the CYP2D6 5′ end (exon 1) and the adjacent high-homology region supports a CYP2D6–CYP2D7 hybrid tandem involving exon 1, consistent with CYP2D6*68, with two CYP2D6 copies plus the hybrid segment. (c) HG00276: A ~50% coverage reduction across the entire CYP2D6 gene indicates a heterozygous deletion (CYP2D6*5), yielding one functional copy. (d) HG01190: A ~50% reduction across most of CYP2D6, combined with increased coverage in the upstream homologous block, indicates co-occurrence of a *heterozygous deletion (5) and a *tandem 68 hybrid. (e) HG00436: A uniform ~50% coverage gain across the whole CYP2D6 region is consistent with a gene duplication (CYP2D6×2), totaling three gene copies. These plots are generated by the automated CYP2D6 module integrated in the Action PharmaKitDx platform, which performs structural variant calling from comparative read-depth profiles and facilitates visual inspection against a co-analyzed internal control.
Figure 1.
Strand-aware coverage analysis of the CYP2D6 locus and homologous regions in five GeT-RM reference samples. Orientation and conventions: The x-axis shows genomic coordinates that increase 5′→3′ along the reference plus (forward) strand. CYP2D6 is encoded on the reverse (minus) strand, so its transcription proceeds right-to-left in the plot. Blue boxes depict the CYP2D6 gene structure (thick = exons, thin = introns); arrowheads indicate the gene’s transcriptional direction. Panels and lines. For each sample—NA12892 (a), NA12878 (b), HG00276 (c), HG01190 (d), HG00436 (e)—the top panel shows absolute read depth (coverage), and the bottom panel shows normalized coverage (adjusted for probe hybridization efficiency). Red lines correspond to the sample under analysis; grey lines are other samples in the sequencing pool; the blue line in the top panel is the internal control (NA17254). Genomic context. Adjacent high-homology blocks (e.g., CYP2D7-derived segments) are included on the x-axis to resolve hybrid and tandem configurations. Sample interpretations (copy-number logic: ~50% decrease = heterozygous loss; ~50% increase = single extra copy): (a) NA12892: No deviations in coverage; consistent with diploid CYP2D6 (two copies; no CNVs). (b) NA12878: A focal ~50% coverage gain at the CYP2D6 5′ end (exon 1) and the adjacent high-homology region supports a CYP2D6–CYP2D7 hybrid tandem involving exon 1, consistent with CYP2D6*68, with two CYP2D6 copies plus the hybrid segment. (c) HG00276: A ~50% coverage reduction across the entire CYP2D6 gene indicates a heterozygous deletion (CYP2D6*5), yielding one functional copy. (d) HG01190: A ~50% reduction across most of CYP2D6, combined with increased coverage in the upstream homologous block, indicates co-occurrence of a *heterozygous deletion (5) and a *tandem 68 hybrid. (e) HG00436: A uniform ~50% coverage gain across the whole CYP2D6 region is consistent with a gene duplication (CYP2D6×2), totaling three gene copies. These plots are generated by the automated CYP2D6 module integrated in the Action PharmaKitDx platform, which performs structural variant calling from comparative read-depth profiles and facilitates visual inspection against a co-analyzed internal control.
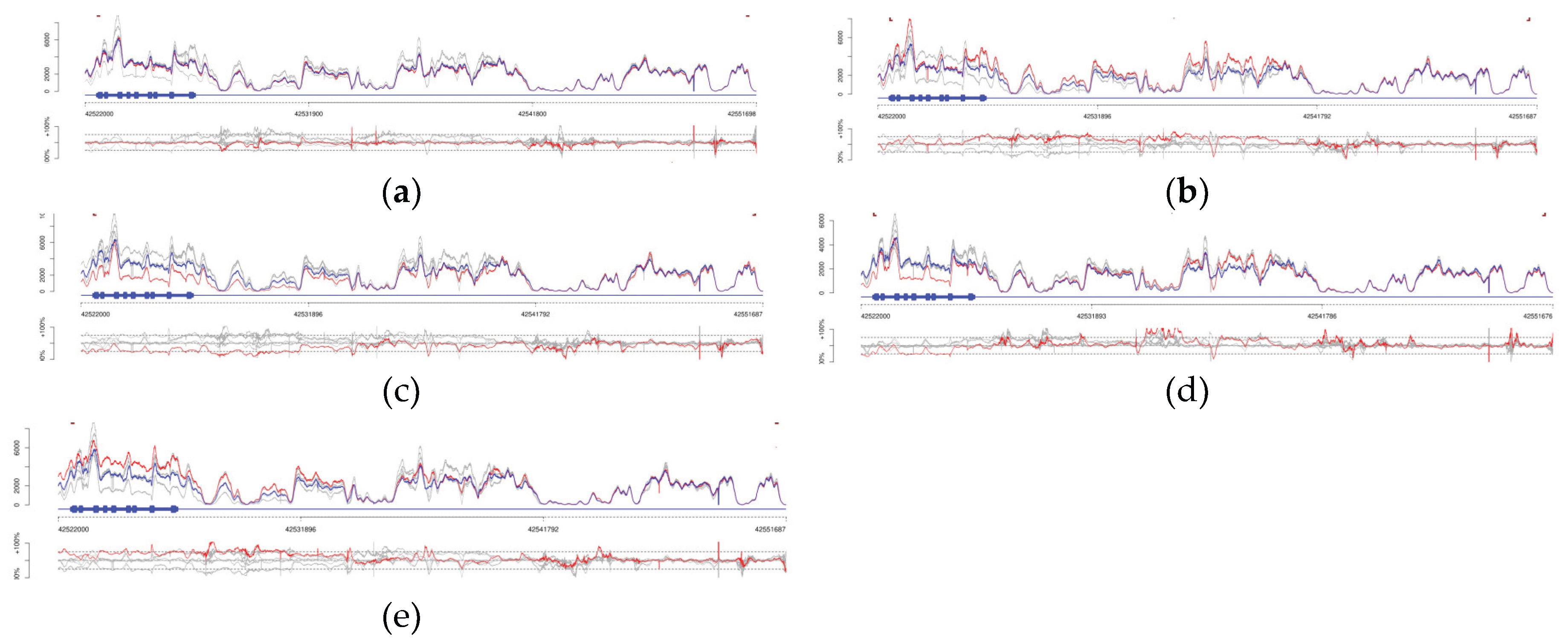

Table 1.
Sequencing quality metrics and analytical performance of the Action PharmaKitDx panel across workflows.
Table 1.
Sequencing quality metrics and analytical performance of the Action PharmaKitDx panel across workflows.
| Parameters | MiSeq (Manual workflow) |
MiSeq (Automated workflow) |
NextSeq 500/550 (Automated workflow) |
NextSeq 1000/2000 (Automated workflow) | |
|---|---|---|---|---|---|
| Sequencing quality metrics | Q30 (%) | 82.2 | 93.4 | 84.3 | 90.9 |
| Clusters passing filter (%) | 82.2 | 89.1 | 89.4 | NA | |
| Mean coverage (×) | 582 | 926 | 1,88 | 1,4 | |
| Bases >30× (%) | 99.3 | 99.4 | >99.5 | >99.5 | |
| Analytical performance metrics | Analytical accuracy (%) | 99.9 | >99.9 | 99.9 | 99.9 |
|
Analytical sensitivity (PPA%) |
99.4 | >99.9 | 99.8 | 99.9 | |
|
Analytical specificity (NPA%) |
>99.9 | >99.9 | >99.9 | >99.9 | |
|
Positive predictive value (PPV %) |
>99.9 | >99.9 | >99.9 | >99.9 | |
| Repeatability (%) | 99.1 | >99.9 | 99.8 | 99.9 | |
| Reproducibility (%) | 99.1 | >99.9 | 99.8 | 99.9 | |
* Analytical performance values represent mean results per workflow. NA, not applicable.
Table 2.
Pharmacogenetic alleles validated in the clinical cohort.
| Gene | Detected Allele(s) | Sample ID(s) | Reference method(s) |
| CYP2D6 | *3, *4, *5, *6, *9, *10, *17, *41, xN | 23V15551, 23T15552, 23Y15555, 23Q15562, 23Z15563, 23P15568, 23R15570, 23V11743 | Allelic discrimination PCR; fluorescent PCR for copy number determination; Sanger sequencing |
| CYP2C19 | *2, *17 | 23R15553, 23Y15555, 23X15564, 23P15568, 23R15570, 23Y11750 | Allelic discrimination PCR |
| CYP2C9 | *2, *3 | 23P15554, 23Y15555, 23R15570, 23R11745, 23Z11738, 23Q11740, 23W11751, 23Q11754, 24U11012, 24S11013, 24X11016 | Sanger sequencing (rs1799853, rs1057910); allelic discrimination PCR |
| CYP1A2 | *1C, *1F | 23Q15562, 23X15564, 23P15568, 23R15570 | Allelic discrimination PCR |
| CYP3A4 | *22 | 23R15570 | Sanger sequencing |
| CYP3A5 | *3, *7 | 23Q15559, 23V15565 | Allelic discrimination PCR |
| DPYD | rs3918290 (*2A), rs75017182+ rs56038477 (HapB3), rs67376798 (D949V), rs55886062 (*13) | 23U15557, 23S15558, 23U15560, 23U11752, 23P11746, 23W11748, 24R11022, 24P11023, 24W11025 | Sanger sequencing; allelic discrimination PCR |
| UGT1A1 | *28, *37, c.1220_1221insG | 23U15557, 23S15558, 23T11744, 23U11749, 23U15560, 23U11752, 24V11017, 24T11018, 24R11019, 24V11020 | STR analysis of (TA)n promoter repeat; Sanger sequencing; whole-exome sequencing |
| TPMT | *2, *3A, *3B, *3C | 23T15566, 23R15567, 23Y15569 | Allelic discrimination PCR |
| NUDT15 | *3 | 23R15567, 23Y15569 | Allelic discrimination PCR |
| RYR1 | c.7858C>T (p.Gln2620*) | 24S11027 | Whole-exome sequencing |
Table 3.
Clinical categories, genes tested, and concordance results in the validation cohort.
| Clinical Category | N (%) | Genes tested | Sample IDs |
|---|---|---|---|
| Oncology (fluoropyrimidines, irinotecan, tamoxifen) | 16 (39%) | DPYD, UGT1A1, CYP2D6 | 23U15557, 23S15558, 23U15560, 23T11744, 23U11749, 23U11746, 23W11748, 23R15570*, 23U11752, 24R11022, 24P11023, 24W11025, 24V11017, 24T11018, 24R11019, 24V11020 |
| Psychiatry (psychotropic therapy optimization) | 10 (24%) | CYP2D6, CYP2C19, CYP2C9, CYP1A2, CYP3A4 | 23V15555, 23Q15562, 23Z15563, 23R15570*, 23V15551, 23T15552, 23R15553, 23P15554, 23P15568, 23X15564 |
| Neurology (siponimod therapy) | 7 (17%) | CYP2C9 | 23R11745, 23Z11738, 23Q11740, 23W11751, 24U11012, 24S11013, 24X11016 |
| Gastroenterology (thiopurines) | 3 (7%) | TPMT, NUDT15 | 23T15566, 23R15567, 23Y15569 |
| Transplantation (tacrolimus therapy) | 2 (5%) | CYP3A5 | 23Q15559, 23V15565 |
| Other individual cases | 4 (10% | CYP2D6, CYP2C19, CYP2C9, RYR1 | 23Y11750, 23Q11754, 23V11743, 24S11027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



