Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Objective: To evaluate the feasibility, usability, and preliminary efficacy of the CUE1 wearable vibrotactile device in real-world, clinic-based older adults with Parkinson’s disease (PD). Methods: A single-arm feasibility study was conducted in 20 over 60-year-old participants with PD attending a routine movement disorders clinic. Par-ticipants used the CUE1 device daily for four weeks. Usability and acceptability were assessed through participant diaries. Motor outcomes were evaluated at two timepoint, baseline and after 4 weeks using MDS-UPDRS III and Timed Up and Go (TUG). Results: Sixteen participants completed the study. The CUE1 was well tolerated with minimal adverse events. Statistically significant improvements were observed in MDS-UPDRS III scores (mean change −4.5, p = 0.04) and TUG times (mean change −2.1s, p = 0.009). Im-provements were most pronounced in participants with greater baseline motor im-pairment. Conclusions: The CUE1 device demonstrated good feasibility, high usability, and promising motor improvements in older, real-world patients with PD who are often underrepresented in clinical trials. These findings support further evaluation of the CUE1 in larger, randomized controlled studies to confirm its clinical benefits and real-world applicability.
Keywords:
Parkinson’s disease
; wearable device
; vibrotactile stimulation
; older adults
; MDS-UPDRS
; Timed Up and Go
1. Introduction
Parkinson’s disease (PD) is defined by bradykinesia, rest tremor, and rigidity, often accompanied by postural and gait abnormalities [1]. It predominantly affects older adults, with a prevalence exceeding 1.9% in individuals aged over 80 years [2]. Despite this, older adults are frequently excluded from clinical trials, resulting in research cohorts that may not reflect the complexity of real-world patients [3]. This limits the generalisability of trial outcomes and complicates clinical decision-making for professionals and patients alike [4].
Pharmacological therapy remains the cornerstone of motor symptom management in PD but is not without limitations. Older adults with PD are more susceptible to adverse drug reactions (ADRs), which contribute to approximately 6.5% of all hospital admissions [5]. Moreover, pharmacological response diminishes over time, and many patients experience motor fluctuations, dyskinesias, or neuropsychiatric complications despite optimal medical management [6].
In advanced PD, device-aided therapies such as deep brain stimulation or continuous subcutaneous apomorphine infusion may offer symptomatic benefit. However, these interventions are often contraindicated in older or comorbid patients due to safety and suitability concerns [7]. Consequently, a substantial proportion of individuals with troublesome motor symptoms lack safe, non-invasive therapeutic alternatives.
The CUE1 is a wearable, non-invasive vibrotactile device designed to improve motor symptoms in ambulatory people with PD. It is the first commercially available device combining pulsed cueing with vibration-based stimulation. Interest in vibrotactile therapy for PD dates back to the 19th century when J.M. Charcot observed symptomatic improvement using a vibrating chair [8] and more recent studies have shown an improvement in motor function following periods of constant vibrotactile stimulation at the wrist in both healthy adults and patients with Parkinson’s disease [9].
Cueing is an established method for improving gait in PD. Cues are defined as discrete targets or references that serve to facilitate and enhance motor execution [10]. Ginis et al proposed three mechanisms underlying the effects of cueing: first, facilitating focused attention on gait (executive role); second, reducing variability and improving spatio-temporal gait parameters (stabilizing role); and third, enabling the coupling of postural control with step initiation (preparatory role) [11]. Preliminary studies have demonstrated that the CUE1 is well tolerated and may improve motor function [12]. However, no prior studies have specifically examined its use in older, real-world patients—a group frequently underrepresented in research but highly relevant to everyday clinical practice. The present study therefore aimed to assess the feasibility, usability, and preliminary efficacy of the CUE1 device in this population.
2. Materials and Methods
Study design
A single arm feasibility study was conducted to assess the acceptability and useability of the CUE1 device and the feasibility of collecting standardised motor outcomes over a four-week period in older adults with PD. The target sample size was 20–25 participants.
Participants
Eligible participants were over the age of 60 with a clinical diagnosis of PD according to the UK Brain bank criteria. Exclusion criteria included:
1) significant co-existing neurological, disorder (e.g. disabling stroke, multiple sclerosis, dementia, motor neurone disease),
2) atypical parkinsonian disorder diagnosis (e.g. multiple systems atrophy, progressive supranuclear palsy or cortical basal degeneration syndrome),
3) co-existing physical impairment or disability causing significant mobility impairment (severe lower limb osteoarthritis)
4) trauma or pain to the sternum,
5) implanted electrical devices (e.g. pacemaker, DBS, TENS machine etc,
6) lacking capacity to consent to the study,
7) adhesive allergy,
8) enrolment in other interventional trials.
Twenty participants were recruited from the movement disorder clinics. Demographic and clinical characteristics including disease duration, disease severity, motor fluctuation status co-morbidities and medication regime were collected.
Intervention
The CUE1 device is a 40 mm diameter, 12 mm thick, disc-shaped non-invasive wearable that delivers 170 Hz vibrotactile stimulation with 800 ms on/off pulsed intervals. It is applied to the sternum using a medical adhesive and worn during waking hours.
Participants received a home visit from a specialist neuro-Physiotherapist who provided full training on the use of the CUE1. Baseline assessments were completed one hour after the last levodopa dose to reduce the risk of motor fluctuations impacting on assessment outcomes. Assessment was then repeated 30 minutes following device fitting. Participants were instructed to wear the device daily for four weeks, documenting usability and tolerance in a diary. At week 4, the same assessor repeated all assessments at the same time of day.
Outcome measures
Primary
Usability and acceptability, assessed via participant diaries (comfort, independence of use, adverse events, willingness to continue).
Secondary outcomes:
Motor performance using the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale part III (MDS-UPDRS III) and the Timed Up and Go (TUG) test, recorded at baseline and four weeks.
Statistical analysis
Descriptive statistics were used to summarise baseline characteristics and feasibility outcomes. Paired t-tests compared baseline and post-intervention scores. Subgroup analyses explored effects of baseline severity (MDS-UPDRS III <25 vs. ≥25), disease duration, and presence of motor fluctuations on treatment response. A principal components analysis (PCA) was performed on the multivariate MDS-UPDRS III data to identify clusters of items that accounted for the greatest variance across participants. The non-centred PCA was conducted in MATLAB (version 9.14.0.2239454, R2023a) using the built-in pca function, based on the difference in MDS-UPDRS III item scores between baseline and follow-up assessments.
Ethics
The study was approved by the local Ethics Committee and NHS Health Research Authority (Ref: 23/EE/0247). Capacity and capability were confirmed by the local hospital (Ref: A096551). The study was registered at clinicaltrials.gov (NCT06430151). All participants provided written informed consent.
3. Results
Participant Characteristics
Twenty participants were enrolled; two were excluded due to vascular parkinsonism and two withdrew. Sixteen participants (mean age 80.5 years; 60% male) completed the study. Median Hoehn and Yahr stage was 2, and mean disease duration was 10 years. Average daily levodopa dose was 500 mg. Eighteen percent reported freezing of gait, 42% had motor fluctuations, and 42% had a history of falls (Table 1).
Useability and acceptability
All 16 participants completed daily diaries. Most (81%) completed them fully, and median daily device use was 7–9 hours. The median comfort score was 5/5, with minimal skin irritation (0.6% of days). Device malfunction occurred in 18.75% of cases, consistent with pre-commercial prototypes (Table 2).
The battery life proved to be satisfactory with a lifespan of more than 10 hours. Overall, 92% of participants indicated willingness to continue using the device after the study, and 92% were able to operate it independently. However, only 54% could independently apply the adhesive patch, often requiring caregiver assistance. No serious adverse events were reported.
Motor scores

Table 3.
Summary of UPDRS, TUG and their 4-week changes.
| UPDRS III (score) | |||||
| Groups | n | Mean (SD) | Median (Min, Max) | p-value | |
| Overall | |||||
| Baseline | 16 | 38.5 (14.8) | 35.5 (9, 61) | ||
| Follow-up | 16 | 34 (11) | 36 (14, 52) | ||
| Change | 16 | -4.5 (8) | -5.5 (-18, 11) | 0.040 | |
| UPDRS | |||||
| Baseline | 1 | 9 | 9 | ||
| <25 | Follow-up | 1 | 14 | 14 | |
| Change | 1 | 5 | 5 | NA | |
| Baseline | 15 | 40.5 (12.9) | 38 (25, 61) | ||
| >25 | Follow-up | 15 | 35.3 (9.9) | 36 (18, 52) | |
| Change | 15 | -5.2 (7.8) | -7 (-18, 11) | 0.024 | |
| Age | |||||
| Baseline | 8 | 34.2 (15.3) | 31 (9, 56) | ||
| <80 | Follow-up | 8 | 30.6 (12) | 30 (14, 52) | |
| Change | 8 | -3.6 (8.3) | -6.5 (-12, 11) | 0.083 | |
| Baseline | 8 | 42.8 (13.9) | 41.5 (26, 61) | ||
| >80 | Follow-up | 8 | 37.4 (9.4) | 40.5 (18, 47) | |
| Change | 8 | -5.4 (8.1) | -5 (-18, 6) | 0.077 | |
| Dyskinesia/Dystonia/Freezing of gait/Fall | |||||
| Baseline | 8 | 40.1 (13.1) | 39 (26, 61) | ||
| No | Follow-up | 8 | 34.1 (10.6) | 36 (18, 47) | |
| Change | 8 | -6 (7.8) |
-7.5 (-18, 6) | 0.031 | |
| Baseline | 8 | 36.9 (17) | 35 (9, 58) | ||
| Yes | Follow-up | 8 | 33.9 (12.1) | 36 (14, 52) | |
| Change | 8 | -3.0 (8.4) | -3 (-14, 11) | 0.157 | |
| Length of diagnosis (years) | |||||
| Baseline | 5 | 39.6 (11.8) | 33 (30, 58) | ||
| <7 | Follow-up | 5 | 32.0 (9.9) | 33 (21, 44) | |
| Change | 5 | -7.6 (7.9) | -9 (-14, 11) | 0.098 |
|
| Baseline | 11 | 38 (16.4) | 38 (9, 61) | ||
| >7 | Follow-up | 11 | 34.9 (11.8) | 36 (14, 52) | |
| Change | 11 | -3.1 (8) | -3 (-18, 11) | 0.016 | |
| TUG (seconds) | |||||
| Groups | n | Mean (SD) |
Median (Min, Max) | p-value | |
| Overall | |||||
| Baseline | 15 | 13.8 (4.3) | 12.6 (7.5, 20.2) | ||
| Follow-up | 15 | 11.7 (3.1) | 11.8 (6.7, 16.4) | ||
| Change | 15 | -2.1 (2.2) | -1.7 (-7.8, 0.2) | 0.009 | |
| UPDRS | |||||
| Baseline | 1 | 7.5 | 7.5 | ||
| <25 | Follow-up | 1 | 7.4 | 7.4 | |
| Change | 1 | -0.1 | -0.1 | NA | |
| Baseline | 12 | 13.8 (4.2) | 12.2 (9.7, 20.2) | ||
| >25 | Follow-up | 12 | 11.6 | 11.5 (6.7, 16.4) | |
| Change | 12 | -2.2 | -1.6 (-7.8, 0.2) | 0.009 | |
| Age | |||||
| Baseline | 6 | 12.2 (4.6) | 10 (7.5, 19) | ||
| <80 | Follow-up | 6 | 9.7 (3) | 8.9 (6.7, 15) | |
| Change | 6 | -2.5 (2.8) | -1.6 (-7.8, -0.1) | 0.083 | |
| Baseline | 7 | 14.3 (4.3) | |||
| >80 | Follow-up | 7 | 12.6 (2.5) | ||
| Change | 7 | -1.7 (2.1) | |||
| Dyskinesia/Dystonia/Freezing of gait/Fall | |||||
| Baseline | 8 | 13.5 (4.4) | 11.4 (9.9, 20.2) | ||
| No | Follow-up | 8 | 11.7 (2.9) | 11.1 (8.7, 16.4) | |
| Change | 8 | -1.8 (1.9) | -1.1 (-4.4, 0.2) | 0.031 | |
| Baseline | 5 | 12.9 (4.8) | 11.8 (7.5, 19) | ||
| Yes | Follow-up | 5 | 10.4 (3.4) | 11.2 (6.7, 15) | |
| Change | 5 | -2.5 (3.2) | -1.7 (-7.8, 0.1) | 0.157 | |
| Length of diagnosis (years) | |||||
| Baseline | 4 | 12.3 (4.4) | 10.2 (9.9, 19) | ||
| <7 | Follow-up | 4 | 9.9 (1.1) | 9.8 (8.7, 11.2) | |
| Change | 4 | -2.4 (3.6) | -1.1 (-7.8, 0.1) | 0.267 | |
| Baseline | 9 | 13.7 (4.5) | 12.6 (7.5, 20.2) | ||
| >7 | Follow-up | 9 | 11.9 (3.5) | 11.9 (6.7, 16.4) | |
| Change | 9 | -1.8 (1.8) | -1.7 (-4.4, 0.2) | 0.016 | |
Results demonstrated a statistically significant overall improvement in both motor outcomes following four weeks of CUE1 use. The mean MDS-UPDRS III score improved from 38.5 at baseline to 34.0 post-intervention (mean change −4.5, p = 0.04), while the mean Timed Up and Go (TUG) time improved from 13.8 seconds to 11.8 seconds (mean change −2.1 s, p = 0.009).
Post-hoc subgroup analyses revealed that participants with greater baseline motor impairment (MDS-UPDRS III ≥25) exhibited a larger improvement in MDS-UPDR III scores (42.8 to 37.4; mean change −5.2), and the improvement in TUG time remained statistically significant within this subgroup.
When adjusting for age, disease duration, and presence of motor fluctuations, no significant between-group differences were observed in MDS-UPDRS III outcomes. However, participants without motor fluctuations demonstrated a statistically significant improvement in TUG time (13.5 s to 11.7 s; mean change −1.8 s, p = 0.031). Similarly, participants with a disease duration greater than seven years showed significant improvement in TUG (13.7 s to 11.9 s; mean change −1.8 s, p = 0.016).
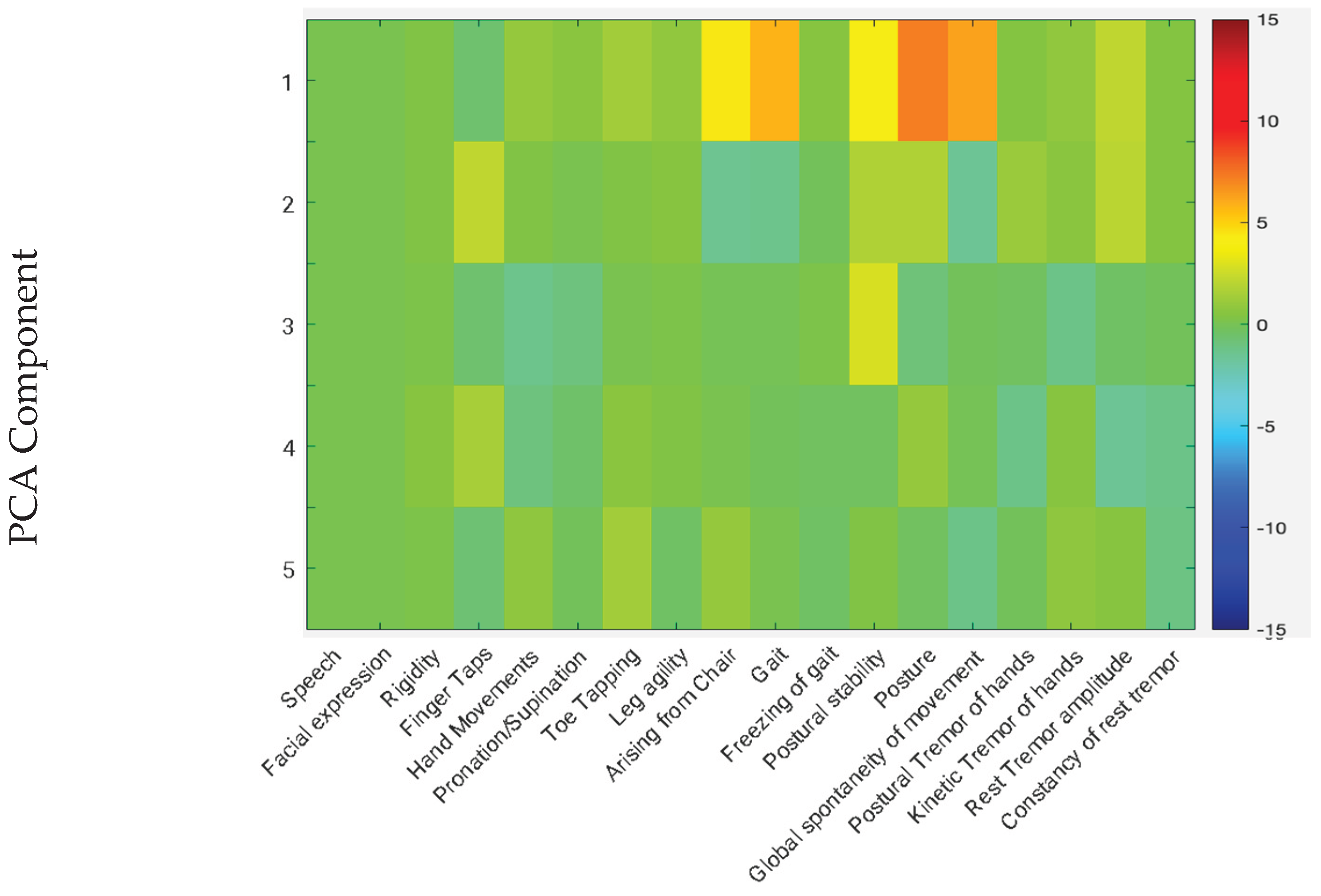
Principal component analysis (PCA) was used to explore the dimensional structure of the MDS-UPDRS III changes. The first five components explained approximately 90% (92.9%) of the total variance, with the first component alone accounting for 69.9%. The primary contributors to this variance were reductions in scores for gait, posture, and global spontaneity of movement, indicating these domains were most consistently responsive to CUE1 use.
Figure 1.
PCA component analysis.
4. Discussion
This study provides preliminary real-world evidence that the CUE1 vibrotactile cueing device is a feasible, safe, and acceptable intervention for older adults with PD. The study was conducted in a clinically representative cohort that is typically underrepresented in research due to advanced age and multimorbidity. Notably, this population is also the group most likely to benefit from non-invasive therapeutic options, as they are often ineligible for device-aided treatments such as deep brain stimulation or continuous infusion therapies [13]. Despite this, few studies have examined the feasibility or acceptability of such interventions in this cohort. The high recruitment and completion rates, coupled with minimal adverse events, support the practicality and tolerability of CUE1 use in real-world clinical settings.
Significant improvements were observed in both MDS-UPDRS III and TUG scores after four weeks of device use, consistent with previous reports of motor benefits from vibrotactile cueing interventions [14]. The median overall improvement in MDS-UPDRS III was −5.5 points, increasing to −7 points among participants with baseline scores >25. Given that the minimally clinically important difference (MCID) for MDS-UPDRS III is −3.25 points [15], these changes suggest a clinically meaningful benefit, particularly in individuals with more advanced motor impairment.
However, when adjusted for age, these improvements were no longer statistically significant, suggesting that advancing age may attenuate responsiveness to cueing-based interventions. This may reflect age-related changes in sensory integration, proprioception, or motor adaptability, which are further impacted in PD. Further studies with larger, stratified samples are needed to confirm whether this represents a true age-dependent effect or a limitation of statistical power in a small cohort.
A statistically significant improvement was also observed in TUG performance, with mean times improving from 13.8 s at baseline to 11.7 s at follow-up. This exceeds both the recently defined MCID (−1.07 s to −1.14 s) and the threshold for substantial clinical benefit (−2.04 s) for single-task TUG [16]. Since a TUG time >13.5 s is associated with increased fall risk [17], the improvement observed here warrants further investigation into potential reductions in fall frequency in future prospective studies.
Principal component analysis indicated that the majority of variance in improvement was driven by changes in gait, posture, and global spontaneity of movement, symptoms that typically respond less well to levodopa therapy [18]. This supports the mechanistic rationale for vibrotactile cueing as a complementary, non-pharmacological strategy targeting motor aspects of PD less responsive to dopaminergic medication.
Limitations
This study has several limitations. The single-arm design without a control group limits the ability to attribute improvements directly to the intervention, and placebo effects cannot be excluded. The small sample size and short four-week follow-up reduce statistical power and prevent evaluation of long-term adherence or sustained benefit. All participants were recruited from a single centre, which may limit generalisability. Although exploratory analyses adjusted for age and disease duration, the study was not powered to fully examine these effects. Finally, usability data were self-reported and may be influenced by recall bias. Despite these limitations, the study provides important real-world evidence supporting the feasibility and tolerability of CUE1 use in older adults with PD. Adequately powered, randomised controlled studies are required with the CUE1 [19] and a large, randomised control trial is planned for 2026.
5. Conclusions
Despite these limitations, this study provides important real-world evidence demonstrating that the CUE1 device is feasible, safe, and well tolerated in older adults with PD. Although improvements attenuated after adjustment for age, the observed trends and strong user acceptability support further evaluation in a larger, randomised controlled trial to confirm efficacy, explore age-related responsiveness, and assess long-term clinical benefits.
Author Contributions
Authors: Ledia Agley, James Kilner, Mark Hensley and Alistair Mackett. Conceptualization: Alistair Mackett. Formal analysis Mark Hensley. Funding acquisition: Alistair Mackett. Investigation: Ledia Agley. Methodology: Alistair Mackett, Ledia Agley. Project administration: Alistair Mackett. Supervision: Alistair Mackett. Writing original draft: Alistair Mackett, Ledia Agley. Writing-review & editing: Ledia Agley, James Kilner, Mark Hensley
Funding
This work was funded by Charco Neurotech Ltd, Cambridge, UK. The APC was funded by Charco Neurotech Ltd, Cambridge, UK
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Cambridge East Ethics Committees and the NHS Health Research Authority (reference: 23/EE/0247). Capacity and capability to conduct this study at Cambridge University Hospitals NHS Foundation Trust was confirmed (reference: A096551). The study was registered at clinicaltrials.gov (reference: NCT06430151)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
AM, JK and MH have all worked in consultancy roles for the device manufacturer. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| PD | Parkinson’s Disease |
| MDS-UPDRS | Movement Disorder Society-Unified Parkinsons Disease Rating Scale |
| TUG | Timed-up-and-go |
References
- Tolosa, E. G. Challenges in the diagnosis of Parkinson's disease. The Lancet Neurology 2021, 20(5), 385–397. [Google Scholar] [CrossRef] [PubMed]
- Pringsheim, T; Jette, N; Frolkis, A; Steeves, TD. The prevalence of Parkinson's disease: a systematic review and meta-analysis. Movement disorders 2014, 29(13), 1583–90. [Google Scholar] [CrossRef] [PubMed]
- Thake, M.; Lowry, A. A systematic review of trends in the selective exclusion of older participant from randomised clinical trials. Arch. Gerontol. Geriatr. 2017, 72, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Crome, P.; Lally, F.; Cherubini, A.; Oristrell, J.; Beswick, A. D.; Clarfield, A. M.; Mills, G. Exclusion of older people from clinical trials: professional views from nine European countries participating in the PREDICT study. Drugs & aging 2011, 28(8), 667–677. [Google Scholar]
- Pirmohamed, M.; James, S.; Meakin, S.; Green, C.; Scott, A.K.; Walley, T.J.; Farrar, K.; Park, B.K.; Breckenridge, A.M. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Zahoor, I.; Shafi, A.; Haq, E. Pharmacological treatment of Parkinson’s disease; Exon Publications, 2018; pp. 129–144. [Google Scholar]
- Antonini, A.; Stoessl, A.J.; Kleinman, L.S.; Skalicky, A.M.; Marshall, T.S.; Sail, K.R.; Onuk, K.; Odin, P.L.A. Developing consensus among movement disorder specialists on clinical indicators for identification and management of advanced Parkinson’s disease: a multi-country Delphi-panel approach. Curr. Med Res. Opin. 2018, 34, 2063–2073. [Google Scholar] [CrossRef] [PubMed]
- Kapur, S. S. Vibration therapy for Parkinson's disease: Charcot's studies revisited. Journal of Parkinson's disease 2012, 2(1), 23–27. [Google Scholar] [CrossRef] [PubMed]
- Macerollo, A.; Palmer, C.; Foltynie, T.; Korlipara, P.; Limousin, P.; Edwards, M.; Kilner, J.M. High-frequency peripheral vibration decreases completion time on a number of motor tasks. Eur. J. Neurosci. 2018, 48, 1789–1802. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, C.; Putzolu, M.; Mezzarobba, S.; Cecchella, M.; Innocenti, T.; Bonassi, G.; Botta, A.; Lagravinese, G.; Avanzino, L.; Pelosin, E. One cue does not fit all: A systematic review with meta-analysis of the effectiveness of cueing on freezing of gait in Parkinson’s disease. Neurosci. Biobehav. Rev. 2023, 150, 105189. [Google Scholar] [CrossRef] [PubMed]
- Ginis, P.; Nackaerts, E.; Nieuwboer, A.; Heremans, E. Cueing for people with Parkinson's disease with freezing of gait: A narrative review of the state-of-the-art and novel perspectives. Ann. Phys. Rehabilitation Med. 2018, 61, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Azoidou, V.; Rowsell, K.; Camboe, E.; Dey, K.C.; Zirra, A.; Quah, C.; Boyle, T.; Gallagher, D.; Noyce, A.J.; Simonet, C. A pilot interventional study on feasibility and effectiveness of the CUE1 device in Parkinson's disease. Park. Relat. Disord. 2025, 133, 107349. [Google Scholar] [CrossRef] [PubMed]
- Moes, H.R.; Henriksen, T.; Sławek, J.; Phokaewvarangkul, O.; Buskens, E.; van Laar, T. Tools and criteria to select patients with advanced Parkinson’s disease for device-aided therapies: a narrative review. J. Neural Transm. 2023, 130, 1359–1377. [Google Scholar] [CrossRef] [PubMed]
- Azoidou, V.; Bhadra, E.; Camboe, E.; Dey, K. C.; Zirra, A.; Quah, C.; Simonet, C. A Sternum-Worn, Non-Invasive Vibrotactile Device to Alleviate Symptoms in Parkinson’s: a Multi-Site Double-Blind Randomised Controlled Trial. medRxiv 2025, 2025–07. [Google Scholar]
- Horváth, K.; Aschermann, Z.; Ács, P.; Deli, G.; Janszky, J.; Komoly, S.; Balázs, É.; Takács, K.; Karádi, K.; Kovács, N. Minimal clinically important difference on the Motor Examination part of MDS-UPDRS. Parkinsonism Relat. Disord. 2015, 21, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh, G.; Eissazade, N.; Fereshtehnejad, S.-M.; Sharabiani, P.T.A.; Shati, M.; Mortazavi, S.S.; Habibi, S.A.H.; SalemiJuybari, M.; Mehdizadeh, M. Minimal clinically important difference and substantial clinical benefits for single- and dual-task timed up and go test following motor-cognitive training in Parkinson’s disease. Age and Ageing 2025, 54. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: a systematic review and meta- analysis. BMC Geriatr. 2014, 14, 14–14. [Google Scholar] [CrossRef] [PubMed]
- Curtze, C.; Nutt, J.G.; Carlson-Kuhta, P.; Mancini, M.; Horak, F.B. Levodopa Is a Double-Edged Sword for Balance and Gait in People With Parkinson's Disease. Mov. Disord. 2015, 30, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- de la Fuente-FernánDez, R.; Ruth, T.J.; Sossi, V.; Schulzer, M.; Calne, D.B.; Stoessl, A.J. Expectation and Dopamine Release: Mechanism of the Placebo Effect in Parkinson's Disease. Science 2001, 293, 1164–1166. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Participant demographic and clinical characteristics.
| n (%) | |
| UPRS, n (%) | |
| <25 | 1 (5.3) |
| >=25 | 15 (78.9) |
| Missing | 3 (15.8) |
| Age, n (%) | |
| <80y | 8 (42.1) |
| >80y | 8 (42.1) |
| Missing | 3 (15.8) |
| Dyskinesia/Dystonia/Freezing of gait/Falls | |
| No | 8 (42.1) |
| Yes | 8 (42.1) |
| Missing | 3 (15.8) |
| Length of diagnosis | |
| <7y | 5 (26.3) |
| >7y | 11 (57.9) |
| Missing | 3 (15.8) |
Table 2.
Usability and acceptability outcomes from patient diaries.
| n (%) | |
| Completion rate of diary | |
| Full, n (%) | 13 (81) |
| Partial, n (%) | 3 (19) |
| Median duration of use per day (hours) | 8 |
| Median duration of charge (hours) | 10 |
| Median comfort of device (1-5) | 5 |
| Skin irritation from adhesive (% of affected days) | 0.6 |
| Other side effects (% of affected days) | 0 |
| Device malfunction | |
| Yes n (%) | 3 (19) |
| No n (%) | 13 (81) |
| Continue to use the device | |
| Yes n (%) | 12 (75) |
| No n (%) | 1 (6) |
| Missing n (%) | 3 (19) |
| Able to independently use the device | |
| Yes n (%) | 12 (75) |
| No n (%) | 1 (6) |
| Missing n (%) | 3 (19) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



