Submitted:
12 February 2026
Posted:
14 February 2026
You are already at the latest version
Abstract
This study examines the political determinants of health access in Africa by analyzing how democratic demand, democratic supply, and perceptions of government health performance shape reported difficulty in accessing health care. We conducted a cross-sectional, multi-country analysis using pooled individual-level data from Afrobarometer Round 8 (2019–2021), comprising 45,589 adult respondents across 34 African countries. Given the hierarchical data structure, we employed generalized estimating equations (GEE) with a logit link to estimate population-averaged associations while accounting for within-country clustering. Health access difficulty was measured as self-reported experiences of going without needed medicines or medical treatment. Democratic demand was operationalized at the individual level, while democratic supply captured country-level perceptions of how democracy functions. We further assessed perceived government handling of basic health services as a mediating mechanism and tested whether democracy moderates socioeconomic inequities in health access. Results indicate that lower democratic supply is strongly associated with higher odds of health access difficulty, independent of individual and community-level factors. Democratic demand exhibits a more complex relationship: individuals with stronger democratic expectations report greater difficulty accessing care, partly mediated by more critical evaluations of government health performance. Mediation analysis confirms that perceptions of government handling of health care explain approximately one-quarter of the total effect of democratic demand on access difficulty. Moderation analyses show that democratic contexts significantly attenuate socioeconomic gradients in health access. Overall, the findings highlight democracy’s dual role as both a structural determinant of health access and an equity-enhancing force in African health systems.
Keywords:
democratic governance
; democratic demand
; democratic supply
; health access difficulty
; health equity
; political determinants of health
; Africa
; government health performance
; socioeconomic status
; mediation analysis
; generalized estimating equations
Introduction
Across Africa, persistent health inequities coexist with substantial variation in democratic governance and public service performance. Despite improvements in aggregate health indicators over recent decades, disparities in access to care, health outcomes, and service quality remain pronounced both within and across countries (Etienne et al., 2010). Scholars and policymakers increasingly recognize that these disparities cannot be explained by economic factors alone. Instead, political institutions, governance quality, and citizen–state relations play a central role in shaping how public resources are allocated and how equitably health systems function (Acemoglu & Robinson, 2013; Sen, 1999).
Democratic governance is commonly theorized as a mechanism through which citizen preferences influence public policy, particularly in sectors, such as health, that are highly sensitive to distributive choices. In democratic systems, competitive elections, political accountability, and civil liberties are expected to incentivize governments to invest in broad-based public goods rather than narrowly targeted benefits (Besley & Kudamatsu, 2006). Empirical research lends partial support to this claim, showing that democracies, on average, perform better than autocracies on indicators such as infant mortality, life expectancy, and responsiveness to health crises (Gerring et al., 2012; Wigley & Akkoyunlu-Wigley, 2017). However, the strength and consistency of this relationship vary considerably, particularly in low- and middle-income regions.
One explanation for this variation lies in the quality of governance rather than the mere presence of electoral democracy. Governance encompasses dimensions such as rule of law, bureaucratic effectiveness, corruption control, and government accountability (Kaufmann & Kraay, 2024). Weak institutions may undermine the potential health benefits of democratic rule by limiting state capacity and distorting service delivery. In several African contexts, democratic reforms have coincided with persistent clientelism, administrative fragility, and uneven implementation of public policies, including in the health sector (Bratton & Van de Walle, 1997; Harrigan et al., 2006). This suggests that democratic governance may influence health equity indirectly, through intermediate mechanisms that translate political accountability into tangible service outcomes.
Public service satisfaction has emerged as one such mechanism linking governance to social outcomes. Satisfaction reflects citizens’ perceptions of accessibility, quality, fairness, and reliability of public services, including healthcare, water, sanitation, and education. From a legitimacy perspective, satisfaction with public services reinforces trust in government and strengthens the social contract, while dissatisfaction can signal governance failures even where formal democratic institutions exist (Rothstein et al., 2012). Empirical evidence from Afrobarometer surveys indicates substantial cross-national and within-country variation in public service satisfaction across Africa, often correlated with perceptions of corruption, responsiveness, and government performance (Bratton et al., 2005).
The link between public service satisfaction and health equity is theoretically grounded in the social determinants of health framework, which emphasizes that health outcomes are shaped by institutional, social, and political conditions rather than healthcare provision alone (Theano, 2010). When citizens perceive health services as available, accessible, affordable, and fair, utilization tends to increase, particularly among marginalized populations, thereby reducing inequities in outcomes. Conversely, dissatisfaction may discourage service use, exacerbate mistrust, and disproportionately harm disadvantaged groups, even when services nominally exist (Gilson, 2003). In African health systems, where out-of-pocket costs, uneven geographic coverage, perceived low service quality, and unavailability of basic/essential medicines remain common, citizen perceptions are especially consequential for equitable access.
Despite these theoretical linkages, existing literature often examines democratic governance, service delivery, or health outcomes in isolation. Studies focusing on democracy and health frequently rely on aggregate outcome measures without accounting for citizen-level perceptions of service performance (Gerring et al., 2012). Conversely, research on public service satisfaction tends to emphasize political trust and regime support, with less attention to downstream health equity implications. Moreover, health equity studies in Africa frequently prioritize socioeconomic or epidemiological explanations while under-theorizing the political and governance context shaping service delivery (Etienne et al., 2010).
This gap points to the need for an integrated analytical approach that simultaneously considers democratic governance, public service satisfaction, and health equity within a multivariate framework. Such an approach allows for the examination of both direct effects—such as the association between governance quality and health equity—and indirect pathways operating through citizen experiences with public services. By situating health equity within broader governance and accountability structures, this perspective aligns with calls for more politically informed health systems research in low- and middle-income countries (Gilson & Raphaely, 2008).
Focusing on Africa is particularly important given the region’s diversity of political regimes, governance capacities, and health system trajectories. From relatively consolidated democracies to hybrid and authoritarian systems, African countries provide a natural laboratory for examining how variations in governance translate into differences in public service satisfaction and, ultimately, health equity. Understanding these relationships is not only of academic interest but also of practical relevance for policymakers seeking to strengthen democratic institutions, improve service delivery, and reduce health disparities in resource-constrained settings. This study had three primary objectives. First, we examined independent associations of democratic demand and democratic supply with health access difficulty across 34 African countries. Second, we tested whether perceived government health performance mediates the democratic demand-health access relationship. Third, we assessed whether democratic governance moderates’ socioeconomic health inequities, examining democracy’s potential as an equity-enhancing force.”
Methods
Study Design and Data Source
We conducted a cross-sectional, multi-country analysis using data from the Afrobarometer Round 8 survey (2019-2021), a nationally representative survey program monitoring social, political, and economic attitudes across Africa. Afrobarometer employs a standardized probability sampling methodology with face-to-face interviews conducted in local languages. The sampling frame consists of a multi-stage, stratified area probability design that generates nationally representative samples within each participating country. For this analysis, we pooled individual-level data from 34 African countries, creating a hierarchical dataset structure with individuals (Level 1) nested within countries (Level 2).
Study Population and Sample
The analytical sample comprised 45,589 adult respondents (≥18 years) from 34 African countries surveyed between 2019 and 2021. Countries were selected based on Afrobarometer’s coverage and data availability. Household sampling employed stratified random selection with probability proportional to population size, followed by random selection of individual respondents within households using Kish tables or similar procedures to ensure within-household randomization.
Measures
Primary Outcome Variable
Health Access Difficulty (HADI). The dependent variable was self-reported difficulty accessing health care, assessed using the Afrobarometer item: “Over the past 12 months, how often, if ever, have you or anyone in your family gone without medicines or medical treatment that you needed?” Responses were dichotomized as 0 = no difficulty (never or only once or twice) and 1 = experienced difficulty (several times, many times, or always). This binary operationalization aligns with public health frameworks emphasizing access as a fundamental determinant of health outcomes and has been validated in previous African health systems research (Health & Organization, 2008).
Primary Predictor Variables
Democratic Demand: Individual-level demand for democracy was measured using Afrobarometer’s multi-item democracy assessment, capturing citizens’ stated preferences for democratic governance versus alternative regime types. Based on the distribution and theoretical considerations, we created a binary indicator where 1 = no democratic demand and 2 = full democratic demand (reference category).
Democratic Supply: Country-level democratic supply represented the institutional quality of democratic governance, measured through citizen responses to questions about their perception of the level of democracy in their country and their satisfaction with how democracy is functioning. Countries were classified into two categories: SSDemo = 1, no democratic supply, and SSDemo = 2 (full democratic supply, reference category).
Mediator Variable
Perceived Government Handling of Health Care: We assessed perceived government performance in health service delivery using the item: “How well or badly would you say the current government is handling improving basic health services?” Responses were coded on a 4-point scale where higher values indicate more favourable evaluations of government health performance.
Control Variables
Demographic Characteristics: Age (Continuous variable measured in years); Gender (Binary indicator, 1 = male, 0 = female as reference).
Socioeconomic Status: Educational Attainment: Four categories (0 = no formal education, 1 = primary, 2 = secondary, 3 = post-secondary education as reference). Employment Status: Binary indicator (1 = employed, 2 = unemployed as reference).
Religious Affiliation: Three categories: 1 = Christian, 2 = Muslim, 3 = Other religions (reference category, including traditional African religions, no religion, and other minority faiths).
Geographic and Contextual Factors. Residence: Binary indicator (1 = rural, 2 = urban as reference). Enumeration Area Infrastructure: Two binary indicators capturing community-level infrastructure: (1) Electricity availability (EA_SVC_A): 0 = absent, 1 = present (reference); (2) Piped water availability (EA_SVC_B): 0 = absent, 1 = present (reference).
Statistical Analysis
Analytical Strategy
We employed a hierarchical analytical strategy with progressively adjusted models to assess the robustness of associations:
- Model 1 (Baseline): Core relationships with minimal demographic adjustment (age, gender)
- Model 2 (Socioeconomic Adjustment): Added educational attainment, employment status, and religious affiliation
- Model 3 (Full Adjustment): Added geographic residence and community infrastructure indicators
Given the clustered nature of our data (individuals nested within countries), we employed Generalized Estimating Equations (GEE) with a binomial distribution and logit link function to predict health access difficulty. GEE was preferred over standard logistic regression because it: (1) accounts for within-country correlation using an exchangeable working correlation structure; (2) provides robust (sandwich) standard errors; (3) produces population-averaged estimates appropriate for policy interpretation; and (4) handles large cluster sizes efficiently. Robust standard errors were clustered at the country level (34 clusters).
Mediation Analysis
We conducted formal mediation analysis using the PROCESS macro for SPSS (Hayes, 2022), implementing Model 4 (simple mediation). The mediation model estimates three key pathways: Path a: Democratic demand → Perceived government health performance (OLS regression); Path b: Perceived government health performance → Health access difficulty (logistic regression); Path c’: Direct effect of democratic demand → Health access difficulty (logistic regression, controlling for mediator).
The indirect effect (a × b) was estimated using bias-corrected bootstrap confidence intervals based on 5,000 resamples. Statistical significance was assessed using 95% bootstrap confidence intervals; intervals excluding zero indicate significant mediation. The proportion mediated was calculated as PM = (a × b) / c, where c = c’ + (a × b) represents the total effect.
Moderation Analysis
To test whether democratic demand moderates socioeconomic health inequities, we specified GEE logistic regression models including: (1) main effects of SES and democratic demand; (2) SES × Democratic Demand interaction term; and (3) full set of covariates. A statistically significant negative interaction coefficient indicates that democratic demand attenuates the association between low SES and health access difficulty—an equity-enhancing moderation pattern. All interaction terms were mean-centred prior to analysis.
Statistical Software and Reporting
All analyses were conducted using SPSS Version 22 (IBM Corp., Armonk, NY). The PROCESS macro version 4.2 (Hayes, 2022) was used for mediation analysis. Statistical significance was assessed at α = 0.05 (two-tailed). We report odds ratios (OR) with 95% confidence intervals for GEE models, unstandardized coefficients (β) with standard errors for mediation paths, and bootstrap 95% confidence intervals for indirect effects.
Ethical Considerations
Data are publicly available through the Afrobarometer Data Portal (www.afrobarometer.org), with this secondary analysis exempt from additional ethical review per institutional policies.
Data Availability
The Afrobarometer Round 8 dataset used in this analysis is freely accessible at www.afrobarometer.org. Statistical code for replication of all analyses is available from the corresponding author upon reasonable request.
Results
Table 1 presents generalized estimating equation (GEE) logistic regression models predicting the likelihood of reporting difficulty in accessing health care among 45,589 respondents. Odds ratios are reported with robust standard errors to account for within-cluster correlation.
Democratic Demand
Across all model specifications, democratic demand is a statistically significant predictor of health access difficulty. Relative to respondents expressing full democratic demand (reference category), those with lower democratic demand exhibit 15–16% lower odds of reporting health access difficulty (ORs ranging from 0.84 to 0.85; p < .05 across models). The consistency of the effect across progressively adjusted models indicates that the association is robust to demographic, socioeconomic, and contextual controls.
Substantively, this pattern suggests that individuals with stronger democratic orientations are more likely to report difficulties in accessing health care, even when objective and contextual factors are held constant. This finding is consistent with an expectations-based interpretation, whereby democratically engaged citizens apply higher standards when evaluating access to public services.
Demographic Controls
Age shows a small but consistent positive association with health access difficulty (OR ≈ 1.001), indicating that older respondents face marginally higher odds of access problems, although the effect size is substantively modest. Gender differences are not statistically significant in any model, suggesting no systematic disparity in reported health access difficulty between men and women after adjustment.
Education
Educational attainment does not emerge as a statistically significant predictor of health access difficulty relative to post-secondary education, although respondents with secondary education show a borderline increase in odds (OR ≈ 1.07, p ≈ .07). Overall, education appears to play a limited independent role once other covariates are included.
Religion
Religion is consistently and significantly associated with health access difficulty. Compared with respondents in the “Other religions” category, Christians and Muslims report significantly higher odds of difficulty accessing health care, with odds ratios ranging from 1.17 to 1.21 (p ≤ .002). These effects are stable across model specifications, indicating persistent group-level disparities that may reflect differences in geographic location, service availability, or reliance on public facilities.
Employment Status
Employment status is not significantly associated with health access difficulty, suggesting that formal employment alone does not confer a clear advantage in health care access once other factors are accounted for.
Place and Infrastructure
Contextual variables reveal important structural effects. Urban residence is associated with 12% higher odds of reporting health access difficulty compared with rural residence (OR = 1.12, p = .015), a finding that likely reflects urban congestion, service overload, or higher expectations rather than absolute service scarcity.
Access to basic infrastructure shows mixed effects. The presence of piped water in the enumeration area is associated with higher reported health access difficulty (OR = 1.15, p = .001), whereas electricity availability is not statistically significant. These results suggest that infrastructure availability alone does not guarantee easier access to health care, and may instead be correlated with urbanization and higher evaluative standards.
As indicated in Table 2, Generalized estimating equation logistic regression results show that democratic supply is a strong and substantively meaningful predictor of health access difficulty. Respondents in contexts classified as no supply of democracy have approximately 48% higher odds of reporting poor health access compared with those in the reference democratic context (OR = 1.48, 95% CI [1.37, 1.60], p < .001). The confidence interval is narrow and far from unity, indicating a large and precisely estimated contextual effect.
Age does not exhibit a statistically meaningful association with health access difficulty, and the gender effect is modest and only marginally significant. The intercept corresponds to a baseline predicted probability of poor health access of roughly 25–30% for individuals in the reference categories.
In model 2, the Generalized estimating equation logistic regression results indicate that democratic supply is a strong and precisely estimated predictor of health access difficulty, even after adjusting for age, gender, education, religion, and employment status. Respondents in contexts classified as no supply of democracy have approximately 48% higher odds of reporting poor health access compared with those in the reference democratic context (OR = 1.48, 95% CI [1.37, 1.60], p < .001). The magnitude and narrow confidence interval indicate a substantively large contextual effect.
Age shows a marginal association with health access difficulty (p = .071), while gender and employment status are not statistically significant in this specification. Among education categories, secondary education is associated with modestly higher odds of poor access (OR = 1.09, p = .033). Religious affiliation exhibits consistent and meaningful associations, with two categories showing 16–21% higher odds of poor access relative to the reference group.
Spatial and infrastructural factors also matter. Urban residents face about 10% higher odds of reporting poor access, and lack of piped water in the enumeration area is associated with significantly worse health access, highlighting the continued importance of basic services

Table 3.
Mediation Analysis of Democratic Demand and Health Access Difficulty through perceived Government Handling of Basic Health Care (N = 45,589). Path a: Effect of Democratic Demand on Perceived Government Handling of Basic Health Care. Path b and c′: Logistic Regression Predicting Health Access Difficulty.
Table 3.
Mediation Analysis of Democratic Demand and Health Access Difficulty through perceived Government Handling of Basic Health Care (N = 45,589). Path a: Effect of Democratic Demand on Perceived Government Handling of Basic Health Care. Path b and c′: Logistic Regression Predicting Health Access Difficulty.
| a | |||||
| Predictor | B | SE | t | p | 95% CI |
| Democratic Demand (DD_Demo) | −0.274 | 0.033 | −8.28 | < .001 | [−0.339, −0.209] |
| R2 = .0015, F(1, 45,587) = 68.51, p < .001 | |||||
| b | |||||
| Predictor | B (log-odds) | SE | Z | p | 95% CI |
| Perceived Government handling of health care | −0.298 | 0.010 | −29.82 | < .001 | [−0.318, −0.278] |
| Democratic Demand (direct effect, c′) | 0.244 | 0.065 | 3.78 | < .001 | [0.117, 0.370] |
| Model fit: −2LL = 54,553.99; Nagelkerke R2 = .031 | |||||
| Direct and Indirect Effects of Democratic Demand on Health Access Difficulty | |||||
| Effect | Estimate (log-odds) | SE / BootSE | p | 95% CI | |
| Direct effect (c′) | 0.244 | 0.065 | < .001 | [0.117, 0.370] | |
| Indirect effect (a × b) | 0.082 | 0.015 | — | [0.053, 0.111] | |
This mediation analysis provides robust evidence that the perceived government handling of basic health care partially mediates the relationship between democratic demand and health access difficulty.
First, higher democratic demand is significantly associated with more favorable evaluations of government handling of basic health care (Path a), indicating that citizens with stronger democratic expectations report better perceived health governance. Second, better government handling of health care is strongly associated with lower odds of experiencing poor health access (Path b), underscoring the central role of governance quality in shaping access outcomes.
Importantly, democratic demand retains a statistically significant direct effect on health access difficulty even after accounting for the mediator, suggesting partial mediation rather than full mediation. The positive indirect effect (log-odds = 0.082, 95% CI [0.053, 0.111]) confirms that a non-trivial portion of democratic demand’s effect on health access operates through perceived government performance in health care.
Figure 1.
Mediation Path Model: Government Health Performance as Pathway from Democratic Demand to Health Access Difficulty. Note. Standardized path coefficients shown. Path a estimated via ordinary least squares regression (R2 = .0015); paths b and c’ estimated via binary logistic regression (coefficients in log-odds metric).
Figure 1.
Mediation Path Model: Government Health Performance as Pathway from Democratic Demand to Health Access Difficulty. Note. Standardized path coefficients shown. Path a estimated via ordinary least squares regression (R2 = .0015); paths b and c’ estimated via binary logistic regression (coefficients in log-odds metric).
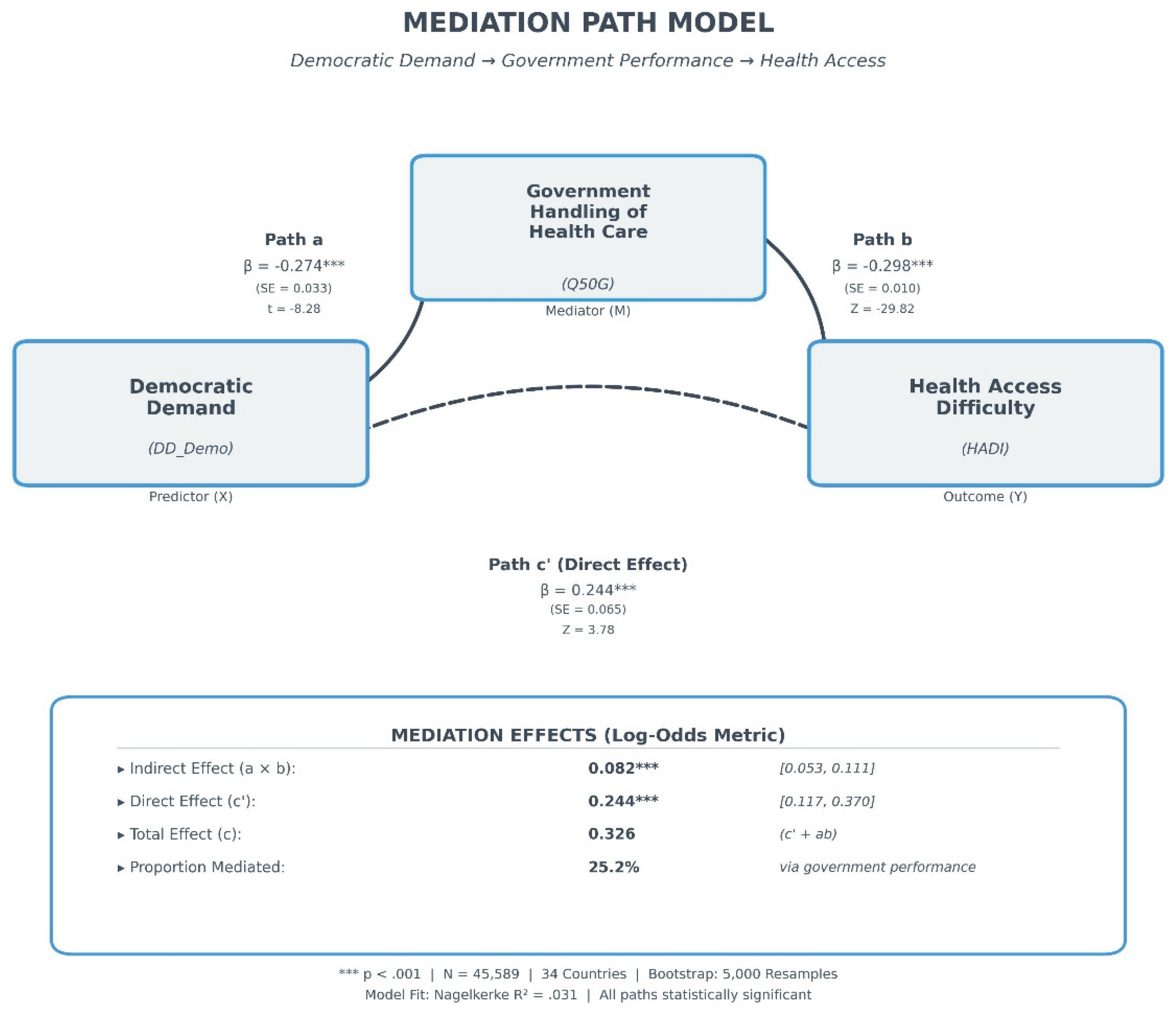
The indirect effect (path a × path b = 0.082) is statistically significant based on 5,000 bootstrap resamples (95% CI [0.053, 0.111]), indicating partial mediation. Approximately 25% of the total effect of democratic demand on health access operates through government health performance perceptions, with the remaining 75% representing direct pathways independent of this mediator. All paths are significant at p < .001. N = 45,589 individuals across 34 African countries (Afrobarometer Round 9, 2021-2023). Model controls for age and gender (not shown for visual clarity). Model fit: Nagelkerke R2 = .031. Bootstrap confidence intervals provide robust inference accounting for sampling variability.
For Path a (Democratic Demand → Government Handling of Health Care), democratic demand is negatively associated with the perceived government handling of basic healthcare service (Path a, B = −0.274, p < .001). Given that higher values of perceived government handling of basic healthcare service represent more favorable evaluations of government handling of basic health care, this result indicates that higher democratic demand is associated with less favorable assessments of government health performance.
Substantively, this suggests that democratically engaged citizens may apply stricter evaluative standards, be more critical of service delivery, or possess greater awareness of governance shortcomings. Rather than reflecting poorer objective performance, the finding is consistent with an expectations mechanism, whereby citizens with stronger democratic orientations evaluate government performance more critically.
For Path b (Government Handling of Health Care → Health Access Difficulty), perceived government handling of health care (Q50G) is negatively associated with health access difficulty (Path b, B = −0.298, p < .001). Higher (more favorable) evaluations of government performance are associated with lower odds of experiencing difficulty in accessing health care. This pathway captures the core service delivery mechanism: better perceived governance in the health sector translates into improved access outcomes for citizens.
Path c′ shows the direct effect of Democratic Demand on Health Access Difficulty. After accounting for government handling of health care, democratic demand retains a positive and statistically significant direct effect on health access difficulty (Path c′, B = 0.244, p < .001). This indicates that higher democratic demand is associated with greater reported difficulty in accessing health care, independent of perceived government performance.
This pattern is consistent with the notion that democratically oriented citizens may report greater access difficulties due to heightened expectations, increased awareness of unmet needs, or lower tolerance for service deficiencies.
Indirect Effect: Mediated Path via Perceived Government Performance
The indirect effect of democratic demand on health access difficulty through perceived government handling of basic healthcare service is positive (Indirect effect = 0.082, 95% CI [0.053, 0.111]). This arises because:
- Democratic demand reduces favorable evaluations of government performance (negative Path a), and
- More favorable government performance reduces health access difficulty (negative Path b).
The product of these two negative paths yields a positive indirect effect, indicating that democratic demand increases reported health access difficulty partly by lowering perceived government performance.
The results support a partial mediation model in which democratic demand influences health access through two complementary pathways:
- An indirect governance-evaluation pathway, whereby higher democratic demand leads to more critical assessments of government health performance, which in turn are associated with worse reported access; and
- A direct expectations pathway, whereby democratic demand independently predicts greater reported access difficulty, likely reflecting higher standards and increased sensitivity to service gaps.
Discussion
Table 1 presents results from a series of generalized estimating equation (GEE) logistic regression models predicting difficulty in accessing health care among 45,589 respondents. The use of GEE accounts for correlated observations within clusters, yielding robust standard errors and population-averaged estimates. Odds ratios (ORs) greater than 1 indicate higher odds of reporting health access difficulty, while values below 1 indicate reduced odds.
Across all model specifications, democratic demand emerges as a consistent and statistically significant predictor of health access difficulty. Compared with respondents expressing full democratic demand (reference category), those with lower democratic demand exhibit significantly lower odds of reporting difficulty accessing health care (ORs ranging from 0.84 to 0.85, p < .05). This suggests that individuals with stronger democratic (governance) expectations may be more critical of service delivery and thus more likely to report barriers to health care access, even after adjusting for sociodemographic and contextual factors (Cohen et al., 2016). Age shows a very small but positive association with health access difficulty. Although the odds ratios are close to unity (OR ≈ 1.001), the effect reaches marginal statistical significance in the more fully adjusted models (p ≈ .05), indicating that older respondents may experience slightly greater difficulty accessing health care. Gender is not a statistically significant predictor across models, suggesting no meaningful difference in reported health access difficulty between men and women after accounting for other covariates. Research shows that political attitudes and institutional trust shape how citizens judge public service delivery, including health systems (Cohen et al., 2016; Scott et al., 2016) . Individuals with stronger democratic values or critical expectations may report more problems when services fall short of their expectations (Grépin & Dionne, 2013; Menon et al., 2025) . This aligns with our interpretation that stronger democratic demand correlates with higher reported difficulty.
Educational attainment, measured relative to post-secondary education, is largely unrelated to health access difficulty. None of the education categories reaches conventional levels of statistical significance, although respondents with secondary education show a marginally higher likelihood of reporting difficulty. This pattern implies that education alone may not be a decisive factor in shaping perceived access to health services once other characteristics are controlled (Jackson, 2009; Zajacova & Lawrence, 2018; Zimmerman et al., 2015). In contrast, religion demonstrates a robust and significant association. Both Christian and Muslim respondents have higher odds of reporting health access difficulty compared with those affiliated with other religions. The magnitude of these effects is moderate but consistent (ORs between 1.17 and 1.21, p ≤ .01), suggesting that religious affiliation may proxy for unobserved cultural, geographic, or socioeconomic factors linked to health service availability or utilization.
Employment status does not significantly predict health access difficulty, indicating that being employed versus unemployed is not independently associated with perceived access barriers in this sample. Evidence in the extant literature is mixed (Eide et al., 2015; Hoven et al., 2023; Minelli et al., 2014; Pharr et al., 2011). However, place-based factors appear more consequential (Eide et al., 2015). Urban residence is associated with higher odds of reporting difficulty accessing health care compared with rural residence (OR = 1.12, p = .015). While counterintuitive, this finding may reflect greater congestion, higher costs, or higher expectations regarding service quality in urban settings. Among community infrastructure variables, the absence of piped water in the enumeration area is significantly associated with greater health access difficulty (OR = 1.15, p = .001), underscoring the importance of basic public infrastructure as a determinant of health system access. In contrast, the presence or absence of electricity in the enumeration area does not show a statistically significant association, suggesting that water infrastructure may be a more salient marker of deprivation relevant to health access in this context. The results indicate that perceived difficulty in accessing health care is shaped by a combination of political attitudes, religious affiliation, age, and community-level infrastructure rather than by gender, employment, or education alone (Aragie et al., 2025; Seidu, 2020). The persistent effect of democratic demand highlights the importance of subjective expectations and political orientations in shaping evaluations of health system performance, while the significance of local infrastructure points to enduring structural inequalities in access to care.
Table 2 reports results from generalized estimating equation (GEE) logistic regression models examining the association between the supply of democracy and reported difficulty in accessing health care among 45,589 respondents. Three nested models are presented, progressively adjusting for individual-level sociodemographic characteristics and community-level infrastructure variables. As in Table 1, odds ratios (ORs) greater than 1 indicate higher odds of reporting difficulty accessing health care. Across all three models, the supply of democracy is a strong and highly significant predictor of health access difficulty. Relative to respondents residing in contexts characterized by a full supply of democracy, those exposed to lower democratic supply exhibit substantially higher odds of reporting difficulty accessing health care (OR ≈ 1.48, p < .001). The stability of this effect across model specifications suggests a robust relationship that is not explained by compositional differences in age, gender, education, religion, employment, residence, or local infrastructure. Substantively, this finding indicates that deficits in democratic supply—such as weaker accountability, limited responsiveness, or constrained institutional performance—are associated with poorer perceived access to essential health services. These findings are consistent with previous studies (Oyèkọ́lá, 2023; Roessler & Schmitt, 2021; Safaei, 2006; Wang et al., 2018) .
Age again shows a very small, positive, but statistically non-significant association with health access difficulty across all models, indicating minimal age-related differences net of other covariates. Gender displays a marginally protective effect for males relative to females (ORs < 1), but this association does not reach conventional levels of statistical significance, suggesting no robust gender disparity in reported access difficulty. With respect to education, respondents with secondary education have significantly higher odds of reporting health access difficulty compared with those with post-secondary education (OR ≈ 1.09, p < .05). No significant differences are observed for respondents with no formal or primary education. This pattern may reflect heightened expectations or greater awareness of service quality among those with intermediate levels of education, rather than objective differences in access. Consistent with Table 1, religious affiliation remains a significant predictor. Both Christian and Muslim respondents are more likely than those in the reference “other religions” category to report difficulty accessing health care, with Muslims exhibiting the largest effect sizes (ORs ≈ 1.21–1.22, p ≤ .001). These associations persist after adjustment for socioeconomic and contextual factors, suggesting that religion may capture broader social, cultural, or geographic dimensions linked to health system access (Idler, 2014; Olivier, 2015; Williams et al., 2010).
Employment status does not significantly predict health access difficulty in any model. However, in the fully adjusted model, urban residence is associated with higher odds of reporting difficulty accessing health care compared with rural residence (OR = 1.11, p = .028). As in Table 1, this counterintuitive finding may reflect congestion, higher transaction costs, or higher expectations of service quality in urban areas, rather than better objective access. Furthermore, community-level infrastructure variables show differentiated effects. The absence of piped water in the enumeration area is consistently associated with increased odds of health access difficulty (OR = 1.15, p < .001), underscoring the role of basic public infrastructure as a marker of structural disadvantage affecting health service access. In contrast, the presence of electricity in the enumeration area is not significantly associated with reported difficulty. Taken together, the findings in Table 2 highlight the central role of democratic supply in shaping perceived access to health care. Even after accounting for individual characteristics and local infrastructure, lower democratic supply is strongly associated with greater health access difficulty. This supports theoretical expectations that democratic institutions and governance quality are critical for effective service delivery and reinforces the importance of political context as a determinant of health system performance alongside socioeconomic and infrastructural factors (Aragie et al., 2025; Seidu, 2020; Williams et al., 2010).
Table 4 presents generalized estimating equation (GEE) logistic regression models assessing whether democracy moderates socioeconomic inequities in difficulty accessing health care among 45,589 respondents. The models progressively adjust for individual demographic characteristics and community-level infrastructure, allowing for an assessment of the robustness of the moderation effect across specifications. Odds ratios (ORs) below 1 indicate reduced odds of reporting health access difficulty.
The central finding across all three models is the strong and statistically significant effect of the SES–Democracy interaction term. The odds ratios are consistently below unity (ORs ranging from 0.895 to 0.900, p < .001), indicating that higher levels of democracy attenuate the association between low socioeconomic status and difficulty accessing health care. Substantively, this suggests that democratic contexts mitigate socioeconomic gradients in health access: as democratic conditions improve, disparities in health access associated with socioeconomic disadvantage are reduced. The stability of this effect across models strengthens confidence in the moderating role of democracy. In contrast, age and gender do not exhibit statistically significant associations with health access difficulty in any model, indicating that, once socioeconomic inequities and democratic context are accounted for, these demographic characteristics play a limited independent role in shaping access barriers. Consistent with earlier tables, religious affiliation remains a significant predictor of health access difficulty. Both Christian and Muslim respondents have higher odds of reporting difficulty accessing health care compared with those in the reference category, with effect sizes remaining stable after adjustment for residence and infrastructure. These findings suggest persistent group-level differences in access that are not fully explained by socioeconomic position or democratic moderation.
Place-based factors again show important associations in the fully adjusted model. Urban residence is associated with significantly higher odds of reporting health access difficulty relative to rural residence (OR = 1.17, p = .002), reinforcing earlier evidence that urban contexts may present distinct barriers to effective access, such as congestion, cost, or service quality mismatches. Similarly, the absence of piped water in the enumeration area is associated with increased odds of health access difficulty (OR = 1.14, p = .001), highlighting the continued importance of basic infrastructure as a determinant of health service accessibility. In contrast, access to electricity in the enumeration area does not significantly predict health access difficulty. The results in Table 4 provide compelling evidence that democracy plays a protective, equity-enhancing role in health systems. By moderating the relationship between socioeconomic status and health access difficulty, democratic contexts appear to reduce the extent to which socioeconomic disadvantage translates into barriers to care. These findings contribute to the literature on political determinants of health by demonstrating not only a direct association between democratic conditions and health access, but also an important conditional effect whereby democracy helps narrow socioeconomic inequities in access to essential health services.
Study Limitation
Several limitations warrant consideration. First, the cross-sectional design precludes causal inference, as reverse causality (health experiences shaping democratic attitudes) or bidirectional relationships cannot be ruled out. Longitudinal panel data are required to establish temporal precedence and test dynamic relationships. Second, the self-reported health access difficulty is subject to recall bias, social desirability bias, and subjective threshold effects, with no objective verification from healthcare utilization records. Dichotomization of the outcome also discards information about the severity and frequency of access barriers. Third, democratic demand and supply are operationalized via perceptual measures rather than objective institutional indicators or behavioral measures of political participation, potentially introducing measurement error and limiting mechanistic inference.
Additionally, the geographic scope is limited to 34 African countries during 2019-2021, restricting generalizability to other world regions, high-income countries, and other time periods. The data collection period encompassed the COVID-19 pandemic onset, which may have temporarily altered relationships. Finally, despite extensive covariate adjustment, residual confounding from unmeasured factors (health literacy, political efficacy, social capital, health insurance coverage, chronic illness burden, state capacity) remains possible. Quasi-experimental designs or randomized interventions would strengthen causal identification.
Despite these limitations, our findings provide robust evidence for democracy’s dual role as a structural determinant and equity-enhancing force in African health systems, with important implications for health policy and democratic development programming.
Conclusion
This study provides comprehensive evidence that democratic governance matters for health access in Africa—not only through institutional supply-side mechanisms but also through citizens’ political attitudes, expectations, and evaluations of government performance. Using nationally representative data from 34 African countries and robust population-averaged modeling techniques, we demonstrate that both the supply of democracy and individual-level democratic demand are systematically associated with reported difficulty in accessing health care. The results show that deficits in democratic supply are consistently linked to poorer access to healthcare. Individuals living in contexts characterized by weaker democratic functioning report substantially higher odds of going without needed medical care, even after adjusting for socioeconomic characteristics, place of residence, and basic community infrastructure. This finding reinforces long-standing theoretical claims that democratic institutions—through accountability, responsiveness, and governance quality—are critical for effective public service delivery. Importantly, the magnitude and stability of this association suggest that democracy operates as a structural determinant of health access, rather than merely reflecting underlying economic or infrastructural conditions. At the same time, the analysis reveals a more nuanced role for democratic demand. Individuals with stronger democratic expectations are more likely to report difficulty accessing health care. Mediation analysis clarifies this relationship by showing that democratic demand is associated with more critical assessments of government handling of health services, which in turn are strongly linked to reported access barriers. Approximately one-quarter of the total effect of democratic demand on health access difficulty operates through these perceptions of government performance, while the remaining effect reflects direct pathways independent of the mediator. This pattern suggests that citizens who value democracy may hold governments to higher standards and are therefore more likely to identify and report shortcomings in service delivery. Rather than indicating worse objective access, higher reported difficulty among democratically oriented citizens may reflect heightened expectations and political awareness. Beyond these direct and mediated effects, a key contribution of this study lies in demonstrating democracy’s equity-enhancing role. The moderation analysis provides compelling evidence that democratic contexts attenuate socioeconomic disparities in health access. In more democratic settings, the association between low socioeconomic status and difficulty accessing care is significantly weaker, indicating that democracy helps buffer disadvantaged groups from structural barriers to health services. This finding advances the literature by showing that democracy not only improves average access outcomes but also shapes how inequalities are translated into lived experiences of access. The study also highlights the importance of place-based and infrastructural factors. Urban residence and the absence of piped water in local communities are consistently associated with higher reported difficulty accessing health care, underscoring that political determinants operate alongside enduring spatial and infrastructural inequalities. In contrast, gender, employment status, and education show limited or inconsistent associations once governance and context are taken into account, suggesting that political and community-level conditions may outweigh individual socioeconomic characteristics in shaping perceived access. Taken together, these findings underscore the need to integrate political context into analyses of health systems performance in Africa. Democracy emerges not as a uniform or simplistic predictor of better health access, but as a multifaceted force that shapes institutions, expectations, accountability, and equity. Policies aimed at improving health access should therefore extend beyond technical health sector reforms to include strengthening democratic governance, enhancing government responsiveness, and addressing the infrastructural foundations of service delivery. By doing so, African health systems may become not only more effective, but also more equitable and politically legitimate.
Author Contributions
Benjamin Otsen: Conceptualization, data curation, Formal Analysis, validation, visualization, writing—original draft, writing—reviewing & editing Samule Asiedu Owusu: Conceptualization, Formal Analysis, validation, visualization, writing—original draft, writing—reviewing & editing. Justice Odoi: Conceptualization, Formal Analysis, validation, visualization, writing—original draft, writing—reviewing & editing. David Oscar Yawson: Conceptualization, Formal Analysis, validation, visualization, supervision, writing—original draft, writing—reviewing & editing. Frederick Ato Armah: Conceptualization, Data curation, Formal Analysis, methodology, supervision, validation, visualization, writing—original draft, writing—reviewing & editing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Availability of data and materials
The data is public and can be found at https://www.afrobarometer.org/data/data-sets/.
Acknowledgments
Not applicable.
Competing Interests
None.
References
- Acemoglu, D.; Robinson, J. A. Why nations fail: The origins of power, prosperity, and poverty; Crown Currency, 2013. [Google Scholar]
- Aragie, H.; Negash, H. K.; Getnet, M.; Tesfaye, W.; Gela, Y. Y.; Asefa, T.; Endale, H. T. Barriers to healthcare access: a multilevel analysis of individual- and community-level factors affecting female youths’ access to healthcare services in Senegal. BMC Health Serv Res 2025, 25(1), 607. [Google Scholar] [CrossRef] [PubMed]
- Besley, T.; Kudamatsu, M. Health and Democracy. American Economic Review 2006, 96(2), 313–318. [Google Scholar] [CrossRef]
- Bratton, M.; Mattes, R.; Gyimah-Boadi, E. Public opinion, democracy, and market reform in Africa; Cambridge University Press, 2005. [Google Scholar]
- Bratton, M.; Van de Walle, N. Democratic experiments in Africa: Regime transitions in comparative perspective; Cambridge university press, 1997. [Google Scholar]
- Cohen, M. J.; Lupu, N.; Zechmeister, E. J. The political culture of democracy in the Americas, 2016/17. Americas 2016, 17. [Google Scholar]
- Eide, A. H.; Mannan, H.; Khogali, M.; van Rooy, G.; Swartz, L.; Munthali, A.; Dyrstad, K. Perceived Barriers for Accessing Health Services among Individuals with Disability in Four African Countries. PLoS One 2015, 10(5), e0125915. [Google Scholar] [CrossRef]
- Etienne, C.; Asamoa-Baah, A.; Evans, D. B. Health systems financing: the path to universal coverage; World Health Organization, 2010. [Google Scholar]
- Gerring, J.; Thacker, S.; Alfaro, R. Democracy and Human Development. The Journal of Politics 2012, 74, 1–17. [Google Scholar] [CrossRef]
- Gilson, L. Trust and the development of health care as a social institution. Soc Sci Med 2003, 56(7), 1453–1468. [Google Scholar] [CrossRef]
- Gilson, L.; Raphaely, N. The terrain of health policy analysis in low and middle income countries: a review of published literature 1994-2007. Health Policy Plan 2008, 23(5), 294–307. [Google Scholar] [CrossRef]
- Grépin, K. A.; Dionne, K. Y. Democratization and universal health coverage: a case comparison of Ghana, Kenya, and Senegal. In Global Health Governance; 2013. [Google Scholar]
- Harrigan, J.; Booth, D.; Cammack, D.; Kanyongolo, E.; Mature, M.; Ngwira, N. Drivers of Change and Development in Malawi; 2006. [Google Scholar]
- Health, W. C. o. S. D. o.; Organization, W. H. Closing the gap in a generation: health equity through action on the social determinants of health: Commission on Social Determinants of Health final report; World Health Organization, 2008. [Google Scholar]
- Hoven, H.; Backhaus, I.; Gerő, K.; Kawachi, I. Characteristics of employment history and self-perceived barriers to healthcare access. Eur J Public Health 2023, 33(6), 1080–1087. [Google Scholar] [CrossRef]
- Idler, E. L. (Ed.) Religion as a Social Determinant of Public Health; Oxford University Press, 2014. [Google Scholar] [CrossRef]
- Jackson, M. I. Understanding links between adolescent health and educational attainment. Demography 2009, 46(4), 671–694. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, D.; Kraay, A. The worldwide governance indicators; 2024. [Google Scholar]
- Menon, A.; Kavanagh, N. M.; Falkenbach, M.; Wismar, M.; Greer, S. L. The role of health and health systems in shaping political engagement and rebuilding trust in democratic institutions. Lancet Reg Health Eur 2025, 53, 101326. [Google Scholar] [CrossRef] [PubMed]
- Minelli, L.; Pigini, C.; Chiavarini, M.; Bartolucci, F. Employment status and perceived health condition: longitudinal data from Italy. BMC public health 2014, 14(1), 946. [Google Scholar] [CrossRef]
- Olivier, J. Religion at the intersection of development and public health in development contexts: From advocacy about faith-based organizations to systems thinking; 2015; pp. 346–358. [Google Scholar]
- Oyèkọ́lá, Ọ. Democracy Does Improve Health. Social Indicators Research 2023, 166(1), 105–132. [Google Scholar] [CrossRef]
- Pharr, J.; Moonie, S.; Bungum, T. The Impact of Unemployment on Mental and Physical Health, Access to Health Care and Health Risk Behaviors; ISRN Public Health, 2011. [Google Scholar] [CrossRef]
- Roessler, M.; Schmitt, J. Health system efficiency and democracy: A public choice perspective. PLoS One 2021, 16(9), e0256737. [Google Scholar] [CrossRef]
- Rothstein, B.; Samanni, M.; Teorell, J. Explaining the welfare state: power resources vs. the Quality of Government. European Political Science Review 2012, 4(1), 1–28. [Google Scholar] [CrossRef]
- Safaei, J. Is democracy good for health? Int J Health Serv 2006, 36(4), 767–786. [Google Scholar] [CrossRef]
- Scott, K. W.; Blendon, R. J.; Benson, J. M. Sick of Health Care Politics? Comparing Views of Quality of Care Between Democrats and Republicans. J Healthc Qual 2016, 38(6), e39–e51. [Google Scholar] [CrossRef] [PubMed]
- Seidu, A.-A. Mixed effects analysis of factors associated with barriers to accessing healthcare among women in sub-Saharan Africa: Insights from demographic and health surveys. PLoS One 2020, 15(11), e0241409. [Google Scholar] [CrossRef]
- Sen, A. Development as Freedom Oxford University Press Shaw TM & Heard. The Politics of Africa: Dependence Development; 1999. [Google Scholar]
- Theano, K. Commission on social determinants of health (2008). Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the commission on social determinants of health; Geneva; world health Organization, 2010; Volume (4), pp. 53–59. Available online: http://www.Who.Int/social_determinants/thecommission/finalreport/en/index. Html.
- Wang, Y.-t.; Mechkova, V.; Andersson, F. Does Democracy Enhance Health? New Empirical Evidence 1900–2012. Political Research Quarterly 2018, 72(3), 554–569. [Google Scholar] [CrossRef]
- Wigley, S.; Akkoyunlu-Wigley, A. The impact of democracy and media freedom on under-5 mortality, 1961-2011. Soc Sci Med 2017, 190, 237–246. [Google Scholar] [CrossRef]
- Williams, D. R.; Mohammed, S. A.; Leavell, J.; Collins, C. Race, socioeconomic status, and health: complexities, ongoing challenges, and research opportunities. Ann N Y Acad Sci 2010, 1186, 69–101. [Google Scholar] [CrossRef] [PubMed]
- Zajacova, A.; Lawrence, E. M. The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Annu Rev Public Health 2018, 39, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, E. B.; Woolf, S. H.; Haley, A.; Quality. Understanding the relationship between education and health: a review of the evidence and an examination of community perspectives. In Population health: behavioral social science insights; Agency for Health-care Research; Rockville, 2015; Volume 22, 1, pp. 347–384. [Google Scholar]
Table 1.
Generalized Estimating Equation Logistic Regression Predicting Health Access Difficulty (N = 45,589).
Table 1.
Generalized Estimating Equation Logistic Regression Predicting Health Access Difficulty (N = 45,589).
| Variable | Model 1 | Model 2 | Model 3 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | |||
| Intercept | 0.428 | 0.094 | < .001 | [0.356, 0.514] | 0.345 | 0.105 | < .001 | [0.281, 0.423] | 0.303 | 0.115 | < .001 | [0.242, 0.380] | ||
| Democratic Demand (ref: Full Demand) | 0.844 | 0.077 | .027 | [0.726, 0.981] | 0.848 | 0.076 | .029 | [0.731, 0.984] | 0.854 | 0.074 | .032 | [0.738, 0.987] | ||
| Age | 1.001 | 0.001 | .105 | [1.000, 1.002] | 1.001 | 0.001 | .057 | [1.000, 1.002] | 1.001 | 0.001 | .049 | [1.000, 1.002] | ||
| Gender (ref: Female) | 0.948 | 0.031 | .087 | [0.891, 1.008] | 0.954 | 0.031 | .128 | [0.897, 1.014] | 0.952 | 0.031 | .110 | [0.897, 1.011] | ||
| Education (ref: post-secondary) | ||||||||||||||
| No formal Education | 0.982 | 0.077 | .809 | [0.844, 1.142] | 0.971 | 0.072 | .686 | [0.843, 1.119] | ||||||
| Primary Education | 1.026 | 0.062 | .683 | [0.909, 1.158] | 1.019 | 0.057 | .742 | [0.912, 1.138] | ||||||
| Secondary Education | 1.074 | 0.039 | .071 | [0.994, 1.160] | 1.071 | 0.039 | .077 | [0.993, 1.156] | ||||||
| Religion(ref: Others) | ||||||||||||||
| Religion (Christianity) | 1.173 | 0.050 | .001 | [1.064, 1.293] | 1.177 | 0.049 | .001 | [1.068, 1.296] | ||||||
| Religion (Muslim) | 1.205 | 0.060 | .002 | [1.071, 1.354] | 1.213 | 0.058 | .001 | [1.083, 1.359] | ||||||
| Employment status (ref: Employed) | 1.033 | 0.028 | .241 | [0.978, 1.091] | 1.030 | 0.027 | .267 | [0.978, 1.085] | ||||||
| Residence (ref: Rural) | 1.121 | 0.047 | .015 | [1.022, 1.230] | ||||||||||
| Electricity in EA (ref: Yes) | 1.043 | 0.051 | .412 | [0.944, 1.151] | ||||||||||
| Piped water in EA (ref: Yes) | 1.154 | 0.042 | .001 | [1.063, 1.252] | ||||||||||
Table 2.
Generalized Estimating Equation Logistic Regression Predicting Health Access Difficulty (N = 45,589).
Table 2.
Generalized Estimating Equation Logistic Regression Predicting Health Access Difficulty (N = 45,589).
| Variable | Model 1 | Model 2 | Model 3 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | |||
| Intercept | 0.363 | 0.101 | < .001 | [0.298, 0.443] | 0.289 | 0.109 | < .001 | [0.234, 0.358] | 0.257 | 0.121 | < .001 | [0.203, 0.326] | ||
| Supply of Democracy (ref: Full supply) | 1.478 | 0.041 | < .001 | [1.365, 1.601] | 1.479 | 0.040 | < .001 | [1.368, 1.599] | 1.478 | 0.040 | < .001 | [1.368, 1.598] | ||
| Age | 1.001 | 0.001 | .109 | [1.000, 1.002] | 1.001 | 0.001 | .071 | [1.000, 1.002] | 1.001 | 0.001 | .062 | [1.000, 1.002] | ||
| Gender (ref: Female) | 0.944 | 0.031 | .064 | [0.888, 1.003] | 0.952 | 0.031 | .105 | [0.896, 1.010] | 0.949 | 0.030 | .083 | [0.895, 1.007] | ||
| Education (ref: Post-secondary) | ||||||||||||||
| No Formal education | 1.015 | 0.077 | .841 | [0.874, 1.180] | 0.996 | 0.072 | .952 | [0.864, 1.147] | ||||||
| Primary Education | 1.046 | 0.064 | .484 | [0.923, 1.185] | 1.032 | 0.058 | .584 | [0.921, 1.157] | ||||||
| Secondary Education | 1.090 | 0.040 | .033 | [1.007, 1.179] | 1.085 | 0.040 | .041 | [1.003, 1.173] | ||||||
| Religion (ref: Others) | ||||||||||||||
| Religion (Christianity) | 1.164 | 0.046 | .001 | [1.063, 1.274] | 1.169 | 0.046 | .001 | [1.067, 1.280] | ||||||
| Religion (Muslim) | 1.211 | 0.059 | .001 | [1.079, 1.360] | 1.222 | 0.058 | < .001 | [1.092, 1.368] | ||||||
| Employment status (ref: Employed) | 1.032 | 0.028 | .257 | [0.977, 1.091] | 1.027 | 0.027 | .314 | [0.975, 1.083] | ||||||
| Residence (ref: Rural) | 1.105 | 0.045 | .028 | [1.011, 1.207] | ||||||||||
| Electricity in EA (ref: Yes) | 1.050 | 0.049 | .322 | [0.953, 1.156] | ||||||||||
| Piped water in EA (ref: Yes) | 1.153 | 0.041 | < .001 | [1.064, 1.249] | ||||||||||
Table 4.
Generalized Estimating Equation Logistic Regression Models Testing Democratic Moderation of Socioeconomic Health Inequities (N = 45,589).
Table 4.
Generalized Estimating Equation Logistic Regression Models Testing Democratic Moderation of Socioeconomic Health Inequities (N = 45,589).
| Variable | Model 1 | Model 2 | Model 3 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | Odds Ratio (Exp(B)) | Robust SE | p | 95% CI for OR | |||
| Intercept | 0.541 | 0.108 | < .001 | [0.438, 0.668] | 0.459 | 0.114 | < .001 | [0.367, 0.574] | 0.407 | 0.122 | < .001 | [0.320, 0.516] | ||
| SESDemocracy | 0.900 | 0.019 | < .001 | [0.867, 0.935] | 0.899 | 0.020 | < .001 | [0.865, 0.934] | 0.895 | 0.018 | < .001 | [0.864, 0.928] | ||
| Age | 1.000 | 0.001 | .546 | [0.999, 1.001] | 1.000 | 0.001 | .560 | [0.999, 1.001] | 1.000 | 0.001 | .492 | [0.999, 1.001] | ||
| Gender (ref: Female) | 0.977 | 0.031 | .453 | [0.919, 1.038] | 0.983 | 0.031 | .580 | [0.925, 1.045] | 0.984 | 0.031 | .602 | [0.926, 1.045] | ||
|
Religion (ref: Others) |
||||||||||||||
| Religion (Christianity) | 1.198 | 0.047 | < .001 | [1.093, 1.314] | 1.196 | 0.046 | < .001 | [1.093, 1.309] | ||||||
| Religion (Muslim) | 1.201 | 0.056 | .001 | [1.077, 1.340] | 1.199 | 0.054 | .001 | [1.079, 1.333] | ||||||
| Residence (ref: Rural) |
1.166 | 0.049 | .002 | [1.060, 1.283] | ||||||||||
| Electricity in EA (ref: Yes) | 1.006 | 0.050 | .902 | [0.913, 1.109] | ||||||||||
| Piped water in EA (ref: Yes) | 1.139 | 0.041 | .001 | [1.052, 1.233] | ||||||||||
NB: SESDemocracy is an interaction term for Socioeconomic status and demand for democracy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



