Submitted:
06 February 2026
Posted:
09 February 2026
You are already at the latest version
Abstract
Background: Addressing the pervasive issue of low medication adherence is a critical step in reducing South Africa's disease burden. While counselling is mandated in key disease initiatives, primary health care services often employ directive, information-based methods that do not sufficiently encourage lasting behavior change. Motivational Interviewing is a person-centered, evidence-based approach that enhances motivation, fosters adherence, and supports active engagement in care. However, the extent of its application in South African PHC remains unexplored. Objectives: This review synthesizes current evidence on MI's usage in South African primary health care, emphasizing its effectiveness, identifying implementation gaps, and its potential to enhance person-centered disease management. Methods: This scoping review followed the Arksey and O'Malley framework and PRISMA-ScR guidelines. The research question was formulated with an expansive scope to comprehensively map MI's application, ensuring alignment with policy-oriented aims to integrate MI systematically into PHC. Electronic databases and grey literature were searched for studies published from 2000 to 2025 on MI or similar counselling in South African PHC and community public sector settings. Data were collected and summarized against established objectives to generate critical insights to inform policy and practice improvements. Results: Of the 38 identified records, 21 studies met the inclusion criteria. Among these, 81% used MI as brief, MI-informed counselling in routine PHC services rather than full-protocol MI. Seventy-six percent focused on HIV adherence, while 62% ad-dressed non-communicable diseases, with emerging evidence in tuberculosis care. Reported benefits included improved medication adherence, increased engagement and retention in care, and stronger patient-provider relationships. Challenges included limited staff training, inadequate supervision or monitoring, and reliance on project-based delivery. Conclusion: Motivational Interviewing is practical and can be scaled up to support behavior change in South African PHCs, particularly to improve adherence and long-term care engagement. However, its effectiveness is constrained by uneven implementation and insufficient system support. Integrating MI into national policies, PHC routines, and workforce training could strengthen person-centered care and improve disease control.
Keywords:
motivational interviewing
; primary health care
; behavior change counselling
; therapy adherence
; disease control
; South Africa
1. Introduction
1.1. Background
South Africa has a complex health profile, with a lasting quadruple burden of disease: communicable diseases (especially HIV and tuberculosis), non-communicable diseases, mental health conditions, and injuries (Mayosi et al., 2012; Bradshaw et al., 2022). Even with improved access to biomedical care, disease control outcomes remain below expectations in many programs, especially in the public-sector PHC (Hammer & Whittaker, 2020). Additional evidence indicates that factors such as nonadherence to treatment, delays in seeking care, unhealthy behaviors, and poor retention significantly affect disease outcomes (Vos et al., 2020; Bradshaw et al., 2022). In South Africa, these problems are exacerbated by inequality, poverty, stigma, multiple illnesses, and health system challenges, placing additional pressure on PHC services to support sustained behavior change (Ngene et al., 2023, pp. 1-10). National health policies stress the importance of counselling and psychosocial support in disease control for HIV, TB, NCDs, and mental health programs (Department of Health [DoH], 2016; DoH, 2023). Still, the effectiveness of counselling in routine PHC services varies, raising concerns about whether current approaches are suitable and consistent. (Sorsdahl et al., 2015)
1.2. Problem Statement
Although counselling is required in major disease programs, South African PHC primarily uses information-giving and prescriptive methods, known as information–education communication (IEC) strategies (WHO, 2010; Ticha et al., 2022). These methods assume that more knowledge leads to behavior change. Still, evidence indicates that knowledge alone is insufficient for sustained adherence, lifestyle change, or long-term care, particularly when ambivalence, stigma, or economic hardship are present (Miller & Rollnick, 2013). By contrast, Motivational Interviewing has been shown to significantly reduce relapse rates across various health settings by actively engaging patients in their care processes (Sorsdahl, Stein, Corrighall, Cuijpers, Smits, Naledi, & Myers, 2015). This highlights the potential inadequacies of IEC approaches and underscores the need to integrate MI into South African PHC to drive meaningful and sustainable behavior change (Da Silva, Schneider & Okello, 2015).
Because of this, South Africa still faces high rates of loss to follow-up in TB and HIV programs, low rates of viral suppression and treatment completion, and poor control of chronic NCDs like diabetes and hypertension (Mwansa-Kambafwile et al., 2020; Bradshaw et al., 2022; Malan et al., 2024). Health workers often report a lack of confidence and skills to manage patient resistance, ambivalence, and withdrawal, which makes counselling less effective (Tichá et al., 2022)2). Although there is international evidence for other counselling methods, there is little summary of how these, particularly Motivational Interviewing, are used in South African PHC.
1.3. Rationale
Motivational Interviewing (MI) is a collaborative, person-centered counselling method that helps people find their own motivation for change by working through ambivalence (Miller & Rollnick, 2013). MI has been shown to be effective for many health behaviors, including medication adherence, reducing substance use, changing lifestyle behaviors, and engaging in chronic disease care (Lundahl et al., 2013).
MI is especially well-suited to PHC contexts because it:
- Can be delivered as brief interventions within routine consultations. It is consistent with task-shifting and multidisciplinary team models.
- Emphasizes empathy, partnership, and autonomy, which are central to people-centered care. This alignment directly supports the PHC re-engineering goals by enhancing patient satisfaction, improving health outcomes, and fostering provider collaboration, which are key PHC performance indicators.
In South Africa, MI aligns well with PHC re-engineering, ward-based outreach teams, new service delivery models, and National Health Insurance (NHI) goals focused on quality, efficiency, and patient experience (DoH, 2011; DoH, 2023). Although MI is mentioned more often in policy and training, its actual use, range, and impact in South African PHC remain scattered and poorly summarized (Da Silva, Schneider, & Okello, 2015).
1.4. Contribution to the Body of Knowledge
This review is the first to fully summarize the use of MI in South African PHC and community public health services. It addresses the decisive policy gap of how Motivational Interviewing can be systematically integrated into national health frameworks to enhance behavior change strategies in PHCs. By demonstrating the practicality and scalability of MI within the current health care models, this review answers the critical policy question: How can MI be implemented comprehensively to bolster existing national health strategies? It shows that MI is mostly used as brief, MI-informed counselling in regular care, especially in HIV and non-communicable disease programs, with some new use in TB services. The review identifies systemic gaps, including limited training, insufficient supervision and monitoring, and project-based delivery. The data show MI to be a practical and scalable counselling method that aligns with PHC re-engineering, people-centered care, and National Health Insurance goals (Rollnick et al., 2008, pp. 101-108). The review outlines steps to integrate MI into policy, workforce training, and research to improve disease control in South Africa.
1.5. Aim of the Review
This scoping review aimed to systematically map and synthesize the existing evidence on the use of Motivational Interviewing as a behaviour-change counselling approach for disease control within South African primary health care and community-based public health services.
1.6. Objectives
The objectives of the review were to:
- Identify how Motivational Interviewing has been applied within South African PHC and community health settings.
- Describe the disease programs and populations in which MI has been used.
- Summarize reported outcomes associated with MI-based interventions for disease control, including adherence, retention in care, and patient engagement. For each reported outcome, align it with a measurable indicator, such as the percentage of patients retained in care, adherence improvement rates, and patient engagement levels assessed using standardized tools or surveys. These metrics will provide a clearer framework for evaluating the effectiveness of MI-based interventions. Identify implementation facilitators, barriers, and gaps to direct future policy, practice, and research.
2. Materials and Methods
2.1. Study Design
A scoping review was conducted to map the extent, nature, and characteristics of the evidence on the use of Motivational Interviewing (MI) as a behavior change counselling approach within South African primary health care (PHC) services. The review followed the five-stage framework proposed by Arksey and O’Malley: (1) identifying the research question; (2) determining relevant studies; (3) study selection; (4) charting the data; and (5) collating, summarizing, and reporting results. Reporting was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR).
2.2. Identifying the Research Question
In accordance with the first stage of the Arksey and O’Malley scoping review framework, the research question was formulated to be broad, exploratory, and encompassing, representing the purpose of a scoping review to map the extent, range, and nature of evidence rather than to assess intervention effectiveness.
The research question was informed by:
- South Africa’s burden of disease and policy emphasis on counselling within primary health care (PHC);
- Emerging use of Motivational Interviewing (MI) in local programs; and
- The absence of a consolidated synthesis of MI use within South African PHC services.
The primary research question guiding this review was: How has Motivational Interviewing been used as a behavior change counselling approach for disease control within South African primary health care and community-based public health services? To operationalize this broad question and guide systematic study identification and data charting, the following sub-questions were specified:
- In what ways has Motivational Interviewing been applied within South African PHC and community health settings?
- Which disease programs and populations have been targeted by MI-based interventions?
- What outcomes related to disease control (e.g., adherence, retention in care, engagement) have been reported in association with MI-based counselling?
- What implementation facilitators, barriers, and gaps are reported in the South African context?
The author intentionally framed these questions to capture both intervention characteristics and health system considerations, guaranteeing alignment with the review’s objective of informing policy, practice, and future research. The research questions also guided the development of the search strategy, eligibility criteria, data extraction framework, and thematic synthesis. The author selected a scoping review approach because the aim was to map how Motivational Interviewing has been applied within South African PHC, identify gaps, and inform implementation, rather than to evaluate intervention effectiveness.
2.3. Determining Relevant Studies
The author conducted electronic database searches in PubMed/MEDLINE, Scopus, Web of Science, PsycINFO, CINAHL, Sabinet, and African Journals Online. In addition, the author identified grey literature through searches of South African Department of Health repositories, provincial health department reports, the Human Sciences Research Council, the World Health Organization, UNAIDS, and university institutional repositories. Searches covered the period from January 2000 to December 2025 and were limited to English-language publications from South Africa. The starting point of 2000 coincides with the introduction of significant health policy reforms in South Africa, including key strategies for controlling communicable and non-communicable diseases. The full search strategy for all databases is provided in Appendix A.
Eligibility Criteria
Studies were eligible for inclusion if they:
- were conducted in South Africa;
- examined Motivational Interviewing or MI-consistent counselling approaches;
- were implemented within PHC or community-based public health settings; and
- addressed disease prevention, compliance with treatment, retention in care, or long-term condition management.
Studies conducted exclusively in specialist or tertiary psychotherapy settings, or those without a clear MI component, were excluded.
2.4. Study Selection
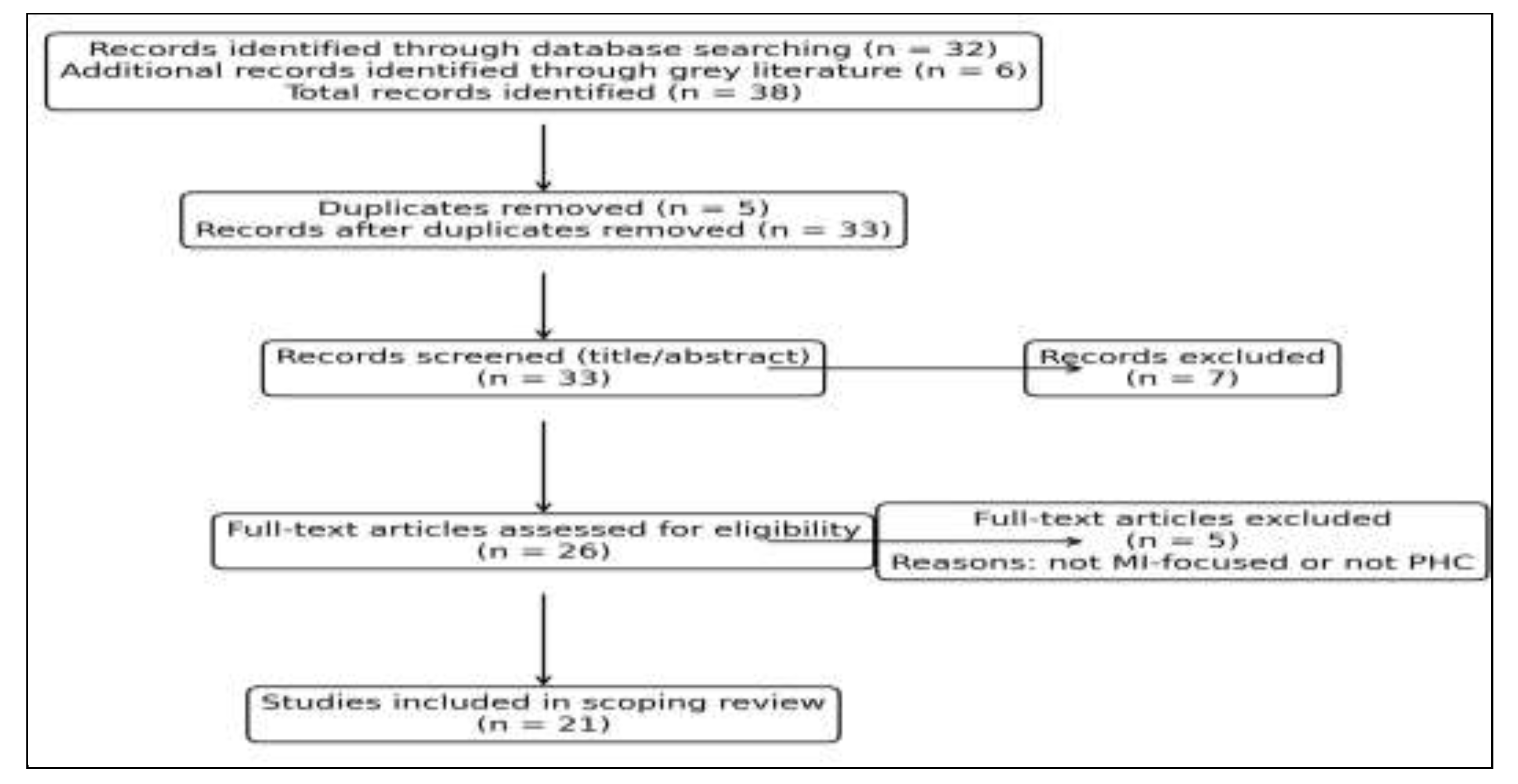
Following duplicate removal, titles and abstracts were screened against the inclusion criteria. Full-text articles were then assessed for eligibility. Reasons for exclusion at the full-text stage included lack of MI content and non-PHC settings. Thus, records identified through database searching (n = 32); additional records identified through grey literature (n = 6); total records identified (n = 38); duplicates removed (n = 5); records screened (title/abstract) (n = 33); records excluded (n = 7); full-text articles assessed for eligibility (n = 26); full-text articles excluded (n = 5; reasons: not MI-focused or not PHC); studies included in the scoping review (n = 21). This study selection process is summarized using a PRISMA-ScR flow diagram in Appendix B.
2.5. Data Charting and Synthesis
The author used a structured data charting form to extract information on study design, setting, population, disease focus, description of the MI intervention, outcomes, and reported implementation facilitators and barriers. Inter-rater reliability checks and pilot testing of the data extraction form were conducted as safeguards to ensure accuracy and consistency in data charting (Büchter et al., 2020). Extracted data were synthesized narratively, with results grouped thematically by disease focus and implementation characteristics.
Risk of Bias and Methodological Considerations
Consistent with PRISMA-ScR guidance, a formal risk-of-bias assessment was not conducted, as the primary purpose of this scoping review was to map available evidence rather than to evaluate intervention effectiveness. However, to strengthen transparency and tackle potential methodological weaknesses, the contracted independent reviewer identified sources of bias across the included studies, which were assessed narratively and reported in the limitations section.
3. Results
A total of 21 studies met the inclusion criteria and were included in the scoping review (Appendix C). The results are presented in accordance with the review objectives.
3.1. Application of Motivational Interviewing within South African PHC and Community Health Settings
The included studies demonstrated that Motivational Interviewing (MI) has been applied in South Africa predominantly as brief, MI-informed counselling, rather than as full-protocol MI. On average, these interventions lasted 10-15 minutes, aligning with the time constraints typically observed in South African PHC settings. PHC clinic nurses and community health workers delivered interventions mainly within public-sector primary health care (PHC) facilities and community-based services, including clinics, ward-based outreach teams, and follow-up support programs (Da Silva et al., 2018; Ticha et al., 2022). Professional nurses primarily delivered MI-based counselling, while lay counsellors, community health workers, and health promoters undertook this task, reflecting task-shifting practices within the South African PHC system (Da Silva et al., 2018; Ticha et al., 2022).
MI principles, such as open-ended questioning, reflective listening, affirmations, and elicitation of change talk, were commonly integrated into routine counselling encounters, including treatment initiation, follow-up visits, and defaulter tracing (Miller & Rollnick, 2013; Malan et al., 2024). However, few studies reported the use of validated fidelity assessment tools, and MI delivery was often described as “MI-based” or “MI-informed” rather than standardized.
3.2. Disease Programs and Populations Targeted by MI Interventions in South Africa
MI interventions were most frequently applied within HIV care, particularly for antiretroviral therapy (ART) adherence, retention in care, and re-engagement following loss to follow-up (DoH, 2016; HIV Retention Study, 2025; UNAIDS, 2024). A second major focus area was non-communicable diseases (NCDs), including diabetes and hypertension, where MI-informed counselling supported lifestyle modification and long-term medication adherence (Malan et al., 2024; Bradshaw et al., 2022).
The review identified emerging evidence in:
- Tuberculosis (TB) treatment support, including adherence counselling and stigma-sensitive interventions (Mwansa-Kambafwile et al., 2020; Foster et al., 2024)
- General PHC populations, where MI principles were used to support health-seeking behavior and continuity of care (Da Silva et al., 2018)
Most interventions targeted adult patients, with limited focus on adolescents, youth, maternal health, or individuals with multimorbidity, despite the growing burden of co-existing conditions in South Africa (Mayosi et al., 2012; Vos et al., 2020).
3.3. Reported Outcomes Associated with MI-Based Interventions
Across included studies, MI-based counselling was associated with several positive outcomes relevant to disease control. These included:
- Improved therapy adherence, particularly in HIV and NCD programs (Lundahl et al., 2013; Malan et al., 2024)
- Enhanced retention in care and reduced disengagement, including improved follow-up attendance and re-engagement after treatment interruption (Mwansa-Kambafwile et al., 2020; HIV Retention Study, 2025)
- Increased patient involvement and motivation, characterized by greater participation in decision-making and openness in discussing barriers to care (Miller & Rollnick, 2013; Ticha et al., 2022)
- Strengthened patient–provider relationships, including increased trust and perceived empathy (Foster et al., 2024)
Outcome measurement varied substantially across studies. Many relied on self-reported adherence, qualitative accounts, or proxy indicators of engagement, while objective clinical outcomes, such as viral suppression, TB treatment completion, or glycemic control, were inconsistently reported (Lundahl et al., 2013; Malan et al., 2024).
3.4. MI Implementation Facilitators and Barriers in South Africa
Facilitators of MI implementation included adherence to person-centered care principles, compatibility with brief counselling encounters, and acceptability among both providers and patients (Miller & Rollnick, 2013; DoH, 2023). Several studies noted that MI enhanced providers’ confidence in managing ambivalence and resistance, particularly in adherence counselling contexts (Ticha et al., 2022).
Common barriers included limited formal training in MI, lack of structured supervision and fidelity monitoring, high workload and time constraints, and inconsistent inclusion into routine service workflows (Da Silva et al., 2018; Ticha et al., 2022; Malan et al., 2024). MI implementation was often project-based, limiting sustainability beyond the pilot phase (Mwansa-Kambafwile et al., 2020). One pragmatic workflow adjustment that could quickly relieve time pressure for nurses is the integration of MI into existing electronic health record (EHR) systems. This adjustment would enable automated prompts and reminders for MI strategies during consultations, reducing cognitive load and time spent recalling MI techniques and thereby improving efficiency (Weimann & Petersen, 2017).
Overall, the results show that MI is primarily utilized in South African PHC as a practical, adapted counselling method integrated into routine services. While studies frequently report improvements in adherence, engagement, and patient experience, the evidence remains fragmented, with considerable variation in intervention design, delivery, and measurement.
4. Discussion
This scoping review synthesized evidence regarding the use of Motivational Interviewing (MI) for behavior change counselling in South African PHC. The results show that MI is predominantly employed as a practical, adapted approach within routine services rather than as a standalone intervention. This approach aligns with the functional realities of South African PHCs, where limited time, high patient volumes, and task shifting necessitate brief, flexible counselling (Da Silva et al., 2018; Ticha et al., 2022).
MI was most consistently applied within HIV adherence counselling and non-communicable disease (NCD) lifestyle management, with more limited and emerging use in tuberculosis (TB) treatment support. This pattern mirrors national programme priorities and funding streams but additionally highlights missed opportunities for wider application, particularly in TB, mental health, adolescent health, and multimorbidity care (Mayosi et al., 2012; Bradshaw et al., 2022). Given that these conditions share common behavioral demands, long-term adherence, sustained self-management, and retention in care, the limited scope of MI use beyond HIV and NCDs amounts to a considerable gap.
Across included studies, MI-based counselling was associated with improved medication adherence, enhanced engagement in care, and strengthened patient–provider relationships (Lundahl et al., 2013; Malan et al., 2024; Mwansa-Kambafwile et al., 2020). These outcomes are consistent with international evidence demonstrating MI’s success in addressing ambivalence and reluctance to change through collaborative, autonomy-supportive communication (Miller & Rollnick, 2013). Notably, several studies reported improvements in engagement, motivation, and trust even where objective clinical outcomes were inconsistently measured, suggesting that MI’s effects may initially manifest through relational and motivational pathways that precede measurable biomedical change (Ticha et al., 2022; Foster et al., 2024).
However, the review also identified substantial variability in how MI was defined, delivered, and evaluated. Most interventions were described as “MI-informed,” with limited use of structured training, supervision, or fidelity assessment tools. This raises concerns about the dilution of MI’s core components and highlights the risk that MI may be reduced to a general interaction mode rather than implemented as a distinct, evidence-based counselling approach (Miller & Rollnick, 2013; Lundahl et al., 2013). The absence of fidelity monitoring adds to the complexity of interpreting outcomes and comparing across studies (Kalthom et al., 2021).
Implementation barriers, including limited training, high workloads, and reliance on short-term, project-based initiatives, reveal broader systemic challenges within South African PHC rather than limitations intrinsic to MI itself (Da Silva et al., 2018; Mwansa-Kambafwile et al., 2020). Conversely, facilitators such as conformity with person-centred care principles, compatibility with brief consultations, and acceptability to both providers and patients underscore MI’s suitability for PHC when enabling system conditions are present (Department of Health [DoH], 2016; DoH, 2023).
To summarise, MI shows considerable potential as an expandable counselling method for disease control in South Africa. However, its impact is constrained by inconsistent implementation, insufficient system support, and limited integration into routine PHC practices.
Strengths and Limitations of the Review
This scoping review has several important strengths. First, it employed a rigorous, transparent methodological approach using the Arksey and O’Malley framework and was reported in line with PRISMA-ScR guidance, thereby enhancing repeatability and methodological credibility. Second, the inclusion of both peer-reviewed and grey literature, including national policy documents and programme reports, enabled a thorough mapping of the use of Motivational Interviewing (MI) in South African primary health care (PHC), extending beyond the academic literature. Third, the review focused explicitly on PHC and community-based public-sector settings, ensuring strong relevance to routine service delivery and health-system implementation. Fourth, by examining MI across multiple disease programs rather than a single condition, the review provides a system-level perspective on behavior change counselling in a context characterized by multimorbidity. Finally, the explicit consideration of implementation factors, such as workforce training, supervision, fidelity, and workflow integration, improves the review’s utility for decision-makers, managers, and practitioners seeking scalable, sustainable approaches to improve disease control.
However, the author acknowledges several limitations. The included evidence base was dominated by qualitative studies, programme evaluations, and small quasi-experimental designs, with few randomized controlled trials conducted in South African PHC settings, limiting causal inference. Selection bias may be present, as many studies relied on convenience samples from single facilities or districts, which may limit generalizability. In addition, MI fidelity was rarely assessed, with many interventions described as “MI-informed” rather than formally evaluated against validated competency measures. Outcome reporting was heterogeneous and frequently depended on self-reported adherence or engagement, while objective clinical indicators were inconsistently measured. Follow-up periods were frequently short, limiting assessment of sustained behavior change. Although the inclusion of grey literature reduced publication bias, some programme reports lacked detailed methodological descriptions. Despite these limitations, the review fulfils its scoping objective by mapping available evidence, identifying gaps, and directing future research and implementation priorities.
Practice Implications
- PHC services should move beyond directive information–education–communication approaches (IEC) and adopt Motivational Interviewing (MI) as a structured, evidence-based counseling method that addresses ambivalence and supports sustained behavior change.
- PHC clinics and community-based services should operationalize MI by integrating it into existing service points, including adherence counseling, chronic disease reviews, defaulter tracing, ward-based outreach team activities, and differentiated service delivery models, rather than treating it as an additional task.
- Nurses, community health workers, health promoters, and adherence counselors require task-appropriate MI training, supported by ongoing supervision and mentoring to maintain competency and adherence under routine workload conditions.
- MI operationalizes people-centered care principles and can strengthen therapy adherence, retention, and patient experience, key performance domains under the National Health Insurance contracting and quality assurance mechanisms (Hanmer & Whittaker, 2020).
- PHC clinics and community-based services should operationalize MI. MI should be applied across HIV, TB, non-communicable diseases, mental health, and multimorbidity care to maximize its contribution to disease control in South Africa’s PHC system (UNAIDS. (2023).
Recommendations
The following recommendations are informed by the findings of this review and consistent with national health system priorities.
For policy and governance, South Africa should,
- Formally adopt Motivational Interviewing as a core counselling approach within national and provincial guidelines for HIV, TB, NCDs, mental health, and PHC re-engineering (DoH, 2016; DoH, 2023).
- Position MI as a health system strengthening intervention, explicitly linked to people-centered care, quality improvement, and National Health Insurance performance objectives (DoH, 2011).
For Workforce development, the health system should,
- Institutionalize MI training within pre-service education, in-service training, and continuing professional development for PHC nurses, community health workers, health promoters, as well as adherence counsellors (Ticha et al., 2022). To ensure training effectiveness, a competency benchmark should be established, utilizing a specific fidelity score or skill checklist. This benchmark would serve as an objective measure to signal that training has been effectively implemented and to help implementers consistently evaluate success (Tricco et al., 2020).
- Prioritize brief MI competencies suitable for routine PHC consultations, supported by structured supervision and mentoring to maintain skill fidelity (Miller & Rollnick, 2013).
For Service delivery and programme integration, the Department of Health should,
- Embed MI into routine PHC workflows, including adherence counselling, chronic disease reviews, defaulter tracing, ward-based outreach team activities, and differentiated service delivery models (Da Silva et al., 2018).
- Expand MI application beyond HIV and NCDs to TB, mental health, adolescent health, and multimorbidity management to maximize system-wide impact (Mayosi et al., 2012; Bradshaw et al., 2022).
For Research and evaluation, academic and research institutions should,
- Strengthen implementation research using appropriate tools to assess scalability, sustainability, and contextual adaptation of MI in PHC settings (Tricco et al., 2018).
- Standardize outcome measurement, incorporating behavioral indicators alongside objective clinical outcomes such as viral suppression, TB treatment completion, and NCD control (Lundahl et al., 2013).
- Conduct economic and workload analyses to support policy decisions on investing in counselling capacity within PHC (Mwansa-Kambafwile et al., 2020).
5. Conclusions
This scoping review demonstrates that Motivational Interviewing has been implemented in South African primary health care as a flexible, person-centred counselling method, chiefly within HIV and NCD programs. The evidence indicates that MI-based counselling is associated with improved adherence, care engagement, and patient–provider relationships, which are important for disease control in contexts characterized by chronic illness and multimorbidity (Lundahl et al., 2013; Bradshaw et al., 2022).
Although it has potential, MI is still applied inconsistently, predominantly in short-term projects, and there is limited standardization in training, supervision, or monitoring. In the absence of comprehensive system-wide integration, the benefits of MI for disease outcomes and PHC performance are unlikely to be fully realized. Establishing MI as a core counselling method may enhance person-centered care, retention, and observance, therewith supporting South Africa’s objectives for universal health coverage and National Health Insurance (Zuma et al., 2023).
Author Contributions
Conceptualization, T.G methodology, TG; validation, TG; formal analysis, TG.; investigation, TG.; data curation, X.X.; writing—original draft preparation, TG.; writing—review and editing, TG. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
In this section, please add the Institutional Review Board Statement and approval number for studies involving humans or animals. You might choose to exclude this statement if the study did not require ethical approval. Please note that the Editorial Office might ask you for further information. Please add “The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving humans. OR “The animal study protocol was approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval)” for studies involving animals. OR “Ethical review and approval were waived for this study due to REASON (please provide a detailed justification).” OR “Not applicable” for studies not involving humans or animals.
Informed Consent Statement
Not applicable because the study did not involve humans.
Data Availability Statement
All relevant supplementary data are provided in the appendices.
Acknowledgments
Sincere gratitude goes to the librarian (who does not wish to be named) for providing technical support in identifying relevant studies and conducting an independent review. During the preparation of this manuscript, the author used ChatGPT to polish the language and grammar. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The author declares no conflicts of interest.
Appendix A: Search Strategy
1. PUBMED (MEDLINE)
(“motivational interviewing”[Title/Abstract]
OR “behaviour change counselling”[Title/Abstract]
OR “behavior change counseling”[Title/Abstract])
AND
(“primary health care”[Title/Abstract]
OR “primary healthcare”[Title/Abstract]
OR “PHC”[Title/Abstract]
OR “community health services”[Title/Abstract])
AND
(“South Africa”[Title/Abstract])
AND
(Adherence OR “treatment adherence.”
OR “retention in care.”
OR “lifestyle modification.”
OR “disease control”)
2. SCOPUS
TITLE-ABS-KEY (“motivational interviewing.”
OR “behaviour change counselling.”
OR “behavior change counseling”)
AND
TITLE-ABS-KEY (“primary health care.”
OR “primary healthcare.”
OR PHC
OR “community health”)
AND
TITLE-ABS-KEY (“South Africa”)
3. WEB OF SCIENCE
TS= (“motivational interviewing”
OR “behaviour change counselling”)
AND
TS= (“primary health care”
OR “community health services”)
AND
TS= (“South Africa”)
4. PsyclNFO
(“motivational interviewing”
OR “behavior change counseling”)
AND
(“primary health care”
OR “community health”)
AND
(“South Africa”)
5. CINAL
(“motivational interviewing”
OR “behavior change counselling”)
AND
(“primary health care”
OR “community-based care”)
AND
(“South Africa”)
6. GREY LITERATURE SEARCH
“Motivational interviewing” AND “South Africa” AND “primary health care”
“Adherence counselling” AND “South Africa” AND PHC
“Behavior change counselling” AND “Department of Health” AND “South Africa”
Appendix B: Prisma Flow Diagram
Figure A1.
PRISMA flow diagram.
Appendix C: Charting of Data

Table A1.
Characteristics of included studies.
| Author(s), Year | Study Design | Setting (Province) | Population / Cadre | Disease Focus | MI Intervention Description | Key Outcomes |
|---|---|---|---|---|---|---|
| Lundahl et al., 2013 | Systematic review (subset SA studies) | Multiple | PHC patients | HIV, NCDs | Brief MI-based counselling delivered by health workers | Improved adherence and engagement |
| Ticha et al., 2022 | Qualitative study | Limpopo | Professional nurses | TB/HIV | MI-informed adherence counselling perceptions | Identified skills gaps and training needs |
| Mwansa-Kambafwile et al., 2020 | Mixed methods | National | TB programme managers | TB | Counselling approaches aligned with MI principles | Reduced loss to follow-up when counselling strengthened |
| Malan et al., 2024 | Cross-sectional | Western Cape | PHC nurses | NCDs | Lifestyle counselling using MI-consistent techniques | Improved patient engagement; variable fidelity |
| Malan et al., 2024 | Qualitative | Gauteng | Health care providers | NCDs | Brief MI approaches in routine PHC | Feasibility, but time constraints noted |
| Da Silva et al., 2018 | Programme evaluation | National | WBOTs (CHWs) | General PHC | Community-based MI-informed counselling | Improved linkage and follow-up |
| Foster et al., 2024 | Qualitative | Eastern Cape | Community members | TB | Stigma-sensitive counselling aligned with MI principles | Improved trust and care-seeking |
| HIV Retention Study, 2025 | Cohort study | Gauteng | PLHIV | HIV | MI-based adherence and re-engagement counselling | Improved retention in care |
| HSRC, 2024 | Programme report | National | TB patients | TB | Behaviour changes counselling with MI elements | Reduced stigma-related disengagement |
| Parwati et al., 2021* | RCT | Comparable LMIC context | TB patients | TB | Structured MI for adherence support | Improved treatment completion |
| Bahri, 2025* | Narrative review | Global (incl. SA) | PHC patients | NCDs | MI for lifestyle modification | Improved self-management behaviours |
| Almansour et al., 2023* | RCT | Global | Adults with NCDs | NCDs | MI lifestyle counselling | Improved adherence and behaviour change |
| Thepwongsa et al., 2025* | Quasi-experimental | Global | PHC providers | Multiple | MI training for providers | Improved counselling competence |
| Mou et al., 2025* | Implementation study | Global | Health workers | Chronic disease | MI skills integration | Improved patient engagement |
| Hazelden Betty Ford Foundation, n.d.* | Evidence synthesis | Global | Multiple | Substance use, chronic disease | MI principles in brief counselling | Strong evidence for scalability |
| DoH, 2016 | Policy document | National | PHC workforce | HIV, TB, NCDs | Mandated counselling aligned with MI | Policy support; weak implementation |
| DoH, 2023 | Policy document | National | PHC services | HIV, TB, STIs | Person-centred counselling frameworks | Emphasis on retention and re-engagement |
| SANAC, 2023 | Strategic plan | National | Health system | HIV, TB | Psychosocial support aligned with MI | Policy-level endorsement |
| WHO, 2024 | Guideline | Global/SA | Health workers | HIV | Adherence counselling aligned with MI | Improved retention and adherence |
| UNAIDS, 2024 | Programme report | National | PLHIV | HIV | Behaviour changes counselling approaches | Supports MI-informed counselling |
| Bradshaw et al., 2022 | Epidemiological analysis | National | Population-level | Multiple | Behavioural determinants highlighted | Justifies the need for MI |
References
- Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. [CrossRef]
- Bradshaw, D., Pillay-van Wyk, V., Laubscher, R., Nojilana, B., Groenewald, P., Msemburi, W., & Dorrington, R. (2022). Trends in cause-of-death mortality in South Africa, 1997–2019. The Lancet Global Health, 10(7), e1091–e1101. [CrossRef]
- Büchter, R. B., Weise, A., & Pieper, D. (2020). Development, testing, and use of data extraction forms in systematic reviews: A review of methodological guidance. BMC Medical Research Methodology, 20, 259. [CrossRef]
- Da Silva, M., Schneider, H., & Okello, D. (2015). Evaluation of a training programme for primary care providers to offer brief behaviour change counselling on risk factors for non-communicable diseases in South Africa. BMC Family Practice 16. [CrossRef]
- Da Silva, M., Schneider, H., & Okello, D. (2018). The role of ward-based outreach teams in South Africa: An analysis of community-level health service delivery. BMC Health Services Research, 18, 307. [CrossRef]
- Department of Health. (2011). Re-engineering primary health care in South Africa. Pretoria: National Department of Health.
- Department of Health. (2013). National Mental Health Policy Framework and Strategic Plan 2013–2020. Pretoria: National Department of Health.
- Department of Health. (2013). Strategic plan for the prevention and control of non-communicable diseases 2013–2017. Pretoria: National Department of Health.
- Department of Health. (2016). Adherence guidelines for HIV, TB, and NCDs: Policy and service delivery guidelines for linkage to care, adherence to treatment, and retention in care. Pretoria: National Department of Health.
- Department of Health. (2017). National health policy: Towards universal health coverage. Pretoria: National Department of Health.
- Department of Health. (2023). National Strategic Plan for HIV, TB, and STIs 2023–2028. Pretoria: National Department of Health.
- Fonner, V. A., Kranzer, K., Kennedy, C. E., Penazzato, M., Butler, J., & Eakle, R. (2016). An integrative review of the efficacy of motivational interviewing in HIV management. AIDS Care 28(11), pp. 1413–1421. [CrossRef]
- Foster, I., Biewer, A., Vanqa, N., et al. (2024). “This is an illness. No one is supposed to be treated badly”: Community-based stigma assessments in South Africa to inform tuberculosis stigma intervention design. BMC Global & Public Health, 2, 41. [CrossRef]
- Hanmer, L., & Whittaker, S. (2020). Public health system challenges in the Free State, South Africa: a situation appraisal to inform health system strengthening. BMC Health Services Research 20. [CrossRef]
- Human Sciences Research Council. (2024). Tuberculosis stigma and community perceptions in South Africa. Pretoria: HSRC.
- Lund, C., Breen, A., Flisher, A. J., Kakuma, R., Corrigall, J., Joska, J. A., … Patel, V. (2011). Poverty and mental disorders in low- and middle-income countries: A systematic review. Social Science & Medicine, 71(3), 517–528. [CrossRef]
- Lundahl, B., Moleni, T., Burke, B. L., Butters, R., Tollefson, D., Butler, C., & Rollnick, S. (2013). Motivational interviewing in medical care settings: A systematic review and meta-analysis of randomised controlled trials. Patient Education and Counselling, 93(2), 157–168. [CrossRef]
- Malan, S., et al. (2024). Lifestyle counselling practices and gaps in South African primary health care services. African Journal of Primary Health Care & Family Medicine, 16(1), a731.
- Mayosi, B. M., Lawn, J. E., van Niekerk, A., Bradshaw, D., Karim, S. S. A., & Coovadia, H. M. (2012). Health in South Africa: Changes and challenges since 2009. The Lancet, 380(9858), 2029–2043. [CrossRef]
- Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change (3rd ed.). New York, NY: Guilford Press.
- Mwansa-Kambafwile, J. R. M., et al. (2020). Initial loss to follow-up of tuberculosis patients in South Africa: Perspectives of programme managers. BMC Public Health, 20, 622. [CrossRef]
- Ngene, N. C., Khaliq, O. P. & Moodley, J. (2023). Inequality in health care services in urban and rural settings in South Africa. African Journal of Reproductive Health 27(2), pp. 1–10. [CrossRef]
- Pitse, S. B. & Risenga, P. R. (2025). An integrated support model for lay health care workers to improve clients’ retention in HIV care. South African Family Practice 67(1). [CrossRef]
- Rollnick, M., Miller, S. & Butler, W. (2008). Motivational interviewing in primary care. British Journal of General Practice 58(552), pp. 101–108. [CrossRef]
- Sibeko, G. (March 17, 2025). Motivational Interviewing: A Pathway to Partnership in Care. International Consortium on Quality in Substance Use Disorders Treatment. https://www.icquality.org/knowledge-share/resources/2025-03/motivational-interviewing-pathway-partnership-care.
- Sorsdahl, K., Stein, D. J., Corrighall, J., Cuijpers, P., Smits, N., Naledi, T., & Myers, B. (2015). The efficacy of a blended motivational interviewing and problem-solving therapy intervention to reduce substance use among patients presenting for emergency services in South Africa: A randomised controlled trial. PubMed 25(11), p. 26576946. [CrossRef]
- South African National AIDS Council. (2023). National Strategic Plan for HIV, TB, and STIs 2023–2028. Pretoria: SANAC.
- Ticha, V., Bimerew, M., & Phetlhu, D. R. (2022). Nurses’ perceptions of tuberculosis with HIV adherence counselling skills in South Africa. Health SA Gesondheid, 27, a1859. [CrossRef]
- Tichá, V., Počíková, Z., Vytlačil, J. & Štěpánová, R. (2022). Real-world effectiveness and safety of fingolimod in patients with multiple sclerosis in the Czech Republic: results from core and extension parts of the GOLEMS study up to 48 months. BMC Neurology 22. [CrossRef]
- Tricco, A. C., et al. (2020). Assessing competence in health professionals’ use of motivational interviewing: A systematic review of training and supervision tools. Patient Education and Counseling, 103(3), 473–483. [CrossRef]
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., … Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. [CrossRef]
- UNAIDS. (2023). A framework for implementing integrated HIV and non-communicable disease care at primary health care facilities in Southern Africa. Southern African Journal of HIV Medicine, 24(1), a1290. [CrossRef]
- UNAIDS. (2024). Global HIV & AIDS statistics – 2024 fact sheet. Geneva: Joint United Nations Programme on HIV/AIDS.
- Vos, T., Lim, S. S., Abbafati, C., Abbas, K. M., Abbasi, M., Abbasifard, M., … Murray, C. J. L. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019. The Lancet, 396(10258), 1204–1222. [CrossRef]
- Weimann, A., & Petersen, I. (2017). Electronic health records in the cloud: Improving primary health care delivery in South Africa. Health Information Management Journal, 46(4), 179–186. [CrossRef]
- World Health Organisation. (2010). Global status report on noncommunicable diseases. Geneva: WHO.
- World Health Organisation. (2024). Adherence support: WHO guideline on HIV service delivery. Geneva: WHO.
- World Health Organisation. (2024). Global tuberculosis report 2024. Geneva: WHO.
- Zuma, K., et al. (2023). Pilot results of Masibambisane: Couples motivational interviewing with mobile breathalyzers to address unhealthy drinking and adherence to antiretroviral therapy in South Africa. JAMA, 330(18), 1763–1772. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



