
Submitted:
10 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
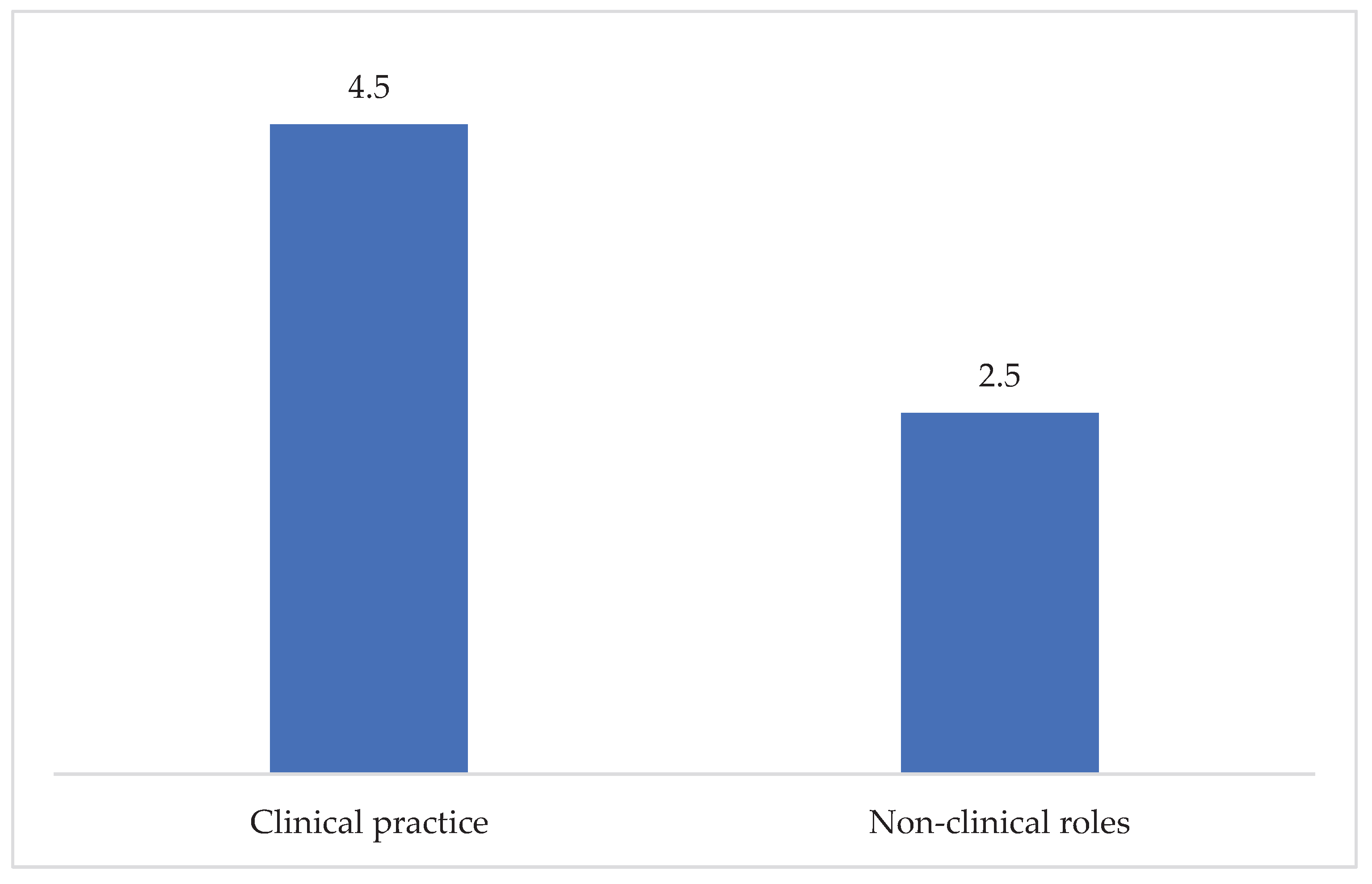
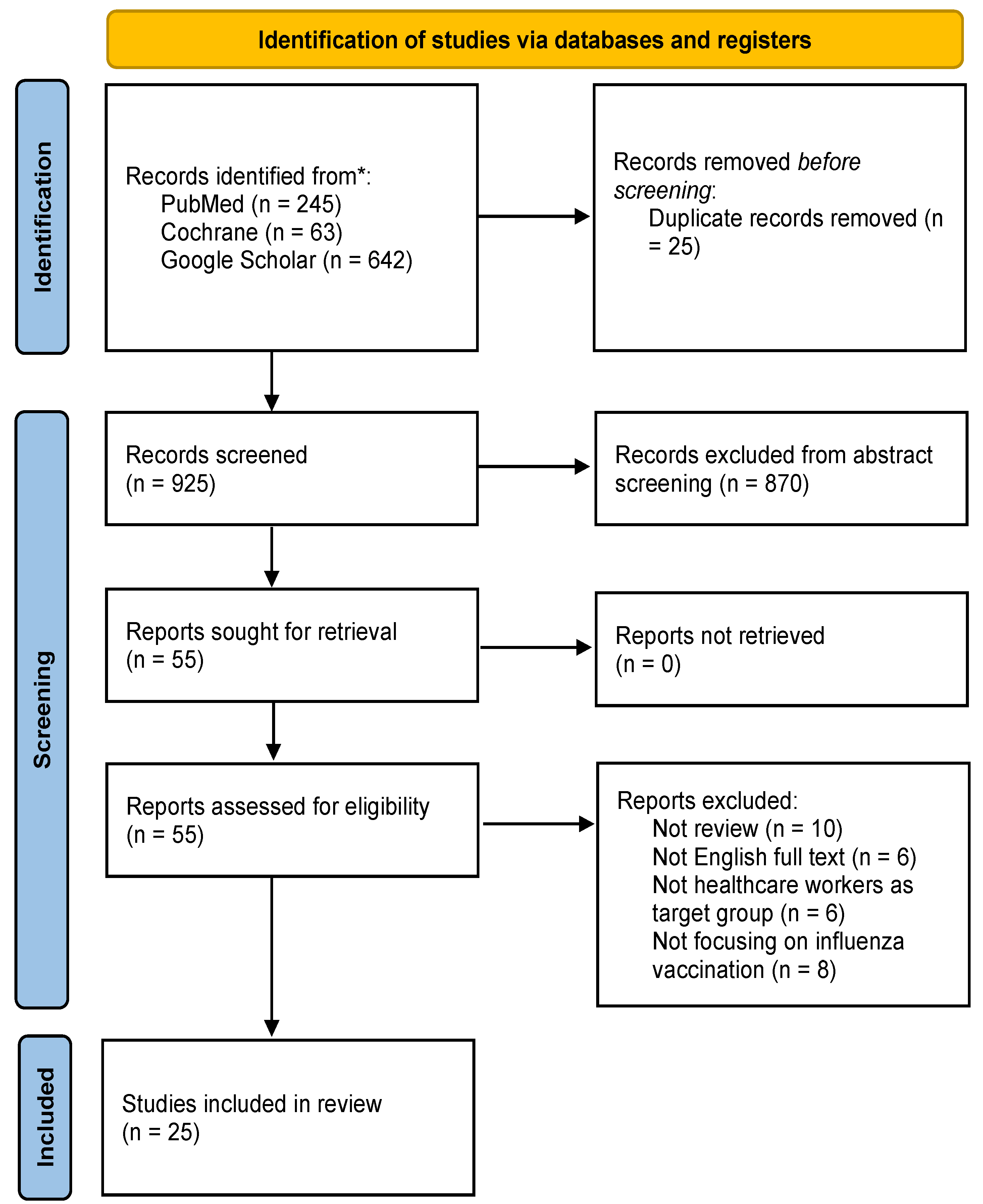
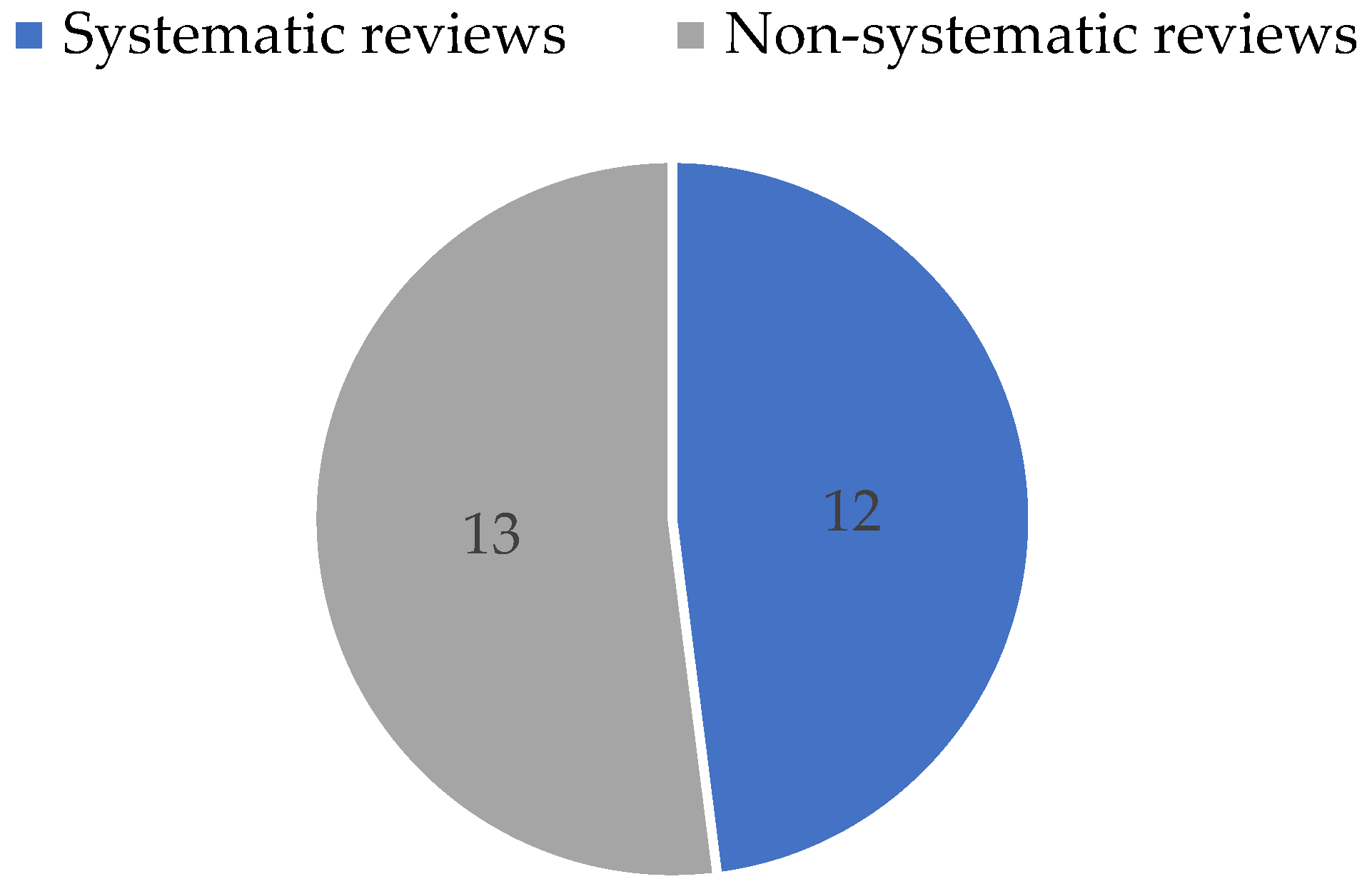
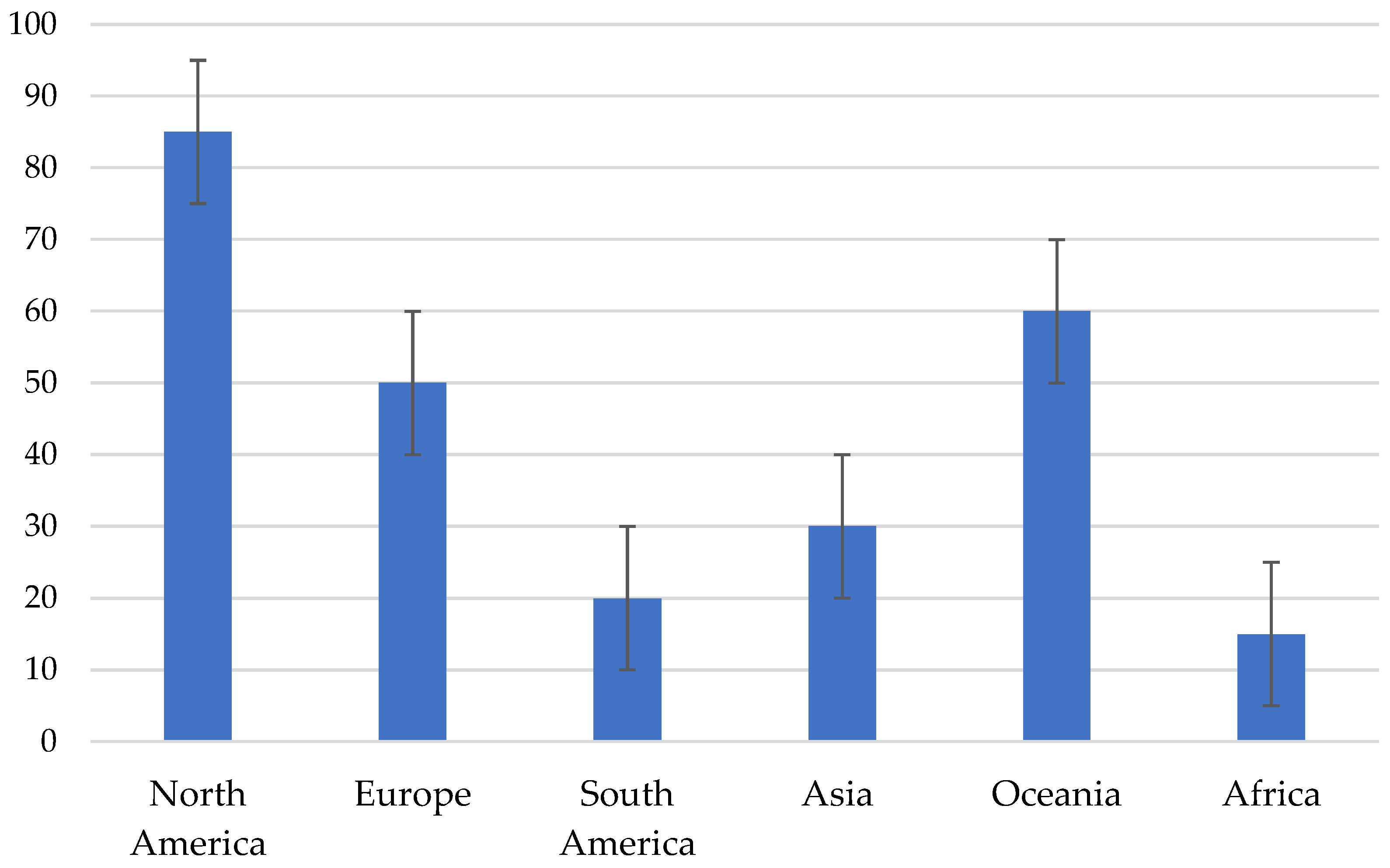
Background: Seasonal influenza remains a major public health challenge worldwide, causing significant morbidity each year and imposing substantial burdens on individuals, healthcare systems and national economies. Vaccination is considered the most effective available strategy for prevention; however, uptake rates vary considerably across countries, with many failing to achieve the recommended coverage levels. The aim of this review is to examine the beliefs, attitudes and behaviors of healthcare professionals worldwide regarding seasonal influenza vaccination. Methods: This is an umbrella review, according to the PRISMA Statement 2020, searching PubMed, Cochrane Library and Google Scholar. The following search terms were used: beliefs, attitudes, behaviors, influenza vaccination, flu vaccine, health professionals, primary health care. Selection criteria were the following: 1) Reviews, 2) Published after 1/1/2000, 3) English language 4) Healthcare professionals as target-population. Results: Twenty-five studies met the selection criteria and were included in this review. Twelve out of 25 studies were systematic reviews. Globally, vaccination uptake among healthcare professionals remains below recommended national and international targets. North America demonstrates the highest vaccination coverage, while the lowest coverage is reported in Africa and South America. Overall, low- and middle-income countries show significantly lower vaccination behavior compared with high-income countries. Attitudes and beliefs appear to shape vaccination behavior in high-income countries. The main driver of acceptance is perceived protection of oneself and family, whereas hesitancy is mainly driven by concerns about side effects and vaccine safety. Across studies, non-physician healthcare professionals consistently demonstrated lower influenza vaccine acceptance compared with physicians while pediatricians and general practitioners were found to receive the influenza vaccine more frequently. In addition, younger physicians and those with fewer years of professional experience showed higher vaccination coverage and a greater likelihood of recommending influenza vaccination to patients. Conclusions: Vaccination coverage, worldwide, is lower than what is recommended by the World Health Organization. Healthcare professionals, working in hospital settings, tend to be vaccinated at a higher rate and are more likely to recommend the vaccine to their patients. The recommendations that health professionals give are influenced by whether they accept influenza vaccines themselves. Beliefs and attitudes seem to influence behavior in countries where structural barriers, such as limited access to primary healthcare and socio-economic status are absent.
Keywords:
1. Introduction
2. Materials and Methods
3. Results
3.1. Selection and Characteristics of Included Studies
3.2. Materials and Methods Used for Data Collection in Included Studies
3.3. Knowledge, Attitudes, Beliefs and Behaviors of Healthcare Professionals Around the World
3.4. Differences Identified Among Healthcare Professionals
4. Discussion
4.1. Implications for Public Health Policy and Practice
5. Conclusions
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orenstein, W.A.; Ahmed, R. Simply Put: Vaccination Saves Lives. Proceedings of the National Academy of Sciences of the United States of America 2017, 114, 4031. [Google Scholar] [CrossRef] [PubMed]
- WHO Vaccines and Immunization. Available online: https://www.who.int/health-topics/vaccines-and-immunization (accessed on 29 August 2024).
- Nandi, A.; Shet, A. Why Vaccines Matter: Understanding the Broader Health, Economic, and Child Development Benefits of Routine Vaccination. Hum Vaccin Immunother 2020, 16, 1900–1904. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Nian, X.; Li, X.; Huang, S.; Duan, K.; Li, X.; Yang, X. The Epidemiology of Influenza and the Associated Vaccines Development in China: A Review. Vaccines (Basel) 2022, 10, 1873. [Google Scholar] [CrossRef] [PubMed]
- Teloniatis, S.; Tzortzi, A.; Behrakis, P. Seasonal Influenza Vaccination Coverage in Greece in 2009 and 2014. Pneumon 2017, 30, 41–48. [Google Scholar]
- Dardalas, I.; Pourzitaki, C.; Manomenidis, G.; Malliou, F.; Galanis, P.; Papazisis, G.; Kouvelas, D.; Bellali, T. Predictors of Influenza Vaccination among Elderly: A Cross-Sectional Survey in Greece. Aging Clin Exp Res 2020, 32, 1821–1828. [Google Scholar] [CrossRef]
- Ryu, S.; Cowling, B.J. Human Influenza Epidemiology. Cold Spring Harb Perspect Med 2021, 11, a038356. [Google Scholar] [CrossRef]
- Boktor, S.W.; Hafner, J.W. Influenza. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2024. [Google Scholar]
- WHO Influenza (Seasonal). Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 29 August 2024).
- Levin, P.J.; Gebbie, E.N.; Qureshi, K. Can the Health-Care System Meet the Challenge of Pandemic Flu? Planning, Ethical, and Workforce Considerations. Public Health Rep 2007, 122, 573–578. [Google Scholar] [CrossRef]
- Fischer, W.A.; Gong, M.; Bhagwanjee, S.; Sevransky, J. Global Burden of Influenza: Contributions from Resource Limited and Low-Income Settings. Glob Heart 2014, 9, 325–336. [Google Scholar] [CrossRef]
- de Courville, C.; Cadarette, S.M.; Wissinger, E.; Alvarez, F.P. The Economic Burden of Influenza among Adults Aged 18 to 64: A Systematic Literature Review. Influenza Other Respir Viruses 2022, 16, 376–385. [Google Scholar] [CrossRef]
- Romanelli, R.J.; Cabling, M.; Marciniak-Nuqui, Z.; Marjanovic, S.; Morris, S.; Dufresne, E.; Yerushalmi, E. The Societal and Indirect Economic Burden of Seasonal Influenza in the United Kingdom. Rand Health Q 2023, 10, 2. [Google Scholar]
- Alasmari, A.; Larson, H.J.; Karafillakis, E. A Mixed Methods Study of Health Care Professionals’ Attitudes towards Vaccination in 15 Countries. Vaccine: X 2022, 12, 100219. [Google Scholar] [CrossRef] [PubMed]
- Taskou, C.; Sarantaki, A.; Beloukas, A.; Georgakopoulou, V.Ε.; Daskalakis, G.; Papalexis, P.; Lykeridou, A. Knowledge and Attitudes of Healthcare Professionals Regarding Perinatal Influenza Vaccination during the COVID-19 Pandemic. Vaccines (Basel) 2023, 11, 168. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Díaz, F. del C.; Jiménez-Corona, M.E.; Ponce-de-León-Rosales, S. Influenza Vaccine and Healthcare Workers. Archives of Medical Research 2011, 42, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Alalag, Z.A.; Al-Jumaili, A.A.; Al-Hamadani, F.Y. A Comprehensive Review of Drivers Influencing Flu Vaccine Acceptance in the Middle East over the Last Six Years: Using Health Belief Model. International Journal of Pharmacy Practice 2022, 30, 5–16. [Google Scholar] [CrossRef]
- Alfouzan, N.; Almujil, A.; Demyati, E.; AlOtaiby, S. Motivators and Barriers for Seasonal Influenza Vaccination among Healthcare Workers in Gulf Cooperation Council Countries: A Systematic Review. IJMDC 2022, 882–890. [Google Scholar] [CrossRef]
- Bellia, C.; Setbon, M.; Zylberman, P.; Flahault, A. Healthcare Worker Compliance with Seasonal and Pandemic Influenza Vaccination. Influenza and Other Respiratory Viruses 2013, 7, 97–104. [Google Scholar] [CrossRef]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors Associated with Uptake of Vaccination against Pandemic Influenza: A Systematic Review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef]
- Dang, A.; Sharma, J. Assessing the Low Influenza Vaccination Coverage Rate Among Healthcare Personnel in India: A Review of Obstacles, Beliefs, and Strategies. Value in Health Regional Issues 2020, 21, 100–104. [Google Scholar] [CrossRef]
- Dardas, L.A.; Al-leimon, O.; Jaber, A.R.; Saadeh, M.; Al-leimon, A.; Al-Hurani, A.; Jaber, A.-R.; Aziziye, O.; Al-salieby, F.; Aljahalin, M.; et al. Flu Shots Unveiled: A Global Systematic Review of Healthcare Providers’ Uptake of, Perceptions, and Attitudes toward Influenza Vaccination. Vaccines 2023, 11, 1760. [Google Scholar] [CrossRef]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza Vaccination in Healthcare Workers: A Comprehensive Critical Appraisal of the Literature. Human Vaccines & Immunotherapeutics 2017, 14, 772. [Google Scholar] [CrossRef]
- Diomidous, M.; Isaakidou, M. Factors Influencing the Implementation of Flu Vaccination in Healthcare Professionals: Pros and Cons. Mater Sociomed 2020, 32, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Xu, S.; Liu, Y.; Ma, X.; Cao, J.; Fan, C.; Bao, S. Influenza Vaccination Rates among Healthcare Workers: A Systematic Review and Meta-Analysis Investigating Influencing Factors. Front. Public Health 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Glenton, C.; Carlsen, B.; Lewin, S.; Wennekes, M.D.; Winje, B.A.; Eilers, R. Consortium, on behalf of the V. Healthcare Workers’ Perceptions and Experiences of Communicating with People over 50 Years of Age about Vaccination: A Qualitative Evidence Synthesis - Glenton, C - 2021; Cochrane Library., 2021. [Google Scholar]
- Guillari, A.; Polito, F.; Pucciarelli, G.; Serra, N.; Gargiulo, G.; Esposito, M.R.; Botti, S.; Rea, T.; Simeone, S. Influenza Vaccination and Healthcare Workers: Barriers and Predisposing Factors. Acta Biomed 2021, 92, e2021004. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.M.; Northam, H.; Webster, A.; Strickland, K. Determinants of Seasonal Influenza Vaccination Hesitancy among Healthcare Personnel: An Integrative Review. Journal of Clinical Nursing 2022, 31, 2112–2124. [Google Scholar] [CrossRef]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are Healthcare Workers’ Intentions to Vaccinate Related to Their Knowledge, Beliefs and Attitudes? A Systematic Review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- Hollmeyer, H.G.; Hayden, F.; Poland, G.; Buchholz, U. Influenza Vaccination of Health Care Workers in Hospitals—A Review of Studies on Attitudes and Predictors. Vaccine 2009, 27, 3935–3944. [Google Scholar] [CrossRef]
- JĘdrzejek, M. jacek; Mastalerz-Migas, A. Seasonal Influenza Vaccination of Healthcare Workers: A Narrative Review. Int J Occup Med Environ Health 2022, 35, 127–139. [Google Scholar] [CrossRef]
- Lorenc, T.; Marshall, D.; Wright, K.; Sutcliffe, K.; Sowden, A. 32Seasonal Influenza Vaccination of Healthcare Workers: Systematic Review of Qualitative Evidence. BMC Health Serv Res 2017, 17, 732. [Google Scholar] [CrossRef]
- Nowak, G.J.; Sheedy, K.; Bursey, K.; Smith, T.M.; Basket, M. 33Promoting Influenza Vaccination: Insights from a Qualitative Meta-Analysis of 14 Years of Influenza-Related Communications Research by U.S. Centers for Disease Control and Prevention (CDC). Vaccine 2015, 33, 2741–2756. [Google Scholar] [CrossRef]
- Prematunge, C.; Corace, K.; McCarthy, A.; Nair, R.C.; Pugsley, R.; Garber, G. 34Factors Influencing Pandemic Influenza Vaccination of Healthcare Workers—A Systematic Review. Vaccine 2012, 30, 4733–4743. [Google Scholar] [CrossRef]
- Seale, H.; Macintyre, C.R. 35Seasonal Influenza Vaccination in Australian Hospital Health Care Workers: A Review. Med J Aust 2011, 195, 336–338. [Google Scholar] [CrossRef]
- Sheldenkar, A.; Lim, F.; Yung, C.F.; Lwin, M.O. 36Acceptance and Uptake of Influenza Vaccines in Asia: A Systematic Review. Vaccine 2019, 37, 4896–4905. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.B.; Souza, F. de O.; Pinho, P. de S.; Santos, D.V. Health Belief Model in Studies of Influenza Vaccination among Health Care Workers. Rev Bras Med Trab 2023, 21, e2022839. [Google Scholar] [CrossRef] [PubMed]
- Sydnor, E.; Perl, T.M. Healthcare Providers as Sources of Vaccine-Preventable Diseases. Vaccine 2014, 32, 4814–4822. [Google Scholar] [CrossRef] [PubMed]
- To, K.W.; Lai, A.; Lee, K.C.K.; Koh, D.; Lee, S.S. Increasing the Coverage of Influenza Vaccination in Healthcare Workers: Review of Challenges and Solutions. Journal of Hospital Infection 2016, 94, 133–142. [Google Scholar] [CrossRef]
- Waszkiewicz, M.; Wnuk, K.; Świtalski, J.; Augustynowicz, A. Knowledge, Attitudes, and Beliefs of Pharmacists Regarding Vaccinations against Influenza and Pneumococci - a Systematic Review. Hum Vaccin Immunother 2025, 21, 2489889. [Google Scholar] [CrossRef]
- National Research Council (US) The Epidemiological Transition in Africa: Are There Lessons from Asia? In The Continuing Epidemiological Transition in Sub-Saharan Africa: A Workshop Summary; National Academies Press (US), 2012.
- Sharma, S.; Verhagen, A.; Elkins, M.; Brismée, J.-M.; Fulk, G.D.; Taradaj, J.; Steen, L.; Jette, A.; Moore, A.; Stewart, A.; et al. Research from Low-Income and Middle-Income Countries Will Benefit Global Health and the Physiotherapy Profession, but It Requires Support. International Journal of Sports Physical Therapy 2023, 18, 83948. [Google Scholar] [CrossRef]
- Nogareda, F.; Gharpure, R.; Contreras, M.; Velandia, M.; Pacis, C.L.; Chevez, A.E.; Azziz-Baumgartner, E.; Salas, D. Seasonal Influenza Vaccination in the Americas: Progress and Challenges during the COVID-19 Pandemic. Vaccine 2023. [Google Scholar] [CrossRef]
- Perl, T.M.; Talbot, T.R. Universal Influenza Vaccination Among Healthcare Personnel: Yes We Should. Open Forum Infectious Diseases 2019, 6, ofz096. [Google Scholar] [CrossRef]
- Gruben, V.; Siemieniuk, R.A.; McGeer, A. Health Care Workers, Mandatory Influenza Vaccination Policies and the Law. CMAJ: Canadian Medical Association Journal 2014, 186, 1076. [Google Scholar] [CrossRef]
- Chen, C.; Liu, X.; Yan, D.; Zhou, Y.; Ding, C.; Chen, L.; Lan, L.; Huang, C.; Jiang, D.; Zhang, X.; et al. 46Global Influenza Vaccination Rates and Factors Associated with Influenza Vaccination. Int J Infect Dis 2022, 125, 153–163. [Google Scholar] [CrossRef] [PubMed]
- González-Block, M.Á.; Gutiérrez-Calderón, E.; Pelcastre-Villafuerte, B.E.; Arroyo-Laguna, J.; Comes, Y.; Crocco, P.; Fachel-Leal, A.; Noboa, L.; Riva-Knauth, D.; Rodríguez-Zea, B.; et al. Influenza Vaccination Hesitancy in Five Countries of South America. Confidence, Complacency and Convenience as Determinants of Immunization Rates. PLoS One 2020, 15, e0243833. [Google Scholar] [CrossRef] [PubMed]
- Awaidi, S.A.; Abusrewil, S.; AbuHasan, M.; Akcay, M.; Aksakal, F.N.; Bashir, U.; Elahmer, O.; Esteghamati, A.; Gahwagi, M.; et al.; Group, 7th MENA-ISN study Influenza Vaccination Situation in Middle-East and North Africa Countries: Report of the 7th MENA Influenza Stakeholders Network (MENA-ISN). Journal of Infection and Public Health 2018, 11, 845. [Google Scholar] [CrossRef] [PubMed]
- González-Block, M.Á.; Portillo, S.P.D.; Laguna, J.A.; Comes, Y.; Crocco, P.; Fachel-Leal, A.; Noboa, L.; Knauth, D.R.; Rodríguez-Zea, B.; Ruoti, M.; et al. Barriers and Facilitators to Influenza Vaccination Observed by Officers of National Immunization Programs in South America Countries with Contrasting Coverage Rates. Cad. Saúde Pública 2022, 38, e00045721. [Google Scholar] [CrossRef]
- Kraigsley, A.M.; Moore, K.A.; Bolster, A.; Peters, M.; Richardson, D.; Arpey, M.; Sonnenberger, M.; McCarron, M.; Lambach, P.; Maltezou, H.C.; et al. Barriers and Activities to Implementing or Expanding Influenza Vaccination Programs in Low- and Middle-Income Countries: A Global Survey. Vaccine 2021, 39, 3419–3427. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Tseroni, M.; Raftopoulos, V.; Bolster, A.; Kraigsley, A.; Bresee, J.; Lambach, P. Influenza Vaccination Policies for Health Workers in Low-Income and Middle-Income Countries: A Cross-Sectional Survey, January-March 2020. Vaccine 2020, 38, 7433–7439. [Google Scholar] [CrossRef]
- Schumacher, S.; Salmanton-García, J.; Liekweg, A.; Rolfes, M.; Seidel, D.; Mellinghoff, S.C.; Cornely, O.A. Increasing Influenza Vaccination Coverage in Healthcare Workers: Analysis of an Intensified on-Site Vaccination Campaign during the COVID-19 Pandemic. Infection 2023, 51, 1417. [Google Scholar] [CrossRef]
- Seale, H.; Leask, J.; MacIntyre, C.R. Attitudes amongst Australian Hospital Healthcare Workers towards Seasonal Influenza and Vaccination. Influenza Other Respir Viruses 2010, 4, 41–46. [Google Scholar] [CrossRef]
- Squeri, R.; Pietro, A.D.; Fauci, V.L.; Genovese, C. Healthcare Workers’ Vaccination at European and Italian Level: A Narrative Review. Acta Bio Medica: Atenei Parmensis 2019, 90, 45. [Google Scholar] [CrossRef]
- Ward, K.; Seale, H.; Zwar, N.; Leask, J.; MacIntyre, C.R. Annual Influenza Vaccination: Coverage and Attitudes of Primary Care Staff in Australia. Influenza and Other Respiratory Viruses 2010, 5, 135. [Google Scholar] [CrossRef]
- Jennings, L.; Huang, Q.S.; Barr, I.; Lee, P.-I.; Kim, W.J.; Buchy, P.; Sanicas, M.; Mungall, B.A.; Chen, J. Literature Review of the Epidemiology of Influenza B Disease in 15 Countries in the Asia-Pacific Region. Influenza and Other Respiratory Viruses 2018, 12, 383. [Google Scholar] [CrossRef] [PubMed]
- de Lusignan, S.; Correa, A.; Ellis, J.; Pebody, R. Influenza Vaccination: In the UK and across Europe. The British Journal of General Practice 2016, 66, 452. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, C.; Rezza, G.; Ricciardi, W. Strategies in Recommending Influenza Vaccination in Europe and US. Human Vaccines & Immunotherapeutics 2018, 14, 693. [Google Scholar] [CrossRef]
- Young, B.E.; Chen, M. Influenza in Temperate and Tropical Asia: A Review of Epidemiology and Vaccinology. Human Vaccines & Immunotherapeutics 2020, 16, 1659–1667. [Google Scholar] [CrossRef]
- Abu-Gharbieh, E.; Fahmy, S.; Rasool, B.A.; Khan, S. Influenza Vaccination: Healthcare Workers Attitude in Three Middle East Countries. International Journal of Medical Sciences 2010, 7, 319. [Google Scholar] [CrossRef]
- Alsuhaibani, M. Barriers and Beliefs among Health-Care Workers Regarding Seasonal Influenza Vaccine in Al-Qassim Region, Saudi Arabia. Human Vaccines & Immunotherapeutics 2019, 16, 313. [Google Scholar] [CrossRef]
- Awadalla, N.J.; Al-Musa, H.M.; Al-Musa, K.M.; Asiri, A.M.; Albariqi, A.A.; Majrashi, H.M.; Alasim, A.A.; Almuslah, A.S.; Alshehri, T.K.; AlFlan, M.A.; et al. Seasonal Influenza Vaccination among Primary Health Care Workers in Southwestern Saudi Arabia. Hum Vaccin Immunother 2020, 16, 321–326. [Google Scholar] [CrossRef]
- Guerrero-Soler, M.; Gras-Valenti, P.; Platas-Abenza, G.; Sánchez-Payá, J.; Sanjuan-Quiles, Á.; Chico-Sánchez, P. Group, on behalf of the P.M.V.W. Impact of the COVID-19 Pandemic on Influenza Vaccination Coverage of Healthcare Personnel in Alicante, Spain. Vaccines 2024, 12, 370. [Google Scholar] [CrossRef]
- Scardina, G.; Ceccarelli, L.; Casigliani, V.; Mazzilli, S.; Napoletano, M.; Padovan, M.; Petillo, A.; Sironi, D.; Brilli, C.; Gattini, V.; et al. Evaluation of Flu Vaccination Coverage among Healthcare Workers during a 3 Years’ Study Period and Attitude towards Influenza and Potential COVID-19 Vaccination in the Context of the Pandemic. Vaccines 2021, 9, 769. [Google Scholar] [CrossRef]
- Calabrò, G.E.; Rumi, F.; Fallani, E.; Ricciardi, R.; Cicchetti, A. The Economic and Fiscal Impact of Influenza Vaccination for Health Care Workers in Italy. Vaccines 2022, 10, 1707. [Google Scholar] [CrossRef]
- Gaskin, C.M.; Woods, D.R.; Ghosh, S.; Watson, S.; Huber, L.R. The Effect of Income Disparities on Influenza Vaccination Coverage in the United States. Public Health Rep 2023, 138, 85–90. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, T.; Yao, M.; Kou, Z.; Li, R. Exploring Barriers to Influenza Vaccine Uptake and Recommendation among Healthcare Providers in the Community in China: A Qualitative Study. Human Vaccines & Immunotherapeutics 2024, 20, 2352916. [Google Scholar] [CrossRef] [PubMed]
- Ott, J.J.; Breteler, J.K.; Tam, J.S.; Hutubessy, R.C.; Jit, M.; Boer, M.R. de Influenza Vaccines in Low and Middle Income Countries: A Systematic Review of Economic Evaluations. Human Vaccines & Immunotherapeutics 2013, 9, 1500. [Google Scholar] [CrossRef]
- Dubé, È.; Farrands, A.; Lemaitre, T.; Boulianne, N.; Sauvageau, C.; Boucher, F.D.; Tapiero, B.; Quach, C.; Ouakki, M.; Gosselin, V.; et al. Overview of Knowledge, Attitudes, Beliefs, Vaccine Hesitancy and Vaccine Acceptance among Mothers of Infants in Quebec, Canada. Hum Vaccin Immunother 2019, 15, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Olivero, E.; Voglino, G.; Corezzi, M.; Rossello, P.; Vicentini, C.; Bert, F.; Siliquini, R. Knowledge, Attitudes and Beliefs towards Compulsory Vaccination: A Systematic Review. Human Vaccines & Immunotherapeutics 2019, 15, 918. [Google Scholar] [CrossRef]
- Pelullo, C.P.; Polla, G.D.; Napolitano, F.; Giuseppe, G.D.; Angelillo, I.F. Healthcare Workers’ Knowledge, Attitudes, and Practices about Vaccinations: A Cross-Sectional Study in Italy. Vaccines 2020, 8, 148. [Google Scholar] [CrossRef]
- Puertas, E.B.; Velandia-Gonzalez, M.; Vulanovic, L.; Bayley, L.; Broome, K.; Ortiz, C.; Rise, N.; Antelo, M.V.; Rhoda, D.A. Concerns, Attitudes, and Intended Practices of Caribbean Healthcare Workers Concerning COVID-19 Vaccination: A Cross-Sectional Study. The Lancet Regional Health – Americas 2022, 9. [Google Scholar] [CrossRef]
- Baral, P.; Ahmed, T.; Fernandez, P.A.; Peters, M.A.; Drouard, S.H.P.; Muhoza, P.; Mwinnyaa, G.; Mwansambo, C.; Nzelu, C.; Tassembedo, M.; et al. Vaccine Hesitancy among Healthcare Workers in Low- and Middle-Income Countries during the COVID-19 Pandemic: Results from Facility Surveys across Six Countries. PLOS ONE 2023, 18, e0288124. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 Vaccine Acceptance and Hesitancy in Low- and Middle-Income Countries. Nat Med 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Corace, K.; Prematunge, C.; McCarthy, A.; Nair, R.C.; Roth, V.; Hayes, T.; Suh, K.N.; Balfour, L.; Garber, G. Predicting Influenza Vaccination Uptake among Health Care Workers: What Are the Key Motivators? Am J Infect Control 2013, 41, 679–684. [Google Scholar] [CrossRef]
- Bellali, T.; Liamopoulou, P.; Karavasileiadou, S.; Almadani, N.; Galanis, P.; Kritsotakis, G.; Manomenidis, G. Intention, Motivation, and Empowerment: Factors Associated with Seasonal Influenza Vaccination among Healthcare Workers (HCWs). Vaccines 2023, 11, 1508. [Google Scholar] [CrossRef]
- Riphagen-Dalhuisen, J.; Gefenaite, G.; Hak, E. Predictors of Seasonal Influenza Vaccination among Healthcare Workers in Hospitals: A Descriptive Meta-Analysis. Occup Environ Med 2012, 69, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Mubarak, S.; AlGhawrie, H.; Qaddumi, B. Knowledge, Attitudes, Concern, Behaviors, and Barriers Associated with the Readiness to Receive Seasonal Influenza Vaccine among Healthcare Workers in Oncology Setting during the COVID-19 Pandemic. Human Vaccines & Immunotherapeutics 2023, 19, 2251836. [Google Scholar] [CrossRef] [PubMed]
- Vijayasaratha, K.; Basumani, K.; Sasank, A. Influenza Vaccination Uptake, Awareness, and Barriers among Healthcare Workers (HCWs) at Tertiary Care Setting in India. European Respiratory Journal 2019, 54. [Google Scholar] [CrossRef]
- Hussein, Y.H.H.; Ibrahim, M.H.; Badran, S.G.; Eldeeb, S.M. Hesitancy for Influenza Vaccine among Healthcare Workers and Mothers of Preschool Children: A Cross-Sectional Study in Zagazig, Egypt. Journal of Family and Community Medicine 2022, 29, 108. [Google Scholar] [CrossRef]
- Hwang, S.W.; Lim, H.B. Barriers and Motivators of Influenza Vaccination Uptake among Primary Healthcare Workers in Singapore. Proceedings of Singapore Healthcare 2014, 23, 126–133. [Google Scholar] [CrossRef]
- Christini, A.B.; Shutt, K.A.; Byers, K.E. Influenza Vaccination Rates and Motivators among Healthcare Worker Groups. Infect Control Hosp Epidemiol 2007, 28, 171–177. [Google Scholar] [CrossRef]
- Simeonsson, K.; Summers-Bean, C.; Connolly, A. Influenza Vaccination of Healthcare Workers: Institutional Strategies for Improving Rates. N C Med J 2004, 65, 323–329. [Google Scholar] [CrossRef]
- Tuckerman, J.L.; Collins, J.E.; Marshall, H.S. Factors Affecting Uptake of Recommended Immunizations among Health Care Workers in South Australia. Hum Vaccin Immunother 2015, 11, 704–712. [Google Scholar] [CrossRef]
- Hadigal, S.; Cook, J. Knowledge and Perception Regarding Effectiveness in Influenza Vaccines among General Practitioners in Germany: A National Survey. Vaccine: X 2022, 12, 100236. [Google Scholar] [CrossRef]
- Hussain, H.; McGeer, A.; McNeil, S.; Katz, K.; Loeb, M.; Simor, A.; Powis, J.; Langley, J.; Muller, M.; Canadian Health Care Worker Study Group; et al. Factors Associated with Influenza Vaccination among Healthcare Workers in Acute Care Hospitals in Canada. Influenza Other Respir Viruses 2018, 12, 319–325. [Google Scholar] [CrossRef]
- Lauer, J.; Kastner, J.; Nutsch, A. Primary Care Physicians and Pandemic Influenza: An Appraisal of the 1918 Experience and an Assessment of Contemporary Planning. J Public Health Manag Pract 2008, 14, 379–386. [Google Scholar] [CrossRef]
- Passi, V.; Johnson, N. The Impact of Positive Doctor Role Modeling. Med Teach 2016, 38, 1139–1145. [Google Scholar] [CrossRef]
- Watanakunakorn, C.; Ellis, G.; Gemmel, D. Attitude of Healthcare Personnel Regarding Influenza Immunization. Infect Control Hosp Epidemiol 1993, 14, 17–20. [Google Scholar] [CrossRef]
- Alauzet, P.; Morand, A.; Mazenq, J.; Gaudart, J.; Bosdure, E.; Dubus, J.-C. Key Role of Pediatricians and Disease for Influenza Vaccination in Children with High-Risk Chronic Diseases. Eur J Pediatr 2021, 180, 303–306. [Google Scholar] [CrossRef]

| Authors | Publication date |
Region | Health profession |
Aim | Materials and methods | Beliefs, attitudes and behaviors |
|---|---|---|---|---|---|---|
| Aguilar-Díaz et al. [16] | 2011 | Worldwide | Health professionals | Identification of factors influencing healthcare workers’ influenza vaccination acceptance | A review of PubMed, OVID, and Google Scholar, resulting in the inclusion of 30 studies | Vaccination coverage among healthcare professionals is low. Factors that act as barriers and increase non-acceptance include perceptions of vaccine effectiveness and safety. Factors that enhance acceptance include perceptions of personal and family safety |
| Alalag et al. [17] | 2022 | Middle East | Health professionals | An investigation of the factors influencing influenza vaccination coverage | Systematic review of PubMed and Google Scholar resulting in the inclusion of 34 studies | Vaccination coverage among healthcare professionals is higher than that of the general population but remains low relative to the desired levels. The increased risk in healthcare professionals’ work environment appears to play some role. Barriers seem to include misconceptions about vaccine safety and effectiveness |
| Alfouzan et al. [18] | 2022 | Middle East | Health professionals | A review of the barriers and motivators influencing healthcare professionals’ uptake of the seasonal influenza vaccine | A systematic review of PubMed, Web of Science, Google Scholar, EMBASE, Scopus, and the Directory of Open Access Journals, resulting in the final inclusion of 20 studies | Vaccination coverage among healthcare professionals is relatively low, below 50%. This may be due to many varied factors, such as perceived safety and perceived effectiveness. Free availability of vaccines and vaccination within healthcare facilities, combined with educational campaigns to change healthcare professionals’ attitudes, can increase vaccination coverage |
| Bellia et al. [19] | 2013 | Worldwide | Health professionals | An investigation of the factors that influence healthcare professionals’ decisions to undergo influenza vaccination | Review of 250 publications in the Web of Science database | The main factors driving healthcare professionals to receive the influenza vaccine are perceived severity of the disease and perceived vulnerability. Some of the reasons for non-compliance are related to the perception that it is a mild illness and, therefore, vaccination is unnecessary |
| Bish et al. [20] | 2011 | Worldwide | Health professionals | An investigation of the factors that determine influenza vaccination coverage | Systematic review of Web of Science resulting in the inclusion of 37 studies | Perceived threat from previous experiences with influenza epidemics or pandemics and perceived effectiveness of the vaccine play an important role in the decision to receive influenza vaccine. Inhibitory factors include the perceived severity of influenza and the perceived safety of the vaccines |
| Dang & Sharma [21] | 2020 | India | Health professionals | Highlighting vaccination coverage and healthcare professionals’ perceptions regarding vaccine effectiveness | Review of 21 publications of PubMed. | Data on vaccination coverage among healthcare professionals in India are limited. However, the increasing incidence of influenza among unvaccinated healthcare professionals indicates low vaccination coverage. The main factors influencing the decision appear to be lack of awareness about availability, doubts about effectiveness, fear of side effects, and perceived risk from the disease |
| Dardas et al. [22] | 2023 | Worldwide | Health professionals | An investigation of the factors that influence healthcare professionals’ decisions to receive influenza vaccination | Systematic review of: Database of Abstracts of Reviews of Effects (DARE), Cochrane Database of Systematic Reviews (CDSR), PubMed, CINAHL, PsycINFO, Scopus, Web of Science, EMBASE. Inclusion of 368 studies | Vaccination coverage among healthcare professionals appears to be positively influenced by the perception that influenza vaccines provide protection for themselves and their families, and negatively influenced by concerns about the safety of influenza vaccines |
| Dini et al. [23] | 2017 | Worldwide | Health professionals | Investigation of the factors influencing healthcare professionals’ decisions to receive the influenza vaccine | Systematic review in 27 databases. Inclusion of 28 studies | Vaccination coverage among healthcare professionals seems to be more often positively influenced by the perception that influenza vaccines will help protect themselves and their families, and negatively influenced by concerns about the safety of influenza vaccines |
| Diomidous & Isaakidou [24] | 2020 | Greece, Europe and USA | Health professionals | Investigation of factors influencing healthcare professionals’ acceptance of the influenza vaccine | Review of PubMed, Medscape, Scopus, Google Scholar. Inclusion of 10 studies | Influenza vaccination coverage among healthcare professionals is low. Healthcare professionals working in health centers and community centers have higher vaccination coverage compared to those working in hospitals. A sense of responsibility toward colleagues and patients appears to positively influence healthcare professionals’ attitudes toward vaccination |
| Fan et al. [25] | 2023 | Worldwide | Health professionals | Assessment of influenza vaccination coverage among healthcare professionals and identification of the factors that determine it | Systematic review of PubMed, EMBASE, CNKI, CBM, Wanfang, and VIP. Meta-analysis conducted. Inclusion of 92 studies | Global vaccination coverage among healthcare professionals is estimated at approximately 40%. The most frequently reported reasons for vaccination are self-protection and protecting family, while the reasons for non-vaccination are perceived ineffectiveness and concerns about potential adverse effects |
| Glenton et al. [26] | 2021 | Worldwide | Health professionals | Investigation of healthcare professionals’ perceptions of influenza vaccination and their impact on patients over 50 years of age | Systematic review of MEDLINE, CINAHL, Scopus, Epistemonikos, and grey literature. Inclusion of 11 studies | It appears that whether patients get vaccinated is significantly influenced by healthcare professionals. By having healthcare professionals as role models, patients are affected not only by communication and guidance but also by the actual behaviors of healthcare professionals regarding influenza vaccination |
| Guillari et al. [27] | 2021 | Worldwide | Health professionals | Investigation of healthcare professionals’ perceptions of influenza vaccination | Review of PubMed and CINAHL. Inclusion of 22 studies | A key factor driving healthcare professionals to get vaccinated is the perception of protecting themselves, their family, and their community. Factors that prevent them from vaccination include fear of illness caused by the vaccines, the perception that they are not at risk, and the belief that their immune system is strong |
| Hall et al. [28] | 2022 | Worldwide | Health professionals | Investigation of healthcare professionals’ attitudes toward influenza vaccination | Systematic review of CINAHL, PsycINFO, Medline, LILACS, Embase, and Scopus. Inclusion of 75 studies | Vaccination coverage among healthcare professionals is lower than the desired levels globally. The decision may be influenced by perceived susceptibility to influenza, perceptions of vaccine effectiveness and safety, and a history of previous influenza infection |
| Herzog et al. [29] | 2013 | Developed countries | Health professionals | Investigation of the impact of healthcare professionals’ beliefs, attitudes, and behaviors regarding vaccination on their recommendations | Systematic review of PubMed, EMBASE, CINAHL, and CENTRAL. Inclusion of 15 studies | It appears to be a connection between healthcare professionals’ beliefs, attitudes, and behaviors and their recommendations for vaccination to the general population. Low vaccination coverage among healthcare professionals may, to some extent, also shape the vaccination coverage of the general population |
| Hollmeyer et al. [30] | 2009 | Worldwide | Health professionals | Investigation of factors influencing healthcare professionals’ acceptance of the influenza vaccine | Review of PubMed. Inclusion of 25 studies | The perception of personal protection and protection of one’s family were key factors promoting acceptance of influenza vaccines. Misconceptions and incorrect knowledge regarding vaccine effectiveness and safety were major barriers leading to non-acceptance |
| JĘdrzejek & Mastalerz-Migas [31] | 2022 | Worldwide | Health professionals | Highlighting the impact of influenza on healthcare professionals and emphasizing the protective effect of influenza vaccination | Review of PubMed. Inclusion of 12 studies | Global influenza vaccination coverage among healthcare professionals is estimated to range from 2% to 44%, while the recommended rate is 90%. This is partly due to gaps in the global literature regarding the clarity of the benefits of influenza vaccination for healthcare professionals. Interventions aimed at changing healthcare professionals’ attitudes may contribute to improving coverage |
| Lorenc et al. [32] | 2017 | Worldwide | Health professionals | Investigation of healthcare professionals’ perceptions of influenza vaccination | Systematic review of MEDLINE, EMBASE, and CINAHL. Inclusion of 25 studies | Healthcare professionals get vaccinated to protect themselves and their patients. Reasons that deter vaccination include doubts about the effectiveness and safety of vaccines and the perception that influenza is not a serious illness |
| Nowak et al. [33] | 2015 | USA | Health professionals | Investigation of healthcare professionals’ perceptions regarding influenza vaccination | Review of 29 unpublished studies supported by the CDC | Vaccination coverage among healthcare professionals is higher compared to the general population but does not reach the desired levels. There are still many misconceptions among healthcare professionals regarding the effectiveness, safety, and accessibility of vaccines, as well as the severity of influenza |
| Prematunge et al. [34] | 2012 | Worldwide | Health professionals | Investigation of factors influencing healthcare professionals’ acceptance of influenza vaccination. | Systematic review of MEDLINE, PubMed, EMBASE, PsycINFO, CINAHL, AMED, Cochrane Library, ProQuest, and grey literature sources. Inclusion of 20 studies | Vaccination coverage shows a huge variation, spanning almost the entire percentage range. The main reasons contributing to acceptance are perceived effectiveness and safety, as well as a history of severe influenza illness |
| Seale & Macintyre [35] | 2011 | Australia | Health professionals | Investigation of influenza vaccination coverage among healthcare professionals within the Australian healthcare system | Review of MEDLINE and EMBASE. Inclusion of 10 studies | Vaccination coverage among healthcare professionals ranges approximately from 15% to 60% and does not reach the desired levels. Coverage is higher in facilities where health promotion interventions for influenza vaccination were implemented. These programs shape healthcare professionals’ beliefs, attitudes, and behaviors |
| Sheldenkar et al. [36] | 2019 | Asia | Health professionals | Investigation of influenza vaccination coverage among healthcare professionals in Asia and the determinants influencing it | Systematic review of PubMed and LISTA EBSCO. Inclusion of 83 studies, of which 32 referred to healthcare professionals | Vaccination coverage among healthcare professionals is the highest recorded in the Asian population, approaching 40%. The main factor contributing to acceptance is perceived effectiveness, while the primary barrier is perceptions regarding vaccine safety |
| Silva et al. [37] | 2023 | Worldwide | Health professionals | Application of the Health Belief Model to interpret influenza vaccination coverage among healthcare professionals | Review of PubMed. Inclusion of 11 studies | The dimensions of the Health Belief Model that appear to be related to healthcare professionals’ vaccination behavior are perceived susceptibility, perceived severity of the disease, perceived benefits, and perceived barriers |
| Sydnor & Perl [38] | 2014 | Worldwide | Health professionals | Highlighting the significance of healthcare professionals’ attitudes and behaviors regarding vaccination | Review of 62 studies in PubMed and EMBASE | Influenza vaccination coverage among healthcare professionals is low. Some of the barriers leading to non-acceptance of vaccination include the perception that influenza is not a serious illness, concerns about vaccine effectiveness and safety, and a lack of awareness about vaccination recommendations |
| To et al. [39] | 2016 | Worldwide | Health professionals | Highlighting influenza vaccination coverage among healthcare professionals and the factors that determine it | Review of 74 studies in PubMed | Vaccination coverage varies significantly by region as well as across different facilities within the same region. Although the benefits of vaccination are evident, coverage is low where it is not mandatory. The main factors hindering healthcare professionals’ vaccination appear to be perceptions regarding the benefits, risks, and effectiveness of vaccines |
| Waszkiewicz et al. [40] | 2025 | Worldwide | Pharmacists | Pharmacists’ knowledge, attitudes, and beliefs regarding influenza and pneumococcal vaccinations | Review of Medeline, Embase and Cochrane library. Inclusion of 24 studies | Pharmacists have unsatisfactory knowledge about influenza and pneumococcal vaccinations. Shortcomings in attitudes and beliefs about vaccination safety were also present, along with deficiencies of promotion of vaccinations. |
| Beliefs and attitudes associated with increased vaccine acceptance | Beliefs and attitudes associated with vaccine hesitancy |
|---|---|
| Protection of self and family | Lack of safety and side effects |
| Effectiveness in preventing transmission | Ineffectiveness and unnecessity |
| Safety of administration | No risk of severe illness |
| Fear of severe illness | Not a priority in daily schedules |
| Role model for general population | Vaccines are not easily accessible |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



