Submitted:
11 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Background: The infection of the cervical epithelium with high-risk human papillomavirus (HR-HPV) accounts for more than 95% of cervical cancer cases. This study aimed to provide epidemiological data and assess the prevalence and genotype distribution of HR-HPV in Bulgaria. Methods: Cervical samples from 190 women were concurrently tested using routine liquid-based cytology (LBC) for 14 HR-HPV genotypes and cytology. HPV detection and genotyping were performed using the clinically validated Alinity m HR-HPV assay. This test provides detailed information on HPV16, HPV18, and HPV45 and categorizes the remaining 11 HR-HPV genotypes into two groups: other HR-HPV A and other HR-HPV groups. Stained LBC samples were reported using the Bethesda System. Results: HR-HPV infection was detected in 16.8% of the women screened, with mean age 38.2 (± 9.8) years. Infection with HPV16 could be seen in 5.3%, HPV18 positive were 2.2% and genotype HPV45 was found in 1.0%. Abnormalities in LBC cytology were observed in 18.9% of women. HR-HPV positivity in normal cytology samples was 5.2% and 63.9% in abnormal smears. Conclusion: Currently, molecular HPV tests are used for cervical cancer screening adjunctively to LBC as a first-line primary cervical cancer screening test for abnormal cell changes in the cervix.
Keywords:
human papillomavirus
; high-risk HPV types
; alinity m HPV
; primary cervical cancer screening
1. Introduction
Human papillomavirus (HPV) is a double-stranded DNA virus within the Papillomaviridae family that is responsible for the most prevalent sexually transmitted infection globally, adversely affecting personal social life[1]. Concurrently, HPV accounts for nearly 5% of all oncological diseases in both women and men worldwide, thereby reducing life expectancy [2]. The Papillomaviridae family includes two subfamilies (First-papillomavirinae and Second-papillomavirinae), comprising 53 genera and over 130 species [3]. Over 200 HPV genotypes have been identified, categorized into different genera (Alpha, Nu/Mu-, Beta-, and Gammapapillomavirus) based on viral genome structure and tropism to human epithelial tissues, affecting epithelial cells at various localizations in the human body[4]. Based on their scientifically established link to carcinogenic potential, mucosal alphapillomaviruses are divided into two primary groups: non-oncogenic, low-risk HPV (LR-HPV), such as types 6 and 11, which are responsible for cutaneous and anogenital warts and respiratory tract papillomas, and oncogenic HPV (HR-HPV), which causes cervical cancer, anogenital cancers, and oropharyngeal cancers, as well as anal, vulvar, vaginal, and penile cancers [5]. Approximately 40 HPV types infect the mucosal epithelium, including types 16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, and 68, which are classified as oncogenic HR-HPVs [6]. International Agency for Research on Cancer (IARC) recognizes 12 HPV types as oncogenic (HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59) and 1 HPV type as “probably oncogenic” (HPV68) [7].
In the 1970s, Prof. Zur Hausen established the relationship between HPV and cervical cancer. A German virologist confirmed the hypothesis that the viral infection found in condyloma acuminata (genital warts) might lead to cervical neoplasia and invasive cancer development. The author was awarded the Nobel Prize in Physiology or Medicine in 2008 [8]. The replacement of cervical carcinogenesis can be summarized in four stages: 1) HPV acquisition, 2) HPV persistence (vs. clearance), 3) progression of a persistent infection to cervical precancer, and 4) invasion. The carcinogenic potential of HPVs is due to the function of viral E6 and E7 oncoproteins that enhance uncontrolled cell proliferation and block apoptosis by inactivating the cell cycle control factors p53 and pRb, respectively [9] .
The prevalence of HPV infection varies geographically and demographically, and is influenced by factors such as sexual behavior, socioeconomic status, healthcare access, and vaccination coverage. HPV infects both men and women, although the disease burden is significantly higher in women due to the high susceptibility of cervical cells to HPV infection [10].Despite the high incidence of HPV infections, 70-90% of infected individuals experience spontaneous resolution within 1-2 years, without progressing to clinical manifest disease. In a minority of cases, infection persists, evading immune system detection, suppressing innate immunity, and hindering the adaptive immune response. Persistent infection is the most significant risk factor for epithelial cell changes, the development of high-grade squamous cell lesions, and the progression to cervical cancer and other malignancies [11].
HR-HPV genotype 16 is responsible for approximately 50% of cervical cancer cases globally, with genotypes 16 and 18 together accounting for approximately 66% of cases. Additionally, five other high-risk types, 31, 33, 45, 52, and 58, contributed to a further 15% of reported cervical cancer cases and 11% of all HPV-related cancers cases [12] Over 50% of women were infected with HPV by the age of 21, which correlates with the peak incidence of cervical cancer occurring between the ages of 40 and 55. Between 5% and 30% of individuals infected with HPV harbor multiple virus types [13]. Due to multiple HPV genotypes, infection with one type of virus does not confer immunity against another type, potentially leading to subsequent infections. Furthermore, the post-infection immune response is often short-lived, allowing for reinfection with the same HPV type [14].
The World Health Organization has developed a global strategy to eliminate cervical cancer as a public health concern. Cervical cancer is frequently referred to as the “cancer of the young, “ with approximately 660,000 new cases and 350,000 deaths annually. This cancer is largely preventable through HPV vaccination and regular screenings, as recommended by national guidelines, and it can be effectively treated if detected early and managed promptly [15]. Countries worldwide are intensifying efforts to eliminate cervical cancer, adhering to the global 90–70–90 targets: ensuring 90% of girls are fully vaccinated with the HPV vaccine by age 15, 70% of women are screened by ages 35 and 45, and 90% of women with pre-cancer or invasive cancer receive appropriate treatment. In numerous European nations, vaccination, screening initiatives, and post-screening treatments have resulted in a reduction in cervical cancer morbidity and mortality [16].
Infection of the cervical epithelium with HR-HPV accounts for more than 95% of cervical cancer cases in women [17]. Cervical cancer is the 4th most frequent cancer among women in Bulgaria and the 2nd most frequent cancer among women between 15 and 44 years of age. Approximately 1,009 new cervical cancer cases are diagnosed annually in Bulgaria. In Eastern Europe, the region Bulgaria accounts for 9.7% of women in the general population are estimated to harbor cervical HPV16 and HPV18 infection, and 84.7% of invasive cervical cancers are attributed to HPV16 or 18. There are still no official data available on the HPV burden in the general population of Bulgaria, and this survey aims to offer a baseline understanding of the prevalence and genotype distribution of HR-HPV in the Bulgarian population. This is essential for developing effective preventive measures to curb HPV transmission, studying its epidemiological patterns, establishing screening protocols, and evaluating and enhancing vaccination programs [18].
The Alinity m HR-HPV assay, developed by Abbott Molecular in the USA, received the CE mark in 2019 as part of a series of advanced molecular assays compatible with the automated continuous random-access Abbott Alinity m system. The Alinity m HR HPV assay received FDA approval in October 2023. This HPV assay is designed to detect and partially detect 14 high-risk HPV genotypes. Extended genotyping for high-risk human papillomavirus types enhances diagnostic precision by identifying additional oncogenic HPV types beyond HPV 16 and 18. The assay provides detailed information on three primary high-risk HPV genotypes-HPV16, HPV18, and HPV45, and categorizes the remaining 11 targeted high-risk HPV genotypes into two groups: HPV31,33,52,58 (other HR-HPV A) and HPV35,39,51,56,59,66,68 (other HR-HPV B) [19].
Since 1941, the Papanicolau-stained smear test has been the standard method for screening for premalignant lesions and cervical cancer. However, it has a false-negative rate ranging from 5% to 20%, influenced by factors such as the population being tested, the quality of the laboratory, and the disease threshold [20].
Owing to the limitations of cytology, primary testing for HR-HPV is recommended worldwide as a cervical cancer screening strategy for women at normal risk. Currently, molecular HPV tests are used for cervical cancer screening adjunctively, liquid-based cytology, as a first-line primary cervical cancer screening test, for screening of abnormal cell changes in the cervix that might lead to cervical cancer, and for the detection of atypical squamous cells of undetermined significance or squamous intraepithelial lesions. This screening and surveillance must be individualized in accordance with professional medical guidelines, taking into account results from prior screenings, medical history, and other risk factors [21].
2. Materials and Methods
Aim of the Study
The objective of this study was to evaluate the prevalence and genotype distribution of high-risk human papillomavirus using the Alinity m analyzer in a cohort of 190 women from the general population across Bulgaria. These individuals were tested at one of the largest medical diagnostic laboratories at the inception of the newly initiated and expanded “National Program for Primary Prevention of Cancer Diseases Caused by Human Papillomavirus 2025-2030” in Bulgaria.
Study Population
This descriptive, cross-sectional study on the persistence of high-risk (HR) HPV was conducted over a six-month period from May 2025 to October 2025 at the Medical Diagnostics Laboratory Synevo in Bulgaria. Cervical swab samples were collected by a gynecologist during consultations using a specialized cervical brush and placed in a container designed for liquid-based cytology (LBC) (ThinPrep PreserveCyt test collection vials, Hologic, UK). The vials containing the specimens in PreservCyt Solution were stored at room temperature and transported to the laboratory for processing. Upon arrival at Synevo, the cervical samples were tested concurrently in routine liquid-based cytology for HR-HPV genotypes and cytology from the same test collection vial, as the solution was formulated to preserve cellular integrity for both cytological evaluation and ancillary molecular testing.
HR-HPV Screening with Alinity m
Women participating in the HPV screening round were evaluated using the fully automated molecular diagnostics analyzer Alinity m (Abbott, USA), employing the high-risk (HR) HPV assay, in accordance with the manufacturer’s instructions. The HR-HPV assay is a qualitative test that facilitates the identification of HR-HPV genotypes and genotype groups within a highly conserved region of L1 at clinically relevant levels. Alinity m HR-HPV is recommended for cervical cancer screening and patient management in alignment with professional medical guidelines, including HPV primary screening, co-testing (adjunctive screening), and triage of atypical squamous cells of undetermined significance (ASC-US) in women to assess the risk of cervical cancer.
Principles of Alinity m HR HPV PCR Procedure
The Alinity m HR HPV assay comprises several sequential steps, including sample preparation, PCR assembly, amplification/detection, and calculation and reporting of the results. The Alinity m system automates the entire assay procedure, eliminating the need for user intervention in the intermediate processing or transfer steps [22].
1. Sample Preparation (Nucleic acid extraction and purification). Nucleic acids from specimens were extracted using the Alinity m Sample Prep Kit 1 and Alinity m System Solutions. Nucleic acid extraction (lysis) disrupted the biological matrix to release the nucleic acid materials and allowed it to adhere to the surface of magnetic microparticles. The magnetic microparticle technology facilitated nucleic acid capture, wash and elution.
2. Nucleic acid amplification. Purified specimen nucleic acids were amplified by real-time polymerase chain reaction (PCR) using a mix composed of thermostable DNA polymerase, dNTPs, MgCl2, and short oligonucleotide primers for the 14 HR-HPV targets and an endogenous human beta-globin sequence. The endogenous human beta-globin sequence was measured in a separate channel and served as an internal control (IC) to evaluate cell adequacy, sample extraction, and amplification efficiency.
3. Nucleic acid detection. Within a single PCR well, the Alinity m HR HPV probes were labeled with different fluorophores that allowed for genotype specific detection of HPV16, 18, and 45 while the remaining 11 HR HPV genotypes were detected as other HR-HPV A (HPV31,33,52,58 genotypes) or other HR-HPV B (HPV35,39,51,56,59,66,68). Amplification of beta-globin sequence was detected also reported separately using a uniquely labeled fluorescent probe.
The Alinity m System’s data analysis software provided two basic types of analysis for а single assay reaction: Ct (threshold method and MaxRatio (Maximum ratio, MR) method. The MaxRatio method is an Abbott’s proprietary algorithm to produce MaxRatio value that is related to PCR efficiency and is used to differentiate positive from negative reactions. Ct threshold method was defined as the cycle number at which the PCR fluorescence signal reached established threshold above the baseline fluorescence level. Every signal was defined either as “HPV detected,” if the cycle number (CN) is less than or equal to a fixed cutoff cycle for that signal, or as “HPV not detected,” if CN is not generated or it was possibly greater than the assay cutoff cycle.
Inclusion criteria were: (1) female sex, (2) cervical samples for liquid-based cytology- ThinPrep (3) HPV test performed on Alinity m (Abbott) in Synevo laboratory, Bulgaria and (4) valid result of the performed HPV test. Exclusion criteria were: (1) women tested for HPV with samples different from LBC (ThinPrep), although Alinity m HR HPV assay is compatible with various collection devices such as: vaginal specimens (simpli-COLLECT™ HPV Collection Kit and Evalyn® Brush) and cervical specimens: SurePath and Alinity m Cervi-Collect Specimen Collection Kit), (2) women tested for HPV with dry swabs, (3) women without parallel LBC result, (4) women with missing data.
Liquid-Based Cytology (LBC)
Cervical specimens were taken by a specialist and immediately rinsed or agitated in a vial containing ThinPrep PreservCyt Solution (Hologic Inc., Marlborough, MA, USA) to optimally preserve cellular morphology and prevent air-drying artifacts. In the Synevo laboratory, the vials were loaded onto an automated ThinPrep processor. The processor disperses the cells, removes debris and obscuring material (such as blood or mucus), and transfers a representative sample of cells onto a glass slide in a uniform, thin layer of cells onto a glass slide for microscopic examination, according to the manufacturer’s instructions. LBC samples stained with Papanicolaou dye were reported by pathology specialists using the 2014 Bethesda System [23]. Specimens were classified based on cytology as negative for intraepithelial lesions (NILM) or any atypical cytology: atypical squamous cells of undetermined significance (ASC-US), low-grade squamous intraepithelial lesions (LSIL), and high-grade intraepithelial lesions (HSIL).
Ethical Statement
All participants signed written consent for testing in the clinical laboratory Synevo, where the established principles of medical ethics and Bulgarian legal requirements were described. The informed consent provided validates that the patient has adequate information about the nature, purpose, risks, benefits, and alternatives of HR-HPV PCR testing. After obtaining approval from the General Manager and Medical Manager of Synevo, we used the laboratory’s electronic database, which contains the data field for the included patients. The principles outlined in the Declaration of Helsinki were followed in this study.
Statistical Analysis
Statistical analysis was performed using the BrightStat.com software. Descriptive statistics, such as proportions, together with corresponding 95% confidence intervals (CI), had been calculated. The prevalence of HPV16, HPV18, and HPV45 genotypes, as well as other HR-HPV A (HPV31,33,52,58 genotypes) and HR-HPV B (HPV35,39,51,56,59,66,68) groups were assessed. Age data are presented as mean ± standard deviation and median. Age groups (15–20, 21–25, 26–30, 31–35, 36–40, 41-45, 46-50, 51-55, 56-60, 61-65) were categorized. The liquid-based cytology results were scored. The relationship between age groups, HPV infections, and liquid-based cytology results was investigated using the chi-square test or Fisher’s exact test. The settlement distribution of the collected HPV samples was visualized using paintmaps.com. Statistical significance was set at p < 0.05.
3. Results
3.1. The Prevalence of HR-HPV Infection
The study population used to evaluate the clinical performance of Alinity m was Bulgarian women aged between 15 and 64 years. A total of 190 Bulgarian women were included (n =190; mean and median age, 37.6 and 37.0 years, respectively). HR-HPV infection was detected in 32 of the 190 women screened, corresponding to an overall infection rate of 16.8% (95% CI: 11.8 to 22.9%, n=32) (Figure 1).
The HPV genotype distribution results obtained from the conducted study showed that 83.2% (95% CI: 77.1 to 88.2%, n=158) of the tested women were HR-HPV negative (Figure 2).
Infection with HPV16 could be seen in 5.3% (95% CI: 2.5 to 9.5%, n=10), HPV18 positive were 2.2% (95% CI: 0.6 to 5.3%, n=4) and genotype HPV45 was found in 1.0% (95% CI: 0.1 to 3.7%, n=2). Women positive for one or more HPV genotypes from group A and B were registered- 2.6% (95% CI: 0.8 to 6.3%, n=5) and 4.7% (95% CI: 2.2 to 8.8%, n=9), respectively. Two outpatients were found to be group A and group B HPV carriers- 1.0% (95% CI: 0.1 to 3.7%, n=2).
The most prevalent HR-HPV genotype in the HPV-positive, colposcopy group (n=32) was HPV16 – 31.2% (95% CI: 16.1 to 50.0%, n=10) (Figure 3).
The rate of HPV18 positive women was 12.5% (95%: 3.5 to 28.9%, n=4), HPV45 – 6.3% (95%: 0.7 to 20.8%, n=2), HR-HPV group A- 15.6% (95%: 5.2 to 32.8%, n=5), HR-HPV group B – 28.1% (95%: 13.7 to 46.7%, n=9) and infection with HPV genotypes from both A and B groups- 6.3% (95%: 0.7 to 20.8%, n=2). High-risk HPV16, HPV18, HPV45 accounted for 50.0% (95%: 31.9 to 68.1%, n=16) of all HPV genotypes tested. HR-HPV infection among colposcopy population from other groups A and B- 43.7% (95%: 26.4 to 62.3%, n=14) could be with single or multiple HPV genotypes.
3.2. Settlement Distribution of the HPV Samples
Cervical swab samples were taken by a gynecologist from different areas in Bulgaria, and majority of them-77.4% (95% CI: 70.7 to 83.1%, n=147) were from the three largest cities in the country–Sofia, Varna, and Plovdiv (Figure 4). The settlement distribution as per HPV specimens investigated in the study was evaluated as follows: Varna- 33.2% (95% CI: 26.5 to 40.3%, n=63); Plovdiv- 28.0% (95% CI: 21.6 to 34.8%, n=53); Sofia- 16.3% (95% CI: 11.4 to 22.5%, n=31); Stara Zagora- 8.4% (95% CI: 4.9 to 13.3%, n=16); Pazardjik- 6.8% (95% CI: 3.7 to 11.4%, n=13); Burgas- 3.2% (95% CI: 1.2 to 6.7%, n=6); Haskovo- 33.2% (95% CI: 0.8 to 6.0%, n=5); Dobrich- 1.0% (95% CI: 0.1 to 3.7%, n=2) and Blagoevgrad- 0.5% (95% CI: 0.01 to 2.9%, n=1).
3.3. The Prevalence of HR-HPV Infection in the Defined Age Groups
The distribution of HR-HPV among different age groups is shown in Table 1. According to the HPV PCR test results, the mean age of the patients was 38.2 (± 9.8) years in the HR-HPV positive group and 34.4 (± 9.9) years in the HR-HPV negative group. The women were divided into 10 age groups: 15–20; 21–25; 26–30; 31–35; 36–40; 41-45; 46-50; 51-55; 56-60 and 61-65 years old.
The majority of HR-HPV-positive results were recorded in women between 31 and 45 years- 56.0% (95%: 37.6 to 73.6%, n=18). Among them, the largest proportion of HPV (+) samples belonged to the 36-40 years old group, with a prevalence of HR-HPV infection of 20.5% (95%: 9.3 to 36.5%, n=8). The age group in second place was 31-35 years old, at 19.4% (95% CI: 8.2 to 36.0%, n=7). The majority of HPV16-positive samples were registered in the 36-40 years old group - 10.3% (95% CI: 2.8 to 24.2%, n=4). All of the HR-HPV group A together with group B positive results were found in the youngest age group: 15- 20 years of age-25,0% (95%: 3.2 to 65.1%, n=2). In addition, the cases were allocated into two age groups: ≤40 years and >40 years. No significant difference was found between the age groups in terms of HR-HPV positivity according to the chi-square test (p=0.6). It was observed that HPV infection rates decreased with increasing age, and HPV-positive results were not registered in the age group 56-50 years.
3.4. The prevalence of HR-HPV Infection and LBC Results
Histopathological examination was performed for all 190 samples (Table 2). Negative for intraepithelial lesion (NILM) results were defined in 81.0% (95%: 74.7 to 86.4%, n=154). Abnormalities in LBC cytology were observed in 18.9% (95%: 13.6 to 25.2%, n=36) of women.
Atypical squamous cells of undetermined significance 15.8% (95%: 10.9 to 21.7%, n=30) showed the highest frequency among abnormal cytology categories, followed by low-grade intraepithelial lesion (LSIL) 1.6% (95%: 0.3 to 4.5%, n=3), and high-grade intraepithelial lesion (HSIL) 1.6% (95%: 0.3 to 4.5%, n=3). With regard HPV genotype distribution according to cervical cytology, HPV16 was the most common genotype in cases with atypical squamous cells of undetermined significance- 20.0% (95%: 7.7 to 38.6%, n=6). Although HR-HPV positivity in normal cytology samples was 5.2% (95%: 2.3 to 9.9%, n=9), it was 63.9% (95%: 46.2 to 79.2%, n=23) in abnormal smear cytology results (p<0,00001).
4. Discussion
To construct an accurate regional map, we evaluated the prevalence of high-risk human papillomavirus (HR-HPV) using the clinically validated Alinity m HR-HPV Assay among women in Bulgaria’s general population. This initiative coincides with the commencement of the newly expanded “National Program for Primary Prevention of Cancer Diseases Caused by Human Papillomavirus 2025-2030” in Bulgaria. Notably, HR-HPV infection is highly prevalent in Bulgaria, with rates among women with normal cytology ranging from approximately 29.8% to 38.8% in large population-based studies. Persistent HPV infection is a primary cause of 99% of cervical cancer cases [24,25].
There are geographical variations in the overall prevalence of HR-HPV infection. Numerous studies have reported different findings regarding the prevalence and distribution of high-risk human papillomavirus types. We propose that these differences may be attributed to factors such as geographic location, study methodologies employed for HPV PCR detection, educational background of patients in healthcare settings, and their awareness of HPV infections. While the global HPV prevalence ranges from 11% to 12%, Africa exhibits the highest rate of 21.1%, followed by Europe at 14.2%, America at 11.5%, and Asia at 9.4%. Eastern Europe continues to report the highest rates of cervical cancer and HPV infection Europe [26]. The HPV epidemiological distribution in Eastern Europe is reported to be 21.4%, whereas in Western Europe, it is 9.0%, ranging from 2% in Spain to approximately 12% in France and Belgium. Poland has a prevalence of 14.4%, the Czech Republic 25.6%, and Lithuania 24.2% [27]. Data from a Latvian study indicated an overall HR-HPV prevalence of 11% in the general population [28]. In Greece, HPV prevalence ranges from 2.5% to 50.7%, whereas in Iran, it varies from 0.6% to 37.9% [1]. Studies from Turkey reported HR-HPV prevalence between 2.4% and 47.7% [29]. A study of 2234 Turkish women found an HPV positivity rate of 38.05%, with HPV 16 being the most common type [30]. In another Turkish study, at least one type of HR-HPV was identified in 9.17% of women [31]. Overall, the HPV-DNA positivity rate in Italy was 35.9% among women [32]. The HR-HPV positivity rate observed in this study aligns with worldwide statistics, with 16.8% of women testing positive for HR-HPV. A meta-analysis found that HPV DNA prevalence among women with normal cytology (ages 17–77) ranged from 5.3% to 35.6%, with a mean prevalence of 2.6% [33].
Globally, the five most prevalent HPV types among women are HPV-16, 18, 31, 58, and 52, collectively accounting for 50% of all HPV infections [34]. In all cases, HPV 16, 18, and 45 were the most common genotypes, and their proportions increased significantly in women with cervical cancer compared to women with normal cytology or low-grade cervical lesions. Research involving over 6,000 women diagnosed with CIN2 or invasive cervical cancer from 17 European countries identified HPV16, HPV18, and HPV45 as the most prevalent types in women with invasive cervical cancer, accounting for 63.3%, 15.2%, and 5.3%, respectively [35]. In this study, HPV16, HPV18, and HPV45 constituted 50% of all genotypes. HPV 16, 18, and 45 are associated with 75% of all squamous cell carcinomas and 94% of all adenocarcinomas, with HPV 45 alone responsible for 12% of all adenocarcinomas [36]. The overall prevalence of HPV16 is 2.8%, varying from 5.6% in Belgium and 10.6% in France to 1.0% in the Netherlands and 1.3% in Norway [27]. A study conducted on over 4,000 Slovenian women with normal cytology found HPV16 and HPV18 to be the most frequently detected HPV types, followed by HPV31, HPV39, HPV51, HPV52, and HPV59 [37]. In our study, the prevalence of HPV16 was found to be 5.3% in the general population and 31.2% in the HR-HPV positive group (colposcopy group), respectively. High-risk HPV16, HPV18, and HPV45 accounted for 50.0% of all HPV genotypes tested.
Bulgaria has a population of 3.06 million women aged 15 years and older, who are at risk of developing cervical cancer[38]. Current data suggest that each year, 1009 women are diagnosed with cervical cancer and 503 of them die from the disease. Cervical cancer screening coverage among women aged 20–69 was 57% in 2019 (lower than the EU average of 71% in the same year), but it has increased by 21% since 2008, when coverage was 47% [39]. A recent study conducted in Bulgaria from 2018 to 2020 that analyzed the economic impact of cervical cancer, the most common complication of sexually transmitted HPV infections, calculated the economic burden of HPV-related malignancies amounted to be 51.3 million euros. These findings indicate that nationwide actions are needed to reduce the ongoing consequences of neoplasms related to HPV [40]. The country has one of the highest rates of cervical cancer incidence and mortality within the European Union, with HPV16 and HPV18 identified in approximately 77% of invasive cervical carcinomas, followed by HPV56, HPV33, and HPV31. HPV16 is detected in approximately 13–17% of Bulgarian women in general population studies, a stark contrast to the distribution in the general population in Europe (2.8%), such as in Germany (2.5%) and France (3.9%). Among women with high-risk HPV infections, HPV16 was reported to be 46% [25]. The distribution of high-risk HPV has been consistently observed in extensive population-based studies of Bulgarian women with normal cytology, as well as in women with abnormal cytology and in high-risk groups, such as female sex workers [41,42].
Clinically validated HR-HPV tests, such as the Alinity m HR-HPV assay, may be valuable in enhancing patient risk stratification. Furthermore, Alinity provides extended genotyping beyond HPV16 and HPV18, which may be beneficial for improving the risk stratification of HR-HPV screen-positive women. We found HR-HPV infection among the colposcopy populations from other groups A and B to be 43.7%. These two groups included HPV56, HPV33, and HPV31, which is entirely consistent with the literature on Bulgaria. Moreover, women in groups A and B were infected with single or multiple HPV genotypes. Numerous molecular epidemiological and diagnostic studies have frequently reported co-infections with multiple high-risk HPV types, with some research suggesting that these co-infections may contribute to the progression of cervical neoplasia [19].
Reports indicate that HR-HPV prevalence is highest among adolescents and young adults and then declines with age, with regional differences in the extent and shape of the age curve. The decrease in HPV prevalence with increasing age can be attributed to fewer new sexual partners and acquired immunity. In women, HR-HPV prevalence typically peaks in those under 25 years old, with estimates around 16.9% in this group, then steadily declines after age 35 in most populations. In some regions, a second, smaller peak may occur in women over 55 years of age, but this varies according to location and sexual behavior patterns [43]. According to our test results, the average age of patients in the HR-HPV positive group was 38.2 (± 9.8) years, compared to 34.4 (± 9.9) years in the HR-HPV negative group. Most HR-HPV-positive results were found in women aged 31 to 45 (56,0%). Of these, The largest proportion of HPV (+) samples (20,5%) belonged to the 36-40-year-old group. The second most common age group was 31-35 years old (19.4%). The HPV16 genotype was most prevalent in the 36-40-year-old group, accounting for 10.3%. All results from HR-HPV groups A and B were found in the youngest age group of 15 to 20 years. Studies have reported no significant link between the risk of developing abnormal cervical cytology and increasing age. Similarly, this study found that increasing the age of HPV-positive women did not significantly increase the risk of high cervical cytology scores (0.6) [44]. We observed that HPV infection rates decreased with age and no HPV-positive results were recorded in women aged 56–50 years.
Population-based studies have elucidated the distribution of high-risk human papillomavirus genotypes within Bulgarian urban centers, with a primary focus on cities, such as Sofia, Plovdiv, Varna, Burgas, Pleven, and Vidin, as well as smaller communities [24,25]. Our research indicated that 77.4% of the female samples were derived from the three largest cities in Bulgaria—Sofia, Varna, and Plovdiv—with HPV16 consistently emerging as the most prevalent genotype. Genotyping high-risk HPV is crucial for evaluating the potential for cervical intraepithelial lesions and associated cancer risk. High-grade lesions and cancer demonstrate similar high-risk HPV genotype patterns, which are distinct from those observed in low-grade lesions and a normal cervix. The prevalence of HPV 16 serves as a significant indicator of cervical cancer risk [45].
In 2018, the World Health Organization (WHO) advocated for a global initiative to eliminate cervical cancer through prevention and early detection, which are recognized as highly cost-effective strategies. The WHO delineates three principal pillars for cervical cancer prevention: primary prevention via HPV vaccination ideally administered prior to the onset of sexual activity. In conjunction with vaccination, one of the strategic pillars is cervical cancer screening utilizing well-established and widely adopted methods such as traditional cytology (Pap smear), Liquid-Based Cytology, and molecular techniques for detecting the HR HPV virus. The WHO emphasizes that HPV-based screening offers superior protection against cervical cancer compared to cytology. For tertiary prevention, given the absence of a virus-specific treatment for HPV infection, precancerous lesions can be effectively managed through ablative methods (destroying abnormal tissue by burning or freezing) or excision, which provides an effective treatment for CIN [46].
The online Cervical Cancer Prevention Policy Atlas illustrates the progress made across Europe in the efforts to prevent cervical cancer. The third edition of the European HPV Prevention Policy Atlas offers current publicly accessible data on cervical cancer for all 48 countries in the European region. Developed by the European Parliamentary Forum on Sexual and Reproductive Rights and backed by the European Cancer Organization, the Atlas aligns with WHO’s strategy for eliminating cervical cancer and Europe’s Beating Cancer Plan. This map highlights HPV awareness levels, access to screening, vaccination, and information as well as the adoption and implementation of national policies for cervical cancer prevention. Each country’s details on these indicators are provided, along with an infographic display of the overall score and ranking for each European nation [47].
Efforts to reduce this cervical cancer burden in Bulgaria have included national vaccination campaigns and screening programs until 2017 with the “National Program for Primary Prevention of Cervical Cancer in the Republic of Bulgaria,” but coverage remains low and political instability has hindered consistent implementation. The first two HPV vaccines approved were Cervarix (bivalent) and Gardasil (quadrivalent), which cover the two most relevant HR-HPV types, 16 and 18. The nonavalent vaccine, Gardasil9, covers additional HR-HPV types 31, 33, 45, 52, and 58. Both quadrivalent and nonavalent vaccines also protect against LR-HPV types 6 and 11. Implementation of the new “National Program for Primary Prevention of Cancer Diseases Caused by Human Papillomavirus 2025-2030” aims to expand organized HPV screening and provide free immunization upon request to girls aged 10–18 years and boys aged 10–14 years. The program is a key element in efforts to reduce the incidence of HPV-related cancers, among which cervical cancer is the leading cancer[47]. The screening program also provides medical and diagnostic tests to establish infection with HPV from a cervical sample. The target group included women between the ages of 25 and 65, regardless of their health insurance status and family burden [48].Epidemiological studies indicate that these vaccine-covered genotypes are responsible for approximately 90% of cervical cancers and a similar percentage of other HPV-related anogenital and oropharyngeal cancers. Despite the availability of HPV vaccines against human papillomavirus, regular screening is crucial for prevention. The Alinity m HR-HPV assay with a channel that includes HPV31,33,52,58, along with the individual readings for HPV16, HPV18, and HPV45, encompasses all high-risk HPV genotypes covered by the nonavalent HPV vaccine, thereby providing an additional layer for risk assessment [49].
Until advancements in molecular methods, Pap smear was used for HPV screening. Recently, owing to the superior detection abilities and high negative predictive value of HPV testing compared to cytology, HPV testing has been implemented as a primary screening tool in the Netherlands, Turkey and Australia, while other counties are at different stages of transition or face challenges in program setup and coverage [50]. The PAP test, which was introduced in Bulgaria in 1974, has been used as a popular screening method, and every female, aged 30 – 40 years, has been entitled to such a test, which was regulated in the activities of general practitioners. The frequency of the prophylactic smear was annual for women between 30 and 40 years old, and if two negative results were obtained, the periodicity was changed to once every 3 years [51]. European guidelines recommend testing women aged 30–-years for HPV every five years or more, adjusting the ages and intervals based on individual risk factors and HPV vaccination history, and shifting from cytology-based screening to primary HPV-based screening, with self-sampling as an option to increase access and coverage [50]. The Human PapillomaVirus For Cervical Cancer (HPV FOCAL) Trial included 19,009 women and showed a significant difference in CIN3+ detection at 48 months (2.3/1000 for HPV testing vs. 5.5/1000 for cytology, p < 0.01), supporting HPV testing as a more sensitive primary screening tool [52]. Currently, Bulgaria is in a transition period from cytological-conventional and LBC screening to HPV DNA screening.
International guidance recommends a clinical validation strategy for novel HR-HPV DNA assays which involves a comparative analysis of samples from a population-based screening cohort using a clinically validated reference HPV assay. Although a large number of HPV assays are commercially available, only a few of them currently meet the criteria defined in the guidelines and can be viewed as clinically validated and reliable for use in primary screening for cervical cancer [53]. VALidation of HPV GENotyping tests was performed using VALGENT, a research framework for comparing and validating HPV tests designed for screening and genotyping according to international validation guidelines. In the study VALGENT-3, conducted with 1600 cervical samples, the clinical accuracy of the assay Alinity m HR HPV was assessed. Based on the results of this evaluation study Alinity fulfills international consensus guideline criteria for primary cervical cancer screening and can be considered clinically validated, demonstrating safety comparable to that of other clinically validated HPV tests [54]. The Alinity m high-risk HPV assay is considered to be indispensable for routine HPV screening, triage of patients with equivocal cytology, ensuring post-therapeutic follow-up, and monitoring vaccine efficacy [19,22].
Across multiple studies, HR-HPV prevalence was consistently higher in specimens with abnormal cytology than in those with normal cytology. The prevalence of high-risk human papillomavirus in cervical specimens with abnormal cytology varies widely depending on the degree of cytological abnormality, the population studied, and geographic region. Worldwide data show that HR-HPV prevalence 37–52% for ASC-US (atypical squamous cells of undetermined significance), in low-grade squamous intraepithelial lesion (LSIL)- 76–79% and in HSIL- 85% [55]. In a large study from China, HR-HPV prevalence was 41.8% in women with cervical cytological abnormalities versus 6.5% in those with normal cytology, with the highest rates observed in high-grade lesions and invasive squamous cell carcinoma (ISCC) [56]. Similarly, in a Turkish cohort, HPV was detected in 79.7% of abnormal cytology cases compared with 18.7% of normal cytology [57]. Studies from Thailand and Belgium reported HR-HPV prevalence in abnormal cytology ranging from 46.7% in atypical squamous cells to 80% in high-grade squamous intraepithelial lesions, and 34.5% in ASC-US to 54.3% in LSIL, respectively [58,59]. A study from 2014 on the prevalence of HPV and the distribution of the viral type in women with normal or abnormal Pap smears in Bulgaria demonstrated a high rate of HPV carriage – 61% of the 355 samples tested, with more than one HPV being found in 53 of the samples [42]. This finding correlates with the presented data in our study, where HR-HPV prevalence in the abnormal cytology smears was accounted for 63.9%. In the present study, atypical squamous cells of undetermined significance (15.8%) showed the highest frequency among abnormal cytology categories, followed by equally distributed LSIL and HSIL intraepithelial lesion – 1.6%. As regards HPV genotype distribution according to cervical cytology, HPV16 was the most common genotype in cases with atypical squamous cells of undetermined significance- 20.0%. Our results showed that although HR-HPV positivity in normal cytology samples was 5.2%, it was 63.9% in abnormal smear cytology samples (p<0.00001). According to the Bethesda system, patients diagnosed with low-grade squamous intraepithelial lesions or atypical squamous cells of uncertain malignant potential are recommended for further investigation, including colposcopy and biopsy, to exclude the presence of cervical intraepithelial neoplasia 2 [23].
5. Conclusions
The implementation of the “National Program for Primary Prevention of Cancer Diseases Caused by Human Papillomavirus 2025-2030” in Bulgaria is of paramount importance, as it directly addresses the country’s persistently high incidence and mortality rates of cervical cancer, which are among the highest in the European Union. This program aims to significantly reduce the burden of HPV-related cancers in Bulgaria by increasing vaccine uptake and screening rates, thereby preventing new cases and reducing both years of life lost and the economic costs associated with cervical cancer. The present study highlights that cervical cancer screening becomes more accessible with the use of the HPV PCR test, which boasts high sensitivity by detecting the presence of HPV in cervical cells, rather than identifying precancerous changes that might result from chronic infection. It is essential that this test be clinically validated and approved. The Alinity m HR-HPV assay is advised for use in population-based screening programs, as it reliably identifies at-risk women while minimizing false positives and unnecessary interventions. This high sensitivity of HPV testing reduces the risk of undetected disease and allows for extended intervals between screenings. The HR-HPV Alinity m platform provides evidence-based risk stratification for cervical cancer screening and offers several advantages in modern laboratory operations. Its random-access design, substantial capacity, cost-effectiveness, and simplified logistics management facilitate the execution of multiple PCR assays without requiring infrastructure modifications, thereby enabling rapid adaptation to the new guidelines.
Author Contributions
Conceptualization and writing—original draft preparation: D.T.T.-D; writing—review and editing: D.T.T.-D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
All study participants provided written informed consent prior to enrollment.
Data Availability Statement
The data that support the findings of this study are not freely available due to reasons of sensitivity and are available from corresponding author upon reasonable request. Data are located in controlled access data storage at Medical diagnostic laboratory “Synevo”, Bulgaria.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kombe Kombe, A. J.; Li, B.; Zahid, A.; Mengist, H. M.; Bounda, G.-A.; Zhou, Y.; Jin, T. Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front. Public Health 2021, 8 (Suppl 5). [Google Scholar] [CrossRef]
- Wang, W.; Sawleshwarkar, S.; Piraveenan, M. Computational Approaches of Modelling Human Papillomavirus Transmission and Prevention Strategies: A Systematic Review. Journal of Biological Dynamics 2025, 19(1). [Google Scholar] [CrossRef]
- Zerbini, F. M.; Crane, A.; Kuhn, J. H.; Simmonds, P.; Lefkowitz, E. J.; Adriaenssens, E. M. Summary of Taxonomy Changes Ratified by the International Committee on Taxonomy of Viruses (ICTV) – General Taxonomy Proposals, 2025. The Journal of General Virology 2025, 106(7). [Google Scholar] [CrossRef]
- Hanft, W.; Stankiewicz Karita, H.; Khorsandi, N.; Vohra, P.; Plotzker, R. Sexually Transmitted Human Papillomavirus and Related Sequelae. Clin Microbiol Rev 2025, 38(1). [Google Scholar] [CrossRef]
- Ouh, Y.-T.; Kim, H. Y.; Yi, K. W.; Lee, N.-W.; Kim, H.-J.; Min, K.-J. Enhancing Cervical Cancer Screening: Review of P16/Ki-67 Dual Staining as a Promising Triage Strategy. Mdpi Ag January 10 2024. [Google Scholar] [CrossRef]
- Einstein, M. H.; Schiller, J. T.; Viscidi, R. P.; Strickler, H. D.; Coursaget, P.; Tan, T.; Halsey, N.; Jenkins, D. Clinician’s Guide to Human Papillomavirus Immunology: Knowns and Unknowns. The Lancet Infectious Diseases 2009, 9(6), 347–356. [Google Scholar] [CrossRef] [PubMed]
- Galati, L.; Chiantore, M. V.; Marinaro, M.; Di Bonito, P. Human Oncogenic Viruses: Characteristics and Prevention Strategies-Lessons Learned from Human Papillomaviruses. Viruses 2024, 16(3), 416. [Google Scholar] [CrossRef] [PubMed]
- Lipsick, J. A History of Cancer Research: Tumor Viruses. Cold Spring Harb Perspect Biol 2021, 13(6), a035774. [Google Scholar] [CrossRef] [PubMed]
- Kusakabe, M.; Taguchi, A.; Sone, K.; Mori, M.; Osuga, Y. Carcinogenesis and Management of Human Papillomavirus-Associated Cervical Cancer. Int J Clin Oncol 2023, 28(8), 965–974. [Google Scholar] [CrossRef]
- Karaoğlan, B. B.; Ürün, Y. Unveiling the Role of Human Papillomavirus in Urogenital Carcinogenesis a Comprehensive Review. Viruses 2024, 16(5), 667. [Google Scholar] [CrossRef]
- Gu, Y.; Li, T.; Zhang, M.; Chen, J.; Shen, F.; Ding, J.; Zhou, G.; Hua, K. The Display between HPV Infection and Host Immunity in Cervical Cancer. Front. Biosci. (Landmark Ed) 2024, 29(12). [Google Scholar] [CrossRef] [PubMed]
- De Sanjosé, S.; Serrano, B.; Tous, S.; Alejo, M.; Lloveras, B.; Quirós, B.; Clavero, O.; Vidal, A.; Ferrándiz-Pulido, C.; Pavón, M. Á.; Holzinger, D.; Halec, G.; Tommasino, M.; Quint, W.; Pawlita, M.; Muñoz, N.; Bosch, F. X.; Alemany, L.; Kulkarni, A. Burden of Human Papillomavirus (HPV)-Related Cancers Attributable to HPVs 6/11/16/18/31/33/45/52 and 58. JNCI cancer spectrum 2018, 2(4). [Google Scholar] [CrossRef] [PubMed]
- Franco, E. L.; Schlecht, N. F.; Saslow, D. The Epidemiology of Cervical Cancer. The Cancer Journal 2003, 9(5), 348–359. [Google Scholar] [CrossRef] [PubMed]
- Ntuli, L.; Mtshali, A.; Mzobe, G.; Liebenberg, L. J.; Ngcapu, S. Role of Immunity and Vaginal Microbiome in Clearance and Persistence of Human Papillomavirus Infection. Front. Cell. Infect. Microbiol. 2022, 12(1). [Google Scholar] [CrossRef]
- Cangelosi, G.; Sacchini, F.; Mancin, S.; Petrelli, F.; Amendola, A.; Fappani, C.; Sguanci, M.; Morales Palomares, S.; Gravante, F.; Caggianelli, G. Papillomavirus Vaccination Programs and Knowledge Gaps as Barriers to Implementation: A Systematic Review. Vaccines 2025, 13(5), 460. [Google Scholar] [CrossRef]
- Fashedemi, O. O.; Ozoemena, O. C.; Peteni, S.; Haruna, A. B.; Shai, L. J. J.; Chen, A.; Rawson, F. J.; Cruickshank, M. E.; Grant, D. M.; Ola, O.; Ozoemena, K. I. Advances in Human Papillomavirus Detection for Cervical Cancer Screening and Diagnosis: Challenges of Conventional Methods and Opportunities for Emergent Tools. Anal. Methods 2025, 17(7), 1428–1450. [Google Scholar] [CrossRef]
- Blanco, R.; Muñoz, J. P. Molecular Insights into HR-HPV and HCMV Co-Presence in Cervical Cancer Development. Cancers 2025, 17(4), 582. [Google Scholar] [CrossRef]
- Organization, W. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention; World Health Organization, 2024. [Google Scholar] [CrossRef]
- Goldstein, D. Y.; Yang, T.; Lucic, D.; Zhang, Y.; Cullum, R.; Kostera, J.; Patel, A. Multi-Center Evaluation of the Alinity m HR HPV Assay with Liquid-Based Cytology Cervical Specimens in the United States. Microbiol Spectr 2025, 13(3). [Google Scholar] [CrossRef]
- Banerjee, D.; Mittal, S.; Mandal, R.; Basu, P. Screening Technologies for Cervical Cancer: Overview. Cytojournal 2022, 19 (Suppl 11), 23. [Google Scholar] [CrossRef]
- Martinelli, M.; Giubbi, C.; Di Meo, M. L.; Perdoni, F.; Musumeci, R.; Leone, B. E.; Fruscio, R.; Landoni, F.; Cocuzza, C. E. Accuracy of Human Papillomavirus (HPV) Testing on Urine and Vaginal Self-Samples Compared to Clinician-Collected Cervical Sample in Women Referred to Colposcopy. Viruses 2023, 15(9), 1889. [Google Scholar] [CrossRef]
- Huang, S.; Gentil, L. G.; Schmidt, C.; Cullum, R.; Zhang, Y.; Nelson, K.; Lucic, D.; Abravaya, K. Comparative Clinical Performance of Alinity m HR HPV, Cobas 4800 HPV, and Cobas 6800 HPV for Cervical Cancer Screening. Microbiol Spectr 2025, 13(9). [Google Scholar] [CrossRef] [PubMed]
- Nayar, R.; Wilbur, D. C. The Bethesda System for Reporting Cervical Cytology: A Historical Perspective. Acta Cytologica 2017, 61(4–5), 359–372. [Google Scholar] [CrossRef] [PubMed]
- Kovachev, S.; Slavov, V.; Slavova, K. Prevalence of Human Papillomavirus Infection in Women in Some Cities and Regions of Bulgaria. Journal of Medical Virology 2013, 85(9), 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Kovachev, S.; Slavov, V. Prevalence of Human Papillomavirus Infection in Women in Bulgaria: A 2017 Update. Journal of Medical Virology 2018, 90(6), 1142–1149. [Google Scholar] [CrossRef]
- Yordanov, A.; Vasileva-Slaveva, M.; Galai, N.; Faraggi, D.; Kubelac, M. P.; Tripac-Iacovleva, I.; Calleja, N.; Di Fiore, R.; Calleja-Agius, J. Cancer of the Cervix in Bulgaria: Epidemiology of a Crisis. Healthcare 2023, 11(3), 318. [Google Scholar] [CrossRef]
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F. X.; De Sanjosé, S. Cervical Human Papillomavirus Prevalence in 5 Continents: Meta-Analysis of 1 Million Women with Normal Cytological Findings. J INFECT DIS 2010, 202(12), 1789–1799. [Google Scholar] [CrossRef]
- Berza, N.; Zodzika, J.; Kivite-Urtane, A.; Baltzer, N.; Curkste, A.; Pole, I.; Nygård, M.; Pärna, K.; Stankunas, M.; Tisler, A.; Uuskula, A. Understanding the High-Risk Human Papillomavirus Prevalence and Associated Factors in the European Country with a High Incidence of Cervical Cancer. European journal of public health 2024, 34(4), 826–832. [Google Scholar] [CrossRef]
- Eroglu, S.; Asgin, N. Frequency and Genotype Distribution of High-Risk Human Papilloma Virus Types in Karabuk Province, Turkey: A Hospital Based Cross-Sectional Study. Ann Med Res 2020, 27(2), 765. [Google Scholar] [CrossRef]
- Hancer, V.; Buyukdogan, M.; Bylykbashi, I.; Oksuz, B.; Acar, M. Prevalence of Human Papilloma Virus Types in Turkish and Albanian Women. J Cytol 2018, 35(4), 252. [Google Scholar] [CrossRef]
- Taskin, M.; Nursal, A.; Oruc, M.; Kariptas, E. Genotype Distribution and Prevalence of High-Risk Human Papillomavirus Infection among Women in Samsun Province of Turkey. Asian Pac J Cancer Prev 2022, 23(7), 2477–2482. [Google Scholar] [CrossRef]
- Piana, A.; Sotgiu, G.; Castiglia, P.; Pischedda, S.; Cocuzza, C.; Capobianco, G.; Marras, V.; Dessole, S.; Muresu, E. Prevalence and Type Distribution of Human Papillomavirus Infection in Women from North Sardinia, Italy. BMC Public Health 2011, 11(1). [Google Scholar] [CrossRef] [PubMed]
- Bergman, H.; Henschke, N.; Villanueva, G.; Loke, Y. K.; Golder, S. P.; Dwan, K.; Crosbie, E. J.; Kyrgiou, M.; Platt, J.; Morrison, J. Human Papillomavirus (HPV) Vaccination for the Prevention of Cervical Cancer and Other HPV-Related Diseases: A Network Meta-Analysis. Cochrane Database of Systematic Reviews 2022, 2022(5). [Google Scholar] [CrossRef]
- Glinska, P.; Macios, A.; Jaworski, R.; Bobinski, M.; Pruski, D.; Przybylski, M.; Zielinska, A.; Sawicki, W.; Nowakowski, A. Baseline Data on Distribution of Human Papillomavirus (HPV) Genotypes in Cervical Samples of Gynecological Patients before Implementation of Population-Based HPV Vaccination Program in Poland. Ginekol Pol 2024, 95(11), 870–878. [Google Scholar] [CrossRef] [PubMed]
- Elfstrom, K. M.; Smelov, V.; Johansson, A. L. V.; Eklund, C.; Naucler, P.; Arnheim-Dahlstrom, L.; Dillner, J. Long Term Duration of Protective Effect for HPV Negative Women: Follow-up of Primary HPV Screening Randomised Controlled Trial. BMJ 2014, 348, g130. [Google Scholar] [CrossRef]
- Holl, K.; Nowakowski, A. M.; Powell, N.; Mccluggage, W. G.; Pirog, E. C.; Collas De Souza, S.; Tjalma, W. A.; Rosenlund, M.; Fiander, A.; Castro Sánchez, M.; Damaskou, V.; Joura, E. A.; Kirschner, B.; Koiss, R.; O’Leary, J.; Quint, W.; Reich, O.; Torné, A.; Wells, M.; Rob, L.; Kolomiets, L.; Molijn, A.; Savicheva, A.; Shipitsyna, E.; Rosillon, D.; Jenkins, D. Human Papillomavirus Prevalence and Type-distribution in Cervical Glandular Neoplasias: Results from a European Multinational Epidemiological Study. Intl Journal of Cancer 2015, 137(12), 2858–2868. [Google Scholar] [CrossRef]
- Učakar, V.; Poljak, M.; Oštrbenk, A.; Klavs, I. Pre-Vaccination Prevalence of Infections with 25 Non-High-Risk Human Papillomavirus Types among 1,000 Slovenian Women in Cervical Cancer Screening. J. Med. Virol. 2014, 86(10), 1772–1779. [Google Scholar] [CrossRef]
- Merdzhanova-Gargova, Y.; Ivanova, M.; Mollova-Kysebekirova, A.; Mihaylova, A.; Parahuleva-Rogacheva, N.; Uchikova, E.; Koleva-Ivanova, M. Advancements in Cervical Cancer Screening: Enhancing HPV Testing and Triage Strategies for Improved Risk Assessment. Biomedicines 2025, 13(7), 1768. [Google Scholar] [CrossRef]
- Oecd, O. Beating Cancer Inequalities: Current Trends and Key Policy Directions. In Organisation for Economic Cooperation Development; 2024. [Google Scholar] [CrossRef]
- Lebanova, H.; Stoev, S.; Naseva, E.; Getova, V.; Wang, W.; Sabale, U.; Petrova, E. Economic Burden of Cervical Cancer in Bulgaria. IJERPH 2023, 20(3), 2746. [Google Scholar] [CrossRef]
- Shikova, E.; Todorova, I.; Ganchev, G.; Kouseva-Dragneva, V.; Kalascheva-Zaimova, P. Prevalence of Human Papillomavirus Infection among Female Sex Workers in Bulgaria. Int J STD AIDS 2011, 22(5), 278–280. [Google Scholar] [CrossRef]
- Grozdanov, P.; Zlatkov, V.; Ganchev, G.; Karagiosov, I.; Toncheva, D.; Galabov, A. S. HPV Prevalence and Type Distribution in Women with Normal or Abnormal Pap Smear in Bulgaria. Journal of Medical Virology 2014, 86(11), 1905–1910. [Google Scholar] [CrossRef]
- Rahangdale, L.; Mungo, C.; O’Connor, S.; Chibwesha, C. J.; Brewer, N. T. Human Papillomavirus Vaccination and Cervical Cancer Risk. BMJ 2022, 379, e070115. [Google Scholar] [CrossRef] [PubMed]
- Spinillo, A.; Dal Bello, B.; Gardella, B.; Roccio, M.; Dacco’, M. D.; Silini, E. M. Multiple Human Papillomavirus Infection and High Grade Cervical Intraepithelial Neoplasia among Women with Cytological Diagnosis of Atypical Squamous Cells of Undetermined Significance or Low Grade Squamous Intraepithelial Lesions. Gynecologic Oncology 2009, 113(1), 115–119. [Google Scholar] [CrossRef] [PubMed]
- Luu, X. Q.; Jun, J. K.; Suh, M.; Oh, J.-K.; Yu, S.-Y.; Choi, K. S. Cervical Cancer Screening, HPV Vaccination, and Cervical Cancer Elimination. JAMA Network Open 2025, 8(8). [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhao, F. H.; Hu, S. Y.; Zhao, X. L.; Qiao, Y. L. Interpretation of WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, Second Edition. Zhonghua yi xue za zhi 2021, 101(34). [Google Scholar] [CrossRef]
- Zhou, L.; Li, Y.; Wang, H.; Qin, R.; Han, Z.; Li, R. Global Cervical Cancer Elimination: Quantifying the Status, Progress, and Gaps. BMC Med 2025, 23(1). [Google Scholar] [CrossRef]
- Todorova, I.; Panayotova, Y.; Kotzeva, T.; Greenley, R.; Mckee, M.; Consortium, C.-S. Cervical Cancer in Bulgaria since EU Accession in 2007: A Struggle in the Face of Political Instability. Health Policy 2026, 164, 105497. [Google Scholar] [CrossRef]
- Oštrbenk Valenčak, A.; Šterbenc, A.; Seme, K.; Poljak, M. Alinity m HR HPV Assay Fulfills Criteria for Human Papillomavirus Test Requirements in Cervical Cancer Screening Settings. J Clin Microbiol 2019, 58(1). [Google Scholar] [CrossRef]
- Marta, P. J.; Smick, A.; Kaur, J.; Beavis, A.; Holschneider, C. Implementation of Primary HPV-Based Cervical Cancer Screening across a Countywide Health System. Gynecologic Oncology Reports 2025, 60. [Google Scholar] [CrossRef]
- Hinkova, N.; Semova, T.; Dimitrov, D.; Vasileva, M.; Racheva, V.; Gorcheva, Z. HPV-Associated Diseases and Their Cytodiagnosis. Acta Medica Bulgarica 2025, 52(2), 30–37. [Google Scholar] [CrossRef]
- Ogilvie, G. S.; Van Niekerk, D.; Krajden, M.; Smith, L. W.; Cook, D.; Gondara, L.; Ceballos, K.; Quinlan, D.; Lee, M.; Martin, R. E.; Gentile, L.; Peacock, S.; Stuart, G. C. E.; Franco, E. L.; Coldman, A. J. Effect of Screening With Primary Cervical HPV Testing vs Cytology Testing on High-Grade Cervical Intraepithelial Neoplasia at 48 Months. JAMA 2018, 320(1), 43. [Google Scholar] [CrossRef]
- Meijer, C. J. L. M.; Berkhof, J.; Castle, P. E.; Hesselink, A. T.; Franco, E. L.; Ronco, G.; Arbyn, M.; Bosch, F. X.; Cuzick, J.; Dillner, J.; Heideman, D. A. M.; Snijders, P. J. F. Guidelines for Human Papillomavirus DNA Test Requirements for Primary Cervical Cancer Screening in Women 30 Years and Older. Intl Journal of Cancer 2008, 124(3), 516–520. [Google Scholar] [CrossRef]
- Dhillon, S. K.; Oštrbenk Valenčak, A.; Xu, L.; Poljak, M.; Arbyn, M. Clinical and Analytical Evaluation of the Alinity m HR HPV Assay within the VALGENT-3 Framework. J Clin Microbiol 2021, 59(6). [Google Scholar] [CrossRef]
- Clarke, M. A.; Risley, C.; Stewart, M. W.; Geisinger, K. R.; Hiser, L. M.; Morgan, J. C.; Owens, K. J.; Ayyalasomayajula, K.; Rives, R. M.; Jannela, A.; Grunes, D. E.; Zhang, L.; Schiffman, M.; Wagner, S.; Boland, J.; Bass, S.; Wentzensen, N. Age-specific Prevalence of Human Papillomavirus and Abnormal Cytology at Baseline in a Diverse Statewide Prospective Cohort of Individuals Undergoing Cervical Cancer Screening in Mississippi. Cancer Medicine 2021, 10(23), 8641–8650. [Google Scholar] [CrossRef]
- Song, L.; Lyu, Y.; Ding, L.; Li, X.; Gao, W.; Wang, M.; Hao, M.; Wang, Z.; Wang, J. Prevalence and Genotype Distribution of High-Risk Human Papillomavirus Infection in Women with Abnormal Cervical Cytology: A Population-Based Study in Shanxi Province, China. CMAR 2020, 12 (Suppl 5), 12583–12591. [Google Scholar] [CrossRef]
- Seneldir, H.; Kir, G. Prevalence of High-Risk Human Papilloma Virus in Liquid-Based Cervical Samples from Turkish Women with Normal and Abnormal Cytology. Diagnostic Cytopathology 2018, 47(2), 100–104. [Google Scholar] [CrossRef]
- Laowahutanont, P.; Karalak, A.; Wongsena, M.; Loonprom, K.; Pukcharoen, P.; Jamsri, P.; Sangrajrang, S. Prevalence of High Risk Human Papillomavirus Infection with Different Cervical Cytological Features among Women Undergoing Health Examination at the National Cancer Institute, Thailand. Asian Pacific Journal of Cancer Prevention 2014, 15(14), 5879–5882. [Google Scholar] [CrossRef]
- Weyn, C.; Garbar, C.; Noël, J.-C.; Weynand, B.; Verhest, A.; D’Olne, D.; Arbyn, M.; Englert, Y.; Fontaine, V. Inter-Laboratory Variability in the Presence of Human Papillomavirus in Normal and Abnormal Cervical Cytology Samples. Cancer Epidemiology 2013, 37(4), 457–461. [Google Scholar] [CrossRef]
Figure 1.
The prevalence of HPV from common Bulgarian population.
Figure 2.
High-risk HPV genotype distribution in the studied cohort (n=190).
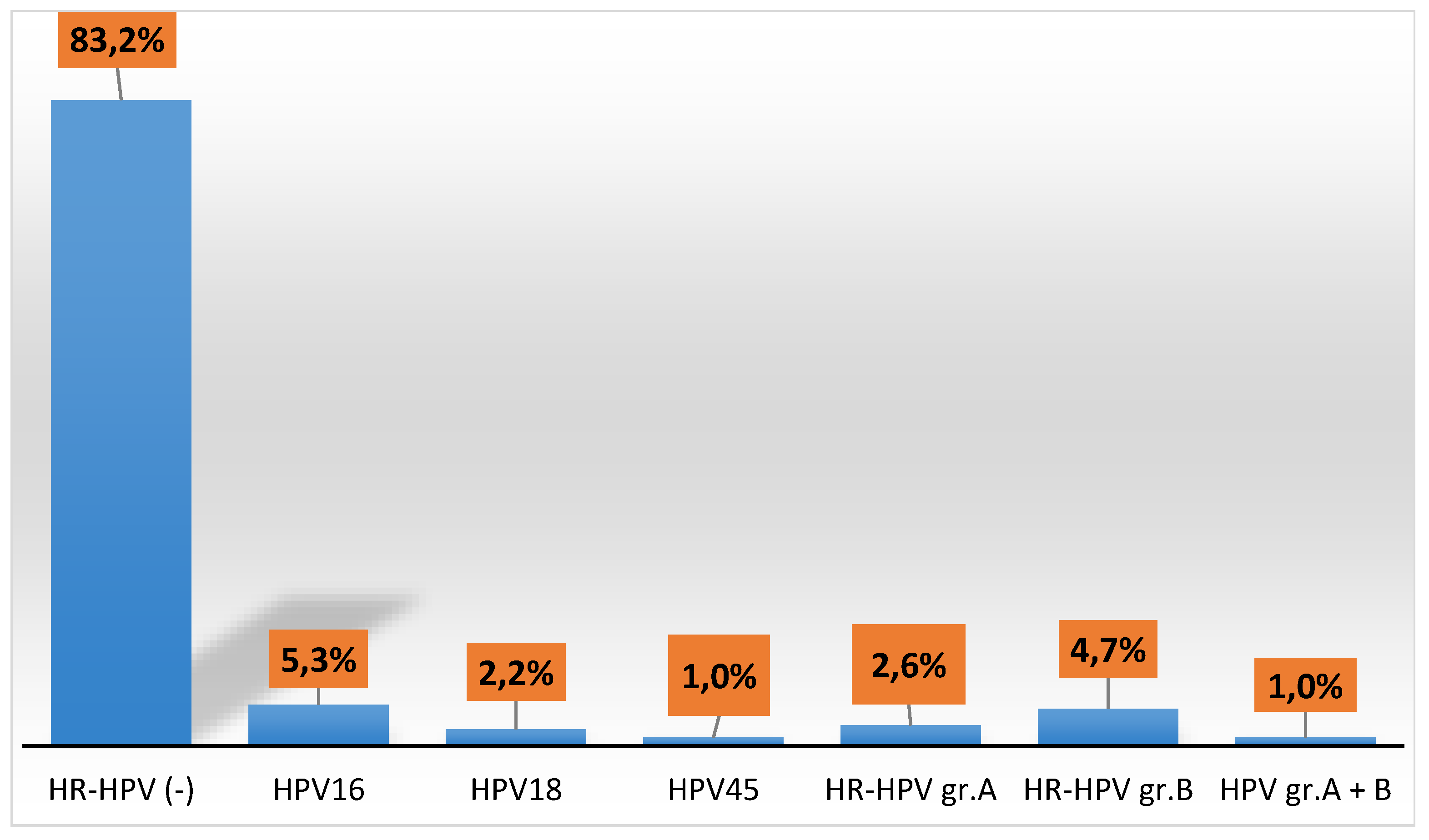
Figure 3.
HR-HPV genotype prevalence in the studied HPV-positive group (n=32).
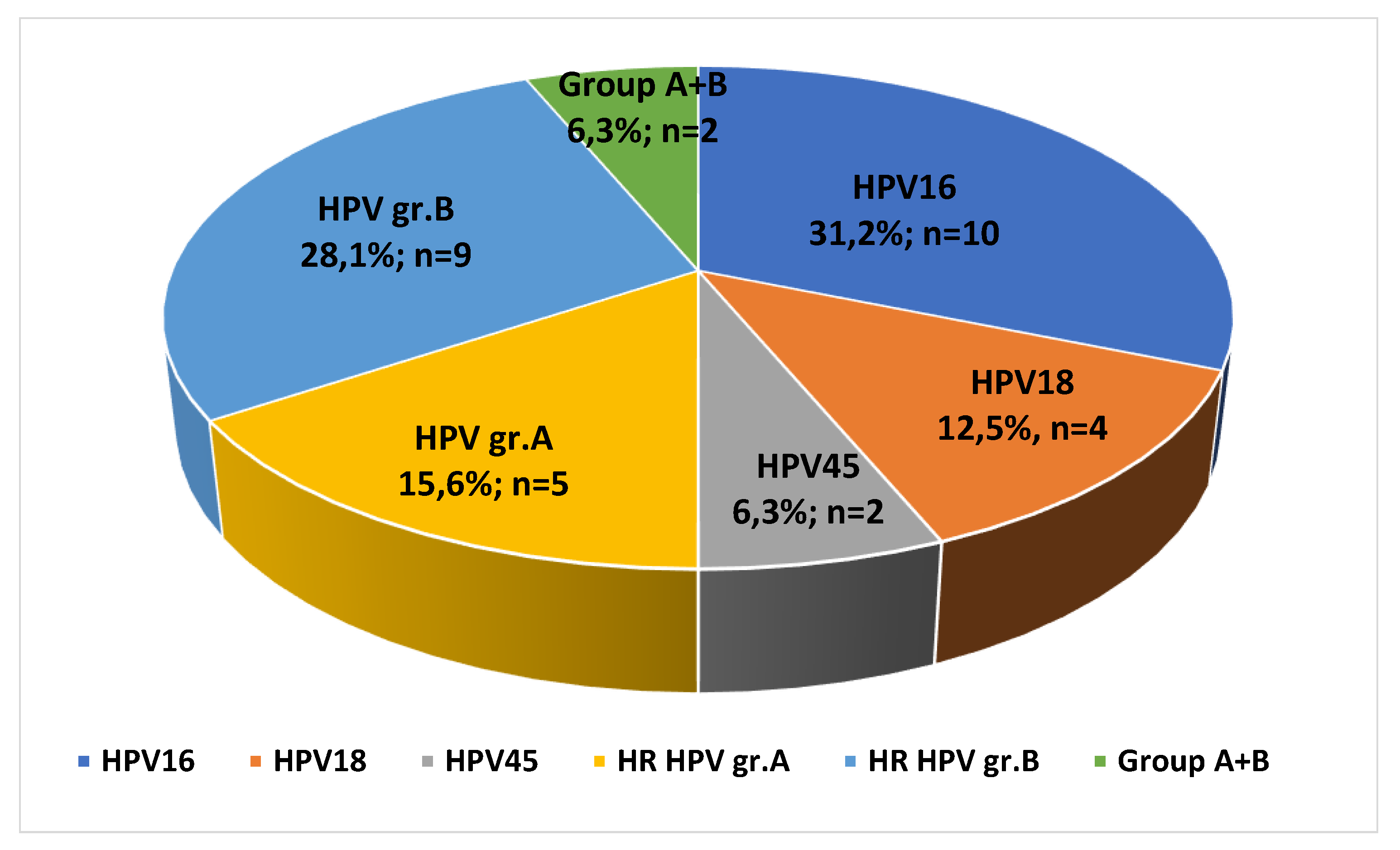
Figure 4.
HPV samples obtained across Bulgaria.
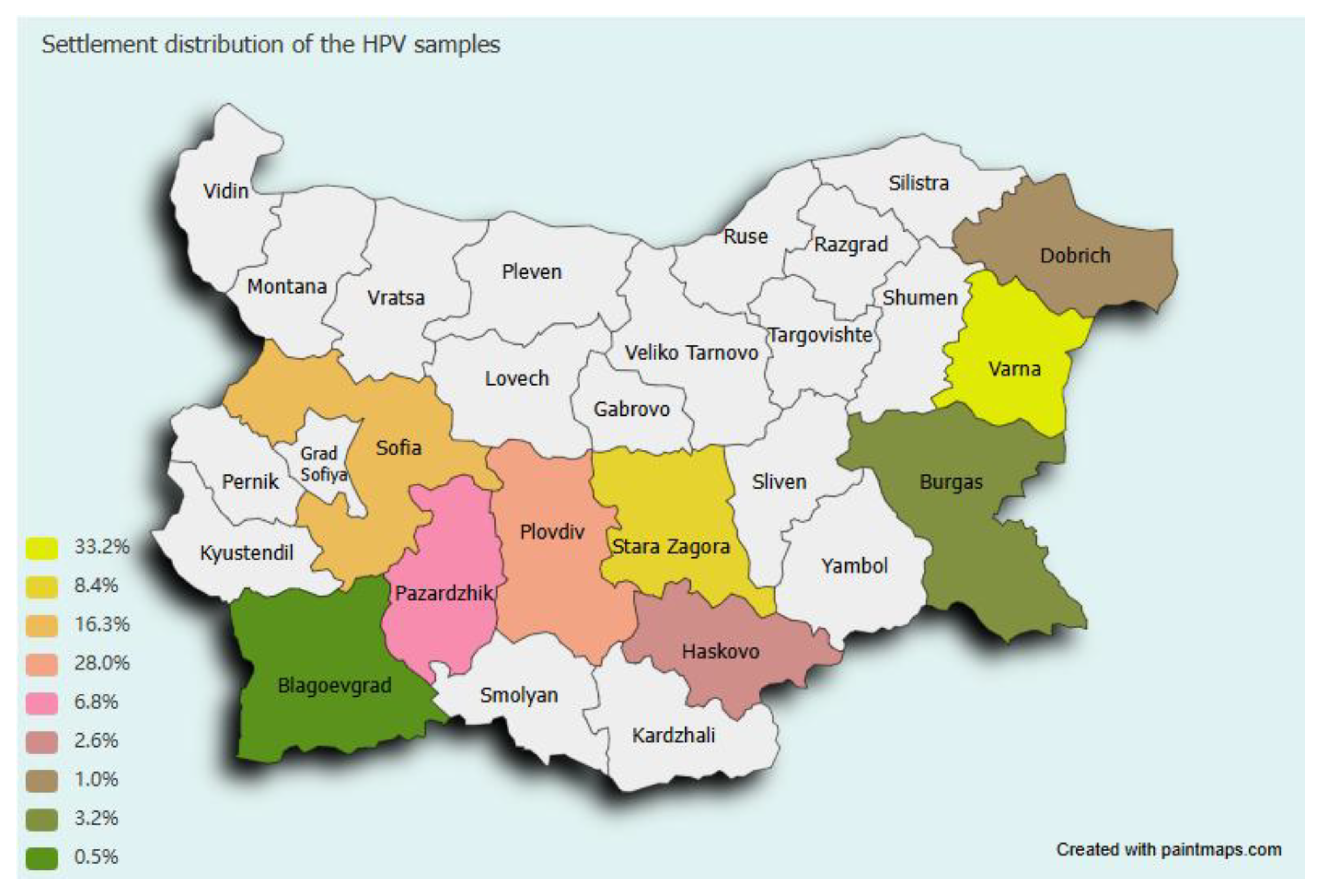

Table 1.
The overall prevalence of HR-HPV among the age groups.
| Age group | 15-20 | 21-25 | 26-30 | 31-35 | 36-40 | 41-45 | 46-50 | 51-55 | 56-60 | 61-65 | Total | |
| n(%) n(%) n(%) n(%) n(%) n(%) n(%) n(%) n(%) n(%) | n(%) | |||||||||||
| Samples | 8(4,2) | 14(7,4) | 24(12,6) | 36(18,9) | 39(20,5) | 26(13,7) | 22(11,6) | 12(6,3) | 7(3,7) | 2(1,1) | 190(100) | |
|
HR-HPV infection |
4(50) |
3(21,4) |
3(12,5) | 7(19,4) |
8(20,5) | 3(11,5) | 2(9,1) |
1(8,3) |
0(0) |
1(50) |
32(16,8) |
|
| HR-HPV genotypes | ||||||||||||
| HPV16 | 0(0) | 1(7,1) | 1(4,2) | 3(8,3) | 4(10,3) | 1(3,8) | 0(0) | 0(0) | 0(0) | 0(0) | 10(31,2) | |
| HPV18 | 1(12,5) | 0(0) | 0(0) | 0(0) | 1(2,6) | 1(3,8) | 0(0) | 1(8,3) | 0(0) | 0(0) | 4(12,5) | |
| HPV45 | 0(0) | 0(0) | 0(0) | 1(2,8) | 1(2,6) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 2(6,3) | |
| group A | 0(0) | 0(0) | 1(4,2) | 0(0) | 1(2,6) | 0(0) | 2(9,1) | 0(0) | 0(0) | 1(50) | 5(15,6) | |
| group B | 1(12,5) | 2(14,3) | 1(4,2) | 3(8,3) | 1(2,6) | 1(3,8) | 0(0) | 0(0) | 0(00 | 0(0) | 9(28,1) | |
| group A+B | 2(25,0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 0(00 | 0(0) | 0(0) | 2(6,3) | |
Table 2.
Bethesda system report of HR-HPV genotypes according to liquid-based cytology results.
|
HR-HPV (-) n(%) |
HPV16 n(%) |
HPV18 n(%) |
HPV45 n(%) |
HR-HPV group A n(%) |
HR-HPV group B n(%) |
HR-HPV groups A+B n(%) |
Total n(%) |
|
|
NILM n(%) |
145 (91,7%) |
2 (20%) |
3 (75%) |
1 50%) |
2 (40%) |
1 (11,1%) |
0(0%) |
154 (81,0%) |
|
ASC-US n(%) |
13 (8,3%) |
6 (60%) |
1 (25%) |
1 (50%) |
3 (60%) |
5 (55,6%) |
1 (50%) |
30 (15,8%) |
|
LSIL n(%) |
0(0%) |
1 (10%) |
0(0%) | 0(0%) | 0(0%) |
2 (22,2%) |
0(0%) |
3 (1,6%) |
|
HSIL n(%) |
0(0%) |
1 (10%) |
0(0%) | 0(0%) | 0(0%) |
1 (11,1%) |
1 (50%) |
3 (1,6%) |
|
Total n(%) |
158 (83,2%) |
10 (5,3%) |
4 (2,1%) |
2 (1,0%) |
5 (2,6%) |
9 (4,7%) |
2 (1,0%) |
190 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



