
Submitted:
04 February 2026
Posted:
06 February 2026
You are already at the latest version
Abstract
Background: Family-centered care is a core principle of contemporary pediatric health and rehabilitation, particularly for children with neurodevelopmental disorders. Con-ceptual frameworks that emphasize functioning, participation, and contextual factors are essential for operationalizing this approach in clinical practice. The International Classification of Functioning, Disability and Health (ICF) and the F-words framework are widely referenced models aligned with these principles; however, their practical integration within family-centered pediatric care remains challenging. The objective of this narrative review was to examine how the ICF and the F-words framework are ap-plied in pediatric neurorehabilitation, to identify conceptual and practical limitations, and to explore strategies that may enhance their use in family-centered care. Methods: A narrative literature review was conducted using the PubMed, Scopus, and Web of Science databases. English-language publications published between 2005 and 2025 were identified using keywords related to the ICF, the F-words framework, neurode-velopmental disorders, childhood disability, and cerebral palsy. Eligible sources in-cluded original research articles, systematic, scoping, and narrative reviews, valida-tion studies, expert reports, and clinical practice guidelines. Articles were selected based on relevance to family-centered pediatric care and the integration of the ICF and F-words frameworks. Results: A short summary of the article’s main findings Thir-ty-one publications were included, representing a broad range of theoretical, empirical, and clinical perspectives. The findings indicate increasing use of both the ICF and the F-words framework in pediatric rehabilitation and family-centered care. However, persistent challenges were identified, including conceptual ambiguity, overlap be-tween frameworks, limited standardization, difficulties in outcome measurement, and inconsistent involvement of families in clinical decision-making. Conclusions: The ICF and the F-words framework offer complementary strengths for supporting fami-ly-centered pediatric care. A structured, integrated approach may improve shared de-cision-making, communication with families, and participation-focused care. Further methodological refinement and practice-oriented guidance are needed to support their consistent and effective implementation in everyday clinical settings.
Keywords:
ICF classification
; F-words
; cerebral palsy
; childhood disability
; neurodevelopmental disorders
1. Introduction
Since the beginning of the twenty-first century, there has been a dynamic evolution in how human disability is conceptualized [1,2,3,4]. This shift is particularly evident in the treatment and rehabilitation of children with developmental and neurological conditions [1,2,4,5,6]. Disabilities resulting from structural and/or functional disorders of the nervous system are typically complex, often involving the musculoskeletal system and producing cognitive, behavioral, and communication difficulties that can affect quality of life across the lifespan [7].
Broadly, the changing perception of childhood disability reflects a gradual unification of traditional biomedical concepts with modern perspectives that acknowledge the influence of social, environmental, and personal factors on child development. Consequently, contemporary therapeutic approaches aim to enhance both family well-being and the timing and context of professional interventions across multiple domains [6,8].
The traditional approach to childhood disability, dominant in the previous century, was rooted in a biomedical paradigm that emphasized identifying and “repairing” the source of dysfunction and observing resulting health changes [4,9,10,11,12]. While this model remains effective in acute medical treatment, it proves insufficient when addressing chronic developmental conditions. The “repair” approach is limited by diagnostic imprecision, particularly in heterogeneous conditions such as cerebral palsy, the scarcity of evidence-based therapeutic methods, the weak association between impairment-level interventions and real-world functioning, and the difficulty in distinguishing treatment effects from natural developmental or compensatory changes. Accordingly, new perspectives have emerged that promote a broader understanding of disability, recognizing its multidimensional determinants and offering a more comprehensive set of responses [1,2,13,14].
The modern biopsychosocial paradigm, encompassing multiple interacting determinants of child development, presents both opportunities and challenges for clinicians seeking to navigate comprehensive rehabilitation processes effectively. One valuable framework for guiding this complex process is the ICF, introduced by the World Health Organization (WHO) in 2001 as a universal conceptual and classificatory model for describing health and disability [1,7,15,16,17].
Complementary to the ICF, the F-words framework – function, family, fitness, fun, friends, and future – offers a child-friendly model that operationalizes ICF concepts in pediatric practice [18,19,20]. Since its introduction in 2012, this framework has gained international recognition for supporting holistic approaches to childhood disability, informing physical activity and rehabilitation practices, and serving as a tool for assessing quality-of-life outcomes [18]. By translating ICF constructs into accessible and engaging language, the F-words facilitate the implementation of child and family-centered care across diverse rehabilitation contexts. Although widely adopted internationally to guide comprehensive, participation-focused care [5,19,21,22], the F-words framework remains less familiar to some professionals compared to the ICF.
Despite their theoretical and practical potential, both the ICF and the F-words framework remain underutilized in clinical settings. This narrative review aims to introduce and integrate these frameworks, critically analyze their limitations, and propose constructive adjustments to enhance clarity, usability, and application in day-to-day pediatric rehabilitation practice. By doing so, the authors intend to encourage healthcare professionals to adopt these concepts, improving coordination and effectiveness in the management of childhood disability.
2. Materials and Methods
A narrative literature review was conducted to examine the application of the ICF and the F-words framework in pediatric care for children with neurodevelopmental disorders. The literature search was performed using the PubMed, Scopus, and Web of Science databases. Searches were limited to English-language publications published between 2005 and 2025. Keywords were searched within the Title and Abstract fields using the following query: (“F-words” AND (“ICF” OR “International Classification of Functioning”) AND (“neurodevelopmental disorders” OR “childhood disability” OR “cerebral palsy”) AND (“review” OR “systematic review” OR “narrative review”)).
Eligible sources included original research articles (randomized controlled trials and observational studies), review articles (systematic, scoping, and narrative reviews), expert reports, validation studies or reports, non-experimental quantitative research, and clinical practice guidelines. Publications were selected based on their relevance to the objectives of the review, methodological clarity, and recency. The search process was iterative and involved repeated screening of the literature until thematic saturation was achieved.
As this study was designed as a narrative review, no formal quality appraisal or risk-of-bias assessment was conducted. Nevertheless, attention was given to the methodological soundness, transparency, and contextual relevance of each included publication. No primary data, datasets, computer code, or experimental protocols were generated or analyzed as part of this review.
3. Results
A total of 31 publications were included in this narrative review, reflecting a diverse range of publication types addressing the ICF and the F-words framework in the context of childhood disability and neurodevelopmental disorders.
The majority of included publications were review articles, including narrative and scoping reviews, which synthesized existing evidence on the conceptual foundations of the ICF and the F-words framework and their application in clinical practice. Systematic reviews contributed higher-level evidence related to clinical guidelines and early intervention strategies. Empirical studies – including non-experimental quantitative research, descriptive comparative studies, and survey-based research – provided insights into the practical implementation and international uptake of the F-words framework. Validation studies supported the methodological robustness of outcome measures and ICF Core Sets. In addition, expert reports, international legal treaties, and editorials offered policy context, foundational guidance, and professional perspectives.
The distribution of included publications by type, together with representative authors and the number of articles within each category, is presented in Table 1.
4. Discussion
4.1. ICF Framework in Childhood Disability: Contributions and Critical Perspectives
The ICF has profoundly influenced contemporary approaches to neurodevelopmental rehabilitation [7]. By organizing information into the domains of Functioning and Disability (Body Structure and Function; Activity and Participation) and Contextual Factors (Environmental and Personal), it offers a comprehensive biopsychosocial framework that extends beyond the traditional biomedical paradigm [1,2,5,23,24,25,27]. This multidimensional structure enables clinicians and researchers to appreciate the complex interactions between biological, psychological, and social determinants of health, thereby supporting a more holistic conceptualization of childhood disability.
The ICF has also played a transformative role in shaping family-centered and participation-oriented models of care, shifting the focus from ‘fixing’ impairments toward promoting function, participation, and family engagement [28,29]. Its standardized terminology facilitates interdisciplinary communication and comparability of research findings across clinical and research settings [16,23,26]. In addition, the development of ICF Core Sets and Common Data Elements has increased the framework’s applicability in both clinical practice and research [35,36,38,39]. Beyond healthcare, the influence of the ICF extends to policy, aligning with the principles of the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD), which conceptualizes disability as the outcome of interactions between individuals and societal barriers rather than as an intrinsic trait [31,34]. This alignment underscores the value of the ICF as a unifying framework for clinical practice, research, and inclusive policy.
Despite its comprehensiveness and impact, the ICF has been subject to sustained critical analysis. Scholars have noted that the framework lacks clearly articulated theoretical foundations, contains overlapping or partially redundant components, and omits a systematic classification of personal factors [30]. Structural inconsistencies have also been identified between the textual description of the framework and its graphical representation. For example, ‘activity’ and ‘participation’ are presented as separate domains, whereas ‘body structures’ and ‘body functions’ are merged into a single block, as shown in the original WHO diagram (Figure 1). Such inconsistencies may obscure conceptual boundaries and complicate the interpretation of relationships among components, potentially limiting clarity and consistency across clinical and research applications.
From a conceptual perspective, some authors argue that the ICF may inadvertently overemphasize biological aspects of functioning relative to psychological and social determinants, thereby weakening the balanced biopsychosocial perspective it is intended to uphold [3]. In response to these concerns, Haslam et al. proposed a socio-psycho-bio model that reverses the traditional hierarchy by placing social and group processes at the forefront, psychological processes at an intermediate level, and biological factors as downstream consequences [32]. Within this framework, health phenomena are embedded in social identity, group membership, and collective life, emphasizing that social connectedness and identity processes shape both psychological and biological outcomes.
Additional limitations relate to the restricted distinction between ‘activity’ and ‘participation’ as well as the positioning of personal and environmental factors within the contextual domain [3,25]. In practical terms, challenges have also been reported in implementing the ICF in everyday rehabilitation. The framework’s complexity and the time required for its application – particularly in autism spectrum disorder and other neurodevelopmental conditions – may hinder its consistent use in clinical settings [42]. Moreover, alignment between commonly used clinical assessment tools and ICF categories remains incomplete, leaving some functional domains underrepresented, especially personal factors, which still lack standardized measurement instruments [13,36].
Nevertheless, these limitations do not diminish the conceptual significance of the ICF. Rather, they highlight the need for continued refinement and contextual adaptation to ensure that the framework remains both theoretically robust and practically feasible. When integrated thoughtfully, the ICF continues to serve as a foundational tool for advancing holistic, person-centered, and inclusive approaches to neurodevelopmental rehabilitation.
4.2. F-Words in Childhood Disability: Practical Contributions and Conceptual Limitations
The F-words framework – comprising function, family, fitness, fun, friends, and future – represents a child-friendly operationalization of the ICF, designed to facilitate holistic and family-centered interventions in pediatric rehabilitation [5,19,21,22,28,33]. Since its introduction in 2012, the framework has gained international recognition, shaping contemporary approaches to childhood disability, informing physical activity and rehabilitation practices, and serving as a tool for evaluating quality-of-life outcomes [19,40]. The F-words emphasize the most meaningful aspects of children’s lives, aligning with the biopsychosocial paradigm by highlighting function, family engagement, physical and mental fitness, joy, peer relationships, and future orientation.
Within this framework, function broadly corresponds to the ICF domains of body structures and functions as well as activities and participation, emphasizing that therapeutic success should be defined not by conformity to normative standards but by meaningful participation in daily tasks and play [18,28]. Family underscores the essential role of caregivers in therapeutic processes, acknowledging that childhood disability affects the well-being of the entire household. Fitness integrates physical and mental health, promoting individualized, ability-based approaches to movement and lifestyle. Fun and friends emphasize joy and social connectedness as intrinsic motivators that enhance engagement in therapy, while future promotes long-term planning aimed at optimizing both present functioning and later quality of life [18].
More recently, freedom has been proposed as an overarching concept linking all six F-words movement, activity and participation (the ability to make choices and engage in diverse experiences), and environmental and personal dimensions (accessibility and autonomy)[3,41]. Central to this notion is the principle of autonomy, which is foundational in both bioethical discourse and UNCRPD [34]. Within this perspective, health can be understood as the freedom to pursue meaningful goals and interests, whereas disability represents a limitation of that freedom. Consequently, interventions should not only aim to reduce impairment but also to enhance participation, dignity, and self-determination. The authors of this paper further extend this view by defining freedom as personal autonomy – the capacity to act and express oneself within one’s own boundaries while minimizing external assistance and dependence on others.
Despite these strengths, integrating the F-words framework with the ICF presents conceptual and practical challenges. Soper et al. argue that the framework remains in an early phase of theoretical development and highlight difficulties in translating its holistic, client-centered principles into consistent, multidisciplinary practice [19,22]. Furthermore, they note that by borrowing from established models such as the ICF, the F-words risk becoming an unquestioned organizing structure that may unintentionally constrain theoretical innovation. Direct attempts to align the F-words with ICF components can create ambiguity. Rosenbaum and Gorter [18], for instance, appear to substitute existing ICF categories (Figure. 2) with corresponding F-words, leaving readers uncertain as to whether the two frameworks should be integrated, used alternately, or treated as complementary.
Figure 2.
F-words overlaid on the International Classification of Functioning, Health and Disability components diagram [18].
Figure 2.
F-words overlaid on the International Classification of Functioning, Health and Disability components diagram [18].
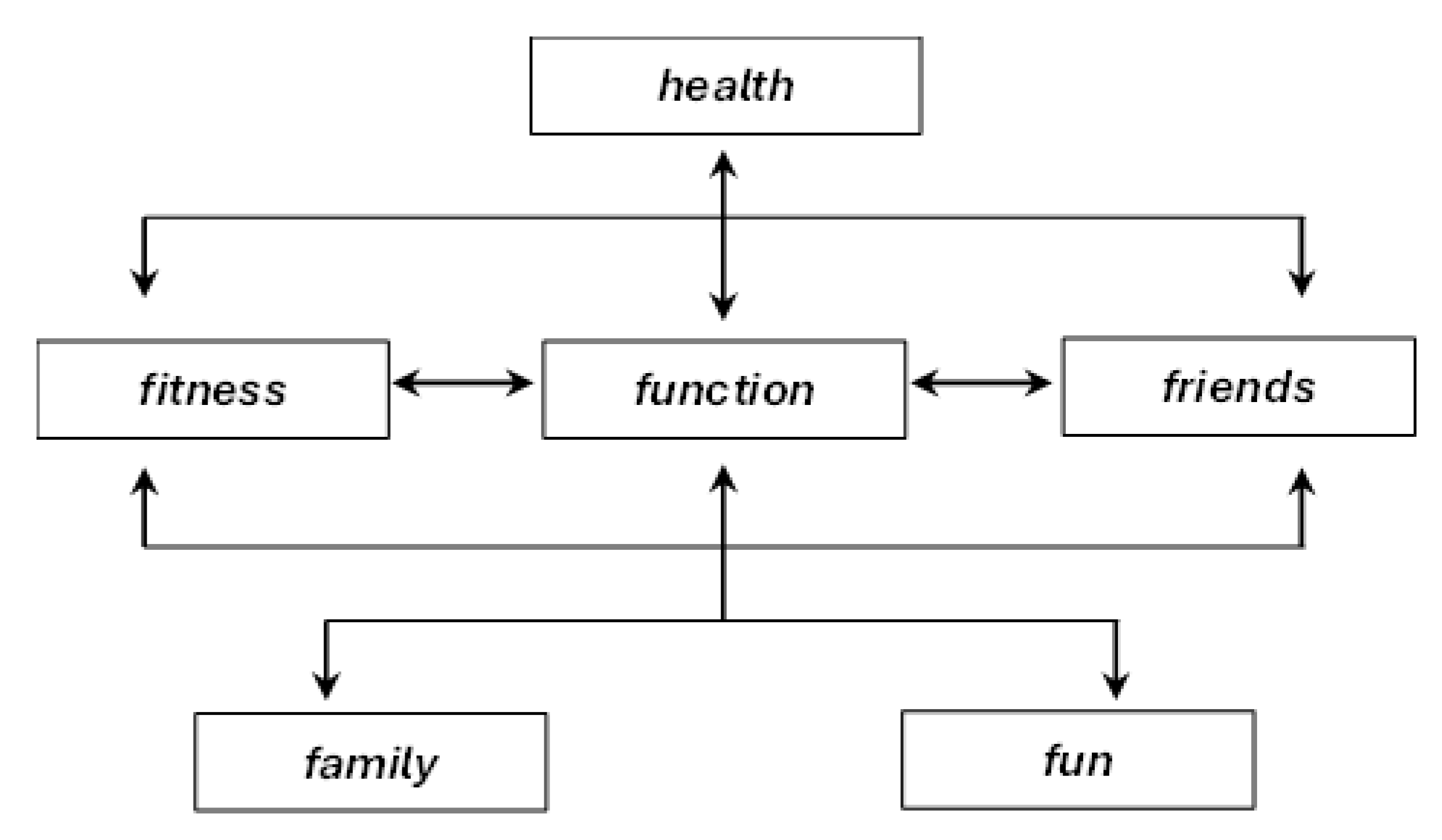
Several F-words overlap with multiple ICF domains – for example, function corresponds simultaneously to body structures and functions and to activities and participation – creating terminological ambiguity and practical challenges [18]. This overlap raises uncertainty as to whether clinicians should replace ICF components with F-words, apply both frameworks in parallel, or treat the F-words as interpretive lenses through which ICF information is understood.
4.3. Proposed Solutions
After highlighting certain points of discussion within the ICF and F-words concepts, it is worth proposing a few practical solutions to existing issues, primarily aimed at reducing ambiguity and eliminating logical gaps. These proposals are presented in the same order as the areas of debate discussed in the previous subsection.
First, to address the inconsistencies between the textual description and the graphical representation of the ICF system, we propose a revision of the existing diagram (Figure. 1), presented here in Figure 3. In this revised version, the separation of the ‘activity and participation‘ component into two subcomponents has been removed, thus simplifying the diagram and aligning it with the official description. Additionally, ‘health condition’ is repositioned as the heading of the framework, which reflects its actual role. This adjustment clarifies that the health condition is not an independent influencing factor, but rather the result of the interactions between the other components. Placing it at the center of the diagram further emphasizes that all ICF components contribute equally to the overall health condition.
The revised diagram is symmetrical and rotation-invariant: regardless of perspective, ‘health condition‘ remains the central element, while the surrounding components retain equal distance. Furthermore, all ICF components are interconnected on an “all-to-all” basis (including ‘self-to-self‘ feedback loops), with bidirectional arrows to illustrate reciprocal relationships. This layout provides a more faithful visualization of the ICF’s underlying principles, as suggested by Rosenbaum and Gorter, and reflects the model’s dynamic nature.
From a clinical standpoint, this approach offers a more flexible interpretive tool. For example, when deviations are diagnosed in the “body structure and function” component, the clinician can consider both targeted interventions “within” this component and supportive strategies that stem from other domains. In turn, these influences can be traced back to their potential effects on the remaining components, thereby encouraging a broader biopsychosocial perspective when analyzing disability. In Figure. 3, the proposed modified diagram is presented twice: on the left side, with a focus on two key ICF sections, and on the right side – highlighting components aligned with the biological and psycho-social paradigms of thinking about health, disease, and disability (the overlap of two paradigms within the ‘environmental factors‘ component can be noticed). While the use of such , ‘overlays’‘ is not necessary, they will certainly help the reader systematize their understanding and perspective of the ICF.
Figure 3. Modified diagram of the International Classification of Functioning, Health and Disability (ICF) components. Additionally, the following are marked: 1) two parts of the ICF, i.e. Functioning and Disability and Contextual Factors (on the left) together with their components; 2) ICF components that fit into the biological and psycho-social medical paradigms (the overlap of the two paradigms is visible in the environmental factors component).
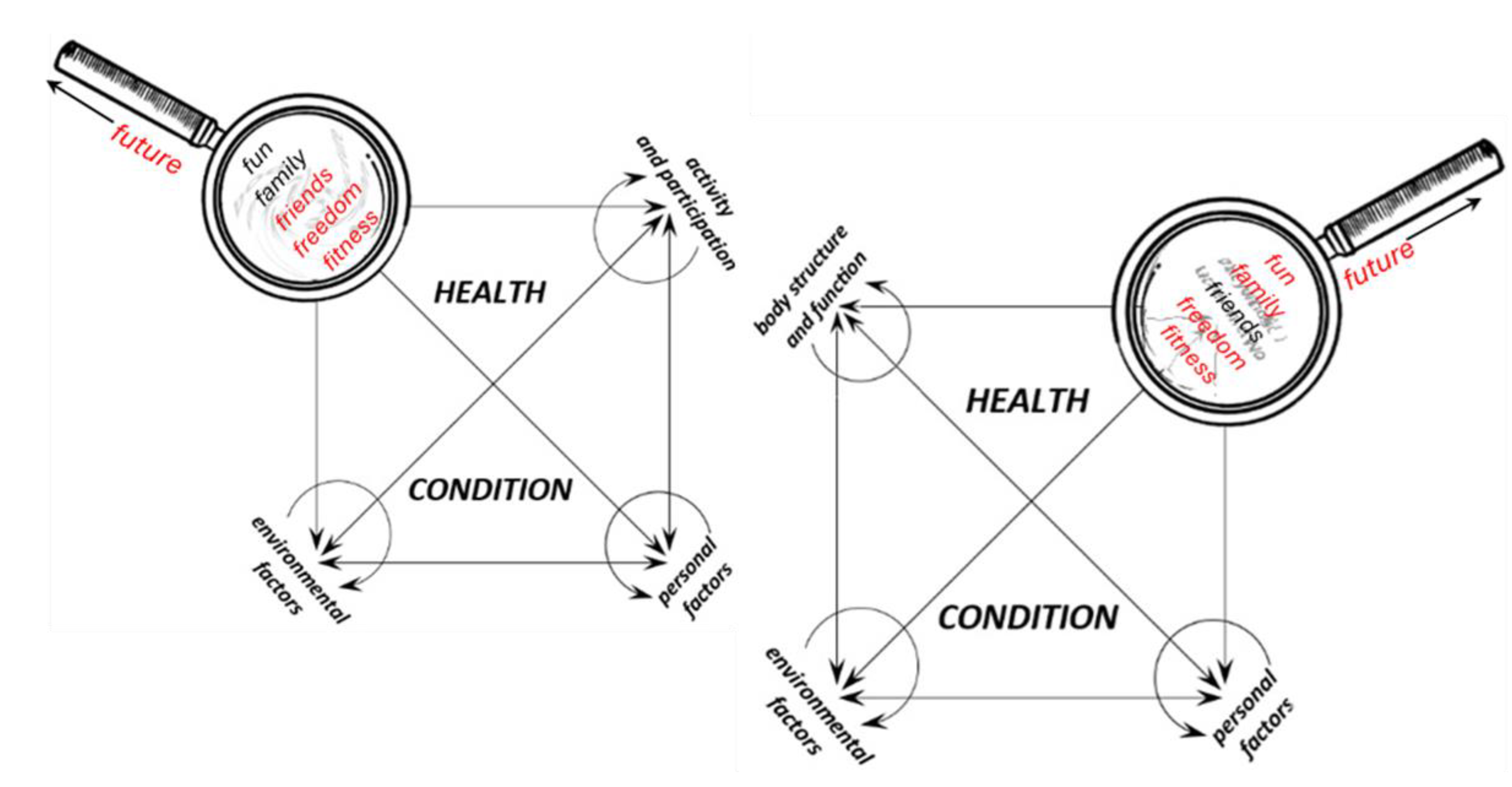
With regard to the F-words, a clearer strategy for integration into the ICF framework is required. Instead of simply substituting ICF components with equivalent F-words, we suggest adopting a dual-layer mapping system. In this approach, the F-words act as a pragmatic overlay that translates the abstract ICF categories into family-centered and practice-friendly concepts. For instance, function could serve as a bridge across both ‘body structures and functions‘ and ‘activities and participation‘ while friends could be directly mapped onto the ‘participation‘ domain. Similarly, family and fun could be anchored within the contextual factors, thereby strengthening the psychosocial dimension of the model (Figure. 4). The final F-word, future has been placed on the handle of the magnifying glass as a general guiding principle for the therapeutic process. It ought to be firmly rooted in the ‘now‘ while focusing on the ‘later‘ aiming – within the existing constraints – to achieve the highest possible level of quality of life and personal happiness [41].
Figure 4.
The method of linking the modified diagram of the International Classification of Functioning, Health and Disability (ICF) components and the F-words concept: 1) based on the ICF, the clinician notices existing deficits; 2) planning the intervention within the body structure and function component, aiming to select appropriate therapeutic measures, the clinician looks at this component through a ‘magnifying glass’, where all the F-words are engraved; 3) different therapeutic measures light up different F-words on the magnifying glass; 4) in the selection process, the clinician prefers those measures that light up the largest number of F-words; 5) the clinician repeats this procedure in the area of other ICF.
Figure 4.
The method of linking the modified diagram of the International Classification of Functioning, Health and Disability (ICF) components and the F-words concept: 1) based on the ICF, the clinician notices existing deficits; 2) planning the intervention within the body structure and function component, aiming to select appropriate therapeutic measures, the clinician looks at this component through a ‘magnifying glass’, where all the F-words are engraved; 3) different therapeutic measures light up different F-words on the magnifying glass; 4) in the selection process, the clinician prefers those measures that light up the largest number of F-words; 5) the clinician repeats this procedure in the area of other ICF.
Such mapping would not replace the ICF but would allow both systems to operate in parallel: the ICF as a standardized classification tool, and the F-words as an accessible framework for clinical practice and communication with families. This dual structure could minimize conceptual overlaps, reduce terminological confusion, and enhance the practical utility of both frameworks. Ultimately, the proposed solution aims to preserve the scientific robustness of the ICF while leveraging the intuitive and motivational appeal of the F-words.
5. Limitations
This review has several limitations that should be acknowledged. First, although the search strategy was conducted in a structured and systematic manner, it is possible that some relevant studies were not identified due to publication bias or the use of search terms that may not have fully captured the breadth of literature related to the ICF and the F-words framework. Second, the included publications were highly heterogeneous with respect to study populations, age groups, and research methodologies, which limits the direct comparability of findings across studies.
Third, much of the existing literature consists of conceptual papers, narrative reviews, and small-scale empirical studies, while robust large-scale and longitudinal investigations remain limited. As a result, the conclusions drawn in this review are necessarily more interpretative than definitive. Finally, this review was restricted to English-language publications, which may have led to the omission of relevant perspectives and findings reported in other languages.
6. Conclusions
The ICF and the F-words framework provide valuable guidance for interdisciplinary teams involved in multidimensional therapeutic processes for children and adolescents with disabilities. Together, they support a shift toward holistic, participation-oriented, and family-centered approaches to pediatric rehabilitation. Despite their recognized conceptual value, both frameworks remain underutilized in everyday clinical practice, a discrepancy that may reflect fragmentation, limited coordination, and the persistence of dogmatic treatment models in pediatric disability care.
Although the ICF and the F-words framework have a long-standing tradition and broad international recognition, they are not free from conceptual and practical limitations. These shortcomings may contribute to misunderstandings, inconsistent implementation, and reluctance among clinicians to adopt them fully in routine practice and in interactions with children and their families. Addressing such barriers is therefore essential to enhance their practical relevance and clinical usability.
The adjustments proposed in this review aim to respond to these challenges by reducing conceptual ambiguity and improving coherence between the two frameworks, without altering their core principles. By preserving the scientific robustness of the ICF and leveraging the accessibility and motivational strengths of the F-words, these modifications may facilitate more consistent application, improve interdisciplinary collaboration, and support more effective, family-centered pediatric rehabilitation practice.
Author Contributions
Conceptualization, A.G. and R.G.; methodology, A.G.; software, J.L.; validation, A.G., A.S. and S.S.; formal analysis, R.G.; investigation, A.G and A.S.; resources, A.G.; data curation, R.G.; writing—original draft preparation, A.G. and R.G.; writing—review and editing, J.L.; visualization, R.G.; supervision, S.S.; project administration, A.S.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ICF | International Classification of Functioning, Disability and Health |
| UNCRPD | United Nations Convention on the Rights of Persons with Disabilities |
| WHO | World Health Organization |
References
- Chagas, P.S.C.; Magalhães, E.D.D.; Sousa Junior, R.R.; Romeros, A.C.S.F.; Palisano, R.J.; Leite, H.R.; Rosenbaum, P. Development of Children, Adolescents, and Young Adults with Cerebral Palsy According to the ICF: A Scoping Review. Dev. Med. Child Neurol. 2023, 65, 745–753. [Google Scholar] [CrossRef]
- Damiano, D.L.; Longo, E.; Carolina de Campos, A.; Forssberg, H.; Rauch, A. Systematic Review of Clinical Guidelines Related to Care of Individuals With Cerebral Palsy as Part of the World Health Organization Efforts to Develop a Global Package of Interventions for Rehabilitation. Arch. Phys. Med. Rehabil. 2021, 102, 1764–1774. [Google Scholar] [CrossRef]
- Dan, B. The ICF as a Socio-Psycho-Biological Model for the Full Participation of Disabled Individuals. Dev. Med. Child Neurol. 2024, 66, 1398–1399. [Google Scholar] [CrossRef]
- Howard, J.J.; Willoughby, K.; Thomason, P.; Shore, B.J.; Graham, K.; Rutz, E. Hip Surveillance and Management of Hip Displacement in Children with Cerebral Palsy: Clinical and Ethical Dilemmas. J. Clin. Med. 2023, 12. [Google Scholar] [CrossRef]
- Longo, E.; Monteiro, R.; Hidalgo-Robles, Á.; Paleg, G.; Shrader, C.; De Campos, A.C. Assigning F-Words as Ingredients of Interventions for Children with Cerebral Palsy Functioning at GMFCS IV and V: A Scoping Review Protocol. Frontiers in rehabilitation sciences 2023, 4. [Google Scholar] [CrossRef] [PubMed]
- NSW Health Management Of Cerebral Palsy In Children: A Guide For Allied Health Professionals; 2018; ISBN 978-1-76000-543-6.
- International Classification of Functioning, Disability and Health; World Health Organization World Health Organization: Geneva, 2001.
- National Institute for Health and Care Excellence (NICE) Spasticity in under 19s: Management. 2016.
- Miller, S.D.; Mayson, T.A.; Mulpuri, K.; O’Donnell, M.E. Developing a Province-Wide Hip Surveillance Program for Children with Cerebral Palsy: From Evidence to Consensus to Program Implementation: A Mini-Review. Journal of Pediatric Orthopaedics Part B 2020, 29, 517–522. [Google Scholar] [CrossRef] [PubMed]
- te Velde, A.; Morgan, C.; Finch-Edmondson, M.; McNamara, L.; McNamara, M.; Paton, M.C.B.; Stanton, E.; Webb, A.; Badawi, N.; Novak, I. Neurodevelopmental Therapy for Cerebral Palsy: A Meta-Analysis. Pediatrics 2022, 149. [Google Scholar] [CrossRef] [PubMed]
- Rutka, M.; Myśliwiec, A.; Wolny, T.; Gogola, A.; Linek, P. Influence of Chest and Diaphragm Manual Therapy on the Spirometry Parameters in Patients with Cerebral Palsy: A Pilot Study. Biomed Res. Int. 2021, 2021. [Google Scholar] [CrossRef]
- Biały, M.; Adamczyk, W.M.; Stranc, T.; Gogola, A.; Gnat, R. The Association between Pelvic Asymmetry and Lateral Abdominal Muscle Activity in a Healthy Population. J. Hum. Kinet. 2025, 97, 77–87. [Google Scholar] [CrossRef]
- Gogola, A.; Gnat, R. Evidence-Based Classification, Assessment, and Management of Pain in Children with Cerebral Palsy : A Structured Review. 2025, 1–18. [Google Scholar] [CrossRef]
- Mys̈liwiec, A.; Saulicz, E.; Kuszewski, M.; Wolny, T.; Knapik, A.; Gogola, A. Self-Evaluation of the Preparation of Physicians and Physiotherapists to Provide Medical Services to People with Intellectual Disability. J. Intellect. Dev. Disabil. 2015, 40, 104–110. [Google Scholar] [CrossRef]
- Rosenbaum, P. Changing the Discourse: We All Must Be Knowledge Brokers. Dev. Med. Child Neurol. 2016, 58, 1204. [Google Scholar] [CrossRef]
- Tempest, S.; Jefferson, R. Engaging with Clinicians to Implement and Evaluate the ICF in Neurorehabilitation Practice. NeuroRehabilitation 2015, 36, 11–15. [Google Scholar] [CrossRef]
- Gogola, A.; Gnat, R.; Snela, S.; Luszawski, J.; Filip, D.; Muzalewski, A.; Paulitsch, F. Effects of Interdisciplinary Therapy in A Patient with Severe Dystonic Cerebral Palsy: A 12-Year Follow-up Case Report. Int. J. Spec. Educ. 2025, 40, 159–170. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Gorter, J.W. The “F-Words” in Childhood Disability: I Swear This Is How We Should Think. Child Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Soper, A.K.; Cross, A.; Rosenbaum, P.; Gorter, J.W. Exploring the International Uptake of the “F-Words in Childhood Disability”: A Citation Analysis. Child Care Health Dev. 2019, 45, 473–490. [Google Scholar] [CrossRef] [PubMed]
- Gogola, A.; Gnat, R. Effects of 12-Week Infant Shantala Massage Program on Maternal Emotional Well-Being Following First-Time Birth. Healthcare 2025, 13, 1895. [Google Scholar] [CrossRef]
- Cross, A.; Rosenbaum, P.; Grahovac, D.; Brocklehurst, J.; Kay, D.; Baptiste, S.; Gorter, J.W. A Web-Based Knowledge Translation Resource for Families and Service Providers (the “f-Words” in Childhood Disability Knowledge Hub): Developmental and Pilot Evaluation Study. JMIR Rehabil. Assist. Technol. 2018, 5, 1–12. [Google Scholar] [CrossRef]
- Soper, A.K.; Cross, A.; Rosenbaum, P.; Gorter, J.W. Service Providers’ Perspectives on Using the ‘F-Words in Childhood Disability’: An International Survey. Phys. Occup. Ther. Pediatr. 2020, 40, 534–545. [Google Scholar] [CrossRef]
- Leonardi, M.; Lee, H.; Kostanjsek, N.; Fornari, A.; Raggi, A.; Martinuzzi, A.; Yáñez, M.; Almborg, A.-H.; Fresk, M.; Besstrashnova, Y.; et al. 20 Years of ICF Uses and Applications around the World. Int. J. Environ. Res. Public Health 2022, 19, 11321. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Namara, M.M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20. [Google Scholar] [CrossRef]
- Badley, E.M. Enhancing the Conceptual Clarity of the Activity and Participation Components of the International Classification of Functioning, Disability, and Health. Soc. Sci. Med. 2008, 66, 2335–2345. [Google Scholar] [CrossRef]
- Madden, R.H.; Bundy, A. The ICF Has Made a Difference to Functioning and Disability Measurement and Statistics. Disabil. Rehabil. 2019, 41, 1450–1462. [Google Scholar] [CrossRef]
- Cieza, A.; Kostansjek, N. The International Classification of Functioning, Disability and Health: The First 20 Years. Dev. Med. Child Neurol. 2021, 63, 363. [Google Scholar] [CrossRef]
- Rosenbaum, P.L.; Novak-Pavlic, M. Parenting a Child with a Neurodevelopmental Disorder. Curr. Dev. Disord. Rep. 2021, 8, 212–218. [Google Scholar] [CrossRef]
- Shanmugarajah, K.; Rosenbaum, P.; Zubairi, M.; Di Rezze, B. A Narrative Review of Function-Focused Measures for Children With Neurodevelopmental Disorders. Frontiers in Rehabilitation Sciences 2021, 2. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, S.K.; Mohammad, A.H.; Ibrahim, A.A.; Abdu, S.I.; Kaka, B. Research Paper: Revisiting the International Classification of Functioning, Disability and Health, a Comprehensive Model for Exploring Disablement in Low and Middleincome Countries: A Narrative Overview. Iranian Rehabilitation Journal 2021, 19, 261–271. [Google Scholar] [CrossRef]
- World Health Organization World Report on Disability; WHO: Geneva, Switzerland, 2011.
- Haslam, S.A.; Haslam, C.; Jetten, J.; Cruwys, T.; Bentley, S. Group Life Shapes the Psychology and Biology of Health: The Case for a Sociopsychobio Model. Soc. Personal. Psychol. Compass 2019, 13, 1–16. [Google Scholar] [CrossRef]
- Jackman, M.; Sakzewski, L.; Morgan, C.; Boyd, R.N.; Brennan, S.E.; Langdon, K.; Toovey, R.A.M.; Greaves, S.; Thorley, M.; Novak, I. Interventions to Improve Physical Function for Children and Young People with Cerebral Palsy: International Clinical Practice Guideline. Dev. Med. Child Neurol. 2022, 64, 536–549. [Google Scholar] [CrossRef] [PubMed]
- United; Nations Convention on the Rights of Persons with Disabilities. In Treaty Series, New York, NY, USA, 2006.
- Liao, H.F.; Hwang, A.W.; Schiariti, V.; Yen, C.F.; Chi, W.C.; Liou, T.H.; Hung, H.C.; Hsieh, Y.H. Validating the ICF Core Set for Cerebral Palsy Using a National Disability Sample in Taiwan. Disabil. Rehabil. 2020, 42, 642–650. [Google Scholar] [CrossRef]
- D’Arcy, E.; Wallace, K.; Chamberlain, A.; Evans, K.; Milbourn, B.; Bölte, S.; Whitehouse, A.J.O.; Girdler, S. Content Validation of Common Measures of Functioning for Young Children against the International Classification of Functioning, Disability and Health and Code and Core Sets Relevant to Neurodevelopmental Conditions. Autism 2022, 26, 928–939. [Google Scholar] [CrossRef]
- Schiariti, V.; Shierk, A.; Stashinko, E.E.; Sukal-Moulton, T.; Feldman, R.S.; Aman, C.; Mendoza-Puccini, M.C.; Brandenburg, J.E. Cerebral Palsy Pain Instruments: Recommended Tools for Clinical Research Studies by the National Institute of Neurological Disorders and Stroke Cerebral Palsy Common Data Elements Project. Dev. Med. Child Neurol. 2024, 66, 610–622. [Google Scholar] [CrossRef]
- Hayden-Evans, M.; Evans, K.; Milbourn, B.; D’Arcy, E.; Chamberlain, A.; Afsharnejad, B.; Whitehouse, A.; Bölte, S.; Girdler, S. Validating the International Classification of Functioning, Disability and Health Core Sets for Autism in a Sample of Australian School-Aged Children on the Spectrum. J. Autism Dev. Disord. 2025, 55, 1424–1437. [Google Scholar] [CrossRef]
- Schiariti, V.; Mahdi, S.; Bölte, S. International Classification of Functioning, Disability and Health Core Sets for Cerebral Palsy, Autism Spectrum Disorder, and Attention-Deficit–Hyperactivity Disorder. Dev. Med. Child Neurol. 2018, 60, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Leite, H.R.; Chagas, P.S. de C.; Rosenbaum, P. Childhood Disability: Can People Implement the F-Words in Low and Middle-Income Countries – and How? Braz. J. Phys. Ther. 2021, 25, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Dan, B. Freedom: An F-Word for Functioning, Disability, and Health. Dev. Med. Child Neurol. 2023, 65, 298. [Google Scholar] [CrossRef]
- Bölte, S. A More Holistic Approach to Autism Using the International Classification of Functioning: The Why, What, and How of Functioning. Autism 2023, 27, 3–6. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The original diagram of the International Classification of Functioning, Health and Disability components presented by the World Health Organisation [7].
Figure 1.
The original diagram of the International Classification of Functioning, Health and Disability components presented by the World Health Organisation [7].
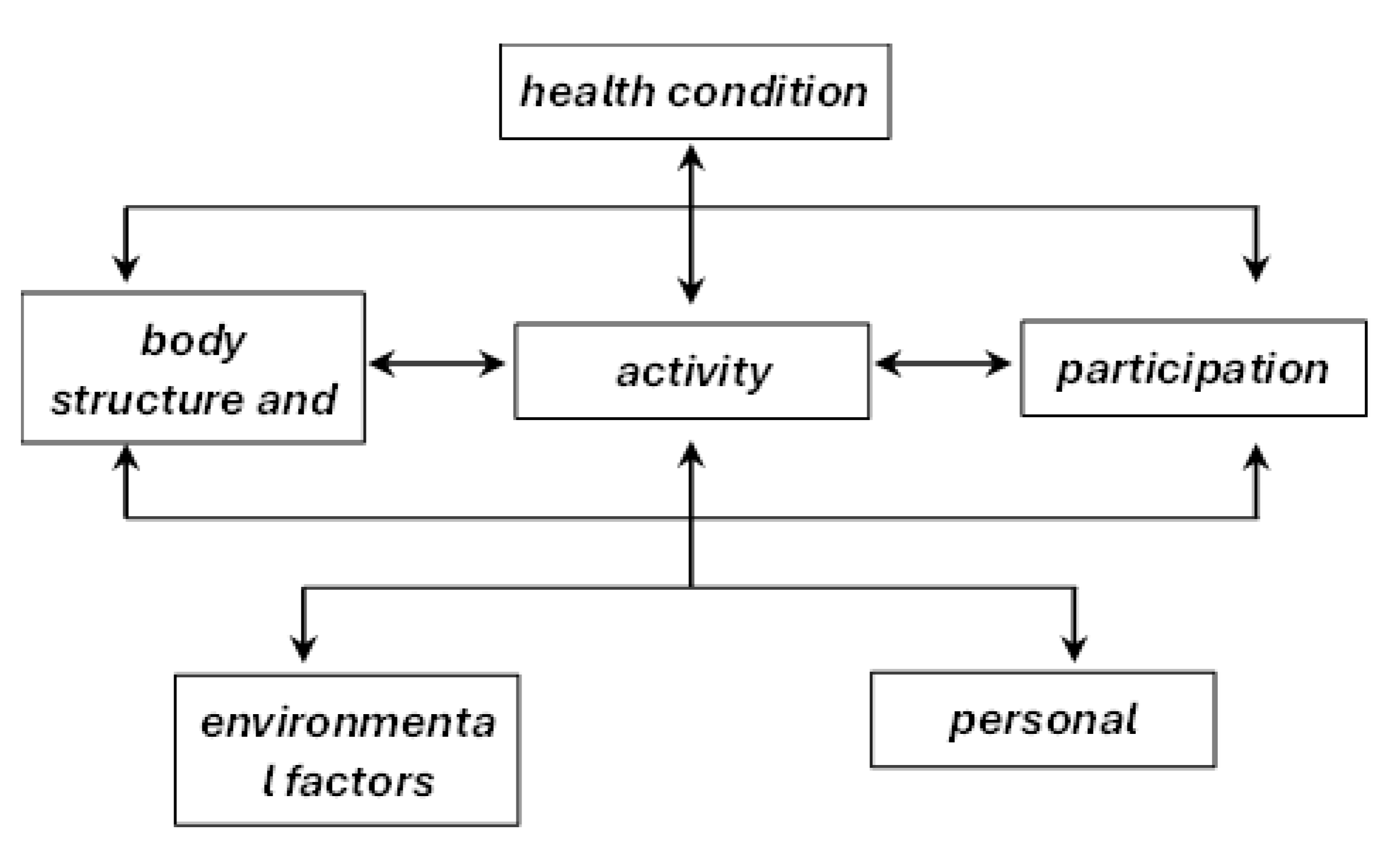

Table 1.
Distribution of included articles by publication type, key authors, and number of publications.
Table 1.
Distribution of included articles by publication type, key authors, and number of publications.
| Publication type | Key authors | Number of articles |
|---|---|---|
| Non-experimental quantitative research | Leonardi et al. (2022)[23] | 1 |
| Systematic reviews | Novak et al., (2020)[24]; Damiano et al. (2021)[2]; | 2 |
| Review articles (scoping, narrative) | Badley (2008)[25]; Rosenbaum & Gorter (2012)[18]; Madden & Bundy, (2019)[26]; Cieza & Kostansjek (2021)[27]; Rosenbaum & Novak-Pavlic (2021)[28]; Shanmugarajah et al. (2021)[29]; Sulaiman et al., 2021)[30]; Longo et al. (2023)[5]; Chagas et al. (2023)[1]; Gogola & Gnat (2025) [13]; | 10 |
| Expert reports | WHO ( 2011) [31] |
1 |
| Theoretical/ conceptual article | Haslam et al., (2019)[32]; | 1 |
| Clinical practice guideline | Jackman et al., (2022)[33]; | 1 |
| International legal treaty | United Nations (2006)[34]; | 1 |
| Validation studies /reports | Cross et al. (2018) [21]; Liao et al. (2020)[35]; D’Arcy et al. (2022)[36]; Schiariti et al. (2020)[37]; Hayden-Evans et al. (2025) [38]; | 5 |
| Descriptive comparative study | Schiariti et al. (2018)[39] | 1 |
| Research studies | Tempest & Jefferson (2015)[16]; Soper et al. (2019, 2020)[19,22]; | 4 |
| Editorials | Leite et al., (2021)[40]; Dan (2023, 2024) [41,3]; Bölte (2023)[42]; | 4 |
| Total | 31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



