
Submitted:
09 February 2026
Posted:
10 February 2026
You are already at the latest version
Abstract
Background: Food bank users experience food insecurity, which is a social determinant of health associated with poorer physical and mental outcomes. However, there is little evidence in Spain regarding the health-related quality of life (HRQoL) of food bank users. Objectives: To assess the HRQoL of users of the Navarra Food Bank (BAN) by identifying the associated factors and comparing it with the general population. Methods: Cross-sectional study of heads of families using the BAN. Simple random sample of 350 from a population of 2,749 families (p and q 0.5). We evaluated HRQoL using the EQ-5D-5L scale via telephone survey. We analyzed scores on the utility index (EQ-5D-5L Index) and the visual analog scale (VAS), as well as the distribution of problems related to mobility, personal care, daily activities, pain/discomfort, and anxiety/depression. To enhance interpretability and avoid the influence of arbitrary thresholds or extreme values, the VAS and EQ-5D-5L Index variables were dichotomized into higher and lower health-related quality of life (HRQoL) groups using a data-driven K-means cluster analysis. Subsequently, binary logistic regression was applied to identify factors associated with the higher HRQoL group, with age, sex, socioeconomic variables, and EQ-5D-5L dimensions included as independent variables. Odds ratios with 95% CI were calculated. Results: The VAS was 73.56 (71.62-75.50) compared to 88.1 in Navarra. The prevalence of problems with mobility, self-care, daily activities, pain/discomfort, and anxiety/depression was higher in all cases than in Navarra: 25.5% vs. 13.0%; 8.7% vs. 5.3%; 19.7% vs. 8.0%; 55.7% vs. 35.7%; and 62.9% vs. 17.3% (all p < 0.001). Sociodemographic variables (age, sex, education, and employment) showed no significant association with HRQoL clusters (p > 0.05). Conversely, controlling for age and sex, belonging to the group with the highest VAS was associated with a lower prevalence of problems: Mobility OR= 3.91 (95% CI: 1.84-8.30); Daily Activities OR= 2.98 (95% CI: 1.16-7.65); Pain/Discomfort OR=3.36 (95% CI: 1.64-6.89); and Anxiety/Depression OR= 2.84 (95% CI: 1.41-5.73). Belonging to the group with the highest EQ-5D-5L Index was not significantly associated with Anxiety/Depression (OR = 1.62; 95% CI: 0.73–3.56), whereas the remaining dimensions showed similar significant associations. Conclusions: Users of the Navarra Food Bank have a significantly worse HRQoL than the general population, primarily associated with a high prevalence of mental health challenges and pain. These findings highlight that food banks are critical touchpoints for the early detection of health vulnerabilities, necessitating a shift from purely nutritional aid toward integrated social and health support models.
Keywords:
health-related quality of life
; food insecurity
; EuroQol EQ-5D-5L
; food banks
; community epidemiology
1. Introduction
Food banks (FB) are non-profit organizations that fulfill a dual essential function. On the one hand, they help alleviate hunger and poverty among vulnerable people, providing a direct response to rising food insecurity (FI) in low-income households, a phenomenon observed even in high-income countries. Systematic reviews conclude that food banks provide an important, immediate response to severe food deprivation and can improve food security and diet quality among users, even though they rarely eliminate food insecurity.[1,2,3,4,5,6]. On the other hand, by rescuing and redistributing surplus food that would otherwise be wasted, FBs play an important role in reducing food waste and, consequently, mitigating the environmental impact associated with its disposal. Diverting surplus food from landfills reduces greenhouse gas emissions because decomposing food waste is a major source of methane, a potent greenhouse gas. Impact assessments estimate that the food recovered and redistributed by food banks each year prevents millions of metric tons of carbon dioxide-equivalent emissions, highlighting their environmental role alongside their social mission [7,8,9].
The first food bank in the United States was established in Phoenix, Arizona, in 1967. [10,11,12,13], and subsequently this model spread to numerous countries worldwide [14,15]. At the European level, the European Federation of Food Banks (FEBA) brings together more than 300 food banks in approximately 30 countries [15].
In Spain, food banks are present in all autonomous communities and are coordinated by the Spanish Federation of Food Banks (FESBAL), which oversees 54 food banks. In 2024, these organizations distributed a total of 115,556 tons of food, benefiting 1,036,890 people [16]. Access to food banks is through referral by social services, following an assessment that confirms the socioeconomic need of the beneficiaries [17,18,19].
The association between poverty and poorer health is well-documented in the scientific literature.[20,21,22,23,24] In this context, food insecurity (FI) has been consistently identified as a social determinant of health with particularly adverse consequences. Available evidence shows that FI is associated with a wide range of health problems, including poorer self-perceived health and a higher prevalence of asthma in children [25], an increased risk of mental disorders [26,27,28,29,30,31] a higher incidence of falls in older people [32], poorer control and management of chronic physical illnesses such as diabetes [33,34,35], and even a higher risk of premature mortality [36].
Likewise, the literature has documented that FI is associated with greater consumption of health resources [37,38], both in children [39] and adults [40]. In addition, a relationship has been observed between FI and poorer quality of health care, especially in children who experience concomitant situations of residential instability and food insecurity [41].
In recent decades, various instruments have been developed to assess people’s subjective perception of their health-related quality of life (HRQoL). Among the most widely used generic instruments are the SF-36 [42], the WHOQOL-BREF [43], the SF-6D [44], and the EQ-5D-5L scale [45], which allow for the assessment of broad dimensions of health status, such as physical and psychological health, social relationships, and the environment.
Although some generic instruments have enabled quantification of the multidimensional impact of food insecurity on well-being and health-related quality of life (HRQoL), the available evidence remains limited and is largely confined to studies conducted in the United States and Canada. Pioneering work in the U.S. adult population (≥18 years) has consistently shown a strong association between FI and poorer HRQoL. In this context, a study. measured HRQoL among people >18 years of age in the U.S. using various instruments and concluded that FI is strongly associated with poorer HRQoL, and that differences between food-secure and food-insecure individuals were best detected using the SF-6D, EQ-5D, and PROPr [46].
In Canada, several studies have shown that people who are food insecure or use food banks have a poorer health-related quality of life, particularly in the mental component. Longitudinal studies of food bank users have observed mental health scores well below the population average [47,48]. This association has subsequently been confirmed in other geographical contexts, including low- and middle-income countries [49].
Theoretical frameworks suggest that food insecurity impacts mental health through both nutritional and non-nutritional pathways [50,51,52,53,54]. Beyond dietary deficiencies, the constant psychological pressure of managing a precarious budget and the social stigma of relying on charity create a state of chronic stress. This ‘stress of financial instability’ triggers physiological and emotional responses that specifically manifest as high rates of anxiety and depression, as the persistent uncertainty of basic needs fulfillment depletes cognitive and emotional resources [25,55,56,57,58,59,60,61,62,63,64,65].
Furthermore, it has been found that food insecurity is associated with a higher prevalence of chronic diseases throughout all stages of life [66,67,68,69]. This impact is particularly pronounced in older women living in poverty [70]. In addition, food insecurity has been linked to less healthy eating patterns, such as higher consumption of ultra-processed foods among adolescents [71,72,73].
The EQ-5D-5L scale is a widely used instrument for assessing HRQoL and is available in more than 170 languages [74]. It has been validated in the Spanish population [75,76] and has been used to assess HRQoL in the 2011–2012 Spanish National Health Survey [77].
In Europe, specifically in Portugal, the EQ-5D-3L scale was used in a population-based study, which observed lower health-related quality of life (HRQoL) in food-insecure households [78]. In the Netherlands, a study analyzed the diet of food bank users and identified high nutritional vulnerability; however, HRQoL was not assessed [79]. In general, the scientific literature on food bank users has focused predominantly on intake and nutritional status, rather than on assessing HRQoL using standardized instruments such as the EuroQol scales.
In Spain, using the Spanish value set of the EQ-5D-5L scale, several studies have identified significant inequalities in HRQoL associated with sociodemographic and health factors, such as age, sex, educational level, social class, body mass index, and the presence of chronic diseases [80].
At the regional level, the EQ-5D-5L scale was used in the 2012 Navarra Situation Diagnosis [81], and the visual analog scale (VAS) of the EQ-5D-5L scale has been incorporated into the Navarra Social and Living Conditions Survey, conducted in 2017, 2021, and 2024 [82].
The selection of Navarra as the study site is particularly relevant due to its distinct socioeconomic landscape and specialized social policy framework, including its unique regional welfare system. Analyzing this region allows for a critical evaluation of how food insecurity persists and impacts health-related quality of life, even in a territory with historically high social protection standards, providing timely evidence on the limitations of current safety nets compared with those in other Spanish autonomous communities.
Despite solid international evidence linking food insecurity to poorer health outcomes and lower HRQoL, there remains a notable lack of studies evaluating these indicators among populations served by food banks in Spain, as well as among people experiencing food insecurity in the Spanish context.
This study offers a triple scientific contribution to the field of food insecurity and public health. Contextually, it provides unprecedented evidence from Spain, filling a critical research gap in Southern Europe where the impact of food insecurity on HRQoL remains understudied despite distinct social protection frameworks. Methodologically, the research moves beyond simple descriptive comparisons by employing Directed Acyclic Graphs (DAGs) to ensure a rigorous, theoretically grounded adjustment for confounding, and utilizing K-means clustering to identify data-driven health profiles that avoid the limitations of arbitrary statistical cut-offs. These rigorous analytical approaches align with contemporary data quality frameworks that emphasize the necessity of robust governance and transparency throughout the data lifecycle to ensure scientific integrity and accountability [83]. Conceptually, this work reframes food banks as more than emergency food distribution sites, proposing them as strategic public health settings for the early identification of mental and physical vulnerability.
In this context, the main objective of this study is to assess the HRQoL of users of the Food Bank of Navarra, a region in northern Spain, to analyze the associated sociodemographic factors, and to compare the results with those of the general population..
2. Materials and Methods
2.1. Study Design and Participants
A cross-sectional study was conducted based on a telephone survey of family heads who were users of the Navarra Food Bank, previously assessed by Social Services and certified as lacking financial resources. The surveys were conducted between November 2024 and February 2025.
2.2. Sampling
Head of the household (household reference person), defined as the primary adult responsible for the household, including fathers or mothers in two-parent households, single parents, and individuals living alone., a sample size of 338 people was calculated to estimate a population proportion, assuming a margin of error of 5%, a confidence level of 95%, and the most unfavorable situation (p = 0.5; q = 0.5).
The selection was made by simple random sampling from the list of Food Bank beneficiaries. Initially, a sample of 398 people was extracted, who were contacted by telephone in the morning or afternoon. Of these, we couldn’t reach 40 people, and 358 people were contacted, of whom 8 refused to participate, so in the end 350 surveys were conducted. Of the 350 participants, 4 did not answer the EQ-5D-5L. That is, there are 346 complete surveys and 4 incomplete ones. (Figure 1)
2.3. Measuring Instrument.
HRQoL was assessed using the EQ-5D-5L scale, in its Spanish-validated version. The questionnaire explores five dimensions: mobility, self-care, daily activities, pain/discomfort, and anxiety/depression.
The EQ-5D-5L visual analog scale (VAS) was also included, in which participants rated their current health status on a scale of 0 to 100, where 0 represents the worst possible health status and 100 represents the best.
The questionnaire also collected sociodemographic variables: age, gender, country of origin (Spanish/foreign), educational level, employment status, and degree of coverage of basic needs (food, housing, employment, clothing, heating supplies, and children’s education), assessed using a three-category Likert ordinal scale: “I have no problems,” “I have some problems,” and “I have many problems.”
2.4. Data Collection Procedure.
Prior to the start of the fieldwork, 30 pilot interviews were conducted to standardize interview and assessment criteria. The interviews were conducted by telephone and in Spanish. When the interviewee was from Morocco and didn’t understand Spanish, the interview was conducted using the validated Morocco’s Arabic version of the ED by two bilingual Arabic-speaking students, who were responsible for interviewing the Arabic-speaking population [84]. The interviews were conducted by telephone in Spanish or Arabic using a standardized protocol. To ensure transparency and participant understanding, a formal script was followed to obtain verbal informed consent (the English translation of this script is provided in Supplementary File S2). The entire team received specific training in interview techniques and in the administration of the EQ-5D-5L scale, with special emphasis on the correct application of the VAS.
This focus on training and the use of standardized protocols represents a critical step in data quality assurance, which is fundamental for maintaining scientific integrity and ensuring the reproducibility of results in healthcare research [83]. Embedding such governance mechanisms during the data collection phase is essential for producing trustworthy data that can reliably support evidence-based public health decisions.
2.5. Statistical Analysis.
Categorical variables were described using frequencies and percentages, and comparisons of proportions were made using the chi-square test, calculating 95% confidence intervals. Numerical variables were described using descriptive statistics and compared using Student’s t-test or nonparametric tests (Mann–Whitney U or Kruskal–Wallis), depending on the distribution of the data. The level of statistical significance was set at p < 0.05.
For the EQ-5D-5L scale, the prevalence of people reporting a problem in each of its five dimensions was estimated. VAS scores were also analyzed, and the EQ-5D-5L Index was calculated using the preference set of the Spanish population, which allows a numerical value to be assigned to self-perceived health status.
We developed two directed acyclic graphs (DAGs) to define the covariate adjustment strategy for multivariable analyses. Separate DAGs were specified because health-related quality of life (HRQoL) was operationalized using two different outcomes—the EQ-5D-5L index value and the EQ visual analogue scale (EQ-VAS)—which capture complementary but not identical constructs (a preference-based health utility derived from the descriptive system vs a global self-rated health score). For each outcome, the corresponding DAG was used to identify a minimally sufficient adjustment set to control for confounding and to avoid inappropriate adjustment for variables on the causal pathway.
Figure 2.
Directed Acyclic Graphs (DAGs) representing the causal framework for health-related quality of life (HRQoL) determinants among food bank users. (a) DAG for the Visual Analogue Scale (VAS) outcome; (b) DAG for the EQ-5D-5L Index outcome. In both models, the degree of coverage of basic needs is defined as the main exposure. The arrows illustrate the hypothesized causal pathways between sociodemographic factors (Age, Sex, Origin, Education), socioeconomic status (Employment), and HRQoL outcomes . Based on these DAGs, a minimally sufficient adjustment set—including age, sex,—was identified to control for potential confounding.
Figure 2.
Directed Acyclic Graphs (DAGs) representing the causal framework for health-related quality of life (HRQoL) determinants among food bank users. (a) DAG for the Visual Analogue Scale (VAS) outcome; (b) DAG for the EQ-5D-5L Index outcome. In both models, the degree of coverage of basic needs is defined as the main exposure. The arrows illustrate the hypothesized causal pathways between sociodemographic factors (Age, Sex, Origin, Education), socioeconomic status (Employment), and HRQoL outcomes . Based on these DAGs, a minimally sufficient adjustment set—including age, sex,—was identified to control for potential confounding.
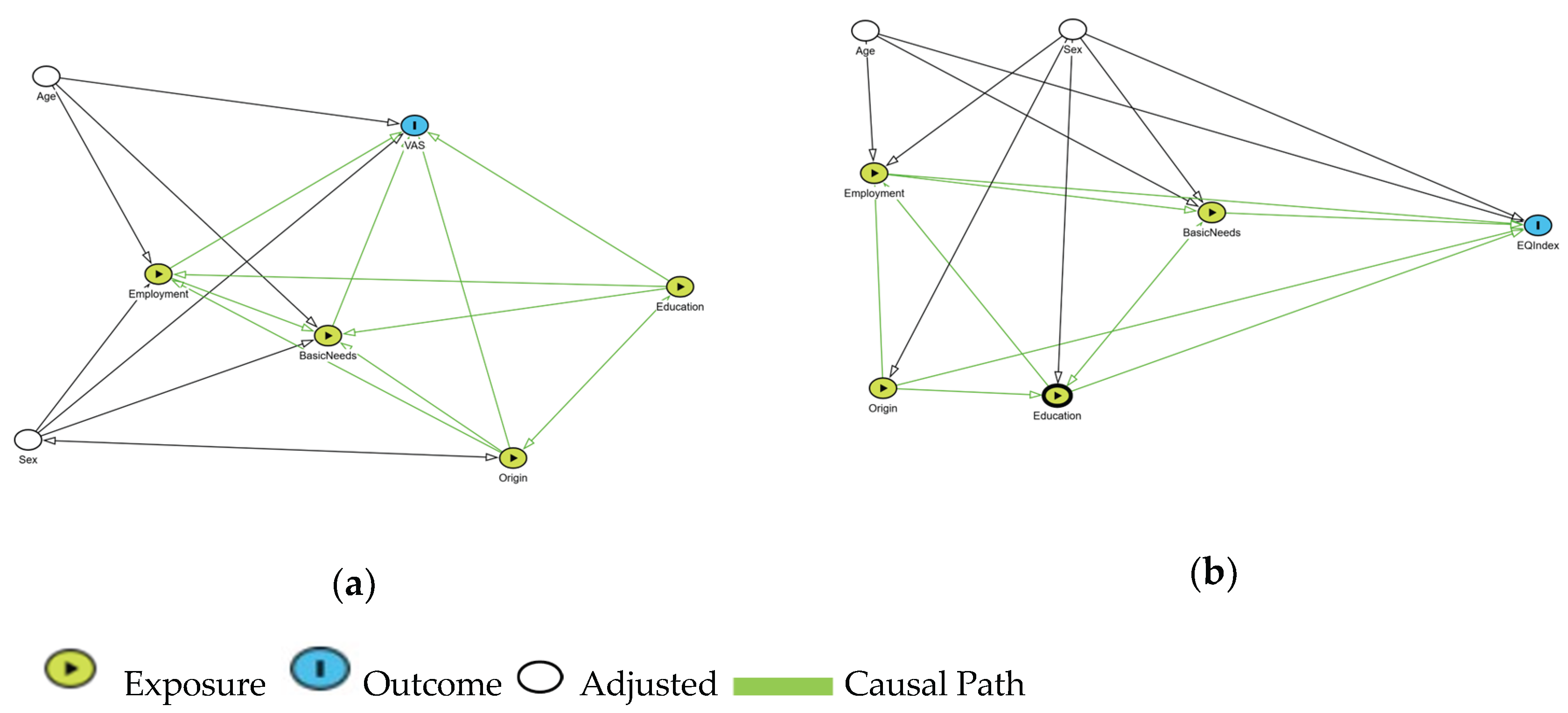
Separate DAGs were specified because health-related quality of life (HRQoL) was operationalized using two different outcomes—the EQ-5D-5L index value and the EQ visual analogue scale (EQ-VAS)—which capture complementary but not identical constructs (Figures S1 and S2). To ensure transparency and reproducibility, the complete DAGitty source code for both models is provided in File S1 of the Supplementary Material.
The structural logic and the identification of the minimally sufficient adjustment set for both multivariable models were founded on directed acyclic graphs (DAGs). Separate DAGs were specified for each outcome—the EQ-5D-5L index value and the EQ visual analogue scale (EQ-VAS)—as they capture complementary but distinct constructs of health-related quality of life (HRQoL). Both causal models share an identical adjustment structure because the underlying theoretical relationships between the exposure (coverage of basic needs, origin, education, and employment) and the sociodemographic confounders remain constant, regardless of the metric used to measure the outcome. Consequently, a single minimally sufficient adjustment set—comprising age, sex—was identified to control for confounding and avoid inappropriate adjustment for variables on the causal pathway. To ensure transparency and reproducibility, the complete DAGitty source code for both models is available in File S1 of the Supplementary Material.
To classify the health-related quality of life (HRQoL) status of the participants, a non-hierarchical K-means cluster analysis (k = 2) was performed based on the Visual Analogue Scale (VAS) and EQ-5D-5L Index scores. This data-driven approach was selected to minimize intragroup variability and maximize extragroup differences, identifying naturally occurring health profiles while avoiding the bias often associated with arbitrary distribution-based cut-offs, such as medians or quartiles [85].
The analytical strategy was structured to distinguish between causal drivers and functional descriptors. While the degree of coverage of basic needs was defined as the primary exposure within the causal framework of the Directed Acyclic Graphs (DAGs) , binary logistic regression models were subsequently used to identify the clinical and functional factors associated with belonging to the higher HRQoL cluster. In these multivariable models, the EQ-5D-5L dimensions were analyzed as the main independent variables to characterize the specific health problems defining each cluster, while the degree of coverage of basic needs and other sociodemographic factors were included as covariates to adjust for confounding and assess their relative predictive weight. Results were expressed as odds ratios (OR) with 95% confidence intervals. Second, to identify the clinical and functional drivers of the observed health states, binary logistic regression models were constructed using HRQoL clusters (higher vs. lower) as the dependent variable. In these models, the EQ-5D-5L dimensions were utilized as the primary independent variables to quantify the weight of specific health problems in predicting cluster membership. Socioeconomic variables, including the degree of coverage of basic needs, were included as covariates to assess their relative contribution alongside functional limitations.
In addition, a Severity Index (SI 0–100), also known as the Sum Score, was constructed based on the levels reported in the five dimensions of the EQ-5D-5L scale. To calculate it, the values of the five dimensions (theoretical range: 5–25) were added together and a linear transformation was applied by subtracting 5 from this sum and multiplying the result by 5, thus obtaining an index with a range from 0 to 100, where 0 represents the total absence of health problems and 100 represents the highest possible degree of severity
The SI was used as a descriptive measure of health status severity, complementary to the EQ-5D-5L Index based on population preferences.
The Severity Index (SI) was described using descriptive statistics and was used as a continuous variable in comparative analyses.
Finally, a descriptive comparison of the results was made with the available data on the general population from the 2011–2012 Spanish National Health Survey, the 2012 Diagnosis of the Situation in Navarra, and the 2024 Social and Living Conditions Survey in Navarra.
DAGs were created and visualized using the free web-based software DAGitty version 3.1[86]. (https://dagitty.net/) Statistical analyses were performed using IBM SPSS Statistics software, version 22.
2.6. Ethical Considerations.
The study was approved by the Ethics, Animal Experimentation, and Biosafety Committee of the Public University of Navarra (UPNA) under code PI-021/24 on October 28, 2024. Informed consent was obtained from all subjects involved in the study. The procedure included a detailed explanation of data protection rights and the voluntary nature of participation, as documented in the verbal consent script (Supplementary File S2).
3. Results
3.1. Participation and Sample
The sample analyzed consisted of 350 users of the Navarra Food Bank, of whom 70.0% were women. The average age was 45.5 years (SD: 12.3), with no statistically significant differences between men and women (Table 1) (Table S1)
Most of the people surveyed were in the 30–44 and 45–59 age groups. In terms of educational level and employment status, basic educational levels and unemployment or precarious employment predominated. Table 2 provides a detailed overview of the main sociodemographic and socioeconomic characteristics of the population studied. Overall, the sample represents an adult population in a situation of socioeconomic vulnerability, with a high burden of family responsibilities and unstable working conditions, consistent with the profile of food bank users.
3.2. EQ-5D-5L Results (Dimensions)
The dimension with the highest prevalence of problems was anxiety/depression, followed by pain/discomfort. More than half of the respondents reported some degree of impairment in both dimensions. In contrast, the prevalence of problems in mobility, self-care, and daily activities was significantly lower. In all dimensions of the EQ-5D-5L, the prevalence of problems was higher than that observed in the general population of Navarra in 2024[82], with particularly marked differences in anxiety/depression and pain/discomfort (Table 3).
3.3. VAS and EQ-5D-5L Index: Consistency and Comparison
The mean Visual Analogue Scale (VAS) score was 73.56 points, with slightly higher values in men than in women. A clear age gradient was observed, with higher scores in younger groups and a progressive decline from the age of 45 onwards.
In all the subgroups analyzed, VAS scores were lower than those observed in the general population of Navarra in 2024 (Table 4).
Similarly, the EQ-5D-5L utility index showed lower values than those described in the general population, with worse results in women and older age groups (Table 5).
3.4. Logistic Regression Models
In order to identify different HRQOL profiles, a cluster analysis was performed using the k-means method, using the VAS and EQ-5D-5L index scores. A two-cluster solution was chosen for reasons of parsimony and interpretability, allowing a clear differentiation between a group with higher HRQOL and another with lower HRQOL, while also avoiding the influence of extreme values that could result from classifications based on quartiles or other arbitrary cut-off points. Table 6 shows the descriptive statistics for both variables for each group.
In the logistic regression models, the sociodemographic and socioeconomic variables explored did not show statistically significant associations with belonging to the group with higher HRQOL. On the contrary, the absence of problems in the EQ-5D-5L dimensions, especially mobility, daily activities, pain/discomfort, and anxiety/depression, was consistently associated with a higher probability of belonging to the group with the best HRQOL (Table 7).
Following the structural logic of the DAGs, age and sex were identified as the minimally sufficient adjustment set to block confounding without introducing overadjustment or social-pathway bias. However, recognizing these results within the framework of social determinants of health, variables such as nationality (78.9% foreign-born) and education level (62% primary/secondary) remain essential for contextualizing the ‘upstream’ vulnerability of this population, even if they were not included in the formal adjustment set to maintain the statistical parsimony of the causal model.
4. Discussion
This study shows that users of the Navarra Food Bank have a significantly lower health-related quality of life (HRQOL) than the general population, with a particularly marked impact on the dimensions of performing daily activities, anxiety/depression, and pain/discomfort.
A substantial part of health status is determined by non-medical factors, including educational level, access to adequate food, and decent housing and working conditions [20]. In this context, there is growing interest in understanding the role of food insecurity in health outcomes [20,21,22], as well as identifying which HRQOL measures best reflect the experience of people who suffer from it.
The EQ-5D-5L is a widely validated instrument that has enabled the identification of significant differences with respect to the general population. Although it was designed for face-to-face administration, its use over the telephone has been widely employed and validated in previous studies [87,88].
In fact, the EuroQol consortium currently has specific guidelines for the telephone administration of the EQ-5D, confirming its validity and reliability in this format. [89].
The values obtained on both the visual analog scale (VAS) and the utility index are worse than those observed in the general population and are consistent with those observed in international studies conducted in the United States [46] and Canada [24]. Our work provides unprecedented evidence in Spain and extends this knowledge to a southern European context, focusing specifically on food bank users. Similarly, the severity index reflects a poorer level of health in the surveyed population compared to the general population.
Our results show a significant impact on HRQOL associated with emotional distress, particularly in the anxiety/depression dimension, plausibly related to situations of life insecurity, chronic stress, and economic uncertainty. These findings are consistent with studies conducted in Spain [90]., which described an increase in diagnoses of depression and anxiety disorders in the most socioeconomically disadvantaged groups following the 2008 economic crisis [90]. Similarly, a recent systematic review conducted in 24 countries confirms the association between economic hardship and mental health deterioration [91].
Overall, our data show that emotional distress is more prevalent than severe physical impairment, consistent with the framework of social determinants of health. This suggests that structural factors that induce food insecurity significantly influence the likelihood of experiencing emotional distress, as observed in previous studies. [59].
Multivariate models indicate that age and gender are not the main determinants of poorer HRQOL, but rather functional limitations and emotional distress. While these findings suggest that functional and emotional domains carry more explanatory weight in our analysis, they must be interpreted with caution. The study sample consists of individuals already identified by social services as lacking financial resources, leading to high socioeconomic homogeneity. Consequently, the lack of significant associations for variables like education or employment status likely reflects a ‘floor effect’ due to limited variability within this highly vulnerable group. It is essential to recognize that socioeconomic position is an ‘upstream’ determinant that precedes both food bank use and health status; therefore, the observed health challenges—such as chronic pain and anxiety—are likely manifestations of the underlying poverty that characterizes the entire cohort. These results are consistent with previous evidence indicating that psychological well-being and limitations in daily activities often carry the greatest explanatory weight in HRQoL models once a state of vulnerability is established [92,93].
The application of non-hierarchical K-means cluster analysis to dichotomize HRQoL outcomes offers significant epidemiological advantages over predefined clinical or distribution-based cut-offs, such as medians or quartiles. This method creates groups by minimizing intragroup variability and maximizing extragroup variability [85], ensuring that the resulting categories represent naturally occurring health profiles within the specific population of food bank users. Furthermore, this approach is more robust for epidemiological research as it corrects the drawbacks of straightforward partitioning methods, which often include individuals with outliers that can produce significant bias in multivariate models [85]. By using a data-driven classification rather than arbitrary thresholds, we reduce misclassification bias and enhance the accuracy of the associations identified, ensuring that the findings reflect the unique socioeconomic and health reality of this vulnerable collective.
In our multivariable models, the absence of significant associations for socioeconomic variables, such as education or employment status, may reflect the limited variability within this highly vulnerable sample, where socioeconomic hardship is a common denominator. Consequently, this approach reduces misclassification bias and strengthens the robustness of the associations identified in our multivariate models. It is acknowledged that a degree of circularity exists in these models, as the EQ-5D dimensions are used to predict clusters derived from the same instrument; however, this serves to confirm the internal consistency of the functional health profiles identified and allows us to quantify which specific health domains contribute most to the perceived HRQoL deficit in this population. Nevertheless, alternative explanations, including potential overadjustment or unmeasured clustering effects, should be considered when interpreting these specific results.
These findings have important implications for public policy: food banks should not be conceived solely as a nutritional response, but also as key spaces for the early detection of health vulnerability, especially in the field of mental health, and for the articulation of social and health coordination strategies.
Among the strengths of the study are an adequate sample size, the use of a validated instrument such as the EQ-5D-5L, and the inclusion of the Arabic-speaking population, which is usually underrepresented in this type of research.
However, the study has limitations inherent to its cross-sectional design, which precludes establishing causal relationships between receiving food aid and HRQoL—a distinction noted in previous longitudinal studies [94]. Beyond this design-related constraint, the timing of data collection (November to February) warrants careful consideration. This period coincides with winter in northern Spain, which may exacerbate self-reported pain and discomfort due to colder temperatures [55,95,96,97]. Additionally, the financial and social pressures associated with the end-of-year holiday season may have temporarily inflated the prevalence of anxiety and depression among these vulnerable households, who often struggle to meet the social expectations and expenses of this period [98,99,100]. A potential selection bias must also be acknowledged [101,102]. This study focused exclusively on users of the Navarra Food Bank, all of whom have undergone social service assessment. Consequently, this population may not be representative of all food-insecure individuals in Spain, as it excludes those who do not access food banks due to stigma, lack of information, or restrictive eligibility criteria. These ‘non-users’ might present different health profiles, and their exclusion limits the generalizability of our findings.
Moreover, as the study relies exclusively on self-perceived health, the results may be subject to subjective bias [103,104,105,106]. Lastly, the absence of a matched comparison with the general population limits the ability to accurately quantify the health gap attributable to food insecurity. Future research should aim to compare food bank beneficiaries with food-insecure non-users to better isolate the effects of aid programs on HRQoL.
Furthermore, the descriptive nature of the comparison with the general population of Navarra is a limitation. As these data were not age- or sex-standardized, the observed health gap may be partially influenced by the demographic specificities of the food bank user population. While the magnitude of the differences in dimensions like anxiety/depression remains striking, future studies should employ direct standardization or matched-pair designs to provide a more refined quantification of the health inequality attributable exclusively to food insecurity.
Future research should adopt longitudinal designs that allow for rigorous control of key socioeconomic variables, such as income level, housing stability, and social support. Cohort studies would facilitate the analysis of HRQOL evolution following Food Bank intervention, overcoming the cross-sectional nature of the present study and providing more robust evidence on the impact of these interventions on physical and emotional well-being.
In conclusion, our results show a clear gap in HRQOL between the vulnerable population served by food banks and the general population, reinforcing the urgent need to integrate mental and social health into policies aimed at combating food poverty.
5. Conclusions
This study provides novel evidence of a profound health-related quality of life (HRQoL) gap between food bank users and the general population in Spain. Our findings reveal that vulnerable populations served by food banks experience significantly lower self-perceived health, with the most severe impact observed in the dimensions of anxiety/depression and pain/discomfort. Because these disparities are primarily linked to functional and emotional distress rather than just demographic factors like age or sex, food insecurity must be addressed as a multidimensional determinant of health.
Methodologically, this research provides a significant contribution by utilizing the EQ-5D-5L scale—a robust, validated instrument—within a framework informed by Directed Acyclic Graphs (DAGs). This approach ensures a theoretically grounded adjustment for confounding variables, enhancing the reliability of the observed associations in a population that remains underrepresented in Southern European public health literature.
In conclusion, the empirical evidence from this study demonstrates a significant HRQoL gap and high prevalence of mental health distress among food bank users compared to the general population. Based on these objective findings, we propose the following normative recommendations: food banks should be strategically re-envisioned as frontline settings for early health vulnerability detection rather than remaining limited to nutritional support. To bridge the identified health inequalities, it is recommended that policymakers prioritize the integration of psychosocial support and formal referral pathways to primary care within the existing food assistance framework.
While the cross-sectional nature of this study precludes the establishment of definitive causal links, the strength of the identified associations underscores the urgent need for longitudinal research to further explore the pathways between food aid interventions and long-term health outcomes.
The primary implication of this research is that food banks should be re-envisioned as strategic frontline settings for early health intervention rather than just nutritional responses. To effectively reduce HRQoL inequalities, it is essential to integrate psychosocial support and formal referral pathways to primary care within the food bank framework. Moving forward, public health policies must prioritize these integrated social-health strategies to move beyond emergency food relief and toward the holistic well-being of food-insecure populations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Directed acyclic graph (DAG) for the association between coverage of basic needs and EQ-VAS; Figure S2: Directed acyclic graph (DAG) for the association between coverage of basic needs and EQ-5D-5L Index; File S1: DAGitty source code for causal models (A) and (B).
Author Contributions
Conceptualization, ABL, FGG and IAO; methodology, ABL, FGG and IAO; software, LGA and FGG; validation, AEV and CHV; formal analysis, ABL, LGA, FGG and IAO; investigation, AEV, CHV and LGA; data curation, ABL, LGA, FGG and IAO; writing—original draft preparation, ABL, LGA, FGG and IAO; writing—review and editing, ABL, AEV, CHV, LGA, FGG and IAO; visualization, LGA; supervision, ABL and IAO; project administration, ABL. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. and approved by the Ethics, Animal Experimentation, and Biosafety Committee of the Public University of Navarra (UPNA) under code PI-021/24 on October 28, 2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The anonymized dataset used in this study is available from the first author upon reasonable request.
Acknowledgments
During the preparation of this manuscript/study. the authors used Grammarly for the purposes of correcting the grammar and improving the flow. The authors have reviewed and edited the output and take full responsibility for the content of this publication.”.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| FB | Food Banks |
| FI | Food Insecurity |
| HRQoL | Health-Related Quality of Life |
References
- Taylor, N.; Boyland, E.; Hardman, C. A. Conceptualising Food Banking in the UK from Drivers of Use to Impacts on Health and Wellbeing: A Systematic Review and Directed Content Analysis. Appetite 2024, 203, 107699. [Google Scholar] [CrossRef] [PubMed]
- Gentilini, U. Banking on Food: The State of Food Banks in High-Income Countries - Institute of Development Studies (Working Paper;415); Brighton, 2013. [Google Scholar]
- Oldroyd, L.; Eskandari, F.; Pratt, C.; Lake, A. A. The Nutritional Quality of Food Parcels Provided by Food Banks and the Effectiveness of Food Banks at Reducing Food Insecurity in Developed Countries: A Mixed-method Systematic Review. Journal of Human Nutrition and Dietetics 2022, 35(6), 1202–1229. [Google Scholar] [CrossRef]
- Mook, L.; Murdock, A.; Gundersen, C. Food Banking and Food Insecurity in High-Income Countries. Voluntas 2020, 31(5), 833–840. [Google Scholar] [CrossRef]
- Bazerghi, C.; McKay, F. H.; Dunn, M. The Role of Food Banks in Addressing Food Insecurity: A Systematic Review. J. Community Health 2016, 41(4), 732–740. [Google Scholar] [CrossRef] [PubMed]
- Byrne, A. T.; Just, D. R. Review: Private Food Assistance in High Income Countries: A Guide for Practitioners, Policymakers, and Researchers. Food Policy 2022, 111, 102300. [Google Scholar] [CrossRef]
- Suaréz Peña, A. C. Food Banks: An Unsung Hero of Climate Action | The Global FoodBanking Network. Available online: https://www.foodbanking.org/blogs/food-banks-an-unsung-hero-of-climate-action/ (accessed on 10 January 2026).
- Garza, F. How Food Banks Prevented 1.8 Million Metric Tons of Carbon Emissions Last Year - Center For Health Law and Policy Innovation; 2024. [Google Scholar]
- Penalver, J. G.; Armijos, A.; Soret, B.; Aldaya, M. M. Food Banks against Climate Change, a Solution That Works: A Case Study in Navarra, Spain. Foods 2022, 11(22), 3645. [Google Scholar] [CrossRef]
- Sharififard, S. Community, Food Insecurity, and a Global Perspective on Campus Food Pantries; Springer Nature Switzerland: Cham, 2024. [Google Scholar] [CrossRef]
- Haynes Stein, A. Hunger in Crisis: Food Bank Practices and the Social Safety Net; University of California Davis, 2024. [Google Scholar]
- St. Mary’s Food Bank. About St. Mary’s Food Bank & Our Mission to End Hunger. Available online: https://www.stmarysfoodbank.org/about-us/ (accessed on 10 February 2026).
- Cotugna, N.; Beebe, P. D. Food Banking in the 21st Century: Much More than a Canned Handout. J. Am. Diet. Assoc. 2002, 102(10), 1386–1388. [Google Scholar] [CrossRef]
- Williams, A.; May, J. A Genealogy of the Food Bank: Historicising the Rise of Food Charity in the UK. Transactions of the Institute of British Geographers 2022, 47(3), 618–634. [Google Scholar] [CrossRef]
- The Global Food Banking Network. How Food Banks Promote Food Security | The Global FoodBanking Network. Available online: https://www.foodbanking.org/promoting-food-security/ (accessed on 10 February 2026).
- Federación Española de Bancos de Alimentos (FESBAL). Federación Española de Bancos de Alimentos. Available online: https://www.fesbal.org.es/ (accessed on 10 February 2026).
- Gómez Garrido, M.; Carbonero Gamundí, M. A.; Viladrich, A. The Role of Grassroots Food Banks in Building Political Solidarity with Vulnerable People. European Societies 2019, 21(5), 753–773. [Google Scholar] [CrossRef]
- de Armiño, K. Erosion of Rights, Uncritical Solidarity and Food Banks in Spain. In InFirst World Hunger Revisited: Food Charity or the Right to Food? Riches, G., Silvasti, T., Eds.; Palgrave Macmillan: London, 2014; pp. pp 131–145. [Google Scholar]
- González-Torre, P. L.; Coque, J. How Is a Food Bank Managed? Different Profiles in Spain. Agric. Human Values 2016, 33(1), 89–100. [Google Scholar] [CrossRef]
- WHO. Social determinants of health. Available online: https://www.who.int/news-room/fact-sheets/detail/social-determinants-of-health (accessed on 10 February 2026).
- Stuff, J. E.; Casey, P. H.; Szeto, K. L.; Gossett, J. M.; Robbins, J. M.; Simpson, P. M.; Connell, C.; Bogle, M. L. Household Food Insecurity Is Associated with Adult Health Status. J. Nutr. 2004, 134(9), 2330–2335. [Google Scholar] [CrossRef] [PubMed]
- Laurence, S.; Durand, E.; Thomas, E.; Chappuis, M.; Corty, J. F. Food Insecurity and Health Status in Deprived Populations, 2014: A Multicentre Survey in Seven of the Social and Medical Healthcare Centres (CASOs) Run by Doctors of the World, France. Public Health 2017, 143, 97–102. [Google Scholar] [CrossRef] [PubMed]
- van der Velde, L. A.; Steyerberg, E. W.; Numans, M. E.; Kiefte-de Jong, J. C. Food Insecurity Status Is of Added Value in Explaining Poor Health: A Cross-Sectional Study among Parents Living in Disadvantaged Neighbourhoods in the Netherlands. BMJ Open 2022, 12(2), e052827. [Google Scholar] [CrossRef]
- Kashem, T.; Al Sayah, F.; Tawiah, A.; Ohinmaa, A.; Johnson, J. A. The Relationship between Individual-Level Deprivation and Health-Related Quality of Life. Health Qual. Life Outcomes 2019, 17(1), 176. [Google Scholar] [CrossRef]
- Gundersen, C.; Ziliak, J. P. Food Insecurity And Health Outcomes. Health Aff. 2015, 34(11), 1830–1839. [Google Scholar] [CrossRef]
- Leung, C. W.; Epel, E. S.; Willett, W. C.; Rimm, E. B.; Laraia, B. A. Household Food Insecurity Is Positively Associated with Depression among Low-Income Supplemental Nutrition Assistance Program Participants and Income-Eligible Nonparticipants. J. Nutr. 2015, 145(3), 622–627. [Google Scholar] [CrossRef]
- Jessiman-Perreault, G.; McIntyre, L. The Household Food Insecurity Gradient and Potential Reductions in Adverse Population Mental Health Outcomes in Canadian Adults. SSM Popul. Health 2017, 3, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Men, F.; Elgar, F. J.; Tarasuk, V. Food Insecurity Is Associated with Mental Health Problems among Canadian Youth. J. Epidemiol. Community Health (1978). 2021, 75(8), 741–748. [Google Scholar] [CrossRef]
- Tarasuk, V.; Mitchell, A.; McLaren, L.; McIntyre, L. Chronic Physical and Mental Health Conditions among Adults May Increase Vulnerability to Household Food Insecurity. J. Nutr. 2013, 143(11), 1785–1793. [Google Scholar] [CrossRef]
- Pourmotabbed, A.; Moradi, S.; Babaei, A.; Ghavami, A.; Mohammadi, H.; Jalili, C.; Symonds, M. E.; Miraghajani, M. Food Insecurity and Mental Health: A Systematic Review and Meta-Analysis – CORRIGENDUM. Public Health Nutr. 2020, 23(10), 1854–1854. [Google Scholar] [CrossRef]
- Elgar, F. J.; Pickett, W.; Pförtner, T.-K.; Gariépy, G.; Gordon, D.; Georgiades, K.; Davison, C.; Hammami, N.; MacNeil, A. H.; Azevedo Da Silva, M.; Melgar-Quiñonez, H. R. Relative Food Insecurity, Mental Health and Wellbeing in 160 Countries. Soc. Sci. Med. 2021, 268, 113556. [Google Scholar] [CrossRef] [PubMed]
- Mosen, D. M.; Banegas, M. P.; Friedman, N.; Shuster, E.; Brooks, N. Food Insecurity Associated with Self-Reported Falls Among Medicare Advantage Members. Popul. Health Manag. 2019, 22(6), 536–539. [Google Scholar] [CrossRef]
- Seligman, H. K.; Davis, T. C.; Schillinger, D.; Wolf, M. S. Food Insecurity Is Associated with Hypoglycemia and Poor Diabetes Self-Management in a Low-Income Sample with Diabetes. J. Health Care Poor Underserved 2010, 21(4), 1227–1233. [Google Scholar] [CrossRef]
- Charkhchi, P.; Fazeli Dehkordy, S.; Carlos, R. C. Housing and Food Insecurity, Care Access, and Health Status Among the Chronically Ill: An Analysis of the Behavioral Risk Factor Surveillance System. J. Gen. Intern. Med. 2018, 33(5), 644–650. [Google Scholar] [CrossRef]
- Walker, R. J.; Egede, J. K.; Thorgerson, A.; Mosley-Johnson, E.; Campbell, J. A.; Egede, L. E. The Burden of Food Insecurity on Quality of Life in Adults with Diabetes. Nutrients 2024, 16(21), 3602. [Google Scholar] [CrossRef] [PubMed]
- Men, F.; Gundersen, C.; Urquia, M. L.; Tarasuk, V. Association between Household Food Insecurity and Mortality in Canada: A Population-Based Retrospective Cohort Study. Can. Med. Assoc. J. 2020, 192(3), E53–E60. [Google Scholar] [CrossRef] [PubMed]
- Tarasuk, V.; Cheng, J.; Gundersen, C.; de Oliveira, C.; Kurdyak, P. The Relation between Food Insecurity and Mental Health Care Service Utilization in Ontario. The Canadian Journal of Psychiatry 2018, 63(8), 557–569. [Google Scholar] [CrossRef]
- Men, F.; Gundersen, C.; Urquia, M. L.; Tarasuk, V. Food Insecurity Is Associated With Higher Health Care Use And Costs Among Canadian Adults. Health Aff. 2020, 39(8), 1377–1385. [Google Scholar] [CrossRef]
- Clemens, K. K.; Le, B.; Anderson, K. K.; Comeau, J.; Tarasuk, V.; Shariff, S. Z. The Association between Household Food Insecurity and Healthcare Costs among Canadian Children. Canadian Journal of Public Health 2024, 115(1), 89–98. [Google Scholar] [CrossRef]
- Tarasuk, V.; Cheng, J.; de Oliveira, C.; Dachner, N.; Gundersen, C.; Kurdyak, P. Association between Household Food Insecurity and Annual Health Care Costs. Can. Med. Assoc. J. 2015, 187(14), E429–E436. [Google Scholar] [CrossRef]
- Ma, C. T.; Gee, L.; Kushel, M. B. Associations Between Housing Instability and Food Insecurity With Health Care Access in Low-Income Children. Ambulatory Pediatrics 2008, 8(1), 50–57. [Google Scholar] [CrossRef] [PubMed]
- Ware, J. E.; Sherbourne, C. D. The MOS 36-Item Short-Form Health Survey (SF-36). I. Conceptual Framework and Item Selection. Med. Care 1992, 30(6), 473–483. [Google Scholar] [CrossRef]
- THE WHOQOL GROUP. Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol. Med. 1998, 28(3), 551–558. [Google Scholar] [CrossRef]
- Wang, L.; Poder, T. G. A Systematic Review of SF-6D Health State Valuation Studies. J. Med. Econ. 2023, 26(1), 584–593. [Google Scholar] [CrossRef]
- Roudijk, B.; Ludwig, K.; Devlin, N. EQ-5D-5L Value Set Summaries. In Value Sets for EQ-5D-5L; Springer International Publishing: Cham, 2022; pp. pp 55–212. [Google Scholar] [CrossRef]
- Hanmer, J.; DeWalt, D. A.; Berkowitz, S. A. Association between Food Insecurity and Health-Related Quality of Life: A Nationally Representative Survey. J. Gen. Intern. Med. 2021, 36(6), 1638–1647. [Google Scholar] [CrossRef]
- Rizvi, A.; Wasfi, R.; Enns, A.; Kristjansson, E. The Impact of Novel and Traditional Food Bank Approaches on Food Insecurity: A Longitudinal Study in Ottawa, Canada. BMC Public Health 2021, 21(1), 771. [Google Scholar] [CrossRef]
- Tarasuk, V.; Mitchell, A.; Dachner, N. Household Food Insecurity in Canada, 2014. Research to Identify Policy Options to Reduce Food Insecurity (PROOF); Research to identify policy options to reduce food insecurity (PROOF): Toronto, 2016. [Google Scholar]
- Selvamani, Y.; Arokiasamy, P.; Chaudhary, M. Association between Food Insecurity and Quality of Life among Older Adults (60+) in Six Low and Middle-Income Countries. Arch. Gerontol. Geriatr. 2023, 114, 105079. [Google Scholar] [CrossRef]
- Goodman, M.; Raimer-Goodman, L.; McPherson, H. M. H.; Woldu, D.; Sharma, S.; Ramphul, R.; Mukiri, F.; Maigallo, A. Navigating the Nexus of Food Insecurity, Anxiety, and Depression in the Face of Climate Change: A Longitudinal Study in Rural Kenya. Depress. Anxiety 2025, 2025(1). [Google Scholar] [CrossRef]
- Orihuela, C. A.; Cox, C.; Evans, R.; Dotson, B.; Mrug, S. Household Food Insecurity, School Connectedness, and Psychosocial Adjustment in Early Adolescence. Journal of School Health 2026, 96(2). [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Sagong, H. Discrimination and Vigilance as Psychosocial Pathways from Food Insecurity to Cognitive Difficulty among U.S. Adults: A Moderated Mediation Analysis. BMC Public Health 2026. [Google Scholar] [CrossRef] [PubMed]
- Gyasi, R. M.; Egyir, N. A. A.; Kwabena-Adade, J.; Amanfo, B. A.; Boateng, S.; Gyapong, M.; Nyamadi, V. M.; Boampong, M. S.; Jacob, L.; Phillips, D. R.; Hajek, A. Psychosocial Mechanisms Largely Mediate the Path between Food Insecurity and Depressive Symptoms in Later Life. Geriatr. Nurs. (Minneap). 2026, 68, 103802. [Google Scholar] [CrossRef]
- Kamal, S. H. M.; SoleimanvandiAzar, N.; Ahmadi, S.; Karimi, S. E.; Basakha, M.; Rampisheh, Z.; Tehrani-Banihashemi, A.; Tayefi, B. Food Insecurity among Waste-Picking Children in Iran and Its Associated Factors. Sci. Rep. 2026. [Google Scholar] [CrossRef]
- Liebe, R. A.; Khan, T.; Azad, R.; Adams, L. M.; Braun, A. C.; Davis, H. A.; Misyak, S. A. Experienced Poverty Stigma Is Associated with Food Insecurity, Mental Health, and Resource Utilization among Southern US Mothers with Low Income. BMC Public Health 2025, 25(1), 2469. [Google Scholar] [CrossRef]
- Pineau, C.; Williams, P. L.; Brady, J.; Waddington, M.; Frank, L. Exploring Experiences of Food Insecurity, Stigma, Social Exclusion, and Shame among Women in High-Income Countries: A Narrative Review. Canadian Food Studies / La Revue canadienne des études sur l’alimentation 2021, 8(3). [Google Scholar] [CrossRef]
- Halverson, M. M.; Appel, E. Y.; Earnshaw, V. A.; Sands, G.; Powell, R.; Rozin, M.; Cruz Cordero, T.; Chrisostam, N.; Kennedy, N.; Katz, S. E.; Sharma, S. V.; Karpyn, A. Food Insecurity-Related Stigma Among Adults in the United States: A Scoping Review. American Journal of Health Promotion 2025. [Google Scholar] [CrossRef] [PubMed]
- Evans, R. W.; Maguet, Z. P.; Stratford, G. M.; Biggs, A. M.; Goates, M. C.; Novilla, M. L. B.; Frost, M. E.; Barnes, M. D. Investigating the Poverty-Reducing Effects of SNAP on Non-Nutritional Family Outcomes: A Scoping Review. Matern. Child Health J. 2024, 28(3), 438–469. [Google Scholar] [CrossRef]
- Pourmotabbed, A.; Moradi, S.; Babaei, A.; Ghavami, A.; Mohammadi, H.; Jalili, C.; Symonds, M. E.; Miraghajani, M. Food Insecurity and Mental Health: A Systematic Review and Meta-Analysis. Public Health Nutr. 2020, 23(10), 1778–1790. [Google Scholar] [CrossRef]
- Davenport, K. A. Hungry Minds: Analyzing the Impact of Food Insecurity and FoodAssistance Programs on Neurocognitive Development AndAssistance Programs on Neurocognitive Development AndChildhood Mental HealthChildhood Mental Health; University of South Carolina: Columbia, 2025. [Google Scholar]
- JIANG, Y.; HU, J.; FENG, L.; REN, Q. The Effect of Scarcity Mindset on the Executive Function in Children Living in Poverty and Its Mechanisms. Advances in Psychological Science 2024, 32(5), 728. [Google Scholar] [CrossRef]
- Begdache, L.; Al-Amery, A.; Nagorny, K. K.; Chowdhury, U.; Rosenberg, L. R.; Ertem, Z. The Interplay of Food Insecurity, Resilience, Stress Mindset, and Mental Distress: Insights From a Cross-Sectional Study. Health Sci. Rep. 2025, 8(5). [Google Scholar] [CrossRef]
- Melchior, M.; Caspi, A.; Howard, L. M.; Ambler, A. P.; Bolton, H.; Mountain, N.; Moffitt, T. E. Mental Health Context of Food Insecurity: A Representative Cohort of Families With Young Children. Pediatrics 2009, 124(4), e564–e572. [Google Scholar] [CrossRef] [PubMed]
- Hadley, C.; Tegegn, A.; Tessema, F.; Cowan, J. A.; Asefa, M.; Galea, S. Food Insecurity, Stressful Life Events and Symptoms of Anxiety and Depression in East Africa: Evidence from the Gilgel Gibe Growth and Development Study. J. Epidemiol. Community Health (1978). 2008, 62(11), 980–986. [Google Scholar] [CrossRef]
- Sendhil, M.; Eldar, S. Scarcity: Why Having Too Little Means So Much; Penguin: London, 2013. [Google Scholar]
- Reid, A. Older Adults With Chronic Disease and Food Insecurity in the United States. J. Gerontol. Nurs. 2021, 47(12), 7–11. [Google Scholar] [CrossRef]
- Hill, N. E.; Palakshappa, D.; Chua, K.-P. Chronic Conditions and Food Insecurity in U.S. Children. JAMA Netw. Open 2025, 8(9), e2533953. [Google Scholar] [CrossRef]
- Laurentino, J. S. L.; Brito, R. C. da S.; de Oliveira-Silva, R. T.; Soares, A.; Pereira, T. da C.; de Lima, E. M.; dos Santos, A. B. M. V.; Palmeira, P. de A. Association between Food Insecurity and Chronic Noncommunicable Diseases in Brazil: A Systematic Review. Revista Brasileira de Epidemiologia 2024, 27. [Google Scholar] [CrossRef]
- Seligman, H. K.; Laraia, B. A.; Kushel, M. B. Food Insecurity Is Associated with Chronic Disease among Low-Income NHANES Participants. J. Nutr. 2010, 140(2), 304–310. [Google Scholar] [CrossRef]
- Aljahdali, A. A.; Na, M.; Leung, C. W. Food Insecurity and Health-Related Quality of Life among a Nationally Representative Sample of Older Adults: Cross-Sectional Analysis. BMC Geriatr. 2024, 24(1), 126. [Google Scholar] [CrossRef]
- Fulay, A. P.; Baylin, A.; Wolfson, J. A.; Lee, J. M.; Martinez-Steele, E.; Leung, C. W. Associations between Food Insecurity and Supplemental Nutrition Assistance Program (SNAP) Participation with Ultra-Processed Food Intake in Lower-Income U.S. Adolescents. J. Nutr. Sci. 2025, 14, e41. [Google Scholar] [CrossRef]
- Ribas, S. A.; Medeiros, F. J.; Teixeira, M. T.; Andrade, P. V.; Rodrigues, M. C. C.; Ferreira, F. C. P. de A. di M.; Villela, L. D.; Neri, D. Household Food Insecurity and Its Association with Diet Quality in High-Risk Children. Cien. Saude Colet. 2025, 30(2). [Google Scholar] [CrossRef]
- Hutchinson, J.; Tarasuk, V. The Relationship between Diet Quality and the Severity of Household Food Insecurity in Canada. Public Health Nutr. 2022, 25(4), 1013–1026. [Google Scholar] [CrossRef]
- Herdman, M.; Badia, X.; Berra, S. El EuroQol-5D: Una Alternativa Sencilla Para La Medición de La Calidad de Vida Relacionada Con La Salud En Atención Primaria. Aten. Primaria 2001, 28(6), 425–429. [Google Scholar] [CrossRef]
- Ramos-Goñi, J. M.; Craig, B. M.; Oppe, M.; Ramallo-Fariña, Y.; Pinto-Prades, J. L.; Luo, N.; Rivero-Arias, O. Handling Data Quality Issues to Estimate the Spanish EQ-5D-5L Value Set Using a Hybrid Interval Regression Approach. Value in Health 2018, 21(5), 596–604. [Google Scholar] [CrossRef]
- Hernandez, G.; Garin, O.; Pardo, Y.; Vilagut, G.; Pont, À.; Suárez, M.; Neira, M.; Rajmil, L.; Gorostiza, I.; Ramallo-Fariña, Y.; Cabases, J.; Alonso, J.; Ferrer, M. Validity of the EQ–5D–5L and Reference Norms for the Spanish Population. Quality of Life Research 2018, 27(9), 2337–2348. [Google Scholar] [CrossRef]
- Encuesta Nacional de Salud. España 2011/12. Serie Informes Monográficos No 3. Calidad de Vida Relacionada Con La Salud En Adultos: EQ-5D-5L; Madrid, 2014.
- Gregório, M. J.; Rodrigues, A. M.; Graça, P.; de Sousa, R. D.; Dias, S. S.; Branco, J. C.; Canhão, H. Food Insecurity Is Associated with Low Adherence to the Mediterranean Diet and Adverse Health Conditions in Portuguese Adults. Front. Public Health 2018, 6. [Google Scholar] [CrossRef]
- Neter, J. E.; Dijkstra, S. C.; Dekkers, A. L. M.; Ocké, M. C.; Visser, M.; Brouwer, I. A. Dutch Food Bank Recipients Have Poorer Dietary Intakes than the General and Low-Socioeconomic Status Dutch Adult Population. Eur. J. Nutr. 2018, 57(8), 2747–2758. [Google Scholar] [CrossRef] [PubMed]
- Arrospide, A.; Machón, M.; Ramos-Goñi, J. M.; Ibarrondo, O.; Mar, J. Inequalities in Health-Related Quality of Life According to Age, Gender, Educational Level, Social Class, Body Mass Index and Chronic Diseases Using the Spanish Value Set for Euroquol 5D-5L Questionnaire. Health Qual. Life Outcomes 2019, 17(1), 69. [Google Scholar] [CrossRef] [PubMed]
- Departamento de Salud. Gobierno de Navarra. Diagnóstico de Situación Navarra 2012; Pamplona, 2024.
- Instituto de Estadística de Navarra (Nastat). Encuesta Social y de Condiciones de Vida, Navarra; Pamplona, 2024. [Google Scholar]
- Guillen-Aguinaga, M.; Aguinaga-Ontoso, E.; Guillen-Aguinaga, L.; Guillen-Grima, F.; Aguinaga-Ontoso, I. Data Quality in the Age of AI: A Review of Governance, Ethics, and the FAIR Principles. Data (Basel). 2025, 10(12), 201. [Google Scholar] [CrossRef]
- Khoudri, I.; Belayachi, J.; Dendane, T.; Abidi, K.; Madani, N.; Zekraoui, A.; Zeggwagh, A. A.; Abouqal, R. Measuring Quality of Life after Intensive Care Using the Arabic Version for Morocco of the EuroQol 5 Dimensions. BMC Res. Notes 2012, 5(1), 56. [Google Scholar] [CrossRef]
- Guillen-Aguinaga, S.; Forga, L.; Brugos-Larumbe, A.; Guillen-Grima, F.; Guillen-Aguinaga, L.; Aguinaga-Ontoso, I. Variability in the Control of Type 2 Diabetes in Primary Care and Its Association with Hospital Admissions for Vascular Events. The APNA Study. J. Clin. Med. 2021, 10(24), 5854. [Google Scholar] [CrossRef]
- Textor, J.; van der Zander, B.; Gilthorpe, M. S.; Liśkiewicz, M.; Ellison, G. T. H. Robust Causal Inference Using Directed Acyclic Graphs: The R Package’ Dagitty. Int. J. Epidemiol. 2017, dyw341. [Google Scholar] [CrossRef]
- Battaglini, D.; Robba, C.; Fedele, A.; Trancǎ, S.; Sukkar, S. G.; Di Pilato, V.; Bassetti, M.; Giacobbe, D. R.; Vena, A.; Patroniti, N.; Ball, L.; Brunetti, I.; Torres Martí, A.; Rocco, P. R. M.; Pelosi, P. The Role of Dysbiosis in Critically Ill Patients With COVID-19 and Acute Respiratory Distress Syndrome. Front. Med. (Lausanne). 2021, 8. [Google Scholar] [CrossRef]
- De Silva, S.; Neto, A. S.; Sathe, A.; Higgins, A. M.; Hodgson, C. L. The Psychometric Properties of the EuroQol 5D Five Level in Survivors of Critical Illness. Crit. Care Med. 2025, 53(1), e151–e160. [Google Scholar] [CrossRef]
- EuroQol Research Foundation. EQ-5D-5L User Guide (Version 4.0.); Rotterdam, 2025. [Google Scholar]
- Gili, M.; Roca, M.; Basu, S.; McKee, M.; Stuckler, D. The Mental Health Risks of Economic Crisis in Spain: Evidence from Primary Care Centres, 2006 and 2010. Eur. J. Public Health 2013, 23(1), 103–108. [Google Scholar] [CrossRef] [PubMed]
- Tibbetts, J.; Chapman, C.; O’Dean, S.; Butterworth, P.; Slade, T. The Longitudinal Relationship between Financial Hardship and Mental Health - A Systematic Review of the Evidence. SSM - Mental Health 2025, 8, 100481. [Google Scholar] [CrossRef]
- van Leeuwen, K. M.; Bosmans, J. E.; Jansen, A. P. D.; Hoogendijk, E. O.; van Tulder, M. W.; van der Horst, H. E.; Ostelo, R. W. Comparing Measurement Properties of the EQ-5D-3L, ICECAP-O, and ASCOT in Frail Older Adults. Value in Health 2015, 18(1), 35–43. [Google Scholar] [CrossRef] [PubMed]
- Makai, P.; Brouwer, W. B. F.; Koopmanschap, M. A.; Stolk, E. A.; Nieboer, A. P. Quality of Life Instruments for Economic Evaluations in Health and Social Care for Older People: A Systematic Review. Soc. Sci. Med. 2014, 102, 83–93. [Google Scholar] [CrossRef]
- Roncarolo, F.; Bisset, S.; Potvin, L. Short-Term Effects of Traditional and Alternative Community Interventions to Address Food Insecurity. PLoS One 2016, 11(3), e0150250. [Google Scholar] [CrossRef]
- Goikolea, J. M.; Miralles, G.; Bulbena Cabré, A.; Vieta, E.; Bulbena, A. [Spanish Adaptation of the Seasonal Pattern Assessment Questionnaire (SPAQ) in the Adult and Children-Adolescent Versions]. Actas Esp. Psiquiatr. 2003, 31(4), 192–198. [Google Scholar]
- Lukmanji, A.; Williams, J. V. A.; Bulloch, A. G. M.; Bhattarai, A.; Patten, S. B. Seasonal Variation in Symptoms of Depression: A Canadian Population Based Study. J. Affect. Disord. 2019, 255, 142–149. [Google Scholar] [CrossRef]
- Øverland, S.; Woicik, W.; Sikora, L.; Whittaker, K.; Heli, H.; Skjelkvåle, F. S.; Sivertsen, B.; Colman, I. Seasonality and Symptoms of Depression: A Systematic Review of the Literature. Epidemiol. Psychiatr. Sci. 2019, 29, e31. [Google Scholar] [CrossRef]
- Wiedermann, C. J.; Barbieri, V.; Reismann, H.; Piccoliori, G.; Engl, A.; Hager von Strobele-Prainsack, D. Perceived Financial Strain and Adolescent Mental Health: Evidence from a Population-Based Study in South Tyrol, Italy. Children 2026, 13(1), 121. [Google Scholar] [CrossRef]
- American Psychological Association (APA). Even a joyous holiday season can cause stress for most Americans. Available online: https://www.apa.org/news/press/releases/2023/11/holiday-season-stress (accessed on 1 February 2026).
- Sansone, R. A.; Sansone, L. A. The Christmas Effect on Psychopathology. Innov. Clin. Neurosci. 2011, 8(12), 10–13. [Google Scholar]
- Rojas-Saunero, L. P.; Glymour, M. M.; Mayeda, E. R. Selection Bias in Health Research: Quantifying, Eliminating, or Exacerbating Health Disparities? Curr. Epidemiol. Rep. 2024, 11(1), 63–72. [Google Scholar] [CrossRef]
- Vandenbroucke, J. P.; von Elm, E.; Altman, D. G.; Gøtzsche, P. C.; Mulrow, C. D.; Pocock, S. J.; Poole, C.; Schlesselman, J. J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. International Journal of Surgery 2014, 12(12), 1500–1524. [Google Scholar] [CrossRef]
- Lazarevič, P. Biases in Assertions of Self-Rated Health. Comparative Population Studies 2023, 48. [Google Scholar] [CrossRef]
- Sutton, M.; Carr-Hill, R.; Gravelle, H.; Rice, N. Do Measures of Self-Reported Morbidity Bias the Estimation of the Determinants of Health Care Utilisation? Soc. Sci. Med. 1999, 49(7), 867–878. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, S.; Weber, D. Reporting Biases in Self-Assessed Physical and Cognitive Health Status of Older Europeans. PLoS One 2019, 14(10), e0223526. [Google Scholar] [CrossRef]
- Dowd, J. B.; Todd, M. Does Self-Reported Health Bias the Measurement of Health Inequalities in U.S. Adults? Evidence Using Anchoring Vignettes From the Health and Retirement Study. The Journals of Gerontology: Series B 2011, 66B(4), 478–489. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participant flow diagram for sampling, recruitment, and survey completeness.
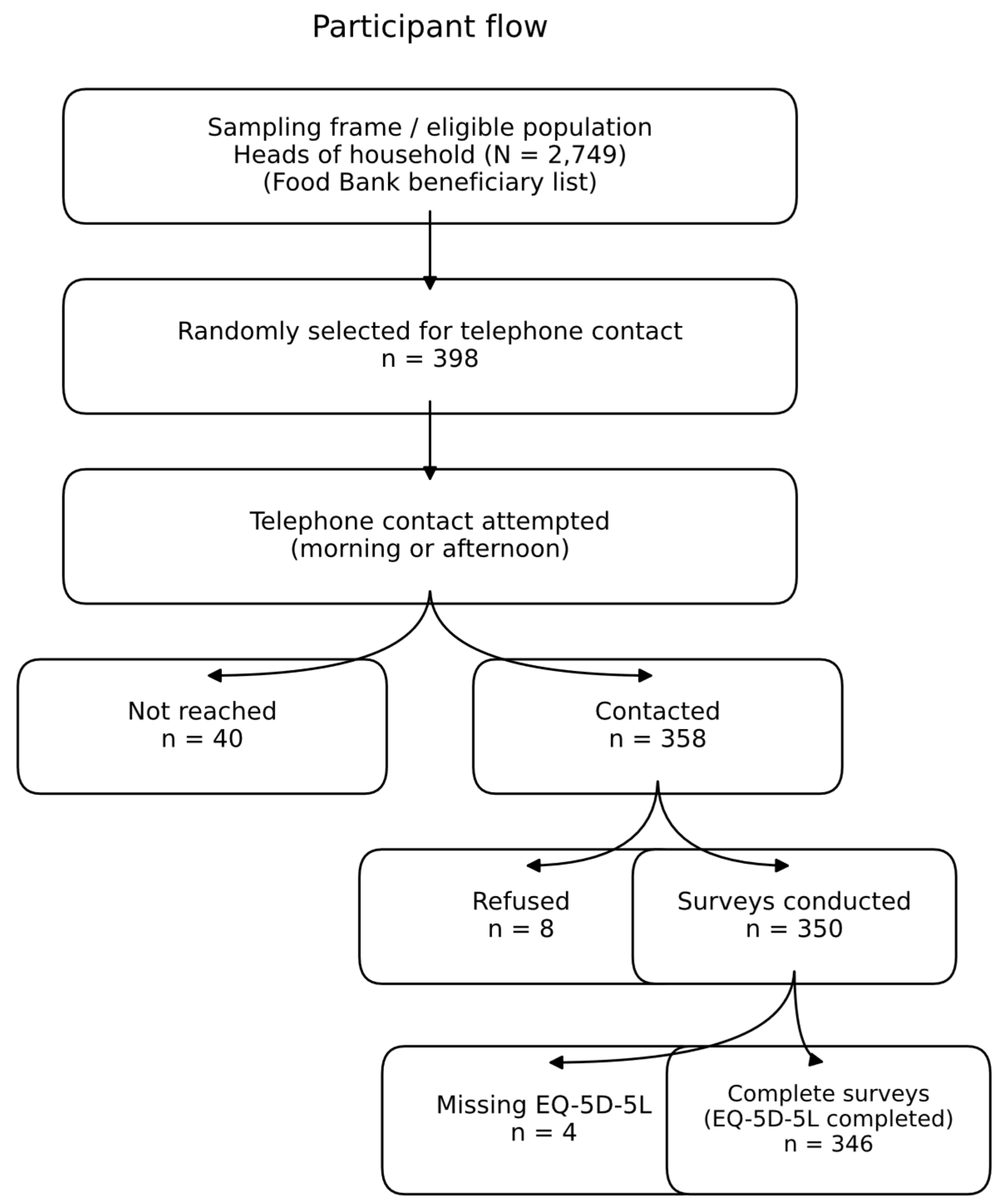

Table 1.
Distribution of the sample by age and sex.
| Sex | N | Mean | SD |
| Male | 105 | 47.2 | 13.2 |
| Female | 245 | 44.7 | 11.8 |
| Total | 350 | 45.5 | 12.3 |
Table 2.
Main sociodemographic and socioeconomic characteristics of the study population (N = 350).
| Sociodemographic and socioeconomic characteristics | Categories |
n (N=350) |
% |
| Employment Status | Full-time employee | 21 | 6.0 |
| Part-time employee | 70 | 20.0 | |
| Unemployed | 92 | 26.3 | |
| Student | 3 | 0.9 | |
| Retired/Pensioner | 22 | 6.3 | |
| Self-employed | 4 | 1.1 | |
| Not working, not looking for work | 59 | 16.9 | |
| Not working due to disability/illness | 20 | 5.7 | |
| Lacks documentation | 59 | 16.9 | |
| How many people live at home? | 1 | 30 | 8.6 |
| 2 | 56 | 16 | |
| 3 | 63 | 18 | |
| 4 | 72 | 20.6 | |
| 5 | 61 | 17.4 | |
| ≥ 6 | 68 | 19.4 | |
| Age Group | 18 to 29 years old | 36 | 10.3 |
| 30 to 44 years old | 143 | 40.9 | |
| 45 to 59 years old | 123 | 35.1 | |
| 60 years or older | 48 | 13.7 | |
| Employment Status | Full-time employee | 21 | 6.0 |
| Part-time employee | 70 | 20 | |
| Unemployed | 92 | 26.3 | |
| Student | 3 | 0.9 | |
| Retired/Pensioner | 22 | 6.3 | |
| Self-employed | 4 | 1.1 | |
| Not working, not looking for work | 59 | 16.9 | |
| Not working due to disability/illness | 20 | 5.7 | |
| Lacks documentation | 59 | 16.9 | |
| Nationality | Spain | 74 | 21.1 |
| Other | 276 | 78.9 | |
| Geographic Origin | Africa | 93 | 26.6 |
| Asia | 2 | 0.6 | |
| Europe | 107 | 30.6 | |
| Latin America | 148 | 42.3 | |
| Education Level | Unable to read or write | 12 | 3.4 |
| No formal education (can read/write) | 37 | 10.6 | |
| Primary or secondary education | 217 | 62 | |
| University or vocational training | 84 | 24 |
Table 3.
Prevalence of reported problems by EQ-5D-5L dimension, % (95% CI).
| Population group | VAS | Mobility | Self-care |
Daily activities |
Pain /Discomfort |
Anxiety /Depression |
| Total | 73.5 (71.6-75.5) |
25.5 (20.9-30.1) |
8.7 (5.7-11.7) |
19.7 (15.5-23.9) |
55.7 (50.4-60.9) |
62.9 (57.8-68.0) |
| Male | 75.8 (72.3-79.3) |
24.8 (16.2-33.3) |
8.9 (3.3-14.6) |
19.8 (11.9-27.7) |
44.6 (34.7-54.4) |
56.4 (46.6-66.3) |
| Female | 72.6 (70.2-74.9) |
25.8 (20.3-31.3) |
8.6 (5.1-12.2) |
19.7 (14.6-24.7) |
60.2 (54.1-66.4) |
65.6 (59.6-71.6) |
| Navarra Total(2024) [82] | 88.1* | 13*** | 5.3* | 8*** | 35.7*** | 22*** |
| Male Navarra [82] | 89.9* | 11.0*** | 4.5*** | 6.1*** | 28.2*** | 17.3*** |
| Female Navarra (2024) [82] | 86.4* | 1.4*** | 6.1 | 9.9*** | 43*** | 26.6*** |
| Spain (2011)[77] | 77.5 | 14.3*** | 6.2 | 11.1*** | 25.5*** | 15.0*** |
| Navarra (2011)[77] | 77.4 | 11.7*** | 4.0 | 8.9*** | 21.1*** | 14.0*** |
VAS= Visual Analogue Scale Chi-square comparison of the Study group with Navarra and Spain. *p < 0.05 **p < 0.01 *** p < 0.001.
Table 4.
Descriptive statistics of the EQ-5D-5L Visual Analog Scale (VAS) in BAN respondents and general population score in Navarre (2024).
Table 4.
Descriptive statistics of the EQ-5D-5L Visual Analog Scale (VAS) in BAN respondents and general population score in Navarre (2024).
| N |
Mean 95% IC |
SD | Median | Navarre (2024) | |
| Total | 345 | 73.56 (71.62-75.50) |
18.28 | 75.0 | 91.4 |
| Men | 102 | 75.83 (72.35-79.36) |
17.86 | 80.0 | 92.9 |
| Women | 243 | 72.60 (70.27-74.92) |
18.41 | 75.0 | 89.9 |
| Age groups | |||||
| 18 to 29 years old | 36 | 76.14 (69.64-82.64) |
19.20 | 80 | 95.7 |
| 30 to 44 years old | 142 | 77.99 (75.46-80.53)* |
15.27 | 80 | 93.9 |
| 45 to 59 years old | 121 | 70.72 (67.31-74.12)* |
18.91 | 70 | 92.6 |
| 60 years old or older | 46 | 65.33 (59.20-71.45)* |
20.61 | 70 | 86.0 |
| Nationality | |||||
| Spain | 73 | 68.63 (63.43-73.83 |
22.3 | 70 | 91.2 |
| Other | 272 | 74.88 (72.87-76.89) |
16.85 | 80 | 92.7 |
| Level of education | |||||
| Cannot read or write | 11 | 72.73 (59.86-85.59 |
19.15 | 70.0 | - |
| No education. but can read and write | 36 | 73.89 (67.39-80.39) |
19.2 | 80 | - |
| Primary or secondary education | 214 | 75.01 (72.64-77.39 |
17.65 | 80 | 92 |
| University education or vocational training | 84 | 69.82 (65.67-73.98) |
19.14 | 70 | 93.8 |
* ANOVA with Scheffé test: significant differences (<0.05) between: Group 60 or older with the 18-29 and 30-44 age groups; the 30-44 age group with the 45-59 age group.
Table 5.
EQ-5D-5L utility index and complementary severity index in Navarra Food Bank users.
| Variable |
Total (n = 346) |
Male (n = 104) |
Male (n = 104) |
| EQ-5D-5L utility index* | 0.815 (0.800–0.831) |
0.838 (0.813–0.862) |
0.806 (0.786–0.825) |
| Complementary severity index (0–100)** | 81.54 (79.80–83.08) |
83.76 (81.33–86.18) |
80.59 (78.64–82.53) |
| Severity index Spain [82] | 93.68 | 96.61 | 91.85 |
* The EQ-5D-5L utility index was calculated using the Spanish population value set [75]. ** The complementary severity index corresponds to the transformation 100 − IS, where higher values indicate better health status and lower severity, and is presented to facilitate comparison with the 2011–2012 National Health Survey.
Table 6.
Descriptive statistics for the Visual Analogue Scale and the EQ-5D-5L Index.
| HRQOL assessment variables | Cluster 2 groups | n | Mean | Median | Percentile 25 | Percentile 75 |
| VAS | Low score | 100 | 50.5 | 12.3 | 50.0 | 50.0 |
| High score | 245 | 83.0 | 10.1 | 80.0 | 75.0 | |
| EQ-5D-5L Index | Low score | 68 | 0.574 | 0.130 | 0.602 | 0.512 |
| High score | 278 | 0.874 | 0.069 | 0.898 | 0.812 |
VAS= Visual Analogue Scale.
Table 7.
Logistic regression adjusting by age and sex for the Visual Analogue Scale (VAS) and the EQ-5D-5L Index.
Table 7.
Logistic regression adjusting by age and sex for the Visual Analogue Scale (VAS) and the EQ-5D-5L Index.
| Model 1: VAS Scale2 | Model 2: EQ-5D-5L Index 3 | |||
| Independent Variable | OR (95% CI)* | p-value** | OR (95% CI) | p-value |
| Age | 0.998 (0.972–1.026) | 0.912 | 1.002 (0.972–1.033) | 0.914 |
| Sex (Male)1 | 1.111 (0.574–2.151) | 0.754 | 1.511 (0.705–3.238) | 0.289 |
| Mobility | 3.910 (1.840–8.308) | <0.001 | 3.024 (1.322–6.919) | 0.009 |
| Self-care | 1.187 (0.361–3.901) | 0.777 | 1.654 (0.578–4.733) | 0.349 |
| Usual activities | 2.983 (1.162–7.653) | 0.023 | 3.266 (1.278–8.343) | 0.013 |
| Pain/discomfort | 3.368 (1.646–6.891) | 0.001 | 4.183 (1.608–10.878) | 0.003 |
| Anxiety/depression | 2.845 (1.412–5.730) | 0.003 | 1.622 (0.737–3.568) | 0.23 |
VAS= Visual Analogue Scale ;* OR (95% CI): Odds Ratio and 95% Confidence Interval. ;** p < 0.05 indicates statistical significance; significant findings are in bold ;1Reference category: Female. ;2 Logistic regression using the high-score cluster based on the Visual Analogue Scale as the dependent variable;. 3 Logistic regression using the high-score cluster based on the EQ-5D-5L Index as the dependent variable.;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



