Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Invasive conjunctival squamous cell carcinoma (CSCC) is an aggressive, ocular surface malignancy. The mean annual age-standardised incidence rate of 0.45 cases per million per year is increasing with an average annual percent rise of 4.5% and occurs mainly in over 65-year-olds in temperate climates but in a younger demographic in the tropics. Invasive CSCC can lead to vision loss either from the destructive effects of the tumour or side effects of therapy, facial disfigurement from radical surgery, and death from metastases. There is no standardised treatment and not all cases are referred to a specialist ocular oncology centre. Recent progress in cancer immunology and genetics has revolutionised the treatment of cutaneous and head and neck SCCs, which share some similarities to invasive CSCC. A better understanding of invasive CSCC and its preinvasive intraepithelial lesions is required to lead to the development of novel targeted and immunotherapies both for local tumour control, globe sparing alternatives and to prevent disseminated disease. This review aims to provide a comprehensive clinical overview of the current knowledge regarding CSSC, its epidemiology, pathogenesis, presentation, diagnosis, management, recent advances in targeted and immunotherapies for personalised treatment of this disease, and early diagnosis strategies to improve patient outcomes.
Keywords:
conjunctival squamous cell carcinoma
; conjunctival squamous cell carcinoma in situ
; conjunctival squamous intraepithelial neoplasia
; ocular surface squamous neoplasia
; ocular oncology
; targeted therapy
; immunotherapy
1. Introduction
Invasive conjunctival squamous cell carcinoma (CSCC) has a worldwide incidence rate of 0.02 to 3.5 per 100,000 and showing increasing incidences in the last decades [1,2,3,4,5]. It typically presents at 60-70 years of age occurring more commonly in fair-skinned males, of increasing age, and following significant sunlight exposure; but presents at 30-40 year-old females in the tropics [2,4,5,6,7]. It has a high recurrence rate and local spread is common. Distant metastasis occur less commonly [8]. Invasive CSSC usually develops from conjunctival squamous intraepithelial neoplasia (CSIN) and in-situ squamous carcinoma. CSIN (also clinically known as ocular surface squamous neoplasia [OSSN]) is a preinvasive lesion and encompasses a spectrum of intraepithelial squamous dysplasia, from mild to severe dysplasia, and can progress to in-situ squamous carcinoma [8,9].
Invasive CSCC usually involves the interpalpebral conjunctiva and limbus (especially the nasal limbus) and can extend onto the cornea. It can also less frequently occur in the caruncle, tarsal, or forniceal conjunctiva. Invasive CSCC presents as a well-demarcated pinkish-grey nodule with keratinisation or ulceration [10]. In the African and Asian population, it often presents with brown surface pigmentation and feeder vessels [11]. It originates from conjunctival epithelium, shows squamous differentiation, and breaches the basement membrane to invade the underlying substantia propria/stroma [6,12,13].
Ultraviolet (UV) radiation, impaired immune surveillance, and immunosuppression (e.g. post-transplant or HIV infection) are well known risk factors. Opportunistic oncogenic viruses such as human immunodeficiency virus, human papilloma virus and Epstein Barr Virus, are linked with immunosuppression [2,4,13,14,15,16,17]. Mutations in TP53, TERT, EGFR, titin, HER2 and DNA repair genes and overexpression of matrix metalloproteinases have been identified in invasive CSCC [13,18,19,20,21,22,23,24,25,26,27,28,29].
The treatment for invasive CSCC varies between considerably between centres but mainly includes surgical excision and/or adjuvant cryotherapy, topical chemotherapy, brachytherapy, proton beam radiotherapy or photon external beam radiation and, in advanced cases with orbital invasion, orbital exenteration [1,6,30,31,32]. Invasive CSCC has a high rate of local recurrence (approx. 10–40%); incidence of up to 24% in regional lymph node metastases and distant metastases of ~6-18% [8,33,34,35,36].
Despite recent successes with targeted and immunotherapies in SCCs elsewhere, data on invasive CSCC treated with similar therapies (EGFR inhibitors, anti-VEGF, anti-PDL1) are promising but limited, often stemming from a single patient or small case series with inoperable or advanced disease prior to surgery [37,38,39,40,41,42,43,44,45,46,47]
This review aims to provide a comprehensive clinical overview of the current understanding of CSCC, its epidemiology, pathogenesis, clinical presentation, diagnosis, treatments, and explore the recent advances in novel biological therapies and future management.
2. Epidemiology
In-situ conjunctival squamous carcinoma is the most common preinvasive ocular surface malignancy and if untreated can progress to invasive CSCC. Its incidence varies geographically: in the UK, it is estimated at 0.4 cases/million/year, whereas both Australia and North America show incidences of 19-35 cases/million/year [48,49]. The mean age-standardised incidence rate worldwide is 0.18 and 0.08 cases/year/100 000 among males and females, respectively. However, the highest age-standardised incidence rate reported from Zimbabwe is 3.4 and 3.0 cases/year/100 000 population for males and females, respectively [2].
Invasive CSCC, although rare compared to SCCs of other sites, is a common ocular surface malignancy. It is the most prevalent ocular surface carcinoma representing approximately 4% to 29% of tumours found in the ocular region [50] [51]. There has been a disconcerting increase in incidence in the last decades with markedly advanced cases presenting following the COVID pandemic. Worldwide the incidence is 2–35 per million [1,2,3,4] occurring more commonly in fair-skinned males (with a ratio of 1.83:1 compared with females), of increasing age, and following significant sunlight exposure [4,5,7] ]. Ultraviolet (UV) radiation is the strongest environmental etiological factor with incidence rate decreasing by 49% per each ten degrees increase in latitude [3].
In the African continent, the disease mainly affects women, at a younger age, and is strongly associated with human immunodeficiency virus (HIV) infection and variably with human papilloma virus (HPV) infection [2,17,52]. The combination of low latitude and high prevalence of HIV and HPV-infections most likely explains the higher incidence of invasive CSCC observed in Africa. A higher prevalence of CSCC is also seen in patients with impaired immune surveillance, certain autoimmune conditions (atopy, ocular cicatricial pemphigoid and xeroderma pigmentosum) and/or immunosuppression with susceptibility to oncogenic viruses HPV and Epstein Barr Virus (EBV) [2,13,14,15,16]. Iatrogenic immunosuppression is also a risk factor.
3. Aetiology and Pathogenesis
The aetiology of SCC is classically understood to be triggered by UV radiation exposure and immunosuppression (due to HIV-infection or post organ transplantation) [4]. Mutations in TP53, TERT, EGFR, titin, and DNA repair genes and overexpression of matrix metalloproteinases, Human Epidermal growth factor Receptor 2 (HER2) and programmed death ligand1 (PD-L1) have been identified in invasive CSCC [18,19,20,21,22,23,24,25,26,27,28,29]. However, none of these are pathognomonic, and have been reported in other conjunctival epithelial neoplasms e.g., pterygia and pingueculae. One study revealed similar UV-mediated driver mutations in both preinvasive and invasive cutaneous SCC and CSCC. TP53 mutations were the most frequent, followed by CDKN2A and PIK3CA [28].
The vulnerability of limbal stem cells to the oncogenic effects of UV radiation and certain viruses is postulated to give rise to most invasive CSCC [13]. UVB exposure may induce preinvasive disease by increase in pyrimidine dimers which damage DNA and disrupt its repair pathways. Proliferation of unrepaired DNA by continued excess UVB exposure or immunosuppression, can manifest CSIN/in-situ carcinoma (preinvasive disease) of the conjunctiva [21,53]. UV exposure also activates c-Jun N-terminal kinase 1 (JNK1), which plays a role in tumour development through phosphorylation and oncogenic signal transduction pathways [54].
UVB radiation has also been implicated in upregulated expression of matrix metalloproteinases (MMPs), particularly MMP-9 and -11) and tissue inhibitors of metalloproteinases (TIMPs) such as TIMP-2 and -3, which promote the tumourigensis via antiapoptotic, proliferative, invasive and metastatic properties [21].
UV-mediated driver mutations in telomerase reverse transcriptase (TERT) promoter and TP53 have been reported in up to 48% of in-situ and invasive CSCC cases. An overexpression of telomerase in the conjunctival epithelium affects telomere length with proliferative and anti-apoptotic functions [20,55]. TP53 mutations disrupt pyrimidine dimer repair pathways [53]. Furthermore, the role of stratifin acting as a p53 mediated inhibitor is also implicated in UV induced p53 pathogenesis [56].
Titin and EGFR mutations have also been reported in both in situ and invasive CSCC. Structural disturbances in nuclear proteins and EGFR translocation from the membrane into the cytoplasm, respectively, are thought to facilitate oncogenic activity [18]. The cytoplasmic staining of EGFR compared with membranous staining has been shown to be an inverse prognostic marker with increased number of orbital exenteration cases [19].
Overexpression of HER2 has been reported in higher grades of CSIN and invasive CSCC suggesting its main role in tumour progression rather than early oncogenic initiation. Anti-HER2 therapy may therefore be a considered in for select patients with advanced disease when conventional topical or surgical treatments are contraindicated [24]. However, there are no clinical trials investigating the role of anti-HER2 treatment on invasive CSCC.
Increased vascular endothelial growth factor (VEGF) and alpha-B crystallin protein expression has also been shown in invasive CSCC. VEGF is an established potent angiogenic factor and alpha-B crystallin is known to promote angiogenesis as a molecular chaperone of VEGF. Furthermore, treatment of invasive CSCC with topical mitomycin C reduced the expression of both [57].
PD-L1 is expressed in around 47% of CSSC, with higher expression levels correlating with invasive and advanced stage (≥T3) tumours and with increased densities of tumour-infiltrating lymphocytes [58,59].
These results are encouraging and may potentially mirror some success in a subset of invasive CSCC as established targeted therapies and PDL-1 targeted treatment blockades used in head and neck and cutaneous SCC.
Since the 1990s, increased incidence rate of invasive CSCC in Africa has been strongly associated with the high prevalence of HIV primarily as well as EBV and HPV (particularly HPV-16 & -18 subtypes, and less commonly HPV-5 & -8) in HIV-infected patients. HIV has an immunosuppressive effect on the limbal stem cells making them vulnerable to oncogenic viruses leading to aggressive invasive CSCC at a younger age with worse prognosis [60]. HPV driven invasive CSCC in immunocompetent patients has been controversial but a recent meta-analysis concluded an eight-fold increase in development of CSIN or invasive CSCC in HPV-infected patients in comparison to healthy control subjects [61]. HPV-16 with early gene expression (active HPV mRNA transcripts confirmed via RNAscope) was shown to cause in-situ carcinoma in a subset of patients who had atopy [62].Another study demonstrated that patients with HPV-positive tumours were significantly younger and had a higher recurrence rate compared to patients with HPV-negative tumours. The HPV-positive tumours also showed a non-keratinising morphology [63].
Other risk factors include: cigarette smoking, chronic inflammation and vitamin A-deficiency. Also there is an increased risk of CSIN/invasive CSCC with autoimmune ocular surface disorders such as ocular cicatricial pemphigoid/mucous membrane pemphigoid, and genetic conditions including and xeroderma pigmentosum [2,14,15].
4. Clinical Presentation and Assessment
CSIN and invasive CSCC most commonly occur in the interpalpebral conjunctiva and limbus (usually nasal limbus). Invasive CSCC frequently invades into the cornea. The caruncle, tarsal, or forniceal conjunctiva are less frequently involved. Advanced or recurrent invasive CSCC may extend to the tarsal and forniceal conjunctiva. The latter locations are also seen in immunosuppressed/immunocompromised patients and in those with atopy associated squamous carcinoma [62].
Most CSIN lesions appear as unilateral, gelatinous and minimally elevated but can also be papilliform or a leukoplakic plaque (due to keratinisation). However, intraepithelial lesions can be clinically indistinguishable from the invasive disease and hence histopathological diagnosis remains the ‘gold’ standard. Invasive CSCC usually presents as a unilateral, elevated, immobile, well-demarcated pearly pink-to-grey nodule, which can be ulcerated, leukoplakic, gelatinous, or papilliform. They often have feeder blood vessels and intrinsic vasculature (Figure 1). Pigmentation is variable, depending on the Fitzpatrick skin type. Patients may present on noticing a mass with/without pigmentation on their eye but can also have significant visual morbidities, such as irritation/burning with redness and reflex tearing, dry eye, pain, vision disturbance, double vision or even vision loss [35,36,64,65,66,67].
Differential diagnoses of invasive CSCC, include: sebaceous cell carcinoma, naevus, melanoma, lymphoma, or eyelid basal cell or squamous cell carcinoma invading the conjunctiva. CSIN can develop in pinguecula, pterygium, viral squamous papillomas and other inflammatory conjunctival conditions. Diagnosis is confirmed on histopathological assessment. Histological assessment in a specialist centre regularly reporting ophthalmic specimens is recommended for accurate diagnosis and grading. [8,50,68]
Clinical examination involves slit lamp biomicroscopy and regular colour photograph-documentation of the anterior segment (including with eversion of eyelids). Toluidine blue (0.05%) vital stain has been shown to be a good screening tool for OSSN/CSIN and can assist in identifying the tumour borders, but is not in widespread use due to high false positive rates [69]. Anterior segment optical coherence tomography (AS-OCT) has been used to distinguish OSSN from other conjunctival lesions. In OSSN/CSIN, the AS-OCT features are those of a hyperreflective lesion that has thickened epithelium, and an abrupt transition between normal and abnormal tissue [70]. However, squamous metaplasia is indistinguishable from OSSN on AS-OCT, highlighting the need for biopsy and histopathological analysis of lesions especially where there is overlap [71]. Other modalities such as ultrasound biomicroscopy and confocal microscopy can be helpful in clinical assessment and to look for intraocular invasion. Magnetic resonance imaging is required to assess orbital invasion. Diffusion and perfusion-weighted MR imaging can help in differentiating invasive CSCC from other eyelid masses [70,72,73,74].
5. Histomorphological Features
Macroscopically CSIN lesions look as flat, cream/white epithelial thickenings/plaques. They may also be mildly raised and papillomatous. Invasive CSCC are usually gelatinous grey/white nodular or papilliform masses without/with surface keratinisation, respectively, or ulcerated/erythematous elevated lesions. Lesions in the tropics can show pigmentation and a lot more surface keratinisation [11,35,36]. Depending on the specimen type, invasion of the cornea and other ocular structures and/or orbital soft tissue can be seen on macroscopic examination.
Microscopically CSIN lesions show a range of epithelial dysplasia (cytological atypia, architectural atypia and lack of maturation), which is graded mild (confined to lower third of epithelium), moderate (involves up to middle third), and severe (extends to upper third but surface differentiation preserved). In-situ squamous carcinoma shows full-thickness epithelial dysplasia. CSIN, including in-situ carcinoma, do not breach the epithelial basement membrane (Figure 2). At low magnification, an abrupt demarcation with the background normal conjunctival epithelium, and with goblet cell loss can be appreciated. At higher magnification, cytological atypia comprises nuclear enlargement and pleomorphism with increased nuclear-to-cytoplasmic ratio, hyperchromatic chromatin and prominent nucleoli. Abnormal mitotic figures are seen at varying levels of the epithelium. Dyskeratosis and apoptotic cells may also be present. Architecturally, the epithelium shows abnormal stratification with loss of normal polarity, and surface keratosis or parakeratosis. The underlying substantia propria/stroma often shows elastotic degeneration from chronic sun exposure. UV-associated cases can resemble skin actinic keratoses [35,36,75,76,77,78,79,80,81,82,83]. High-risk HPV-associated cases usually lack surface keratinisation or parakeratosis, show full thickness epithelial dysplasia and have a basaloid appearance [62,63].
Invasive CSCC usually arises from conjunctival in-situ squamous carcinoma but breaches the basement membrane invading the underlying stroma (Figure 2). The invasive carcinoma can be infiltrative or exhibit pushing borders and show stromal desmoplasia. Perineural and lymphovascular invasion may be present. Histological classification of invasive CSCC includes: conventional (showing various degrees of keratinisation); basaloid (poorly differentiated with pleomorphic cells with scant basophilic cytoplasm); spindle cell (poorly differentiated with pleomorphic spindled cells); pigmented (CSCC with melanosis and melanophages); acantholytic (acantholytic and dyskeratotic cells with apoptotic debris); and with mucinous differentiation (intracytoplasmic and extracellular mucin but no true gland formation, overlying in situ component with mucinous differentiation). Immunohistochemistry is usually only required for diagnosis in poorly differentiated tumours. For intraepithelial lesions, p53 is expressed in the dysplastic cells. In poorly differentiated invasive carcinomas, CSCC is positive for broad-spectrum/pan and high molecular weight cytokeratins. Diffuse nuclear and cytoplasmic ‘block-like’ p16 positivity can be predictive of high-risk HPV infection but requires molecular techniques to confirm HPV DNA or RNA presence [35,36,62,63,65,69,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91].
In-situ conjunctival squamous carcinoma and invasive CSSC are staged by the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC) T (tumour size), N (nodal spread), and M (metastasis) eighth edition classification system, which has been validated for the risk of tumour recurrence, development of metastasis and survival [92,93].
6. Treatment and Prognosis
There is no standard of care treatment and little trial evidence for the therapies in use for in-situ conjunctival squamous carcinoma or invasive CSCC; consequently, management varies considerably between ophthalmic and specialised ocular oncology centres. For localized, solitary tumours, this includes: surgical excision (wide local) +/− amniotic membrane allograft and +/− adjuvant cryotherapy, topical chemotherapy (mitomycin C, 5-fluorouracil or interferon alpha-2b), radiotherapy (brachytherapy, proton beam or photon external beam), enucleation, or radical orbital exenteration for advanced cases with local tissue invasion [6,12,30,31,32,94].
Surgical excision with a ‘no touch’ technique and wide margins of smaller localised tumours (<5 mm) is the most frequent approach. Alcohol application allows resection of the corneal component by corneal epitheliectomy. Adjunct cryotherapy usually applied in double- or triple- freeze-thaw cycles to the margins and base of the tumour after resection, limits spread. In diffuse recurrences, for example of the tarsal conjunctiva, cryotherapy spray can be applied to limit regrowth. Eyes with intraocular invasion may be salvaged with localized radiotherapy with proton beam radiotherapy or plaque brachytherapy but if tumour control cannot be achieved, enucleation may become necessary. For advanced cases of invasive CSCC with periocular and orbital invasion, radical orbital exenteration is performed, which leads to considerable facial disfigurement.[95,96,97]
Topical chemotherapy agents, such as interferon alpha 2b (IFNa-2b), 5-fluorouracil (5-FU), or mitomycin C (MMC), can be used as adjuncts to surgery or even as monotherapies in certain cases. IFNa-2b has immunomodulatory mechanisms and inhibits cell proliferation and can be administered as single subconjunctival injection or a regime of topical eye drops. MMC utilises its DNA alkylating properties to inhibit RNA synthesis and tumour growth. Antimetabolite 5-FU blocks DNA synthesis by inhibiting thymidylate sulphate [96,97,98,99,100]. In a multicentre, randomised, placebo-controlled trial, Gichuhi et al. showed that a surgical ‘no touch’ technique together with 5-FU drops four times a day for 4 weeks reduced recurrence at 1 year from 36% to 11% [101].
HPV vaccine has been used in conjunctival in-situ squamous carcinoma to treat in a recalcitrant lesion [102]. In this case, 4 intramuscular doses of 9-valent HPV vaccine resulted in a dramatic reduction in the size of the tumour, though not full resolution. This approach has also been used in conjunctival papillomas [103,104].
Visudyne photodynamic therapy has also been tried in conjunctival in-situ squamous carcinoma, though with higher rates of recurrence than excision. Its use is limited to cases that cannot have surgical excision for relatively localised disease [105]. Recently, a laser activated anticancer virus-drug particle conjugate has been developed for small uveal melanomas (belzupacap sarotalocan or AU-011; Aura Biosciences, Boston, USA). Such an approach for localised treatment of CSIN/in-situ and invasive CSSC is an attractive option.
Radiotherapy options include: brachytherapy (beta radiation using strontium-90, iodine-125, ruthenium-106) directly on the tumour or surgical bed post excision; proton bean radiotherapy (tantalum markers and high precision delivery using Bragg peak, 48-60Gy); gamma knife stereotactic radiosurgery; or external beam radiation. These have been used to preserve the eye, periocular tissues and ocular function; as primary treatment for unresectable invasive CSCC, patients not suitable for surgery, or post-surgery for positive/narrow margins or recurrent disease [106,107,108,109].
Postoperative complications include scarring, limbal stem cell failure, ulceration/non-healing defects, glaucoma, cataract and vision loss. Complication rates and risk of recurrence are high (5-56%; most within first year but even after 5years), especially in large tumours and cases with positive surgical margins, warranting close long-term follow up. Lymph node metastases occur in ~2-24% and usually involve preauricular, parotid, submandibular and/or cervical nodes, depending on invasive CSCC location. Distant metastasis may also involve the lungs, bone and spleen and brain (~6.2-18%). Risk factors for metastasis include tumour thickness, histological poor differentiation and spindle cell carcinoma subtype, and orbital invasion/high tumour staging. Poor prognostic indicators include high-staged tumours (T3/T4), positive surgical margins and nodal metastases. Overall 5-year survival in localised invasive CSCC reported to be as high as 95% but 70% in advanced cases. The overall risk of tumour-related death ranges from 2-5% [8,32,33,34,35,36,110,111,112,113].
The use of genetics for prognostication in invasive CSCC is currently limited. However, advances in characterising invasive CSCC molecular drivers are offering insight into potential targeted therapies already in use of other cancer types. Targeted and immunotherapies have recently become promising options for advanced CSCC as an alternative to orbital exenteration although data are limited, with only those from small case series or single case studies in patients with inoperable disease or as first-line therapy prior surgery in advanced cases [37,38,39,40,41,42,43,44]. A summary of immune checkpoint inhibitors (ICI), namely PDL-1, is presented in Table 1.
Given the overexpression of EGFR, its role in prognosis, and the success of EGFR inhibitors in treating head and neck SCC, El-Sawy et al reported significant tumour shrinkage in 2 patients treated with EGFR inhibitors for advanced orbital SCC who had refused orbital exenteration [19,45]. Small clinical studies have investigated the use of anti-VEGF agents, such as bevacizumab and ranibizumab, given VEGF established role in angiogenesis and tumourigenesis [47,114,115]. Clinical studies on targeted therapies in CSCC patients are summarised in Table 2.
6. Future Direction and Conclusion
CSCC is an invasive ocular surface cancer with increasing global incidence. Given its rarity in comparison to other SCCs, international multicentre collaboration is pivotal to obtain sufficient numbers in order to progress translational research and enlist patients into clinical trials. The recent developments in cancer genetics and immunology present exciting new frontiers for better understanding CSCC pathogenesis for earlier diagnosis and provide new targets for therapy in order to achieve better patient outcomes. Insight into the molecular drivers of development and its integration with clinical and histomorphological evaluation will allow earlier diagnosis, improve risk stratification and prognostication, and identify patients for specific therapies (i.e., ‘personalised/precision medicine’). This will further enable the development of clear management guidelines and enrolment into targeted therapies earlier than current practice, facilitating improved outcomes and reduce risk of metastatic disease. Other novel methods through biotechnology and bioengineering offer exciting developments in non-invasive methods of earlier diagnosis of preinvasive disease and prognostic prediction through to targeted therapies and drug delivery methods with sustained, localised release to minimise complication rates, improve patient compliance and treatment outcomes.
Author Contributions
Conceptualization, Y.K.; writing—original draft preparation, M.M. and Y.K.; writing—review and editing, M.M., Y.K., H.S.M., M.S.S. and S.G; supervision, Y.K., H.S.M., M.S.S. and S.G. All authors have read and agreed to the published version of the manuscript.
Funding
The research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Acknowledgments
The authors would like to thank the clinical imaging team in St Paul’s Eye Unit, Liverpool for providing the colour anterior segment photographs.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Yang, J; Foster, CS. Squamous Cell Carcinoma of the Conjunctiva. International Ophthalmology Clinics 1997, 37(4), 73–85. [Google Scholar] [CrossRef] [PubMed]
- Gichuhi, S; Sagoo, MS; Weiss, HA; Burton, MJ. Epidemiology of ocular surface squamous neoplasia in Africa. Trop Med Int Health 2013, 18(12), 1424–43. [Google Scholar] [CrossRef]
- Newton, R; Ferlay, J; Reeves, G; Beral, V; Parkin, DM. Effect of ambient solar ultraviolet radiation on incidence of squamous-cell carcinoma of the eye. Lancet 1996, 347(9013), 1450–1. [Google Scholar] [CrossRef] [PubMed]
- Sun, EC; Fears, TR; Goedert, JJ. Epidemiology of squamous cell conjunctival cancer. Cancer Epidemiology, Biomarkers & Prevention 1997, 6(2), 73–7. [Google Scholar]
- Darwich, R; Ghazawi, FM; Le, M; Rahme, E; Alghazawi, N; Zubarev, A; et al. Epidemiology of invasive ocular surface squamous neoplasia in Canada during 1992-2010. Br J Ophthalmol. 2020, 104(10), 1368–72. [Google Scholar] [CrossRef]
- Yin, VT; Merritt, HA; Sniegowski, M; Esmaeli, B. Eyelid and ocular surface carcinoma: diagnosis and management. Clin Dermatol 2015, 33(2), 159–69. [Google Scholar] [CrossRef]
- Emmanuel, B; Ruder, E; Lin, SW; Abnet, C; Hollenbeck, A; Mbulaiteye, S. Incidence of squamous-cell carcinoma of the conjunctiva and other eye cancers in the NIH-AARP Diet and Health Study. Ecancermedicalscience 2012, 6, 254. [Google Scholar]
- McKelvie, PA; Daniell, M; McNab, A; Loughnan, M; Santamaria, JD. Squamous cell carcinoma of the conjunctiva: a series of 26 cases. Br J Ophthalmol. 2002, 86(2), 168–73. [Google Scholar] [CrossRef]
- Margo, CE; White, AA. Ocular surface squamous neoplasia: terminology that is conceptually friendly but clinically perilous. Eye (Lond) 2014, 28(5), 507–9. [Google Scholar] [CrossRef]
- Donaldson, MJ; Sullivan, TJ; Whitehead, KJ; Williamson, RM. Squamous cell carcinoma of the eyelids. Br J Ophthalmol. 2002, 86(10), 1161–5. [Google Scholar] [CrossRef]
- Gichuhi, S; Macharia, E; Kabiru, J; Zindamoyen, AM; Rono, H; Ollando, E; et al. Clinical Presentation of Ocular Surface Squamous Neoplasia in Kenya. JAMA Ophthalmol. 2015, 133(11), 1305–13. [Google Scholar] [CrossRef] [PubMed]
- Gichuhi, S; Sagoo, MS. Squamous cell carcinoma of the conjunctiva. Community Eye Health 2016, 29(95), 52–3. [Google Scholar]
- Gichuhi, S; Ohnuma, S; Sagoo, MS; Burton, MJ. Pathophysiology of ocular surface squamous neoplasia. Exp Eye Res. 2014, 129, 172–82. [Google Scholar] [CrossRef] [PubMed]
- Kaliki, S; Vempuluru, VS; Ghose, N; Gunda, S; Vithalani, NM; Sultana, S; et al. Ocular surface squamous neoplasia in India: a study of 438 patients. Int Ophthalmol. 2022, 42(6), 1915–26. [Google Scholar] [CrossRef] [PubMed]
- Choi, CJ; Jakobiec, FA; Zakka, FR; Foster, CS; Chodosh, J; Freitag, SK. Conjunctival Squamous Cell Neoplasia Associated With Ocular Cicatricial Pemphigoid. Ophthalmic Plast Reconstr Surg 2017, 33(6), e157–e60. [Google Scholar] [CrossRef]
- Galati, L; Combes, JD; Gupta, P; Sen, R; Robitaille, A; Brancaccio, RN; et al. Detection of a large spectrum of viral infections in conjunctival premalignant and malignant lesions. Int J Cancer 2020, 147(10), 2862–70. [Google Scholar] [CrossRef]
- Hämmerl, L; Ferlay, J; Borok, M; Carrilho, C; Parkin, DM. The burden of squamous cell carcinoma of the conjunctiva in Africa. Cancer Epidemiol. 2019, 61, 150–3. [Google Scholar] [CrossRef]
- Djulbegovic, MB; Uversky, VN; Karp, CL; Harbour, JW. Functional impact of titin (TTN) mutations in ocular surface squamous neoplasia. Int J Biol Macromol. 2022, 195, 93–101. [Google Scholar] [CrossRef]
- Sakai, A; Tagami, M; Kakehashi, A; Katsuyama-Yoshikawa, A; Misawa, N; Wanibuchi, H; et al. Expression, intracellular localization, and mutation of EGFR in conjunctival squamous cell carcinoma and the association with prognosis and treatment. PLoS One 2020, 15(8), e0238120. [Google Scholar] [CrossRef]
- Scholz, SL; Thomasen, H; Reis, H; Möller, I; Darawsha, R; Müller, B; et al. Frequent TERT Promoter Mutations in Ocular Surface Squamous Neoplasia. Invest Ophthalmol Vis Sci. 2015, 56(10), 5854–61. [Google Scholar] [CrossRef]
- Ng, J; Coroneo, MT; Wakefield, D; Di Girolamo, N. Ultraviolet Radiation and the Role of Matrix Metalloproteinases in the Pathogenesis of Ocular Surface Squamous Neoplasia. Investigative Ophthalmology & Visual Science 2008, 49(12), 5295–306. [Google Scholar] [CrossRef]
- Ateenyi-Agaba, C; Dai, M; Le Calvez, F; Katongole-Mbidde, E; Smet, A; Tommasino, M; et al. TP53 mutations in squamous-cell carcinomas of the conjunctiva: evidence for UV-induced mutagenesis. Mutagenesis 2004, 19(5), 399–401. [Google Scholar] [CrossRef]
- Mahale, A; Alkatan, H; Alwadani, S; Othman, M; Suarez, MJ; Price, A; et al. Altered gene expression in conjunctival squamous cell carcinoma. Modern Pathology 2016, 29(5), 452–60. [Google Scholar] [CrossRef]
- Paulina García de Alba Graue EE, Pablo Zoroquiain, Ana Beatriz, Toledo Dias, Miguel Burnier. HER2 as a possible therapeutic target in squamous cell carcinoma of the conjunctiva. Annals of Eye Science 2018, 3. [CrossRef]
- Asnaghi, L; Alkatan, H; Mahale, A; Othman, M; Alwadani, S; Al-Hussain, H; et al. Identification of multiple DNA copy number alterations including frequent 8p11.22 amplification in conjunctival squamous cell carcinoma. Invest Ophthalmol Vis Sci. 2014, 55(12), 8604–13. [Google Scholar] [CrossRef]
- Starita, N; Buonaguro, L; Buonaguro, FM; Tornesello, ML. Telomerase promoter mutations in human immunodeficiency virus-related conjunctiva neoplasia. J Transl Med. 2018, 16(1), 77. [Google Scholar] [CrossRef]
- Lin, SY; Liao, SL; Hong, JB; Chu, CY; Sheen, YS; Jhuang, JY; et al. TERT promoter mutations in periocular carcinomas: implications of ultraviolet light in pathogenesis. Br J Ophthalmol. 2016, 100(2), 274–7. [Google Scholar] [CrossRef]
- Lazo de la Vega, L; Bick, N; Hu, K; Rahrig, SE; Silva, CD; Matayoshi, S; et al. Invasive squamous cell carcinomas and precursor lesions on UV-exposed epithelia demonstrate concordant genomic complexity in driver genes. Mod Pathol. 2020, 33(11), 2280–94. [Google Scholar] [CrossRef]
- Di Girolamo, N; Atik, A; McCluskey, PJ; Wakefield, D. Matrix metalloproteinases and their inhibitors in squamous cell carcinoma of the conjunctiva. Ocul Surf. 2013, 11(3), 193–205. [Google Scholar] [CrossRef]
- Kenawy, N; Garrick, A; Heimann, H; Coupland, SE; Damato, BE. Conjunctival squamous cell neoplasia: the Liverpool Ocular Oncology Centre experience. Graefes Arch Clin Exp Ophthalmol. 2015, 253(1), 143–50. [Google Scholar] [CrossRef]
- Yousef, YA; Finger, PT. Squamous carcinoma and dysplasia of the conjunctiva and cornea: an analysis of 101 cases. Ophthalmology 2012, 119(2), 233–40. [Google Scholar] [CrossRef]
- Miller, CV; Wolf, A; Klingenstein, A; Decker, C; Garip, A; Kampik, A; et al. Clinical outcome of advanced squamous cell carcinoma of the conjunctiva. Eye (Lond) 2014, 28(8), 962–7. [Google Scholar] [CrossRef]
- Faustina, M; Diba, R; Ahmadi, MA; Esmaeli, B. Patterns of regional and distant metastasis in patients with eyelid and periocular squamous cell carcinoma. Ophthalmology 2004, 111(10), 1930–2. [Google Scholar] [CrossRef]
- Chauhan, S; Sen, S; Sharma, A; Tandon, R; Kashyap, S; Pushker, N; et al. American Joint Committee on Cancer Staging and clinicopathological high-risk predictors of ocular surface squamous neoplasia: a study from a tertiary eye center in India. Arch Pathol Lab Med. 2014, 138(11), 1488–94. [Google Scholar] [CrossRef]
- Yamamoto H, Mudhar HS, Cherepanoff S, Eberhart CG, Heindl LM, Ferreira T. Conjunctival squamous cell carcinoma. In: Board WCoTE, editor. WHO Classification of Tumours: Eye and Orbit Tumours. WHO Classification of Tumours series. 13. 5 ed. Lyon, France: International Agency for Research on Cancer; 2025.
- Heegaard S, Alkatan H, Eberhart CG, M. HL. Conjunctival squamous intraepithelial neoplasia. In: Board WCoTE, editor. WHO Classification of Tumours: Eye and Orbit Tumours. WHO Classification of Tumours series. 13. 5 ed. Lyon, France: International Agency for Research on Cancer; 2025.
- Demirci, H; Elner, VM; Demirci, FY; Robinson, DR; Chinnaiyan, A; Schlachter, D; et al. Immunotherapy for Conjunctival Squamous Cell Carcinoma with Orbital Extension. Ophthalmology 2021, 128(5), 801–4. [Google Scholar] [CrossRef]
- Demirci, H; Vo, JN; Wu, YM; Elner, V; Chinnaiyan, AM; Robinson, D; et al. Next-Generation Sequencing-Based Molecular Profiling of Conjunctival Squamous Cell Carcinoma and Its Potential Application for Therapy. Ophthalmol Sci. 2025, 5(5), 100801. [Google Scholar] [CrossRef]
- Kanda, M; Jayawickrema, N; Davagnanam, I; Samia-Aly, E; Gupta, T; Daniel, C. Cemiplimab in advanced periocular conjunctival and cutaneous squamous cell carcinoma: a United Kingdom case series. Orbit 2025, 1–11. [Google Scholar] [CrossRef]
- Esmaeli, B; Fan, J; Goldberg, H; Lu, T; Gross, ND; Akhave, N; et al. Immune checkpoint inhibitors with or without chemotherapy for orbital, conjunctival, and ocular adnexal squamous cell carcinoma. Canadian Journal of Ophthalmology 2025, 60(1), e38–e51. [Google Scholar] [CrossRef]
- Azad, AD; Zhang, JJ; Emerick, KS; Shalhout, SZ; Kaufman, HL; Miller, DM; et al. Immunotherapy for Advanced Conjunctival Squamous Cell Carcinoma: Treatment Failures. Ophthalmic Plast Reconstr Surg. 2025, 41(6), 646–50. [Google Scholar] [CrossRef]
- Ceylanoglu, KS; Eisenberg, A; Worden, FP; Elner, VM; Demirci, H. Use of Cemiplimab, an Immune Checkpoint Inhibitor for Conjunctival Intraepithelial Neoplasia. Cornea 2024, 43(4), 528–30. [Google Scholar] [CrossRef]
- Steren, B; Burtness, B; Bhatia, A; Demirci, H; Shinder, R; Yoo, D; et al. Cemiplimab for Orbital Squamous Cell Carcinoma in 11 Cases. Ophthalmic Plastic & Reconstructive Surgery 2022, 38(5), 496–502. [Google Scholar] [CrossRef]
- Hoffmann, M; Schardt, J; Ionescu, C; Wolf-Schnurrbusch, UE; Wagner, F; Dettmer, MS; et al. Long lasting response to anti-PD-1 therapy of recurrent conjunctival squamous cell carcinoma-A case report and systematic review of the literature. Current Problems in Cancer: Case Reports 2021, 4, 100088. [Google Scholar] [CrossRef]
- El-Sawy, T; Sabichi, AL; Myers, JN; Kies, MS; William, WN; Glisson, BS; et al. Epidermal Growth Factor Receptor Inhibitors for Treatment of Orbital Squamous Cell Carcinoma. Archives of Ophthalmology 2012, 130(12), 1608–11. [Google Scholar] [CrossRef]
- Youn, GM; Case, AG; Jarin, T; Li, B; Swarup, A; Naranjo, A; et al. The Use of Panitumumab-IRDye800CW in a Novel Murine Model for Conjunctival Squamous Cell Carcinoma. Translational Vision Science & Technology 2022, 11(7), 23. [Google Scholar]
- Finger, PT; Chin, KJ. Refractory Squamous Cell Carcinoma of the Conjunctiva Treated With Subconjunctival Ranibizumab (Lucentis): A Two-Year Study. Ophthalmic Plastic & Reconstructive Surgery 2012, 28(2), 85–9. [Google Scholar]
- Pe'er, J. Ocular surface squamous neoplasia. Ophthalmol Clin North Am. 2005, 18(1), 1–13, vii. [Google Scholar] [CrossRef]
- Turner, HC; Budak, MT; Akinci, MA; Wolosin, JM. Comparative analysis of human conjunctival and corneal epithelial gene expression with oligonucleotide microarrays. Invest Ophthalmol Vis Sci. 2007, 48(5), 2050–61. [Google Scholar] [CrossRef]
- Mehta, M; Fay, A. Squamous cell carcinoma of the eyelid and conjunctiva. Int Ophthalmol Clin. 2009, 49(1), 111–21. [Google Scholar] [CrossRef]
- Shields, CL; Demirci, H; Karatza, E; Shields, JA. Clinical survey of 1643 melanocytic and nonmelanocytic conjunctival tumors. Ophthalmology 2004, 111(9), 1747–54. [Google Scholar] [CrossRef]
- Ateenyi-Agaba, C. Conjunctival squamous-cell carcinoma associated with HIV infection in Kampala, Uganda. Lancet 1995, 345(8951), 695–6. [Google Scholar] [CrossRef]
- Daya-Grosjean, L; Dumaz, N; Sarasin, A. The specificity of p53 mutation spectra in sunlight induced human cancers. J Photochem Photobiol B 1995, 28(2), 115–24. [Google Scholar] [CrossRef]
- Dérijard, B; Hibi, M; Wu, IH; Barrett, T; Su, B; Deng, T; et al. JNK1: a protein kinase stimulated by UV light and Ha-Ras that binds and phosphorylates the c-Jun activation domain. Cell. 1994, 76(6), 1025–37. [Google Scholar] [CrossRef]
- Blackburn, EH. Telomeres and telomerase: their mechanisms of action and the effects of altering their functions. FEBS Lett. 2005, 579(4), 859–62. [Google Scholar] [CrossRef]
- Chauhan, S; Sen, S; Chauhan, SS; Pushker, N; Tandon, R; Kashyap, S; et al. Stratifin in ocular surface squamous neoplasia and its association with p53. Acta Ophthalmol. 2021, 99(8), e1483–e91. [Google Scholar] [CrossRef]
- Dong, Z; Kase, S; Ando, R; Fukuhara, J; Kinoshita, S; Dong, Y; et al. Expression of αB-crystallin and vascular endothelial growth factor in conjunctival squamous cell carcinoma. Anticancer Res. 2013, 33(9), 3745–51. [Google Scholar]
- Nagarajan, P; El-Hadad, C; Gruschkus, SK; Ning, J; Hudgens, CW; Sagiv, O; et al. PD-L1/PD1 Expression, Composition of Tumor-Associated Immune Infiltrate, and HPV Status in Conjunctival Squamous Cell Carcinoma. Invest Ophthalmol Vis Sci. 2019, 60(6), 2388–98. [Google Scholar] [CrossRef]
- Slater, NA; Googe, PB. PD-L1 expression in cutaneous squamous cell carcinoma correlates with risk of metastasis. J Cutan Pathol. 2016, 43(8), 663–70. [Google Scholar] [CrossRef]
- Muchengeti, M; Bohlius, J; Dhokotera, TG. Conjunctival cancer in people living with HIV. Curr Opin Infect Dis. 2021, 34(1), 1–7. [Google Scholar] [CrossRef]
- Ramberg, I; Møller-Hansen, M; Toft, PB; Funding, M; Heegaard, S. Human papillomavirus infection plays a role in conjunctival squamous cell carcinoma: a systematic review and meta-analysis of observational studies. Acta Ophthalmologica 2021, 99(5), 478–88. [Google Scholar] [CrossRef]
- Griffin, H; Mudhar, HS; Rundle, P; Shiraz, A; Mahmood, R; Egawa, N; et al. Human papillomavirus type 16 causes a defined subset of conjunctival in situ squamous cell carcinomas. Mod Pathol. 2020, 33(1), 74–90. [Google Scholar] [CrossRef]
- Ramberg, I; Toft, PB; Georgsen, JB; Siersma, VD; Funding, M; Jensen, DH; et al. Conjunctival intraepithelial neoplasia and carcinoma: distinct clinical and histological features in relation to human papilloma virus status. Br J Ophthalmol. 2021, 105(6), 878–83. [Google Scholar] [CrossRef]
- Cervantes, G; Rodríguez, AA, Jr.; Leal, AG. Squamous cell carcinoma of the conjunctiva: clinicopathological features in 287 cases. Can J Ophthalmol. 2002, 37(1), 14-9; discussion 9-20. [Google Scholar] [CrossRef]
- Krachmer, JH; Mannis, MJ; Holland, EJ. Cornea: Fundamentals, Diagnosis, and Management. American Orthoptic Journal. 2011, 61, 147. [Google Scholar]
- Nelson, KD; McSoley, JJ. Clinical findings and management of conjunctival intraepithelial neoplasia. Optometry 2011, 82(1), 15–21. [Google Scholar] [CrossRef]
- Shields, CL; Shields, JA. Tumors of the conjunctiva and cornea. Surv Ophthalmol. 2004, 49(1), 3–24. [Google Scholar] [CrossRef]
- KWITKO, ML; BONIUK, M; ZIMMERMAN, LE. Eyelid Tumors With Reference to Lesions Confused With Squamous Cell Carcinoma: I. Incidence and Errors in Diagnosis. Archives of Ophthalmology 1963, 69(6), 693–7. [Google Scholar] [CrossRef]
- Gichuhi, S; Macharia, E; Kabiru, J; Zindamoyen, AMb; Rono, H; Ollando, E; et al. Toluidine blue 0.05% vital staining for the diagnosis of ocular surface squamous neoplasia in Kenya. JAMA ophthalmology 2015, 133(11), 1314–21. [Google Scholar] [CrossRef]
- Thomas, BJ; Galor, A; Nanji, AA; El Sayyad, F; Wang, J; Dubovy, SR; et al. Ultra high-resolution anterior segment optical coherence tomography in the diagnosis and management of ocular surface squamous neoplasia. The ocular surface 2014, 12(1), 46–58. [Google Scholar] [CrossRef]
- Stevens, SM; Reyes-Capo, DP; Patel, U; Choudhary, A; Khzam, RA; Tang, V; et al. Clinical and Optical Coherence Tomography Comparison Between Ocular Surface Squamous Neoplasia and Squamous Metaplasia. Cornea 2023, 42(4), 429–34. [Google Scholar] [CrossRef]
- Xu, Y; Zhou, Z; Wang, M; Liu, F; Qu, H; Hong, J. The clinical value of in vivo confocal microscopy for diagnosis of ocular surface squamous neoplasia. Eye 2012, 26(6), 781–7. [Google Scholar] [CrossRef]
- Liu, Z; Karp, CL; Galor, A; Al Bayyat, GJ; Jiang, H; Wang, J. Role of optical coherence tomography angiography in the characterization of vascular network patterns of ocular surface squamous neoplasia. Ocul Surf. 2020, 18(4), 926–35. [Google Scholar] [CrossRef]
- Karp, CL; Mercado, C; Venkateswaran, N; Ruggeri, M; Galor, A; Garcia, A; et al. Use of High-Resolution Optical Coherence Tomography in the Surgical Management of Ocular Surface Squamous Neoplasia: A Pilot Study. Am J Ophthalmol. 2019, 206, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Jaworski, A; Wolffsohn, JS; Napper, GA. Detection, aetiology and management of conjunctival intraepithelial neoplasia. Ophthalmic Physiol Opt. 2000, 20(5), 371–80. [Google Scholar] [CrossRef] [PubMed]
- Lee, GA; Hirst, LW. Ocular surface squamous neoplasia. Surv Ophthalmol. 1995, 39(6), 429–50. [Google Scholar] [CrossRef] [PubMed]
- Erie, JC; Campbell, RJ; Liesegang, TJ. Conjunctival and corneal intraepithelial and invasive neoplasia. Ophthalmology 1986, 93(2), 176–83. [Google Scholar] [CrossRef]
- Grossniklaus, HE; Green, WR; Luckenbach, M; Chan, CC. Conjunctival lesions in adults. A clinical and histopathologic review. Cornea 1987, 6(2), 78–116. [Google Scholar] [CrossRef]
- Mauriello, JA, Jr.; Napolitano, J; McLean, I. Actinic keratosis and dysplasia of the conjunctiva: a clinicopathological study of 45 cases. Can J Ophthalmol. 1995, 30(6), 312–6. [Google Scholar]
- Kao, AA; Galor, A; Karp, CL; Abdelaziz, A; Feuer, WJ; Dubovy, SR. Clinicopathologic correlation of ocular surface squamous neoplasms at Bascom Palmer Eye Institute: 2001 to 2010. Ophthalmology 2012, 119(9), 1773–6. [Google Scholar] [CrossRef]
- Reese, A; Margo, CE. Conjunctival squamous intraepithelial neoplasia and its differential diagnosis. J Clin Pathol. 2022, 75(5), 354–8. [Google Scholar] [CrossRef]
- Mishra, DK; Taneja, S; Singh, V; Veena, U; Kaliki, S. Histopathological spectrum of ocular surface squamous neoplasia: A retrospective study of 776 lesions. Indian J Pathol Microbiol. 2022, 65(1), 3–7. [Google Scholar] [CrossRef]
- Hamam, R; Bhat, P; Foster, CS. Conjunctival/corneal intraepithelial neoplasia. Int Ophthalmol Clin. 2009, 49(1), 63–70. [Google Scholar] [CrossRef]
- Pizzarello, LD JF. Bowen's disease of the conjunctiva: a misnomer Ocular and adnexal tumors 1978, 553–71.
- Iliff, WJ; Marback, R; Green, WR. Invasive Squamous Cell Carcinoma of the Conjunctiva. Archives of Ophthalmology 1975, 93(2), 119–22. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z; Li, B; Shi, J; Xu, X; Li, L; Gao, F. Intraocular Extension of Conjunctival Squamous Cell Carcinoma. Ophthalmologica 2007, 221(3), 200–3. [Google Scholar] [CrossRef] [PubMed]
- Cottel, WI. Perineural invasion by squamous-cell carcinoma. J Dermatol Surg Oncol. 1982, 8(7), 589–600. [Google Scholar] [CrossRef]
- Albert, DM; Jakobiec, FA. Principles and practice of ophthalmology; Saunders, 2000. [Google Scholar]
- Vempuluru, VS; Kapoor, AG; Kaliki, S; Jajapuram, SD; Mohamed, A; Mishra, DK. Comparative evaluation of clinical characteristics of biopsy-proven conjunctival intraepithelial neoplasia and invasive squamous cell carcinoma using image processing software programs. International Ophthalmology 2021, 41(4), 1301–7. [Google Scholar] [CrossRef] [PubMed]
- Nanji, AA; Mercado, C; Galor, A; Dubovy, S; Karp, CL. Updates in Ocular Surface Tumor Diagnostics. Int Ophthalmol Clin. 2017, 57(3), 47–62. [Google Scholar] [CrossRef]
- Mittal, R; Rath, S; Vemuganti, GK. Ocular surface squamous neoplasia - Review of etio-pathogenesis and an update on clinico-pathological diagnosis. Saudi J Ophthalmol. 2013, 27(3), 177–86. [Google Scholar] [CrossRef]
- Singh, S; Mohamed, A; Kaliki, S. Ocular surface squamous neoplasia: analysis based on the 8th American Joint Committee on Cancer classification. International Ophthalmology 2019, 39(6), 1283–91. [Google Scholar] [CrossRef]
- Brierley, JD; Gospodarowicz, M; Wittekind, C. TNM Classification of Malignant Tumours, 8 ed.; Wiley-Blackwell: Oxford, UK, 2017. [Google Scholar]
- Adler, E; Turner, JR; Stone, DU. Ocular surface squamous neoplasia: a survey of changes in the standard of care from 2003 to 2012. Cornea 2013, 32(12), 1558–61. [Google Scholar] [CrossRef]
- Shields, JA; Shields, CL; De Potter, P. Surgical management of conjunctival tumors. The 1994 Lynn B. McMahan Lecture. Arch Ophthalmol. 1997, 115(6), 808–15. [Google Scholar] [CrossRef]
- Al Bayyat, G; Arreaza-Kaufman, D; Venkateswaran, N; Galor, A; Karp, CL. Update on pharmacotherapy for ocular surface squamous neoplasia. Eye and Vision. 2019, 6(1), 24. [Google Scholar] [CrossRef]
- Ali, MJ; Pujari, A; Dave, TV; Kaliki, S; Naik, MN. Clinicopathological profile of orbital exenteration: 14 years of experience from a tertiary eye care center in South India. International Ophthalmology 2016, 36(2), 253–8. [Google Scholar] [CrossRef]
- Karp, CL; Galor, A; Chhabra, S; Barnes, SD; Alfonso, EC. Subconjunctival/perilesional recombinant interferon α2b for ocular surface squamous neoplasia: a 10-year review. Ophthalmology 2010, 117(12), 2241–6. [Google Scholar] [CrossRef]
- Nanji, AA; Moon, CS; Galor, A; Sein, J; Oellers, P; Karp, CL. Surgical versus medical treatment of ocular surface squamous neoplasia: a comparison of recurrences and complications. Ophthalmology 2014, 121(5), 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Joag, MG; Sise, A; Murillo, JC; Sayed-Ahmed, IO; Wong, JR; Mercado, C; et al. Topical 5-Fluorouracil 1% as Primary Treatment for Ocular Surface Squamous Neoplasia. Ophthalmology 2016, 123(7), 1442–8. [Google Scholar] [CrossRef]
- Gichuhi, S; Macharia, E; Kabiru, J; Zindamoyen, AM; Rono, H; Ollando, E; et al. Topical fluorouracil after surgery for ocular surface squamous neoplasia in Kenya: a randomised, double-blind, placebo-controlled trial. Lancet Glob Health 2016, 4(6), e378-85. [Google Scholar] [CrossRef] [PubMed]
- Zein, M; De Arrigunaga, S; Amer, MM; Galor, A; Nichols, AJ; Ioannides, T; et al. Therapeutic Response to Treatment of a Papillomatous Ocular Surface Squamous Neoplasia With Intramuscular Human Papillomavirus Vaccine. Cornea 2024, 43(8), 1049–52. [Google Scholar] [CrossRef] [PubMed]
- Sripawadkul, W; AlBayyat, G; Galor, A; Wylegala, A; Nichols, AJ; Ioannides, T; et al. Resolution of a Presumed Conjunctival Papilloma After Therapeutic Treatment With the Human Papillomavirus Vaccine. JAMA Ophthalmol. 2022, 140(4), 434–5. [Google Scholar] [CrossRef]
- Seth, I; Roberts, P; Cadieux, D. Gardasil-9 Vaccine as a Possible Treatment Option for Human Papillomavirus Conjunctival Papilloma. Ophthalmology 2023, 130(5), 532. [Google Scholar] [CrossRef]
- Cekiç, O; Bardak, Y; Kapucuoğlu, N. Photodynamic therapy for conjunctival ocular surface squamous neoplasia. J Ocul Pharmacol Ther. 2011, 27(2), 205–7. [Google Scholar] [CrossRef]
- Arepalli, S; Kaliki, S; Shields, CL; Emrich, J; Komarnicky, L; Shields, JA. Plaque Radiotherapy in the Management of Scleral-Invasive Conjunctival Squamous Cell Carcinoma: An Analysis of 15 Eyes. JAMA Ophthalmology 2014, 132(6), 691–6. [Google Scholar] [CrossRef]
- Panda, BB; Dasmajumdar, SK; Sadangi, D; Tripathy, SR. Radiation therapy in conjunctival squamous cell carcinoma. BMJ Case Rep. 2023, 16(7). [Google Scholar] [CrossRef] [PubMed]
- Zheng, T; Wang, D; Miao, Y; Dong, M; Liu, Q; Zhang, Q; et al. Clinical efficacy and safety of proton radiotherapy for ocular conjunctival malignancies: a systematic review and meta-analysis. Front Public Health 2025, 13, 1486988. [Google Scholar] [CrossRef] [PubMed]
- Graue, GF; Tena, LB; Finger, PT. Electron beam radiation for conjunctival squamous carcinoma. Ophthalmic Plast Reconstr Surg. 2011, 27(4), 277–81. [Google Scholar] [CrossRef]
- Abt, NB; Zhao, J; Huang, Y; Eghrari, AO. Prognostic factors and survival for malignant conjunctival melanoma and squamous cell carcinoma over four decades. Am J Otolaryngol. 2019, 40(4), 577–82. [Google Scholar] [CrossRef]
- Vempuluru, VS; Indusekhar, H; Mohamed, A; Kaliki, S. Metastatic conjunctival squamous cell carcinoma: a study of 5 patients. Int Ophthalmol. 2022, 42(10), 3097–108. [Google Scholar] [CrossRef] [PubMed]
- Bellerive, C; Berry, JL; Polski, A; Singh, AD. Conjunctival Squamous Neoplasia: Staging and Initial Treatment. Cornea 2018, 37(10), 1287–91. [Google Scholar] [CrossRef]
- Alkatan, HM; Al-Motlak, MA; Al-Shedoukhy, AA. Metastatic Squamous Spindle Cell Carcinoma of the conjunctiva. Saudi J Ophthalmol. 2010, 24(4), 155–8. [Google Scholar] [CrossRef]
- Asena, L; Dursun Altınörs, D. Topical Bevacizumab for the Treatment of Ocular Surface Squamous Neoplasia. Journal of Ocular Pharmacology and Therapeutics 2015, 31(8), 487–90. [Google Scholar] [CrossRef]
- Faramarzi, A; Feizi, S. Subconjunctival bevacizumab injection for ocular surface squamous neoplasia. Cornea 2013, 32(7), 998–1001. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Anterior segment photographs of invasive CSCC with presence of feeder vessels. Middle top row and bottom row images shows corneal invasion. Brown surface pigmentation is seen in patients from the tropics (image bottom right). Image on right (top and bottom) shows surface keratinisation.
Figure 1.
Anterior segment photographs of invasive CSCC with presence of feeder vessels. Middle top row and bottom row images shows corneal invasion. Brown surface pigmentation is seen in patients from the tropics (image bottom right). Image on right (top and bottom) shows surface keratinisation.
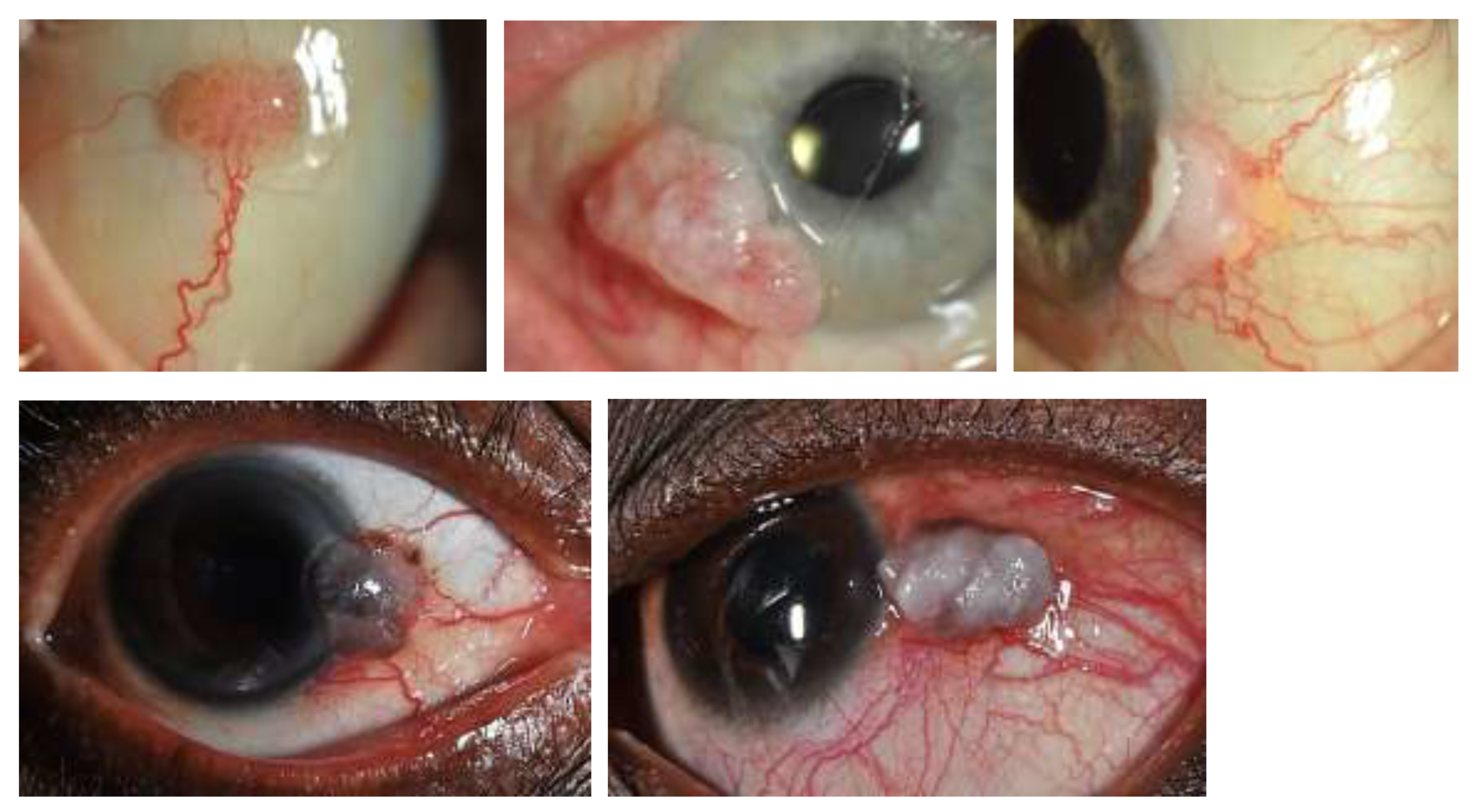
Figure 2.
Haematoxylin and eosin staining photomicrographs showing in-situ conjunctival squamous carcinoma (image on the left) and invasive CSCC (image on the right).
Figure 2.
Haematoxylin and eosin staining photomicrographs showing in-situ conjunctival squamous carcinoma (image on the left) and invasive CSCC (image on the right).
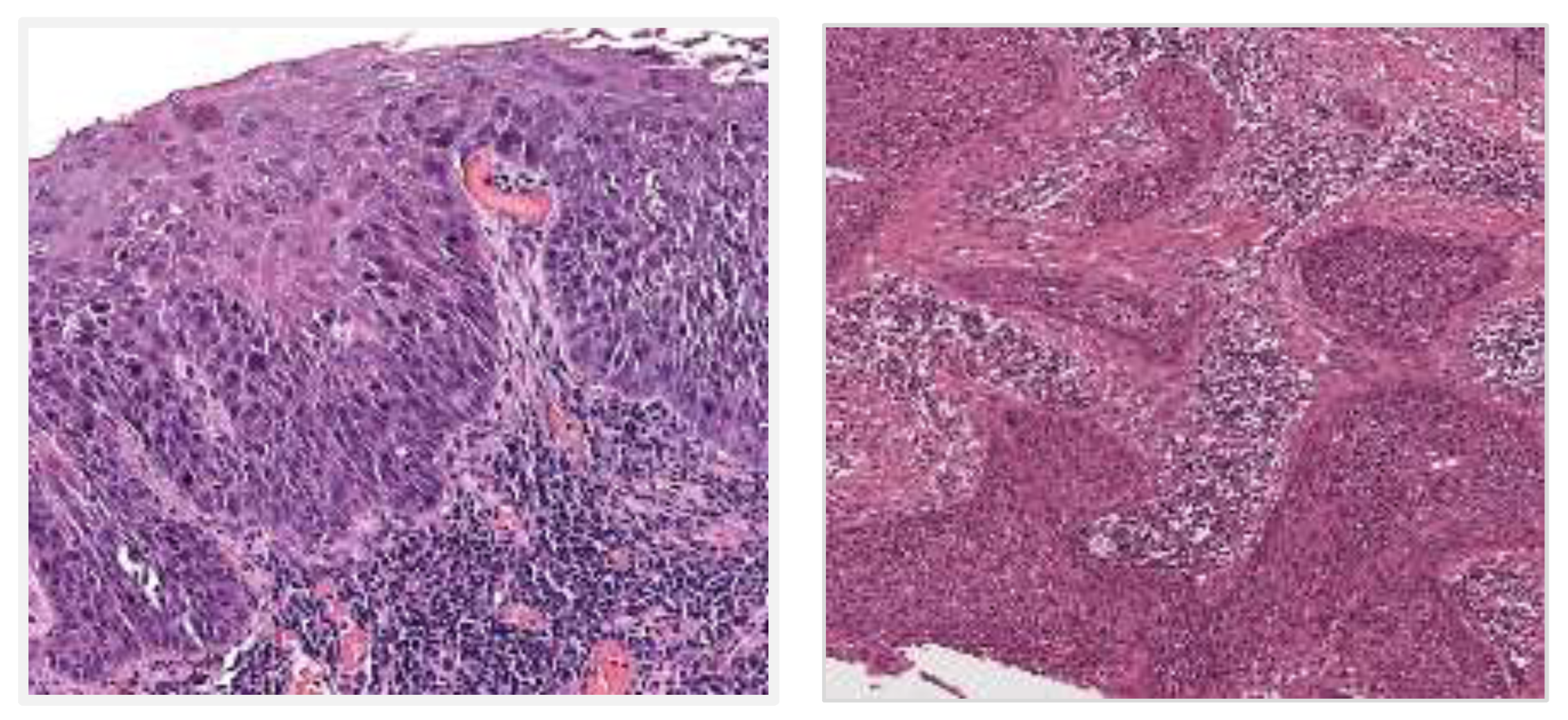

Table 1.
Anti-PDL1 therapies in invasive CSCC.
| Study | Patient (s) | Stage | Primary treatment | Agent used | Dosage | Outcome | Adverse reactions |
|---|---|---|---|---|---|---|---|
| Esmaeli et al, 2025 [40] | 17 (5 CSCC) | Advanced periocular SCC (orbital, conjunctival, lacrimal) | Neoadjuvant or definitive systemic ICI therapy | Cemiplimab or Pembrolizumab | Not specified | 5 complete responses, 8 partial responses, 4 stable disease. At least 1 CSCC with nodal metastasis achieved complete response and avoided surgery | Not specified |
| Azad et al, 2025 [41] | 5 | Advanced CSCC | Systemic ICI therapy | Not specified | Not specified | All showed progression, 3 required exenteration | |
| Kanda et al, 2025 [39] | 9 | Advanced CSCC | Systemic ICI therapy | Cemiplimab | Not specified | 22% complete response, 33% partial response, 44% progressed | Hypothyroidism, hepatitis |
| Ceylanoglu et al, 2024 [42] | 70Y, Male | CSIN lesion on ocular surface | Excisional biopsy with cryotherapy | Cemiplimab | 350 mg IV every 3 weeks | Response shown in metastatic lesions. CSIN continued to grow. | Not specified |
| Ceylanoglu et al, 2024 [42] | 84Y, Female | CSIN of inferior bulbar and palpebral conjunctiva | Excisional biopsy with cryotherapy | Cemiplimab | 350 mg IV every 3 weeks | Progression of CSIN | Not specified |
| Steren et al, 2022 [43] | 11 | CSCC with orbital involvement | Excisional biopsy | Cemiplimab | 350 mg IV every 3 weeks | Complete response in 9/11 patients | Not specified |
| Hoffmann et al, 2021 [44] | 59Y, Female | Recurrent CSCC | Radiotherapy | Cemiplimab | 3mg/kg IV every 2 weeks | Resolution after 19 months of treatment | None reported |
| Demirci at al, 2020 [37] | 5 (82M, 59M, 86F, 71M, 61M) |
Advanced CSCC with orbital involvement | Excisional biopsy | Pembrolizumab and Cemiplimab | Pembrolizumab – 350 mg every 3 weeks Cemiplimab – 200mg every 3 weeks |
4/5 patients complete response. 1 showed progression | 86M – Colitis, 86F – Rash, pain |
Table 2.
Targeted therapies in invasive CSSC.
| Study | Patient (s) | Stage | Primary treatment | Agent used | Dosage | Outcome | Adverse reactions |
|---|---|---|---|---|---|---|---|
| El Sawy et al, 2022 (EGFR inhibitor) [45] | 2 | Advanced CSCC | Topical/systemic therapy with surgery | Erlotinib, Cetuximab | Not specified | Regression of ocular tumour size after 7.5 months | None reported |
| Asena et al, 2015 (anti-VEGF) [114] | 6 | CSCC | Topical targeted therapy | Bevacizumab | 5 mg/ml eye drops, 4 times daily for 8 weeks | 2/6 complete tumour resolutions, 4 patients required excisional surgery | None reported |
| Faramarzi et al, 2013 (anti-VEGF) [115] | 10 | Combination of CSIN and CSCC | Perilesional/subconjunctival injection with excision/cryotherapy if needed | Bevacizumab | 2 injections at 2 week interval | Mean tumour area reduced by 25% after 1st and 42% after 2nd injection, complete disappearance in 2 eyes with CSIN only | None reported |
| Finger et al, 2012 (anti-VEGF) [47] | 5 | Recurrent CSCC | Excision, cryotherapy or topical therapy | Ranibizumab | 0.5 mg monthly or bimonthly | 3/5 complete responses, 2 failed treatment | None reported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



