Submitted:
18 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Intravenous lipid therapy (ILE) is used to treat neurotoxicosis in companion animals, but clinical evidence for in vivo xenobiotic partitioning and benefit remains limited. This study evaluated associations between the log n-octanol/water partition coefficient (log P), in vivo plasma partitioning, and early neurological outcome. In a case series from eight veterinary hospitals, dogs and cats with suspected neurotoxicosis received ILE; blood collected before and at the end of infusion was separated into lipid and aqueous fractions and analyzed by gas chromatography-mass spectrometry. Log P values were retrieved from PubChem. Outcome (improved vs not improved) was the change from baseline to 4- 6 h after ILE start. Thirty-four cases were analyzed (27 dogs, 7 cats; 17 xenobiotics). At end of infusion, lipid-phase concentrations exceeded aqueous concentrations in 28/34 cases, and log P did not correlate with the lipid-to-aqueous ratio. Improvement occurred in 14/34 animals and was associated with higher lipid-to-aqueous xenobiotic ratios (geometric mean ratio 5.7; 95% CI 1.73–19.05; P = 0.007). Overall, in vivo lipid sequestration was frequent and related to early improvement, whereas log P alone did not predict partitioning or outcome.
Keywords:
log P
; lipid sink
; lipid shuttle
; neurotoxin
; feline
; canine
1. Introduction
Acute neurotoxicosis in companion animals is a common, potentially life-threatening emergency that can require rapid therapeutic interventions [1,2,3]. Conventional decontamination and supportive care suffice in most patients, but severe intoxications often require consideration of adjunctive therapies such as intravenous lipid emulsion therapy (ILE) early in the clinical course [4,5,6,7,8]. Intravenous lipid emulsion therapy has demonstrated efficacy in local-anesthetic systemic toxicity (LAST) in both experimental animals and humans, and has been incorporated into guidelines for severe LAST [9,10,11,12,13]. Its use has since extended to other species and non-LAST poisonings, particularly those causing neurotoxicosis. However, studies of clinical efficacy remain heterogeneous and sometimes contradictory, complicating bedside decision-making [5,8,13,14,15,16,17,18,19,20,21,22,23,24,25]. There are many different, often low-incidence, poisonings that could potentially benefit from ILE therapy [4].
Understanding ILE’s mechanisms of action is therefore essential to guide use across different poisonings. Several mechanisms have been proposed [19]. The lipid sink hypothesis posits an intravascular lipid phase that sequesters lipophilic xenobiotics from the largely aqueous plasma, reducing pharmacologically active (“aqueous” or “free”) concentrations and promoting diffusion away from target tissues such as the central nervous system [10,19]. The lipid shuttle hypothesis extends this concept by proposing that lipid-bound xenobiotics are subsequently and continuously transported to organs of metabolism and elimination [26,27,28]. Clinical studies directly supporting xenobiotic sequestration and its association with clinical outcomes remain limited and often contradictory [6,7,8,19,29].
The log10 n-octanol/water partition coefficient (log P) is commonly used to estimate lipophilicity and predict partitioning behavior [30,31]. A relation between a higher log P and reduction of the xenobiotic concentration in the aqueous fraction has been demonstrated in vitro [29,32]. Several in vitro and in vivo studies have measured decreased aqueous-phase concentrations or demonstrated lipid sequestration for high-log P toxins, typically single local anesthetics [10,27,28,30,33,34,35,36]. Consequently, whether log P accurately predicts in vivo sequestration of xenobiotics other than local anesthetics, and in general, into the lipid plasma phase remains uncertain [8,19,29].
The aim of this study was to evaluate, in companion animals with neurotoxicosis receiving intravenous lipid emulsion therapy, whether an in vitro measure of lipophilicity (log P), correlates with in vivo plasma xenobiotic partitioning and clinical outcome, and whether partitioning was associated with short term neurological outcome.
2. Materials and Methods
2.1. Study Design
Prospective, multicenter case-series conducted at eight European veterinary referral hospitals. All procedures complied with institutional animal care, use requirements and relevant veterinary ethics guidance.
2.2. Study Population
All client-owned dogs and cats with acute neurological signs that were presented between June 2020 and November 2021 were screened. Final enrollment required both a history suggestive of neurotoxin exposure, witnessed or suspected, and a clinical presentation consistent with neurotoxicosis (e.g., acute tremors, ataxia, seizures, altered mentation). Patients with pre-existing conditions that contraindicated lipid infusion, e.g., congestive heart failure, known lipid-metabolism disorders, hypersensitivity to emulsion components, were not enrolled.
2.3. Treatment Protocol
A 20% soybeanoil emulsion (Medialipid® 20% [B. Braun, Melsungen, Germany] or Intralipid® 20% [Fresenius Kabi, Bad Homburg, Germany]) was administered as a 1.5 mL/kg intravenous bolus over 1 min, immediately followed by a continuous infusion at 0.25 mL/kg/min for 60 min. Up to two identical additional cycles were permitted at the clinician’s discretion if clinically indicated and if post-centrifugation plasma was not macroscopically lipemic [6,7].
Intravenous lipid emulsion was used off-label for treatment of toxicosis in veterinary patients at participating centers and according to local regulations and institutional policies.
Concomitant care followed standard of care at the attending clinician’s discretion.
2.4. Blood Sampling and Processing
Samples were drawn immediately before initiation of intravenous lipid emulsion (ILE) therapy (T0), immediately after the infusion ended (T1), and 4 h after completion of the infusion (T5). Depending on patient size, 2–4 mL of blood was collected by venipuncture or via an indwelling catheter into ethylenediaminetetraacetic acid (EDTA) tubes. Whole blood was centrifuged as soon as possible; plasma was separated and stored at −20 °C, then shipped frozen to the laboratory Interactions Cellules Environnement, VetAgro Sup, Campus Vétérinaire, Marcy-l’Étoile, France for further analysis.
After thawing, post-ILE samples (T1 and T5) were centrifuged at 9,000 × g to separate an upper lipid layer and an aqueous plasma phase. Aliquots of pre-ILE plasma (T0) and of both the lipid and aqueous phases (T1 and T5) were subjected to liquid-liquid extraction using ToxiVials type A and B (Advion Interchim Scientific®, Montluçon, France). When sample volume was insufficient, ultrapure water was added to reach the minimum extraction volume.
For extraction, samples were transferred to ToxiVials, mixed, and centrifuged at 2,500 × g for 5 min at 20 °C. The organic supernatant was collected into concentration cups, evaporated to dryness at 37 °C, and reconstituted in 0.5 mL ethanol. Analytical runs included blanks between clinical specimens and a full calibration/quality-control set for each batch.
2.5. Xenobiotic Identification and Quantification
Analyses were performed on an Agilent gas chromatography–mass spectrometry (GC–MS) 5973 (Agilent Technologies Inc., Wilmington, Delaware, USA) with a 30 m capillary column and helium carrier, splitless (3 µL) injection, and the following oven program: 75 °C (0 min), 20 °C min−1 to 200 °C (2 min hold), 8 °C / min to 250 °C (3 min hold), then 25 °C/min to 280 °C (15 min hold; total run-time 33.7 min). Data were acquired in full-scan and selected ion monitoring (SIM) modes; tentative full-scan identifications were confirmed against authentic standards or pharmacy-grade products. Selected ion monitoring quantification used four diagnostic ions per analyte following Lemarchand et al. (2012) and an in-house protocol adapted for lipid matrices [37]. Routine SIM covered >30 xenobiotics, with supplementary calibrations as needed.
2.6. Physicochemical Data
Log P were retrieved from PubChem (accessed April 2024; see also Data Availability below). When multiple xenobiotics were detected in a sample, the xenobiotic with the highest concentration was used for analysis.
2.7. Clinical Outcome
A physical examination focused on neurological signs was conducted by the attending clinicians from baseline through 4–6 h after ILE continuous-rate infusion was stopped. Findings were recorded in a dedicated electronic medical record at each center and subsequently transcribed by a designated clinician onto prespecified data-collection forms. Two experienced reviewers (AV, JCC) independently evaluated the clinical data and produced concise clinical summaries, blinded to xenobiotic identifications and all fraction-specific concentrations. Clinical outcome within the 4–6 h window was rated as a binary endpoint (“improved” versus “not improved”). Discordant reviewer ratings were resolved by discussion, comparing the case summaries and referencing similar cases in the study population to reach a consensus classification for analysis.
2.8. Data Handling and Statistical Analysis
Values for xenobiotic concentrations below the level of quantification (LOQ, 0.01 mg/L) were displayed in tables as “<LOQ” and assigned 0.005 mg/L (½ LOQ) for analyses. Descriptive results are reported as median (range), unless stated otherwise. Associations between log P and post-ILE xenobiotic concentrations, and between log P and the end-of-infusion lipid-to-aqueous ratio, were examined using Spearman’s rank correlation. General linear models were fitted to log10-transformed outcomes to examine these relationships. Model coefficients (β) were back-transformed so that 10^β (the geometric mean ratio, GMR) quantifies the multiplicative change in the outcome per +1 unit of log P or early neurological improvement (improved/not improved). Model validity was assessed by visual inspection of the residuals.
Association between rounded log P values and early neurological improvement (improved/not improved) was tested using a two-sided Fisher’s exact test.
Inter-observer agreement for binary and ordinal ratings was summarized as percent agreement with exact 95% confidence intervals (CIs) and a two-sided exact binomial test versus 50% agreement. Results are presented as estimates with 95% CIs. A P = .05 was considered significant. Given the small sample size and sparse strata, no adjustment models for additional covariates were done. Analyses were prespecified as exploratory to describe patterns and generate hypotheses. All statistical analyses were performed in R version 4.2.3 [38].
3. Results
3.1. Study Population
Eighty-three animals were enrolled (60 dogs, 23 cats) that received a total of 85 ILE treatments with one cat undergoing three cycles. After applying post hoc exclusion criteria 34 cases (27 dogs, 7 cats) remained for further analysis (Figure 1).
Additionally, for paired T0-T1 comparisons, one dog was excluded as this T0 sample was not available, resulting in 33 cases (26 dogs, 7 cats) for T0-T1 comparisons. Given the small number of cats that remained after applying exclusion criteria, statistical analyses were limited to dogs and all animals combined.
Of the dogs, 22 of 27 were purebred and 5 mixed bred. Most common breeds were Labrador Retriever (n = 4) and American Staffordshire Terrier (n = 2). Median age was 2.8 years (0.3–8.8) and body weight 15.6 (2.0–40.0) kg; 17 dogs were female (7 spayed, 10 intact) and 10 male (3 neutered, 7 intact). Four of 7 cats were Domestic Shorthair and 3 had no breed recorded. Median age was 0.9 years (0.2–15.2) and body weight 4.3 (1.5–4.9) kg. Three cats were female (1 spayed, 2 intact) and 4 male (1 neutered, 3 intact).
3.2. Treatments
Upon evaluation of the submitted data it was concluded clinicians did not strictly adhere to the ILE therapy protocol. Twenty-one out of 34 ILE treatments strictly adhered to the treatment protocol. A post-enrollment adjustment was made and a bolus followed by a continuous-rate infusion in the range totaling 15–30 mL/kg within 70 minutes was allowed.
Sedatives were most frequently used (16/34), followed by intravenous crystalloids (13/34) and anti-emetics (10/34), as additional treatments. A single patient could receive more than one treatment and the same treatment at different time points, either before, during or after ILE therapy. Concurrent treatments are summarized in Supplementary Table S1.
3.3. Xenobiotic Identification, Quantification and Physicochemistry
Xenobiotics identified at T1, frequency, and their log P are shown in Table 1.
Seventeen different xenobiotics were identified; permethrin (9/34) and Δ9-THC (6/34) predominated. Log P showed a wide range of 1–7.0, with a median of 4.1.
Samples from T5 were not analyzed further because the lipid phase was usually absent or too small for reliable fraction-specific quantification.
In 14/33 cases (42%), the xenobiotic concentration at either T0, the T1 aqueous or lipid phase was below the lower limit of quantification. The T0 plasma concentration exceeded the T1 aqueous concentration in 12/33 cases (36%), was lower in 11/33 (33%), and equal in 10/33 (30%). Individual fraction concentrations at T0 and T1 are provided in Supplementary Table S2.
At T1, lipid phase concentrations exceeded aqueous in 28/34 cases (82%); the median lipid-to-aqueous ratio was 5.1 (0.04–978) (Figure 2).
3.4. Log P and Xenobiotic Concentrations
Scatterplots of log P versus T1 lipid concentration, T1 aqueous concentration, and the T1 lipid-to-aqueous ratio showed wide dispersion (Figure 3).
- Log P = base-10 logarithm of the n-octanol/water partition coefficient (derived from PubChem)
- Lipid-to-aqueous ratio = lipid fraction concentration divided by the aqueous fraction concentration
Spearman’s rank correlations were weak and not statistically significant in dogs and in all animals combined (Table 2).
In linear models, each 1-unit increase in log P in dogs was associated with a 29% lower T1 aqueous concentration (GMR 0.71; 95% CI 0.54–0.94; P=.02). The association was weak and was not statistically significant when cats were included. No significant associations were identified in the linear models for T1 lipid concentration or for the T1 lipid-to-aqueous ratio in dogs or in all animals combined (Table 3).
3.5. Short-Term Neurological Outcome, Xenobiotic Concentrations, and log P
Generalized tremors were most common at presentation (21/34, 62%), followed by ataxia (18/34, 53%), altered consciousness (15/34, 44%), localized tremors (6/34, 18%), and seizures (5/34, 15%). For early neurological clinical outcome (improved vs not improved), inter-observer agreement was 23/34 (95% CI, 0.50–0.83; P=.058). All discrepancies were resolved satisfactorily by consensus before final analyses. Improvement was recorded in 14/34 cases. Animals that improved had higher T1 lipid-to-aqueous ratios than those that did not (dogs: GMR 8.09; 95% CI 2.31–28.38; P=.003, 709% higher; dogs and cats: GMR 5.75; 95% CI 1.73–19.05; P=.007, 475% higher (Figure 4)).
- Lipid-to-aqueous ratio = lipid fraction concentration divided by the aqueous fraction concentration.
- Boxes show median and range from the first to the third quartile; whiskers extend to values within 1.5 times the interquartile range.
- Early neurological outcome was defined as the neurological improvement from the start of intravenous lipid emulsion administration to 4–6 hours afterwards. Outcome was assessed independently by two observers; disagreements were resolved by consensus.
Analyses of the lipid and aqueous fractions considered separately did not identify significant between-group differences. Figure 5 presents the log P versus early neurological outcome. No association was found between rounded log P values (P = .981).
- Log P = base-10 logarithm of the n-octanol/water partition coefficient (derived from PubChem)
- Boxes show median and range from the first to the third quartile; whiskers extend to values within 1.5 times the interquartile range.
- Early neurological outcome was defined as the neurological improvement from the start of intravenous lipid emulsion administration to 4–6 hours afterwards. Outcome was assessed independently by two observers; disagreements were resolved by consensus.
4. Discussion
In this multicenter clinical case series, xenobiotic concentrations in ILE treated patients were generally higher in the plasma lipid phase compared to the aqueous phase suggesting partitioning to the lipid phase. Moreover, lipid-to-aqueous ratio was positively associated with early neurological improvement. Lipid-to-aqueous ratio and clinical outcome were not associated with log P.
These in vivo observations in a clinical setting suggest lipid-mediated redistribution (lipid sink/lipid shuttle) as a dominant mechanism of ILE therapy in neurotoxicosis, consistent with contemporary reviews that consider the lipid sink/shuttle hypothesis the main mechanism, and cardiometabolic effects as only mainly relevant to the hemodynamically unstable LAST context [19,20,39,40]. Partitioning has been observed in vitro when paired lipid and aqueous fractions were measured in human plasma or serum; xenobiotic concentrations were higher in the lipid fraction than in the aqueous [34,41,42]. Support for a lipid-mediated redistribution as ILE therapy’s primary mechanism was also found in vivo in swine. Amiodarone preferentially entered the lipid phase with lower concentrations in the aqueous (lipid-poor) fraction and was associated with prevention of hypotension [36].
If lipid capture and redistribution is indeed the operative pathway, clinicians need a way to predict how much capture will occur for a given xenobiotic in each patient. The log P naturally suggests itself as the first predictor to test, because it is the standard proposed physicochemical factor for lipophilicity in toxicology and drug design and is widely available [30,31]. The log P may indeed be a good predictor of both xenobiotic plasma distribution and clinical efficacy in case of xenobiotics with an extremely high log P and, under physiological circumstances, are unionized like local anesthetics and permethrin [21,43].
Current reviews and position statements however, recommend moving beyond log P to the distribution coefficients at physiological pH 7.4 (logD7.4) and other descriptors, when estimating whether a xenobiotic will meaningfully partition into the lipid phase in vivo [19,44]. The dissociation coefficient at physiological pH (logD7.4) takes into account the ionized species in water at a pH 7.4 as well, making it more physiologically relevant for in vivo lipophilicity assessment [44]. However, logD7.4 is less available and can yield major method-to-method differences, while computed values vary across software and training sets [25,44]. Still, an in vitro study that evaluated both log P and logD7.4, demonstrated that log P correlated more than logD7.4 with neurotoxic xenobiotic distribution behavior [29]. This suggests logD7.4 on itself also does not reliably predict xenobiotic distribution and ILE therapy efficacy, and several different physicochemical factors could be involved in how effective ILE therapy may be.
Also, in this dataset log P did not associate with the lipid-to-aqueous ratio and clinical outcome, and only modestly with the aqueous concentration. The measured lipid-to-aqueous was associated with early neurological improvement, suggesting that phase partitioning is clinically relevant. However, since log P did not associate with lipid-to-aqueous phase, it does not seem a good in vitro surrogate for phase partitioning, except perhaps in xenobiotics with extreme lipophilicity. This contrasts with earlier in vitro support for using log P to anticipate reductions in the aqueous fraction or lipid sequestration. That support mainly comes from in single-analyte systems and frequently with local anesthetics with an extremely high, and therefore possibly dominant log P [29,33]. Accordingly, caution is warranted against relying on log P alone for triage or efficacy prediction, despite its frequent use in clinical practice [4,32,43,45,46].
The limitations of log P in patients are physicochemically explicable. Log P of a certain toxin assumes the presence of unionized species of a compound, therefore ignores pKa-dependent ionization at physiologic pH, as well as plasma-protein binding, lipid-droplet-surface interactions, the presence of contributing metabolites of a toxin, and several patient-dependent factors (hemodynamics, co-therapies) [47]. As a result, in vitro lipophilicity can diverge markedly from real-world partitioning [19,48]. Li et al. quantified lipid emulsion efficacy with two measures: how many drug molecules each droplet can hold and how quickly molecules move from water into oil. Using calorimetry and a continuous partitioning assay across several drugs, they derived equations that predicted and prospectively confirmed lower plasma concentrations and shorter half-life in rats, outperforming the log P as predictor [49]. Extending such approaches across multiple toxin classes, across species and into clinical sampling frameworks could refine the understanding of the lipid-mediated mechanism in ILE therapy and improve clinical decision-making.
Several important limitations of this study must be acknowledged. Although the initial sample size was substantial, post-exclusion numbers were modest, with very small toxin- and species-specific strata. Precision and power were reduced, the risk of false-negative findings increased, and opportunities to adjust for clustering, explore dose-response, or conduct reliable subgroup analyses were limited. Also, numbers across toxins and species were unequal, which limited generalizability and prevented robust statistical adjustment for clustering.
Multicenter clinician-selected enrolment may have introduced selection bias through site-specific case-mix and referral patterns; with the small post-exclusion sample we could not adjust for site-level clustering. Furthermore, the population was likely enriched for severe intoxications because clinicians selected these cases for adjunctive therapy. Although this reflects current clinical practice, this could increase between-patient variability and can obscure true treatment benefits over a short 4–6-hour observation window.
Protocol deviations from ILE administration were common, which may have introduced noise in associations. The post-enrollment more liberal regimen, i.e., a bolus followed by a continuous-rate infusion in the range totaling 15–30 mL/kg within 70 minutes, was consistent with published veterinary large multicenter data that report a wide ranges of doses including our range [50]. Although not optimal, this is probably acceptable because the immediate pharmacologic objective is to rapidly generate an intravascular lipid phase; guidance and practice therefore use a bolus followed by a short infusion [19]. Once a circulating lipid phase exists, redistribution is thought to be primarily driven by major changes in physicochemistry rather than minor dose-related responses [19,32,40,41,49].
In addition to variability in the ILE treatment itself there was also variability in the concurrent treatment. This allowed clinicians to adhere to standard of care but heterogeneity in treatments could have masked or exaggerated the ILE effect. For both the variability in ILE dosing and in concurrent treatments, numbers were too small to control for possible clustering.
Outcome assessment occurred within a 4–6-hour window after treatment because this was the expected time-frame in which the lipid-sink would be effective [40]. However, in most of our samples the lipid fraction at 5 hours after the start of ILE was very small, possibly indicating the beneficial effect of ILE had largely decreased. Therefore, doing a neurological assessment sooner could have increased sensitivity of associations. Also, our finding of a minimal lipid fraction at 5 hours after the start of ILE led us to discard these samples taken at this second, time-point after ILE therapy. It would have been informative to analyze concentration change over time to see whether for example greater partitioning to the lipid fraction would lead to a greater reduction in concentration over time and if also the lipid-to-aqueous ratio would change.
Despite a broad GC-MS panel, many cases initially included cases were excluded because no xenobiotic was identified, suggesting potential diagnostic error or concentrations below limit of detection. However, it also must be considered that some cases were “misdiagnosed” and were not related to an intoxication. A relatively high number of samples had concentrations below the limit of detection; for analysis these were imputed at half the limit of quantification. These features can bias the toxin spectrum toward more readily detected agents, distort lipid-to-aqueous ratios, and under- or overestimate associations between lipid sequestration and clinical outcome.
Neurological recovery scoring was structured and blinded but unvalidated. Dual independent scoring followed by consensus likely reduced random error but reintroduced subjectivity when initial agreement was suboptimal.
5. Conclusions
In clinical veterinary patients with suspected neurotoxicant exposure, ILE therapy sequestered xenobiotics into a plasma lipid phase in vivo and higher sequestration was associated with early neurological improvement. These findings provide in vivo clinical support for the lipid sink hypothesis. However, log P did not correlate with in vivo sequestration and clinical outcome. It suggests log P should not be used as the single predictor of xenobiotic plasma partitioning; additional physicochemical indicators should be considered, especially when log P is low. Future in vivo clinical studies should consider a more multifactorial predictive approach that considers the relative importance of other physicochemical factors to predict ILE efficacy in neurotoxicosis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Concept & Research Question: J.H.R., A.V., A.K., C.P.-N.; Study Design: C.P.-N., J.H.R., A.V.; Data Collection/Processing: J.C.-C., A.V., J.H.R., C.P.-N., P.B.; Statistical Analysis: J.C.M.V., J.H.R., A.V.; Report Writing: A.V., J.H.R., J.C.M.V., P.B.; Other: A.K. (pharmacology and toxicology interpretation of data; steering initial direction in writing); P.B. (laboratory analyses; methodology description of the toxicological analysis). All authors have read and agreed to the published version of the manuscript.
Funding
Dômes Pharma (Pont-du-Château, France) provided financial support for data collection and laboratory analyses; the funder had no role data analysis, interpretation, and/or manuscript preparation.
Institutional Review Board Statement
The animal study protocol was approved by the Comité d’Éthique de VetAgro Sup, Marcy-l’Étoile, France (protocol code 2055; favorable opinion 3 September 2020).
Informed Consent Statement
Written informed consent was obtained from the owners of all client-owned animals prior to enrolment.
Data Availability Statement
De-identified participant-level data (species, site, ILE regimen, sampling timepoints, GC-MS concentrations, lipid-to-aqueous ratios, adverse events, and 4–6 h neurological outcome scores), the variable codebook, and the analysis code used to generate the results are available from the corresponding author upon reasonable request. Log P values were retrieved in April 2024 from PubChem; PubChem CIDs per xenobiotic are listed in Table 1.
Acknowledgments
We gratefully acknowledge the collaborating veterinary clinics and their staff for support with patient recruitment, data collection, and patient care: Hospital Clínic Veterinari, Universitat Autònoma de Barcelona, Spain (Dr Lluis Bosch); University of Bologna, Italy (Dr Massimo Giunti, Ms Cecilia Bulgarelli); Hospital Veterinario Bom Jesus, Braga, Portugal (Dr João Araujo); Clinique vétérinaire HOPia, Guyancourt, France (Dr Anthony Barthélémy); SIAMU, VetAgro Sup, Marcy-l’Étoile, France; Centre Hospitalier Vétérinaire Meaux, France (Dr Christophe Bille); Oniris – École Nationale Vétérinaire de Nantes, France (Dr Jack-Yves Deschamps, Ms Mallory Salmon); Clinica Veterinaria AniCura Varese, Italy (Dr Linda Perissinotto); and the Universiteitskliniek voor Gezelschapsdieren, Utrecht University, the Netherlands. The authors used Grammarly for Windows (v1.2.220.1800) to assist with language editing (grammar and readability). No new scientific content, analyses, or references were generated by the tool.
Conflicts of Interest
The authors declare no other financial or personal relationships that could have influenced this study. The authors confirm that no third-party material requiring permission has been reused; all figures and tables are original to this work.
References
- Curti, R.; Kupper, J.; Kupferschmidt, H.; et al. Von Hanf bis Schokolade: Tiervergiftungen im Wandel der Zeit. Eine retrospektive Aufarbeitung der Kasuistik des Schweizerischen Toxikologischen Informationszentrums (1997–2006). [A retrospective study of animal poisoning reports to the Swiss Toxicological Information Centre (1997–2006)]. Schweiz Arch Tierheilkd. 2009, 151, 265–273. German. [CrossRef]
- Berny, P.; Caloni, F.; Croubels, S.; et al. Animal poisoning in Europe. Part 2: Companion animals. Vet J. 2010, 183, 255–259.
- Means, C.; Wismer, T. An overview of trends in animal poisoning cases in the United States: 2011 to 2017. Vet Clin North Am Small Anim Pract. 2018, 48, 899–907.
- Markert, C.; Heilmann, R.M.; Kiwitz, D.; et al. Intravenous lipid emulsion for the treatment of poisonings in 313 dogs and 100 cats (2016–2020). Front Vet Sci. 2023, 10, 1272705. [CrossRef]
- Taftachi, F.; Sanaei-Zadeh, H.; Sepehrian, B.; et al. Lipid emulsion improves Glasgow Coma Scale and decreases blood glucose level in the setting of acute non-local anesthetic drug poisoning—a randomized controlled trial. Eur Rev Med Pharmacol Sci. 2012, 16 (Suppl 1), 38–42.
- Robben, J.H.; Dijkman, M.A. Lipid therapy for intoxications. Vet Clin North Am Small Anim Pract. 2017, 47, 435–450.
- Gwaltney-Brant, S.; Meadows, I. Intravenous lipid emulsions in veterinary clinical toxicology. Vet Clin North Am Small Anim Pract. 2018, 48, 933–942.
- Bilvanisi, S.; Gülen, M.; Sabak, M.; et al. Intravenous lipid emulsion therapy in drug overdose and poisoning: An updated review. Eurasian J Med. 2024, 56, 205–212. [CrossRef]
- Hallberg, D.; Holm, I.; Obel, A.L.; et al. Fat emulsions for complete intravenous nutrition. Postgrad Med J. 1967, 43, 307–316.
- Weinberg, G.L.; VadeBoncouer, T.; Ramaraju, G.A.; et al. Pretreatment or resuscitation with a lipid infusion shifts the dose-response to bupivacaine-induced asystole in rats. Anesthesiology. 1998, 88, 1071–1075.
- Weinberg, G.; Ripper, R.; Feinstein, D.L.; et al. Lipid emulsion infusion rescues dogs from bupivacaine-induced cardiac toxicity. Reg Anesth Pain Med. 2003, 28, 198–202.
- Rosenblatt, M.A.; Abel, M.; Fischer, G.W.; et al. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Anesthesiology. 2006, 105, 217–218.
- Neal, J.M.; Barrington, M.J.; Fettiplace, M.R.; et al. The third American Society of Regional Anesthesia and Pain Medicine practice advisory on local anesthetic systemic toxicity: Executive summary 2017. Reg Anesth Pain Med. 2018, 43, 113–123.
- Sirianni, A.J.; Osterhoudt, K.C.; Calello, D.P.; et al. Use of lipid emulsion in the resuscitation of a patient with prolonged cardiovascular collapse after overdose of bupropion and lamotrigine. Ann Emerg Med. 2008, 51, 412–415, 415.e1. [CrossRef]
- Cave, G.; Harvey, M. Intravenous lipid emulsion as antidote beyond local anesthetic toxicity: A systematic review. Acad Emerg Med. 2009, 16, 815–824.
- Crandell, D.E.; Weinberg, G.L. Moxidectin toxicosis in a puppy successfully treated with intravenous lipids. J Vet Emerg Crit Care (San Antonio). 2009, 19, 181–186.
- Cao, D.J.; Heard, K.; Foran, M.; et al. Intravenous lipid emulsion in the emergency department: A systematic review of recent literature. J Emerg Med. 2015, 48, 387–397. [CrossRef]
- Tampakis, K.; Vogiatzakis, N.; Kontogiannis, C.; et al. Intravenous lipid emulsion as an antidote in clinical toxicology: A systematic review. Eur Rev Med Pharmacol Sci. 2020, 24, 7138–7148.
- Jaffal, K.; Chevillard, L.; Mégarbane, B. Lipid emulsion to treat acute poisonings: Mechanisms of action, indications, and controversies. Pharmaceutics. 2023, 15, 1396. [CrossRef]
- Fettiplace, M.R.; Weinberg, G. Lipid emulsion for xenobiotic overdose: Pro. Br J Clin Pharmacol. 2023, 89, 1708–1718.
- Peacock, R.E.; Hosgood, G.; Swindells, K.L.; et al. A randomized, controlled clinical trial of intravenous lipid emulsion as an adjunctive treatment for permethrin toxicosis in cats. J Vet Emerg Crit Care (San Antonio). 2015, 25, 597–605.
- Lundgren, S.; Dreimanis, K.; Engdahl, K.; et al. Alpha-chloralose poisoning in 25 cats: Clinical picture and evaluation of treatment with intravenous lipid emulsion. J Feline Med Surg. 2024, 26, 1098612X241235776. [CrossRef]
- Levine, M.; Hoffman, R.S.; Lavergne, V.; et al. Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity. Clin Toxicol (Phila). 2016, 54, 194–221.
- Behnoush, A.H.; Alizadeh, N.; Emami, M.; et al. Effects of intravenous lipid emulsion administration in acute tramadol poisoning: A randomized controlled trial. J Emerg Med. 2024, 66, 154–162.
- Gosselin, S.; Hoegberg, L.C.G.; Hoffman, R.S.; et al. Evidence-based recommendations on the use of intravenous lipid emulsion therapy in poisoning. Clin Toxicol (Phila). 2016, 54, 899–923.
- Shi, K.; Xia, Y.; Wang, Q.; et al. The effect of lipid emulsion on pharmacokinetics and tissue distribution of bupivacaine in rats. Anesth Analg. 2013, 116, 804–809.
- Litonius, E.; Tarkkila, P.; Neuvonen, P.J.; Rosenberg, P.H. Effect of intravenous lipid emulsion on bupivacaine plasma concentration in humans. Anaesthesia. 2012, 67, 600–605. [CrossRef]
- Heinonen, J.A.; Litonius, E.; Backman, J.T.; Neuvonen, P.J.; Rosenberg, P.H. Intravenous lipid emulsion entraps amitriptyline into plasma and can lower its brain concentration—an experimental intoxication study in pigs. Basic Clin Pharmacol Toxicol. 2013, 113, 193–200.
- Barker, K.; Stewart, M.; Rutter, A.; Tranter, S.; Fellows, L. An in vitro study to determine the impact of lipid emulsion on partitioning of a broad spectrum of drugs associated with overdose. BJA Open. 2024, 10, 100292. [CrossRef]
- Jones, E.; Walton, S.A.; Davis, J.; Council-Troche, M. An in vitro evaluation of intravenous lipid emulsion on three common canine toxicants. Front Vet Sci. 2024, 11, 1482871. [CrossRef]
- Hwang, Y.; Sohn, J.T. Effect of lipid emulsion on neuropsychiatric drug-induced toxicity: A narrative review. Medicine (Baltimore). 2024, 103, e37612. [CrossRef]
- French, D.; Armenian, P.; Ruan, W.; Wong, A.; Drasner, K.; Olson, K.R.; et al. Serum verapamil concentrations before and after Intralipid therapy during treatment of an overdose. Clin Toxicol (Phila). 2011, 49, 340–344. [CrossRef]
- Tikhomirov, M.; Jajor, P.; Śniegocki, T.; et al. Predicting the efficacy of opioid sequestration by intravenous lipid emulsion using biologically relevant in vitro models of drug distribution. Sci Rep. 2022, 12, 18683. [CrossRef]
- Ruan, W.; French, D.; Wong, A.; Drasner, K.; Wu, A.H.B. A mixed (long- and medium-chain) triglyceride lipid emulsion extracts local anesthetic from human serum in vitro more effectively than a long-chain emulsion. Anesthesiology. 2012, 116, 334–339.
- Samuels, T.L.; Willers, J.W.; Uncles, D.R.; et al. In vitro suppression of drug-induced methaemoglobin formation by Intralipid in whole human blood: Observations relevant to the lipid sink theory. Anaesthesia. 2012, 67, 60–67.
- Niiya, T.; Litonius, E.; Petäjä, L.; Neuvonen, P.J.; Rosenberg, P.H. Intravenous lipid emulsion sequesters amiodarone in plasma and eliminates its hypotensive action in pigs. Ann Emerg Med. 2010, 56, 402–408.e2. [CrossRef]
- Lemarchand, C.; Rosoux, R.; Pénide, M.E.; Berny, P. Tissue concentrations of pesticides, PCBs and metals among ospreys (Pandion haliaetus) collected in France. Bull Environ Contam Toxicol. 2012, 88, 89–93. [CrossRef]
- R Core, T.e.a.m. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing;2023.
- Liu, Y.; Zhang, J.; Yu, P.; et al. Mechanisms and efficacy of intravenous lipid emulsion treatment for systemic toxicity from local anesthetics. Front Med (Lausanne). 2021, 8, 756866.
- Lee, S.H.; Sohn, J.T. Mechanisms underlying lipid emulsion resuscitation for drug toxicity: A narrative review. Korean J Anesthesiol. 2023, 76, 171–182.
- Mazoit, J.X.; Le Guen, R.; Beloeil, H.; et al. Binding of long-lasting local anesthetics to lipid emulsions. Anesthesiology. 2009, 110, 380–386.
- Laine, J.; Lokajová, J.; Parshintsev, J.; Kaukonen, A.M.; Kostiainen, R.; Wiedmer, S.K. Interaction of a commercial lipid dispersion and local anesthetics in human plasma: Implications for drug trapping by lipid-sinks. Anal Bioanal Chem. 2010, 396, 2599–2607. [CrossRef]
- Lee, S.H.; Kim, S.; Sohn, J.T. Lipid emulsion treatment for drug toxicity caused by non-local anesthetic drugs in pediatric patients: A narrative review. Pediatr Emerg Care. 2023, 39, 53–59.
- Bhal, S.K.; Kassam, K.; Peirson, I.G.; Payne, A.J. The rule of five revisited: Applying log D in place of log P in drug-likeness filters. Mol Pharm. 2007, 4, 556–560.
- Fernandez, A.L.; Lee, J.A.; Rahilly, L.; et al. The use of intravenous lipid emulsion as an antidote in veterinary toxicology. J Vet Emerg Crit Care (San Antonio). 2011, 21, 309–320.
- Markert, C.; Heilmann, R.M.; Kiwitz, D.; et al. A retrospective evaluation of confirmed and suspected poisonings in 166 cats between 2016 and 2020. Vet World. 2023, 16, 1940–1951.
- Doak, B.C.; Over, B.; Giordanetto, F.; Kihlberg, J. Oral druggable space beyond the rule of 5: Insights from drugs and clinical candidates. Chem Biol. 2014, 21, 1115–1142.
- Manallack, D.T. The pK(a) distribution of drugs: Application to drug discovery. Perspect Med Chem. 2007, 1, 25–38.
- Li, Z.; Li, M.; Sun, H.; et al. Prediction of drug capturing by lipid emulsions in vivo for the treatment of a drug overdose. J Control Release. 2022, 346, 148–157.
- Kiwitz, D.; Markert, C.; Dörfelt, R. Clinical effects and adverse effects of intravenous lipid emulsion treatment in dogs and cats with suspected poisoning. PLoS One. 2024, 19, e0298828.
Figure 1.
Stepwise exclusion flow chart for the final study population (27 dogs and 7 cats) with suspected neurotoxicosis receiving intravenous lipid emulsion therapy. Step 5: A total intravenous lipid emulsion dose of 15–30 mL/kg completed within 70 min (bolus plus short CRI) was sufficient for inclusion; other protocols were excluded.
Figure 1.
Stepwise exclusion flow chart for the final study population (27 dogs and 7 cats) with suspected neurotoxicosis receiving intravenous lipid emulsion therapy. Step 5: A total intravenous lipid emulsion dose of 15–30 mL/kg completed within 70 min (bolus plus short CRI) was sufficient for inclusion; other protocols were excluded.
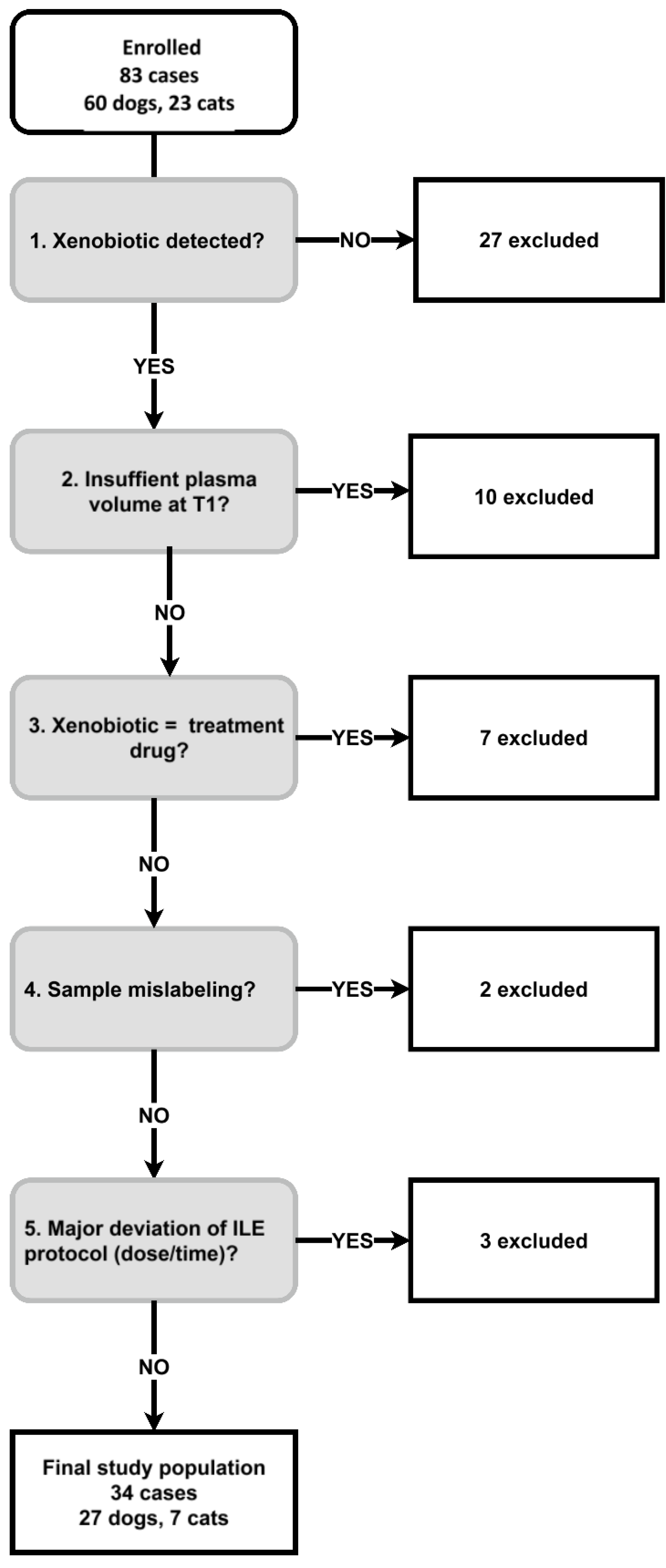
Figure 2.
Xenobiotic plasma concentrations in lipid versus aqueous fraction following intravenous lipid emulsion therapy in 34 companion animals with suspected neurotoxicosis. The limit of quantification (LOQ) was 0.01 mg/L; values reported as “<LOQ” were plotted at 0.005 mg/L (½ LOQ).
Figure 2.
Xenobiotic plasma concentrations in lipid versus aqueous fraction following intravenous lipid emulsion therapy in 34 companion animals with suspected neurotoxicosis. The limit of quantification (LOQ) was 0.01 mg/L; values reported as “<LOQ” were plotted at 0.005 mg/L (½ LOQ).
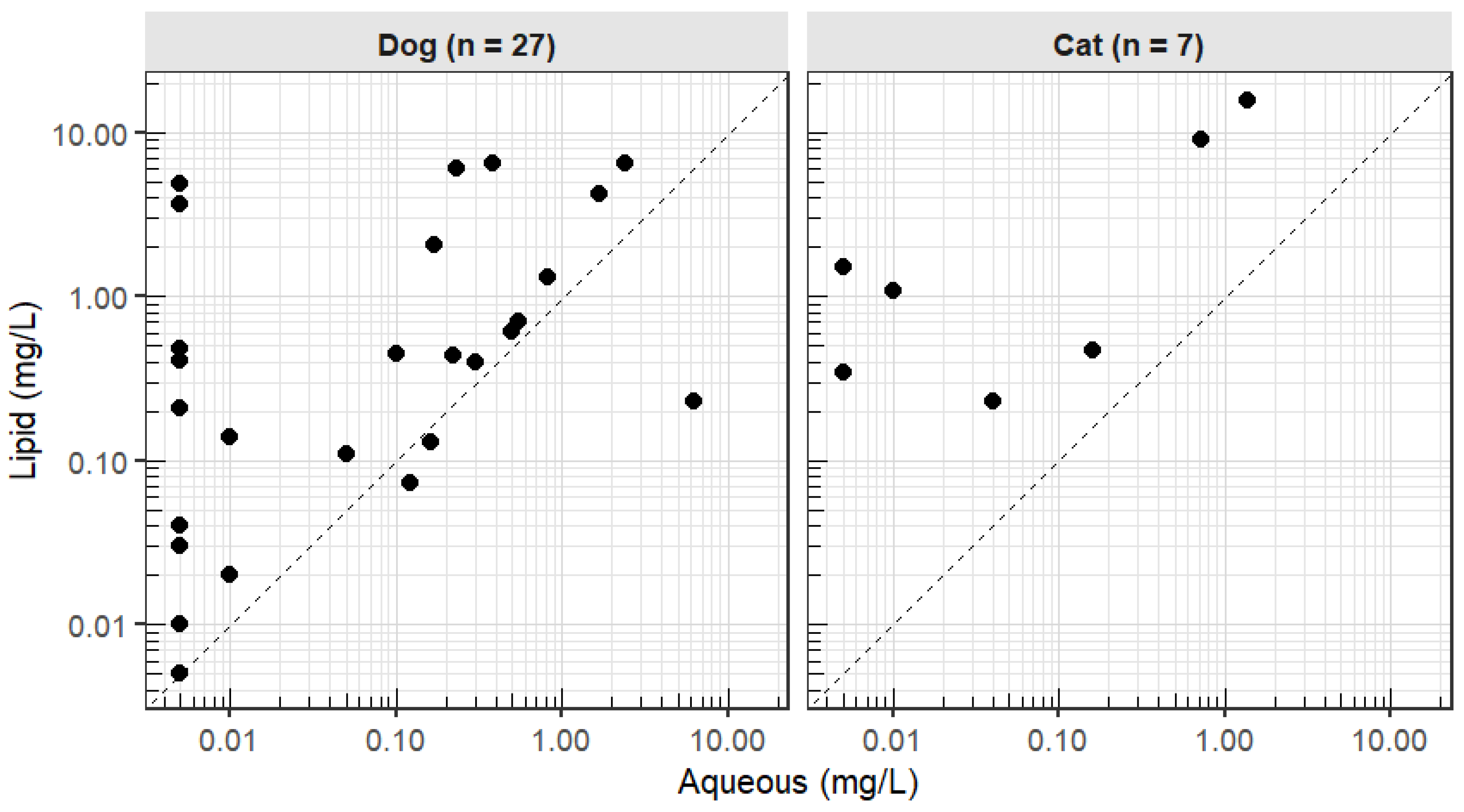
Figure 3.
Xenobiotic plasma concentrations (lipid, aqueous, lipid-to-aqueous ratio) versus log P following intravenous lipid therapy in 27 dogs and 7 cats with suspected neurotoxicosis.
Figure 3.
Xenobiotic plasma concentrations (lipid, aqueous, lipid-to-aqueous ratio) versus log P following intravenous lipid therapy in 27 dogs and 7 cats with suspected neurotoxicosis.
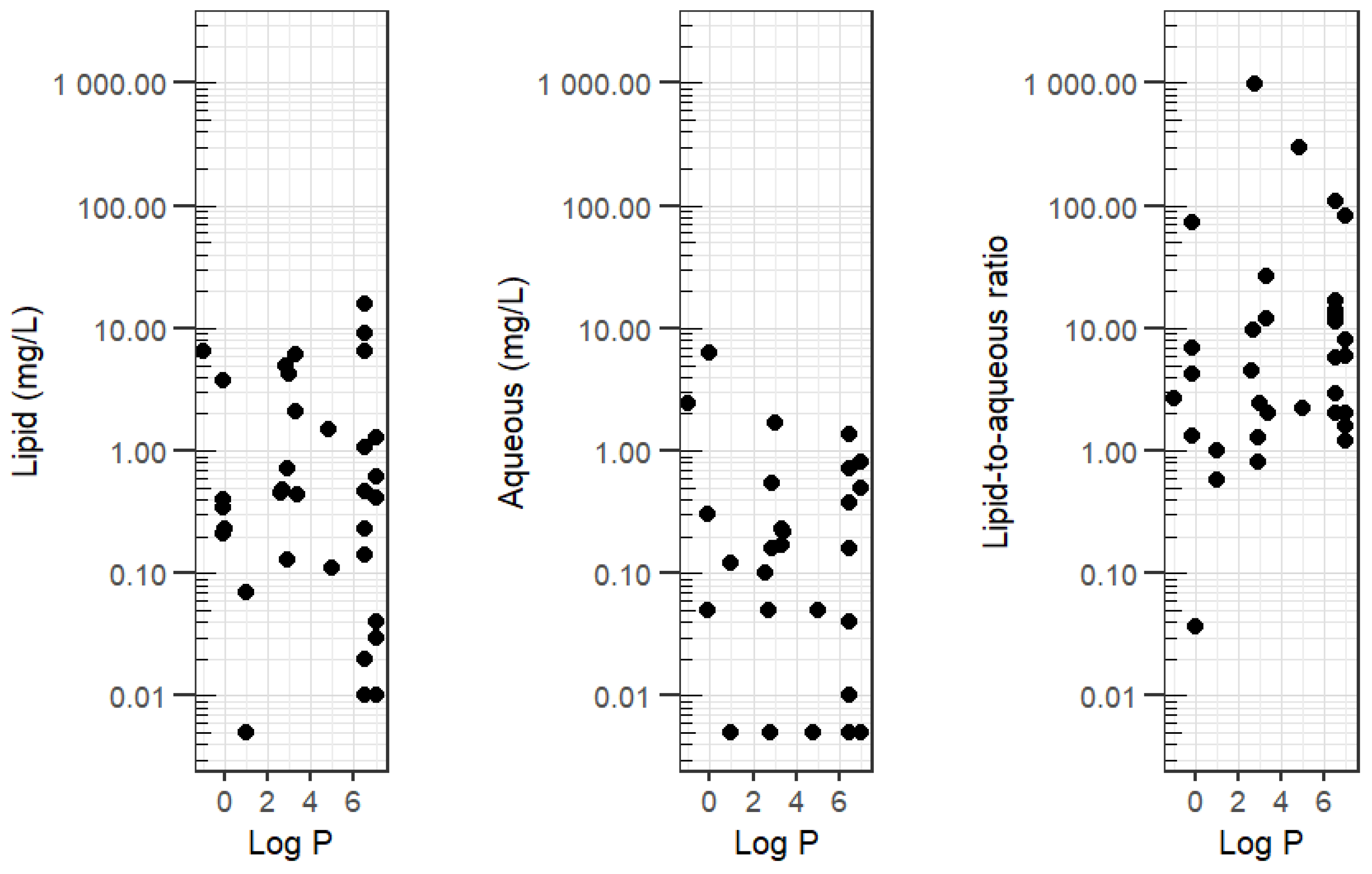
Figure 4.
Xenobiotic lipid-to-aqueous ratio versus early neurological outcome following intravenous lipid emulsion therapy in 27 dogs and 7 cats with suspected neurotoxicosis.
Figure 4.
Xenobiotic lipid-to-aqueous ratio versus early neurological outcome following intravenous lipid emulsion therapy in 27 dogs and 7 cats with suspected neurotoxicosis.
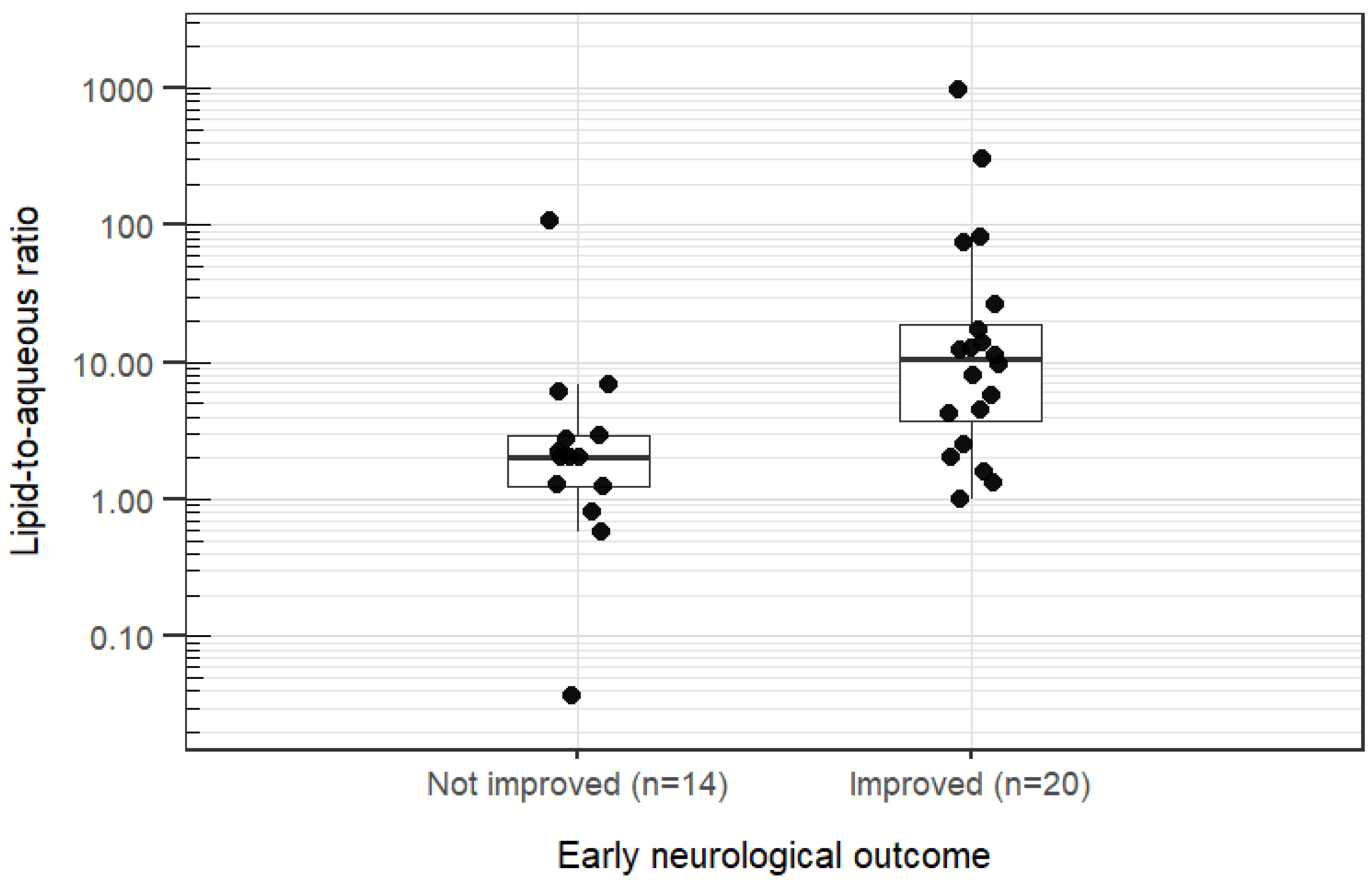
Figure 5.
Log P versus early neurological outcome following intravenous lipid emulsion therapy in 27 dogs and 7 cats with suspected neurotoxicosis.
Figure 5.
Log P versus early neurological outcome following intravenous lipid emulsion therapy in 27 dogs and 7 cats with suspected neurotoxicosis.
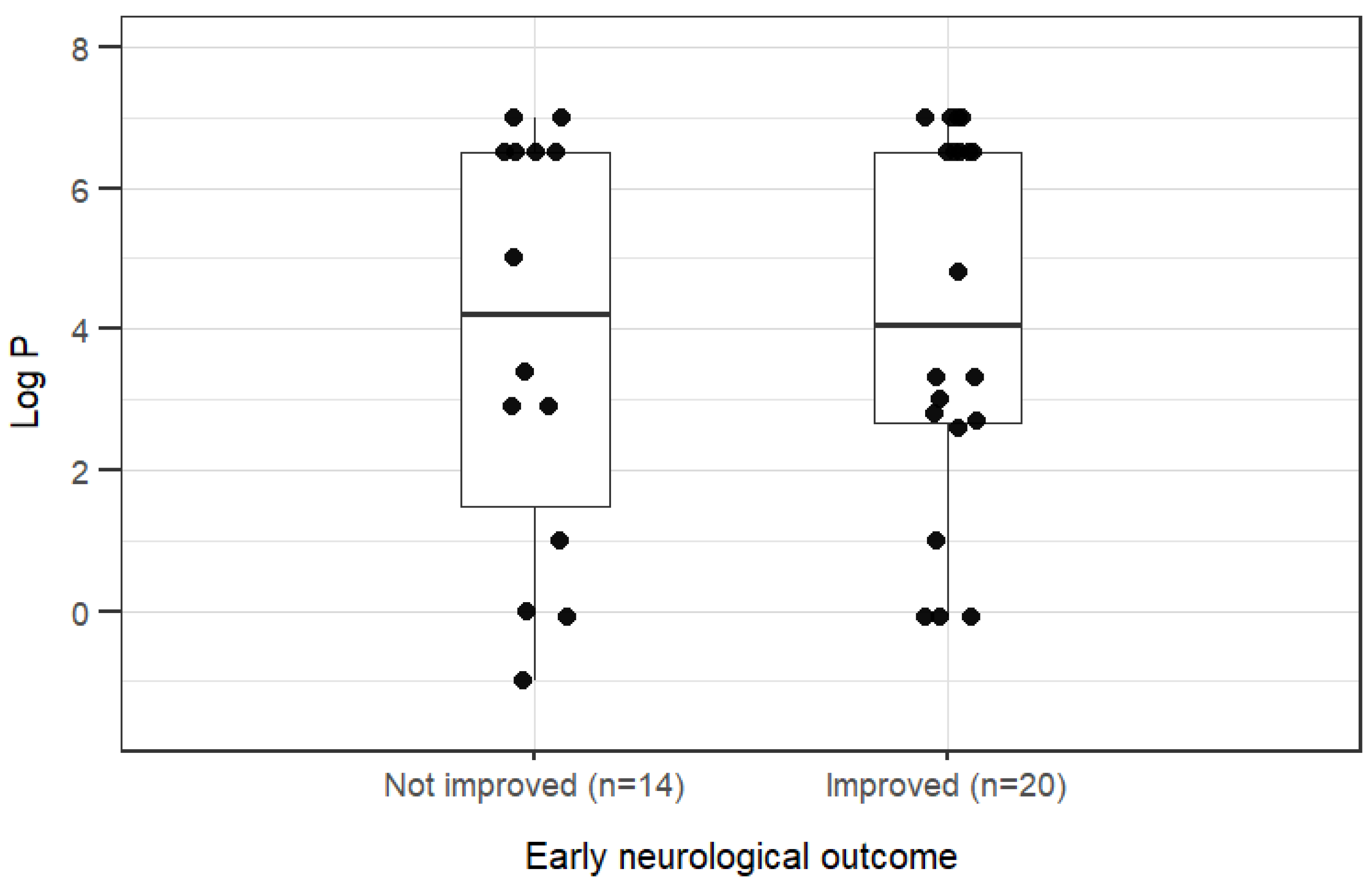

Table 1.
Xenobiotics detected in blood plasma following intravenous lipid emulsion therapy, frequency, and log Pa, in 27 dogs and 7 cats with suspected neurotoxicosis.
Table 1.
Xenobiotics detected in blood plasma following intravenous lipid emulsion therapy, frequency, and log Pa, in 27 dogs and 7 cats with suspected neurotoxicosis.
| Xenobiotic | Dogs and Cats (n) | Dogs (n) | Cats (n) | Log P | CAS RN | PubChem CID |
| Permethrin | 9 | 4 | 5 | 6.5 | 52645-53-1 | 40326 |
| Δ9-Tetrahydrocannabinol | 6 | 6 | 0 | 7.0 | 1972-08-3 | 16078 |
| Diethyl phosphate | 2 | 1 | 1 | -0.2b | 598-02-7 | 654 |
| Alpha-chloralose | 2 | 2 | 0 | 1.0 | 15879-93-3 | 7057995 |
| Pyrilamine | 2 | 2 | 0 | 3.3 | 91-84-9 | 4992 |
| Caffeine | 2 | 2 | 0 | -0.1 | 58-08-2 | 2519 |
| Menthone | 1 | 1 | 0 | 3.0 | 89-80-5 | 26447 |
| Baclofen | 1 | 1 | 0 | -1.0 | 1134-47-0 | 2284 |
| Amitriptyline | 1 | 1 | 0 | 4.9 | 50-48-6 | 2160 |
| Metronidazole | 1 | 1 | 0 | 0b | 443-48-1 | 4173 |
| Geraniol | 1 | 1 | 0 | 2.9b | 106-24-1 | 637566 |
| Menthol | 1 | 1 | 0 | 3.2 | 89-78-1 | 16666 |
| 2,5-Dimethoxy-p-cymene | 1 | 1 | 0 | 3.4b | 14753-08-3 | 6427071 |
| Tramadol | 1 | 1 | 0 | 2.6b | 27203-92-5 | 33741 |
| Olanzapine | 1 | 1 | 0 | 3.0 | 132539-06-1 | 4585 |
| 3,6-Dimethoxy-9H-carbazole | 1 | 1 | 0 | 2.8b | 57103-01-2 | 644464 |
| Pyriproxyfen | 1 | 0 | 1 | 4.8b | 95737-68-1 | 91753 |
| Total | 34 | 27 | 7 | 4.1(-1.0 to 7.0)c |
a Log P = base-10 logarithm of the n-octanol/water partition coefficient; CAS RN: Chemical Abstracts Service Registry Number; PubChemCID: PubChem Compound Identifier (accessed April 2024, see also data availability statement). B Computed values (XLogP3 3.0) are shown when measured log P values were unavailable on PubChem. Median (range).
Table 2.
Spearman correlation between xenobiotic log Pa, plasma fraction concentration (lipid, aqueous), and the lipid-to-aqueous ratiob following intravenous lipid emulsion therapy in 34 companion animals with suspected neurotoxicosis.
Table 2.
Spearman correlation between xenobiotic log Pa, plasma fraction concentration (lipid, aqueous), and the lipid-to-aqueous ratiob following intravenous lipid emulsion therapy in 34 companion animals with suspected neurotoxicosis.
| ρc | pValue | |
| Dogs (n = 27) | ||
| lipid | -0.24 | 0.22 |
| aqueous | -0.31 | 0.11 |
| lipid-to-aqueous ratio | 0.14 | 0.48 |
| Dogs + Cats (N = 34) | ||
| lipid | -0.12 | 0.50 |
| aqueous | -0.26 | 0.14 |
| lipid-to-aqueous ratio | 0.16 | 0.36 |
a Log P: base-10 logarithm of the n-octanol/water partition coefficient (derived from PubChem; accessed April 2024). b Lipid-to-aqueous ratio = lipid concentration divided by the aqueous concentration. c Spearman rank correlation coefficient.
Table 3.
Strength of association xenobiotic log Pa on xenobiotic plasma fraction concentration (lipid, aqueous), and the lipid-to-aqueous ratio following intravenous lipid emulsion therapy in 34 companion animals with suspected neurotoxicosis.
Table 3.
Strength of association xenobiotic log Pa on xenobiotic plasma fraction concentration (lipid, aqueous), and the lipid-to-aqueous ratio following intravenous lipid emulsion therapy in 34 companion animals with suspected neurotoxicosis.
| GMR (95% CI)b | pValue | |
| Dogs (n = 27) | ||
| lipid | 0.80 (0.60–1.07) | 0.14 |
| aqueous | 0.71 (0.54–0.94) | 0.02 |
| lipid-to-aqueous ratioc | 1.13 (0.86–1.48) | 0.39 |
| Dogs + cats (N = 34) | ||
| lipid | 0.91 (0.70–1.19) | 0.50 |
| aqueous | 0.78 (0.61–1.01) | 0.07 |
| lipid-to-aqueous ratio | 1.17 (0.92–1.48) | 0.22 |
a Log P: base-10 logarithm of the n-octanol/water partition coefficient (derived from PubChem; accessed April 2024) b GMR: back transformed geometric mean ratio (10^ β) on the original-scale outcome (mg/L) per +1 unit of log P. c Lipid-to-aqueous ratio = lipid fraction concentration divided by the aqueous fraction concentration.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



