
Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Background/Aim: Hepatitis D virus (HDV) infection is the most severe form of viral hepatitis but is under-recognized. We evaluated HDV screening frequency and clinical characteristics of HDV-positive patients in our liver center in the United States. Method: Patients with chronic hepatitis B (CHB) evaluated between January 2021 and December 2023 were included. For those tested anti-HDV(+), HDV RNA was performed and clinical data were recorded. Results: Among 1,337 (M=716, F=621) CHB patients, 93.3% were foreign-born. The cohort included 74.9% Asians, 12.3% Blacks, 9.1% Whites and 1.3% Hispanics. HDV screening significantly increased after 2011 reflecting an increase in HDV awareness. Patients aged 18-40 years had the highest screening rate of 58%. Overall, 13 (1.95%) were tested HDV positive and 11 were repeatedly HDV RNA(+). PWID was noted in 5 of 11. Despite low HBV DNA levels, all had ≥stage 2 fibrosis, and 7 had advanced stage 3-4 disease. After a median follow-up of 8.75 years, 8 (73%) developed hepatic decompensation and 4 had hepatocellular carcinoma. Conclusion: HDV screening reached 51.3% among our predominantly foreign-born CHB patients. The high prevalence of advanced fibrosis at diagnosis underscores the importance of HDV screening. Early diagnosis and effective therapy are urgently needed for this challenging disease.
Keywords:
HDV
; chronic hepatitis D
; anti-HDV
; HDV RNA
1. Introduction
The accurate prevalence of hepatitis D virus (HDV) infection is uncertain due to limited surveillance and reporting. Based on systematic reviews and meta-analysis, Stockdale et al estimated approximately 12 million people have HDV infection worldwide [1], and Chen et al. reported a significant higher global prevalence of 60 million.[2] Compared to hepatitis B virus (HBV) mono-infection, HDV co-infection generally has a more severe disease progression with a 3.2-fold higher risk in hepatocellular carcinoma(HCC), and about 2-fold increase in decompensated cirrhosis and mortality. [3]
Despite its significant clinical impact, hepatitis D is often under-recognized and under-diagnosed. United States is considered a low to intermediate HDV endemic region. [4,5] NHANES data from 2011 to 2016 estimated that approximately 357,000 Americans had either past or ongoing HDV infection. [6] Quest Diagnostics data of the United States (US) from 2016 to 2020 reported that only 6.7% of patients with chronic hepatitis B (CHB) were screened for HDV; among those tested, 2.2% were anti-HDV positive.[5] In 2013, Gish et al. reported an 8% prevalence of HDV in a cohort of CHB patients in California; the majority of those patients were born in the US. [7]
The variations in HDV prevalence across the US populations likely due to differences in HDV transmission patterns and inconsistent HDV screening practices. A recent Veterans Affairs (VA) study in a predominantly US-born CHB cohort reported a HDV prevalence of 3.3%. Among those tested anti-HDV positive, there were 31% White, 32.9% Black, 14.6% Hispanic/Latino, 5.1% Asian and 16.5% Others. [8] In the developed countries, persons who inject drugs (PWID), men who have sex with men (MSM) and immigrants from endemic regions were identified to have high risks for HDV transmission. [5,9,10]
HDV infection is not a reportable disease in the US, and there is no comprehensive nationwide surveillance.[11] The burden of HDV in the US may be underestimated especially among immigrants from endemic regions such as sub-Saharan Africa, Eastern Europe, and Asia.[1] The majority of the patients with CHB were foreign-born in our tertiary liver center. This study evaluated the rate of HDV infection among our CHB patients and the HDV screening practice of our hepatologists.
2. Study Population and Methods
This retrospective study was conducted at the Beth Israel Deaconess Medical Center (BIDMC), Boston, Massachusetts. USA and was approved by the Institutional Review Board (IRB). Adult patients (≥18 years) with a known diagnosis of CHB who were seen in the outpatient Liver Center between January 1, 2021, and December 31, 2023 were included. Both new referrals and follow-up patients seen in this time period were eligible. Patients were identified using chronic hepatitis B and hepatitis D specific ICD codes in Epic and WebOMR electronic medical records.
A systematic chart review was performed to capture demographic variables (age, sex, race/ethnicity, country of birth) for all the selected patients. The dates on which the patients underwent first HDV screening with an anti-HDV antibody were recorded. HDV screening patterns and demographic characteristics were analyzed. HDV prevalence was calculated as the proportion of anti-HDV positive individuals among those screened.
Patients with chronic hepatitis D were defined by the presence of anti-HDV and detectable HDV RNA. HDV RNA (Quest Diagnostics) results were available in medical records. For the anti-HDV (+) patients, detailed epidemiologic and clinical data were recorded. Risk factors for HBV/HDV transmission such as history of intravenous drug use (IVDU), blood transfusion, sexual exposure, occupational exposure, tattoos and body piercing were captured. Laboratory results included HBV tests (HBsAg, anti-HBs, HBeAg, HBV DNA), HCV biomarkers (anti-HCV, HCV RNA), anti-HIV, liver panel (ALT, AST, alkaline phosphatase, bilirubin, albumin), platelet and alpha-fetoprotein (AFP). Available liver imaging (liver ultrasound, FibroScan, and MRI) and liver biopsies reports were recoded. Hepatic fibrosis stage was assessed by available liver biopsy or FibroScan examination. Clinical features such as liver-related complications (cirrhosis, hepatocellular carcinoma, esophageal and gastric varices, ascites, hepatic encephalopathy) were systematically reviewed.
3. Statistical Analysis
GraphPad Prism Version 9.4.1 and EXCEL were applied for descriptive statistics and graphs. Two-sample t-tests were used to compare means between groups. Chi-square tests without Yates correction were used to compare categorical variables of groups.
4. Results
4.1. Characteristics of the CHB Patient Cohort
A total of 1337 patients with CHB were seen between January 2021 and December 2023 at our liver center. The dates of their initial visits were between 2/11/1999 and 12/15/2023. 716 (53.6%) of them were males and 621 (46.4%) were females, with a mean age of 54.7 years. Information on country of birth was available for 1302 (97.4%) patients. Among them, 1247 (93.3%) were foreign-born, and only 55 (6.7%) were born in the United States. The racial distribution of the cohort included 1002 (74.9%) Asians, 165 (12.3%) Blacks, 121 (9.1%) Whites, 17 (1.3%) Hispanics, and 31 (2.3%) patients with unknown race. [Figure 1]
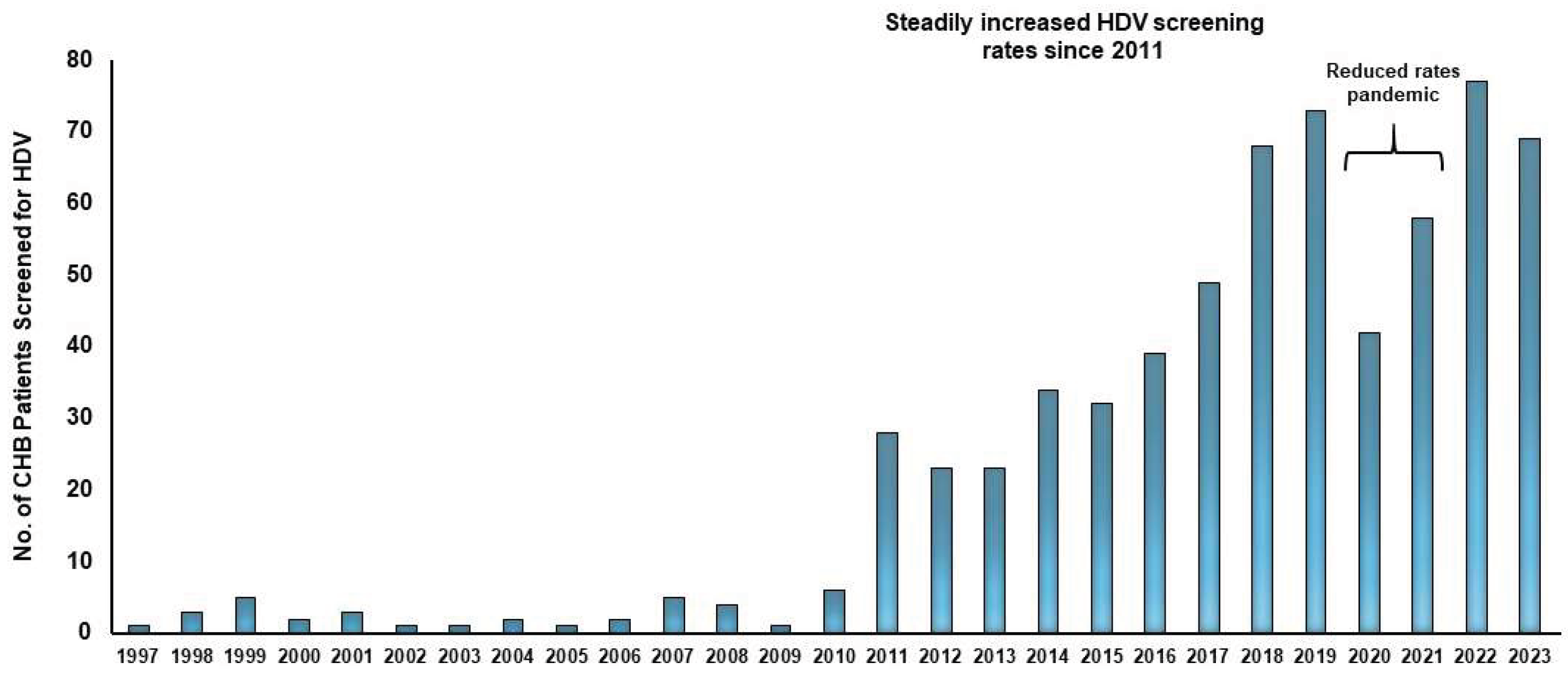
The trend of HDV screening increased over the years, with a significant increase after 2011. [Figure 2] A total of 655 anti-HDV tests were conducted between 2011 and 2023. Of note, a temporary drop in screening occurred during 2020-2021 which was due to limited in-person visits during the COVID-19 pandemic.
Among those with known country of birth, 668 patients (51.3%) underwent HDV screening at least once. For those with HDV screening, US-born patients were older than the foreign-born ones (mean age 62.6 years vs. 52.9 years, p=0.0005) and had a lower screening rate (36% vs. 50.8%, p=0.036). Among the foreign-born patients, HDV screening frequencies were relatively uniform across racial groups: 50% in Asians, 52% in Blacks, 52% in Whites and 63% among Hispanics.
HDV screening rates varied by age. Individuals aged 18-40 years had the highest screening rate (58%) followed by those aged 41-60 years (49.8%) and lowest for those aged >60 years (46%), p=0.02. Among non-US born patients, Asian males were screened more frequently than females. (55.4% vs. 44.8%, p=0.0008) For the other non-US born races, there was no significant differences in HDV screening between male and female genders.
A total of 13 (8 males, 5 females) out of the 668 CHB patients were tested anti-HDV positive; the HDV prevalence was, therefore, 1.95% in our cohort. Eleven of the 13 patients were confirmed to have chronic hepatitis D with repeatedly detectable HDV RNA. None of the patients with hepatitis D had HIV infection.

Table 1.
Characteristics of the 13 anti-HDV(+) patients.
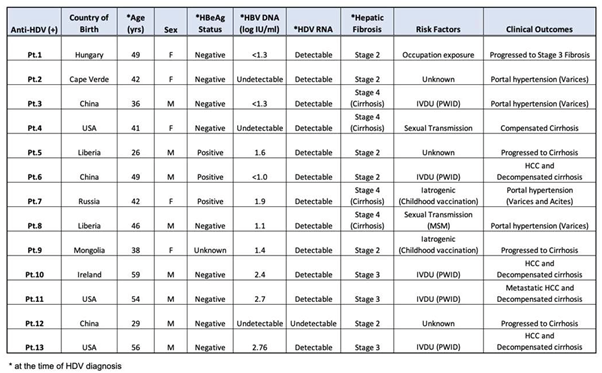
The majority, 10 or 77%, of the anti-HDV positive patients were foreign-born. Among them, 4 were from Asia, 3 from Africa, 2 from Europe and 1 from Russia. The risk factors for HDV transmission could be identified in 7 of the foreign-born patients; PWID in 3, MSM in 1, occupational exposure in 1 and childhood vaccination with contaminated needle were likely the causes in 2. Among the 3 US-born patients, 2 were PWID. The mean age when positive anti-HDV was first noted was 43.6 years with range between 26 and 59 years. At baseline, all 13 patients were documented to have at least stage 2 hepatic fibrosis either by liver biopsy or Fibroscan. Advanced fibrosis was present in 7 (54%); 4 had cirrhosis and 3 had stage 3 fibrosis. HBeAg status was available for 12 patients; 9 were HBeAg (-) and 3 were HBeAg (+). Seven patients were on HBV antiviral therapy at baseline with either undetectable or <1.6 log IU/mL HBV DNA. The remaining six patients were untreated initially; all had relatively low HBV DNA levels ranging from <1.3 to 2.76 log IU/mL. Despite the low level of HBV DNA replication, 7 of them had at least stage 3 fibrosis when hepatitis D was identified. All untreated patients were subsequently started on nucleos(t)ide analog therapy and achieved suppressed HBV DNA levels at follow up.
At a median follow-up duration of 8.75 years, 8 of 11 patients with persistently detectable HDV RNA experienced hepatic complications. Four (Pts 6,10,11,13) developed hepatic decompensation and hepatocellular carcinoma (HCC), and the other 4 (Pts 2,3,7,8) experienced progressive portal hypertension with varices, and/or ascites. All the patients with HCC had history of injection drug use and prior HCV exposure. Pt.6 and Pt.10 responded to Y90 radioembolization, Pt.13 underwent liver transplantation without HCC recurrence. Pt. 11 developed metastatic HCC despite radioembolization and was in palliative care.
Only 3 (Pts 5, 6, 7) patients received pegylated interferon (peg-IFN) for chronic hepatitis D. The other patients either had contraindication to interferon or refused therapy. Pt. 5 achieved undetectable HDV RNA during two years of therapy but relapsed within one month post treatment. He later progressed to cirrhosis. Pt. 6 was non-compliant to peg-IFN due to side-effects and later developed hepatic decompensation and HCC. Pt. 7 received peg-IFN and later bulevirtide. She could not tolerate full dose peg-IFN and had no virological response to bulevirtide monotherapy. The patient later developed hepatic decompensation and had successful liver transplantation.
5. Discussion
The majority of the patients with CHB in our tertiary liver center were foreign-born. Overall, 51.3% of 1337 CHB patients evaluated in our liver clinics between 1999 and 2023 had at least one anti-HDV test. In comparison, Wong et al. reported only 6.7% of CHB patients in the Quest cohort (2016–2020) and 19.7% in the Veterans Affairs cohort (2010–2020) were tested for HDV.[5] The discrepancy in screening rates was likely a reflection of the heightened awareness of hepatitis D among the liver specialists. Our rate of HDV screening increased significantly in the period 2011-2023 compared to the decade 1999-2010.
The prevalence of positive anti-HDV was 1.95% among those screened. We found that 58% of the patients aged 18 to 40 years had anti-HDV testing. In contrast, only 46% of those older than 60 years were screened. US-born patients were older and were less frequently tested for HDV. The anti-HDV positivity rate was much lower in our study with predominantly immigrants compared to studies focusing on persons with high risk for HDV transmission. A San Francisco study reported that among PWID with positive HBsAg between 1998-2000, the prevalence of HDV RNA was 35.6%. The study also reported that the prevalence of HDV viremia was 14.3% in patients with < 9 years of drug use and 61.1% in patients with >30 years of IVDU.[10] Similarly, a study in a cohort of PWID in Baltimore found the rate of positive anti-HDV among patients with CHB increased from 29% in 1988-1989 to 50% in 2005-2006. [9]
There were a number of studies that focused on the HDV prevalence in the predominantly US-born populations. In a recent publication on 4817 veterans with HBV infection, 3.3% were positive for anti-HDV.[8] The result was consistent with a meta-analysis from 1998 to 2019 that the anti-HDV prevalence among HBsAg positive persons visiting liver clinics in the WHO regions of North America was 3.3%.[1] Another recent nationwide US study noted 1.2% anti-HDV positivity among HBsAg positive samples. 33% of the anti-HDV positive samples were positive for HDV RNA.[12] The HDV prevalence among foreign-born population in the US remains uncertain. Our study did not focus on high-risk groups such as PWID. Injection drug use, however, was the risk noted in 5 out of 8 patients with identifiable route of HDV transmission. This finding highlighted the importance of obtaining a detailed clinical history on potential HDV exposures regardless the place of birth of the patients.
It is recognized that patients with HBV and HDV co-infection generally have more severe liver disease and clinical outcomes compared to those with HBV mono-infection. In a VA study, John BV et al aimed to identify the factors associated with a composite outcome of HCC, decompensation, and liver-related mortality in hepatitis D. They found that the anti-HDV(+) patients had a higher incidence of composite liver-related outcome compared to those with HBV alone at both 5 years (23.84 vs. 7.98, p < 0.001) and 10 years (19.14 vs. 10.18, p < 0.001). Since only 29 (28%) of the anti-HDV positive patients had HDV RNA testing, the exact number of patients with chronic hepatitis D was uncertain.[8] This VA study reported that cirrhosis was present in 12.7% of the anti-HDV positive patients at diagnosis compared to 7.5% of those without HDV. We also observed advanced stage 3-4 fibrosis in 7 out of 13 anti-HDV positive patients and 8 of them developed hepatic decompensation or cirrhosis after a median follow up duration of 8.75 years. In our practice, younger patients aged between 18 and 40 years were more likely to have HDV screening. In reality, 9 (69%) of the patients with HDV infection were older than 40 years. Considering the potential severe clinical outcomes associated with HDV infection, it underscored the importance to perform HDV screening regardless of the age of the patients.
Our study results concurred with the published literature that patients with HDV infection more frequently had HBeAg negative CHB with low level of HBV DNA replication and had established fibrosis. [13,14] Lee et al, for example, reported 39 of 55 (71%) patients with chronic hepatitis D had either undetected or HBV DNA <3 log IU/ml. Moreover, all but 1 of the 55 subjects had > stage 2 fibrosis at the time of HDV screening.[15]. These observations highlight the importance to consider the diagnosis of chronic hepatitis D in CHB patients with low HBV DNA replication and advanced liver disease.
The significant global variations of disease prevalence, the lack of diagnostic tests and treatment options especially in resource-limited regions [16] contributed to different national and international HDV screening and management strategies. The European Association for the Study of the Liver (EASL) [17] and Asian-Pacific Association for the Study of the Liver (APASL) [18] recommended HDV testing in all HBsAg-positive patients. The current American Association for the Study of Liver Diseases (AASLD) guideline recommends only risk-based screening for HDV.[19] The WHO proposed screening all HBsAg positive patients for HDV, particularly in countries with high HDV prevalence, and prioritizing screening for patients with advanced liver disease, high risk behaviors and migrants from HDV endemic area. [20] Risk-based HDV screening would miss a large number of HDV cases, [21] In our study, 3 of the 13 anti-HDV positive cases had uncertain routes of HDV acquisition. The lack of provider awareness, diagnostic infrastructures and financial resources, however, would make universal HDV screening for patients with CHB challenging. The detailed cost effectiveness of HDV screening data is unavailable. Given the high incidence of adverse clinical outcomes and impact on health care associated with chronic hepatitis D, it is reasonable to conduct anti-HDV screening for all CHB patients at least once with repeat testing on those with high risks in regular intervals.
Currently treatment options for HDV infection are limited but timely diagnosis is still important for appropriate monitoring and reducing HDV transmission. Pegylated interferon has been the only therapy for chronic hepatitis D but it is poorly tolerated and are contraindicated in decompensated liver disease. In a meta-analysis on peg-IFN therapy, Abdrakhman A et al reported that undetectable HDV RNA at 24 weeks post therapy was only 29% (range 17-49%) after 48 to 96 weeks of treatment.[22] Bulevirtide, the sodium taurocholate co-transporting polypeptide (NTCP) inhibitor is currently approved in Europe and Australia. [23,24] The combination of peg-IFN alfa-2a and bulevirtide 2 mg or 10 mg for 96 weeks were associated with a virological response rate of 32 % and 46% at 24 weeks post therapy, respectively.[25] Bulevirtide is pending Food and Drug Administration (FDA) approval in the US.
Our study has some limitations due to its retrospective chart review design. We could not determine the exact timing of HDV acquisition and some patients had incomplete clinical and laboratory data. Since not all our patients with chronic hepatitis B were screened for HDV, its true prevalence may be underestimated. The strengths of the study were our large foreign-born patient populations and long follow-up duration of over 8 years on those HDV infected subjects. These provided valuable insights on our HDV screening practice, the chronic hepatitis D disease progression and management challenges.
In conclusion, our study highlighted the unmet needs of HDV infection. As new, effective therapy is becoming available, universal HDV screening in all HBsAg-positive patients is an effective strategy for early diagnosis and management of chronic hepatitis D.
Author Contributions
Conceptualization: DTYL, RR, SBS; Data curation: SA, RR, SBS, MR, NK, KH, FU, UIJC, KUR, AU; Formal analysis: DTYL, SA, RR, SBS; Methodology: DTYL, SA, RR, SBS; Supervision: DTYL; Visualization: SA, RR, SBS, DTYL; Writing- original draft: SA, RR, SBS, DTYL; Writing- review & editing: RA, SP, SA, DTYL.
Funding
This research was funded by Gilead Sciences, Inc (Grant number-IN-US-980-6662).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Beth Israel Deaconess Medical Center (protocol code 2023P000555 approved on 3/25/2024).”.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The data presented in this study originate from the author’s original research involving HDV screening. Due to ethical and privacy considerations, the data are not publicly available.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Stockdale, A.J.; Kreuels, B.; Henrion, M.Y.; Giorgi, E.; Kyomuhangi, I.; de Martel, C.; Hutin, Y.; Geretti, A.M. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J. Hepatol. 2020, 73, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Shen, D.-T.; Ji, D.-Z.; Han, P.-C.; Zhang, W.-M.; Ma, J.-F.; Chen, W.-S.; Goyal, H.; Pan, S.; Xu, H.-G. Prevalence and burden of hepatitis D virus infection in the global population: a systematic review and meta-analysis. Gut 2018, 68, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Razavi, H.A. Hepatitis D double reflex testing of all hepatitis B carriers in low-HBV- and high-HBV/HDV-prevalence countries. J Hepatol 2023, 79, 576–580. [Google Scholar] [CrossRef]
- Kushner, T.; Serper, M.; Kaplan, D.E. Delta hepatitis within the Veterans Affairs medical system in the United States: Prevalence, risk factors, and outcomes. J. Hepatol. 2015, 63, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.J.; Kaufman, H.W.; Niles, J.K.; Chen, C.; Yang, Z.; Kapoor, H.; Cheung, R.; Gish, R.G. Low Performance of Hepatitis Delta Virus Testing Among 2 National Cohorts of Chronic Hepatitis B Patients in the United States. Am. J. Gastroenterol. 2022, 117, 2067–2070. [Google Scholar] [CrossRef] [PubMed]
- Patel, E.U.; Thio, C.L.; Boon, D.; Thomas, D.L.; Tobian, A.A.R. Prevalence of Hepatitis B and Hepatitis D Virus Infections in the United States, 2011–2016. Clin. Infect. Dis. 2019, 69, 709–712. [Google Scholar] [CrossRef]
- Gish, R.G.; Yi, D.H.; Kane, S.; Clark, M.; Mangahas, M.; Baqai, S.; A Winters, M.; Proudfoot, J.; Glenn, J.S. Coinfection with hepatitis B and D: Epidemiology, prevalence and disease in patients in Northern California. J. Gastroenterol. Hepatol. 2013, 28, 1521–1525. [Google Scholar] [CrossRef]
- John, B.V.; Bastaich, D.; Amoli, M.M.; Wong, R.J.; Evon, D.M.; Rogal, S.S.; Ross, D.B.; Morgan, T.R.; Spector, S.A.; Villada, G.; et al. Association of HDV infection and HCC, hepatic decompensation, and all-cause and liver-related death in a national cohort. Hepatology 2024, 81, 1822–1835. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Farzadegan, H.; Feld, J.J.; Mehta, S.H.; Winters, M.; Glenn, J.S.; Kirk, G.D.; Segev, D.L.; Nelson, K.E.; Marks, M.; et al. Prevalence, Correlates, and Viral Dynamics of Hepatitis Delta among Injection Drug Users. J. Infect. Dis. 2010, 202, 845–852. [Google Scholar] [CrossRef]
- Mahale, P.; Aka, P.V.; Chen, X.; Liu, P.; Fram, B.J.; Wang, A.S.; Simenel, S.; Tseng, F.-C.; Chen, S.; Edlin, B.R.; et al. Hepatitis D Viremia Among Injection Drug Users in San Francisco. J. Infect. Dis. 2018, 217, 1902–1906. [Google Scholar] [CrossRef]
- Assadi-Rad, M.; E Acosta, B.; Hesterman, M.C.; Fallon, B.S.; Hill, R.L.; Farnsworth, E.W.; Barbeau, B.; Vilven, D.; Lynch, K.M.; Weller, M.L. Hepatitis Delta Virus Reporting Requirements in the United States and Territories: A Systematic Review. Open Forum Infect. Dis. 2024, 11. [Google Scholar] [CrossRef]
- Stark, D.L.; Falekun, S.; Jorgensen, S.; Slev, P. Prevalence of Hepatitis D in the United States. J. Appl. Lab. Med. 2025, 10, 1133–1139. [Google Scholar] [CrossRef]
- Fouad, R.; Abdo, M.; Eldeen, H.G.; Sabry, D.; Atef, M.; Ahmed, R.; Zayed, N. Influence of delta virus infection on the virologic status in Egyptian patients with chronic hepatitis B virus genotype D. J. Med Virol. 2015, 88, 837–842. [Google Scholar] [CrossRef]
- Shah, P.A.; Choudhry, S.; Reyes, K.J.C.; Lau, D.T.Y. An update on the management of chronic hepatitis D. Gastroenterol. Rep. 2019, 7, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.M. Hepatitis B virus infection. N Engl J Med 1997, 337, 1733–1745. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.T.Y.; Jackson, K.; A Picchio, C.; Kramvis, A.; Sonderup, M.; Lemoine, M.; Matthews, G.; Howell, J.; Coffin, C.S.; Hellard, M.; et al. Availability of point-of-care HBV tests in resource-limited settings. Lancet Gastroenterol. Hepatol. 2024, 9, 1073–1076. [Google Scholar] [CrossRef]
- European Association for the Study of the; L. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Organization, W.H. Guidelines for the prevention, diagnosis, care and treatment for people with chronic hepatitis B infection. 2024: Geneva.
- Nathani, R.; Leibowitz, R.; Giri, D.; Villarroel, C.; Salman, S.; Sehmbhi, M.; Yoon, B.H.; Dinani, A.; Weisberg, I. The Delta Delta: Gaps in screening and patient assessment for hepatitis D virus infection. J. Viral Hepat. 2022, 30, 195–200. [Google Scholar] [CrossRef]
- Abdrakhman, A.; Ashimkhanova, A.; Almawi, W.Y. Effectiveness of pegylated interferon monotherapy in the treatment of chronic hepatitis D virus infection: A meta-analysis. Antivir. Res. 2021, 185, 104995. [Google Scholar] [CrossRef] [PubMed]
- Koh, C.; Heller, T.; Glenn, J.S. Pathogenesis of and New Therapies for Hepatitis D. Gastroenterology 2019, 156, 461–476.e1. [Google Scholar] [CrossRef]
- Park, J.; Sayed, A.; Nasir, S.A.; Lim, J.K. Advances in treatment of hepatitis delta virus infection: Update on novel investigational drugs. World J. Virol. 2025, 14, 102673. [Google Scholar] [CrossRef] [PubMed]
- Asselah, T.; Chulanov, V.; Lampertico, P.; Wedemeyer, H.; Streinu-Cercel, A.; Pântea, V.; Lazar, S.; Placinta, G.; Gherlan, G.S.; Bogomolov, P.; et al. Bulevirtide Combined with Pegylated Interferon for Chronic Hepatitis D. New Engl. J. Med. 2024, 391, 133–143. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Racial distributions of the 1,337 patients with chronic hepatitis B.
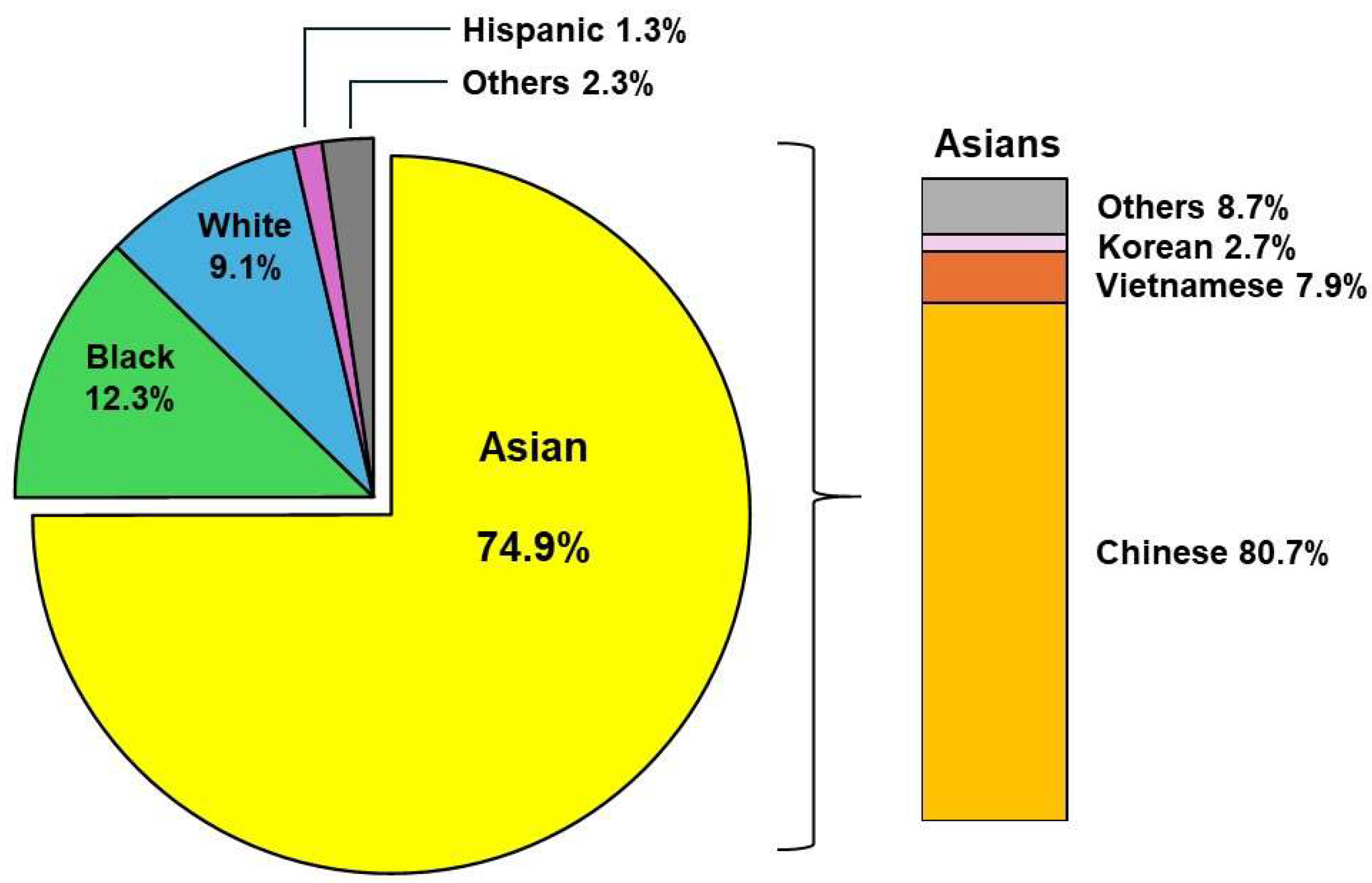
Figure 2.
The trend of anti-HDV screening among CHB patients at our liver center (1997 to 2023).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



