Submitted:
04 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
Background: Peripheral artery disease (PAD) progressing to chronic limb-threatening ischemia (CLTI) is associated with high morbidity and limb loss. Diabetes mellitus (DM) is a major modifier of disease distribution and outcomes. The Bollinger score, GLASS classification, and WIfI staging are complementary tools for assessing anatomical burden and limb threat. The aim of this study was to analyze the associations between these scoring systems in diabetic CLTI, with Bollinger and GLASS assessed on digital subtraction angiography, and with a focus on segmental infra-popliteal versus global anatomical evaluation. Methods: This single-center, retrospective observational study included 136 patients with CLTI who underwent endovascular revascularization between May 2021 and May 2023. Baseline demographics and comorbidities, angiographic severity, WIfI stage, Bollinger score (whole leg; above- and below-knee), GLASS staging (global; femoropopliteal/infra-popliteal segments), and outcomes (technical success, bypass conversion, major amputation, and one-year mortality) were analyzed. Results: Patients were classified into a diabetic group (DM; n = 85) and a non-diabetic group (NDM; n = 51). Diabetic patients more frequently presented with infra-inguinal stenoses >50% (55.3% vs. 35.3%, p = 0.024) but fewer complete occlusions (83.5% vs. 96.1%, p = 0.028). WIfI stage 1 tended to be more frequent in diabetics (54.1% vs. 33.3%, p ≈ 0.08). Bollinger scores were lower in the DM group for the whole leg (30.07 ± 16.34 vs. 36.78 ± 16.09, p = 0.018) and for the below-knee segment (20.53 ± 15.88 vs. 26.86 ± 13.93, p = 0.015). Conclusions: In this cohort, diabetic patients with CLTI exhibited a distinct distal angiographic pattern characterized by prevalent infra-popliteal stenoses and lower additive Bollinger scores. Segmental infra-popliteal assessment showed stronger clinical relevance than global evaluation, with below-knee Bollinger scores and GLASS infra-popliteal stages demonstrating the closest association with WIfI severity. These findings highlight the dominant role of distal disease in diabetic arteriopathy and support a segment-focused approach to endovascular planning.
Keywords:
chronic limb-threatening ischemia
; peripheral arterial disease
; diabetes mellitus
; endovascular revascularization
; Bollinger score
; GLASS classification
; WIfI staging
Abstract
Background: Peripheral artery disease (PAD) progressing to chronic limb-threatening ischemia (CLTI) is associated with high morbidity and limb loss. Diabetes mellitus (DM) is a major modifier of disease distribution and outcomes. The Bollinger score, GLASS classification, and WIfI staging are complementary tools for assessing anatomical burden and limb threat. The aim of this study was to analyze the associations between these scoring systems in diabetic CLTI, with Bollinger and GLASS assessed on digital subtraction angiography, and with a focus on segmental infra-popliteal versus global anatomical evaluation. Methods: This single-center, retrospective observational study included 136 patients with CLTI who underwent endovascular revascularization between May 2021 and May 2023. Baseline demographics and comorbidities, angiographic severity, WIfI stage, Bollinger score (whole leg; above- and below-knee), GLASS staging (global; femoropopliteal/infra-popliteal segments), and outcomes (technical success, bypass conversion, major amputation, and one-year mortality) were analyzed. Results: Patients were classified into a diabetic group (DM; n = 85) and a non-diabetic group (NDM; n = 51). Diabetic patients more frequently presented with infra-inguinal stenoses >50% (55.3% vs. 35.3%, p = 0.024) but fewer complete occlusions (83.5% vs. 96.1%, p = 0.028). WIfI stage 1 tended to be more frequent in diabetics (54.1% vs. 33.3%, p ≈ 0.08). Bollinger scores were lower in the DM group for the whole leg (30.07 ± 16.34 vs. 36.78 ± 16.09, p = 0.018) and for the below-knee segment (20.53 ± 15.88 vs. 26.86 ± 13.93, p = 0.015). Conclusions: In this cohort, diabetic patients with CLTI exhibited a distinct distal angiographic pattern characterized by prevalent infra-popliteal stenoses and lower additive Bollinger scores. Segmental infra-popliteal assessment showed stronger clinical relevance than global evaluation, with below-knee Bollinger scores and GLASS infra-popliteal stages demonstrating the closest association with WIfI severity. These findings highlight the dominant role of distal disease in diabetic arteriopathy and support a segment-focused approach to endovascular planning.
1. Introduction
Peripheral artery disease (PAD) progressing to chronic limb-threatening ischemia (CLTI) is associated with substantial morbidity, limb loss, and mortality, particularly in the presence of diabetes mellitus (DM). Over the last two decades, endovascular treatment has become the default first-line strategy for most infra-inguinal lesions, supported by contemporary guidelines and randomized evidence favoring less peri-procedural risk compared with open bypass in appropriately selected patients, particularly those with focal or anatomically accessible lesions, significant comorbidity burdens limiting surgical options, and clinical presentations in which limb perfusion can be effectively restored through minimally invasive revascularization [1,2,3,4]. While percutaneous transluminal angioplasty remains the backbone of infra-inguinal endovascular treatment, adjunctive stenting is frequently employed for complex lesions, flow-limiting dissection, residual stenosis, or to rescue suboptimal angioplasty.
Diabetes mellitus profoundly reshapes PAD biology and anatomy. In these patients, arteriopathy is characterized by distal, multi-segmental, and frequently calcific disease, impaired collateralization, and microcirculatory dysfunction (versus non-diabetics). This phenotype translates into more severe infra-popliteal involvement, higher wound-related risk, and a tendency toward stenotic—rather than long occlusive—lesions in the distal bed. Contemporary translational and clinical literature highlights medial arterial calcification, microangiopathy, and endothelial dysfunction as mechanistic drivers of this pattern and as potential determinants of endovascular feasibility, recoil, and durability [5,6,7]. These differences justify segment-specific assessment and careful integration of clinical and anatomical staging when planning revascularization in CLTI, especially in patients with diabetes mellitus.
To standardize decision-making and outcome prediction, complementary scoring systems are recommended. The Society for Vascular Surgery WIfI classification grades Wound, Ischemia, and Fi (foot infection) to estimate amputation risk and the expected benefit of revascularization; higher grades correlate with delayed wound healing, increased risk of major amputation, and mortality [8,9]. The Bollinger score offers a semi-quantitative, segmental measure of atherosclerotic burden across the lower-limb arterial tree and has been used in trials/registries to relate angiographic severity to outcomes [10,11,12]. The Global Limb Anatomic Staging System (GLASS) synthesizes femoropopliteal (FP) and infra-popliteal (IP) complexity to anticipate crossing difficulty and technical durability and to guide “endovascular-first” vs hybrid/surgical strategies in CLTI [1,13,14]. Together, WIfI (clinical limb threat), Bollinger (anatomic burden), and GLASS (revascularization complexity) form a pragmatic, complementary framework that can align bedside urgency with angiographic feasibility.
From a revascularization-planning perspective, the literature converges on several lesion- and patient-level determinants of outcome: stenosis vs occlusion, lesion length and multiplicity, multilevel involvement and runoff, infra-popliteal dominance, and co-morbidities (notably DM and CKD). These features influence technical success, patency, limb salvage, and the need for target lesion revascularization and should be documented with uniform criteria [1,4,15]. Standardized reporting and consistent use of objective hemodynamic and clinical endpoints enable valid comparisons across techniques and centers and are increasingly emphasized in modern CLTI pathways [15].
Despite this framework, comparative data contrasting DM versus NDM CLTI phenotypes using all three tools—WIfI, Bollinger, and GLASS—remain limited in Eastern European populations, where access patterns, referral timing, and risk-factor profiles may differ from those reported in Western cohorts. Addressing this gap has practical relevance for endovascular planning, resource allocation, and limb-preservation pathways.
Therefore, we aimed to analyze the particularities of diabetic patients with CLTI undergoing endovascular revascularization and to quantify the relationships among WIfI stage, Bollinger score (whole leg; above- and below-knee), and GLASS classification (global; femoropopliteal and infra-popliteal segments), with particular emphasis on segmental infra-popliteal assessment in comparison with global limb evaluation.
2. Materials and Methods
2.1. Study Design and Patient Population
This retrospective, observational, single-center study was conducted in the Vascular Surgery Clinic of “Sf. Spiridon” Emergency Hospital, Iași, Romania. We included patients aged ≥18 years with PAD and CLTI (defined as ischemic rest pain lasting >2 weeks, with or without tissue loss) who underwent endovascular revascularization between May 2021 and May 2023.
Patients were divided into a diabetic (DM) and a non-diabetic (NDM) group. Clinical and biological characteristics, angiographic severity, and outcomes were compared between groups. In addition, we analyzed the relationships among WIfI stage, Bollinger score (whole leg; above- and below-knee), and GLASS classification (global; femoropopliteal and infra-popliteal segments) to identify segment-specific patterns characteristic of diabetic CLTI, thereby clarifying the alignment between clinical limb threat, anatomic disease burden, and procedural complexity in a real-world Eastern European cohort.
Type DM was defined based on documented medical history, ongoing antidiabetic therapy, and/or HbA1c ≥6.5% recorded at admission or during hospitalization. The duration of diabetes and the type of antidiabetic therapy (oral agents, insulin) were also recorded when available. The exclusion criteria were acute ischemia; aorto-iliac disease; recent bypass; no indication for revascularization; Raynaud’s; aortic dissection; inability to provide informed consent (e.g., unconscious or intubated patients).
2.2. Clinical and Paraclinical Data Collection
We analyzed the following parameters: 1. Baseline demographics/comorbidities; 2. Angiographic severity (angiography, computer tomography angiography); 3. The scores: WIfI stage (Table 1), Bollinger score (whole leg; above/below knee; Table 2), GLASS staging (global; FP/IP segments; Table 3). Data collection was performed in a standardized manner at the time of inclusion, integrating information obtained from medical history, physical examination, laboratory data, imaging studies, and the hospital electronic medical record system.
Primary endpoint included technical success, defined as restoration of inline flow to the foot with less than 30% residual stenosis in the treated segment on completion angiography. Secondary endpoint included conversion to bypass surgery, major amputation, and one year mortality. Conversion to bypass surgery and mortality were retrospectively assessed using institutional medical records until December 2024, based on a predefined observational cutoff chosen by the investigators. Mortality data were limited to events recorded within our hospital database completed by telephonic interview with general practician.
2.3. Scoring Systems
The WIfI classification is designed for patients presenting with ischemic rest pain localized to the forefoot and supported by hemodynamic testing (ankle–brachial index <0.40, ankle pressure <50 mmHg, toe pressure <30 mmHg, or TcPO2 <39 mmHg); diabetic foot ulcers; nonhealing foot or leg ulcers persisting for more than two weeks; or any degree of foot or leg gangrene. Each component score (W, I, FI) is subsequently combined to estimate the 1-year amputation risk (Table 1) [8].
WIfI staging was calculated retrospectively for each patient of our study by reviewing individual medical records and operative charts. Hemodynamic parameters (ankle–brachial index, ankle pressure, toe pressure, and/or transcutaneous oxygen pressure), when available, were used exclusively to assign the ischemia component in accordance with guideline-recommended thresholds. Because these measurements were not systematically recorded in a standardized numeric format across all patients, raw hemodynamic values were not extracted or analyzed as independent variables, and no separate table of ABI or TcPO₂ values was generated.
The final WIfI stage was entered into a dedicated database for analysis.
The Bollinger score assigns points based on four severity categories: complete occlusion, stenosis >50%, stenosis ≤50% but >25%, and plaques impinging ≤25%. Severity scores are then summed within each arterial segment. To capture lesion distribution, scores are calculated separately for the whole limb, the above-knee segment, and the below-knee segment. This additive approach reflects both the extent and multiplicity of atherosclerotic disease within each anatomical region (Table 2) [10].
GLASS classifies limb complexity by grading the femoropopliteal and infra-popliteal segments from 0 to 4 based on lesion severity. The two segmental grades are then combined to generate an overall limb stage (Stage I–III), which correlates with expected technical success and patency after endovascular revascularization.
Stage I means mild complexity and is associated with <10% technical failure and >70% chance of limb patency at 12 months. Stage II means medium complexity and is associated with <20% technical failure and a 50–70% chance of limb patency at 12 months.
Stage III means high complexity and is associated with >20% technical failure and <50% chance of limb patency at 12 months. Stages I and II predict a patency of >70%, respectively, with 50–70% thus defining patients who after an endovascular procedure should not return to the clinic for treatment on the same limb for a period of at least one year, Stage III predicts a patency of <50%; Patients categorized with this stage have ahigh chance of returning for repeat procedures on the affected limb (Table 3) [6].
2.4. Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality using histogram inspection, Q–Q plots, and the Shapiro–Wilk test. Normally distributed variables are presented as mean ± standard deviation (SD), whereas non-normally distributed variables are reported as median and interquartile range (IQR).
Comparisons between diabetic and non-diabetic patients were performed using the independent-samples t-test for normally distributed variables and the Mann–Whitney U test for skewed distributions. Categorical variables were summarized as absolute counts and percentages, and group comparisons were carried out using the chi-squared (χ²) test or Fisher’s exact test when expected frequencies were below 5.
Correlations between angiographic scoring systems—including Bollinger global and segmental scores (femoropopliteal, infra-popliteal), GLASS femoropopliteal/infra-popliteal stages, and WIfI ischemia grade—were evaluated using Spearman’s rank correlation coefficient (ρ). Correlation strength was interpreted according to standard thresholds: weak (<0.30), moderate (0.30–0.59), and strong (≥0.60). In this dataset, the global Bollinger Score demonstrated moderate correlation with GLASS IP stage (ρ ≈ 0.41–0.48) and weaker correlation with FP disease burden (ρ ≈ 0.20–0.30). The strongest association was observed between infra-popliteal Bollinger burden and WIfI ischemia grade (ρ ≈ 0.50 among patients in DM group).
Weighted Kappa (κw) was used to quantify agreement between angiographic scoring systems. Kappa was used to assess the degree of concordance between ordinal scales for measuring infra-popliteal disease severity. The global κw coefficient was 0.558 for the entire cohort, indicating moderate agreement between Bollinger IP burden and GLASS IP staging. Subgroup analyses showed κw = 0.625 in the DM group (substantial agreement) and κw = 0.485 in the NDM group (moderate agreement). Segmental analysis showed that concordance was higher in the infra-popliteal region compared to the femoropopliteal axis, consistent with the anatomical distribution of disease severity.
Where applicable, logistic regression was performed to evaluate predictors of technical success and limb-related clinical outcomes. Variables with p < 0.10 in univariate testing and those considered clinically important were included in multivariable models.
A two-tailed p-value <0.05 was considered statistically significant. Given the exploratory nature of several anatomical and subgroup comparisons, p-values between 0.05 and 0.10 were interpreted as indicating a statistical trend.
3. Results
A total of 136 patients were included, of whom 62.5% (n=85) had DM. Baseline characteristics of patients included in the study are presented in Table 4. The two groups were comparable in age and sex distribution, with a mean age of approximately 70 years in both (p=0.737). However, urban residence was significantly more common among diabetics (72.9% vs. 49.0%, p=0.005), suggesting potential lifestyle and socioeconomic contributors to disease patterns.
While not statistically significant, hypertension (85.9% vs. 74.5%), chronic kidney disease (18.8% vs. 13.7%), and prior stroke (11.9% vs. 3.9%) were more prevalent among the DM group, consistent with the systemic comorbidity burden typically associated with diabetes mellitus. These comorbidities likely contribute to a more complex vascular phenotype and may influence endovascular planning and outcomes.
3.1. Angiographic Severity and WIfI Stages
Angiographic severity according to WIfI stages is presented in Table 5. Significant differences emerged in lesion type: patients in the DM group exhibited more frequent stenoses >50% (55.3% vs. 35.3%, p=0.024), but fewer complete occlusions (83.5% vs. 96.1%, p=0.028). This pattern reflects the diffuse, multi-segmental nature of diabetic arteriopathy, in which extensive calcific narrowing may coexist with patent segments rather than long total occlusions.
WIfI stage 1 occurred more often among DM group (54.1% vs. 33.3%, p≈0.08), a trend that may reflect earlier recognition of ischemic symptoms or different limb-threat profiles. In DM group, neuropathy often masks ischemic pain, leading to a deceptively mild clinical presentation in which small, superficial ulcers receive a low WIfI wound score, despite the presence of advanced infra-popliteal disease.
The correlation heatmap between WIfI stage, Bollinger whole-leg score, and global GLASS stage is presented in Figure 1. The strongest association was observed between Bollinger and GLASS (ρ = 0.643), with weaker but significant correlations between WIfI and the two angiographic scores.
In the infrapopliteal analysis, Bollinger BK and GLASS-IP demonstrated a strong correlation (ρ = 0.713), whereas their associations with WIfI stage remained modest (ρ = 0.245–0.266).
The spatial distribution of disease confirmed that correlations between clinical WIfI grade and angiographic burden were strongest in infra-popliteal segments, particularly among patients in DM group (Figure 2).
3.2. Bollinger and GLASS Scores
Bollinger scoring revealed that patients in the DM group had lower total and below-knee scores, while above-knee scores were similar (Table 6). This suggests that diabetic atherosclerosis, despite being extensive, may translate into a lower additive angiographic occlusive burden due to its predominantly distal and calcific stenotic pattern.
GLASS global staging tended to be higher in the DM group (stage 2–3 more frequently) though differences were not statistically significant.
The distribution of Bollinger scores, confirms a downward shift in diabetics across all segments, and the close relationship between below-knee Bollinger and GLASS infra-popliteal (IP) stages. This finding reinforces that infra-popliteal disease drives clinical severity in diabetic CLTI.
3.3. Outcomes of Revascularization
Overall technical success was achieved in 74.3% of procedures, with no difference between DM and NDM groups (75.3% vs. 72.5%, NS) – Table 7. Bypass conversion rates were identical (11.8% in both), while major amputation occurred more often in the DM group (9.4% vs. 3.9%), though without statistical significance. Mortality during hospitalization was low in both groups (3.5% vs. 2.0%). These results highlight that diabetes does not significantly affect immediate technical success, but the clinical trajectory post-revascularization may remain less favorable, possibly due to infection, wound healing, and microcirculatory impairment.
3.4. Correlations Between Scoring Systems
Correlations Between Scoring Systems are presented in Table 8. There were strong and significant correlations between Bollinger–GLASS (ρ=0.643, p<0.001), WIfI–Bollinger (ρ=0.290, p<0.001), WIfI–GLASS (ρ=0.173, p=0.044). At the segmental level, the correlation was strongest below the knee, particularly between Bollinger-IP and GLASS-IP (ρ=0.713, p<0.001). This underscores the key role of the infra-popliteal compartment in determining both clinical severity and anatomical complexity, especially in DM group.
To facilitate an integrated interpretation of the relationships among clinical limb threat, anatomical disease burden, and revascularization complexity, a tree diagram was constructed (Figure 3). This diagram does not represent a statistical model or predictive hierarchy, but rather a conceptual visualization summarizing the strength and direction of associations observed in the correlation and agreement analyses
Specifically, we illustrated how WIfI clinical staging, Bollinger anatomical scoring, and GLASS anatomic–technical classification interrelates, emphasizing the progressive convergence of these systems at the infra-popliteal (below-knee) level. Branch proximity reflects the relative strength of correlations and weighted agreement, with shorter distances indicating stronger associations. The diagram highlights that infra-popliteal Bollinger burden and GLASS-IP staging cluster most closely, consistent with the strong Spearman correlation (ρ = 0.713) and moderate-to-substantial weighted agreement observed in the DM group. In contrast, femoropopliteal GLASS staging shows a weaker association with WIfI clinical severity, underscoring the limited capacity of proximal anatomy alone to reflect limb threat.
Weighted Kappa coefficients between the investigated scores (overall and stratified by diabetes status is presented in Table 9. No significant agreement was found between GLASS FP and GLASS IP, or between GLASS FP and WIfI. A weak agreement was observed between GLASS IP and WIfI in the whole cohort (0.183), rising to acceptable in diabetics (0.392).
Weighted Kappa analysis confirmed moderate overall agreement (κ=0.558) between qualitative Bollinger score and GLASS stages, improving to substantial in the DM group (κ=0.625) and decreasing slightly in the NDM group (κ=0.485). No significant agreement was found between GLASS FP and GLASS IP, or between GLASS FP and WIfI. A weak agreement was observed between GLASS IP and WIfI in the whole cohort (0.183), rising to an acceptable level in the DM group (0.392).
These results suggest that, in the DM group, both scores describe a similar underlying anatomical burden dominated by distal multisegmented disease.
3.5. Associations with Technical Success Rate
Further analysis explored predictors of revascularization outcomes. The presence of plaques (<25%) was associated with a significantly higher success rate (OR=0.33, p=0.006), driven primarily by the NDM group (p=0.012).
The plaques with non-significant stenoses are linked to higher success (Table 10), which is statistically significant in the NDM group but not in the DM group, reflecting the complex influence of diffuse calcification and vessel rigidity.
Stent implantation, required in 22.8% of patients (n=31), was more common in the DM group (23.5%) but showed different efficacy patterns (Table 11). Among patients in the NDM group, none of the stented cases failed (success 100%), whereas in the DM group, technical success was higher with stents (26.6% vs. 14.3%) not statistically significant.
Overall, stenting improved procedural success (p=0.04), particularly in lesions amenable to scaffolding, emphasizing its selective benefit in proximal or focal disease rather than diffuse infra-popliteal calcification.
The consistent correlation among WIfI, Bollinger, and GLASS supports their complementary use in comprehensive limb-threat assessment.
These findings collectively strengthen the rationale for a standardized scoring-based workflow in CLTI management to optimize revascularization strategy, anticipate procedural challenges, and improve outcome comparability.
4. Discussion
This study provides an in-depth comparative evaluation of patients in the DM and the NDM group with chronic limb-threatening ischemia treated endovascularly, integrating three complementary scoring systems: the WIfI clinical staging, Bollinger anatomical scoring, and the GLASS classification. By combining angiographic and clinical data, the study delineates distinctive vascular phenotypes and outcome patterns associated with DM in patients with advanced PAD.
Our analysis confirmed that diabetes modifies the topography and morphology of arterial lesions. Patients in the DM group had significantly more distal stenoses (>50%) and fewer complete occlusions (p = 0.024 and p = 0.028, respectively), with lower Bollinger scores for both the whole leg and below-knee segments (p = 0.018 and p = 0.015). These findings likely reflect the distinct pathophysiology of diabetic arteriopathy, characterized by diffuse calcific stenoses, medial arterial calcification, and impaired collateral formation rather than by long, focal occlusions. At first glance, this pattern may appear counterintuitive given the well-established association between diabetes and diffuse, multilevel arterial disease. However, angiographic scoring systems such as Bollinger may underestimate disease severity in calcified yet patent distal segments. In contrast, in the NDM group, patients more often presented with proximal, focal, and occlusive lesions, consistent with the macro-atherosclerotic pattern typical of classic atherosclerotic PAD.
The trend toward higher WIfI stage 1 prevalence among diabetics (54.1% vs. 33.3%, p≈0.08) may reflect earlier recognition or less overt tissue loss at the time of intervention, possibly due to more frequent wound surveillance in diabetic foot programs. Many diabetics develop small, superficial ulcers that are classified as WIfI W1 lesions, despite harboring severe and multilevel infra-popliteal disease. This clinic–anatomic mismatch underscores the limitations of relying solely on wound appearance to estimate limb threat in the diabetic foot and highlights the importance of detailed infra-popliteal assessment in this population. The moderate-to-strong correlations between WIfI, Bollinger, and GLASS (ρ=0.29–0.64, p<0.001) reinforce the internal consistency of these tools and validate their concurrent use for stratification.
Also, segmental analysis revealed stronger correlations below the knee, particularly between Bollinger-IP and GLASS-IP (ρ=0.713, p<0.001), and between WIfI and Bollinger-IP (ρ=0.266, p=0.002). This emphasizes the prognostic importance of the infra-popliteal arterial bed, which represents the “bottleneck” for limb salvage in diabetic CLTI. The weighted Kappa analysis demonstrated a moderate-to-substantial agreement between Bollinger and GLASS overall (κ=0.558), rising to substantial in diabetics (κ=0.625). This improvement suggests that, in DM group, the two systems capture similar anatomical complexity and burden, supporting their interchangeability in distal disease assessment.
In contrast, agreement between GLASS FP and WIfI was weak or absent, underscoring that proximal anatomic stages do not necessarily reflect clinical ischemic severity. The mild-to-moderate agreement between GLASS IP and WIfI in diabetics (κ=0.392) suggests that infra-popliteal disease more directly impacts tissue loss and clinical presentation, consistent with the microvascular compromise seen in diabetic limbs.
The association of plaques <25% with higher technical success, statistically significant in NDM group (p=0.012), indicates that mild-to-moderate lesions or “crossable” plaques predict procedural feasibility. In DM group, this relationship was absent, likely because even minimal plaques coexist with extensive calcification, microvascular rarefaction, and arterial wall stiffening, reducing endovascular compliance. These findings resonate with prior studies showing that diabetic PAD involves both macrovascular obstruction and medial sclerosis, making luminal restoration technically challenging and potentially less durable.
Technical success rate was high overall (≈74%) and comparable between groups, confirming that diabetes does not preclude immediate procedural success when modern endovascular techniques are applied. However, outcome stratification revealed clinically relevant patterns: amputation was more frequent in DM group (9.8% vs. 3.9%), mortality slightly higher (3.5% vs. 2.0%), and bypass rates equal (≈11.8%). While not statistically significant, these trends underscore the multifactorial risk burden in DM group, where infection, neuropathy, and impaired wound healing contribute more than anatomy alone. Sex-related differences in CLTI presentation and outcomes have also been reported, with female sex being associated with distinct peri-procedural risk profiles and mortality patterns, underscoring the importance of individualized risk stratification in advanced PAD [16].
When outcomes were analyzed by lesion characteristics, stent implantation correlated with higher technical success (p=0.04), particularly in the NDM group, where no technical failures occurred among those with stents. In the DM group, this association was weaker, possibly due to longer lesion length, smaller vessel caliber, and diffuse disease, leading to increased recoil and restenosis. The observation that success was less stent-dependent in DM group aligns with contemporary evidence that angioplasty alone may suffice for selected infra-popliteal lesions where excessive stenting could compromise runoff or future bypass options.
The integration of scoring systems yields several insights. WIfI quantifies clinical limb threat, Bollinger measures global and segmental atherosclerotic burden, and GLASS stratifies anatomical complexity relevant for revascularization planning. Their combined interpretation allows not only anatomical grading but also functional and prognostic mapping of ischemia. The strong below-knee inter-score correlations confirm that infra-popliteal scoring, especially in DM group, holds the highest discriminatory and predictive value. This supports a shift toward routine inclusion of segmental Bollinger and GLASS-IP scoring in decision-making, particularly for “endovascular-first” strategies.
Comparing with literature, our data both support and expand prior findings. BASIL and BASIL-2 analyses linked Bollinger scores to long-term outcomes, with DM often showing higher total scores due to multi-segmental disease [12]. In contrast, our cohort’s lower diabetic Bollinger scores may reflect earlier endovascular intervention or partial scoring limitations in calcified yet patent segments. Hess et al. [17] similarly reported equivalent revascularization success across DM and NDM patients, with diabetics having higher amputation rates, mirroring our trends. Schmitt et al. [18] and Torres et al. [19] highlighted that DM independently alters PAD distribution and outcomes, confirming the translational relevance of our findings in Eastern European populations.
Previous angiographic studies have consistently shown that diabetic PAD is characterized by distal and infra-popliteal predominance, with diffuse, multi-segmental involvement and fewer focal occlusions compared with non-diabetic disease. Contemporary cohort analyses and registry data confirm that diabetes fundamentally alters lesion distribution and morphology, particularly below the knee, reinforcing the relevance of segmental anatomical assessment in CLTI [15,20,21,22]. Several investigators have highlighted the limitations of global anatomical scoring systems in capturing the true disease burden in diabetic CLTI, particularly in the presence of diffuse calcification and patent but functionally compromised distal vessels. Segment-specific scoring approaches have therefore been proposed to better reflect procedural complexity and limb-threat severity in this population [23,24,25].
Guideline-based frameworks and surgical reference standards emphasize the need to integrate anatomical, clinical, and functional parameters when evaluating CLTI, particularly in complex diabetic presentations. The convergence of our findings with these established concepts supports the external validity and clinical applicability of an integrated scoring strategy in contemporary endovascular practice [26].
From a clinical standpoint, these results support an integrated, score-driven approach in CLTI evaluation. The joint use of WIfI, Bollinger, and GLASS can standardize documentation, enhance multidisciplinary discussions, and refine procedural planning. In particular, recognizing the “infra-popliteal dominance” of diabetic PAD may prompt earlier revascularization, more aggressive wound management, and closer post-procedural follow-up.
In the context of contemporary endovascular management of CLTI, the present analysis emphasizes the role of complementary clinical and anatomical scoring systems, with particular focus on segmental infra-popliteal disease. The consistent correlations observed between WIfI, Bollinger, and GLASS—especially at the infra-popliteal level—support the internal coherence and clinical relevance of the findings. The main limitations include the retrospective, single-center design and the absence of long-term patency and limb-salvage data. Nevertheless, the use of standardized angiographic assessment and a well-characterized cohort strengthens the validity of the observed associations.
Future prospective multicenter studies should incorporate objective calcification indices, duplex-derived flow metrics, and long-term clinical endpoints, including major adverse limb events (MALEs), reinterventions, and limb salvage, to further optimize the predictive integration of these complementary tools
5. Conclusions
In diabetic patients with CLTI, anatomical evaluation should move beyond global limb scoring and prioritize segmental infra-popliteal assessment. When planning endovascular revascularization, below-knee Bollinger burden and GLASS infra-popliteal staging should be systematically integrated alongside WIfI, as they more accurately reflect distal disease severity and procedural complexity.
Adopting a segment-focused, score-driven planning strategy may improve anatomical stratification and guide endovascular decision-making, facilitating earlier, more targeted revascularization, clearer selection of endovascular versus surgical strategies, and more consistent limb-salvage pathways in diabetic CLTI.
Author Contributions
Conceptualization, A.D.B., G.L.B. and M.F.; methodology, A.D.B. and M.F.; software, A.D.B., A.F.O., M.M.G., P.C.M., and B.-M.C.; validation, G.L.B., R.F.P., J.D., and L.I.; formal analysis, C.D.; investigation, A.D.B., A.F.O., P.C.M.; resources, L.I. , J.D. and G.L.B.; data curation, C.D. and A.D.B.; writing—original draft preparation, G.L.B., M.F. and A.D.B.; writing—review and editing, D.M.T., A.B., A.F.O., P.C.M., M.M.F. and I.M.A.; visualization, R.F.P. and D.M.T.; supervision, M.F.; project administration, A.D.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Research Ethics Committee of the Grigore T. Popa University of Medicine and Pharmacy, Iasi, Romania, approval no. 357/12.11.2023.
Informed Consent Statement
Informed consent was obtained from all patients prior to the endovascular procedure. For this retrospective analysis using anonymized data, the requirement for additional consent was waived by the Ethics Committee.
Data Availability Statement
During the preparation of this manuscript, the authors used ChatGPT 5.0 for the purpose of language correction. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PAD | Peripheral Arterial Disease |
| DM | Diabetic Mellitus |
| NDM | Non-Diabetic Mellitus |
| CLI | Critical Limb Ischemia |
| CLTI | Chronic Limb-Threatening Ischemia |
References
- Conte, MS; Bradbury, AW; Kolh, P; et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019, 58(1S), S1–S109.e33. [Google Scholar] [CrossRef]
- Bradbury, AW; Adam, DJ; Bell, J; et al. The BASIL trial: randomized comparison of bypass surgery versus angioplasty in severe limb ischemia. J Vasc Surg. 2010, 51((5) Suppl, 5S–17S. [Google Scholar] [CrossRef]
- Farber, A; Rosenfield, K; Menard, MT; et al. Endovascular revascularization versus surgical bypass for CLTI: results from BEST-CLI trial. N Engl J Med. 2022, 387(25), 2305–2316. [Google Scholar] [CrossRef]
- Aboyans, V; Ricco, JB; Bartelink, MEL; et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases. Eur Heart J. 2024, 45(5), 765–830. [Google Scholar] [CrossRef]
- Bunte, MC; Jacobson, J; Javaheri, A; et al. Patterns of arterial calcification in diabetes and their impact on revascularization. Circulation. 2020, 141(1), 99–114. [Google Scholar]
- Boyko, EJ; Lipsky, BA; Giurini, JM; et al. Pathophysiology and prevention of diabetic foot complications. Diabetes Care. 2021, 44(7), 1463–1471. [Google Scholar] [CrossRef]
- Norgren, L; Fowkes, FGR; Aboyans, V; et al. Update on peripheral artery disease: pathophysiology and management. Nat Rev Cardiol. 2022, 19(12), 760–776. [Google Scholar]
- Cerqueira, LO; Duarte, EG; Barros, AL; Cerqueira, JR; Araújo, WB. WIfI classification and limb outcomes after endovascular treatment for critical limb ischemia. J Vasc Bras. 2020, 19, e20200089. [Google Scholar]
- Hicks, CW; Canner, JK; Mathioudakis, N; et al. The WIfI classification system predicts wound healing and amputation in diabetic foot ulcer patients. J Vasc Surg. 2020, 71(2), 631–640. [Google Scholar] [CrossRef]
- Bollinger, A. An extension of the Bollinger scoring system for the quantitative assessment of peripheral atherosclerosis. Angiology. 1981, 32(4), 240–250. [Google Scholar] [CrossRef]
- Benson, RA; Meecham, L; Bate, G; Bradbury, AW. Disease quantified: Bollinger score reproducibility in angiographic assessment. Eur J Vasc Endovasc Surg. 2016, 52(1), 88–94. [Google Scholar] [CrossRef]
- Zielinski, LP; Chowdhury, MM; Carter, M; Worsfold, BP; Coughlin, PA. Variability in reporting Bollinger and GLASS scores: implications for standardization. Eur J Vasc Endovasc Surg. 2020, 59(4), 595–603. [Google Scholar] [CrossRef]
- Fitridge, R; Hinchliffe, RJ; Zierler, RE; et al. IWGDF/ESVS/SVS Guidelines on the diagnosis, prognosis and management of peripheral artery disease and diabetic foot. Eur J Vasc Endovasc Surg. 2023, 65(1S), S1–S79. [Google Scholar] [CrossRef]
- Hinchliffe, RJ; Forsythe, RO; Apelqvist, J; et al. Performance of GLASS and WIfI for predicting outcomes after revascularization in CLTI. Eur J Vasc Endovasc Surg. 2021, 62(1), 93–102. [Google Scholar] [CrossRef]
- Mustapha, JA; Diaz-Sandoval, LJ; Saab, F; et al. Role of scoring systems in predicting technical success in diabetic CLTI. Vasc Med. 2022, 27(3), 268–278. [Google Scholar]
- Ferraresi, R; Faglia, E; Clerici, G; et al. Sex-related differences and factors associated with peri-procedural mortality in chronic limb-threatening ischemia. Journal of Personalized Medicine 2023, 13(2), 316. [Google Scholar] [CrossRef]
- Hess, CN; Rogers, RK; Wang, TY; et al. Major adverse limb events and mortality in peripheral artery disease: insights from the EUCLID trial. J Am Coll Cardiol. 2020, 75(5), 498–508. [Google Scholar] [CrossRef]
- Schmitt, VH; Hobohm, L; Vosseler, M; et al. Temporal trends in hospitalizations and outcomes in diabetic vs. non-diabetic peripheral artery disease. Diabet Med. 2022, 39(8), e14854. [Google Scholar] [CrossRef]
- Torres, C; Ujueta, F; Rogers, E; et al. Outcomes after endovascular therapy for CLTI in diabetic patients: insights from a national registry. J Am Heart Assoc. 2022, 11(5), e024593. [Google Scholar]
- Morosetti, D; Farina, A; Speziale, F; et al. Infrapopliteal angioplasty outcomes in diabetic versus non-diabetic patients: a real-world multicenter experience. Int Angiol. 2021, 40(3), 220–229. [Google Scholar]
- Randon, C; Jacobs, B; De Ryck, F; et al. Long-term outcome of infrapopliteal angioplasty in diabetic critical limb ischemia. Eur J Vasc Endovasc Surg. 2020, 60(1), 77–86. [Google Scholar]
- Kim, HK; Park, J; Cho, S; et al. Correlation of WIfI stage with angiographic findings and outcomes after revascularization. Ann Vasc Surg. 2022, 79, 247–256. [Google Scholar] [CrossRef]
- Anwar, MA; Georgakarakos, E; Antoniou, GA; et al. Diabetic versus non-diabetic arterial disease: anatomical patterns and clinical implications. Ann Vasc Surg. 2023, 94, 76–84. [Google Scholar] [CrossRef]
- Faglia, E; Clerici, G; Caminiti, M; et al. Evaluation of infrapopliteal angioplasty in diabetic critical limb ischemia: predictors of failure. Diabetes Care. 2019, 42(6), e100–e103. [Google Scholar] [CrossRef]
- Beropoulis, E; Stavroulakis, K; Schwindt, A; et al. Long-term outcomes of infrapopliteal angioplasty: impact of diabetes and WIfI stage. J Endovasc Ther. 2020, 27(5), 766–775. [Google Scholar]
- Norgren, L; Hiatt, WR; Dormandy, JA. Peripheral arterial disease: pathophysiology and natural history. In Rutherford’s Vascular Surgery and Endovascular Therapy., 9th ed.; Sidawy, AN, Perler, BA, Eds.; Elsevier: Philadelphia, PA, 2019; pp. 1234–1250. [Google Scholar]
Figure 1.
Correlation heatmap (Spearman’s ρ) between WIfI stage, Bollinger whole-leg score, and global GLASS stage.
Figure 1.
Correlation heatmap (Spearman’s ρ) between WIfI stage, Bollinger whole-leg score, and global GLASS stage.
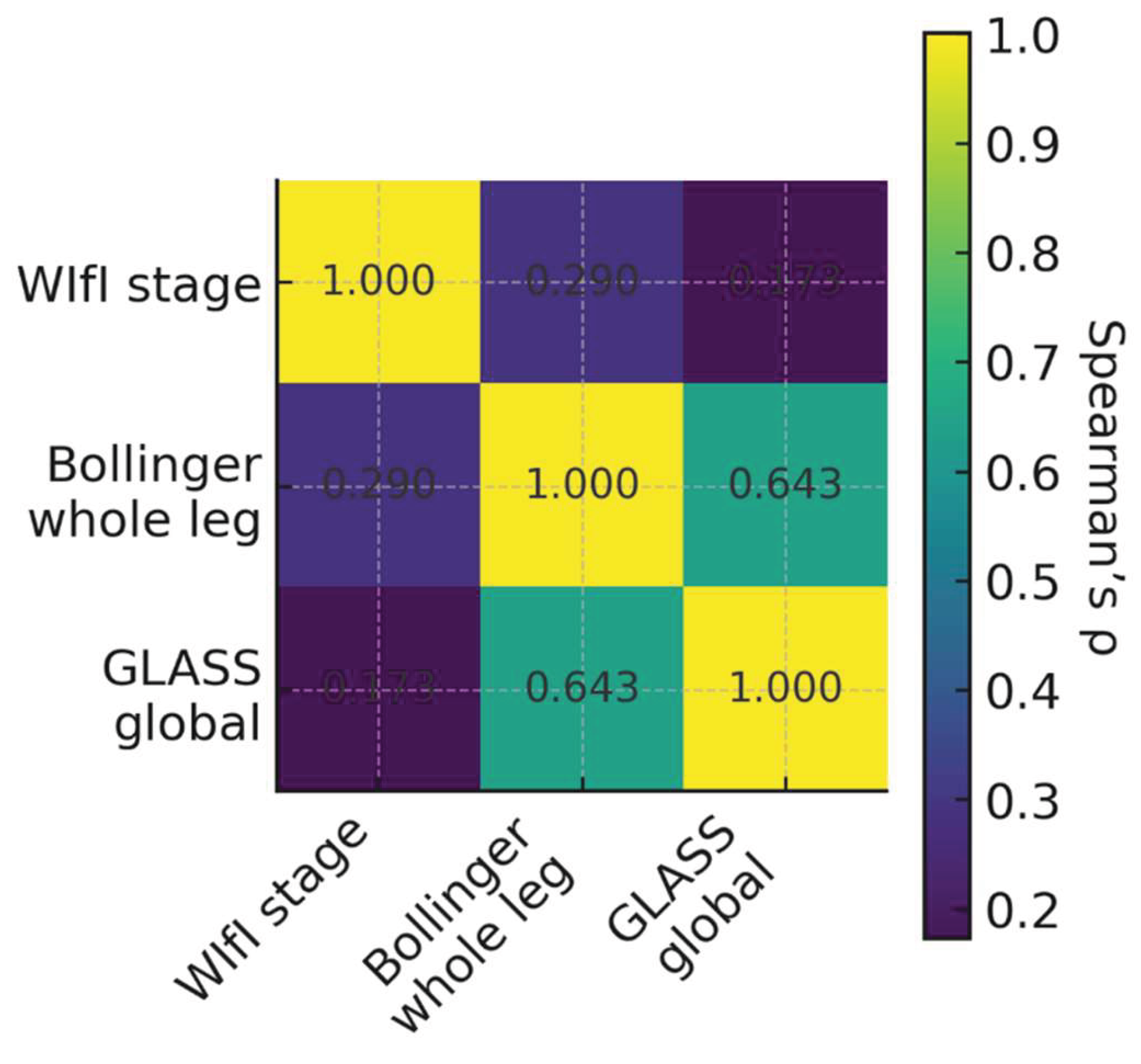
Figure 2.
Spearman’s ρ correlation heatmap between WIfI stage, infra-popliteal Bollinger score (below-knee burden), and GLASS-IP stage. IP infra-popliteal.
Figure 2.
Spearman’s ρ correlation heatmap between WIfI stage, infra-popliteal Bollinger score (below-knee burden), and GLASS-IP stage. IP infra-popliteal.
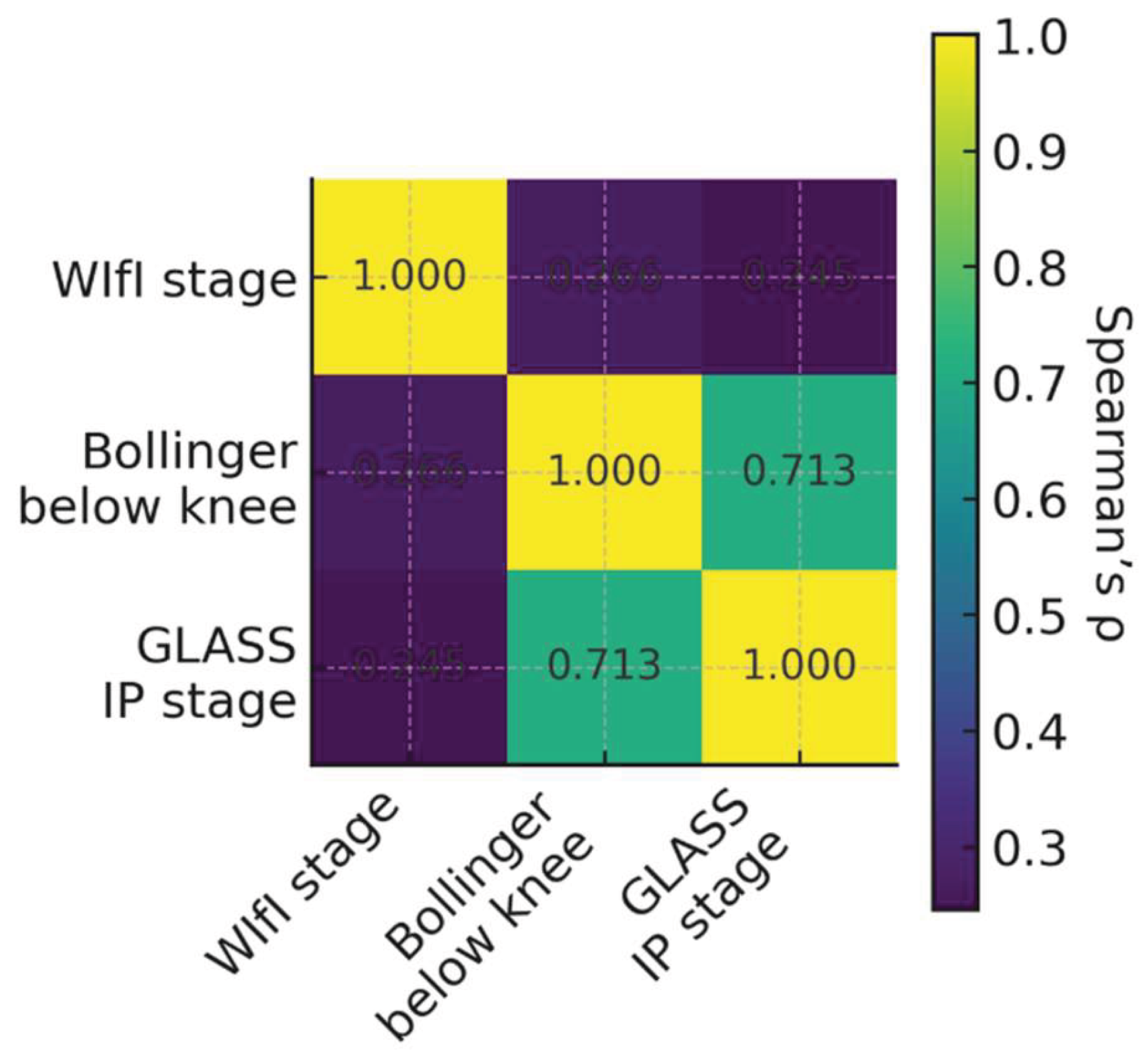
Figure 3.
Hierarchical relationships among WIfI clinical staging, Bollinger anatomical scoring, and GLASS anatomic–technical complexity classification. CLTI, chronic limb-threatening ischemia; FP, femoropopliteal; IP, infra-popliteal; TS, technical success.
Figure 3.
Hierarchical relationships among WIfI clinical staging, Bollinger anatomical scoring, and GLASS anatomic–technical complexity classification. CLTI, chronic limb-threatening ischemia; FP, femoropopliteal; IP, infra-popliteal; TS, technical success.
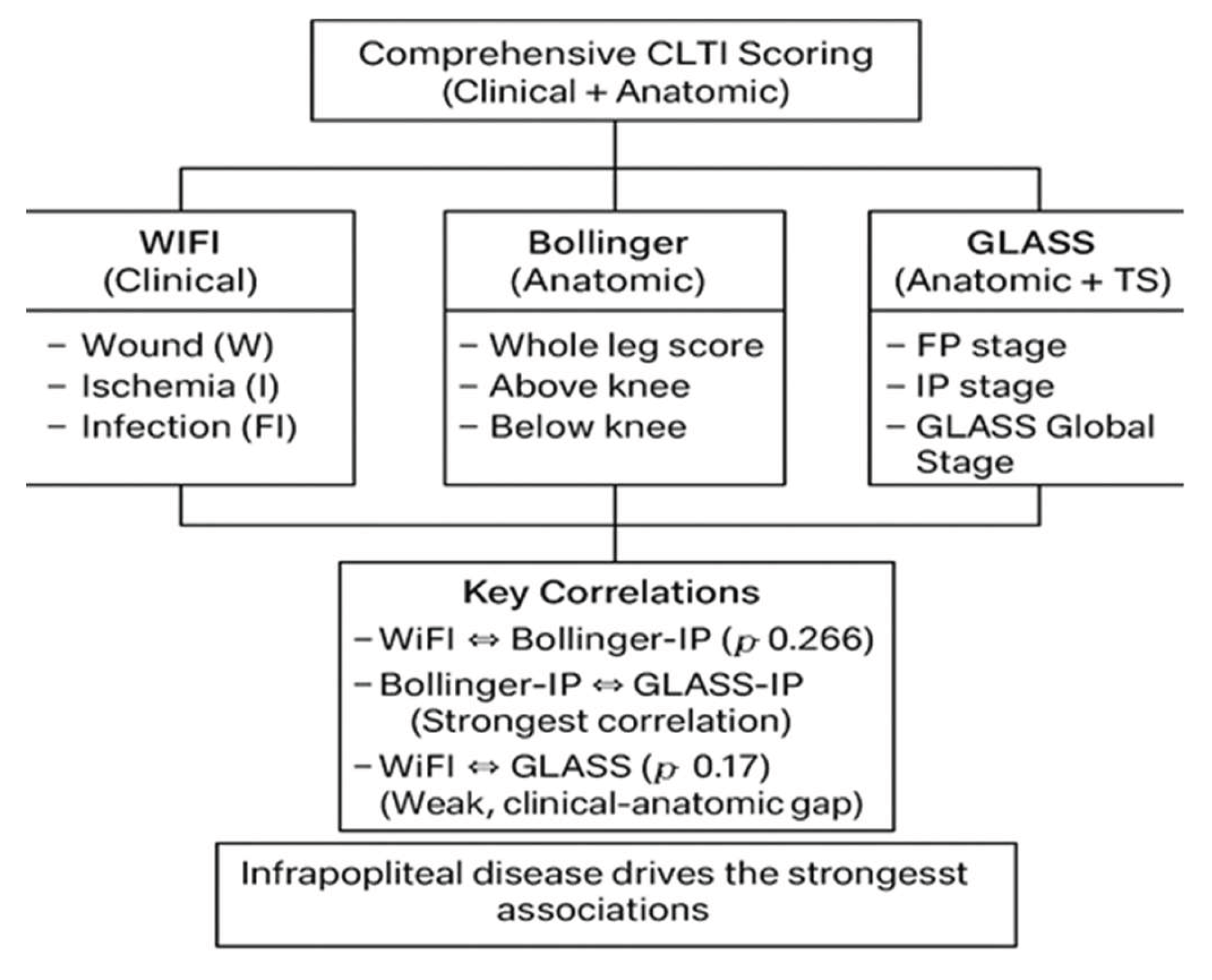

Table 1.
WIfI Classification System.
| Component | Score | Description |
|---|---|---|
| W (Wound) – Tissue loss | 0 | No ulcer (ischemic rest pain may be present) |
| 1 | Small, superficial ulcer on the foot or leg, without gangrene | |
| 2 | Deep ulcer with exposure of bone, joint, or tendon; limited gangrene confined to the toes | |
| 3 | Extensive deep ulceration involving the heel or forefoot; extensive gangrene | |
| I (Ischemia) – Hemodynamic impairment | ABI | Ankle pressure (mmHg) |
| 0 | ≥0.80 | |
| 1 | 0.60–0.79 | |
| 2 | 0.40–0.59 | |
| 3 | <0.40 | |
| FI (Foot Infection) – Infection severity | 0 | No clinical signs or symptoms of infection |
| 1 | Local infection involving only skin and subcutaneous tissue | |
| 2 | Local infection involving deeper structures (e.g., fascia, muscle, tendon, bone) | |
| 3 | Systemic inflammatory response syndrome |
Table 2.
Stratification using the Bollinger score.
| Location | Occlusion | Stenosis >50% | Stenosis ≤50% |
|---|---|---|---|
| Single | - | 4 | 2 |
| Multiple ≤ half | 13 | 5 | 3 |
| Multiple > half | 15 | 6 | 4 |
Table 3.
Glass stages.
|
Femoropopliteal segment |
4 | III | III | III | III | III |
| 3 | II | II | II | III | III | |
| 2 | I | II | II | II | III | |
| 1 | I | I | II | II | III | |
| 0 | - | I | I | II | III | |
|
Infra-popliteal segment |
0 | 1 | 2 | 3 | 4 |
Table 4.
Baseline characteristics of patients included in the study.
| PARAMETER | NDM Group (n=51) |
DM Group (n=85) |
P-value |
|---|---|---|---|
| Female, n(%) | 12 (23.5) | 27 (31.8) | 0.304 |
| Urban residence, n (%) | 25 (49.0) | 62 (72.9) | 0.005** |
| Age, years (mean ±sd) | 69.78±11.38 | 69.89±8.57 | 0.737 |
| Hypertension, n (%) | 38 (74.5) | 73 (85.9) | 0.097 |
| Obesity, n (%) | 4 (7.8) | 13 (15.3) | 0.203 |
| Heart failure, n (%) | 17 (33.3) | 24 (28.2) | 0.531 |
| Atrial fibrillation, n (%) | 15 (29.4) | 16 (18.8) | 0.154 |
| Prior mi, n (%) | 2 (3.9) | 7 (8.2) | 0.483 |
| Chronic coronary syndrome, n (%) | 8 (15.7) | 17 (20.0) | 0.530 |
| Cardiomyopathy, n (%) | 1 (2.0) | 5 (5.9) | 0.410 |
| Dilated cardiomyopathy, n (%) | 4 (7.8) | 4 (4.7) | 0.473 |
| Chronic kidney disease, n (%) | 7 (13.7) | 16 (18.8) | 0.443 |
| Prior stroke, n (%) | 2 (3.9) | 10 (11.9) | 0.210 |
Table 5.
Angiographic severity according with WIfI stages in the diabetes mellitus (DM) and non-diabetes (NDM) groups. NS non-significant.
Table 5.
Angiographic severity according with WIfI stages in the diabetes mellitus (DM) and non-diabetes (NDM) groups. NS non-significant.
| VARIABLE | NDM Group (N=51) |
DM Group (N=85) |
P-value |
|---|---|---|---|
| >50% stenosis, n (%) | 18 (35.3) | 47 (55.3) | 0.024* |
| Any occlusion, n (%) | 49 (96.1) | 71 (83.5) | 0.028* |
| Wifi stage 1, n (%) | 17 (33.3) | 46 (54.1) | 0.083+ |
| Stents present, n (%) | 11 (21.6) | 20 (23.5) | NS |
Table 6.
The Bollinger score in the DM group versus the NDM group.
| PARAMETER | NDM Group | DM Group | P-value |
|---|---|---|---|
| Bollinger whole leg, mean±sd | 36.78±16.09 | 30.07±16.34 | 0.018* |
| Bollinger above knee, mean±sd | 9.92±8.01 | 9.54±6.96 | 0.941 |
| Bollinger below knee, mean±sd | 26.86±13.93 | 20.53±15.88 | 0.015* |
| Glass global: std 1, n (%) | 23 (45.1) | 28 (32.9) | NS |
| Glass global: std 2, n (%) | 18 (35.3) | 35 (41.2) | NS |
| Glass global: std 3, n (%) | 10 (19.6) | 22 (25.9) | NS |
Table 7.
Success rate in the DM group versus NDM group.
| OUTCOME | NDM Group (n=51) |
DM Group (n=85) |
P-value |
|---|---|---|---|
| Technical success, n (%) | 37 (72.5) | 64 (75.3) | NS |
| Bypass, n (%) | 6 (11.8) | 10 (11.8) | NS |
| Major amputation, n (%) | 2 (3.9) | 8 (9.4) | NS |
| Death, n (%) | 1 (2.0) | 3 (3.5) | NS |
Table 8.
Correlations Between Scoring Systems.
| CORRELATION (overall) | ρ | P-value |
|---|---|---|
| WIfI ↔ Bollinger (whole leg) | 0.290 | <0.001 |
| WIfI ↔ GLASS (global) | 0.173 | 0.044 |
| Bollinger (whole leg) ↔ GLASS (global) | 0.643 | <0.001 |
| BOLL (whole leg)↔ GLASS (global) | 0.567 | <0.001 |
| Above knee: Bollinger ↔ GLASS-FP | 0.762 | <0.001 |
| Below knee: WIfI ↔ Bollinger-IP | 0.266 | 0.002 |
| Below knee: Bollinger-IP ↔ GLASS-IP | 0.713 | <0.001 |
Table 9.
Weighted Kappa coefficients between the investigated scores (overall and stratified by diabetes status). IF infra-popliteal; FP femuro-popliteal.
Table 9.
Weighted Kappa coefficients between the investigated scores (overall and stratified by diabetes status). IF infra-popliteal; FP femuro-popliteal.
| Group | Weighted Kappa | Std. Error | z | p-value | 95% CI l.inf | 95% CI l. sup |
|
|---|---|---|---|---|---|---|---|
| BOL whole – GLASS STD | Total cohort | 0.558 | 0.062 | 6.618 | <0.001** | 0.436 | 0.679 |
| NDM group | 0.485 | 0.088 | 4.157 | <0.001** | 0.312 | 0.658 | |
| DM group | 0.625 | 0.074 | 5.797 | <0.001** | 0.480 | 0.771 | |
| GLASS FP – GLASS IP | Total cohort | 0.037 | 0.086 | 0.434 | 0.664 | -0.133 | 0.206 |
| NDM group | 0.100 | 0.162 | 0.716 | 0.474 | -0.218 | 0.417 | |
| DM group | -0.019 | 0.095 | -0.176 | 0.860 | -0.205 | 0.168 | |
| GLASS FP – WIfI stage | Total cohort | -0.010 | 0.077 | -0.123 | 0.902 | -0.161 | 0.141 |
| NDM group | 0.121 | 0.107 | 1.034 | 0.301 | -0.090 | 0.331 | |
| DM group | -0.102 | 0.105 | -0.962 | 0.336 | -0.308 | 0.104 | |
| GLASS IP – WIfI stage | Total cohort | 0.183 | 0.088 | 2.239 | 0.025* | 0.011 | 0.356 |
| NDM group | -0.088 | 0.129 | -0.715 | 0.474 | -0.340 | 0.164 | |
| DM group | 0.392 | 0.087 | 3.805 | <0.001** | 0.221 | 0.563 |
Table 10.
Plaques with non-significant stenoses predicted higher success in the NDM group. DM diabetes mellitus; NS non-significant.
Table 10.
Plaques with non-significant stenoses predicted higher success in the NDM group. DM diabetes mellitus; NS non-significant.
| Group | OR for failure (plaques present vs. absent) |
95% CI | P-value |
|---|---|---|---|
| Overall | 0.33 | 0.15–0.74 | 0.006** |
| NDM group | 0.19 | 0.05–0.74 | 0.012* |
| DM group | — | — | NS |
Table 11.
Distribution of stent implantation and association with technical success (overall and stratified by diabetes status). DM diabetes mellitus; NDM non-diabetic.
Table 11.
Distribution of stent implantation and association with technical success (overall and stratified by diabetes status). DM diabetes mellitus; NDM non-diabetic.
| Subgroup | With stent n (%) | Without stent n (%) | Technical success (%) | Technical failure (%) | P-value |
|---|---|---|---|---|---|
| Total cohort | 31 (22.8) | 105 (77.2) | 27.7% | 8.6% | 0.04* |
| NDM group | 11 (21.6) | 40 (78.4) | 29.7% | 0% | NS |
| DM group | 20 (23.5) | 65 (76.5) | 26.6% | 14.3% | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



