1. Introduction
Achondroplasia is the most common form of short-limb dwarfism in humans, affecting more than 250,000 individuals worldwide. More than 95% of patients have a mutation in the gene for fibroblast growth factor receptor 3 (FGFR3) and more than 80% of these are new mutations [
1]. One of the most evident disorder associated with achondroplasia is short stature, which is evident at birth. [
2,
3]. This are reflected in the quality of life experienced by the patients with achondroplasia. They also had significantly lower self-teem values and significantly lower quality-of-life indices[
4].
Extended limb lengthening is a worldwide accepted treatment option for height enhancement [
5,
6,
7]. In tibia, bone lengthening has been performed through osteotomies and lateral or circular external fixators devices.
Related to complications for tibial lengthening, subluxation of the proximal tibiofibular joint has been observed [
8]. This difference is attributed to fibular distraction appeared to progress slower than the tibial distraction secondary to counter-tension exerted by the soft tissues[
9].
Additionally, the role of distraction - resisting forces in the restriction of knee and ankle range of motion and in axial deviation of the tibia is well established [
10]. Several studies have reported increased knee laxity and valgus angulation of the tibia due to proximal fibular migration [
9,
11].
We investigated the clinical and radiological effects when the fibula head is not fixed to the tibia during the tibial lengthening in achondroplasic patients.
2. Materials and Methods
This was a retrospective, unicenter study including all the achondroplasic patients (Apendix A.1) who were underwent bilateral tibial lengthening by distraction osteogenesis with use of a unilateral external fixation at our institution from 2007 to 2016 because of a short stature. We excluded patients with idiopathic short stature, secondary a another skeletal dysplasia or patients with limb length discrepancy
This study was conducted in accordance with the principles of the Declaration of Helsinki while a high level of confidentiality, in terms of the protection of personal data as required by Spanish Law (LOPD 3/2018), was also ensured. Written informed consent was obtained from all participants.
The lengthening procedure was performed with use of distraction osteogenesis by the senior author with more than thirty years of experience in this technique. First, the distal tibiofibular joint was fixed and stabilized with a palmer nail. The fixation of the distal tibiofibular joint was done to prevent heel valgus deformitythat results from proximal migration of the lateral malleolus during tibial lengthening.
After that, the osteotomy of the fibula between its middle and distal one-thirds was realized, and a segment of bone approximately one cm in length was excised to avoid early consolidation (Apendix A.2). Then, percutaneous tenotomy of the Achilles tendon proposed by Vilarrubias [
5],Aldegheri[
8] (with three incisions) was implemented. Postoperatively, the ankle was immobilized in a plaster cast-boot to maintain a 90º during the period of distraction.
Afterward 2 cortical-bone hydroxyapatite (5mm) screws were inserted in the proximal metaphysis of the tibia and 2 distally, in order to respect the growth plate. We made a subperiosteal (multiholes) osteotomy through an (1.5cm) anterior incision over the proximal part of the tibia. It is aligned to the long axis of the tibia, two centimetres distally to the proximal screws. Finally, the medial unilateral external fixation device was placed.
In the period of distraction, they can stand up and take small steps, but for long distances they move in wheelchair with leg extensions.
We started the distraction between four to five days after the surgery. A rate of one millimetre per day, 0.25mm every six hours by means of a unilateral external fixation. This rate was subsequently adjusted commensurate with the degree of ossification seen on the radiographs.
Removal of the external fixator was done when three cortices showed satisfactory corticalization on radiographs (Apendix A.3). All patients were evaluated clinically and radiographically every four weeks during the distraction and the consolidation period.
The parameters that were assessed to determine the outcome included the increase in length (in centimeters and as a percentage of the preoperative length) [
8] , the mean external fixation index (computed by dividing the number of days in the external fixator by the final regenerate length) [
12] and the presence of major complications.
The radiographs were evaluated with regard to four parameters: (1) mechanical axis deviation (MAD) (Figure 1), measured on long standing radiographs preoperatively and at the last follow-up; (2) the tibiofibular distraction difference (TFDD) (Figure 2), calculated by subtracting total fibular distraction from total tibial distraction at the end of the distraction period; (3) the proximal fibular migration (PFM) (Figure 3), comparing the position of the fibular head relative to the tibial plateau on the preoperative radiograph and the radiograph made at the end of the distraction period; (4) tibial angulation (Figure 4), calculated by comparing the orientation of the joint lines of the knee and ankle on preoperative radiographs with those on the postoperative radiographs [
11,
13]. Regarding knee deformity, a value of >8mm valgus MAD or a tibial valgus angulation of > 10º was assumed to by clinically important because a residual deformity of such magnitude might warrant surgical correction [
8].
Statistical analysis was carried out using the SPSS software for Windows (Version 16.0. Chicago, SPSS Inc). The (non-parametric) Mann-Whitney U test was used to compare differences on lengthening between genders. Also Mann-Whitney U test was used to compare the variables between the group which develop any complication and the group without complications.
Correlations have been analyzed calculating Pearson Correlation Coefficient. To analyze the relation between the percentages of tibial lengthening with other variables, we have categorized it in 4 groups, and compared the differences through Kruskall-Wallis non-parametric test.
3. Results
40 patients and 80 tibial segments were evaluated. The mean age at the time of the surgery was 11.97 years old (range, 9.30-16.40 years). 25 were male and 15 were female. The mean duration of follow-up was 9.41 years (range, 3.10 to 13.9 years).
The mean amount of lengthening was 15.03 cm (SD 2.25) (range, 11.40 to 18.50) and the mean percentage lengthening was 84.64% (range, 62.21% to 138%) of the original tibial length. The mean external fixation index (EFI) was 19.78 days/cm (SD 4.25) (range, 13.9 to 31.11) with a mean preoperatively mechanical axis deviation (MAD) of 11.91 mm (SD 17.36) (range, -22.45 to 59.74) and 8.2mm (SD 15,25) (range, -21.91 to 49.88) at the final follow-up. According to these results, we observed a total of 53 genu varus and 18 of valgus with only 10 of these with > 10 mm at the final follow-up.
The mean tibiofibular distraction difference (TFDD) was 3.80 cm (SD 1.43) (range, 1.40 to 7.47). The mean proximal fibular migration (PFM) was 19.09 mm (SD 4.57) (range, 10.48 to 29.37) and the mean preoperatively amount of tibial angulation was -6.4º (SD 8.80º) (range, -23.58 to 15.24º) and 7.16º (SD 7.30º) (range, -12.9 to 28.6) at the final follow-up. The tibia was found in varus in 59 segments and in valgus in 15 segments preoperatively.
At the final follow-up we found 1 tibia in varus and 75 in valgus. In the valgus deviation, 26 had more than 10º without association between the proximal fibular subluxation and gender (p>0.05).
On clinical examination at the time of the latest follow-up no peroneal nerve abnormality was found. Any patient reported swelling or tenderness at the proximal tibiofibular joint. No patient presented a subjective sense of instability at the knee joint during walking or running.
Mayor complications during lengthening appeared in 23 of the 80 segments (28.7%). The premature consolidation of the fibula occurred in 2 cases; we resolved them with another osteotomy and new excision of bone. In 12 cases a valgus deviation needed a corrective osteotomy at the apex of the deformity with internal fixation or keeping the external fixator device.
A combination of valgus and torsional deviation showed up in 4 segments. All of this required a osteotomy at the apex of the deformity and internal fixation. A deviation in varus occurred in one patient, who presented a varus deviation preoperatively and it didn’t improve with the lengthening. We corrected it with a osteotomy and internal fixation. We observed a fracture post lengthening after a trauma, it healed with a plaster cast. Limited of knee extension was noted commonly during the lengthening procedure [
10], we had 2 segments with this problem, whom we can remedied with a long leg cast in extension of the knee. It had resolved completely at the end of the follow-up period. Equinus contracture appeared in 6 segments, only in 2 cases we needed a new percutaneous tenotomy. In the other 4 cases we resolved them with a boot cast. A delay in consolidation was recorded in 2 occasions; they required a changing of the external fixation device to heal.
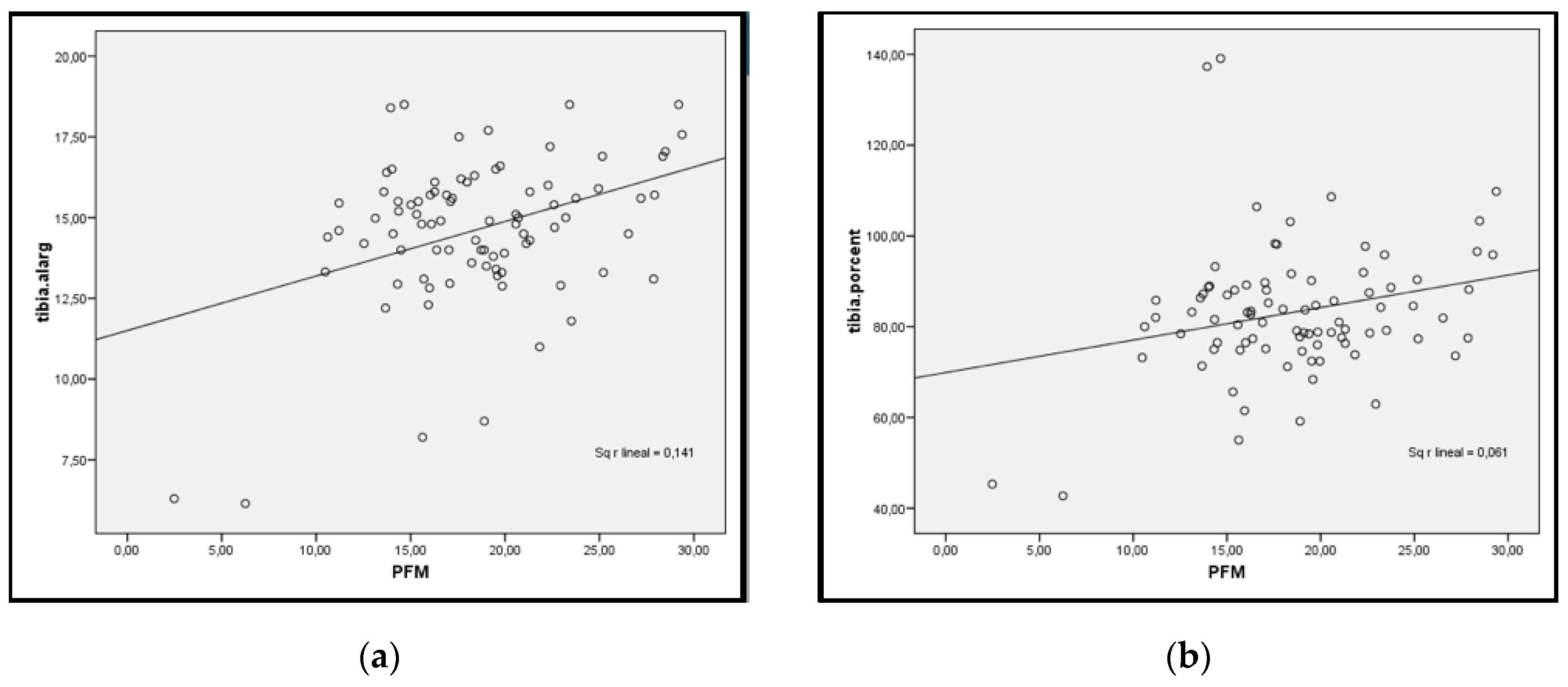
When we analysed the differenceaccording the magnitude of lengthening and we found that the degree of proximal fibular migration was linearly correlated with the amount of tibial lengthening. (
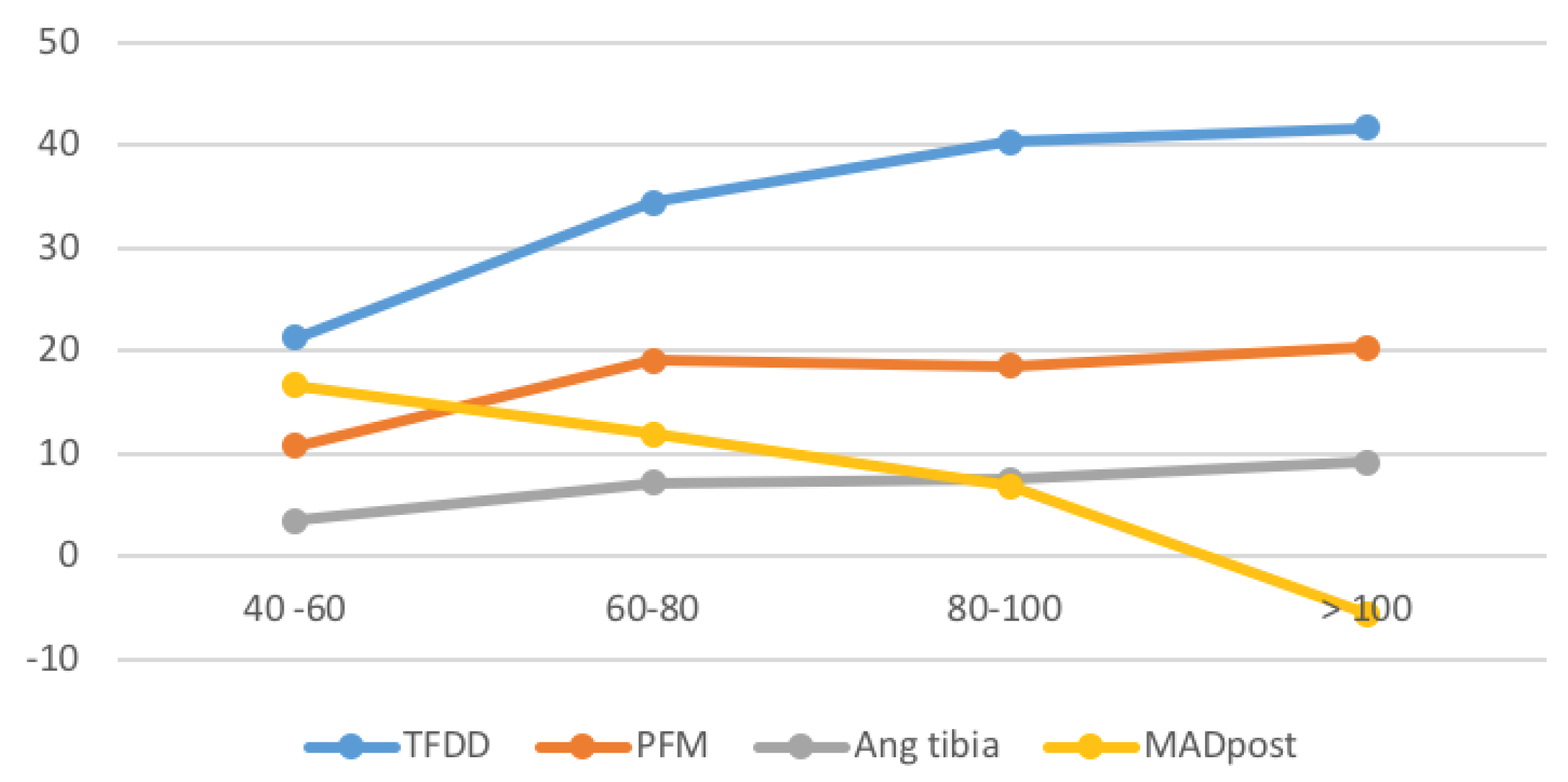
Figure 5). The tibiofibular distraction difference, proximal fibular migration and tibial angulation were found to increase with the increase in the percentage of lengthening. In reference to the mechanical axis deviation when we see the graph, it showed a rapid decrease (valgus change) beyond 100 % lengthening. In other words the risk to present a valgus is higher above than 100% of tibial lengthening. (
Figure 6). When we analyzed the radiological parameters comparing the different groups of percentage of lengthening, only the tibiofibular distraction difference was significantly different according to percentage lengthening (p<0.05) (
Table 1). Then we applied the multiple comparison correction, and it showed a linearly correlation between the tibiofibular distraction difference and the percentage of lengthening. (
Figure 7).
The summary of the comparison according to postoperative MAD is in
Table 2. Here we observed the appearance of postoperative valgus of the knee. Valgus of the knee (valgus change of MAD) increased with the increased lengthening. The amount of elongation differed significantly among the groups with different postoperative alignment (p<0.05). The percentage of lengthening presented statistical significant difference in relation with the postoperative mechanical axial deviation (p<0.05). However the proximal fibular migration was not associated with the valgus deformity of the knee (p> 0.05).
At the end, if we reviewed the relation between our parameters and the presence of major complications we can concluded that the magnitude of fibula resection and the mechanical axis deviation were associated with the presence of complications (p<0.05) (
Table 3). In contrast, the proximal fibular migration and the magnitude of lengthening were not.
4. Discussion
In the present study, compared to other series in which patients were affected with different skeletal dysplasias, we have included patients with achondroplasia, whom have a specific patterns in the lower limbs. [
8,
9,
11,
13]We review the clinical and radiological effects when the fibula head is not fixed to the tibia during the tibial lengthening.
The mediolateral instability and the fibular overgrowth may be presented in patients with achondroplasia, and they could improve when the peroneal head pulled down during distraction in order to obtain a normal tibiofibular relationship [
11].
According to Hatzokos et al, our study showed that the extent of the proximal fibular migration was directly related with the amount of tibial lengthening (figure 5 and 6). Like in our study, other authors observed fibular lengthening appeared to progress more slowly than did tibial lengthening, and there was less fibular lengthening overall [
9,
11]. We found that the tibiofibular distance difference increased proportionally to the increase of lengthening. We observed statistically differences in relation with the percentage of lengthening (p<0,05) and linearly correlation between the tibiofibular distraction difference and the percentage of elongation (p< 0.05). This can be explained by the fact that the fibular lengthening was not caused by a rigid external fixator directly attached to the bone but evolved indirectly through the tension exerted by the soft tissues, mainly by the intact distal portion of the interosseous membrane [
9].
An increase of valgus angulation related to the elongation percentage of the tibia has been reported with a rapid increase of tibial valgus angulation beyond 50% lengthening [
11] And it found that the mechanical axis deviation increased rapidly in the midrange of 25-50% of lengthening and then slowed down when the lengthening percentage increased more than 50%[
13]. In our study the trends in the magnitude of tibial angulation and the mechanical axis deviation as a function of percentage tibial lengthening was different. We observed a tibial angulation increased steadily with the increases of the lengthening. Instead the MAD, only showed a rapidly decrease (change to valgus) beyond 100% lengthening.
Although the proximal migration of the fibula was associated with a valgus change in the mechanical axis deviation [
13], our study did not. The only relation that we found with the variation of the mechanical axis deviation during the tibial lengthening was with the amount of elongation. We observed different amount of lengthening in the patients who presented a valgus deformity of the knee. Hence, limiting the lengthening to <100% will minimize the number of valgus deformity of the knee joint.
It is well accepted in the literature that associated problems increase proportionally as the percentage of lengthening increases [
14,
15]. Paley mentioned that the soft tissues in patients with achondroplasia tolerate lengthening with fewer problems, perhaps because the muscle lengths exceed the bone lengths before lengthening [
10]. In our study we didn’t observe difference of amount of lengthening in the patients who presented complication
The mechanical axis deviation was associated with the presence of major complications. In eight segments a valgus deviation and in four segments a valgus deviation had associated torsional deviation. All required a tibial osteotomy at the apex of the deformity. When the valgus was alone, sometimes is possible to reduce the deformity with the external fixator device. If it’s not possible, an internal fixation was used. As we have referred before, a good way to control the mechanical axis deviation, in limiting the elongation to < 100% of the initial length of the tibia.
Premature consolidation of the fibular osteotomy site is a problem that can required a surgical treatment during the tibial lengthening. This was why we included the premature consolidation of the fibula inside de major complications. Paley considered it an obstacle [
15], nevertheless Aldegheri assumed it like a complication. [
8]. We observed a relation between the fibula resection and the presence of complications. In all the segments that the premature consolidation appeared was needed a new osteotomy of the fibula. Kim et al, observed 10 premature consolidation of the fibula among 120 tibial segments. In this series the osteotomy was performed without the excision of the fibula. Hence, the amount of resection of the fibula is important to prevent the premature consolidation of the fibula[
13].
Some authors have reported the presence of complications associated with the proximal fibular migration [
12,
13]. In our series, we didn’t find it. Our patients, didn’t present abnormal mobility of the fibular head, swelling or tenderness at the proximal tibiofibular joint or subjective sense of instability at the knee joint during walking or running. In agreement with other authors [
8,
9], subluxation of the fibula was a radiographic observation that did not produce clinical symptoms or signs. In the case of patients with achondroplasia we think that could normalize the relation between the head of the fibula and the tibia.
5. Conclusions
In summary, we found that the proximal fibular migration is common in patients undergoing bilateral tibial lengthening using unilateral external fixation. However, no valgus deformity, angulation of the tibia or presence of major complications was found in relation with the proximal fibular migration. These findings indicate that the fixation of the proximal tibiofibular joint is not required in bilateral tibial lengthening with unilateral external fixation in achondroplasic patients.
Funding
The authors did not receive grants or outside funding in support of their research or preparation of this manuscript. They did not receive payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation educational institution, or other charitable or nonprofit organization with which the authors are affiliated or associated.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data acquired from the patients who participated in this research is private and it is contained at the Hospital Universitari Dexeus patient’s database.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MAD |
Mechanical axis deviation |
| TFDD |
Tibiofibular distraction difference |
| MADpost |
Postoperative mechanical axis deviation |
| PFM |
Proximal fibular migration |
Appendix A
Appendix A.1: Achondroplasic Patient Before Undergoing Tibial Lengthening Procedure
Appendix A.2: Achondroplasic Patient Undergoing Tibial Lengthening with the Use of an External Fixation Device to Perform Distraction Osteogenesis and Growth
Appendix A.3: Achondroplasic Patient Who Has Finalized the Tibial Lengthening Procedure Successfully
References
- Horton, WA; Hall, JG; Hecht, JT. Achondroplasia. Lancet Lond Engl. 2007, 370(9582), 162–72. [Google Scholar] [CrossRef] [PubMed]
- Shirley, ED; Ain, MC. Achondroplasia: manifestations and treatment. J Am AcadOrthop Surg. 2009, 17(4), 231–41. [Google Scholar] [CrossRef] [PubMed]
- Bailey, JA. Orthopaedic aspects of achondroplasia. J Bone Joint Surg Am. 1970, 52(7), 1285–301. [Google Scholar] [CrossRef] [PubMed]
- Gollust, SE; Thompson, RE; Gooding, HC; Biesecker, BB. Living with achondroplasia: attitudes toward population screening and correlation with quality of life. PrenatDiagn 2003, 23(12), 1003–8. [Google Scholar] [CrossRef] [PubMed]
- Vilarrubias, JM; Ginebreda, I; Jimeno, E. Lengthening of the lower limbs and correction of lumbar hyperlordosis in achondroplasia. Clin Orthop. 1990, (250), 143–9. [Google Scholar] [CrossRef]
- Paley, D. Current techniques of limb lengthening. J Pediatr Orthop. 1988, 8(1), 73–92. [Google Scholar] [CrossRef] [PubMed]
- Aldegheri, R; Trivella, G; Renzi-Brivio, L; Tessari, G; Agostini, S; Lavini, F. Lengthening of the lower limbs in achondroplastic patients. A comparative study of four techniques. J Bone Joint Surg Br. 1988, 70(1), 69–73. [Google Scholar] [CrossRef] [PubMed]
- Aldegheri, R. Distraction osteogenesis for lengthening of the tibia in patients who have limb-length discrepancy or short stature. J Bone Joint Surg Am. 1999, 81(5), 624–34. [Google Scholar] [CrossRef] [PubMed]
- Hatzokos, I; Drakou, A; Christodoulou, A; Terzidis, I; Pournaras, J. Inferior subluxation of the fibular head following tibial lengthening with a unilateral external fixator. J Bone Jt Surg-Am 2004, 86(7), 1491–6. [Google Scholar] [CrossRef] [PubMed]
- Paley, D. Current techniques of limb lengthening. J Pediatr Orthop. 1988, 8(1), 73–92. [Google Scholar] [CrossRef] [PubMed]
- Shyam, AK; Song, H-R; An, H; Isaac, D; Shetty, GM; Lee, SH. The Effect of Distraction-Resisting Forces on the Tibia During Distraction Osteogenesis. J Bone Jt Surg-Am 2009, 91(7), 1671–82. [Google Scholar] [CrossRef] [PubMed]
- Isaac, D; Fernandez, H; Song, H-R; Kim, T-Y; Shyam, AK; Lee, S-H; et al. Callus patterns in femur lengthening using a monolateral external fixator. Skeletal Radiol. 2008, 37(4), 329–34. [Google Scholar] [CrossRef] [PubMed]
- Kim, S-J; Agashe, MV; Song, S-H; Song, H-R. Fibula-related complications during bilateral tibial lengthening: 60 patients followed for mean 5 years. Acta Orthop. 2012, 83(3), 271–5. [Google Scholar] [CrossRef] [PubMed]
- Antoci, V; Ono, CM; Antoci, V; Raney, EM. Bone lengthening in children: how to predict the complications rate and complexity? J Pediatr Orthop. 2006, 26(5), 634–40. [Google Scholar] [CrossRef] [PubMed]
- Paley, D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop. 1990, (250), 81–104. [Google Scholar] [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).