Submitted:
12 February 2026
Posted:
13 February 2026
You are already at the latest version
Abstract
Background: Hormone receptor-positive/HER2-negative (HR+/HER2−) early breast cancer (EBC) presents a persistent risk of relapse, even beyond 5 years, driving adjuvant intensification strategies. This review analyzes the clinical evidence for CDK4/6 inhibitors (CDK4/6i) in the adjuvant setting and integrates it with molecular findings to support the concept of the “carry-over” effect, understood as a lasting benefit that persists after the end of active treatment, reflected by a sustained separation of invasive disease-free survival (iDFS) curves during follow-up. Relevant sections: The main adjuvant trials in EBC are reviewed, considering the “carry-over” effect. Also, emerging biomarkers and the impact of financial toxicity are described. Results: PALLAS and PENELOPE-B (palbociclib) did not demonstrate an overall benefit in iDFS, with results potentially influenced by discontinuation, toxicity, and risk heterogeneity; however, translational analyses suggest a possible benefit in subgroups defined by biomarkers. In contrast, monarchE (abemaciclib) and NATALEE (ribociclib) showed significant improvements in iDFS, and in the case of abemaciclib, also a signal of benefit in overall survival, supporting the existence of a clinically relevant post-treatment effect. Conclusions: From a biological perspective, the review proposes that “carry-over” would not be a uniform class effect, but rather the result of a sequence of events modulated by pharmacological selectivity (CDK4 vs. CDK6 and additional targets), the induction of cellular senescence, and immunomodulatory effects that could favor the control of micrometastases. In addition, elements that influence interpretation and the need to optimize adherence and toxicity management to “materialize” the benefit in a potentially curable context are discussed.
Keywords:
early breast cancer
; hormone receptor (HR)-positive/HER2-negative
; CDK4/6 inhibitors
; adjuvant therapy
; “carry-over” effect
1. Introduction
Luminal early breast cancer (HR+/HER2− EBC) accounts for approximately 70% of all breast cancer cases and is characterized by an indolent course and a persistent risk of late recurrence, even beyond 5 years after initial treatment [1]. Notably, up to 30% of patients’ experience recurrence, a rate significantly higher than other subtypes of breast cancer, underscoring the importance of targeted treatment strategies. Most patients are diagnosed at an early stage, and the staging (tumor size and nodal involvement) is a strong predictor of recurrence [2].
Major risk factors include family history, older age, prolonged estrogen exposure, and obesity. In patients with HR+/HER2− EBC, these factors are compounded by the possibility of late relapses [3]. The sustained risk of recurrence has driven the study of more effective, targeted therapies such as cyclin-dependent kinases (CDK) 4/6 inhibitors, which, when combined with endocrine therapy (ET), aim to improve invasive disease-free survival (iDFS), a key endpoint associated with delayed metastatic relapse and disease progression [4].
Although CDK4/6 inhibitors such as abemaciclib and ribociclib have been approved for adjuvant treatment of HR+/HER2− EBC, questions remain regarding the optimal ET partner and the main factors that compromise adherence [5]. Likewise, de-escalation strategies and replacement of ET with innovative therapies are being evaluated [6,7].
In this work, we review the clinical evidence from pivotal adjuvant trials of CDK4/6 inhibitors in HR+/HER2− EBC and integrate these data with current molecular insights to examine the biological basis of a “carry-over” effect, defined as a phenomenon that allows HR+/HER2- EBC patients to remain free of invasive recurrence during follow-up. By linking trial outcomes with mechanisms such as kinase selectivity, induction of cellular senescence, and immunomodulatory effects, we aim to provide a clinic molecular perspective on the durability of benefit beyond the active treatment period and its relevance for patient selection and adjuvant treatment strategies.
2. Relevant Sections
To date, there are trials with CDK4/6 inhibitors as adjuvant therapy that have not demonstrated a “carry-over” effect (PALLAS, PENELOPE) and others in which it is observed (monarchE, NATALEE) as shown in Table 1.
- a)
- PALLAS trial
The phase III, open-label PALLAS clinical trial evaluated the efficacy of adding palbociclib for 2 years to adjuvant ET in patients with HR+/HER2− stage II–III EBC (n=5753). No statistically significant improvement in iDFS was achieved: the 3-year iDFS rate was 88.2% with palbociclib + ET vs. 88.5% with ET alone (HR: 0.93; 95% CI, 0.76–1.15; p=0.51) [8]. One of the main factors that may have influenced the results was the high overall discontinuation rate of palbociclib (42.4%), with 21.7% discontinuing due to adverse events, mainly neutropenia and fatigue [8,9]. The most frequent AEs included neutropenia (83.5%), leukopenia (55.1%), and fatigue (41.0%). Even though 58.7% of patients had “high-risk” disease, the potential clinical benefit of treatment may vary depending on the lower-risk proportion. To address this, is vital to contrast palbociclib discontinuation issues with abemaciclib more effective toxicity management strategies, which include proactive dose adjustments and early intervention for side effects such as diarrhea. Toxicity management strategies, a regularly scheduled monitoring and timely dose adjustments can significantly reduce AEs. Early intervention for common side effects can also be crucial. For instance, patients experiencing diarrhea can benefit from immediate anti-diarrheal medications, and those with neutropenia may require growth factor support or temporary treatment pauses to maintain optimal safety and adherence. It positions toxicity management as part of the “carry-over equation” and sharpens clinical relevance by suggesting actionable practice changes to reduce discontinuation rates.
Although subgroup analyses did not show an overall clinical benefit, a subsequent translational analysis identified a composite biomarker (luminal A with ERBB2-related signaling features and/or ER-positive/PgR-negative) that showed a significant improvement in iDFS with palbociclib (HR: 0.55; 95% CI, 0.34–0.90; p=0.017), suggesting that efficacy may depend on appropriate patient selection. Long-term follow-up analysis of the PALLAS trial showed no overall survival (OS) benefit with palbociclib + ET compared with ET alone (5-year OS was 92.6% with palbociclib vs. 93.2% with ET alone, HR 1.09, 95% CI 0.89-1.33, p=0.4051). Moreover, no significant iDFS benefit of palbociclib was observed in any subgroups [9]. Exploratory analyses from PALLAS showed no benefit regardless of clinical stage (IIA vs. IIB/III) [10] or with concomitant medications such as proton pump inhibitors (PPIs); its use was not associated with higher rates of neutropenia [11].
- b)
- PENELOPE-B trial
The PENELOPE-B trial was a phase III, randomized, double-blind, placebo-controlled clinical study that evaluated the efficacy of palbociclib as adjuvant treatment in women with HR+/HER2− EBC with residual disease after neoadjuvant chemotherapy (n=1250). Eligible patients had a “high risk” of relapse, defined by a CPS-EG score ≥3, or 2 with positive nodal involvement at surgery (ypN+). Patients were assigned to receive palbociclib (125 mg orally for 21 days of a 28-day cycle, for 1 year) plus standard ET, or ET plus placebo. The primary endpoint was iDFS, while secondary endpoints included distant recurrence-free survival (DRFS), OS, pharmacokinetics (PK), safety, and quality of life.
After a median follow-up of 42.8 months, the study did not meet its primary endpoint, with an iDFS rate of 81.2% in the palbociclib group vs. 77.7% in the placebo group (HR: 0.93; 95% CI: 0.74–1.17; p=0.525). No significant differences were observed in OS (HR: 0.87; 95% CI: 0.61–1.22; p=0.420) or DRFS. The most frequent AEs with palbociclib were neutropenia (95.7%), leukopenia (99.2%), and anemia (73.9%), with grade 3–4 events in 70.0%, 56.1%, and 3.2%, respectively. The treatment discontinuation rate was 19.6%, with 5.3% attributed to toxicity. PENELOPE-B failed to demonstrate an iDFS improvement in patients with residual disease after neoadjuvant treatment. Despite a selected high-risk population and good treatment adherence, the overall results of PENELOPE-B did not support the routine use of palbociclib [12].
A final survival report from the PENELOPE-B trial showed no significant improvement in iDFS, DRFS, or locoregional relapse rate. No benefits across major subgroups were found, except in lobular breast cancer (LBC), with a trend toward better survival outcomes in favor of palbociclib (HR 0.45, 95% CI 0.19-1.07, p=0.062 for OS and HR 0.52, 95% CI 0.28-0.97, p=0.035 for iDFS) [13].
In an exploratory analysis of the PALLAS and PENELOPE-B trials using molecular subgroups defined by biomarkers, an iDFS benefit was observed only in patients with a favorable genomic profile, which included luminal A subtype and low levels of the serum marker thymidine kinase 1 (TKa) at baseline and after 7 months of treatment (HR 0.63; 95% CI 0.42–0.95; p=0.025), vs. those without these biomarkers (HR: 1.11; p=0.56) [14]. Currently, these biomarkers, are under investigation for clinical application. While not yet standard, they have the potential to enhance patient selection by identifying individuals who may benefit most from CDK4/6 inhibitor therapies.
- c)
- monarchE trial
The phase III monarchE study evaluated the efficacy of abemaciclib in combination with adjuvant ET in patients with HR+/HER2− EBC (n=5637) with “high risk” of recurrence, defined as ≥4 positive lymph nodes (N2), or 1–3 nodes with high-risk features (tumor ≥5 cm, histologic grade 3, or Ki-67 ≥20%). Patients received abemaciclib 150 mg twice daily (BID) for 24 months. At 3 years of follow-up, the abemaciclib + ET group showed a significant improvement in iDFS, with a rate of 89.1% compared to 83.4% with ET alone, reflecting an absolute difference (Δ) of 5.7%. At 5 years, the rates were 86.7% vs. 80.6% with ET alone (HR 0.68; 95% CI 0.599–0.772; p<0.001; Δ 6.5%). Distant metastasis-free survival (DMFS) also improved significantly (HR 0.68; 95% CI 0.565–0.820; p<0.001) with abemaciclib + ET. Regarding safety, common AEs such as diarrhea (83%), neutropenia (45.2%), and fatigue (39.2%) were reported and were generally manageable with dose adjustments [15].
The efficacy of adjuvant abemaciclib was maintained in subgroups such as older patients (≥65 years), although with a higher incidence of gastrointestinal AEs and treatment discontinuations [16].
An update at 6.3 years of follow-up from monarchE continues to demonstrate sustained benefit in iDFS (7-year iDFS: 77.4% with abemaciclib + ET vs. 70.9% with ET), DRFS (7-year DRFS 80.0% with abemaciclib + ET vs. 74.9% with ET alone), and OS (7-year OS: 86.8% with abemaciclib + ET vs. 85.0% with ET alone, Δ 1.8%). The OS benefit was consistent across all evaluated subgroups, including fewer patients with distant metastases in the abemaciclib group. These results support the use of abemaciclib as adjuvant therapy in “high-risk” patients, the first CDK4/6 inhibitor to demonstrate an OS benefit in the adjuvant setting in HR+/HER2− EBC [17]. These outcomes led to the approval of abemaciclib by international health authorities for the treatment of HR+/HER2− EBC patients with node-positive disease at high risk for recurrence [18,19].

Table 1.
CDK4/6 inhibitor trials in HR-positive/HER2-negative early breast cancer.
| Trial | Phase | Treatment | Population (n) | iDFS rate (%) | CDK4/6 inhibitor duration | Long-term follow-up and absolute difference | Toxicity (common AEs) | Key messages |
|---|---|---|---|---|---|---|---|---|
| PALLAS [8,9,10,11] | III | Palbociclib + ET | “High-risk” HR+/HER2− EBC (n=5753) |
88.2 | 2 years | 3 years No “carry-over” effect |
Neutropenia (83.5%) |
|
| PENELOPE-B [12,13] |
III | Palbociclib + ET | HR+/HER2− EBC (n=1250) |
81.2 | 1 year | 42.8 months No “carry-over” effect |
Neutropenia (95.7%) |
|
| monarchE [15,16,17,18,19] | III | Abemaciclib + ET | High-risk stage II–III HR+/HER2− EBC (n=5637) |
86.7 | 2 years |
|
Diarrhea (83%), neutropenia (45.2%), fatigue (39.2%) |
|
| NATALEE [20,21,22,23] | III | Ribociclib + ET | Stage II–III HR+/HER2− EBC, including N0 (n=5101) |
90.4 | 3 years |
|
Neutropenia (44% grade 3–4), elevated liver enzymes, QTc prolongation |
|
* Notes Δ: Absolute difference; AEs: adverse events; DRFS: distant recurrence-free survival; EBC: early breast cancer; ET: endocrine therapy; HR+: hormone receptor positive; iDFS: invasive disease-free survival, OS: overall survival; TKa: Thymidine Kinase.
One important consideration is that the absolute benefit of abemaciclib over ET alone in terms of iDFS (Δ 6.5%), DRFS (Δ 5.1%), and OS (Δ 1.8%), is maintained throughout follow-up, supporting the hypothesis of a potential “carry-over” effect associated with this CDK4/6 inhibitor. These percentages translate into a tangible impact on patient care, potentially reducing the risk of disease recurrence and prolonging survival. During patient counseling or shared decision-making between clinicians and patients, these figures can help discuss the value of incorporating abemaciclib into adjuvant therapy. This data-driven dialogue can empower patients to make informed choices about their treatment options, balancing efficacy with life-quality considerations. As Figure 1 illustrates, the sustained plateau in iDFS over time visually supports the assertion of a “carry-over” effect, suggesting a long-term benefit beyond active treatment
- d)
- NATALEE trial
The phase III, randomized, open-label NATALEE clinical trial evaluated the efficacy of ribociclib combined with ET, specifically a nonsteroidal aromatase inhibitor (NSAI), as adjuvant treatment in patients with stage II and III HR+/HER2− EBC (n=5101). Patients received ribociclib at a dose of 400 mg daily (3 weeks on treatment followed by 1 week off) for 36 months, in combination with an NSAI administered for at least 60 months. At 3 years, iDFS was significantly improved with ribociclib plus NSAI compared with NSAI alone (90.4% vs. 87.1%; HR for invasive disease, recurrence, or death, 0.749; 95% CI 0.62–0.91; p=0.0012), Δ 3.3%. This effect was maintained across evaluated subgroups, including node-negative patients (N0), those with stage II–III disease, and premenopausal patients. The most frequent AEs with ribociclib were neutropenia (44% grade 3–4), elevations in liver enzymes, and corrected QT-interval (QTc) prolongation, which occurred less frequently with the dose used than with the metastatic setting (600 mg). Almost 20% of patients discontinued ribociclib due to toxicity, despite the reduced dose. NATALEE included a broad patient population, expanding its clinical applicability [20].
Similar to the monarchE study, a “carry-over” effect with adjuvant ribociclib is observed in IDFS during follow-up (Figure 2). A key question for future trials is the optimal duration of ribociclib treatment: is there a greater benefit with a 36-month course than with a 24-month one? Currently, the recommended duration for ribociclib in adjuvant therapy is 36 months. This question could guide the design of next-step trials and help refine treatment protocols by determining if extending the duration further enhances long-term outcomes.
During 4 years of follow-up, iDFS was 88.5% with ribociclib + ET vs. 83.6% with ET alone (HR 0.715; p<0.0001), Δ 4.9% [21]. A 5-year follow-up update showed that ribociclib + ET continues to provide a benefit vs. ET alone in HR+/HER2− EBC (Δ 4.5%) in iDFS and across all subgroups, including N0 disease (HR 0.60). The OS follow-up is ongoing, with a trend toward improvement in favor of ribociclib (HR 0.80, 0.637-1.003, p=0.026) [22]. NATALEE results have also enabled regulatory approval of ribociclib in a broad group of patients [23].
4. Discussion
Understanding the “Carry-Over” Effect: Molecular Mechanisms and Pathways
- a)
- Selectivity of CDK4/6 inhibitor
CDK4/6i are orally administered small molecules that competitively bind to the adenosine triphosphate (ATP)-binding cleft of CDK4 and CDK6 [24]. Although they all share the same primary mechanism of action, they exhibit distinct biochemical properties that influence their selectivity. Palbociclib and ribociclib are structurally similar, derived from a pyrido [2,3-d]pyrimidin-7-one scaffold [25], which features a large lipophilic chain. In contrast, abemaciclib is derived from a 2-anilino-2,4-pyrimidine–[5-benzimidazole] scaffold [24]. Structural differences could lead to variations in binding affinity and kinase selectivity; specifically, differentiation in CDK4 versus CDK6 affinity has been correlated with divergent survival outcomes in previous trials. Palbociclib shows relatively balanced inhibitory activity against CDK4 (Half-maximal Inhibitory Concentration [IC₅₀] ~11 nanomolar [nM]) and CDK6 (IC₅₀~15 nM), while ribociclib (CDK4 IC₅₀~10 nM, CDK6 IC₅₀~39 nM) and abemaciclib (CDK4 IC₅₀~2 nM, CDK6 IC₅₀~9.9 nM) display greater selectivity for CDK4. Notably, abemaciclib also targets other CDK family members (CDK1, CDK2, CDK5, CDK9, CDK14, CDKs16-18, GSK3α/β, CAMKIIγ/δ, and PIM1 kinases) [26]. This could contribute to a “carry-over” effect by inducing cellular senescence during follow-up and may therefore not represent a true “class effect” shared by all CDK4/6 inhibitors [27].
- b)
- Induction of cellular senescence
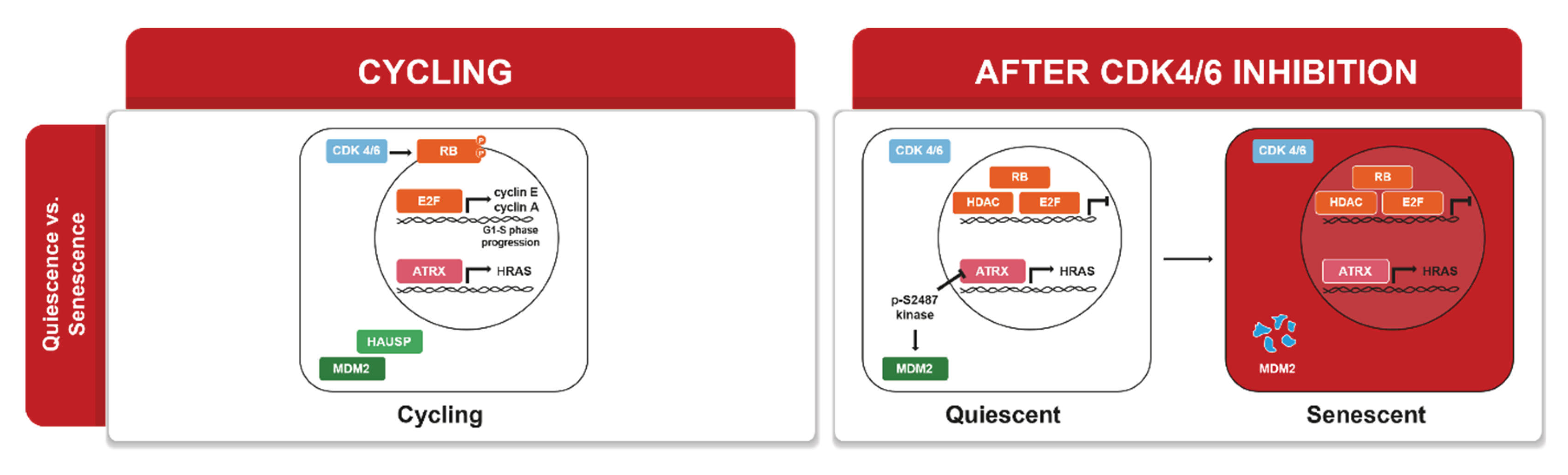
CDK4/6 inhibitors lead to a cytostatic arrest of tumor cells in the G1 phase by maintaining Retinoblastoma Protein (pRB) in an unphosphorylated state. A key question is whether this arrest is transient (reversible quiescence) or becomes permanent (senescence). Studies have observed events such as the redistribution of alpha-thalassemia mental retardation X-linked (ATRX) gene on chromatin and sustained repression of proliferation promoters (e.g., HRAS, MYC) necessary to lock in the senescent state (Figure 3) [28]. Senescent cells often develop a Senescence-Associated Secretory Phenotype (SASP), characterized by the secretion of cytokines, chemokines, and proteases. For instance, palbociclib has been shown to induce the overexpression of VCAM-1 and other pro-inflammatory SASP molecules in endothelial cells. Due to its additional inhibition of CDK9 and CDK2, abemaciclib produces unique transcriptional changes. CDK9, part of the Positive Transcription Elongation Factor b (P-TEFb) complex necessary for transcriptional elongation, when inhibited, can lead to a marked reduction in the expression of short-lived genes such as MYC and Myeloid Cell Leukemia-1 (MCL1) [29].
In fact, abemaciclib has been observed to decrease MYC levels more significantly than the other inhibitors and to rapidly sensitize MCL1-dependent cells to apoptosis. Additionally, abemaciclib may inhibit Glycogen Synthase Kinase 3 Beta (GSK3β), thereby activating the Wnt/β-catenin pathway and stabilizing nuclear β-catenin. Although Wnt/β-catenin typically promotes proliferation, in the presence of CDK4/6 blockade, the resulting cyclin D accumulation cannot drive the cycle forward and may sequester CDK inhibitors, altering feedback loops [30]. Palbociclib and ribociclib do not significantly impact the Wnt/GSK3β pathway [31]. A trial that described the dose-response curves showed that abemaciclib was found to be 5.5 times more potent at inducing cytostasis than palbociclib based on growth rate 50 (GR50) values [32].
- c)
- Immunomodulation by CDK4/6 inhibitors
Preclinical evidence suggests that CDK4/6 inhibitors exert antitumor effects not only through senescence but also through immunomodulation, which is a second, and perhaps equally critical, component of their therapeutic action. By positioning immune effects as a co-equal driver of the “carry-over” effect, new possibilities for synergy with immune-checkpoint inhibitors can be explored [33]. Proposed mechanisms include cell-cycle blockades, modulation of energy metabolism, induction of autophagy, and enhancement of immune responses. These effects arise through interactions between tumor cells and immune cells, tumor-antigen presentation, and SASP release that leads to recruitment of immune cells, activation of effector T lymphocytes, depletion of regulatory T cells (Tregs), and depletion of myeloid-derived suppressor cells (MDSCs), which are potent inhibitors within the tumor microenvironment [34].
- d)
- “Carry-over” as a “series of events”
The “carry-over” effect of CDK4/6 inhibitors is likely not a single phenomenon in HR+/HER2− EBC, but rather the occurrence of multiple events such as eradication of micrometastatic disease during a critical treatment period (preventing the growth of metastatic niches in bone or lymph nodes in HR+/HER2− breast cancer), or cellular reprogramming that leads to non-proliferative states with durable responses (senescence) [35]. In a study conducted in mice and breast cancer patients, CDK4/6 inhibition was observed to reveal a senescent state through SASP activation in p53-enriched targets, without reliance on pro-inflammatory components [36].
Another event is a “post-treatment” effect that persists during follow-up. In NATALEE, the iDFS benefit after completing 3 years of ribociclib reinforces the “carry-over” hypothesis, supporting the idea that a finite duration of a CDK4/6 inhibitor can translate into long-term iDFS gains (while OS remains immature, the trend favors improvement).
5. Future Directions
Additional considerations regarding the “carry-over” effect
- Statistical analysis and trial design: Interpreting the “carry-over” effect may require statistical caution, as Kaplan–Meier curves can show delayed separation or non-proportional hazards depending on the treatment, making time-period analyses important. In addition, differences in trial design, high treatment discontinuation rates, and potential informative bias complicate interpretation. Although iDFS is an emerging endpoint in EBC, it has not yet been validated as a surrogate endpoint for OS in this setting [37].
- Type of oncologic treatment and “delayed effects”: For treatments such as immunotherapy, there are reports that reflect a delayed effect, which is typical for these agents, in contrast to targeted therapies such as CDK4/6 inhibitors, which produce faster response times (8–9 weeks) and, with the “carry-over” effect, may also maintain post-treatment responses [38].
- Early resistance and biomarkers: In HR+/HER2− EBC, several biomarkers of early resistance are being evaluated, such as cyclin E1 (CCNE1) amplification, which may explain failure with palbociclib and ribociclib in certain patient subgroups through parallel activation of the CDK2 pathway, “bypassing” CDK4/6 inhibition and leading to accelerated tumor growth and poor outcomes in the metastatic setting [39]. Another emerging biomarker is circulating tumor DNA (ctDNA) to detect minimal residual disease (MRD) and to guide strategies for treatment intensification or de-escalation [40]. Currently, the implementation of CCNE1 amplification or ctDNA MRD testing in routine clinical practice varies. While some centers have started incorporating these tests to better stratify patient treatment plans, their broad use is still limited due to the need for further validation and consensus on clinical guidelines. Clinicians should consider these biomarkers’ availability and integrate them into treatment discussions where applicable to tailor therapies more effectively [41].
- Clinical benefit in a potentially “curable” setting: The clinical relevance of the “carry-over” effect depends on patients achieving sufficient drug exposure. Therefore, prevention and proactive management of toxicities (e.g., diarrhea with abemaciclib, transaminitis and QTc prolongation with ribociclib), as well as maintaining adherence, are essential to preserve the “carry-over” mechanism. Since these patients are potentially “curable”, it is crucial to emphasize that in HR+/HER2− EBC, adjuvant therapy is not only about efficacy, but also about quality of life and tolerability, including discontinuations due to adverse events from adjuvant CDK4/6 inhibitors [42].
- “Financial toxicity”: The decision to use CDK4/6 inhibitors such as abemaciclib and ribociclib by agencies such as the National Institute for Health and Care Excellence (NICE) guidelines highlights the relevance of the “carry-over” effect as a treatment strategy that impacts health-system budgets (treatment duration + cost + adherence + toxicity and toxicity-related costs) [43,44].
- “De-escalation” strategies in HR+/HER2− EBC: Recently, at the 2025 San Antonio Breast Cancer Symposium (SABCS), the lidERA study showed an iDFS benefit with giredestrant [a next-generation oral selective estrogen receptor degrader (SERD)] 30 mg orally once daily (QD) vs. ET alone (3-year iDFS: 92.4% with giredestrant vs. 89.6% with standard ET; HR 0.70; 95% CI 0.57–0.87; p=0.014) [45]. This strategy of replacing classic ET (tamoxifen and NSAI) with an oral SERD is likely to generate intense debate between intensification vs. replacement (“de-escalation”) strategies for adjuvant therapy in HR+/HER2− EBC. Currently, giredestrant and similar SERDs are being reviewed for regulatory approval, with expectations that they will be recommended for HR+/HER2− EBC patients who may not benefit optimally from traditional ET. These advancements could significantly influence clinical decision-making by offering a tailored approach to treatment.
6. Conclusions
Evidence shows a “carry-over” effect with the CDK4/6 inhibitors abemaciclib and ribociclib + ET in HR+/HER2− EBC as a treatment-intensification strategy, with improvements in iDFS, DRFS, and, more recently, a significant OS improvement with abemaciclib. This “carry-over” effect is reflected by sustained separation of the Kaplan-Meier curves during follow-up beyond the active treatment period with CDK4/6 inhibitors and is explained by molecular mechanisms leading to cellular senescence, immunomodulation, and immune-system activation with finite CDK4/6 inhibitor exposure, contributing to control of micrometastatic disease and a reduction in distant recurrences.
The magnitude and duration of the “carry-over” effect depend not only on the drug itself, but also on other factors that may influence outcomes, such as trial design (sample size, “high-risk” criteria, drug duration or dose, discontinuation rate, among others). Therefore, “carry-over” effect is a multistage clinic-molecular “phenomenon” that also depends on treatment adherence.
In clinical practice, “carry-over” is clinically relevant when it is realized through adherence to therapy, including strategies to manage toxicities and sustain adherence. Treatment discontinuation can diminish the potential post-treatment benefit.
Available studies support the use of abemaciclib and ribociclib, which provide iDFS benefit (and abemaciclib has also demonstrated an OS improvement), reinforcing the concept that a finite adjuvant intervention with a CDK4/6 inhibitor translates into a durable impact in a potentially curative setting. The lack of benefit with palbociclib, contrasted with favorable results in some biomarker-defined subgroups, suggests that CDK4/6 inhibitor selectivity is determinant, and use may be considered in specific clinic-molecular profiles.
Evaluating potential biomarkers (e.g., TKa, pRB, MRD by ctDNA, etc.) will enable identification of EBC populations at risk for early relapses and help to define treatment intensification or de-escalation strategies, optimizing benefit while reducing toxicity. Emerging therapies such as adjuvant oral SERDs (giredestrant) broaden the debate: intensification (CDK4/6 inhibitor + ET) will likely be used in high-risk patients, while replacement (de-escalation) of ET with SERDs may be used in selected subgroups. “Carry-over” may be a key criterion to guide the best treatment strategy. Which patients should we de-escalate first? This critical question invites researchers and clinicians to translate the insights from “carry-over” effect into developing new trial concepts, ultimately aiming to refine patient selection and enhance therapeutic outcomes.
The implications of “carry-over” extend beyond clinical efficacy; “financial toxicity” and health-system sustainability are also relevant, especially for innovative, high-cost treatments administered for years. These positions “carry-over” effect as a valid argument to justify (or question) treatments in the context of health policy.
Author Contributions
All authors have contributed equally for the manuscript elaboration.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Δ | Absolute difference |
| AEs | Adverse events |
| ATP | Adenosine triphosphate |
| ATRX | Alpha-thalassemia mental retardation X-linked |
| BID | Twice per day |
| CCNE1 | Cyclin E1 amplification |
| CDK 4/6 | Cyclin-dependent kinase 4/6 |
| CPS-EG | Combining Clinical/Pathological Stage and Estrogen Receptor Status/Grade |
| ctDNA | Circulating tumor DNA |
| DRFS | Distant recurrence-free survival |
| EBC | Early breast cancer |
| ER | Estrogen receptor |
| erbB2 | HER2/neu |
| ET | Endocrine therapy |
| GR50 | Growth rate 50 inhibition |
| GSK3β | Glycogen Synthase Kinase 3 Beta |
| HR (+) | Hormone receptor-positive |
| IC50 | Half-maximal Inhibitory Concentration |
| iDFS | Invasive disease-free survival |
| LBC | Lobular breast cancer |
| MCL-1 | Myeloid Cell Leukemia-1 |
| MDSCs | Myeloid-derived suppressor cells |
| MRD | Minimal residual disease |
| nM | Nanomolar |
| NICE | National Institute for Health and Care Excellence |
| NSAI | Nonsteroidal aromatase inhibitor |
| OS | Overall survival |
| PgR | Progesterone receptor |
| PK | Pharmacokinetics |
| PPIs | Proton pump inhibitors |
| pRB | Retinoblastoma Protein |
| P-TEFb | Positive Transcription Elongation Factor b |
| QTc | Corrected Q-T interval |
| SABCS | San Antonio Breast Cancer Symposium |
| SASP | Senescence-Associated Secretory Phenotype |
| SERD | Selective Estrogen Receptor Degrader |
| TKa | Thymidine Kinase 1 |
| Tregs | Regulatory T cells |
| ypN+ | Positive node involvement at surgery |
References
- Fasching PA, Kreipe H, Del Mastro L, et al. Identification of Patients with Early HR+ HER2− Breast Cancer at High Risk of Recurrence. Geburtshilfe Frauenheilkd. 2024 Feb 8;84(2):164–184. [CrossRef]
- Varzaru VB, Popescu R, Vlad DC, et al. Predictors of Recurrence and Overall Survival in Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy and Surgery: A Comprehensive Statistical Analysis. Cancers 2025, 17(6), 924. [CrossRef]
- Łukasiewicz S, Czeczelewski M, Forma A, et al. Breast Cancer—Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies—An Updated Review. Cancers (Basel). 2021 Aug 25;13(17):4287. [CrossRef]
- Gil-Gil M, Alba E, Gavilá J, et al. The role of CDK4/6 inhibitors in early breast cancer. Breast. 2021 May 25;58:160–169. [CrossRef]
- Gnant M, Singer CF, Rinnerthaler G, et al. Position paper on CDK4/6 inhibitors in early breast cancer. memo 16, 135–144 (2023). [CrossRef]
- Ge R. Escalating and de-escalating treatments in HR+HER2− early-stage breast cancer. Transl Breast Cancer Res. 2022 Apr 30;3:11. [CrossRef]
- Geyer Ch, Bardia A, Harbeck N, et al. lidERA Breast Cancer (BC): Phase III adjuvant study of giredestrant vs. physician’s choice of endocrine therapy (PCET) in patients (pts) with estrogen receptor-positive, HER2-negative early BC (ER+, HER2– eBC). J Clin Oncol 41, TPS616(2023). [CrossRef]
- Gnant M, Dueck AC, Frantal S, et al. Adjuvant Palbociclib for Early Breast Cancer: The PALLAS Trial Results (ABCSG-42/AFT-05/BIG-14-03). J Clin Oncol 40, 282-293(2022). [CrossRef]
- Mayer EL, Hlauschek D, Gnant M, et al. Palbociclib with adjuvant endocrine therapy in early breast cancer: 5-year follow-up analysis of the global multicenter, open-label, randomized phase III PALLAS trial (ABCSG-42/AFT-05/PrE0109/BIG-14-13). Annals of Oncology. 2025. [CrossRef]
- DeMichele A, Dueck AC, Hlauschek D, et al. Outcomes in stage IIA versus stage IIB/III in the PALLAS trial [ABCSG-42/AFT-05/PrE0109/BIG-14-13]). Breast Cancer Res. 2025 Jan 23;27:12. [CrossRef]
- Agostinetto E, Pfeiler G, Hlauschek D, et al. Drug-drug interactions between palbociclib and proton pump inhibitors in early breast cancer: an exploratory analysis of PALLAS (ABCSG-42/AFT-05/BIG-14-13/PrE0109). ESMO Open. 2025 Jan 3;10(1):104096. [CrossRef]
- Loibl S, Marmé F, Martin M, et al. Palbociclib for Residual High-Risk Invasive HR-Positive and HER2-Negative Early Breast Cancer—The Penelope-B Trial. J Clin Oncol 39, 1518-1530(2021). [CrossRef]
- Loibl S, Martin M, Bonnefoi H, et al. Final survival results from the PENELOPE-B trial investigating palbociclib versus placebo for patients with high-risk HR+/HER2− breast cancer and residual disease after neoadjuvant chemotherapy. Annals of Oncology. 2025. [CrossRef]
- Loibl S, Denkert C, Liu Y, et al. Abstract PD17-05: Development and Validation of a Composite Biomarker Predictive of Palbociclib + Endocrine Treatment Benefit in Early Breast Cancer: PENELOPE-B and PALLAS Trials. Cancer Res (2023) 83 (5_Supplement): PD17-05. [CrossRef]
- Johnston SRD, Toi M, O’Shaughnessy J, et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. 2022 Dec 6;24(1):77–90. [CrossRef]
- Hamilton EP, Kim JH, Eigeliene N, et al. Efficacy and safety results by age in monarchE: Adjuvant abemaciclib combined with endocrine therapy (ET) in patients with HR+, HER2-, node-positive, high-risk early breast cancer (EBC). J Clin Oncol 41, 501(2023). [CrossRef]
- Johnston S, Martin M, O’Shaughnessy J, et al. Overall survival with abemaciclib in early breast cancer. Annals of Oncology. 2025. [CrossRef]
- Verzenio® (Abemaciclib) tablets, for oral use. Food and Drug Administration (FDA) label. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-early-breast-cancer-indication-abemaciclib-endocrine-therapy.
- Verzenios. Abemaciclib. European Medicines Agency (EMA) Medicine overview. https://www.ema.europa.eu/en/medicines/human/EPAR/verzenios.
- Slamon D, Lipatov O, Nowecki Z, et al. Ribociclib plus Endocrine Therapy in Early Breast Cancer. N Engl J Med 2024;390:1080-1091. [CrossRef]
- Fasching PA, Stroyakovskiy D, Yardley DA, et al. Ribociclib Plus Endocrine Therapy in Hormone Receptor-Positive/ERBB2-Negative Early Breast Cancer: 4-Year Outcomes from the NATALEE Randomized Clinical Trial. JAMA Oncol. 2025 Nov 1;11(11):1364-1372. [CrossRef]
- Crown J, Stroyakovskii D, Yardley DA, et al. Adjuvant ribociclib plus nonsteroidal aromatase inhibitor therapy in patients with HR-positive/HER2-negative early breast cancer: 5-year follow-up of NATALEE efficacy outcomes and updated overall survival. ESMO Open. 2025 Oct 17;10(11):105858. [CrossRef]
- https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancerhematologic-malignancies-approval-notifications.
- Tripathy D, Bardia A, Sellers WR. Ribociclib (LEE011): mechanism of action and clinical impact of this selective cyclin-dependent kinase 4/6 inhibitor in various solid tumors. Clin Cancer Res. 2017;23(13):3251–62. [CrossRef]
- Asghar U, Witkiewicz AK, Turner NC, Knudsen ES. The History and Future of Targeting Cyclin-Dependent Kinases in Cancer Therapy. Nat Rev Drug Discovery (2015) 14(2):130–46. [CrossRef]
- Gelbert LM, Cai SF, Lin X, et al. Preclinical Characterization of the CDK4/6 Inhibitor LY2835219: in-Vivo Cell Cycle-Dependent/Independent Anti-Tumor Activities Alone/in Combination with Gemcitabine. Invest New Drugs (2014) 32(5):825–37. [CrossRef]
- Klapp V, Buqué A, Bloy N, et al. Cellular senescence in the response of HR+ breast cancer to radiotherapy and CDK4/6 inhibitors. J Transl Med. 2023 Feb 10;21(1):110. [CrossRef]
- Wells CI, Vasta JD, Corona CR, et al. Quantifying CDK Inhibitor Selectivity in Live Cells. Nat Commun (2020) 11(1):2743. [CrossRef]
- Kovatcheva M, Liao W, Klein ME, et al. ATRX is a regulator of therapy induced senescence in human cells. Nat Commun, 2017 Aug 30;8(1):386. [CrossRef]
- Crozier L, Foy R, Mourey BL, et al. CDK4/6 inhibitors induce replication stress to cause long-term cell cycle withdrawal. EMBO J. 2022 Jan 17;41(6):e108599. [CrossRef]
- Martorana F, Vita Sanó M, Valerio MR, et al. Abemaciclib pharmacology and interactions in the treatment of HR+/HER2− breast cancer: a critical review. Ther Adv Drug Saf. 2024 Apr 25;15. [CrossRef]
- Cousins EM, Goldfarb D, Yan F, et al. Competitive Kinase Enrichment Proteomics Reveals that Abemaciclib Inhibits GSK3β and Activates WNT Signaling. Mol Cancer Res. 2017 Nov 13;16(2):333–344. [CrossRef]
- Zhang Y, Chen B, Zhang R, et al. Emerging immunomodulatory effects of CDK4/6 inhibitors in breast cancer therapy: A comprehensive review. Tumor Discovery 2025, 4(3), 16–31. [CrossRef]
- Zhang Sh, Xu Q, Sun W, et al. Immunomodulatory effects of CDK4/6 inhibitors. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer. 2023. [CrossRef]
- George MA, Qureshi S, Omene C, et al. Clinical and Pharmacologic Differences of CDK4/6 Inhibitors in Breast Cancer. Front. Oncol, 2021. [CrossRef]
- Wang B, Varela-Eirin M, Brandenburg SM, et al. Pharmacological CDK4/6 inhibition reveals a p53-dependent senescent state with restricted toxicity. EMBO J 41, EMBJ2021108946 (2022). [CrossRef]
- Niraula S. Adjuvant CDK4/6 inhibitors in breast cancer: Interpreting trial design, evidence, and uncertainty. Cancer Treatment Reviews. 2025. [CrossRef]
- Flandre P, O’Quigley J. Comparing Kaplan-Meier Curves with Delayed Treatment Effects: Applications in Immunotherapy Trials. Journal of the Royal Statistical Society Series C: Applied Statistics, Volume 68, Issue 4, August 2019, 915–939. [CrossRef]
- Turner NC, Liu Y, Zhu Z, et al. Cyclin E1 Expression and Palbociclib Efficacy in Previously Treated Hormone Receptor–Positive Metastatic Breast Cancer. J Clin Oncol. 2019 Feb 26;37(14):1169–1178. [CrossRef]
- Sabit H, Attia MG, Mohamed N, et al. Beyond traditional biopsies: the emerging role of ctDNA and MRD on breast cancer diagnosis and treatment. Discov Oncol. 2025 Mar 6;16:271. [CrossRef]
- Panet F, Papakonstantinou A, Borrell M, et al. Use of ctDNA in early breast cancer: analytical validity and clinical potential. NPJ Breast Cancer. 2024 Jun 19;10(1):50. [CrossRef]
- Hussain M, Brezden-Masley Ch, Henning JW. Clinician’s guide: expert insights on the use of CDK4/6 inhibitors in patients with early breast cancer. Therapeutic Advances in Medical Oncology. March 20, 2025. [CrossRef]
- Abemaciclib with endocrine therapy for adjuvant treatment of hormone receptor-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence. TA810. National Institute for Health and Care Excellence (NICE). TA810. 20 July 2022. https://www.nice.org.uk/guidance/ta810.
- Ribociclib with an aromatase inhibitor for adjuvant treatment of hormone receptor-positive HER2-negative early breast cancer at high risk of recurrence. TA1086. National Institute for Health and Care Excellence (NICE). 08 August 2025. https://www.nice.org.uk/guidance/TA1086.
- https://www.aacr.org/about-the-aacr/newsroom/news-releases/novel-endocrine therapy-giredestrant-improves-disease-free-survival-over-standard-of-care-for-patients-with-early-stage-breast-cancer-in-phase-iii-lidera-trial/.
Figure 1.
“Carry over” effect on iDFS of monarchE trial.
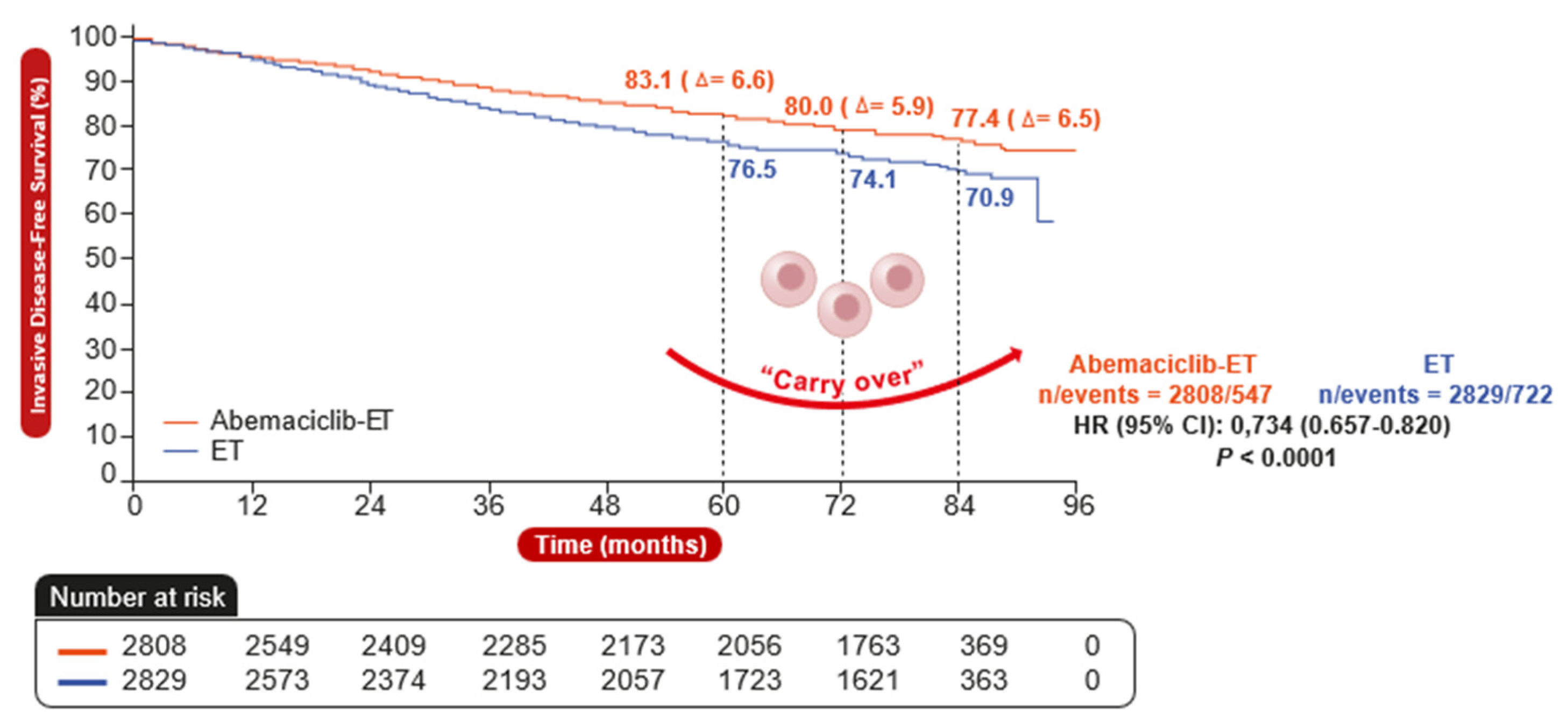
Figure 2.
“Carry over” effect on iDFS of NATALEE trial.
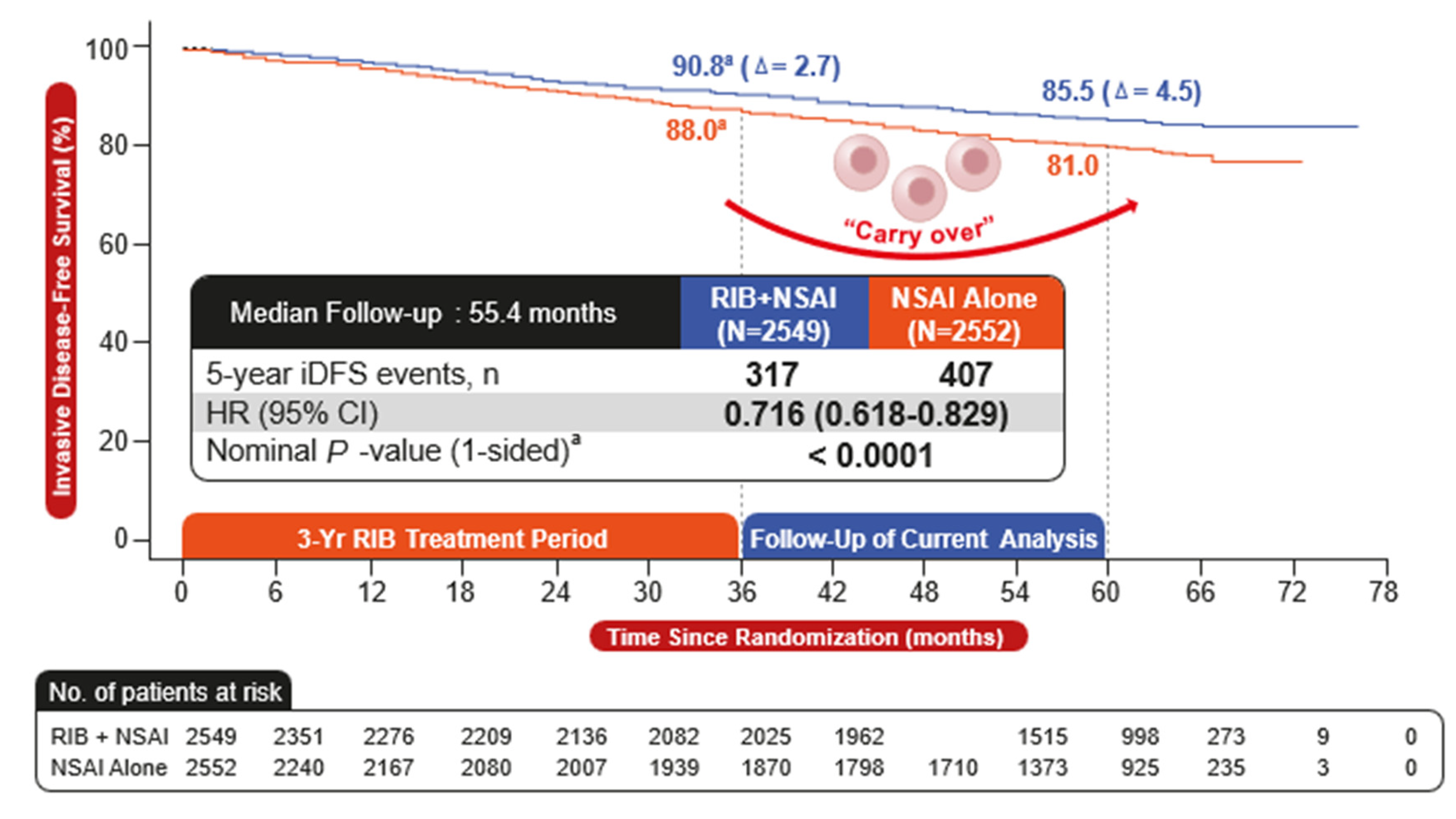
Figure 3.
CDK4/6 inhibitors and senescence. Adapted by: ME Klein, et al. Cancer Cell. 2018 Jul 9;34(1):9-20.
Figure 3.
CDK4/6 inhibitors and senescence. Adapted by: ME Klein, et al. Cancer Cell. 2018 Jul 9;34(1):9-20.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



