
Submitted:
01 September 2025
Posted:
02 September 2025
You are already at the latest version
Abstract
Background: Since the introduction of the hepatitis B virus (HBV) vaccination program in Oman in 1990, the HBV prevalence has markedly decreased. However, hepatitis D virus (HDV) infection, which is associated with progressive liver disease in patients with chronic HBV, remains understudied in the Omani population. This study aimed to estimate HDV’s seroprevalence, characterize its virological and clinical features, and identify factors associated with anti-HDV positivity among adults with an HBV infection in Oman. Methods: We conducted a multicenter cross-sectional study in 2024 at two referral hospitals and two polyclinics in Oman. Adult patients with chronic HBV (HBsAg-positive for > 6 months) were enrolled. Demographic, clinical, laboratory, imaging, and elastography data were collected. The total anti-HDV antibodies were tested using an ELISA; HDV RNA was tested for anti-HDV-positive or equivocal results. Fibrosis was assessed using transient elastography and clinical evaluation. Logistic regression identified predictors independently associated with anti-HDV positivity. Results: Among 639 patients (59.3% male; mean age of 46.6 ± 8.8 years), 36 patients were anti-HDV-positive, resulting in an HDV seroprevalence of 5.63% (95% CI: 4.10–7.70). Only one anti-HDV-positive patient had detectable HDV RNA, which became undetectable on follow-up without HDV treatment. The anti-HDV-positive patients were more frequently female and had a higher frequency of prior blood transfusions. In a multivariable analysis, blood transfusions were independently associated with anti-HDV positivity (OR of 36.72, 95% CI: 4.03–334.24; p =0.001), whereas male sex was associated with lower odds of being anti-HDV-positive (OR of 0.10, 95% CI: 0.04–0.28; p < 0.001). All the anti-HDV-positive patients had mild fibrosis (F0–F1). Conclusions: Our study demonstrated an anti-HDV prevalence of 5.63% among adults with chronic HBV infection in Oman, while active viremia appeared to be rare. Blood transfusions were the main identified risk factor. Given the very low HDV viremia and potential limitations of the assay used, targeted screening of higher-risk groups may be efficient, but universal one-time screening remains reasonable where feasible to avoid missed cases.
Keywords:
hepatitis B virus
; hepatitis D virus
; seroprevalence
; risk factors
; Oman
; fibrosis
1. Introduction
Hepatitis delta virus (HDV) is a hepatotropic virus with a small, single-stranded ribonucleic acid (RNA) genome (1). This genome encodes a delta antigen without an outer coat or envelope. Therefore, HDV uses hepatitis B virus surface antigen (HBsAg) protein as a coat or envelope for entry into hepatocytes. The replication of HDV produces two HDV antigens and a ribonucleoprotein complex. Although HBsAg is required for entry into the hepatocyte, other viral replication processes, such as assembly, release, and transmission, can occur without the need for HBsAg (2).
Co-infection of hepatitis B virus (HBV) and HDV can occur at the same time or as an HDV superinfection of a patient with HBV. Simultaneous infection with HBV and HDV is associated with clearance of both viruses in most cases, whereas HDV superinfection in patients with HBV tends to persist, leading to a chronic infection associated with a worse clinical outcome than HBV monoinfection (3). This progressive course is characterized by rapid progression to advanced fibrosis, cirrhosis, decompensated cirrhosis, and development of hepatocellular carcinoma (HCC) (4).
The prevalence of chronic HDV infection, as estimated by the World Health Organization (WHO), is around 4.5% of patients with an HBsAg infection (5). This prevalence has marked geographical variations, with the highest prevalence in Mongolia, China, Pakistan, Iran, Turkey, Romania, and sub-Saharan Africa (6). A recent study by the Polaris Observatory Collaborators evaluating HBsAg-positive patients in 25 countries demonstrated the highest anti-HDV prevalence of 60% in Mongolia. However, after adjustment for the total number of patients with HBV and positive HDV RNA, China had the highest absolute number of HDV RNA-positive cases (7).
Since HDV is dependent on HBV for cell entry and infectivity, HBV vaccination is expected to decrease the risk of HDV infection. A study from Italy by Pan et al. showed a marked reduction in the prevalence of HDV from 25% in 1983 to 8.3% in 1997, which was attributed to HBV vaccination (6). With the adoption of HBV vaccination in many countries around the globe, the incidence of new cases of HDV, as well as its prevalence, is expected to decrease markedly.
In Oman, the estimated chronic HBV prevalence was around 2–7% before a nationwide vaccination program was introduced in 1990 (8). Subsequent studies revealed a marked reduction in the HBV prevalence (8-10), with blood donor positivity declining from 4% in 1990 to 1% in 2010 (9). However, despite Oman’s proximity to HDV-endemic countries, local data on the HDV prevalence remain scarce. This study therefore sought to determine the prevalence of HDV in Oman and characterize the clinical features of patients with an HBV/HDV co-infection. It is predicted that prevalence data will provide important information for the selection of an appropriate HDV screening strategy in Oman.
2. Methods
2.1. Study Design and Patient Population
This multicenter cross-sectional study was conducted from January through December 2024 at two referral hospitals within the Medical City for Military and Security Services (MCMSS) and two affiliated polyclinics serving the northern and interior regions. These two hospitals and two polyclinics accept patients from all over Oman. Adult Omani patients with a chronic HBV infection, defined as persistent HBsAg positivity for more than six months, and under routine follow-up at one of the participating sites were included.
We excluded patients with isolated anti-HBc and those missing core data required to determine the primary outcome.
2.2. Data Collection
Demographic, clinical, and risk factor information (including information on prior transfusions, surgeries, travel to regions with high HDV endemicity, participants’ family history, alcohol consumption, and smoking) were collected from the clinical record and confirmed at clinic visits where feasible. Laboratory investigations, including liver biochemistry tests and serologies for HBV, HCV, HDV, and HIV, were conducted. Patients with a positive or equivocal total anti-HDV result were tested for HDV RNA as described below. Radiological data were also collected, including through an ultrasound and/or computer tomography of the abdomen and liver stiffness measurement (LSM) using vibration-controlled transient elastography (VCTE).
2.3. Serological Tests
A HBV infection was diagnosed based on the detection of HBsAg positivity for more than six months, along with detectable serum HBV DNA levels, assessed using the Abbott Real Time HBV assay (Abbott Molecular Inc., Wiesbaden, Germany) or the COBAS® AmpliPrep/COBAS® TaqMan® (version 2.0) assay (Roche Diagnostics, Branchburg, NJ, USA). The lower limits of detection for each assay were 12 and 15 IU/mL, respectively.
A HDV infection was diagnosed when total anti-HDV antibodies, predominantly IgG, were detected using a competitive enzyme-linked immunosorbent assay (ELISA) based on a two-step methodology. Testing was performed using a commercially available kit (HDV Ab ELISA, Dia.Pro Diagnostic Bioprobes S.r.l., Via G. Carducci 27, 20099 Sesto San Giovanni, Milan, Italy). According to the manufacturer, the assay demonstrates sensitivity and specificity greater than 98%. The tests were performed at the Central Public Health Laboratory (CPHL), Oman, and the anti-HDV antibody results were interpreted based on the ratio of the sample optical density at 450 nm (OD450) to the assay cut-off value (Co/S ratio). A Co/S ratio of < 0.9 was considered negative, 0.9–1.1 equivocal, and >1.1 positive for anti-HDV antibodies. In patients with positive or equivocal serology, HDV RNA testing was performed to confirm an active infection.
Testing for HDV RNA was performed through a real-time polymerase chain reaction (PCR) using the CFX96™ Real-Time PCR Detection System (BIO-RAD Laboratories, Hercules, CA, USA), following the manufacturer’s instructions. The assay’s lower limit of detection was 20 IU/mL (1.30 log IU/mL), with a quantification range from 50 to 3,500,000 IU/mL. Amplification was performed using reagents from Eurobio (Les Ulis, France) according to the manufacturer’s instructions
2.4. Statistical Analysis
Continuous variables were expressed as the mean ± the standard deviation (SD) or median (interquartile range, IQR), depending on the data distribution. Categorical variables were summarized as counts and percentages. Comparisons between the anti-HDV-positive and -negative patients were performed using an independent samples t-test or Mann–Whitney U test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables, as appropriate.
To identify factors associated with anti-HDV positivity, univariate logistic regression analyses were initially performed for demographic, clinical, and laboratory variables. Variables that were statistically significant in the univariate analysis were included in a multivariate logistic regression model to determine the independent predictors. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Statistical significance was defined as a two-tailed p-value of < 0.05.
All analyses were conducted using Stata version 14 (StataCorp LP; College Station, TX, USA).
2.5. Ethical Approval
Ethical approval for this study was obtained from the ethics committee of the Medical City for Military and Security Services (MCMSS), Muscat, Oman (ethical approval number AFMS-MREC: 001/2024). This ethical approval covered all the participating sites. The study was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki (2013 revision) issued by the World Medical Association. Information sheets were given to and consent forms were obtained from all the patients.
3. Results
3.1. Patient Characteristics
A total of 715 patients with chronic hepatitis B were screened, of whom 76 positive for anti-HBc and negative for HBsAg were excluded. The study ultimately included 639 HBsAg-positive adults from all the participating centers (Figure 1). Of these, 379 patients (59.3%) were male, with a mean age of 46.6 ± 8.8 years. Thirty-six patients (5.6%) were anti-HDV-positive, and only one was HDV RNA-positive. This patient subsequently cleared the infection spontaneously without specific HDV treatment.
Five patients were co-infected with HCV and one patient with HIV. Seven patients with HBV had received a liver transplant, four of them for decompensated cirrhosis and three for HCC.
A total of 109 patients (17.1%) were receiving antiviral therapy for HBV. Significant fibrosis (≥F2) was identified in 27 patients (4.23%), advanced fibrosis (≥F3) in 3 patients (0.47%), and cirrhosis (F4) in 13 (2.03%). Table 1 summarizes the demographic, clinical, and laboratory characteristics of the study population according to the participants’ anti-HDV status.
3.2. HDV Seroprevalence and Virological Findings
A total of 36 patients (5.6%) tested positive for total anti-HDV. Only one patient had detectable HDV RNA, which subsequently became undetectable during a follow-up without HDV treatment (Figure 2). The majority of patients were HBeAg-negative (607 patients, 94.99%), and the mean HBV DNA level was 3.18 ± 1.42 log10 IU/mL.
A comparison between the anti-HDV-positive and -negative patients revealed that the anti-HDV-positive patients were relatively younger (mean age of 44.0 vs. 46.8 years, p = 0.03) and the majority were female (80.1%). A history of blood transfusion was significantly more frequent among anti-HDV-positive patients than anti-HDV-negative patients (8.3% vs. 0.5%). There were no significant differences in regard to complications such as development of HCC or the requirement for liver transplantation or HBV treatment (Table 1).
Laboratory parameters, including the liver enzymes, bilirubin, albumin, and HBV DNA levels, were generally comparable between the anti-HDV-positive and -negative patients.
3.3. Fibrosis Assessment
Liver fibrosis was evaluated non-invasively through LSM with a FibroScan® device using VCTE (Echosens, Paris, France). Predefined cut-off values were applied to categorize the fibrosis severity: significant fibrosis (F2 Metavir) was ≥ 7.2 kPa, advanced fibrosis (F3 Metavir) was ≥ 8.8 kPa, and cirrhosis (F4 Metavir) was ≥ 11 kPa (11).
Cirrhosis was defined based on either an LSM of more than 11 kPa or a clinician’s determination of the patient as cirrhotic in the medical records. In cases where there was a discrepancy between the transient elastography score and the clinician’s assessment, the clinician’s evaluation was considered definitive.
Based on LSM and/or clinical evaluation, all the anti-HDV-positive patients had mild fibrosis (F0–F1) with a liver elasticity of < 7.2 kPas, while significant or advanced fibrosis (≥F2) was only observed in anti-HDV-negative patients (Table 1).
3.4. Factors Associated with Anti-HDV Positivity
In the univariate logistic regression analysis, female gender and a history of blood transfusion or surgery were significantly associated with anti-HDV positivity (Table 2). However, when adjustment for other covariates was performed in the multivariate analysis, blood transfusions were the strongest independent predictor of HDV positivity (OR of 36.72, 95% CI: 4.03–334.24; p = 0.001). Male gender was associated with significantly lower odds of anti-HDV positivity (OR of 0.10, 95% CI: 0.04–0.28; p < 0.001), indicating a protective effect not seen in females. An increasing age appeared to modestly reduce the likelihood of anti-HDV positivity (OR of 0.94, 95% CI: 0.90–0.99; p = 0.05). Although a history of surgery showed a potential association in the univariate analysis (OR of 2.31, 95% CI: 0.97–5.52; p = 0.05), this effect was not statistically significant in the multivariate model (OR 1.47, 95% CI: 0.53–4.08; p = 0.46), suggesting that it was not an independent risk factor in this patient population.
4. Discussion
Oman is geographically located near countries with a high HDV prevalence, such as Pakistan, Iran, and certain parts of India (5, 12, 13). Over the past two decades, both medical tourism and leisure travel to and from these regions have increased, potentially contributing to HDV exposure in the Omani population, especially individuals traveling for medical tourism (14). This study included patients from all regions of Oman and therefore provides a contemporary estimate of the HDV exposure among HBsAg-positive patients, reporting an anti-HDV prevalence of 5.63%. This prevalence is lower than that reported in a study by Aldhahri et al. in 1993, which investigated the prevalence of HDV among high-risk patients such as those undergoing hemodialysis and renal transplants (15). Aldhahri et al. identified anti-HDV in 7.7% of hemodialysis patients and 22.2% of renal transplant recipients, while none of the healthy HBsAg-positive controls tested positive for anti-HDV (15). This previous study targeted high-risk patients (dialysis and transplant recipients), limiting its generalizability to the broader population of HBsAg-positive patients. However, the current study included a broader and more representative sample of HBsAg-positive patients. In addition, the differences in the prevalence are most likely due to the use of the latest highly sensitive and specific assays to detect both HBV and HDV markers in the current study, as mentioned in the Methods Section, compared to the first-generation ELISA kits (Abbott Laboratories, USA) used in the previous study (16). Other factors that may have contributed to the lower prevalence in the current study are improvements in infection control measures in Oman, implementation of a national HBV vaccination program in 1990 (9), and implementation of strict blood transfusion safety measures (17).
Compared to its neighboring countries, Oman’s HDV prevalence falls within an intermediate range. Recent regional data show an anti-HDV prevalence among HBsAg-positive patients ranging from 0% to 21.8%, with most estimates ranging between 2 and 10%, depending on the studied population (18). Single-center studies reported HDV prevalences of 7.7% in Saudi Arabia, 6.6% in Iraq, and 0% in Yemen (18). The estimated pooled prevalence in the Eastern Mediterranean Region is 3.5%, indicating that Oman’s current HDV burden aligns with regional patterns but may be slightly higher. However, direct comparisons must be interpreted with caution due to differences in the sampling methods, population risk profiles, and assay characteristics (5).
In the current study, 5.63% of HBsAg-positive patients tested positive for anti-HDV antibodies. However, only one patient had detectable HDV RNA, the levels of which gradually decreased to become undetectable by the time this study was conducted without HDV treatment. The patient was offered pegylated interferon but refused it and started on entecavir for HBV. The presence of anti-HDV (IgG or total) antibodies in HBsAg-positive patients indicates prior exposure to HDV, while the presence of HDV RNA is required to confirm active replication of the virus (6). A recent systematic review and meta-analysis by Stockdale et al. including more than five thousand anti-HDV-positive patients reported detectable HDV RNA in 58.5% of cases (95% CI: 52.4–64.5), emphasizing that a significant number of anti-HDV-positive patients cleared the virus spontaneously and did not have an active infection (5). Furthermore, the meta-analysis by Stockdale, together with two other recent meta-analyses, reported that the HDV infection prevalence ranged from 4.5% to 13.0% among HBsAg-positive patients, with a higher prevalence of 14.6% to 18.6% among patients followed up at hepatology clinics. These reported prevalences are higher than those observed in our study. Such differences in the global HDV prevalence are most likely due to the use of different assays that differ markedly in their diagnostic accuracy due to the absence of a unified recommended diagnostic methodology, as well as limited access to HBV vaccination and effective HDV treatment in many countries with high HDV endemicity (5, 19, 20).
The high prevalence of anti-HDV positivity and HDVRNA negativity underscores the importance of including both serologic and molecular testing when planning HDV surveillance programs. Depending entirely on the anti-HDV seropositivity can cause overestimation of the active disease burden, particularly in countries where spontaneous viral clearance is common. In contrast, HDV RNA testing offers a more precise assessment of active viral replication, infectivity, and the disease burden. However, careful interpretation is advised as the diagnostic performance of HDVRNA tests is highly variable. Due to the high genetic heterogeneity of the HDV genome, some HDVRNA assays may produce false-negative results or underestimate the viral load for certain genotypes. In a study by Salpini et al. evaluating the performance of various quantitative HDVRNA assays across 30 laboratories, several assays underestimated the viral load by more than 1 log10 IU/mL, and while the linearity was generally good, only a few assays maintained accuracy at low HDVRNA levels (<1000 IU/mL). Overall, the assay performance was heterogeneous, underscoring the importance of careful assay selection and interpretation of HDVRNA results in clinical practice (21).
Our results, therefore, suggest that while past HDV exposure remains detectable in a subset of HBsAg-positive Omani patients, the actual prevalence of active HDV infection may be very low.
Our findings are particularly important because the majority of our patients were recruited from hepatology clinics, where higher rates of detectable HDV RNA would typically be expected (5). Several factors may explain our observations. Firstly, they may reflect a true reduction in active HDV infection in Oman, potentially due to improved HBV vaccination coverage, infection control measures, or reduced exposure to high-risk factors (9). Secondly, the anti-HDV-positive patients may have previously cleared the virus, consistent with the known persistence of anti-HDV antibodies after HDVRNA clearance (2). Thirdly, it is possible that differences in HDV genotypes across regions or over time may have contributed to the observed findings (22). Unfortunately, HDV genotyping could not be performed in our patients as only one patient had previously shown detectable HDV RNA, and the viral load at the time of this study was too low to allow for genotype testing. As a result, we were unable to explore the potential impact of different HDV genotypes on disease progression or viral characteristics in the Omani patients. Previous studies have identified eight different HDV genotypes that differ in their genomic sequence by at least 35% (23). Compared with genotype 2, which is most commonly found in the Middle East, genotype 1 is associated with a higher risk of adverse outcomes and lower remission rates. This may partly explain the high rate of spontaneous HDV clearance and the absence of advanced fibrosis observed in our patients, assuming that our patients were predominantly infected with genotype 2 (20),(24).
Our study’s findings raise an important question: should we recommend screening for all HBsAg-positive patients or limit screening to high-risk patients? Screening all HBsAg-positive patients for HDV is recommended by the European Association for the Study of the Liver (EASL) and the guidelines of the Asian Pacific Association for the Study of the Liver (APASL) (25, 26). The guidance from the American Association for the Study of Liver Diseases (AASLD) is different as they recommend screening only high-risk HBsAg patients, such as those co-infected with HIV, men who have sex with men, and immigrants from areas with a high HDV prevalence (27). Investigation of HDV risk factors revealed that a history of blood transfusion was a strong independent predictor of anti-HDV positivity (OR of 34.91), highlighting the key role of parenteral exposure in HDV transmission. Notably, this finding persisted despite Oman’s implementation of strict blood transfusion safety measures, including mandatory screening for HBV in all blood donors and adherence to international transfusion safety standards (28). The residual risk may be attributed to infections acquired before the introduction of strict screening programs or from exposure in private medical or emergency settings where strict testing may not have been consistently applied (29). In addition, many patients from Oman had traveled to neighboring countries with high HDV endemicity for medical tourism. Although a history of travel to endemic areas was not statistically significant, the specific purpose of travel, whether for leisure or medical care, was not examined in detail. Similar trends in countries with strict transfusion safety standards indicate that transfusions received longer ago and lifetime exposure still contribute to HDV infection (30, 31)
While co-infections with viruses such as HCV and HIV were not significantly associated with anti-HDV positivity in our study, this was most likely due to the low prevalence of HDV and the limited number of high-risk patients, as the majority of HIV patients in Oman are managed by infectious disease specialists, even in cases with HBV or HCV co-infections. Other studies have demonstrated a significantly higher prevalence, such as 15% among individuals with an HIV co-infection or a pooled OR of 10.0 among anti-HCV-positive patients(32),(33). The small number of patients with HIV and HCV co-infections in our study also limited our ability to establish strong statistical associations. Nonetheless, our data suggest that, in our clinical setting, co-infection with HCV or HIV does not appear to predict anti-HDV positivity. This reinforces the importance of using context-specific screening strategies rather than depending on global risk assumptions, especially in regions where HDV’s epidemiology remains incompletely explored and inadequately characterized.
More than half of the anti-HDV-positive patients had no known risk factors for HDV infection. This finding is in agreement with multiple previous studies highlighting that HDV can occur outside well-known high-risk groups (34, 35). A recent study from Spain by Palom et al. showed that 60% of those who tested positive for anti-HDV had no known risk factors for HDV infection (34). The same study showed that by applying universal screening for HDV, the prevalence of anti-HDV positivity remained similar, but the absolute number of diagnosed cases increased fivefold. Therefore, relying on risk factors may not be an appropriate approach.
Multiple factors must be taken into consideration before the implementation of a screening program in Oman. These include the prevalence of HBV, which was demonstrated to be low among individuals born after the introduction of the HBV vaccination program (9), the prevalence of HDV, and the availability of accurate and cost-effective diagnostic tests (36) and safe and effective treatments (37).
Our study found that anti-HDV-positive patients were slightly younger than anti-HDV-negative patients. However, this age difference was only marginally non-significant after adjusting for other factors. The mean age of the entire study cohort was 46.61 ± 8.76, while the mean age of those with anti-HDV positivity was 44.00 ± 7.73, indicating that most of the patients were most likely infected with HBV before the introduction of HBV vaccination in Oman in 1990 (10). Multiple studies have demonstrated the important role of HBV vaccination in reducing the incidence and prevalence of HDV infection (38, 39). An Italian study by Stroffolini et al. evaluated the incidence of acute HDV from 1991 to 2019, demonstrating a significant decrease from 3.2 per million population in 1987 to 0.04 per million in 2019, following the introduction of compulsory HBV vaccination. This trend highlights the effectiveness of HBV vaccination in controlling HDV transmission (38).
Our study is different from most previous studies, which demonstrated male gender to be a risk factor for HDV (30, 40, 41). In our study, anti-HDV positivity was higher among female patients. The biological basis for gender differences in susceptibility to HDV infection remains unclear. This may be related to greater exposure to parenteral risk factors, such as blood transfusions or surgical procedures, as indicated by our regression analysis (42). Additionally, female patients have more access to health care facilities, leading to increased detection of prior HDV exposure (43). Given the small number of anti-HDV-positive cases, these results must be interpreted cautiously and require further investigation in larger population-based studies.
The results from laboratory investigations, including investigations of liver chemistry and HBV DNA levels, were similar between anti-HDV-positive and -negative patients. This was likely due to the absence of advanced liver fibrosis among anti-HDV-positive patients, as evaluated using Fibroscan. The liver elastography measurements showed that all the anti-HDV-positive patients had mild fibrosis (liver stiffness of < 7 kPa), whereas significant fibrosis was observed exclusively in anti-HDV-negative patients. These findings were likely due to low HDV replication, a shorter active infection duration before spontaneous clearance of HDV RNA, and infection with the less virulent HDV genotype 2, which predominates in the Middle East. In contrast, persistent HDV RNA, particularly associated with genotypes 1 and 5, which are the most common in Europe and Africa, respectively, has been consistently identified as a major risk factor for progression to advanced fibrosis and increased mortality (44-47). The low rate of detectable HDV RNA in our cohort further supports this observation.
This study has some limitations, including the cross-sectional design, which prevented assessment of causality or changes over time in HDV infection. The presence of only a single patient with detectable HDV RNA restricted the evaluation of viral replication, the genotypes, and the disease severity. Additionally, the low prevalence of HIV and HCV co-infections and limited exposure data may have caused us to underestimate the associations with high-risk factors. Finally, despite using sensitive assays, variability in HDV RNA detection could have led to underestimation of the active infections.
Our study has several important implications. Firstly, it provides the first contemporary, nationally representative estimate of HDV exposure among HBsAg-positive patients in Oman, complementing the results from an older study of high-risk patients. Secondly, the observed associations with a younger age, female gender, and a history of blood transfusion highlight possible future target groups for screening and follow-up. Thirdly, despite the overall low prevalence and mild disease burden observed, the potential for aggressive HDV-related liver disease remains, requiring routine anti-HDV testing, particularly before initiating HBV antiviral therapy or performing liver transplantation.
From a public health perspective, the 5.63% anti-HDV prevalence found in the current study supports the integration of HDV screening into national hepatitis B management strategies, as recommended by international associations such as the EASL and APASL, particularly given that HDV can be asymptomatic yet progress rapidly to cirrhosis or HCC (25, 26). The low rate of active HDV replication also provides an opportunity for targeted interventions before significant hepatic damage occurs, such as enrollment in surveillance programs or initiation of new HDV-specific therapies where indicated.
Finally, the discrepancy between our findings and the higher HDV prevalence reported in meta-analyses and neighboring countries underscores the need for standardized diagnostic methods, longitudinal follow-ups, and region-specific epidemiological studies (18). Differences in the assay sensitivity, population risk profiles, and historical transmission likely contributed to the observed variability. Future studies should focus on molecular characterization of HDV, assessment of viral replication, and the long-term outcomes in anti-HDV-positive patients to fully determine the clinical significance of HDV exposure in Oman.
In conclusion, despite the anti-HDV prevalence of 5.63% among HBsAg-positive patients in Oman, active infection is rare, and significant fibrosis is uncommon. Female gender and a history of blood transfusion are key predictors of anti-HDV positivity. These results emphasize the importance of routine HDV testing, risk stratification, and continued monitoring to prevent progression to advanced liver disease.
Author Contributions
All the authors participated in this research and contributed to the final version of the manuscript. K.M.A. and W.A.-T. participated in concept design and the writing of the manuscript and supervised the study. H.O. performed the statistical analysis and participated in the writing of the manuscript. M.E.-K., S.A., H.A., A.A. (Amal Anwar), A.A. (Abdullah AlKalbani), and B.R.K. participated in the writing, editing, and final revision of the manuscript. A.A. (Alya AlKalbani), M.A. (Malak AlSawafi), and M.A. (Munira AlShukaili) participated in patient recruitment and follow-up and data collection. All the authors have read and agreed on the submitted manuscript.
Funding
No funding was required for this research.
Informed Consent Statement
This study was approved by the Armed Forces Medical Services Research Ethics Committees (AFMS-MREC: 001/2024).
Conflicts of Interest
The authors declare no conflicts of interest related to this study and the preparation of this article.
References
- Mentha, N.; Clément, S.; Negro, F.; Alfaiate, D. A review on hepatitis D: From virology to new therapies. J. Adv. Res. 2019, 17, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Urban, S.; Neumann-Haefelin, C.; Lampertico, P. Hepatitis D virus in 2021: Virology, immunology and new treatment approaches for a difficult-to-treat disease. Gut 2021, 70, 1782–1794. [Google Scholar] [CrossRef] [PubMed]
- Negro, F.; Lok, A.S. Hepatitis D: A Review. JAMA 2023, 330, 2376–2387. [Google Scholar] [CrossRef]
- Scheller, L.; Hilgard, G.; Anastasiou, O.; Dittmer, U.; Kahraman, A.; Wedemeyer, H.; Deterding, K. Poor clinical and virological outcome of nucleos (t) ide analogue monotherapy in HBV/HDV co-infected patients. Medicine 2021, 100, e26571. [Google Scholar] [CrossRef]
- Stockdale, A.J.; Kreuels, B.; Henrion, M.Y.; Giorgi, E.; Kyomuhangi, I.; de Martel, C.; Hutin, Y.; Geretti, A.M. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J. Hepatol. 2020, 73, 523–532. [Google Scholar] [CrossRef]
- Pan, C.; Gish, R.; Jacobson, I.M.; Hu, K.-Q.; Wedemeyer, H.; Martin, P. Diagnosis and management of hepatitis delta virus infection. Dig. Dis. Sci. 2023, 68, 3237–3248. [Google Scholar] [CrossRef]
- Razavi-Shearer, D.; Child, H.; Razavi-Shearer, K.; Voeller, A.; Razavi, H.; Buti, M.; Tacke, F.; Terrault, N.; Zeuzem, S.; Abbas, Z. Adjusted estimate of the prevalence of hepatitis delta virus in 25 countries and territories. J. Hepatol. 2024, 80, 232–242. [Google Scholar] [CrossRef]
- Al-Naamani, K.; Al-Maqbali, A.; Al-Sinani, S. Characteristics of hepatitis B infection in a sample of Omani patients. Sultan Qaboos Univ. Med. J. 2013, 13, 380. [Google Scholar] [CrossRef] [PubMed]
- Al Awaidy, S.T.; Bawikar, S.P.; Al Busaidy, S.S.; Al Mahrouqi, S.; Al Baqlani, S.; Al Obaidani, I.; Alexander, J.; Patel, M.K. Progress toward elimination of hepatitis B virus transmission in Oman: Impact of hepatitis B vaccination. Am. J. Trop. Med. Hyg. 2013, 89, 811. [Google Scholar] [CrossRef]
- Al-Naamani, K.; Al-Harthi, R.; Al-Busafi, S.A.; Al Zuhaibi, H.; Al-Sinani, S.; Omer, H.; Rasool, W. Hepatitis B related liver cirrhosis in Oman. Oman Med. J. 2022, 37, e384. [Google Scholar] [CrossRef]
- Cornberg, M.; Sandmann, L.; Jaroszewicz, J.; Kennedy, P.; Lampertico, P.; Lemoine, M.; Lens, S.; Testoni, B.; Lai-Hung Wong, G.; Russo, F.P. EASL Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2025, 83, 502–583. [Google Scholar] [CrossRef]
- Aftab, M.; Amin, I.; Idrees, M.; Ali, A.; Rafique, S.; Naz, S. Molecular epidemiology of hepatitis delta and hepatitis B viruses circulating in two major provinces (East and North-West) of Pakistan. Infect. Genet. Evol. 2018, 64, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Safarpour, A.R.; Shahedi, A.; Fattahi, M.R.; Sadeghi, E.; Akbarzadeh, M.; Ahmadi, L.; Nikmanesh, N.; Fallahzadeh Abarghooee, E.; Shamsdin, S.A.; Akrami, H.; et al. Epidemiology of Hepatitis D Virus and Associated Factors in Patients Referred to Level Three Hepatitis Clinic, Fars Province, Southern Iran. Iran. J. Med. Sci. 2025, 50, 220–228. [Google Scholar]
- Al-Asmi, A.; Al-Jabri, F.S.; Al-Amrani, S.A.; Al Farsi, Y.; Al Sabahi, F.; Al-Futaisi, A.; Al-Adawi, S. Medical Tourism and Neurological Diseases: Omani Patients’ Experience Seeking Treatment Abroad. Oman Med. J. 2024, 39, e628. [Google Scholar] [CrossRef]
- Al-Dhahry, S.H.; Aghanashinikar, P.N.; Al-Marhuby, H.A.; Buhl, M.R.; Daar, A.S.; Al-Hasani, M.K. Hepatitis B, delta and human immunodeficiency virus infections among Omani patients with renal diseases: A seroprevalence study. Ann. Saudi Med. 1994, 14, 312–315. [Google Scholar] [CrossRef]
- Coller, K.E.; Butler, E.K.; Luk, K.-C.; Rodgers, M.A.; Cassidy, M.; Gersch, J.; McNamara, A.L.; Kuhns, M.C.; Dawson, G.J.; Kaptue, L. Development and performance of prototype serologic and molecular tests for hepatitis delta infection. Sci. Rep. 2018, 8, 2095. [Google Scholar] [CrossRef]
- Darbandi, A.; Mashati, P.; Yami, A.; Gharehbaghian, A.; Namini, M.T.; Gharehbaghian, A. Status of blood transfusion in World Health Organization-Eastern Mediterranean Region (WHO-EMR): Successes and challenges. Transfus. Apher. Sci. 2017, 56, 448–453. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Al-Rifai, A.; Sanai, F.M.; Alghamdi, A.S.; Sharara, A.I.; Saad, M.F.; van Selm, L.; Alqahtani, S.A. Hepatitis delta virus infection prevalence, diagnosis and treatment in the Middle East: A scoping review. Liver Int. 2023, 43, 116–123. [Google Scholar] [CrossRef]
- Miao, Z.; Zhang, S.; Ou, X.; Li, S.; Ma, Z.; Wang, W.; Peppelenbosch, M.P.; Liu, J.; Pan, Q. Estimating the global prevalence, disease progression, and clinical outcome of hepatitis delta virus infection. J. Infect. Dis. 2020, 221, 1677–1687. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Shen, D.-T.; Ji, D.-Z.; Han, P.-C.; Zhang, W.-M.; Ma, J.-F.; Chen, W.-S.; Goyal, H.; Pan, S.; Xu, H.-G. Prevalence and burden of hepatitis D virus infection in the global population: A systematic review and meta-analysis. Gut 2019, 68, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Salpini, R.; Piermatteo, L.; Caviglia, G.P.; Bertoli, A.; Brunetto, M.R.; Bruzzone, B.; Callegaro, A.; Caudai, C.; Cavallone, D.; Chessa, L.; et al. Comparison of diagnostic performances of HDV-RNA quantification assays used in clinical practice: Results from a national quality control multicenter study. J. Clin. Virol. 2025, 180, 105850. [Google Scholar] [CrossRef] [PubMed]
- Wranke, A.; Pinheiro Borzacov, L.M.; Parana, R.; Lobato, C.; Hamid, S.; Ceausu, E.; Dalekos, G.N.; Rizzetto, M.; Turcanu, A.; Niro, G.A. Clinical and virological heterogeneity of hepatitis delta in different regions world-wide: The Hepatitis Delta International Network (HDIN). Liver Int. 2018, 38, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Le Gal, F.; Brichler, S.; Drugan, T.; Alloui, C.; Roulot, D.; Pawlotsky, J.M.; Dény, P.; Gordien, E. Genetic diversity and worldwide distribution of the deltavirus genus: A study of 2152 clinical strains. Hepatology 2017, 66, 1826–1841. [Google Scholar] [CrossRef]
- Su, C.W.; Huang, Y.H.; Huo, T.I.; Shih, H.H.; Sheen, I.J.; Chen, S.W.; Lee, P.C.; Lee, S.D.; Wu, J.C. Genotypes and viremia of hepatitis B and D viruses are associated with outcomes of chronic hepatitis D patients. Gastroenterology 2006, 130, 1625–1635. [Google Scholar] [CrossRef]
- Liver, E.A.f.t.S.o.t. EASL Clinical Practice Guidelines on hepatitis delta virus. J. Hepatol. 2023, 79, 433–460. [Google Scholar] [CrossRef]
- Sarin, S.; Kumar, M.; Lau, G.; Abbas, Z.; Chan, H.; Chen, C.; Chen, D.; Chen, H.; Chen, P.; Chien, R. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Al-Riyami, A.Z.; Daar, S. Transfusion in Haemoglobinopathies: Review and recommendations for local blood banks and transfusion services in Oman. Sultan Qaboos Univ. Med. J. 2018, 18, e3. [Google Scholar] [CrossRef]
- Al-Busafi, S.A.; Al-Harthi, R.; Al-Naamani, K.; Al-Zuhaibi, H.; Priest, P. Risk factors for hepatitis B virus transmission in Oman. Oman Med. J. 2021, 36, e287. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, L.; Csiki, I.E.; Iacob, S.; Gheorghe, C.; Trifan, A.; Grigorescu, M.; Motoc, A.; Suceveanu, A.; Curescu, M.; Caruntu, F.; et al. Hepatitis Delta Virus Infection in Romania: Prevalence and Risk Factors. J. Gastrointestin. Liver. Dis. 2015, 24, 413–421. [Google Scholar] [CrossRef]
- Ordieres, C.; Navascués, C.A.; González-Diéguez, M.L.; Rodríguez, M.; Cadahía, V.; Varela, M.; Rodrigo, L.; Rodríguez, M. Prevalence and epidemiology of hepatitis D among patients with chronic hepatitis B virus infection: A report from Northern Spain. Eur. J. Gastroenterol. Hepatol. 2017, 29, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Béguelin, C.; Atkinson, A.; Boyd, A.; Falconer, K.; Kirkby, N.; Suter-Riniker, F.; Günthard, H.F.; Rockstroh, J.K.; Mocroft, A.; Rauch, A. Hepatitis delta infection among persons living with HIV in Europe. Liver Int. 2023, 43, 819–828. [Google Scholar] [CrossRef] [PubMed]
- Yen, D.W.; Soriano, V.; Barreiro, P.; Sherman, K.E. Triple Threat: HDV, HBV, HIV Coinfection. Clin. Liver Dis. 2023, 27, 955–972. [Google Scholar] [CrossRef]
- Palom, A.; Rando-Segura, A.; Vico, J.; Pacín, B.; Vargas, E.; Barreira-Díaz, A.; Rodríguez-Frías, F.; Riveiro-Barciela, M.; Esteban, R.; Buti, M. Implementation of anti-HDV reflex testing among HBsAg-positive individuals increases testing for hepatitis D. JHEP Rep. 2022, 4, 100547. [Google Scholar] [CrossRef] [PubMed]
- Elzouki, A.N.; Bashir, S.M.; Elahmer, O.; Elzouki, I.; Alkhattali, F. Prevalence and risk factors of hepatitis D virus infection in patients with chronic hepatitis B infection attending the three main tertiary hospitals in Libya. Arab. J. Gastroenterol. 2017, 18, 216–219. [Google Scholar] [CrossRef]
- Stelzl, E.; Ciesek, S.; Cornberg, M.; Maasoumy, B.; Heim, A.; Chudy, M.; Olivero, A.; Miklau, F.N.; Nickel, A.; Reinhardt, A. Reliable quantification of plasma HDV RNA is of paramount importance for treatment monitoring: A European multicenter study. J. Clin. Virol. 2021, 142, 104932. [Google Scholar] [CrossRef]
- Wranke, A.; Hardtke, S.; Heidrich, B.; Dalekos, G.; Yalçin, K.; Tabak, F.; Gürel, S.; Çakaloğlu, Y.; Akarca, U.S.; Lammert, F. Ten-year follow-up of a randomized controlled clinical trial in chronic hepatitis delta. J. Viral Hepat. 2020, 27, 1359–1368. [Google Scholar] [CrossRef]
- Stroffolini, T.; Morisco, F.; Ferrigno, L.; Pontillo, G.; Iantosca, G.; Cossiga, V.; Crateri, S.; Tosti, M.E.; SEIEVA collaborating group. Acute Delta Hepatitis in Italy spanning three decades (1991–2019): Evidence for the effectiveness of the hepatitis B vaccination campaign. J. Viral Hepat. 2022, 29, 78–86. [Google Scholar] [CrossRef]
- Lin, H.H.; Lee, S.S.J.; Yu, M.L.; Chang, T.T.; Su, C.W.; Hu, B.S.; Chen, Y.S.; Huang, C.K.; Lai, C.H.; Lin, J.N. Changing hepatitis D virus epidemiology in a hepatitis B virus endemic area with a national vaccination program. Hepatology 2015, 61, 1870–1879. [Google Scholar] [CrossRef]
- Adepoju, V.A.; Udah, D.C.; Adnani, Q.E.S. Prevalence, Risk Factors, and Clinical Profiles of Hepatitis D Virus in Nigeria: A Systematic Review, 2009–2024. Viruses 2024, 16, 1723. [Google Scholar] [CrossRef]
- Lee, W.-C.; Chen, T.-K.; Han, H.-F.; Lin, Y.-C.; Hwang, Y.-M.; Kao, J.-H.; Chen, P.-J.; Liu, C.-J. Investigating the prevalence and clinical effects of hepatitis delta viral infection in Taiwan. J. Microbiol. Immunol. Infect. 2021, 54, 901–908. [Google Scholar] [CrossRef]
- Gombotz, H.; Schreier, G.; Neubauer, S.; Kastner, P.; Hofmann, A. Gender disparities in red blood cell transfusion in elective surgery: A post hoc multicentre cohort study. BMJ Open 2016, 6, e012210. [Google Scholar] [CrossRef]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.J.; Robbins, J.A. Gender differences in the utilization of health care services. J. Fam. Pract. 2000, 49, 147–152. [Google Scholar] [PubMed]
- Roulot, D.; Brichler, S.; Layese, R.; BenAbdesselam, Z.; Zoulim, F.; Thibault, V.; Scholtes, C.; Roche, B.; Castelnau, C.; Poynard, T. Origin, HDV genotype and persistent viremia determine outcome and treatment response in patients with chronic hepatitis delta. J. Hepatol. 2020, 73, 1046–1062. [Google Scholar] [CrossRef]
- Palom, A.; Rodríguez-Tajes, S.; Navascués, C.A.; García-Samaniego, J.; Riveiro-Barciela, M.; Lens, S.; Rodríguez, M.; Esteban, R.; Buti, M. Long-term clinical outcomes in patients with chronic hepatitis delta: The role of persistent viraemia. Aliment. Pharmacol. Ther. 2020, 51, 158–166. [Google Scholar] [CrossRef]
- Kamal, H.; Westman, G.; Falconer, K.; Duberg, A.S.; Weiland, O.; Haverinen, S.; Wejstål, R.; Carlsson, T.; Kampmann, C.; Larsson, S.B. Long-term study of hepatitis delta virus infection at secondary care centers: The impact of viremia on liver-related outcomes. Hepatology 2020, 72, 1177–1190. [Google Scholar] [CrossRef] [PubMed]
- Bockmann, J.-H.; Grube, M.; Hamed, V.; von Felden, J.; Landahl, J.; Wehmeyer, M.; Giersch, K.; Hall, M.T.; Murray, J.M.; Dandri, M. High rates of cirrhosis and severe clinical events in patients with HBV/HDV co-infection: Longitudinal analysis of a German cohort. BMC Gastroenterol. 2020, 20, 24. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of HDV screening. Abbreviations: HBsAg, hepatitis B surface antigen; HBcAg, hepatitis B core antigen; anti-HDV, antibody to hepatitis D virus; HDV RNA, ribonucleic acid from hepatitis D virus.
Figure 1.
Flow diagram of HDV screening. Abbreviations: HBsAg, hepatitis B surface antigen; HBcAg, hepatitis B core antigen; anti-HDV, antibody to hepatitis D virus; HDV RNA, ribonucleic acid from hepatitis D virus.
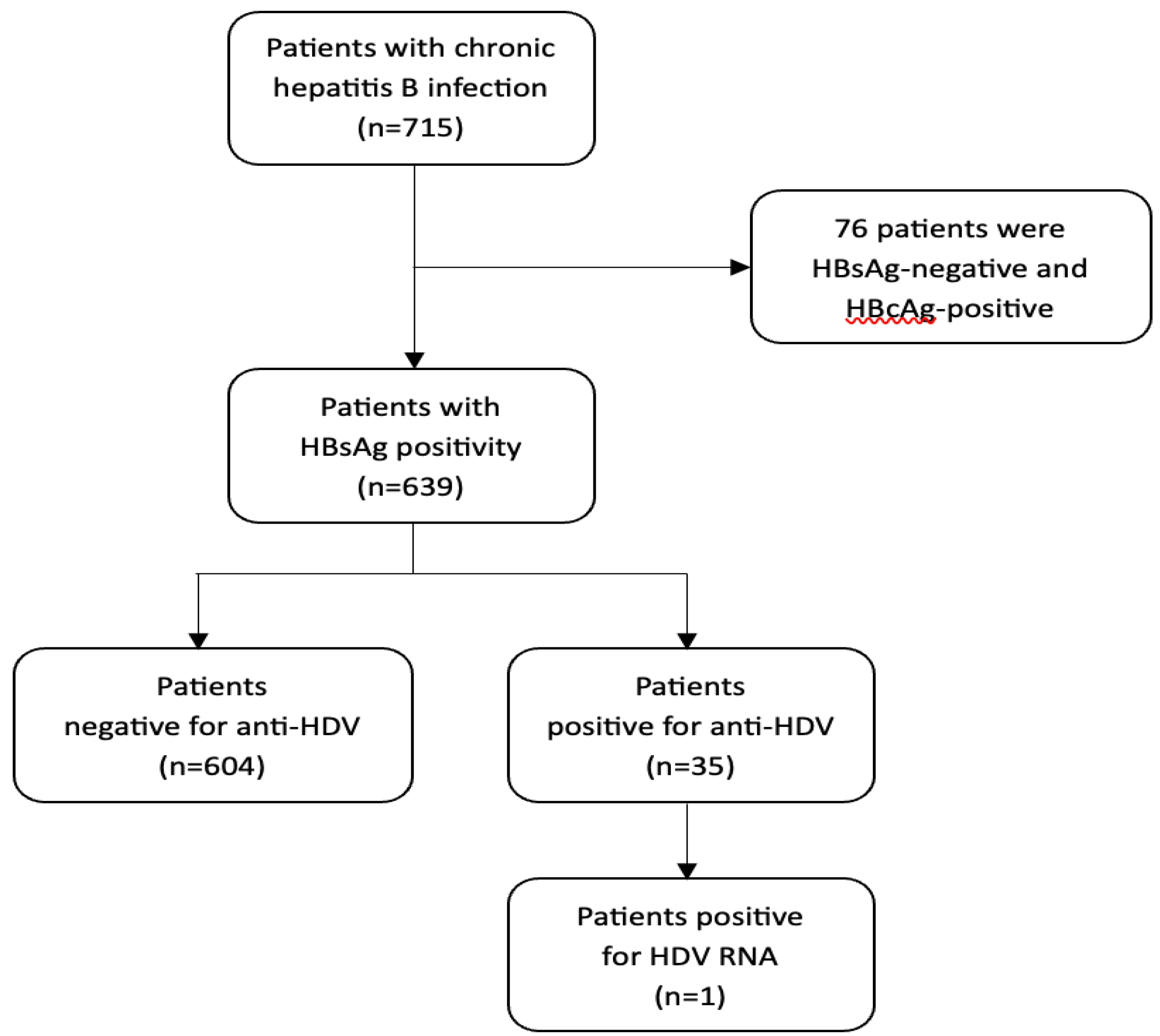
Figure 2.
Decline in the HDV RNA level in a single patient with detectable HDV RNA. The dashed line indicates the lower limit of detection (20 IU/mL = 1.3 Log10).
Figure 2.
Decline in the HDV RNA level in a single patient with detectable HDV RNA. The dashed line indicates the lower limit of detection (20 IU/mL = 1.3 Log10).
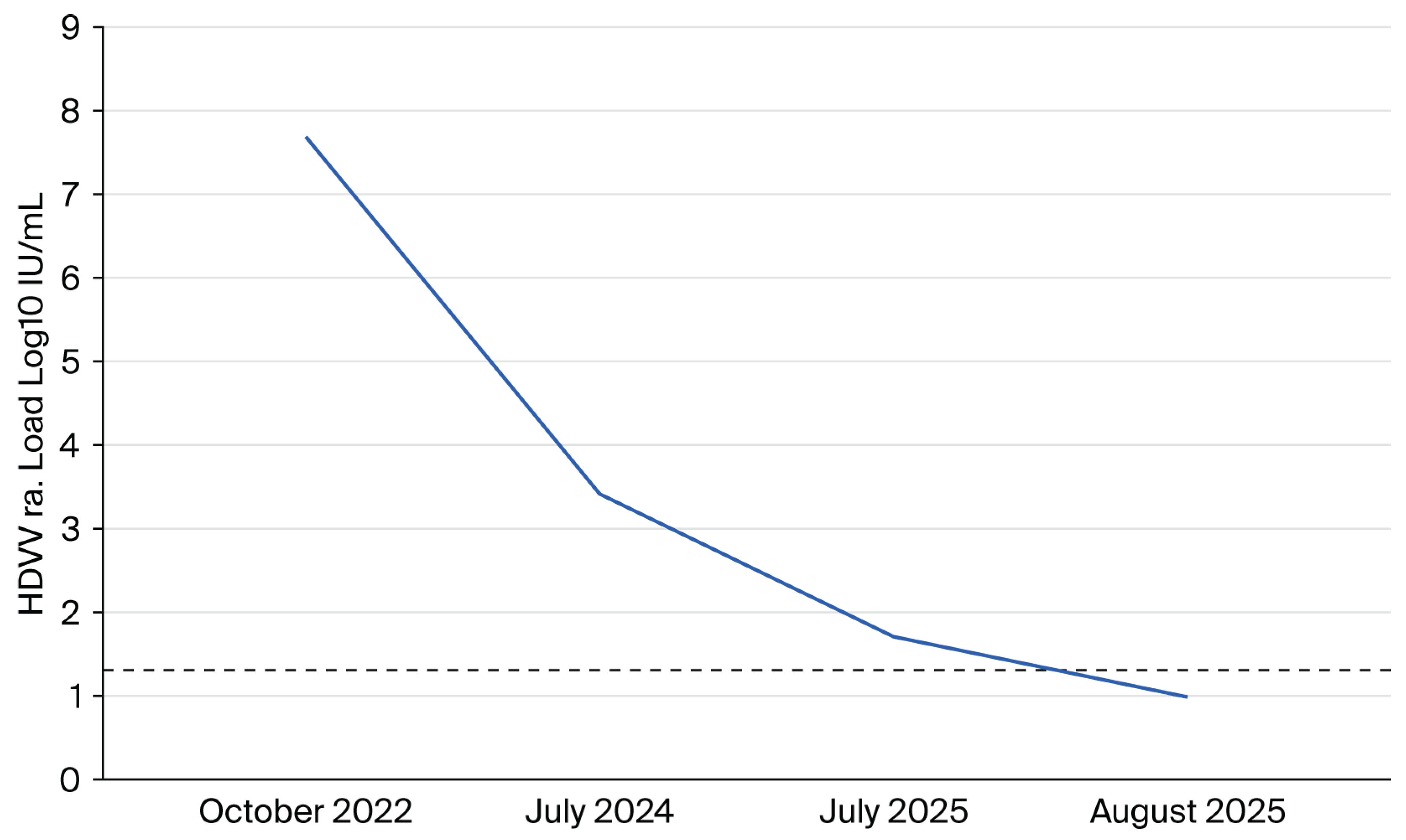

Table 1.
Comparison between subgroups of studied population according to their anti-HDV status.
| Variables | Total Cohort n = 639 (%) |
Negative for HDV n = 603 (%) |
Positive for HDV n = 36 (%) |
p-Value** | |
|---|---|---|---|---|---|
| Demographic | Age (mean ± SD) | 46.61 ± 8.76 Range of 28–85 |
46.77 ± 8.80 | 44.00 ± 7.73 | 0.07 |
| Male gender | 379 (59.31) | 372 (61.69) | 7(19.44) | <0.001 | |
| Married | 623 (97.50) | 587 (97.35) | 36 (100.00) | 0.32 | |
| Clinical | DM | 47 (7.36) | 45 (7.46) | 2 (5.56) | 0.67 |
| Hypertension | 35 (5.48) | 33 (5.47) | 2 (5.56) | 0.98 | |
| Dyslipidemia | 18 (2.82) | 18 (2.99) | 0 (0.00) | 0.29 | |
| CKD | 3 (0.47) | 3 (0.50) | 0 (0.00) | 0.67 | |
| Liver transplantation | 7 (1.10) | 6 (1.00) | 1 (2.78) | 0.32 | |
| MASLD | 266 (41.69) | 253 (41.96) | 13 (37.14) | 0.57 | |
| HCC | 3 (0.47) | 3 (0.50) | 0 (0.00) | 0.67 | |
| HBV treatment | 109 (17.06) | 106 (17.58) | 3 (8.33) | 0.15 | |
| Risk factors | Travel to endemic area | 373 (58.37) | 355 (58.87) | 18 (50.00) | 0.29 |
| Family history of HBV | 93 (14.55) | 86 (14.26) | 7 (19.44) | 0.39 | |
| Blood transfusion | 6 (0.94) | 3 (0.50) | 3 (8.33) | <0.001 | |
| History of surgery | 64 (10.02) | 57 (9.45) | 7 (19.44) | 0.05 | |
| Alcohol intake | 7 (1.10) | 7 (1.16) | 0 (0.00) | 0.52 | |
| Smoking | 4 (0.63) | 4 (0.66) | 0 (0.00) | 0.62 | |
| Co-infection | HCV | 5 (0.78) | 5 (0.83) | 0 (0.00) | 0.58 |
| HIV | 1 (0.16) | 1 (0.17) | 0 (0.00) | 0.81 | |
| Labs (mean ± SD) |
Total bilirubin | 9.12 ± 8.77 | 9.19 ± 8.93 | 7.91 ± 5.41 | 0.39 |
| Serum albumin | 43 ± 5 | 43 ± 5 | 42 ± 4 | 0.16 | |
| ALT | 30 ±28 | 30 ± 29 | 24 ± 16 | 0.15 | |
| AST | 26 ± 17 | 26 ± 17 | 24± 19 | 0.69 | |
| ALP | 73 ± 28 | 74 ± 28 | 68 ± 25 | 0.28 | |
| HBe Ag | 32 (5.01) | 31 (5.14) | 1 (2.78) | 0.53 | |
| HBVDNA (log) | 3.18 ± 1.42 | 3.19 ± 1.43 | 3.03 ± 1.42 | 0.55 | |
| Fibrosis * | F0–F1 | 596 (93.27) | 560 (92.87) | 36 (100) | 0.43 |
| F2 | 27 (4.23) | 27 (4.48) | 0 (0.00) | ||
| F3 | 3 (0.47) | 3 (0.50) | 0 (0.00) | ||
| F4 | 13 (2.03) | 13 (2.16) | 0 (0.00) | ||
Abbreviations: HDV, hepatitis D virus; DM, Diabetes Mellitus; CKD, Chronic Kidney Disease; MASLD, Metabolic Dysfunction-Associated Steatotic Liver Disease; HCC, hepatocellular carcinoma; HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, Human Immunodeficiency Virus; ALT, Alanine Aminotransferase; AST, Aspartate Aminotransferase; ALP, Alkaline Phosphatase; AFP, Alpha-Fetoprotein; HBeAg, HBV antigen; F0–F4, fibrosis stages. * Fibrosis stage is based on liver stiffness measurement (LSM) with FibroScan® device using vibration-controlled transient elastography (VCTE). ** p-value of differences between HDV-positive and -negative patients.
Table 2.
Logistic regression analysis of factors associated with anti-HDV positivity.
| Variables | Univariate Logistic Regression | Multivariate Logistic Regression | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age | 0.96 (0.92–1.00) | 0.07 | 0.94 (0.90–0.99) | 0.05 |
| Male gender | 0.15 (0.06–0.35) | <0.001 | 0.10 (0.04–0.28) | <0.001 |
| History of surgery | 2.31 (0.97–5.52) | 0.05 | 1.47 (0.53–4.08) | 0.46 |
| Blood transfusion | 18.18 (3.53–93.56) | <0.001 | 36.72 (4.03–334.24) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



