Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Previous studies suggested that the COVID-19 pandemic exposed children to an increased risk of greater body weight accumulation; however, the evidence found is limited to examining relatively short periods in children from Asian, European, or North American countries and, in most cases, using cross-sectional designs, while studies with longitudinal designs are scarce. To our knowledge, to date, no study involving Brazilian children has examined temporal trends in body weight during the pandemic period using a longitudinal approach. Objective: To report temporal trends in the weight status of children aged 6 to 11 years prior, during, and post-school closures in response to restrictions imposed by the COVID-19 pandemic, using a six-year school-based cohort design (2020–2025). Method: Weight status was analyzed using the body mass index and diagnostic criteria proposed by IOFT. Initial data collection took place in 2020 (pre-pandemic period), in 2021 and 2022 (pandemic period), and in 2023, 2024, and 2025 (post-pandemic period), after the reopening of schools. Results: The data collected confirmed that restrictions imposed to mitigate the adverse impact of the COVID-19 pandemic, including the full or partial closure of schools, substantially increased children's weight above what would be expected for their gender and age. After two years of the pandemic period, 23% of children identified in the pre-pandemic period with normal body weight migrated to overweight, while 34% of overweight children became obese. Data equivalent to the post-pandemic period showed signs of a reduction in the excess body weight accumulated during the pandemic; however, the prevalence rates of overweight and obesity remained significantly higher than in the pre-pandemic period. Conclusion: The findings suggest that the harmful effects contributing to the greater accumulation of body weight during the COVID-19 pandemic were not reversed spontaneously, even five years after its onset. Therefore, specific actions to prevent, combat, and control overweight and obesity are essential to avoid present and future adverse consequences for children's health.
Keywords:
COVID-19
; pandemic
; health behavior
; cohort studies
; overweight
; obesity
; Brazil
1. Introduction
Global estimates suggest that 93.1 million children aged 5–14 years were living with excess body weight in 2021, with expectations that the prevalence of obesity in this population may double by the end of this decade [1]. In Brazil, the number of young people with excess body weight follows the global trend and has more than tripled over the past five decades. More recent data indicate that, regardless of gender, race/skin color, or social and economic conditions, one in four Brazilian youths presents excess body weight (≈25%) [2]. According to the World Obesity Atlas and the World Health Organization, if more effective interventions are not implemented, by 2030 Brazil’s youth population may rank fifth worldwide among countries with the highest prevalence rates of overweight and obesity [3].
At any stage of the life course, overweight and obesity are not merely issues of excessive body weight gain but rather multifactorial conditions that induce a range of physical and psychoemotional health complications. Moreover, consequences of overweight and obesity that were previously thought to occur only in adulthood are being identified with increasing frequency among youths [4]. In addition to the physical health risks (e.g., hypertension and type 2 diabetes), pediatric overweight and obesity are associated with a greater risk of depressive symptoms, disordered eating and body dissatisfaction, as well as lower self-esteem and health-related quality of life (HRQoL). Children with overweight and obesity are also more likely to experience negative social consequences compared with their peers, such as being exposed to weight-based stigma and victimization across environmental settings (e.g., home, school, and health care) [5].
In this context, following the emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the etiological agent of COVID-19, identified in December 2019, the World Health Organization declared a Public Health Emergency of International Concern, and subsequently SARS-CoV-2 was characterized as a worldwide pandemic. In Brazil, a Public Health Emergency of National Importance was declared in February 2020, followed by the implementation of a series of social and public health measures, including social distancing, home isolation, restricted mobility, and, at times, even lockdowns, as a preventive action to contain the rate of community transmission of the virus. An inevitable consequence of these self-confinement measures was a drastic and sudden change across a broad spectrum of daily life routines. For children, as in many other countries, there was full or partial school closure and the consequent interruption of in-person teaching activities, with teachers providing instruction exclusively or partially through online resources.
According to a UNESCO report, Brazil was considered one of the countries in which schools remained closed for the longest period in response to the COVID-19 pandemic. Data showed that from March 2020 to January 2022, Brazilian primary and secondary schools remained fully closed for an average of 39 weeks. When partial school closures are also considered, this duration increases to 78 weeks. As a point of comparison, during the same period, schools in China and the United States remained fully closed for no more than 12 weeks and partially closed for 27 and 58 weeks, respectively [6]. Although Brazilian health authorities declared the end of the Public Health Emergency of National Importance only in April 2022, as of February 2022 all Brazilian schools had reopened and resumed fully in-person instruction.
Although social and public health restrictions were necessary, one of the main adverse side effects of full or partial school closures was the increased exposure of children to obesogenic behaviors. The interruption of in-person schooling reduced the need to engage in extracurricular tasks and decreased opportunities for active transportation [7]. The closure of sports facilities, parks, and outdoor play areas further limited children’s opportunities for physical activity [8]. At the same time, due to prolonged time spent at home and limited options for active entertainment, sedentary behavior, screen time, and sleep duration increased markedly [9]. Additionally, changes in eating habits were reported, including an increased intake of snacks and processed foods [10]. Furthermore, deprivation and emotional stress contributed to exacerbating psychological distress and the deterioration of mental health, outcomes frequently associated with excess body weight [11].
In this scenario, previous studies suggested that the COVID-19 pandemic exposed children to an increased risk of greater body weight accumulation; however, the evidence found is limited to examining relatively short periods in children from Asian, European, or North American countries and, in most cases, using cross-sectional designs [12,13], while studies with longitudinal designs are scarce [14]. To our knowledge, to date, no study involving Brazilian children has examined temporal trends in body weight during the pandemic period using a longitudinal approach. Studies with this purpose are particularly important and may help to elucidate the harmful impact that occurred during this period, considering that excess body weight identified in childhood tends to track into adulthood [15], is strongly associated with children’s current and future health [16], and with a higher incidence of psychosocial events [17].
Therefore, the objective of the current study was to fill this important gap and to report temporal trends in the weight status of children aged 6 to 11 years prior, during, and post-school closures in response to restrictions imposed by the COVID-19 pandemic, using a six-year school-based cohort design (2020–2025).
2. Methods
2.1. Study Design
This is a six-year, longitudinal, school-based observational study involving children with an initial age of approximately 6 years enrolled in municipal public schools in Cambé, Paraná, Brazil. The intervention protocols were approved by the Research Ethics Committee of the Local University (3.412.665/2019). The children’s parents or guardians signed an Informed Consent Form, granting permission for the children to participate in the study. At the time of data collection, verbal consent was requested from the participants.
The city of Cambé is in the north-central region of Paraná State, Brazil, with a subtropical climate and a population of approximately 110,000. Its economy is based on agricultural activities, public services, and industry, and it is considered an important development hub in the southern region of the country. According to the Human Development Atlas of Brazil, Cambé is a city with a high Average Human Development Index of 0.734. Considering the infant mortality rate, another indicator classically used to assess the level of development of a region, the available information indicates 11 deaths per 1,000 live births.
2.2. Participants
The selection of participants for the study was carried out by inviting the entire universe of students enrolled at the beginning of the 2020 school year (pre-pandemic period, prior-school closures) in the 1st year of elementary education at the 44 public schools existing in the urban region from Cambé, Paraná (N = 1,183). In this case, all parents or guardians of the students were contacted and informed about the nature and objectives of the project, as well as the principles of confidentiality and non-influence on academic performance. Authorization was requested so that the students could participate in data collection.
The following exclusion criteria were adopted: (a) lack of authorization from parents or guardians; (b) absence from school on the day scheduled for data collection; (c) any physical problem that precluded the anthropometric measurements; and (d) chronological age less than 5.5 years and more than 6.5 years. Therefore, the initial sample consisted of 876 participants, representing a recruitment success of 74%.
All participants selected for the initial sample were contacted during the same period in the subsequent five years: 2021 and 2022 (the pandemic period, with total or partial school closures) and 2023, 2024 e 2025 (the post-pandemic period, one, two and three years post schools reopened) for anthropometric measurements. Participants diagnosed with SARS-CoV-2 or those with reports from parents or guardians of disease symptoms were excluded from the sample. Therefore, for data analysis, only the 722 participants (380 girls and 342 boys) who completed all six waves of follow-up were considered, resulting in a 17% loss from the beginning to the end of the follow-up. Figure 1 illustrates the student participation in the study.
2.3. Procedures
The initial data collection took place in February 2020 (the pre-pandemic period, prior-school closures), when the average age of the participants was 6.2 ± 0.2 years. The students were subsequently followed up annually through anthropometric measurements in February 2021 and 2022 (pandemic period, total or partial closure of schools) and 2023, 2024 and 2025 (post-pandemic period, one, two and three years’ post-school reopening), when the average ages of the students were between 7.1±0.2 and 11.1±0,1 years.
The data collection procedure included identifying gender and age, and measuring height and body mass. The researchers comprised physical education teachers from schools that had previously been trained in measurement procedures. The anthropometric measurements (height and body mass) were conducted individually in a private location within the schools, adhering to anti-epidemic control procedures (social distancing, disinfection, and air ventilation), and using standardized and identical protocols across the four monitoring waves.
The participants' chronological age was determined in years and months by comparing the date of data collection with their date of birth. An aluminum stadiometer with a 1 mm scale (Seca, Hamburg, Germany, model 870) was used to measure height. For body mass measurements, an anthropometric scale with a 10-gram setting, Seca brand (Hamburg, Germany, model 879), was used. The scale was calibrated after every ten measures, following procedures presented by the World Health Organization [18]. Replicas were made for every ten students to ensure data quality for height and body mass measurements. The magnitudes of the technical measurement error ranged between 1 mm and 4 mm for height measurements and 10 g and 40 g for body mass measurements.
The body mass index (BMI) was calculated using the ratio of body mass measurements, expressed in kilograms, to height, expressed in meters squared (kg/m²). The diagnostic criteria suggested by the International Obesity Task Force (IOTF) were applied to classify the weight status (underweight, normal weight, overweight, and obesity) of participants [19].
2.4. Statistical Analysis
The statistical analysis of the data was performed using the Statistical Package for the Social Sciences (SPSS, version 31). The anthropometric data were initially compared with the normal curve using the Kolmogorov-Smirnov test. Height and body mass measurements showed normal distributions. Descriptive statistics (mean and standard deviation) were used to characterize the sample, and covariance analysis with interactions involving two classification criteria (gender and age) was performed.
Regarding weight status, specific proportions and their respective 95% confidence intervals (95%CI) were identified and stratified by gender and follow-up period. Statistical differences were analyzed using contingency tables involving the non-parametric chi-square test (χ2) for linear trend. The chances of children having excess body weight (overweight + obesity) in the pandemic/2021, pandemic/2022, post-pandemic/2023, post-pandemic/2024, and post-pandemic/2025 monitoring periods, compared to the pre-pandemic/2020 period, were identified through the values of odds ratios accompanied by 95%CI, calculated using binary logistic regression analysis with adjustments for gender and age. Statistical significance was pre-established at p < 0.05.
3. Results
Table 1 presents the participants' height, body mass, and body mass index measurements, categorized by gender and study period. Girls and boys showed statistically similar measurements; however, the values found in the three anthropometric outcomes indicated an increase with advancing age.
Regarding the weight status of the participants, using the specific cut-off points for gender and age proposed by IOFT, it was found that girls had lower rates of underweight prevalence and higher rates of overweight prevalence than boys (χ2 = 11.925; p < 0,001). Specifically considering the study's follow-up waves, there was a significant tendency for both gender to present increased prevalence rates of overweight and obesity in the pandemic periods, during which schools remained totally or partially closed, and post-pandemic, when schools had already been reopened, compared to the pre-pandemic period, before the closure of schools (girls: χ2 = 9.096; p < 0.001; boys: χ2 = 9.937; p < 0.001) – Table 2.
Figure 2 presents the individual changes in the participants' weight status over the six monitoring waves. At the end of the pandemic period and school closures (2022), the number of children identified as overweight and obese in the pre-pandemic period (prior-school closures) increased from 133 to 198 and from 60 to 101, respectively. During the same period, only seven children who were identified as overweight in the pre-pandemic period transitioned to a normal weight status. Of a group of 490 children initially identified as having normal weight, 113 accumulated enough body weight to be classified as overweight. In comparison, no more than five children moved to a low body weight at the end of the pandemic and school closures. Data equivalent to the post-pandemic period, when schools had already been reopened for at least a year, showed a tendency to a reduction in the greater accumulation of body weight achieved in pandemic periods when schools remained totally or partially closed; however, the rates of excess body weight were still above those identified in the pre-pandemic period, before the closure of schools. During this period, the reduction in body weight was more evident in children initially identified as having normal weight and overweight, in contrast to those identified as obese, who showed more subtle signs of reestablishing body weight.
Table 3 presents binary logistic regression models indicating the risk of children having excess body weight (overweight + obesity) during pandemic periods, when schools remained totally or partially closed, and post-pandemic, when schools had already been reopened for at least one year. The odds ratio values adjusted for gender and age suggest that, in the first pandemic period/2021, children were 50% (OR = 1.50 [95%CI 1.08 – 2.64]; p = 0.032) more likely to have excess body weight than in the pre-pandemic period/2020, while in the second pandemic period/2022 exposure to excess body weight almost doubled (OR = 1.96 [95%CI 1.41 – 3.45]; p < 0.001). In the follow-up waves, equivalent to the post-pandemic period (2023, 2024, and 2025) a declining trend in risk exposure for excess body weight was identified, although it remained statistically significant.
4. Discussion
The current study examined the impact of school closures as a measure to contain the COVID-19 pandemic on the weight status of children aged 6 to 11 years, using six-year (2020-2025) school-based cohort data. The main results showed a significant increase in the prevalence rates of excess body weight in the two years in which schools remained totally or partially closed (pandemic periods 2021 and 2022) compared to the pre-pandemic period/2020, before the closure of schools. Data equivalent to the post-pandemic period (2023, 2024, and 2025), when schools had already been reopened for at least a year, showed a tendency to a reduction in the greater accumulation of body weight achieved in the pandemic periods 2021 and 2022, during which schools remained closed; however, the rates of excess body weight were still significantly above those identified in the pre-pandemic period.
These findings raise concerns for public health in the coming years, as the immediate and long-term consequences of excess body weight on children's health are widely recognized [4,5,15,16,17]. Furthermore, a meta-analysis study found that children with excess body weight may be at a five times greater risk of becoming obese adults compared to their peers with normal body weight and, consequently, more exposed to associated comorbidities [20]. Regarding the increase in body weight above what would be expected for gender and age [19], specifically during the COVID-19 pandemic, our results align with those of other studies employing cross-sectional [12,13] and longitudinal [13] designs. However, while these other studies included children of different ages, ethnicities, economic levels, and cultural backgrounds, and gathered samples from various geographic regions around the world, which may indicate a global representation of the effects of restrictions imposed to mitigate the adverse impact of COVID-19 on weight status; on the other hand, they focused exclusively on immediate effects equivalent to the first year of the pandemic (2020).
To date, there is a lack of data on the long-term effects of the COVID-19 pandemic and subsequent periods on body weight variation in children. A study was conducted with Australian children for a period equivalent to 21 months after the start of the pandemic [21], and another with Austrian children between March/2020 and November/2022 [22]. Similar to what was found in the present study, in both studies, the prevalence rates of overweight and obesity increased immediately after the start of pandemic restrictions; however, with lower rates. After these initial changes, from the second year of the pandemic onwards, the increase in body weight tended to stabilize. Subsequently, the prevalence rates of overweight and obesity gradually returned to rates close to those found in the pre-pandemic period. In our study, a tendency towards body weight stabilization was also observed; however, the prevalence rates of overweight and obesity did not return to pre-pandemic levels (March 2020) by the end of the study (March 2025). It is also noteworthy that in the Australian and Austrian samples, the risk of disproportionate body weight gain during the pandemic period was greater in children with pre-existing overweight or obesity, a finding that was confirmed in the current study.
Interestingly, no differences were identified between the gender in the trends toward increasing body weight induced by anti-epidemic measures. These findings differ from other studies that examined variations in body weight in response to the COVID-19 crisis using cross-sectional designs, which found more pronounced increases in girls than in boys [23]. On the other hand, the data from the present study showed that in the post-pandemic period, the recovery of prevalence rates of overweight and obesity to values close to the pre-pandemic period was lower in girls, suggesting more pronounced residual impacts on their body weight and leaving them with more visible pandemic effects even three years after schools reopened (2025). The reasons for this gender difference could not be analyzed in our study; however, according to findings from a previous study, it is speculated that this may be mainly due to the different inter-gender changes observed in obesogenic behaviors resulting from the restrictions imposed by the COVID-19 pandemic [24].
The weight status is influenced by the interaction of various lifestyle behaviors, including eating habits, physical activity, screen time, and sleep [25]. The restricted mobility, social distancing, and interruption of in-person school activities due to the isolation measures imposed to combat the COVID-19 pandemic resulted in profound changes in the lifestyle behaviors of families, particularly among children [26].
Regarding eating habits, mobility restrictions limited the frequency of purchases of foodstuffs and, consequently, tended to increase the consumption of processed and canned foods, which are easier to acquire and store and have a longer shelf life, which can directly impact children's nutrition. Moreover, the interruption of face-to-face classes deprived children of consuming school meals prepared according to a planned and nutritionally balanced menu. In this scenario, several children who depended financially on school meals to complement the food offered at home had less availability of nutritious food [27]. A previous study found that changes in children's eating habits may have influenced the type of snack foods taken from home to school after the return of in-person classes, providing strong evidence that unhealthy eating behaviors acquired during the COVID-19 pandemic persist in the daily lives of families [28].
Two other lifestyle behaviors significantly impacted by the actions resulting from the COVID-19 pandemic are the reduction in physical activity and the increase in screen time [29]. Schools are an ideal environment to enhance children's physical activity. This scenario enables students to participate in physical education classes, engage in sports, play active games, and interact in groups, thereby reducing the likelihood of using screen-based equipment [30]. However, with the temporary closure of schools, children remained without this school support for an extended period. Further aggravating this situation, children demonstrated difficulty accessing public areas, parks, and clubs where they can play or engage in activities that would increase physical activity and reduce screen time.
Furthermore, the school environment can help define the routines and structures necessary for children's mealtimes, physical activity, sleeping periods, and lifestyle behaviors, thus implying a greater risk of overweight and obesity without these routines [23]. In this context, school vacation periods are usually associated with a greater increase in body weight due to the dysregulation of these three lifestyle behaviors [31], and the COVID-19 pandemic extraordinarily exacerbated this effect with the interruption of in-person school activities. A previous study, which investigated the perception of parents of children between four and 12 years old, pointed out that the children's daily screen time more than doubled, physical activity time decreased by half, and bedtime was postponed by around two hours during the period in which schools remained closed because of the COVID-19 pandemic [32].
The effects inherent to the social distancing measures imposed to mitigate the adverse impact of COVID-19 also generated repercussions on family and friendship relationships, as well as on mental health outcomes. Children who previously spent a large portion of the day in schools and other environments involving social interaction with peers were, for extended periods, restricted exclusively to the home environment, removed from their routines and exposed to a context of uncertainty, stress, and psychological distress [33], which strongly affected their mental health. A systematic review and meta-analysis synthesized data from longitudinal studies comparing pre-pandemic and pandemic estimates and demonstrated a significant increase in episodes of depression and anxiety among children during the COVID-19 pandemic [34]. In this context, it is widely recognized that depressive and anxiety symptoms tend to potentiate lifestyle behaviors that may increase the risk of overweight and obesity in childhood and adolescence [35,36].
The study has some strengths. It is a longitudinal design with anthropometric annual measurements that allow comprehensive conclusions about the short- and medium-term impact of the COVID-19 pandemic restrictions on children's weight status. A representative sample was recruited, encompassing the entire universe of students in the 1st year of primary education in public schools in the urban region of Cambé, Paraná, with an acceptable rate of refusal to participate in the study (9%), thereby ensuring greater reliability of the findings. All anthropometric measurements were taken annually by trained personnel, increasing the data collection quality. Possible seasonal interferences in anthropometric measurements were eliminated, considering that data collection was carried out at the same time of year (February). Another strong point worth mentioning was the analysis of body weight in different weight status, which produced more detailed findings on the impact of the pandemic periods.
The limitations of the study must also be recognized. For one, as the study focuses on a specific population of children attending public elementary schools in Cambé, Paraná, the findings may have limitations in their generalizability to the child population of other Brazilian regions. However, due to the study design, the participant selection procedures, the large sample, and the methodological rigor used in collecting and processing the data, it is quite likely that the results found can describe, with satisfactory conditions, the short and medium-term impact of COVID-19 pandemic restrictions on the weight status of children in cities in the northern region of Paraná. Furthermore, the analyses were adjusted for gender and age but not for other demographic data that could produce some residual confusion, such as the economic condition of the families. However, the financial condition of families can be estimated, as the selected students belong exclusively to public schools, although the collected data does not have the power to identify the economic status of the study participants. Moreover, the reasons for changes in body weight cannot be identified, as no data are available on potential mediators of lifestyle behaviors, including eating habits, physical activity, screen time, sleep, and psycho-emotional factors related to the pandemic. It is essential to consider that participation in the study was voluntary; therefore, possible selection bias cannot be ruled out.
5. Conclusions
Our results suggest that the restrictions imposed to mitigate the adverse impact of the COVID-19 pandemic, including the total or partial closure of schools, substantially increased the body weight of the children above what would be expected for gender and age. After two years of the pandemic period, 23% of children identified in the pre-pandemic period with normal body weight migrated to overweight, while 34% of overweight children became obese. Data equivalent to the post-pandemic period showed signs of a reduction in the excess body weight accumulated during the pandemic; however, the prevalence rates of overweight and obesity remained significantly higher than in the pre-pandemic period. Therefore, the study findings suggest that the harmful effects contributing to the greater accumulation of body weight during the COVID-19 pandemic were not reversed spontaneously, even five years after its onset. Thus, specific actions to prevent, combat, and control overweight and obesity are essential to avoid present and future adverse consequences for children's health.
Author Contributions
Conceptualization, D.P.G., S.L.S. and A.B.G.; methodology, D.P.G., S.L.S. and A.B.G.; software, D.P.G; validation, D.P.G., S.L.S. and A.B.G.; formal analysis, D.P.G., S.L.S. and A.B.G.; investigation, D.P.G., S.L.S. and A.B.G.; resources, D.P.G., S.L.S. and A.B.G.; data curation, D.P.G.; writing—original draft preparation, D.P.G.; writing—review and editing, D.P.G., S.L.S. and A.B.G.; visualization, D.P.G., S.L.S. and A.B.G.; supervision, D.P.G; project administration, D.P.G.; funding acquisition, D.P.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. D.P.G is a Research Productivity Fellow at Brazilian National Board for Scientific and Technological Development–CNPq.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Local University (Reference No. 3,412,665/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors wish to thank all the participants involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- GBD 2021 Adolescent BMI Collaborators. Global, regional, and national prevalence of child and adolescent overweight and obesity, 1990-2021, with forecasts to 2050: a forecasting study for the Global Burden of Disease Study 2021. Lancet 2025, 405, 785-812.
- Guedes, D.P.; Mello, E.R.B. Prevalence of overweight and obesity among Brazilian children and adolescents: Systematic review and meta-analysis. ABCS Health Sci 2021, 46, e021301. [CrossRef]
- World Obesity Federation. World Obesity Atlas 2025. London: World Obesity Federation. 2025.
- Li, L.; Sun, F.; Du, J.; Li, Z.; Chen, T.; Shi, X. Behavior-change lifestyle interventions for the treatment of obesity in children and adolescents: A scoping review. Ann. N. Y. Acad. Sci. 2025, 1543, 31-41. [CrossRef]
- Jebeile, H.; Kelly, A.S.; O'Malley, G.; Baur, L.A. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol 2022,10, 351-365. [CrossRef]
- United Nations Educational, Scientific and Cultural Organization – UNESCO. COVID-19 Educational Disruption and Response [Internet]. Paris, UNESCO. 2022. Available from: https://www.unesco.org/en/articles/covid-19-educational-disruption-and-response.
- Kharel, M.; Sakamoto, J.L.; Carandang, R.R.; Ulambayar, S.; Shibanuma, A.; Yarotskaya. E.; Basargina, M.; Jimba, M. Impact of COVID-19 pandemic lockdown on movement behaviours of children and adolescents: a systematic review. BMJ Glob. Health 2022, 7, e007190. [CrossRef]
- Wunsch, K.; Kienberger, K.; Niessner, C. Changes in physical activity patterns due to the Covid-19 pandemic: a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2022, 19, 2250. [CrossRef]
- Runacres, A.; Mackintosh, K.A.; Knight, R.L.; Sheeran, L.; Thatcher, R.; Shelley, J.; McNarry, M.A. Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11286. [CrossRef]
- Bennett, G.; Young, E.; Butler, I.; Coe, S. The impact of lockdown during the COVID-19 outbreak on dietary habits in various population groups: a scoping review. Front. Nutr 2021, 8, 626432. [CrossRef]
- Tang, S.; Xiang, M.; Cheung, T.; Xiang, Y.T. Mental health and its correlates among children and adolescents during COVID-19 school closure: The importance of parent child discussion. J. Affect. Disord. 2021, 279, 353-360. [CrossRef]
- Khan, M.A.; Menon, P.; Govender, R.; Abu Samra, A.M.; Allaham, K.K.; Nauman, J.; Östlundh, L.; Mustafa, H.; Smith, J.E.M.; AlKaabi, J.M. Systematic review of the effects of pandemic confinements on body weight and their determinants. Br. J, Nutr. 2022, 127, 298-317. [CrossRef]
- Anderson, L.N.; Yoshida-Montezuma, Y.; Dewart, N.; Jalil, E.; Khattar, J.; De Rubeis, V.; Carsley, S.; Griffith, L.E.; Mbuagbaw, L. Obesity and weight change during the COVID-19 pandemic in children and adults: A systematic review and meta-analysis. Obes Rev. 2023, 24, e13550. [CrossRef]
- Jarnig, G.; Jaunig, J.; Kerbl, R.; Strenger, V.; Haeusler, G.; van Poppel, M.N.M. Acceleration in BMI gain following COVID-19 restrictions. A longitudinal study with 7- to 10-year-old primary school children. Pediatr Obes. 2022, 17, e12890. [CrossRef]
- St Fleur, R.G.; Tanofsky-Kraff, M.; Yanovski, J.A.; Horton, N.J.; Hirschhorn, J.N.; Field, A.E. Phenotyping children and adolescents with obesity using behavioral, psychological, and familial data. Obesity (Silver Spring) 2023, 31, 3016-3024. [CrossRef]
- Park, M.H.; Falconer, C.; Viner, R.M.; Kinra, S. The impact of childhood obesity on morbidity and mortality in adulthood: a systematic review. Obes. Rev. 2012, 13, 985-1000. [CrossRef]
- Morales-Suárez-Varela, M.; López-García, E.; Peraita-Costa, I.; Pérez Puente, J.M.; Llopis-Morales, A.; Llopis-Gonzalez, A.; Guallar-Castillón, P. Obesity and mental health in childhood and adolescence: A scoping review of recent scientific evidence. Children 2025, 12, 1512. [CrossRef]
- World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. [Technical Report Series n° 854]. Geneva: WHO. 1995.
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 2012, 7, 284-294. [CrossRef]
- Simmonds, M.; Burch, J.; Llewellyn, A.; Griffiths, C.; Yang, H.; Owen, C. The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: a systematic review and meta-analysis. Health Technol. Assess. 2015, 19, 1-336. [CrossRef]
- Bond, D.M.; Seimon, R.; Schneuer, F.J.; Baur, L.A.; Craig, M.; Alexander, S. Impact and recovery of the COVID-19 pandemic on weight status of children and adolescents. Clin. Obes. 2023, 13, e12579. [CrossRef]
- Irschik, S.; Brandt, J.B.; Eisenkolbl, J. COVID-19 pandemic-related weight gain in the pediatric population declined after restrictions ended, except among obese patients. Front. Public Health 2023, 11, 1260269. [CrossRef]
- Jenssen, B.P.; Kelly, M.K.; Powell, M.; Bouchelle, Z.; Mayne, S.L.; Fiks, A.G. COVID-19 and changes in child obesity. Pediatrics 2021, 147, e2021050123. [CrossRef]
- de Bruijn, A.G.M.; Te Wierike, S.C.M.; Mombarg, R. Trends in and relations between children's health-related behaviors pre-, mid- and post-Covid. Eur. J. Public Health 2023, 33, 196-201. [CrossRef]
- Schrempft, S.; van Jaarsveld, C.H.M.; Fisher, A.; Herle, M.; Smith, A.D.; Fildes, A. Variation in the heritability of child body mass index by obesogenic home environment. JAMA Pediatr. 2018, 172, 1153-1160.
- Browne, N.T.; Snethen, J.A.; Greenberg, C.S.; Frenn, M.; Kilanowski, J.F.; Gance-Cleveland, B. When pandemics collide: the impact of COVID-19 on childhood obesity. J. Pediatr. Nurs. 2021, 56, 90-98. [CrossRef]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19-related school closings and risk of weight gain among children. Obesity (Silver Spring) 2020, 28, 1008-1009. [CrossRef]
- Parnham, J.C.; Laverty, A.A.; Majeed, A.; Vamos, E.P. Half of children entitled to free school meals did not have access to the scheme during COVID-19 lockdown in the UK. Public Health 2020, 187, 161-164. [CrossRef]
- Neville, R.D.; Lakes, K.D.; Hopkins, W.G.; Tarantino, G.; Draper, C.E.; Beck, R. Global changes in child and adolescent physical activity during the COVID-19 pandemic: a systematic review and meta-analysis. JAMA Pediatr. 2022, 176, 886-894.
- An, R. Projecting the impact of the coronavirus disease-2019 pandemic on childhood obesity in the United States: A microsimulation model. J. Sport Health Sci. 2020, 9, 302-312. [CrossRef]
- von Hippel, P.T.; Workman, J. From kindergarten through second grade, U.S. children's obesity prevalence grows only during summer vacations. Obesity (Silver Spring) 2016, 24, 2296-2300.
- Beck, A.L.; Huang, J.C.; Lendzion, L.; Fernandez, A.; Martinez, S. Impact of the coronavirus disease 2019 pandemic on parents' perception of health behaviors in children with overweight and obesity. Acad. Pediatr. 2021, 21, 1434-1340. [CrossRef]
- Kamoshida, S.; Nihonmatsu, N.; Takagi, G.; Wakashima, K. The relationship between family variables and family social problems during the COVID-19 pandemic. PLoS ONE 2022, 17, e0270210. [CrossRef]
- Madigan, S.; Racine, N.; Vaillancourt, T.; Korczak, D.J.; Hewitt, J.M.A.; Pador, P.; Park, J.L.; McArthur, B.A.; Holy, C.; Neville, R.D. Changes in depression and anxiety among children and adolescents from before to during the COVID-19 pandemic: A systematic review and meta-analysis. JAMA Pediatr. 2023, 177, 567-581.
- Sutaria, S.; Devakumar, D.; Yasuda, S.S.; Das, S.; Saxena, S. Is obesity associated with depression in children? Systematic review and meta-analysis. Arch. Dis. Child. 2019, 104, 64-74. [CrossRef]
- Burke, N.L.; Storch, E.A. A meta-analysis of weight status and anxiety in children and adolescents. J. Dev. Behav. Pediatr. 2015, 36, 133-145. [CrossRef]
Figure 1.
Flowchart of the study population and participants.
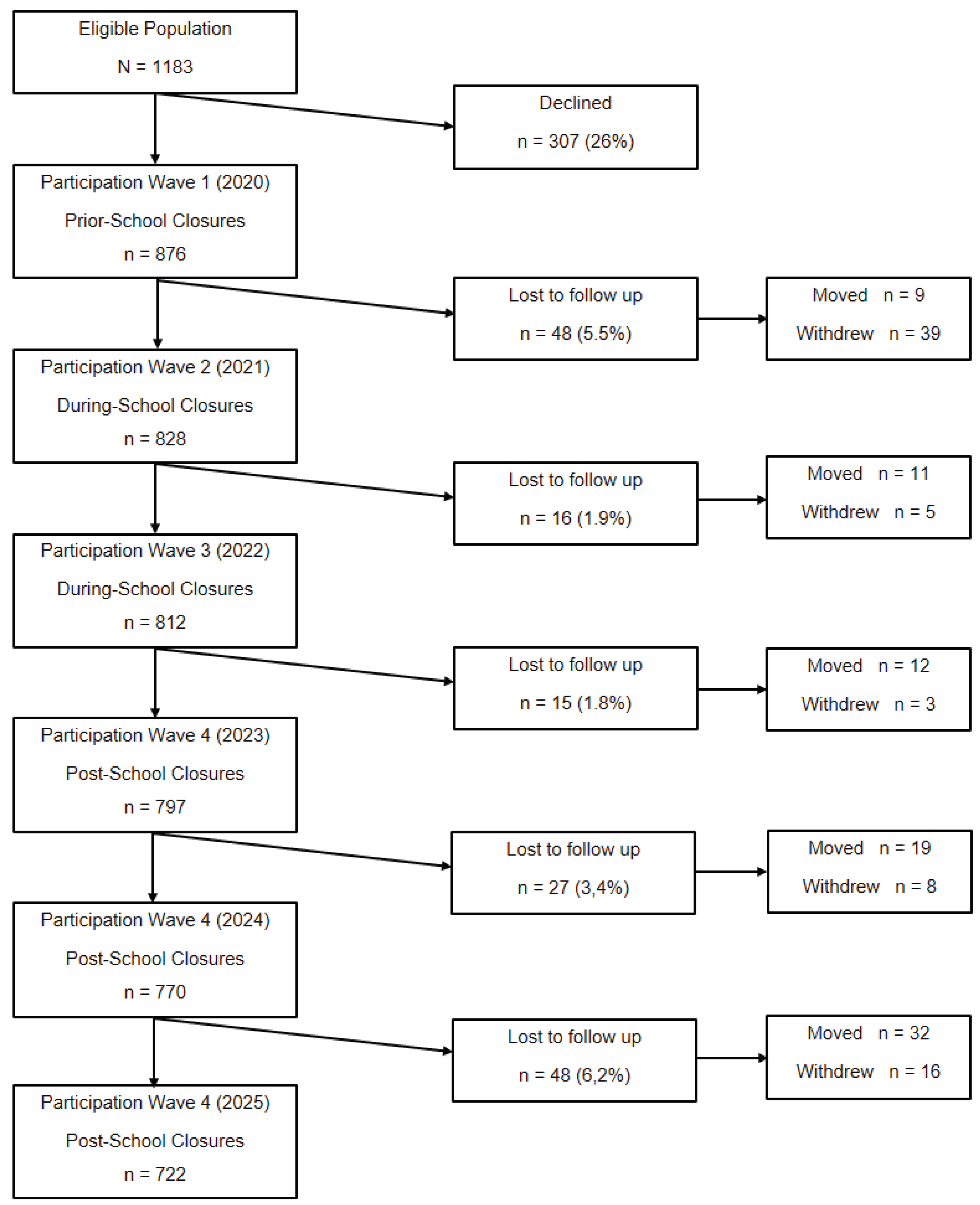
Figure 2.
Individual changes in children’s weight status throughout the six monitoring waves of the COVID-19 Pandemic.
Figure 2.
Individual changes in children’s weight status throughout the six monitoring waves of the COVID-19 Pandemic.
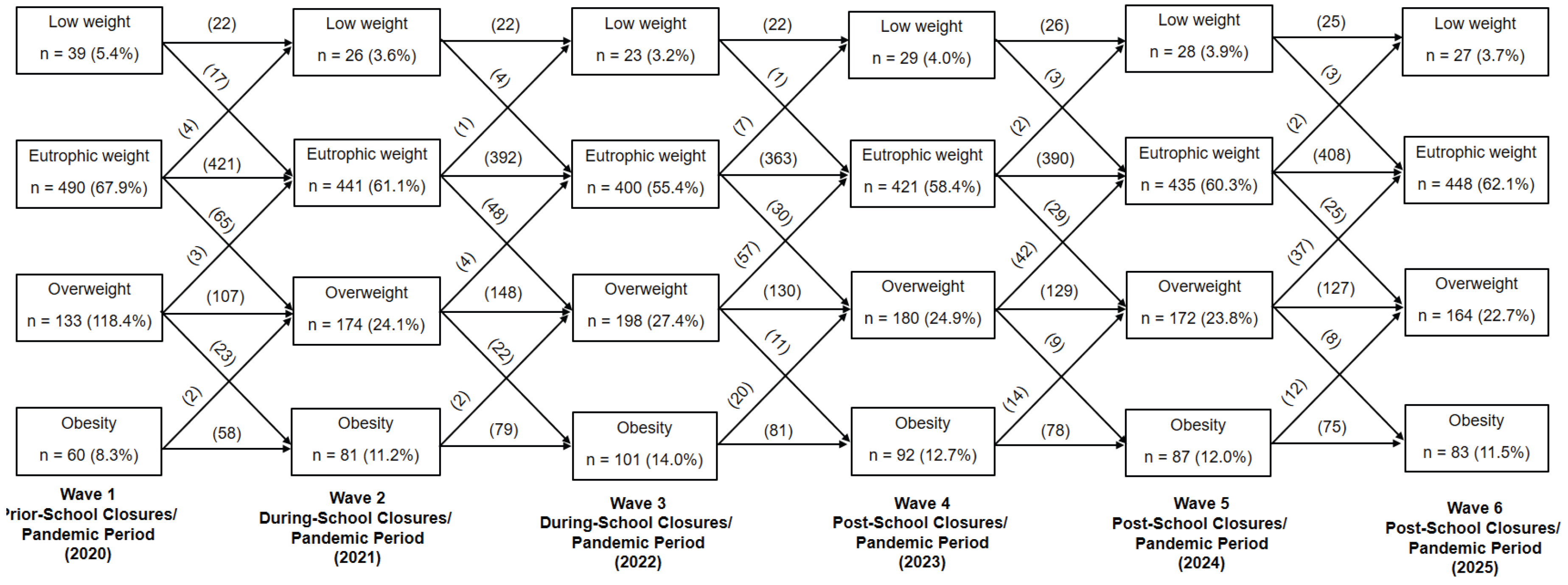

Table 1.
Mean values, standard deviation, and “F” statistics equivalent to the height, body mass, and body mass index measurements of the participants (n = 722).
Table 1.
Mean values, standard deviation, and “F” statistics equivalent to the height, body mass, and body mass index measurements of the participants (n = 722).
| Age | Stature (cm) | Weight (kg) | BMI (kg/m2) | ||||
| Waves | (years) | Girls | Boys | Girls | Boys | Girls | Boys |
| Prior-School Closures/ Pandemic/2020 | 6.2±0,2 | 117.6±5.4 | 119.4±5,7 | 22.7±4,4 | 23.5±4.8 | 16.4±2.4 | 16.6±2.4 |
| During-School Closures/ Pandemic/2021 | 7.1±0,2 | 123.0±6.6 | 124.3±6.1 | 25,5±5.2 | 25.9±5.4 | 16.9±2.5 | 17.5±2.6 |
| During-School Closures/ Pandemic/2022 | 8.1±0,2 | 127.9±6,9 | 129.6±6.6 | 28.1±5,8 | 29.2±5.8 | 17.3±2.6 | 17.8±2.8 |
| Post-School Closures/ Pandemic/2023 | 9.0±0,1 | 134.3±7.3 | 132.2±7.0 | 31.1±6.3 | 32,9±6.9 | 17,6±2.6 | 18.1±2.9 |
| Post-School Closures/ Pandemic/2024 | 10.2±0,2 | 140.2±7.7 | 141.1±7.4 | 34.9±6.9 | 35.3±7.3 | 17.9±2.7 | 18.4±2.8 |
| Post-School Closures/ Pandemic/2025 | 11.1±0,1 | 146.9±8.2 | 145.9±7.8 | 38.2±7.5 | 37.7±7.6 | 18.4±2.8 | 18.7±3.0 |
| F Age: | 158.617 (p < 0.001) | 291.539 (p < 0.001) | 4.732 (p = 0,013) | ||||
| F Gender: | 1.218 (p = 0.143) | 2.783 (p = 0.048) | 2.485 (p = 0.072) | ||||
| F Interaction: | 2.423 (p = 0.094) | 2.458 (p = 0.109) | 1.862 (p = 0.118) | ||||
Table 2.
Prevalence rates (%) of weight status according to the International Obesity Task Force (IOFT) criteria.
Table 2.
Prevalence rates (%) of weight status according to the International Obesity Task Force (IOFT) criteria.
| Prior-school closures (2020) |
During-school closures (2021-2022) |
Post-school closures (2023) |
Post-school closures (2024) |
Post-school closures (2025) |
||
| 6 years | 7 years | 8 years | 9 years | 10 years | 11 years | |
| Girls | ||||||
| Low weight | 4.6 (4.2 – 5.1) | 2.9 (2.6 – 3.3) | 2.6 (2.4 – 2.9) | 3.5 (3.2 – 3.9) | 3.4 (3.1 – 3.8) | 3.2 (2.9 – 3.6) |
| Normal weight | 67.4 (64.0 – 70.9) | 60.5 (57.3 – 63.8) | 54.4 (51.6 – 57.3) | 57.2 (54.4 – 60.1) | 59.2 (56.1 – 62.4) | 61.1 (57.9 – 64.4) |
| Overweight | 19.9 (18.7 – 21.2) | 25.9 (24.4 – 27.5) | 28.9 (27.3 – 30.6) | 26.7 (25.2 – 28.3) | 25.5 (24.0 – 27.1) | 24.3 (22.8 – 25.9) |
| Obesity | 8.1 (7.3 – 9.0) | 10.7 (9.8 – 11.7) | 14.1 (13.2 – 15.2) | 12.6 (11.8 – 13.6) | 11.9 (11.1 – 12.9) | 11.4 (10.6 – 12.3) |
| Boys | ||||||
| Low weight | 6.3 (5,7 – 7.0) | 4.3 (3.9 – 4.8) | 3.9 (3.5 – 5.4) | 4.7 (4.3 – 5.2) | 4.6 (4.2 – 5.1) | 4.4 (4.0 – 4.9) |
| Normal weight | 68.4 (65.0 – 71.9) | 61.8 (58.7 – 65.0) | 56.1 (53.3 – 59.0) | 59.2 (56.2 – 62.3) | 61.1 (58.0 – 64.3) | 62.9 (59.7 – 66.2) |
| Overweight | 16.6 (15.6 – 17.8) | 22.2 (20.8 – 23.7) | 25.6 (25.1 – 27.2) | 23.2 (21.8 – 24.7) | 22.2 (20.8 – 23.7) | 21.2 (19.9 – 22.6) |
| Obesity | 8.7 (7.9 – 9.6) | 11.7 (10.9 – 12.6) | 14.4 (13.5 – 15.6) | 12.9 (12.0 – 13.9) | 12.1 (11.3 – 13.0) | 11.6 (10.8 – 12.5) |
| χ2Wave | Girls: 9.096 (p < 0.001) | Boys: 9.937 (p < 0.001) | ||||
| χ2Gender | 11.925 (p < 0.001) | |||||
Table 3.
Chances of children having excess body weight (overweight + obesity) in the pandemic and post-pandemic periods compared to the pre-pandemic period.
Table 3.
Chances of children having excess body weight (overweight + obesity) in the pandemic and post-pandemic periods compared to the pre-pandemic period.
| Waves | Prevalence Rate (CI95%) | OR (CI95%) | p |
| Prior-school closures/pandemic (2020) | 26.7 (25.1 – 28.4) | Reference | |
| During-school closures/pandemic (2021) | 35.3 (33.2 – 37.5) | 1.50 (1.08 – 2.64) | 0.032 |
| During-school closures/pandemic (2022) | 41.6 (39.3 – 44.0) | 1.96 (1.41 – 3.45) | < 0.001 |
| Post-school closures/pandemic (2023) | 37.8 (35.6 – 40.1) | 1.67 (1.20 – 2.94) | 0.019 |
| Post-school closures/pandemic (2024) | 35.9 (33.8 – 38.1) | 1.54 (1.11 – 2.71) | 0.027 |
| Post-school closures/pandemic (2025) | 34.3 (32.3 – 36.4) | 1.43 (1.03 – 2.53) | 0.045 |
Values adjusted for gender and age.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



