Submitted:
11 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
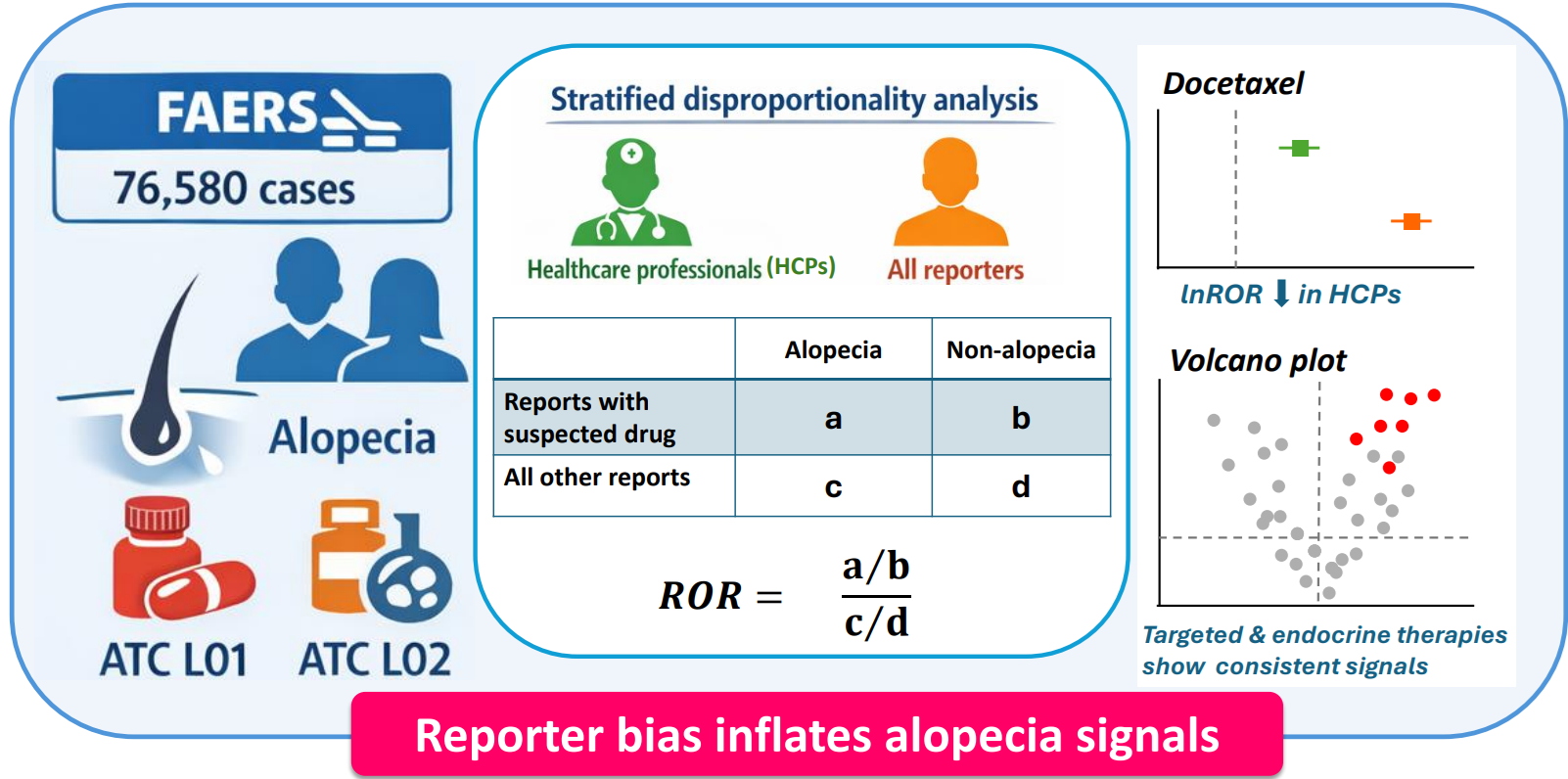
Background/Objectives: Cancer therapy–induced alopecia (CTIA) profoundly affects patients’ quality of life. This study conducted a disproportionality analysis of CTIA using the FDA Adverse Event Reporting System (FAERS) database to provide an overview of drug-specific signal distributions by systematically evaluating the impact of reporter type on CTIA signal detection. Methods: FAERS data from January 2004 to September 2024 were analyzed to extract alopecia-related Preferred Terms included under the Medical Dictionary for Regulatory Activities High Level Term “Alopecias.” Reporting odds ratios (RORs) were calculated to assess disproportionality. A primary analysis including all reports and a stratified analysis restricted to reports submitted by healthcare professionals (HCPs) were performed. No individual case-level clinical review was conducted. Results: Approximately 90% of alopecia reports were associated with female patients, and approximately 40% of these reports were linked to breast cancer. In the disproportionality analysis including all reporters, the highest ROR [95% confidence interval (CI)] was observed for docetaxel [58.31 (57.46–59.17)]. In the analysis restricted to HCP reports, the highest ROR was observed for vismodegib [23.92 (21.86–26.17)], whereas that for docetaxel markedly decreased to 3.68 (3.48–3.89). For molecular targeted agents, statistically significant signals were maintained even in the HCP-restricted analysis. Conclusions: Reporter characteristics substantially influence the detection of alopecia signals, with patients amplifying signals reflecting psychological harm and HCPs amplifying signals reflecting pharmacological plausibility. These findings should be interpreted as hypothesis-generating and warrant further validation using prospective or clinical datasets.
Keywords:
FAERS
; disproportionality analysis
; alopecia
; reporter bias
; healthcare professional stratification
; reporting odds ratio
; hypothesis-generating study
1. Introduction
Changes in physical appearance associated with cancer treatment, particularly alopecia, profoundly affect patients’ self-perception, interpersonal relationships, and health-related quality of life (HRQoL) [1,2,3]. Hair both symbolizes health status and reflects social roles and cultural identity, making hair loss a major source of psychosocial stress [1,2,3].
Alopecia associated with cancer therapy is classically categorized into acute, extensive hair loss caused by cytotoxic chemotherapy [chemotherapy-induced alopecia (CIA)] [4], and chronic diffuse alopecia resulting from alterations in the hormonal milieu [endocrine therapy–induced alopecia (EIA)] [5]. In recent years, characteristic alopecia patterns associated with molecular targeted therapies and immunotherapies have been reported [6], highlighting drug-specific manifestations of hair loss.
Advances in cancer treatment have led to prolonged survival; thus, patients can experience long-term treatment-related adverse effects even after achieving remission. Although alopecia does not directly affect survival, it has been suggested to reduce patients’ willingness to continue treatment and impair adherence [3], and it is increasingly recognized as a clinically relevant issue that might influence long-term treatment outcomes. However, alopecia deemed mild or predictable is often insufficiently captured in clinical trials, making it difficult to comprehensively assess its occurrence and characteristics in real-world clinical practice.
Spontaneous reporting systems (SRSs) represent valuable resources for comprehensively collecting safety information for drugs, and they provide complementary findings to clinical trials by capturing rare adverse events or symptoms that are difficult to detect in controlled settings. Nevertheless, SRS data are inherently susceptible to reporting bias, as reporting depends on the characteristics and motivations of reporters. Consequently, mild or expected adverse events tend to be underreported [7,8,9]. Moreover, adverse events related to HRQoL are frequently reported by patients but less frequently reported by healthcare professionals (HCPs) [10,11,12].
Against this background, the present study evaluated signals of cancer therapy–induced alopecia associated with antineoplastic and endocrine therapies using an exploratory, hypothesis-generating disproportionality analysis based on the FDA Adverse Event Reporting System (FAERS). In addition, we quantitatively assessed the impact of reporter type (HCPs vs. non-HCPs) on reporting odds ratios (RORs). Signal patterns across drug classes were further visualized using volcano plots, and integrated interpretations were attempted from both pharmacological and reporting bias perspectives. Given the exploratory and hypothesis-generating nature of this study, analyses were conducted under the hypothesis that restricting reports to those submitted by HCPs would result in lower RORs for appearance-related, HRQoL-associated adverse events than analyses including all reports.
2. Materials and Methods
2.1. Data Source and Study Period
This study utilized FAERS, a spontaneous reporting database maintained by the US FDA. Reports submitted between January 2004 and September 2024 (October 2024 data release) were included in the analysis [13]. Data curation, including coding, mapping, and data cleaning, was conducted by ArkMS Inc. (https://www.arkms.co.jp/; accessed November 30, 2025). This process included normalization of drug names registered in FAERS (standardization to generic names and consolidation of synonyms and spelling variants) and assignment of Anatomical Therapeutic Chemical (ATC) codes to each drug.
2.2. Terminology for Target Drugs and Adverse Events
Drug classes were defined using the ATC Classification System developed by the WHO Collaborating Centre for Drug Statistics Methodology [14]. The ATC systematically classifies medicinal products according to their site of action, therapeutic use, pharmacological properties, and chemical characteristics using a five-level hierarchical structure. The first level (anatomical main group) includes 14 major anatomical/pharmacological groups (e.g., L = antineoplastic and immunomodulating agents). The second level (therapeutic subgroup) classifies drugs based on therapeutic use (e.g., L01 = antineoplastic agents). The third level (pharmacological subgroup) classifies drugs based on pharmacological action or mechanism (e.g., L01C = plant alkaloids and other natural products). The fourth level (chemical subgroup) groups drugs sharing similar chemical structures or pharmacological features (e.g., L01CD = taxanes). The fifth level (chemical substance) consists of Individual active substances (e.g., L01CD01 = paclitaxel).Each drug is assigned up to five hierarchical ATC codes, allowing flexible aggregation and comparison across different classification levels. In this study, drugs classified under the second-level ATC categories L01 (antineoplastic agents) and L02 (endocrine therapy) were included.
The Medical Dictionary for Regulatory Activities (MedDRA) is a standardized international medical terminology with a five-level hierarchical structure: System Organ Class (SOC), High Level Group Term (HLGT), High Level Term (HLT), Preferred Term (PT), and Lowest Level Term (LLT).
To comprehensively and clinically appropriately capture alopecia-related adverse events, this study targeted all PTs classified under the HLT “Alopecias” based on MedDRA version 27.1. A complete list of the PTs included in the analysis is provided in Supplementary Table S1.
2.3. Selection Criteria for Drugs and Adverse Events
In addition to the aforementioned criteria, drugs registered in the FAERS drug information (DRUG) table as “primary suspect” or “secondary suspect” were included in the analysis. Meanwhile, PTs in which the etiology corresponded to, radiation therapy-related events, events localized to injection or application sites, drugs not classified under ATC categories L01 or L02-, and drugs registered as “concomitant” or “interaction” were excluded.
2.4. Outcomes
The primary assessment outcome differences in signal detection according to reporter type. Meanwhile, secondary outcomes included a comprehensive evaluation of alopecia-related signals and visualization of signal patterns using volcano plots.
2.5. Data Extraction and Integration
FAERS DRUG, adverse reaction information (REAC), patient demographic data (DEMO), and indication information (INDI) tables were used. These tables were integrated using the primary ID as a common key, and an inner join with the INDI table was additionally performed using the drug sequence number.
To construct the analytical datasets, the DRUG and REAC tables were merged by primary ID to identify cases (primary IDs) that included combinations of target drugs (ATC categories L01 and L02) and alopecia-related adverse events (MedDRA HLT “Alopecias”). Next, the DEMO table was linked to the extracted primary IDs to append patient background information, including sex, age, body weight, reporting country, and reporter type (occupation code). Subsequently, the INDI table was merged using the primary ID and corresponding drug sequence number to aggregate the indication data. Through this series of integration steps, analytical dataset encompassing drug–adverse event–patient background–indication information was constructed (Figure 1).
Based on this integrated dataset, case-based (primary ID–level) aggregations were performed according to the analytical objectives, and tables were created to visualize reporting distributions by drug and reporter occupation. To ensure analytical consistency, age and body weight were standardized. Age recorded in days, weeks, months, or decades was converted to years. For decade-based entries, the midpoint value (e.g., 35 years for “30s”) was assigned as a representative value. Body weight recorded in pounds was converted to kilograms. These standardized variables were used to generate descriptive statistics of patient characteristics and analytical tables for subsequent disproportionality and reporter-stratified analyses.
The requirements for ethical approval and informed consent were waived by the Ethics Committee of Meiji Pharmaceutical University because this study used anonymized data from a publicly available database and did not involve identifiable human subjects.
This flowchart illustrates the data curation process used to construct the analysis datasets from FAERS. DRUG, REAC, DEMO, and INDI tables were integrated after removing duplicated records. Alopecia-related adverse events were identified using PTs under the MedDRA HLT “Alopecias,” and antineoplastic agents classified under ATC codes L01 and L02 were selected. Reports submitted by healthcare professionals (physicians, pharmacists, nurses, and other HCPs) and non-HCPs were distinguished. Based on this process, six datasets were generated: analysis dataset A, patient background table A, and indication table A, which included all reporters, and analysis dataset B, patient background table B, and indication table B, which were restricted to HCP reports.
2.6. Assessment of Reporting Frequency and Reporter Characteristics
To identify drugs associated with alopecia, the reporting frequencies of drugs and alopecia-related adverse events included in the analytical dataset were summarized, and drugs with high reporting frequencies were extracted. To examine reporter characteristics and differences in reporting patterns according to reporter type, heatmaps were generated to visualize the distribution of reports by reporter occupation for the top 25 drugs with the highest reporting frequencies.
To aggregate reporter characteristics, alopecia-related PTs were integrated and treated as a single adverse event group (alopecia-related events). Reporter occupation (occupation code) was evaluated on a case basis (primary ID level). The reporter occupation associated with each primary ID was classified according to the occupation code recorded in the DEMO table. Both the analysis of reporter composition and the generation of heatmaps were performed using case-based aggregation.
2.7. Disproportionality Analysis
To evaluate the association between each target drug and alopecia-related adverse events, all alopecia-related events were treated as a single outcome group, and reporting odds ratios (RORs) and 95% confidence intervals (CIs) were calculated (Figure 2).
Disproportionality analyses were conducted on a report-level basis using a case/non-case approach. For each drug–event combination, a 2 × 2 contingency table was constructed on the basis of unique FAERS reports identified by primary IDs. To avoid duplicate counting because of follow-up reports, records were deduplicated, ensuring that each primary ID was counted only once. All analyses were therefore performed on a one report per primary ID basis. In this study, the term “case” refers to a unique FAERS report after deduplication rather than a clinical case defined by CASEID.
Each cell represents the number of cases (primary IDs) classified as follows:
(a) cases in which the drug of interest (antineoplastic agents classified under ATC codes L01 or L02) was reported as a suspect drug and alopecia (MedDRA HLT “Alopecias”) was reported;
(b) cases in which the drug of interest was reported as a suspect drug but alopecia was not reported;
(c) cases in which drugs other than the drug of interest were reported as suspect drugs and alopecia was reported; and
(d) cases in which drugs other than the drug of interest were reported as suspect drugs and alopecia was not reported.
Based on this analysis, RORs and their associated 95% CIs were calculated, and statistical significance was assessed using Fisher’s exact test. In this study, all ROR calculations were performed using a case-based approach.
2.8. Stratified Analysis Restricted to HCPs
Given the potential impact of reporter characteristics on adverse drug reaction reporting patterns and signal detection, a stratified analysis restricted to reports submitted by HCPs, including physicians, pharmacists, nurses, and other healthcare workers, was performed.
2.8.1. Definition of Stratification Criteria
HCP reports were identified using the occp_cod variable in the DEMO table of the FAERS database. In this study, reports with occupation codes MD, PH, RN, HP, and OT were defined as reports submitted by HCPs.
2.8.2. Rational and Analytical Purpose
Reports submitted by HCPs are generally considered to have higher diagnostic accuracy and more reliable causal assessments, thereby potentially minimizing the influence of reporting bias. In contrast, patient reports tend to capture subjective symptoms and quality of life (QoL)–related impacts, which might alter the nature of detected signals in analyses that do not restrict reporter type. Accordingly, this study aimed to extract more objective and clinically meaningful signals through stratified analyses restricted to HCP reports while acknowledging the complementary value of patient-reported information.
2.9. Statistical Analysis
In both the all-reporter and HCP-restricted analyses, RORs and 95% CIs were calculated, and statistical significance was assessed using Fisher’s exact test. When zero cells were present, the Haldane–Anscombe correction (adding 0.5 to each cell) was applied to stabilize estimates [15].
In addition, volcano plots were generated to visualize the results of the HCP-restricted analysis. Natural logarithms of the RORs (lnROR) and −log10(p-values) were calculated, and signals were defined as lnROR > 0 and −log10(p) > 1.3 (i.e., ROR > 1 and p < 0.05).
Data processing and statistical analyses were performed using JMP Pro 18.2 (SAS Institute Inc., Cary, NC, USA) and Python (pandas, SciPy; https://www.python.org/). Forest plots and heatmaps were generated using R (version 4.5.1; The R Foundation for Statistical Computing, Vienna, Austria) and the RStudio environment (PBC, Boston, MA, USA). The “forestploter” package was used for forest plots, and the “pheatmap” package was used for heatmaps. Given the exploratory nature of this study, the significance threshold was set at p < 0.05.
3. Results
3.1. Baseline Characteristics of the Analytical Dataset
In total, 76,580 cases were included in the analysis. Sex information was available for 62,565 cases. Of these, 56,378 cases (90.11%) involved female patients, whereas 6097 cases (9.75%) involved male patients. Sex was classified as unknown in 90 cases (0.14%). Among the 45,821 cases for which age information was available, the median age was 57 years [interquartile range (IQR) = 47–66]. Body weight information was available for 22,371 cases, and the median weight was 75 kg (IQR = 64–91 kg).
Country information was available for 76,308 cases. The largest number of reports originated from the US (52,928 cases, 69.36%), followed by Canada (11,800 cases, 15.46%), the UK (1683 cases, 2.21%), Germany (1331 cases, 1.74%), and Japan (1113 cases, 1.46%). Meanwhile, country information was missing for 1335 cases (1.75%) As the numbers of reports from Germany was comparable to that of reports with missing country information, Japan was included to present the top six reporting countries.
Indication information was available for 71,767 cases. In the all-reporter dataset, breast cancer-related PTs predominated, including “Breast cancer female” (13,615 cases, 18.97%), “Breast cancer” (7635 cases, 10.64%), “Breast cancer metastatic” (3025 cases, 4.22%), and “Triple negative breast cancer” (699 cases, 0.97%). Collectively, breast cancer-related indications accounted for more than 35% of all cases. “Rheumatoid arthritis” was the second most frequent indication, reported in 9270 cases (12.92%).

Table 1.
Baseline characteristics of cases included in the analysis dataset.
| a. All Reporter Types | b. Healthcare Professionals Only | ||||||
| (n = 76,580) | (n = 27,838) | ||||||
| Characteristics | No. | (%) | No. | (%) | |||
| Gender | |||||||
| Data available | 62,565 | Data available | 24,560 | ||||
| Female | 56,378 | 90.11% | Female | 21,488 | 87.49% | ||
| Male | 6,097 | 9.75% | Male | 3,015 | 12.28% | ||
| Unknown | 90 | 0.14% | Unknown | 57 | 0.23% | ||
| Age (years old) | |||||||
| Data available | 45,821 | Data available | 17,802 | ||||
| less than 30 | 1,190 | 2.60% | less than 30 | 710 | 3.99% | ||
| 30-39 | 2,474 | 5.40% | 30-39 | 818 | 4.60% | ||
| 40-49 | 10,267 | 22.41% | 40-49 | 4,457 | 25.04% | ||
| 50-59 | 12,355 | 26.96% | 50-59 | 3,954 | 22.21% | ||
| 60-69 | 11,624 | 25.37% | 60-69 | 4,190 | 23.54% | ||
| 70-79 | 6,190 | 13.51% | 70-79 | 2,861 | 16.07% | ||
| 80 or more | 1,721 | 3.76% | 80 or more | 812 | 4.56% | ||
| Median (IQR) | 57(47-66) | Median (IQR) | 58(45-67) | ||||
| Body weight (kg) | |||||||
| Data available | 22,371 | Data available | 6,434 | ||||
| less than 40 | 169 | 0.76% | less than 40 | 112 | 1.74% | ||
| 40-49 | 802 | 3.59% | 40-49 | 337 | 5.24% | ||
| 50-59 | 2,855 | 12.76% | 50-59 | 890 | 13.83% | ||
| 60-69 | 4,829 | 21.59% | 60-69 | 1,620 | 25.18% | ||
| 70-79 | 4,294 | 19.19% | 70-79 | 1,024 | 15.92% | ||
| 80-89 | 3,181 | 14.22% | 80-89 | 635 | 9.87% | ||
| 90-99 | 3,321 | 14.85% | 90-99 | 1,445 | 22.46% | ||
| 100 or more | 2,920 | 13.05% | 100 or more | 371 | 5.77% | ||
| Median(IQR) | 75(64-91) | Median(IQR) | 72(62-93) | ||||
| Reported countries (Top6) | |||||||
| Data available | 76,308 | Data available | 27,711 | ||||
| United States | 52,928 | 69.36% | United States | 10,429 | 37.64% | ||
| Canada | 11,800 | 15.46% | Canada | 9,741 | 35.15% | ||
| United Kingdom | 1,683 | 2.21% | Germany | 1,079 | 3.89% | ||
| Country Not Specified | 1,335 | 1.75% | Japan | 1,004 | 3.62% | ||
| Germany | 1,331 | 1.74% | United Kingdom | 944 | 3.41% | ||
| Japan | 1,113 | 1.46% | Italy | 800 | 2.89% | ||
| Indication (pt_term, Top15) | |||||||
| Data available | 71,767 | 28,190 | |||||
| Product used for an unknown indication | 14,038 | 19.56% | Rheumatoid Arthritis | 7,740 | 27.46% | ||
| Breast Cancer Female | 13,615 | 18.97% | Product used for an unknown indication | 5,687 | 20.17% | ||
| Rheumatoid Arthritis | 9,270 | 12.92% | Breast Cancer | 1,728 | 6.13% | ||
| Breast Cancer | 7,635 | 10.64% | Breast Cancer Metastatic | 1,251 | 4.44% | ||
| Breast Cancer Metastatic | 3,025 | 4.22% | Breast Cancer Female | 1,160 | 4.12% | ||
| Chemotherapy | 1,355 | 1.89% | Chronic Myeloid Leukaemia | 456 | 1.62% | ||
| Invasive ductal breast carcinoma | 1,020 | 1.42% | Basal Cell Carcinoma | 407 | 1.44% | ||
| Chronic Myeloid Leukaemia | 985 | 1.37% | Non-Small Cell Lung Cancer | 357 | 1.27% | ||
| Basal Cell Carcinoma | 976 | 1.36% | Ovarian Cancer | 277 | 0.98% | ||
| Lung Neoplasm Malignant | 742 | 1.03% | Psoriatic Arthropathy | 222 | 0.79% | ||
| Ovarian Cancer | 734 | 1.02% | Renal Cell Carcinoma | 197 | 0.70% | ||
| Triple-negative breast cancer | 699 | 0.97% | Colorectal Cancer Metastatic | 194 | 0.69% | ||
| Non-Small Cell Lung Cancer | 651 | 0.91% | Arthritis | 193 | 0.69% | ||
| Prostate Cancer | 587 | 0.82% | Neoplasm Malignant | 189 | 0.67% | ||
| Gastrointestinal Stromal Tumour | 529 | 0.74% | Lung Neoplasm Malignant | 184 | 0.65% | ||
Reports submitted by HCPs included physicians, pharmacists, nurses, health professionals, and other HCPs, as defined by occupation codes in the DEMO table.
3.2. Alopecia-Related PTs Included in the Analysis
In total, 22 PTs were classified under the HLT “Alopecias.” After excluding PTs as specified in the exclusion criteria, 13 PTs representing alopecia types for which drug involvement could not be excluded were included in the analysis. The complete list of included PTs is provided in Supplementary Table S1. Seborrhoeic alopecia was not present in the analytical dataset. The most frequent reported term was alopecia, followed by madarosis and alopecia areata (Table 2a).
3.3. Drug-Specific Reporting Frequencies
The top 25 drugs with the highest number of alopecia-related reports are presented in Table 3a. The number of reports was highest for docetaxel, followed by methotrexate and cyclophosphamide.
3.4. Distribution of Reporter Characteristics
Reporter occupation was aggregated on a case basis (primary ID level) for cases reporting alopecia-related events. Reports submitted by consumers and legal professionals accounted for more than half of all cases, whereas reports from HCPs accounted for 36.92% of cases (Figure 3). When drug- and occupation-specific reporting counts were visualized using a heatmap, certain drugs exhibited marked clustering in reports from consumers and legal professionals (Figure 4). For docetaxel, reports from consumers and legal professionals were particularly prominent, with 14,148 reports submitted by consumers and 14,720 reports submitted by legal professionals (Supplementary Table S2).
Percentages were calculated on the basis of unique primary case IDs. The outer ring represents reporter categories (HCPs vs. non-HCPs), whereas the inner ring presents the distribution of FAERS occupation codes, including physicians, pharmacists, registered nurses, health professionals, other health professionals, consumers, and lawyers. HCPs comprised physicians, pharmacists, registered nurses, health professionals, and other HCPs.
This heatmap visualizes the distribution of alopecia-related adverse event cases across the top 25 drugs with the highest reporting frequency stratified by reporter occupation. Each cell represents the number of unique primary cases (primary IDs) in which a given drug–alopecia combination was reported by a specific reporter occupation category.
Reporter occupation was defined on the basis of the occupation code recorded in the FAERS DEMO table and classified as consumers (CN), lawyers (LW), physicians (MD), pharmacists (PH), registered nurses (RN), other health professionals (OT), and health professionals (HP). Color intensity indicates the number of cases, with darker colors representing a higher number of reported cases.
3.5. Disproportionality Analysis in the All-Reporter Dataset
Disproportionality analysis using RORs was conducted to evaluate the association between each target drug and alopecia-related adverse events. All included alopecia-related PTs were treated as a single outcome group for ROR calculation. Several antineoplastic agents exhibited strong associations with alopecia-related events, most notably docetaxel (ROR = 58.31, 95% CI = 57.46–59.17, p < 0.001). Elevated RORs were also observed for vismodegib (ROR: 19.35, 95% CI: 18.24–20.52, p < 0.001) and trastuzumab (ROR = 8.23, 95% CI = 8.00–8.47, p < 0.001). Conversely, some drugs, such as leuprorelin (ROR = 0.99, 95% CI = 0.93–1.06, p = 0.764), did not exhibit statistically significant associations with alopecia (Table 4a).
3.6. Results of the Stratified Analysis Restricted to HCPs
3.6.1. Patient Characteristics in the HCP-Restricted Dataset
The baseline characteristics of cases reported by HCPs are summarized in Table 1b. Female patients predominated, and the median age was 58 years (IQR = 45–67). Indication information was available for 28,190 cases. The most frequent indication was rheumatoid arthritis (7740 cases, 27.46%), followed by product used for unknown indication (5687 cases, 20.17%), breast cancer (1728 cases, 6.13%), breast cancer metastatic (1251 cases, 4.44%), and breast cancer female (1160 cases, 4.12%).
3.6.2. Alopecia-Related PTs Reported by HCPs
Table 2b presents the distribution of alopecia-related PTs reported by HCPs. Alopecia was the most frequently reported PT, accounting for 49,986 reports, followed by madarosis (754 reports) and alopecia areata (469 reports).
3.6.3. Drug-Specific Reporting Frequencies in HCP Reports
In the dataset restricted to reports submitted by healthcare professionals (HCPs), drug-specific reporting frequencies for alopecia-related adverse events are summarized in Table 3b.
Methotrexate was the most frequently reported drug (11,863 reports), followed by rituximab (7,929 reports) and palbociclib (3,470 reports). Endocrine therapies and molecular targeted agents, including letrozole, fulvestrant, ribociclib, and vismodegib, were also among the frequently reported drugs in the HCP-restricted dataset.
In contrast, docetaxel, which ranked highest in the all-reporter analysis, showed a lower ranking in the HCP-restricted dataset (1,408 reports). Other cytotoxic chemotherapeutic agents, such as cyclophosphamide, carboplatin, and doxorubicin, were reported but did not dominate the top-ranked drugs.
Overall, the distribution of frequently reported drugs differed between the HCP-restricted and all-reporter datasets, reflecting variations in reporting patterns according to reporter type.
3.6.4. Disproportionality Analysis in the HCP-Restricted Dataset
Disproportionality analysis based on alopecia-related PTs was conducted using reports submitted by HCPs only. The results for drugs with high reporting frequencies are presented in Table 4b. Several drugs demonstrated statistically significant associations with alopecia-related events, including vismodegib (ROR = 23.92, 95% CI = 21.86–26.17, p < 0.001) and palbociclib (ROR = 11.34, 95% CI = 10.94–11.75, p < 0.001). By contrast, a significant association was noted for cisplatin (ROR = 1.05, 95% CI = 0.96–1.15, p = 0.326). Oxaliplatin featured an ROR below unity (ROR = 0.87, 95% CI = 0.79–0.95, p = 0.003), suggesting no positive association with alopecia.
3.6.5. Differences in RORs According to Reporter Type
Figure 5 compares changes in RORs for major drugs between the all-reporter dataset and the HCP-restricted dataset. For docetaxel, lnROR values were markedly higher in the all-reporter analysis than in the HCP-restricted analysis, suggesting potential overestimation of the association because of reporting bias.
The forest plots present the lnROR and 95% CIs for major drugs associated with alopecia-related adverse events. Results derived from reports submitted by HCPs and those submitted by all reporters (ALL) are presented for comparison.
3.6.6. Volcano Plot
Volcano plots depicting the lnROR and −log10(p) were generated to visually assess potential safety signals by jointly considering the strength of association with alopecia and statistical significance. As presented in Figure 6, drugs demonstrating statistically suggestive associations with alopecia included 23 of the top 25 drugs by reporting frequency that satisfied the criteria of lnROR > 0 and p < 0.05 (Table 4b), as well as 22 additional drugs with at least 100 reports that met the same statistical thresholds. In total, 45 drugs were identified as potential alopecia-related signals.
Each point represents an individual drug. The x-axis represents the lnROR, reflecting the strength of association with alopecia-related adverse events. The y-axis represents −log10(p) obtained from Fisher’s exact test, indicating statistical significance. Drugs labeled in red correspond to the top 25 drugs by reporting frequency (Table 4b). Blue points indicate drugs with 100 or more reports. Labeled drugs located in the first quadrant (lnROR > 0 and −log10(p) > 1.3) demonstrate statistically significant associations with ROR > 1 and are interpreted as drugs with potential alopecia-related safety signals.
4. Discussion
The most prominent and clinically meaningful finding of this study was the identification of a substantial reporter-related bias in alopecia-related safety signals derived from the FAERS database, particularly for docetaxel. Although docetaxel exhibited an extremely high ROR in the overall dataset, this signal markedly attenuated when the analysis was restricted to reports submitted by HCPs, resulting in estimates that were more consistent with existing clinical trial data [16]. This discrepancy appears to be largely attributable to the disproportionate number of reports submitted by consumers and legal professionals, potentially reflecting ongoing litigation in the US concerning permanent chemotherapy–induced alopecia. These findings underscore that the reporter type can substantially distort signal estimates, particularly for adverse events that are visually apparent and emotionally distressing, such as alopecia, and therefore are more likely to stimulate patient-driven or legally motivated reporting.
4.1. Characteristics of Alopecia Reporting and Pharmacological Background
In this study, we analyzed reporting patterns of cancer treatment-related alopecia using the FAERS database and examined the influence of reporter characteristics on signal detection. Alopecia-related adverse events were defined using 13 PTs classified under the MedDRA HLT “Alopecias” after excluding congenital, infectious, radiation-induced, and localized forms of alopecia. Target drugs were defined as those classified under ATC categories L01 and L02.
The inclusion of both antineoplastic and endocrine therapies was based on the biological rationale that cytotoxic injury and hormonal alterations can affect the hair cycle and hair follicle stem cell function, thereby contributing to alopecia [5,17,18,19,20,21,22]. This approach was particularly relevant for breast cancer populations, in which chemotherapy and endocrine therapy are frequently combined or administered sequentially [20,21,23].
Cancer treatment-related alopecia can be broadly categorized into three mechanistic types. First, CIA is characterized by acute, extensive hair loss resulting from DNA damage and apoptosis in rapidly proliferating hair matrix keratinocytes, typically manifesting as anagen effluvium. Second, EIA, associated with agents such as tamoxifen and aromatase inhibitors, presents as chronic, diffuse hair thinning resembling female-pattern hair loss attributable to hormonal dysregulation. Third, targeted therapies, including EGFR inhibitors, Hedgehog pathway inhibitors, and CDK4/6 inhibitors, can induce drug-specific alopecia patterns through direct interference with hair follicle signaling pathways and cell cycle regulation. These diverse mechanisms collectively explain the heterogeneity of alopecia observed in clinical practice and justify the inclusion of both L01 and L02 drug classes in the present analysis.
CIA occurs when cytotoxic agents target rapidly dividing hair matrix cells and induce DNA damage and p53-mediated apoptosis, leading to premature hair follicle regression and shedding [4]. Taxanes, particularly docetaxel and paclitaxel, exert strong cytotoxic effects on hair follicle stem cells, and their ability to induce severe alopecia is well recognized [4,24]. Previous FAERS-based analyses also identified strong alopecia signals for docetaxel [25], consistent with the findings from our all-reporter dataset.
Clinical studies have demonstrated that docetaxel carries a higher risk of permanent chemotherapy–induced alopecia (pCIA) than paclitaxel [26,27,28], with cumulative doses exceeding 400 mg/m2 associated with irreversible follicular damage [26]. The marked discrepancy in RORs between paclitaxel and docetaxel in our overall dataset might reflect differences in pCIA risk.
Genetic susceptibility can further contribute to pCIA. A single nucleotide polymorphism (rs1202179) in the ABCB1 gene, which encodes P-glycoprotein, has been significantly associated with pCIA (odds ratio = 3.79, 95% CI = 2.17–6.62, p = 3.05 ×10−6) [29]. P-glycoprotein plays a protective role by exporting docetaxel from cells, including hair follicle stem cells. The risk allele is associated with reduced ABCB1 expression, leading to intracellular accumulation of docetaxel and irreversible follicular damage.
Endocrine therapies, such as tamoxifen and aromatase inhibitors, induce alopecia by altering the hormonal milieu and disrupting the hair cycle [30]. Compared with CIA, EIA tends to be chronic and sometimes poorly reversible, exerting a profound impact on patients’ self-image and perceived femininity [31].
Vismodegib, a Hedgehog pathway inhibitor, disrupts hair follicle regeneration by inhibiting pathways essential for anagen maintenance and stem cell differentiation [32,33]. Clinical trials have reported alopecia incidence rates of 40%–60% for Hedgehog inhibitors [32,34], with alopecia typically presenting with delayed, diffuse, and non-scarring symptoms [35]. The detection of a strong vismodegib signal in this study aligns well with these pharmacological and clinical observations.
Palbociclib, a CDK4/6 inhibitor, arrests the cell cycle in the G1 phase and suppresses proliferation in both tumor cells and hair follicle epithelial cells, potentially shortening the anagen phase and inducing diffuse alopecia [36]. Clinical reports describe mostly mild and reversible alopecia [37,38]. Interestingly, preclinical studies suggest that CDK4/6 inhibition can protect hair follicle stem cells from taxane-induced damage [39], indicating context-dependent effects on hair biology.
In the HCP-restricted analysis, a substantial proportion of reports involved rheumatologic indications. Methotrexate, a cornerstone disease-modifying antirheumatic drug, is widely used in long-term treatment regimens [40,41] and is well known to cause alopecia through folate antagonism [42,43]. Methotrexate-associated alopecia is generally reversible, and it can be mitigated by folic acid supplementation or dose adjustment [44]. Chronic disease management and structured follow-up by rheumatologists might facilitate more systematic adverse event reporting by healthcare professionals. Conversely, CIA often anticipated and transient, potentially leading to underreporting by clinicians. This reporting asymmetry might explain why consumer reports are enriched for oncology-related alopecia, whereas HCP reports more frequently involve rheumatologic drugs, reflecting structural differences in reporting culture across disease areas.
4.2. Reporter Type and Bias in Reporting Patterns
This study demonstrated that consumer and legal professional reports constituted the majority of alopecia-related FAERS submissions, whereas reports from HCPs accounted for approximately one-third of all alopecia-related submissions. This pattern suggests that appearance-related and QoL adverse events, although highly salient to patients, might be deprioritized by clinicians who focus primarily on life-threatening toxicities.
Reports concerning docetaxel were principally submitted consumers and legal professionals (Figure 4). In the US, multidistrict litigation (MDL 2740) concerning permanent alopecia allegedly caused by docetaxel is ongoing [45,46,47,48,49,50]. These legal actions highlight a disconnect between patient expectations and clinical communication regarding the potential permanence of alopecia.
Within this context, docetaxel featured an exceptionally high ROR in the all-reporter analysis but a substantially weaker signal decreased in the HCP-restricted analysis. This pattern strongly suggests that reporter bias inflated the signal [7,51]. In phase III clinical trials, both docetaxel and paclitaxel have been linked to a high incidence of high alopecia, with docetaxel causing grade 3/4 non-hematologic toxicity [16]. In our HCP-restricted analysis, the RORs for these agents were more comparable, aligning more closely with trial data.
Although HCP reports tend to offer higher diagnostic accuracy, patient reports provide valuable insights into symptom burden, daily functioning, and emotional impact. Prior studies have indicated that patient reports more frequently capture QoL-related adverse events and psychological distress [52,53]. Therefore, stratifying analyses by reporter type might allow both clinically robust signal detection and a more comprehensive understanding of patient experience.
4.3. HCP-Stratified Analysis and Visualization Using Volcano Plots
Volcano plots simultaneously visualize effect size (lnROR) and statistical significance [−log10(p)], facilitating intuitive identification of clinically relevant signals among numerous drugs [54]. To minimize reporter-related bias and enhance pharmacological plausibility, volcano plots were constructed based on HCP-only reports.
This approach highlighted persistent and statistically significant alopecia signals for targeted therapies and endocrine agents, including Hedgehog pathway inhibitors (vismodegib), CDK4/6 inhibitors (palbociclib, ribociclib), and endocrine therapies (letrozole, anastrozole, exemestane, fulvestrant, tamoxifen). These findings are consistent with established mechanisms involving hair follicle cycling and hormonal regulation [32,35,37,38,39].
Signals detected for monoclonal antibodies (trastuzumab, pertuzumab, and rituximab) likely reflect combination regimens and disease context rather than direct drug effects. HER2-targeted antibodies are commonly administered with taxanes or anthracyclines, which are primary drivers of CIA [55,56,57]. Rituximab is frequently used in both lymphoma and autoimmune diseases, often in combination with cytotoxic agents or MTX [58,59,60]. Therefore, the elevated RORs observed for rituximab in the HCP-restricted analysis likely reflect the attribution complexities inherent to FAERS rather than a direct causal effect. Because ROR indicates reporting disproportionality rather than causality [7], these signals must be interpreted cautiously. Drug-specific, indication-stratified, and monotherapy-focused analyses are required for more definitive risk assessment.
4.4. Psychological Impact of Alopecia and QoL
Approximately 90% of alopecia reports in this study involved female patients, with breast cancer accounting for nearly 40% of cases. This distribution likely reflects heightened sensitivity to appearance-related changes among women [61]. Persistent alopecia following chemotherapy has been reported in a subset of patients [62,63,64,65], leading to long-term impairment of self-esteem, social functioning, and HRQoL.
Alopecia has been identified as a major barrier to treatment initiation and adherence [3,66], with some patients describing it as more distressing than mastectomy [67]. Patient-reported outcome measures, such as the EORTC QLQ-BR42, the updated breast cancer-specific QoL module that replaced the provisional BR45 version, assess distress related to hair loss [68,69], underscoring its clinical relevance.
Notably, up to 8% of patients reportedly refuse chemotherapy because of cosmetic concerns [1], and CIA has been associated with acute stress disorder and PTSD-like symptoms [70,71]. Preventive strategies, such as scalp cooling, have displayed efficacy in reducing CIA [72,73], whereas therapeutic options, including topical and oral minoxidil, remain investigational [74,75,76]. For EIA and pCIA, evidence-based interventions remain limited.
Psychosocial interventions, particularly appearance care programs, have emerged as important supportive strategies. Programs such as Look Good Feel Better aim to preserve self-image through cosmetic counseling and have demonstrated benefits in emotional well-being and self-efficacy [77,78,79]. Integrating biological and psychosocial approaches is therefore essential for comprehensive alopecia management.
4.5. Study Limitations and Future Directions
This study carried several limitations inherent to spontaneous reporting systems. FAERS is subject to underreporting, missing data, and reporting bias, and it does not allow causal inference. Detailed information on dose, treatment duration, and combination regimens is often unavailable, limiting granular risk assessment. Non-serious adverse events, such as alopecia, might be disproportionately influenced by patient perception and external stimuli, and the absence of statistical disproportionality does not equate to the absence of risk.
Additionally, FAERS primarily reflects US reporting patterns, which can limit generalizability. Future research integrating electronic health records and prospective cohort studies is needed to better characterize temporal relationships, risk factors, and intervention effects. Prospective evaluations of preventive and supportive strategies, particularly for persistent alopecia, are warranted to inform patient-centered care and personalized risk mitigation.
5. Conclusions
This study conducted a comprehensive disproportionality analysis using a large-scale spontaneous reporting database to evaluate alopecia signals associated with antineoplastic and endocrine therapies. By incorporating a stratified analysis restricted to reports submitted by HCPs, we demonstrated that certain drugs exhibit substantial differences in the reporting proportion of alopecia between all reporters and HCPs.
These findings provide database-level evidence that alopecia, although typically regarded as a medically non-severe adverse event, represents a clinically meaningful issue for patients, exerting a considerable psychological burden and potentially influencing motivation to continue treatment. This underscores the importance of recognizing cancer treatment-related alopecia as both a QoL-related adverse event and a clinical challenge that can affect treatment adherence and psychosocial well-being.
Furthermore, visualization using volcano plots enabled the comprehensive and intuitive identification of drugs associated with higher alopecia risk. This approach might provide a practical foundation for considering preventive strategies and psychosocial support prior to treatment initiation. Collectively, these findings contribute to the development of a patient-centered drug safety evaluation framework and provide scientific support for establishing comprehensive care systems addressing alopecia in cancer therapy.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Preferred Terms included in the MedDRA High Level Term “Alopecias” used for the disproportionality analysis; Table S2: Reporter type-specific counts of alopecia cases for the top 25.
Author Contributions
Conceptualization, Y.U.; Methodology, Y.U.; Software, A.Y. and Y.U.; Validation, A.Y. and Y.U.; Formal analysis, A.Y. and Y.U.; Investigation, A.Y. and Y.U.; Data curation, A.Y. and Y.U.; Visualization, A.Y.; Writing—original draft preparation, A.Y.; Writing—review and editing, A.Y. and Y.U.; Supervision, Y.U.; Project administration, Y.U.; Funding acquisition, Y.U. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partially supported by the Grants-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (JSPS), Grant Number 22K06707.
Institutional Review Board Statement
Ethical review and approval were waived for this study because it used anonymized data from a publicly available database and did not involve identifiable human subjects.
Informed Consent Statement
Not applicable
Data Availability Statement
The data analyzed in this study are publicly available from the FDA Adverse Event Reporting System.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (OpenAI, accessed in 2026) for the purpose of assisting in the generation of a draft graphical abstract illustration. The authors reviewed, edited, and integrated the generated content and take full responsibility for the final content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FAERS | FDA Adverse Event Reporting System |
| SRS | Spontaneous reporting system |
| AE | Adverse event |
| MedDRA | Medical Dictionary for Regulatory Activities |
| HLT | High Level Term |
| PT | Preferred Term |
| LLT | Lowest Level Term |
| ATC | Anatomical Therapeutic Chemical Classification System |
| HCPs | Healthcare professionals |
| ROR | Reporting odds ratio |
| lnROR | Natural logarithm of the reporting odds ratio |
| CI | Confidence interval |
| IQR | Interquartile range |
| CTIA | Cancer therapy–induced alopecia |
| CIA | Chemotherapy-induced alopecia |
| EIA | Endocrine therapy–induced alopecia |
| pCIA | Permanent chemotherapy–induced alopecia |
| QoL | quality of life |
| HRQoL | Health-related quality of life |
References
- McGarvey, E.L.; Baum, L.D.; Pinkerton, R.C.; Rogers, L.M. Psychological sequelae and alopecia among women with cancer. Cancer Pract. 2001, 9, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Hunt, N.; McHale, S. The psychological impact of alopecia. BMJ 2005, 331, 951–953. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, J.; Maunsell, E.; Provencher, L. Chemotherapy-induced alopecia and effects on quality of life among women with breast cancer: A literature review. Psychooncology 2008, 17, 317–328. [Google Scholar] [CrossRef]
- Paus, R.; Haslam, I.S.; Sharov, A.A.; Botchkarev, V.A. Pathobiology of chemotherapy-induced hair loss. Lancet Oncol. 2013, 14, e50–e59. [Google Scholar] [CrossRef]
- Freites-Martinez, A.; Shapiro, J.; Chan, D.; Fornier, M.; Modi, S.; Gajria, D.; Dusza, S.; Goldfarb, S.; Lacouture, M.E. Endocrine therapy-induced alopecia in patients with breast cancer. JAMA Dermatol. 2018, 154, 670–675. [Google Scholar] [CrossRef]
- Belum, V.R.; Marulanda, K.; Ensslin, C.; Gorcey, L.; Parikh, T.; Wu, S.; Busam, K.J.; Gerber, P.A.; Lacouture, M.E. Alopecia in patients treated with molecularly targeted anticancer therapies. Ann. Oncol. 2015, 26, 2496–2502. [Google Scholar] [CrossRef] [PubMed]
- Cutroneo, P.M.; Sartori, D.; Tuccori, M.; Crisafulli, S.; Battini, V.; Carnovale, C.; Rafaniello, C.; Capuano, A.; Poluzzi, E.; Moretti, U.; Raschi, E. Conducting and interpreting disproportionality analyses derived from spontaneous reporting systems. Front. Drug Saf. Regul. 2024, 3, 1323057. [Google Scholar] [CrossRef]
- Petracek, J.; Fialova, M. Spontaneous reporting systems. In Principles and Practice of Pharmacovigilance and Drug Safety;Chapter 10; Springer: Cham, Switzerland, 2023. [Google Scholar] [CrossRef]
- Palleria, C.; Leporini, C.; Chimirri, S.; Marrazzo, G.; Sacchetta, S.; Bruno, L.; Lista, R.M.; Staltari, O.; Scuteri, A.; Scicchitano, F.; Russo, E. Limitations and obstacles of the spontaneous adverse drug reactions reporting: Two “challenging” case reports. J. Pharmacol. Pharmacother. 2013, 4, S66–S72. [Google Scholar] [CrossRef]
- Dueck, A.C.; Mendoza, T.R.; Mitchell, S.A.; Reeve, B.B.; Castro, K.M.; Rogak, L.J.; Atkinson, T.M.; Bennett, A.V.; Denicoff, A.M.; O’Mara, A.M.; Li, Y.; Clauser, S.B.; Bryant, D.M.; Bearden, J.D., III; Gillis, T.A.; Harness, J.K.; Siegel, R.D.; Paul, D.B.; Cleeland, C.S.; Schrag, D.; Sloan, J.A.; Abernethy, A.P.; Bruner, D.W.; Minasian, L.M.; Basch, E. National Cancer Institute PRO-CTCAE Study Group. Validity and reliability of the U.S. National Cancer Institute’s patient-reported outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). JAMA Oncol. 2015, 1, 1051–1059. [Google Scholar] [CrossRef]
- Minasian, L.M.; O’Mara, A.; Mitchell, S.A. Clinician and patient reporting of symptomatic adverse events in cancer clinical trials: Using CTCAE and PRO-CTCAE® to provide two distinct and complementary perspectives. Patient Relat. Outcome Meas. 2022, 13, 249–258. [Google Scholar] [CrossRef]
- Veitch, Z.W.; Shepshelovich, D.; Gallagher, C.; Wang, L.; Abdul Razak, A.R.; Spreafico, A.; Bedard, P.L.; Siu, L.L.; Minasian, L.; Hansen, A.R. Underreporting of symptomatic adverse events in phase I clinical trials. J. Natl. Cancer Inst. 2021, 113, 980–988. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Adverse Event Reporting System (FAERS). Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-adverse-event-reporting-system-faers-database (accessed on 5 December 2025).
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2024; World Health Organization: Oslo, Norway, 2024; Available online: https://www.whocc.no.
- Lawson, R. Small sample confidence intervals for the odds ratio. Commun. Stat. Simul. Comput. 2004, 33, 1095–1113. [Google Scholar] [CrossRef]
- Jones, S.E.; Erban, J.; Overmoyer, B.; Budd, G.T.; Hutchins, L.; Lower, E.; Laufman, L.; Sundaram, S.; Urba, W.J.; Pritchard, K.I.; Mennel, R.; Richards, D.; Olsen, S.; Meyers, M.L.; Ravdin, P.M. Randomized phase III study of docetaxel compared with paclitaxel in metastatic breast cancer. J. Clin. Oncol. 2005, 23, 5542–5551. [Google Scholar] [CrossRef]
- Slaught, C.; Roman, M.; Yashar, S.; Holland, V.; Goh, C. Permanent alopecia in breast cancer patients: Role of taxanes and endocrine therapies. Cutis 2021, 107, E17–E22. [Google Scholar] [CrossRef] [PubMed]
- Freites-Martinez, A.; Chan, D.; Sibaud, V.; et al. Assessment of quality of life and treatment outcomes of patients with persistent postchemotherapy alopecia. JAMA Dermatol. 2019, 155, 724–728. [Google Scholar] [CrossRef]
- Dubin, C.; Lamb, A. Hair regrowth in endocrine therapy alopecia with dutasteride treatment in a woman with estrogen-positive breast cancer. JAAD Case Rep. 2023, 35, 5–7. [Google Scholar] [CrossRef]
- Moscetti, L.; Fabbri, M.A.; Sperduti, I.; et al. Adjuvant aromatase inhibitor therapy in early breast cancer: What factors lead patients to discontinue treatment? Tumori 2015, 101, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, L.; Calhoun, C.; Helzlsouer, K.J. Aromatase inhibitor therapy and hair loss among breast cancer survivors. Breast Cancer Res. Treat. 2013, 142, 435–443. [Google Scholar] [CrossRef]
- Saggar, V.; Wu, S.; Dickler, M.N.; Lacouture, M.E. Alopecia with endocrine therapies in patients with cancer. Oncologist 2013, 18, 1126–1134. [Google Scholar] [CrossRef]
- Wysocki, P.J. Combination of chemotherapy and endocrine treatment in breast cancer—Is it still a taboo? Oncol. Clin. Pract. 2024, 20, 302–307. [Google Scholar] [CrossRef]
- Blanpain, C. CDK4/6 inhibition mitigates stem cell damage in a novel model for taxane-induced alopecia. EMBO Mol. Med. 2019, 11, e201911031. [Google Scholar] [CrossRef]
- Zhao, Q.; Nian, Z.; He, Y.; Lai, L.; Liu, W.; Huang, S.; Yang, L. Toxicity spectrum of taxanes: A safety analysis from pre-marketing to post-marketing. Expert Opin. Drug Saf. 2025. [Google Scholar] [CrossRef]
- Martin, M.; de la Torre-Montero, J.C.; Lopez-Tarruella, S.; Pinilla, K.; Casado, A.; Fernandez, S.; Jerez, Y.; Puente, J.; Palomero, I.; Gonzalez Del Val, R.; et al. Persistent major alopecia following adjuvant docetaxel for breast cancer: Incidence, characteristics, and prevention with scalp cooling. Breast Cancer Res. Treat. 2018, 171, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Adderley, H.; Alameddine, M.; Armstrong, A.; Arundell, D.; Fox, R.; Harries, M.; Lim, J.; Salih, Z.; Tetlow, C.; Wong, H.; Thorp, N. Permanent hair loss associated with taxane chemotherapy use in breast cancer: A retrospective survey at two tertiary UK cancer centres. Eur. J. Cancer Care (Engl.) 2021, 30, e13395. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.M.; Haberland, N.I.; Miteva, M.; Wikramanayake, T.C. Chemotherapy-induced alopecia by docetaxel: Prevalence, treatment and prevention. Curr. Oncol. 2024, 31, 5709–5721. [Google Scholar] [CrossRef]
- Núñez-Torres, R.; Martín, M.; García-Sáenz, J.Á.; Rodrigo-Faus, M.; Del Monte-Millán, M.; Tejera-Pérez, H.; Pita, G.; de la Torre-Montero, J.C.; Pinilla, K.; Herraez, B.; Peiró-Chova, L.; Bermejo, B.; Lluch, A.; González-Neira, A. Association between ABCB1 genetic variants and persistent chemotherapy-induced alopecia in women with breast cancer. JAMA Dermatol. 2020, 156, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Blümel, J.E.; Lavín, P.; Vallejo, M.S.; Sarrá, S. Menopause or climacteric, just a semantic discussion or has it clinical implications? Climacteric 2014, 17, 235–241. [Google Scholar] [CrossRef]
- Nguyen, M.; Kraft, S. Approaches to management of endocrine therapy-induced alopecia in breast cancer patients. Support. Care Cancer 2025, 33, 199. [Google Scholar] [CrossRef]
- Lacouture, M.E.; Dréno, B.; Ascierto, P.A.; Dummer, R.; Basset-Seguin, N.; Fife, K.; et al. Characterization and management of Hedgehog pathway inhibitor-related adverse events in patients with advanced basal cell carcinoma. Oncologist 2016, 21, 1218–1229. [Google Scholar] [CrossRef]
- Wang, L.C.; Liu, Z.Y.; Gambardella, L.; Delacour, A.; Shapiro, R.; Yang, J.; Sizing, I.; Rayhorn, P.; Garber, E.A.; Benjamin, C.D.; Williams, K.P.; Taylor, F.R.; Barrandon, Y.; Ling, L.; Burkly, L.C. Conditional disruption of hedgehog signaling pathway defines its critical role in hair development and regeneration. J. Invest. Dermatol. 2000, 114, 901–908. [Google Scholar] [CrossRef]
- Migden, M.R.; Guminski, A.; Gutzmer, R.; Dirix, L.; Lewis, K.D.; Combemale, P.; Herd, R.M.; Kudchadkar, R.; Trefzer, U.; Gogov, S.; Pallaud, C.; Yi, T.; Mone, M.; Kaatz, M.; Loquai, C.; Stratigos, A.J.; Schulze, H.J.; Plummer, R.; Chang, A.L.; Cornélis, F.; Lear, J.T.; Sellami, D.; Dummer, R. Treatment with two different doses of sonidegib in patients with locally advanced or metastatic basal cell carcinoma (BOLT): A multicentre, randomised, double-blind phase 2 trial. Lancet Oncol. 2015, 16, 716–728. [Google Scholar] [CrossRef]
- Ferguson, J.S.; Hannam, S.; Toholka, R.; Chong, A.H.; Magee, J.; Foley, P. Hair loss and Hedgehog inhibitors: A class effect? Br. J. Dermatol. 2015, 173, 262–264. [Google Scholar] [CrossRef]
- Sibaud, V.; Sollena, P. Dermatologic toxicities to inhibitors of cyclin-dependent kinases CDK 4 and 6: An updated review for clinical practice. Ann. Dermatol. Venereol. 2023, 150, 208–212. [Google Scholar] [CrossRef]
- Tripathy, D.; Im, S.A.; Colleoni, M.; Franke, F.; Bardia, A.; Harbeck, N.; et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): A randomised phase 3 trial. Lancet Oncol. 2018, 19, 904–915. [Google Scholar] [CrossRef] [PubMed]
- Im, S.A.; Mukai, H.; Park, I.H.; Masuda, N.; Shimizu, C.; Kim, S.B.; et al. Palbociclib plus letrozole as first-line therapy in postmenopausal Asian women with metastatic breast cancer: Results from the phase III, randomized PALOMA-2 study. J. Glob. Oncol. 2019, 5, JGO.18.00173. [Google Scholar] [CrossRef] [PubMed]
- Purba, T.S.; Ng’andu, K.; Brunken, L.; Smart, E.; Mitchell, E.; Hassan, N.; et al. CDK4/6 inhibition mitigates stem cell damage in a novel model for taxane-induced alopecia. EMBO Mol. Med. 2020, 12, e11031. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.M.; Bergstra, S.A.; Kerschbaumer, A.; Sepriano, A.; Aletaha, D. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update https://doi.org/10.1136/ard-2022-223356 (doi.org in Bing) Free Law Project; CourtListener. Taxotere (Docetaxel) Products Liability Litigation, MDL No. 2740—Docket. Ann. Rheum. Dis. 2023, 82, 3–18. Available online: https://www.courtlistener.com/docket/17279738/in-re-taxotere-docetaxel-products-liability-litigation/ (accessed on 7 December 2025).
- Fraenkel, L.; Bathon, J.M.; England, B.R.; StClair, E.W.; Arayssi, T.; Carandang, K.; et al. 2021 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res. (Hoboken) 2021, 73, 924–939. [Google Scholar] [CrossRef] [PubMed]
- Klareskog, L.; van der Heijde, D.; de Jager, J.P.; Gough, A.; Kalden, J.; Malaise, M.; et al. Therapeutic effect of the combination of etanercept and methotrexate compared with each drug alone in patients with rheumatoid arthritis: Double-blind randomized controlled trial. N. Engl. J. Med. 2000, 343, 1586–1593. [Google Scholar] [CrossRef]
- Lalani, R.; Lyu, H.; Vanni, K.; Solomon, D.H. Low-dose methotrexate and mucocutaneous adverse events: Results of a systematic literature review and meta-analysis of randomized controlled trials. Arthritis Care Res. (Hoboken) 2020, 72, 1140–1146. [Google Scholar] [CrossRef]
- van Ede, A.E.; Laan, R.F.; Rood, M.J.; Huizinga, T.W.; van de Laar, M.A.; van Denderen, C.J.; Westgeest, T.A.; Romme, T.C.; de Rooij, D.J.; Jacobs, M.J.; de Boo, T.M.; van der Wilt, G.J.; Severens, J.L.; Hartman, M.; Krabbe, P.F.; Dijkmans, B.A.; Breedveld, F.C.; van de Putte, L.B. Effect of folic or folinic acid supplementation on the toxicity and efficacy of methotrexate in rheumatoid arthritis: A forty-eight week, multicenter, randomized, double-blind, placebo-controlled study. Arthritis Rheum. 2001, 44, 1515–1524. [Google Scholar] [CrossRef]
- Judicial Panel on Multidistrict Litigation (JPML). IN RE: Taxotere (Docetaxel) Products Liability Litigation. MDL No. 2740. Transfer Order; JPML: Washington, DC, USA, 2016; Available online: https://www.jpml.uscourts.gov/sites/jpml/files/MDL-2740-Initial_Transfer-09-16.pdf (accessed on 7 December 2025).
- Judicial Panel on Multidistrict Litigation. MDL Statistics Report—Distribution of Pending MDL Dockets by Actions Pending—July 1, 2025 . Judicial Panel on Multidistrict Litigation: Washington, DC, USA, 2025. Available online: https://www.jpml.uscourts.gov/sites/jpml/files/Pending_MDL_Dockets_By_Actions_Pending-July-1-2025_0.pdf (accessed on 7 December 2025).
- Judicial Panel on Multidistrict Litigation. MDL Statistics Report—Distribution of Pending MDL Dockets by District—October 1, 2025 . Judicial Panel on Multidistrict Litigation: Washington, DC, USA, 2025. Available online: https://www.jpml.uscourts.gov/sites/jpml/files/Pending_MDL_Dockets_By_District-October-1-2025.pdf (accessed on 7 December 2025).
- United States District Court; Eastern District of Louisiana. MDL-2740: IN RE: Taxotere (Docetaxel) Products Liability Litigation—MDL Docket Page . Available online: https://www.laed.uscourts.gov/case-information/mdl-mass-class-action/taxotere (accessed on 7 December 2025).
- United States District Court; Eastern District of Louisiana. Order and Reasons, IN RE: Taxotere (Docetaxel) MDL No. 16-2740 . Rec. Doc. 16778. 21 May 2024. Available online: https://www.govinfo.gov/content/pkg/USCOURTS-laed-2_16-md-02740/pdf/USCOURTS-laed-2_16-md-02740-86.pdf (accessed on 7 December 2025).
- Project, Free Law; CourtListener. Taxotere (Docetaxel) Products Liability Litigation, MDL No. 2740—Docket . Available online: https://www.courtlistener.com/docket/17279738/in-re-taxotere-docetaxel-products-liability-litigation/ (accessed on 7 December 2025).
- European Medicines Agency (EMA). Spontaneous Adverse Drug Reactions—Subgroup Report . EMA/HMA: London, UK, 2018; Available online: https://www.ema.europa.eu/en/documents/report/spontaneous-adverse-drug-reactions-subgroup-report_en.pdf (accessed on 7 December 2025).
- Rolfes, L.; van Hunsel, F.; van der Linden, L.; Taxis, K.; van Puijenbroek, E. The quality of clinical information in adverse drug reaction reports by patients and healthcare professionals: A retrospective comparative analysis. Drug Saf. 2017, 40, 607–614. [Google Scholar] [CrossRef]
- Inch, J.; Watson, M.C.; Anakwe-Umeh, S. Patient versus healthcare professional spontaneous adverse drug reaction reporting: A systematic review. Drug Saf. 2012, 35, 807–818. [Google Scholar] [CrossRef]
- Uesawa, Y. Adverse effect predictions based on computational toxicology techniques and large-scale databases. Yakugaku Zasshi 2018, 138, 185–190. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Tan, A.R.; Im, S.A.; Mattar, A.; Colomer, R.; Stroyakovskii, D.; Nowecki, Z.; De Laurentiis, M.; Pierga, J.Y.; Jung, K.H.; Schem, C.; Hogea, A.; Badovinac Crnjevic, T.; Heeson, S.; Shivhare, M.; Kirschbrown, W.P.; Restuccia, E.; Jackisch, C.; FeDeriCa Study Group. Fixed-dose combination of pertuzumab and trastuzumab for subcutaneous injection plus chemotherapy in HER2-positive early breast cancer (FeDeriCa): A randomised, open-label, multicentre, non-inferiority, phase 3 study. Lancet Oncol. 2021, 22, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Ventura, I.; Salcedo, N.P.; Pérez-Bermejo, M.; Pérez-Murillo, J.; Tejeda-Adell, M.; Tomás-Aguirre, F.; Legidos-García, M.E.; Murillo-Llorente, M.T. Pertuzumab in combination with trastuzumab and docetaxel as adjuvant doublet therapy for HER2-positive breast cancer: A systematic review. Int. J. Mol. Sci. 2025, 26, 1908. [Google Scholar] [CrossRef]
- Yajima, A.; Uesawa, Y. A comprehensive analysis of adverse events associated with HER2 inhibitors approved for breast cancer using the FDA Adverse Event Reporting System (FAERS). Pharmaceuticals 2025, 18, 1510. [Google Scholar] [CrossRef] [PubMed]
- Genentech, Inc. Rituxan (rituximab) Injection, for Intravenous Use; U.S. Prescribing Information; Food and Drug Administration: Silver Spring, MD, USA, 2021; Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/103705s5464lbl.pdf (accessed on 7 December 2025).
- Puiu, T.; Reimer, D.; Sokumbi, O. Rituximab-induced alopecia universalis in a patient with bullous pemphigoid. J. Drugs Dermatol. 2022, 21, 894–895. [Google Scholar] [CrossRef]
- Oke, A.R.; Young-Min, S. Successful treatment of alopecia universalis with rituximab therapy. Rheumatology (Oxford) 2020, 59, keaa109.005. [Google Scholar] [CrossRef]
- Saris, L.M.H.; Vlooswijk, C.; Kaal, S.E.J.; Nuver, J.; Bijlsma, R.M.; van der Hulle, T.; Kouwenhoven, M.C.M.; Tromp, J.M.; Lalisang, R.I.; Bos, M.E.M.M.; van der Graaf, W.T.A.; Husson, O. A negative body image among adolescent and young adult (AYA) cancer survivors: Results from the population-based SURVAYA study. Cancers 2022, 14, 5243. [Google Scholar] [CrossRef]
- Tallon, B.; Blanchard, E.; Goldberg, L.J. Permanent chemotherapy-induced alopecia: Case report and review of the literature. J. Am. Acad. Dermatol. 2010, 63, 333–336. [Google Scholar] [CrossRef]
- Lefevre, T.; Kruszynski, J.; Hamill, M.; et al. Permanent hair loss associated with taxane chemotherapy use in breast cancer: A retrospective survey at two tertiary UK cancer centres. Breast 2020, 54, 74–81. [Google Scholar] [CrossRef]
- Kluger, N.; Jacot, W.; Frouin, E.; Rigau, V.; Poujol, S.; Dereure, O.; Guillot, B.; Romieu, G.; Bessis, D. Permanent scalp alopecia related to breast cancer chemotherapy by sequential fluorouracil/epirubicin/cyclophosphamide (FEC) and docetaxel: A prospective study of 20 patients. Ann. Oncol. 2012, 23, 2879–2884. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Kim, I.R.; Choi, E.K.; Im, Y.H.; Park, Y.H.; Ahn, J.S.; Lee, J.E.; Nam, S.J.; Lee, H.K.; Park, J.H.; et al. Permanent chemotherapy-induced alopecia in patients with breast cancer: A 3-year prospective cohort study. Oncologist 2019, 24, 414–420. [Google Scholar] [CrossRef]
- Nozawa, K.; Toma, S.; Shimizu, C. Distress and impacts on daily life from appearance changes due to cancer treatment: A survey of 1,034 patients in Japan. Glob. Health Med. 2023, 5, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Browall, M.; Gaston-Johansson, F.; Danielson, E. Postmenopausal women with breast cancer: Their experiences of the chemotherapy treatment period. Cancer Nurs. 2006, 29, 34–42. [Google Scholar] [CrossRef]
- European Organisation for Research and Treatment of Cancer (EORTC). EORTC QLQ-BR42 Module (English, Final Version); EORTC: Brussels, Belgium, 2024; Available online: https://www.eortc.org/app/uploads/sites/2/2024/04/BR42-Module-English-FINAL.doc (accessed on 7 December 2025).
- Bjelic-Radisic, V.; Cardoso, F.; Cameron, D.; Brain, E.; Kuljanic, K.; da Costa, R.A.; Conroy, T.; Inwald, E.C.; Serpentini, S.; Pinto, M.; Weis, J.; Morag, O.; Lindviksmoen Astrup, G.; Tomaszweksi, K.A.; Pogoda, K.; Sinai, P.; Sprangers, M.; Aaronson, N.; Velikova, G.; Greimel, E.; Arraras, J.; Bottomley, A. EORTC Quality of Life Group and Breast Cancer Group. An international update of the EORTC questionnaire for assessing quality of life in breast cancer patients: EORTC QLQ-BR45. Ann. Oncol. 2020, 31, 283–288. [Google Scholar] [CrossRef]
- Williams, J.; Wood, C.; Cunningham-Warburton, P. A narrative study of chemotherapy-induced alopecia. Oncol. Nurs. Forum 1999, 26, 1463–1468. [Google Scholar]
- Boehmke, M.M.; Dickerson, S.S. Symptom, symptom experiences, and symptom distress encountered by women with breast cancer undergoing current treatment modalities. Cancer Nurs. 2005, 28, 382–389. [Google Scholar] [CrossRef]
- Shen, X.F.; et al. Efficacy of scalp cooling for prevention of chemotherapy-induced alopecia: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5090–5103. [Google Scholar] [PubMed]
- Trujillo-Martín, M.M.; de Armas-Castellano, A.; González-Hernández, Y.; González-Pacheco, H.; Infante-Ventura, D.; Del Pino-Sedeño, T.; Ramallo-Fariña, Y.; Abt-Sack, A.; Rueda Domínguez, A.; Serrano-Aguilar, P. Scalp cooling for the prevention of chemotherapy-induced alopecia: Systematic review and meta-analysis. Rev. Esp. Salud Publica 2023, 97, e202303024. (In Spanish) [Google Scholar]
- Duvic, M.; Lemak, N.A.; Valero, V.; Hymes, S.R.; Farmer, K.L.; Hortobagyi, G.N.; Trancik, R.J.; Bandstra, B.A.; Compton, L.D. A randomized trial of minoxidil in chemotherapy-induced alopecia. J. Am. Acad. Dermatol. 1996, 35, 74–78. [Google Scholar] [CrossRef]
- Godse, K.; De, A.; Vedamurthy, M.; Shankar, D.S.K.; Shah, B.; Girdhar, M.; Bhat, R.; Ganjoo, A.; Tahiliani, S.; Patil, A. Low-dose oral minoxidil in the treatment of alopecia: Evidence- and experience-based consensus statement of Indian experts. Int. J. Trichology 2023, 15, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Kuo, A.M.; Reingold, R.E.; Ketosugbo, K.F.; Pan, A.; Kraehenbuehl, L.; Dusza, S.; Gajria, D.; Lake, D.E.; Bromberg, J.F.; Traina, T.A.; Fornier, M.N.; Gucalp, A.; D’Alessandro, B.M.; Rotemberg, V.; Dauscher, M.; Shapiro, J.; Goldfarb, S.B.; Markova, A.; Lacouture, M.E. Oral minoxidil for late alopecia in cancer survivors. Breast Cancer Res. Treat. 2024, 208, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Taggart, L.R.; Ozolins, L.; Hardie, H.; Nyhof-Young, J. Look good feel better workshops: A “big lift” for women with cancer. J. Cancer Educ. 2009, 24, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Tamai, N.; Kanai, H.; Osaka, M.; Kondo, K.; Yamazaki, T.; Sanada, H.; Kamibeppu, K. Effects of the appearance care program for breast cancer patients receiving chemotherapy: A mixed method study. Cancer Rep. (Hoboken) 2020, 3, e1242. [Google Scholar] [CrossRef]
- Vagnini, D.; Grassi, M.M.; Valenti, F.; Bombardieri, E.; Saita, E. Beauty therapy to support psychosocial recovery from oncological care: A qualitative research on the lived experience of women with breast cancer treated with chemotherapy. Curr. Oncol. 2024, 31, 2527–2541. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of data curation and construction of analysis datasets.
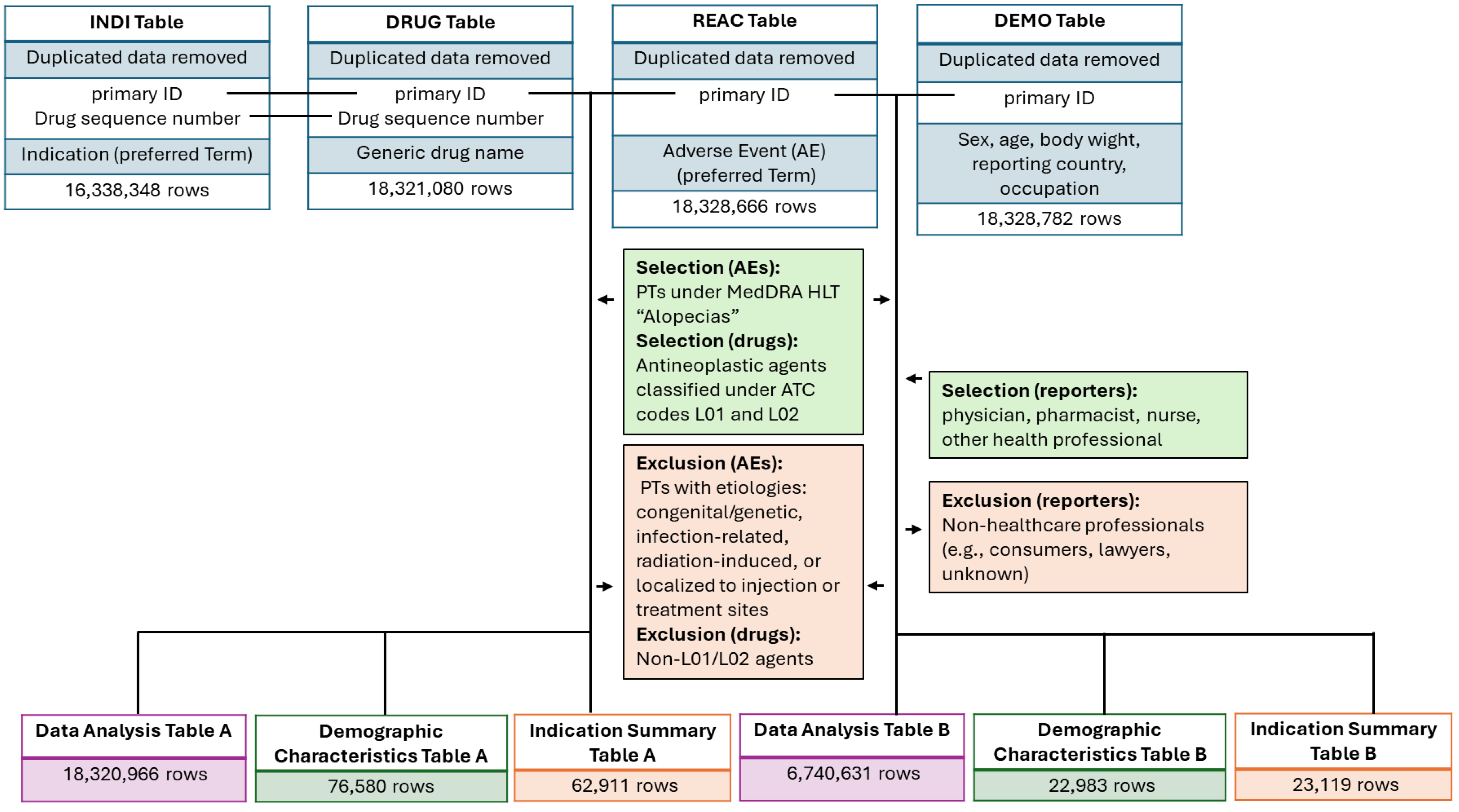
Figure 2.
Structure of the 2 × 2 contingency table used for disproportionality analysis in the FAERS database.
Figure 2.
Structure of the 2 × 2 contingency table used for disproportionality analysis in the FAERS database.
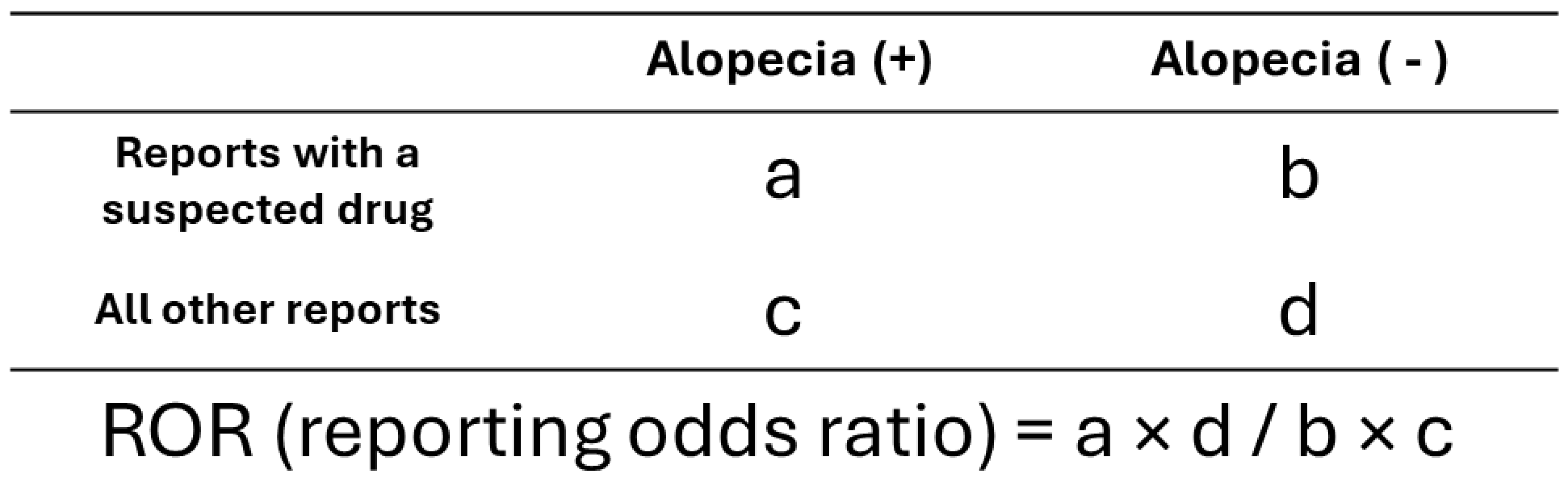
Figure 3.
Case-based distribution of reporter types for alopecia-related adverse event reports in FAERS.
Figure 3.
Case-based distribution of reporter types for alopecia-related adverse event reports in FAERS.
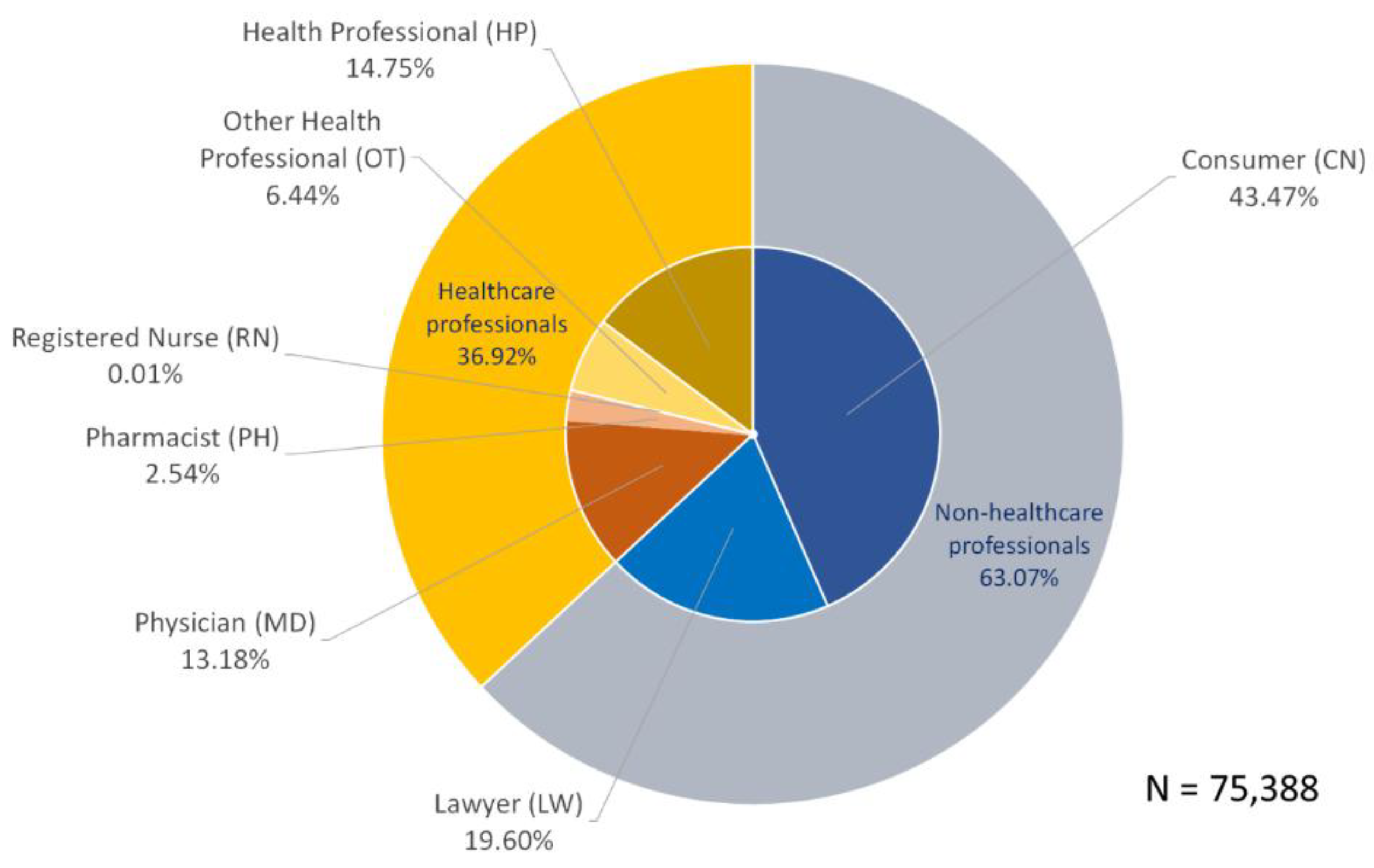
Figure 4.
Case-based heatmap of alopecia-related adverse event reports by drug and reporter occupation.
Figure 4.
Case-based heatmap of alopecia-related adverse event reports by drug and reporter occupation.
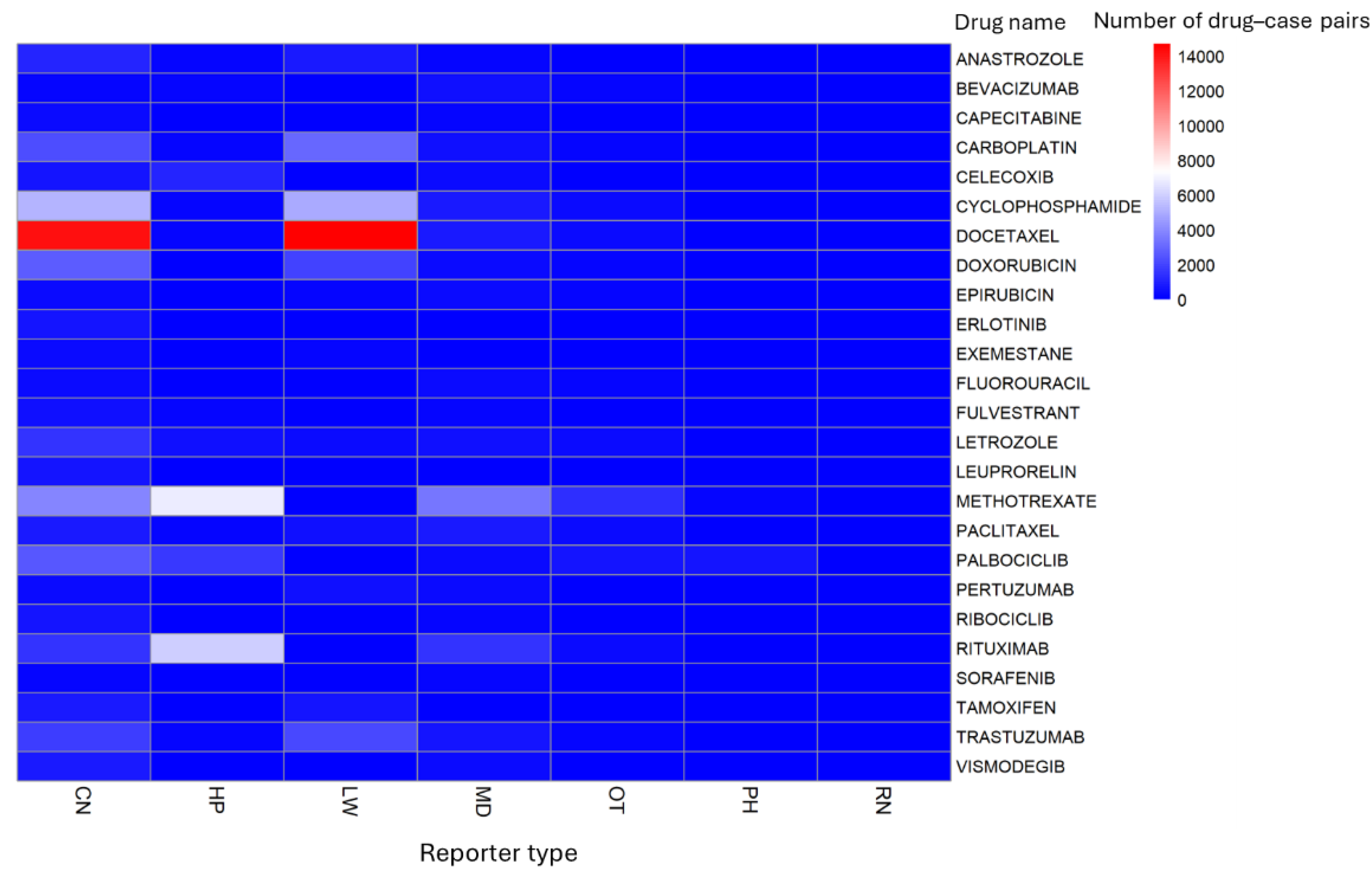
Figure 5.
Comparison of drug-specific lnRORs for alopecia-related adverse events between all reporters and HCPs.
Figure 5.
Comparison of drug-specific lnRORs for alopecia-related adverse events between all reporters and HCPs.
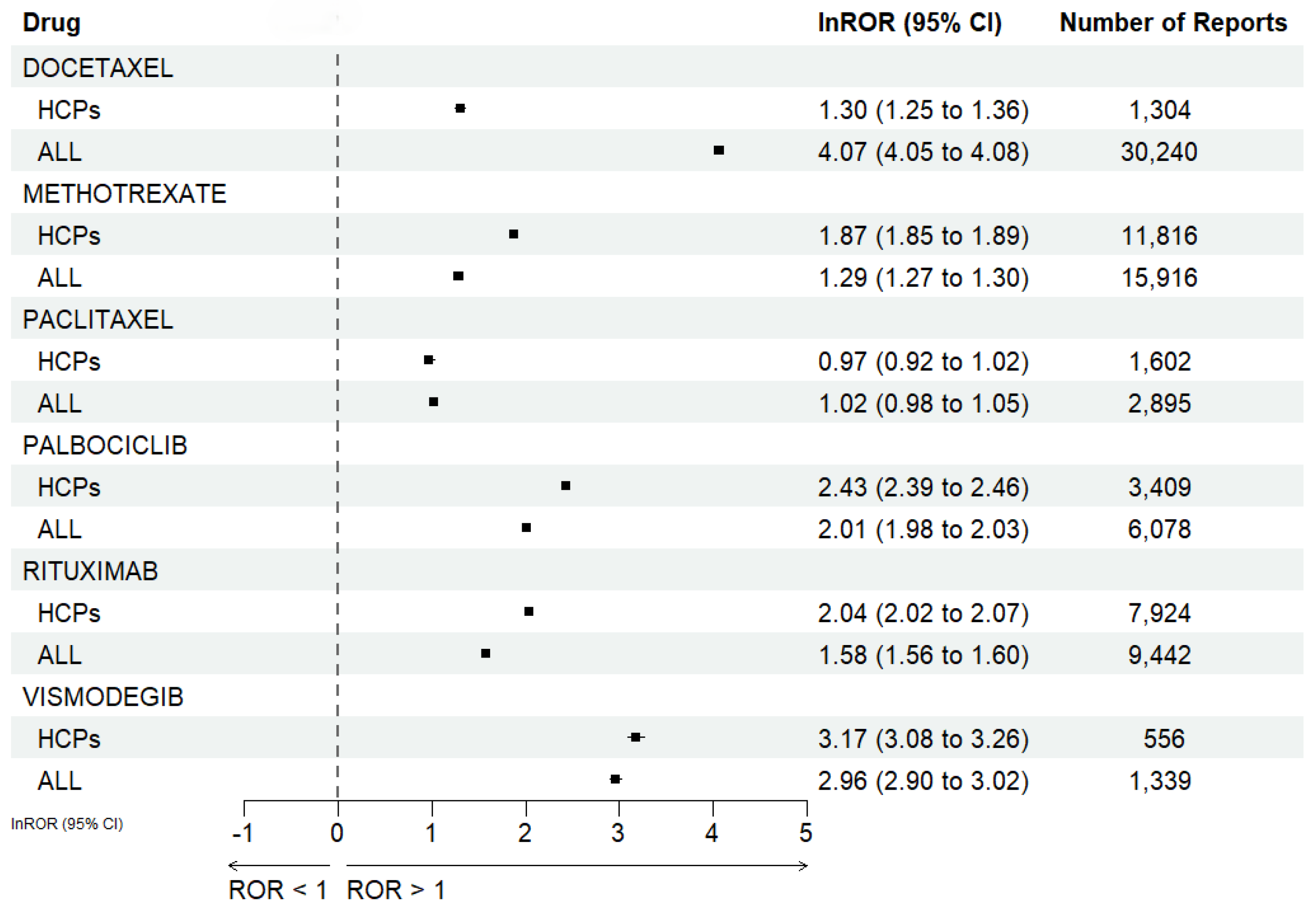
Figure 6.
Volcano plot of L01 and L02 drugs for alopecia-related adverse events based on reports from HCPs.
Figure 6.
Volcano plot of L01 and L02 drugs for alopecia-related adverse events based on reports from HCPs.
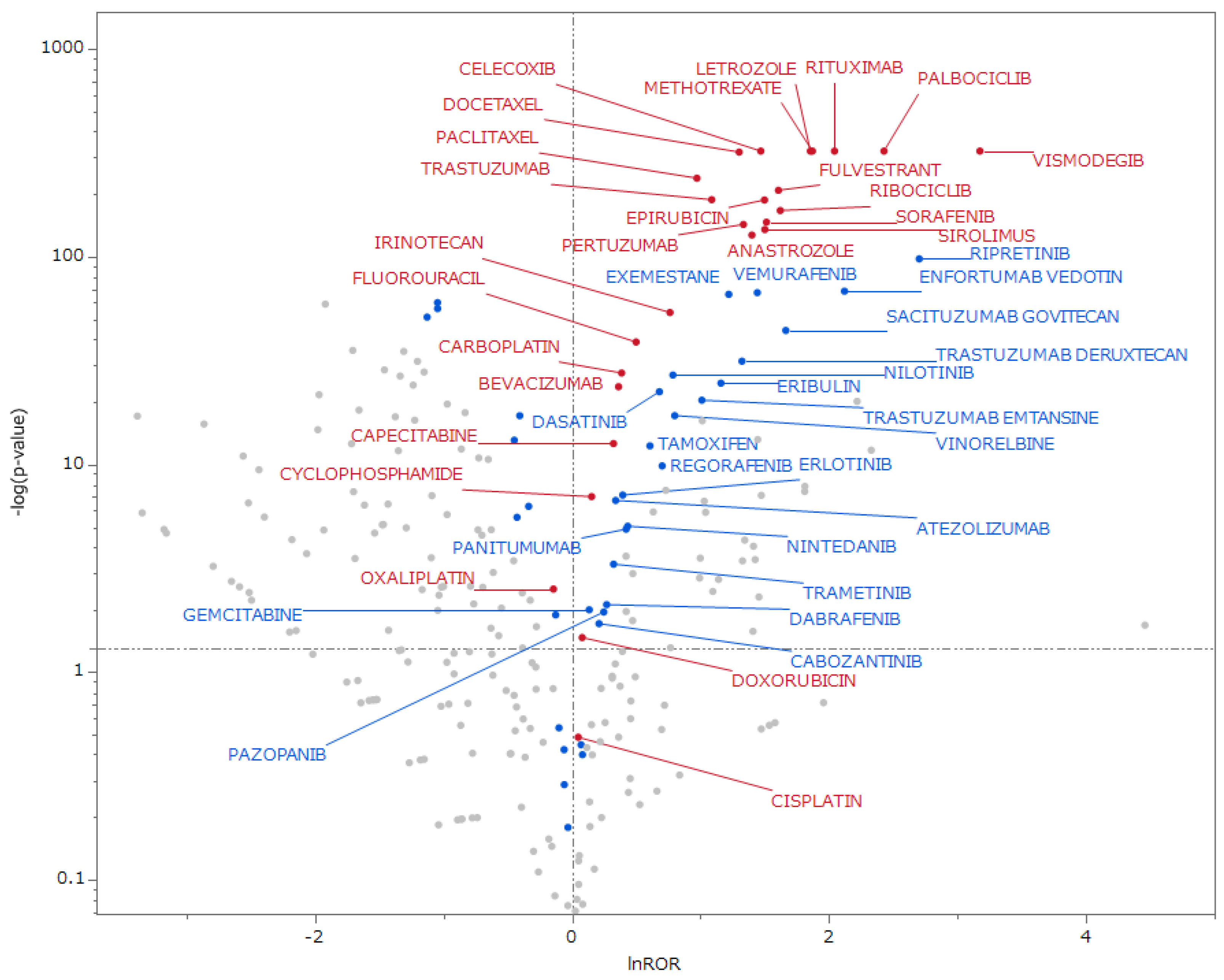
Table 2.
Number of reports by PTs for alopecia-related adverse events.
| a. All Reporter Types | b. Healthcare Professionals Only | |||
|---|---|---|---|---|
| Adverse Event | Number of Reports | Adverse Event | Number of Reports | |
| ALOPECIA | 135,323 | ALOPECIA | 49,986 | |
| MADAROSIS | 17,871 | MADAROSIS | 754 | |
| ALOPECIA AREATA | 1,203 | ALOPECIA AREATA | 469 | |
| ALOPECIA TOTALIS | 294 | DIFFUSE ALOPECIA | 176 | |
| DIFFUSE ALOPECIA | 278 | ALOPECIA TOTALIS | 130 | |
| HYPOTRICHOSIS | 168 | ALOPECIA SCARRING | 74 | |
| ALOPECIA SCARRING | 105 | ANDROGENETIC ALOPECIA | 52 | |
| ANDROGENETIC ALOPECIA | 79 | HYPOTRICHOSIS | 40 | |
| ALOPECIA UNIVERSALIS | 61 | ALOPECIA UNIVERSALIS | 32 | |
| LICHEN PLANOPILARIS | 18 | LICHEN PLANOPILARIS | 14 | |
| FOLLICULAR MUCINOSIS | 15 | FOLLICULAR MUCINOSIS | 13 | |
| NON-SCARRING ALOPECIA | 4 | NON-SCARRING ALOPECIA | 4 | |
Reports submitted by HCPs included physicians, pharmacists, nurses, health professionals, and other HCPs, as defined by occupation codes in the DEMO table.
Table 3.
Top 25 drugs with the highest number of alopecia-related reports.
| a. All Reporter Types | b. Healthcare Professionals Only | ||||
| (n = 155,419) | (n = 51,744) | ||||
| Rank | Drug Name | Number of Reports | Drug Name | Number of Reports | |
| 1 | DOCETAXEL | 37,305 | METHOTREXATE | 11,863 | |
| 2 | METHOTREXATE | 16,038 | RITUXIMAB | 7,929 | |
| 3 | CYCLOPHOSPHAMIDE | 14,557 | PALBOCICLIB | 3,470 | |
| 4 | RITUXIMAB | 9,454 | CELECOXIB | 1,728 | |
| 5 | CARBOPLATIN | 8,258 | PACLITAXEL | 1,623 | |
| 6 | DOXORUBICIN | 6,698 | LETROZOLE | 1,507 | |
| 7 | TRASTUZUMAB | 6,539 | DOCETAXEL | 1,408 | |
| 8 | PALBOCICLIB | 6,182 | CYCLOPHOSPHAMIDE | 1,374 | |
| 9 | LETROZOLE | 3,850 | TRASTUZUMAB | 1,091 | |
| 10 | PACLITAXEL | 3,233 | CARBOPLATIN | 979 | |
| 11 | ANASTROZOLE | 3,050 | BEVACIZUMAB | 909 | |
| 12 | CELECOXIB | 2,681 | FLUOROURACIL | 838 | |
| 13 | TAMOXIFEN | 2,104 | DOXORUBICIN | 779 | |
| 14 | PERTUZUMAB | 1,960 | EPIRUBICIN | 614 | |
| 15 | FLUOROURACIL | 1,487 | FULVESTRANT | 614 | |
| 16 | VISMODEGIB | 1,382 | CAPECITABINE | 588 | |
| 17 | FULVESTRANT | 1,290 | PERTUZUMAB | 585 | |
| 18 | EPIRUBICIN | 1,272 | VISMODEGIB | 571 | |
| 19 | BEVACIZUMAB | 1,210 | IRINOTECAN | 539 | |
| 20 | RIBOCICLIB | 1,192 | RIBOCICLIB | 481 | |
| 21 | CAPECITABINE | 994 | ANASTROZOLE | 469 | |
| 22 | EXEMESTANE | 961 | SORAFENIB | 469 | |
| 23 | LEUPRORELIN | 926 | CISPLATIN | 440 | |
| 24 | ERLOTINIB | 923 | SIROLIMUS | 434 | |
| 25 | SORAFENIB | 826 | OXALIPLATIN | 410 | |
Reports submitted by HCPs included physicians, pharmacists, nurses, health professionals, and other HCPs, as defined by occupation codes in the DEMO table.
Table 4.
Associations of drugs with alopecia-related adverse events.
| a. All Reporter Types | |||||
|---|---|---|---|---|---|
| drug | ROR | 95%CI [lower, upper] | lnROR | 95%CI [lower, upper] | p-value |
| DOCETAXEL | 58.31 | [57.46, 59.17] | 4.07 | [4.05, 4.08] | p < 0.001 |
| VISMODEGIB | 19.35 | [18.24, 20.52] | 2.96 | [2.90, 3.02] | p < 0.001 |
| TRASTUZUMAB | 8.23 | [8.00, 8.47] | 2.11 | [2.08, 2.14] | p < 0.001 |
| ANASTROZOLE | 8.02 | [7.70, 8.35] | 2.08 | [2.04, 2.12] | p < 0.001 |
| TAMOXIFEN | 7.60 | [7.23, 7.99] | 2.03 | [1.98, 2.08] | p < 0.001 |
| PALBOCICLIB | 7.44 | [7.25, 7.64] | 2.01 | [1.98, 2.03] | p < 0.001 |
| LETROZOLE | 6.60 | [6.38, 6.84] | 1.89 | [1.85, 1.92] | p < 0.001 |
| CYCLOPHOSPHAMIDE | 6.59 | [6.46, 6.72] | 1.89 | [1.87, 1.90] | p < 0.001 |
| PERTUZUMAB | 6.19 | [5.88, 6.51] | 1.82 | [1.77, 1.87] | p < 0.001 |
| CARBOPLATIN | 5.94 | [5.79, 6.09] | 1.78 | [1.76, 1.81] | p < 0.001 |
| EPIRUBICIN | 5.13 | [4.83, 5.44] | 1.63 | [1.58, 1.69] | p < 0.001 |
| DOXORUBICIN | 4.97 | [4.83, 5.10] | 1.60 | [1.58, 1.63] | p < 0.001 |
| RIBOCICLIB | 4.91 | [4.63, 5.21] | 1.59 | [1.53, 1.65] | p < 0.001 |
| RITUXIMAB | 4.86 | [4.75, 4.96] | 1.58 | [1.56, 1.60] | p < 0.001 |
| FULVESTRANT | 4.57 | [4.32, 4.84] | 1.52 | [1.46, 1.58] | p < 0.001 |
| EXEMESTANE | 4.22 | [3.94, 4.52] | 1.44 | [1.37, 1.51] | p < 0.001 |
| SORAFENIB | 3.95 | [3.68, 4.24] | 1.37 | [1.30, 1.44] | p < 0.001 |
| METHOTREXATE | 3.62 | [3.56, 3.68] | 1.29 | [1.27, 1.30] | p < 0.001 |
| PACLITAXEL | 2.76 | [2.66, 2.87] | 1.02 | [0.98, 1.05] | p < 0.001 |
| CELECOXIB | 2.10 | [2.02, 2.18] | 0.74 | [0.70, 0.78] | p < 0.001 |
| ERLOTINIB | 2.00 | [1.87, 2.14] | 0.69 | [0.63, 0.76] | p < 0.001 |
| FLUOROURACIL | 1.59 | [1.51, 1.68] | 0.46 | [0.41, 0.52] | p < 0.001 |
| BEVACIZUMAB | 1.06 | [1.00, 1.12] | 0.06 | [0.00, 0.12] | p = 0.042 |
| CAPECITABINE | 1.05 | [0.99, 1.12] | 0.05 | [-0.01, 0.12] | p = 0.114 |
| LEUPRORELIN | 0.99 | [0.93, 1.06] | -0.01 | [-0.08, 0.06] | p = 0.764 |
| b. Healthcare Professionals Only | |||||
| drug | ROR | 95%CI [lower, upper] | lnROR | 95%CI [lower, upper] | p-value |
| VISMODEGIB | 23.92 | [21.86, 26.17] | 3.17 | [3.08, 3.26] | p < 0.001 |
| PALBOCICLIB | 11.34 | [10.94, 11.75] | 2.43 | [2.39, 2.46] | p < 0.001 |
| RITUXIMAB | 7.72 | [7.53, 7.91] | 2.04 | [2.02, 2.07] | p < 0.001 |
| METHOTREXATE | 6.50 | [6.37, 6.63] | 1.87 | [1.85, 1.89] | p < 0.001 |
| LETROZOLE | 6.39 | [6.06, 6.74] | 1.86 | [1.80, 1.91] | p < 0.001 |
| RIBOCICLIB | 5.06 | [4.62, 5.55] | 1.62 | [1.53, 1.71] | p < 0.001 |
| FULVESTRANT | 4.99 | [4.60, 5.41] | 1.61 | [1.53, 1.69] | p < 0.001 |
| SORAFENIB | 4.54 | [4.14, 4.99] | 1.51 | [1.42, 1.61] | p < 0.001 |
| SIROLIMUS | 4.49 | [4.08, 4.94] | 1.50 | [1.41, 1.60] | p < 0.001 |
| EPIRUBICIN | 4.47 | [4.12, 4.85] | 1.50 | [1.42, 1.58] | p < 0.001 |
| CELECOXIB | 4.35 | [4.14, 4.56] | 1.47 | [1.42, 1.52] | p < 0.001 |
| ANASTROZOLE | 4.06 | [3.70, 4.46] | 1.40 | [1.31, 1.49] | p < 0.001 |
| PERTUZUMAB | 3.80 | [3.49, 4.13] | 1.33 | [1.25, 1.42] | p < 0.001 |
| DOCETAXEL | 3.68 | [3.48, 3.89] | 1.30 | [1.25, 1.36] | p < 0.001 |
| TRASTUZUMAB | 2.97 | [2.79, 3.16] | 1.09 | [1.03, 1.15] | p < 0.001 |
| PACLITAXEL | 2.64 | [2.51, 2.78] | 0.97 | [0.92, 1.02] | p < 0.001 |
| IRINOTECAN | 2.14 | [1.97, 2.34] | 0.76 | [0.68, 0.85] | p < 0.001 |
| FLUOROURACIL | 1.65 | [1.54, 1.76] | 0.50 | [0.43, 0.57] | p < 0.001 |
| CARBOPLATIN | 1.47 | [1.38, 1.57] | 0.39 | [0.32, 0.45] | p < 0.001 |
| BEVACIZUMAB | 1.44 | [1.35, 1.54] | 0.36 | [0.30, 0.43] | p < 0.001 |
| CAPECITABINE | 1.38 | [1.27, 1.50] | 0.32 | [0.24, 0.41] | p < 0.001 |
| CYCLOPHOSPHAMIDE | 1.17 | [1.10, 1.23] | 0.15 | [0.10, 0.21] | p < 0.001 |
| DOXORUBICIN | 1.08 | [1.01, 1.16] | 0.08 | [0.01, 0.15] | p = 0.034 |
| CISPLATIN | 1.05 | [0.96, 1.15] | 0.05 | [-0.05, 0.14] | p = 0.326 |
| OXALIPLATIN | 0.87 | [0.79, 0.95] | -0.14 | [-0.24, -0.05] | p = 0.003 |
Reports submitted by HCPs included physicians, pharmacists, nurses, health professionals, and other HCPs, as defined by occupation codes in the DEMO table.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



