Submitted:
04 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
Purpose: To evaluate the safety, feasibility, and functional outcomes of subtenon autologous platelet-rich plasma (PRP) in patients with retinitis pigmentosa (RP) and Extensive Macular Atrophy with Pseudodrusen-like Appearance (EMAP), two degenerative retinal diseases sharing convergent inflammatory and neurodegenerative pathways. Methods: This prospective, comparative pilot study included adult patients diagnosed with RP or EMAP who received three subtenon injections of autologous PRP (1.5 mL per injection) administered at baseline (Month 0), Month 2, and Month 4. Functional outcomes were assessed from baseline to Month 6, with primary endpoints including best-corrected visual acuity (BCVA, logMAR) and visual field preservation, evaluated by the Field Preservation Deviation Index (FPDI) and Mean Deviation (MD) using automated perimetry. Secondary outcomes included 30-Hz flicker electroretinography (ERG) amplitude (phase 1), structural retinal parameters on optical coherence tomography (OCT)—central macular thickness and ellipsoid zone integrity—and ocular safety outcomes, including intraocular pressure and adverse events. Paired analyses were performed, with subgroup comparisons between RP and EMAP. Results: Thirteen patients were included in the analysis. In the overall cohort, mean BCVA showed a mild, non-significant improvement from 0.99 ± 0.71 logMAR at baseline to 0.90 ± 0.51 logMAR at Month 6 (p = 0.283). When stratified by diagnosis, patients with RP (n = 6) demonstrated a statistically significant improvement in BCVA (p = 0.048), whereas patients with EMAP (n = 7) showed functional stability without significant change (p = 0.619). Visual field parameters (MD and FPDI/VFI) remained stable in both groups, with a non-significant trend toward functional preservation, particularly in the RP subgroup. Quantitative paired analysis of flicker ERG amplitude was limited by incomplete data; however, descriptive evaluation demonstrated preservation of measurable responses without evidence of electrophysiological deterioration. Two transient and manageable ocular adverse events were observed (one episode of mild anterior uveitis in an RP patient with prior uveitis history and one episode of acute ocular hypertension in an EMAP patient attributed to an angle-closure mechanism). No infectious complications, sustained inflammation, or permanent ocular morbidity were reported. Conclusions: Subtenon autologous PRP demonstrated a favorable ocular safety profile and was associated with a preferential functional benefit in retinitis pigmentosa, while functional stability was observed in patients with EMAP. These findings suggest that PRP-based regenerative and immunomodulatory therapy may be more effective in degenerative retinal diseases where residual viable retinal cells and functional plasticity are present, as observed in retinitis pigmentosa, while primarily providing stabilizing effects in aggressive macular atrophic phenotypes such as EMAP. Larger, controlled studies with longer follow-up are warranted to further define the role of subtenon PRP in degenerative retinal diseases.
Keywords:
platelet-rich plasma
; subtenon injection
; retinitis pigmentosa
; extensive macular atrophy with pseudodrusen-like appearance (EMAP)
; degenerative retinal diseases
; neuroprotection
; immunomodulation
; regenerative therapy
1. Introduction
Retinal degenerative diseases encompass a heterogeneous group of conditions characterized by progressive photoreceptor loss and irreversible visual impairment. Among these, retinitis pigmentosa (RP) represents the most common inherited retinal dystrophy, while Extensive Macular Atrophy with Pseudodrusen-like Appearance (EMAP) has emerged as a distinct and particularly aggressive degenerative macular phenotype. Despite differences in etiology and clinical presentation, both conditions ultimately converge toward progressive retinal dysfunction and substantial visual disability, for which broadly applicable disease-modifying therapies remain limited [1,2].
Retinitis pigmentosa is a genetically and phenotypically heterogeneous group of inherited retinal dystrophies marked by progressive degeneration of photoreceptors, typically beginning with rod dysfunction and followed by secondary cone involvement [1]. Clinically, this process manifests as nyctalopia, gradual constriction of the visual field, and eventual impairment of central vision in advanced stages. Although recent advances in gene-specific therapies, optogenetics, and cell-based approaches have expanded treatment options for selected molecular subtypes, the majority of patients with RP still lack therapeutic strategies capable of broadly modifying disease progression or preserving visual function across diverse genotypes [2,23].
Extensive Macular Atrophy with Pseudodrusen-like Appearance is a distinct degenerative macular disorder first described by Hamel et al. [3], characterized by early-onset bilateral macular atrophy, pseudodrusen-like deposits extending beyond the posterior pole, progressive loss of the outer retina and retinal pigment epithelium, and marked chorioretinal thinning [3,4]. Unlike classical inherited retinal dystrophies, EMAP primarily affects the macula and follows a rapid and highly predictable course toward severe central vision loss. Multimodal imaging studies have demonstrated extensive involvement of the photoreceptor–RPE–Bruch’s membrane complex, progressive enlargement of atrophic areas, and significant functional decline [4,5,6].
Increasing experimental and clinical data suggest that both RP and EMAP are driven not only by primary degenerative mechanisms but also by sustained para-inflammatory and immune-mediated processes at the level of the outer retina, retinal pigment epithelium, and choroid [8,9]. Dysregulation of microglial activity, oxidative stress, complement activation, and chronic release of inflammatory mediators contribute to secondary neuronal damage, accelerate photoreceptor loss, and amplify structural and functional decline in degenerative retinal diseases [8,9,10,11]. In this context, inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), have been implicated as key modulators of retinal neurodegeneration [10,11,12].
Within this biological framework, autologous platelet-rich plasma (PRP) has emerged as a potential multimodal biologic therapy in regenerative medicine. PRP is a concentrated suspension of platelets in plasma, enriched with endogenous growth factors and cytokines, including platelet-derived growth factor, transforming growth factor-beta, insulin-like growth factor-1, basic fibroblast growth factor, and other bioactive mediators [15,16,17,18]. Collectively, these factors may support retinal homeostasis by modulating inflammatory signaling, enhancing chorioretinal perfusion, stabilizing the extracellular matrix, and promoting cellular survival pathways within the neuroretina and retinal pigment epithelium [15,16,17,18].
In ophthalmology, PRP has been explored in several degenerative and inflammatory ocular conditions. Notably, multiple studies investigating subtenon autologous PRP in retinitis pigmentosa have reported functional stabilization and, in selected cases, modest improvements in best-corrected visual acuity, visual field sensitivity, and electrophysiological parameters [19,20,21,22]. These findings suggest that PRP may act as a biologic modulator of the degenerative retinal microenvironment, rather than a curative intervention, particularly in diseases where residual viable retinal cells and functional plasticity persist.
The subtenon route of administration was selected to allow gradual and sustained diffusion of PRP-derived bioactive factors toward the posterior segment, including the choroid, retinal pigment epithelium, and outer retina, while minimizing the procedural risks associated with intravitreal delivery [17,18]. This approach is particularly suitable for chronic degenerative retinal diseases, in which safety, repeatability, and long-term tolerability are critical considerations.
Accordingly, this prospective, comparative pilot study was designed to investigate the feasibility, ocular safety, and functional outcomes of repeated subtenon administration of autologous PRP in patients with retinitis pigmentosa and EMAP. By integrating multimodal functional assessments—such as best-corrected visual acuity, visual field preservation indices, and electrophysiological testing—with structural imaging biomarkers on optical coherence tomography, the study aims to generate preliminary real-world data to inform the design of future controlled clinical trials evaluating regenerative and immunomodulatory strategies for inherited and degenerative retinal disorders characterized by progressive photoreceptor loss and macular atrophy [23].
2. Materials and Methods
2.1. Study Design and Ethics
This study was designed as a prospective, comparative, open-label pilot clinical study evaluating the safety, feasibility, and functional outcomes of subtenon autologous platelet-rich plasma (PRP) in patients with degenerative retinal diseases, specifically retinitis pigmentosa (RP) and Extensive Macular Atrophy with Pseudodrusen-like Appearance (EMAP).The study was conducted in accordance with the Declaration of Helsinki and national regulations for research involving human subjects. Ethical approval was obtained from the Brazilian National Research Ethics Committee (CONEP)(CAAE: 77066424.0.0000.0317). The protocol was registered at ClinicalTrials.gov (NCT07341919; Unique Protocol ID: RETINA-PRP Study). All participants provided written informed consent prior to enrollment.
2.2. Study Population and Eligibility Criteria
Inclusion Criteria
Participants were eligible if they met all of the following criteria:
- Age ≥ 18 years;
- Clinical diagnosis of retinitis pigmentosa (RP) or EMAP, confirmed by multimodal retinal imaging;
- Best-corrected visual acuity (BCVA) of counting fingers at 1 meter or better (≤ 1.9 logMAR) in the study eye;
- Measurable visual field using iCare COMPASS automated perimetry (10-2 or 24-2 strategy) with acceptable reliability indices;
- Clear ocular media allowing safe periocular injection and high-quality optical coherence tomography (OCT)imaging;
- Ability and willingness to comply with scheduled study visits.
For the electrophysiology subgroup, a recordable baseline 30-Hz flicker electroretinogram (ERG) response (signal-to-noise ratio ≥ 3:1 and amplitude ≥ 3.0 µV) was required; absence of a measurable flicker response did not exclude participation in the main study.
- Exclusion Criteria
Exclusion criteria included:
- Active ocular inflammation or infectious ocular disease;
- Active choroidal neovascularization or other macular diseases unrelated to RP or EMAP;
- Uncontrolled glaucoma (IOP > 21 mmHg despite treatment) or non-related optic neuropathies;
- Significant media opacity impairing imaging quality or injection safety;
- Recent ocular interventions that could confound outcomes (intravitreal therapy, periocular corticosteroid injection, or major intraocular surgery within 3 months);
- Known hypersensitivity to materials used in PRP preparation or injection;
- Coagulopathy or contraindications to periocular injections (platelet count < 100,000/µL or INR > 1.5);
- Pregnancy or breastfeeding;
- Uncontrolled systemic disease or participation in another interventional clinical trial within 3 months prior to enrollment.
2.3. Platelet-Rich Plasma Preparation
All participants underwent standard serological testing and hematologic evaluation prior to blood collection. Autologous PRP was prepared under sterile conditions using a double-spin centrifugation protocol in a closed system. Peripheral venous blood (30–60 mL) was collected into sodium citrate tubes, with an additional EDTA tube obtained for baseline platelet count.
The first centrifugation was performed at 300 × g for 10 minutes, separating plasma and buffy coat from red blood cells. The plasma and buffy coat were transferred to a sterile tube and subjected to a second centrifugation at 640 × g for 10 minutes to concentrate platelets. The supernatant platelet-poor plasma was partially discarded, and the platelet pellet was resuspended in the remaining plasma to obtain the final PRP product. Platelet quantification demonstrated a mean 2.8-fold increase compared with baseline. Microbiological cultures were performed to ensure sterility prior to administration.
2.4. Intervention Protocol
Participants received subtenon injections of autologous PRP at a dose of 1.5 mL per injection, administered in the inferotemporal quadrant under topical anesthesia. The treatment followed a three-dose regimen, with injections at:
- Baseline (Month 0),
- Month 2 (M2),
- Month 4 (M4).
The subtenon route was selected to allow sustained paracrine diffusion of PRP-derived bioactive factors toward the choroid, retinal pigment epithelium, and outer retina, while minimizing risks associated with intravitreal delivery. No additional biological or regenerative ocular therapies were permitted during the study period.
2.5. Clinical Assessments and Follow-Up
Participants underwent standardized clinical, functional, and imaging assessments from baseline to Month 6. Baseline evaluations included BCVA (logMAR), automated visual field testing (iCare COMPASS), OCT assessment of central macular thickness and ellipsoid zone integrity, and intraocular pressure (IOP) measurement. When available, 30-Hz flicker ERG was performed to assess macular cone function.
Safety visits were conducted 7–14 days after each PRP injection to monitor adverse events, including slit-lamp examination, fundus evaluation, and IOP measurement. Comprehensive functional and structural evaluations were repeated at Month 6, which served as the primary endpoint for outcome analysis.
2.6. Outcome Measures
The primary outcome measures were changes in:
- Best-corrected visual acuity (BCVA, logMAR);
- Visual field preservation, assessed by Field Preservation Deviation Index (FPDI) and Mean Deviation (MD).
- When FPDI was unavailable, the Visual Field Index (VFI) was used as a surrogate.Secondary outcomes included:
- 30-Hz flicker ERG amplitude (phase 1, µV);
- Structural OCT parameters (central macular thickness and ellipsoid zone length);
- Safety outcomes, including IOP changes and ocular adverse events.
- Spectral-domain optical coherence tomography (SD-OCT) was performed at baseline and Month 6 to evaluate macular structure and to exclude confounding or safety-related retinal changes. OCT assessment included screening for cystoid macular edema (CME), choroidal neovascularization (CNV), central macular thickness, and qualitative evaluation of ellipsoid zone (EZ) integrity. Patients with active CME or CNV were excluded from enrollment. Throughout the study period, no new-onset CME or CNV was detected. Ellipsoid zone abnormalities were common at baseline and were considered reflective of underlying disease severity rather than treatment-related effects.
2.7. Statistical Analysis
Continuous variables are presented as mean ± standard deviation or median with interquartile range, as appropriate. Normality was assessed using the Shapiro–Wilk test. Paired comparisons between baseline and follow-up were performed using the paired t-test or Wilcoxon signed-rank test. Subgroup analyses were conducted according to diagnosis (RP vs. EMAP). Between-group comparisons of change scores were assessed using the Mann–Whitney U test, and correlations with age were evaluated using Spearman’s rank correlation coefficient. Due to the exploratory nature of this pilot study, no adjustment for multiple comparisons was applied. A two-sided p value < 0.05 was considered statistically significant.
3. Results
3.1. Study Population
A total of 13 patients with degenerative retinal diseases were included in the analysis, comprising 6 patients with retinitis pigmentosa (RP) and 7 patients with Extensive Macular Atrophy with Pseudodrusen-like Appearance (EMAP). All participants completed the planned treatment protocol consisting of three subtenon injections of autologous platelet-rich plasma (PRP) and had at least one post-treatment follow-up visit. Paired best-corrected visual acuity (BCVA) data were available for all 13 patients, paired visual field data for 9 patients, and partial electrophysiological data for a subset of patients.
The overall study design and follow-up schedule are summarized in Figure 1, illustrating the prospective, comparative framework, treatment timeline, and outcome assessments from baseline to Month 6 in patients with retinitis pigmentosa (RP) and Extensive Macular Atrophy with Pseudodrusen-like Appearance (EMAP).
3.2. Best-Corrected Visual Acuity
In the overall cohort, mean BCVA improved from 0.99 ± 0.71 logMAR at baseline to 0.90 ± 0.51 logMAR at Month 6, although this change did not reach statistical significance (p = 0.283).
When stratified by diagnosis, patients with retinitis pigmentosa (RP) demonstrated a statistically significant improvement in BCVA, with mean values improving from 1.01 ± 0.75 logMAR at baseline to 0.92 ± 0.68 logMAR at Month 6 (p = 0.048). In contrast, patients with EMAP showed functional stability, with mean BCVA changing from 0.97 ± 0.74 logMAR to 0.88 ± 0.36 logMAR, without a statistically significant difference (p = 0.619).
The magnitude of BCVA change (ΔlogMAR) did not differ significantly between RP and EMAP groups (p = 0.942).
Individual trajectories of best-corrected visual acuity (BCVA), expressed in logMAR, are shown in Figure 2A for the overall cohort, demonstrating marked inter-individual variability with a predominance of functional stability and mild improvement over the 6-month follow-up period.
When stratified by diagnosis, patients with retinitis pigmentosa exhibited a consistent trend toward visual acuity improvement or stabilization, as illustrated in Figure 2B, whereas patients with EMAP showed predominantly stable BCVA trajectories without consistent functional gains (Figure 2C). These individual patterns are further summarized by the distribution of BCVA change (ΔlogMAR) in Figure 3, which demonstrates a shift toward negative ΔlogMAR values (indicating improvement) in the RP group, while the EMAP group clustered closer to zero, consistent with functional stability.
3.3. Visual Field Outcomes
Paired automated visual field data were available for 9 patients. In the overall cohort, mean deviation (MD) showed a small, non-significant improvement from –10.83 ± 8.78 dB at baseline to –10.23 ± 8.69 dB at Month 6 (p = 0.352).
Visual field preservation was primarily assessed using the Field Preservation Deviation Index (FPDI). When FPDI was unavailable, the Visual Field Index (VFI) was used as a surrogate, as both indices represent the percentage of preserved visual field function. In the overall cohort, mean FPDI/VFI increased from 63.17% at baseline to 65.00% at follow-up, corresponding to a mean change of +1.83 percentage points, which was not statistically significant (p = 0.597).
Visual field preservation, assessed using the Field Preservation Deviation Index (FPDI) or Visual Field Index (VFI) when FPDI was unavailable, is summarized in Figure 4. In the overall cohort, mean FPDI/VFI values remained stable from baseline to Month 6. Subgroup analysis suggested a modest trend toward improved visual field preservation in RP, whereas EMAP patients demonstrated stable visual field indices, with no evidence of accelerated deterioration during follow-up.
Subgroup analysis revealed that patients with RP (n = 3 with paired data) exhibited an increase in mean FPDI/VFI from 51.33% to 58.33% (mean Δ = +7.0 percentage points), although this change did not reach statistical significance (p = 0.250). Patients with EMAP (n = 6) showed no improvement, with mean FPDI/VFI changing from 69.08% to 68.33%(mean Δ = –0.75 percentage points; p = 0.874).
Between-group comparisons of change scores for MD and FPDI/VFI did not demonstrate statistically significant differences between RP and EMAP (p = 0.381 and p = 0.517, respectively).
3.4. Electrophysiological Outcomes
Electrophysiological assessment using 30-Hz flicker electroretinography (ERG) was available only as incomplete paired data, precluding formal longitudinal inferential analysis. Descriptive evaluation demonstrated mean baseline amplitudes of 3.81 ± 4.19 µV (phase 1) and 5.26 ± 4.45 µV (phase 2), compared with post-treatment means of 3.16 ± 2.99 µV and 3.96 ± 3.43 µV, respectively. No qualitative evidence of electrophysiological deterioration or loss of recordable responses was observed during follow-up.
3.5. Safety and Adverse Events
Spectral-domain optical coherence tomography (SD-OCT) analysis demonstrated no evidence of treatment-emergent cystoid macular edema (CME) or choroidal neovascularization (CNV) in any treated eye throughout the follow-up period. All patients included in the analysis were free of active CME or CNV at baseline, and this structural stability was maintained at Month 6. Central macular thickness showed no clinically meaningful changes at the group level. Ellipsoid zone (EZ) abnormalities were frequently observed at baseline in both retinitis pigmentosa and EMAP patients, reflecting advanced outer retinal involvement; however, no qualitative worsening or new disruption of the EZ attributable to treatment was identified during follow-up.
Two ocular adverse events were recorded during the follow-up period. One patient with RP developed mild anterior uveitis approximately three weeks after PRP injection; this patient had a documented history of HLA-B27–associated uveitis. The inflammatory episode resolved completely with topical corticosteroid therapy and did not recur.
One patient with EMAP experienced acute ocular hypertension (intraocular pressure of 40 mmHg) approximately 10 days after treatment, without signs of intraocular inflammation. The episode occurred during travel and was managed with short-term oral acetazolamide, followed by laser peripheral iridotomy. Intraocular pressure subsequently normalized and remained stable without ongoing treatment. This event was attributed to a primary angle-closure mechanism, rather than a direct inflammatory or toxic effect of PRP.
No additional ocular or systemic adverse events were observed. Overall, subtenon PRP injection demonstrated a favorable safety profile, with adverse events being infrequent, transient, and manageable, and without evidence of sustained ocular morbidity.
4. Discussion
In this prospective comparative pilot study, subtenon autologous platelet-rich plasma (PRP) was associated with a preferential functional benefit in patients with retinitis pigmentosa (RP), particularly in best-corrected visual acuity, whereas patients with Extensive Macular Atrophy with Pseudodrusen-like Appearance (EMAP) demonstrated functional stability without significant improvement. These differential responses likely reflect fundamental differences in disease biology, residual retinal viability, and functional plasticity between the two conditions, despite shared downstream degenerative and inflammatory mechanisms.
4.1. Differential Biological Substrate in RP and EMAP
Retinitis pigmentosa is primarily characterized by progressive photoreceptor degeneration, initially affecting rods and subsequently cones, while substantial portions of the inner retinal architecture and retinal pigment epithelium (RPE) may remain structurally preserved for prolonged periods, particularly in earlier and intermediate stages of the disease [1,2]. Importantly, experimental and clinical evidence suggests that photoreceptor dysfunction often precedes irreversible cell loss, creating a therapeutic window during which neurotrophic and immunomodulatory interventions may partially restore or stabilize retinal function [2,23].
In contrast, EMAP is defined by early-onset bilateral macular atrophy, widespread pseudodrusen-like deposits, and early involvement of the RPE–Bruch’s membrane–choriocapillaris complex, leading to irreversible structural loss at the macular level [3,4,5,6]. Longitudinal imaging studies have demonstrated rapid enlargement of atrophic areas and predictable progression toward severe central vision loss [4,5,6]. In this context, therapeutic strategies relying primarily on cellular rescue or metabolic modulation, rather than tissue replacement, are inherently limited in their capacity to produce measurable short-term functional gains.
4.2. Mechanistic Rationale for PRP Effects in RP
PRP contains a complex mixture of growth factors, cytokines, and bioactive molecules, including platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), insulin-like growth factor-1 (IGF-1), vascular endothelial growth factor (VEGF), and other mediators with neurotrophic, anti-apoptotic, and immunomodulatory properties [15,16,17,18]. Beyond angiogenic effects, these factors modulate inflammatory signaling, enhance cellular metabolism, and support synaptic function, which may be particularly relevant in degenerative retinal diseases characterized by chronic cellular stress rather than complete tissue loss [9,10,17].
In RP, chronic low-grade inflammation, oxidative stress, mitochondrial dysfunction, and microglial activation have been identified as secondary drivers of disease progression, independent of the primary genetic defect [8,9,10,11]. By modulating the retinal microenvironment, subtenon PRP may reduce inflammatory signaling, improve metabolic coupling, and enhance the functional performance of surviving photoreceptors and downstream retinal circuits. This mechanism is consistent with the statistically significant improvement in BCVA observed in the RP subgroup, despite the absence of marked changes in visual field indices or electrophysiological parameters over the relatively short follow-up period.
4.3. Limited Functional Plasticity in EMAP
The lack of measurable functional improvement observed in EMAP patients likely reflects the advanced structural compromise of the macula, where the therapeutic target—viable photoreceptors and RPE cells—is substantially reduced or absent [3,4,5,6]. Although PRP-mediated modulation of inflammation or choroidal perfusion could theoretically slow disease progression, such effects may not translate into short-term improvements detectable by visual acuity or automated perimetry.
Importantly, the functional stability observed in EMAP patients in this cohort may still represent a clinically meaningful outcome, given the typically aggressive and relentless natural history of macular atrophy in this condition [4,5,6]. However, longer follow-up periods and quantitative structural endpoints, such as atrophy area progression and ellipsoid zone mapping, would be required to determine whether PRP exerts a true disease-modifying effect in EMAP.
The differential functional response observed between retinitis pigmentosa and EMAP is visually reinforced by the BCVA trajectory plots (Figures 2A–C) and the distribution of ΔlogMAR values (Figure 3). While RP patients demonstrated a preferential functional benefit, EMAP patients showed stability rather than improvement, likely reflecting fundamental differences in residual retinal viability and functional plasticity between these two degenerative phenotypes.
Visual field data (Figure 4) further support this interpretation, as functional field preservation was maintained in both groups, with a tendency toward greater functional reserve in RP. Importantly, the absence of visual field deterioration in EMAP patients may itself represent a clinically meaningful outcome given the aggressive and predictable natural history of macular atrophy in this condition.
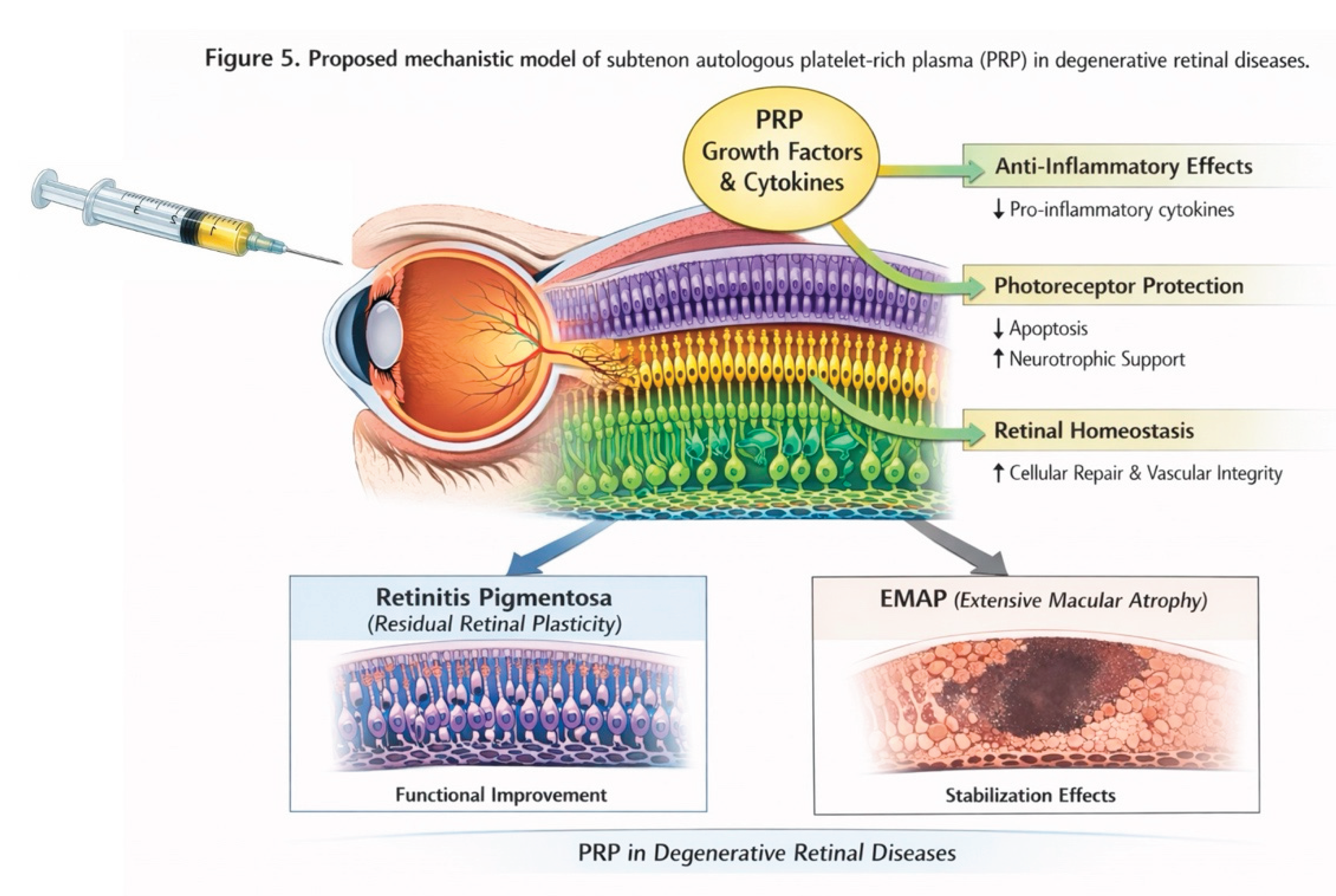
The proposed biological rationale underlying these observations is summarized schematically in Figure 5, which illustrates a mechanistic model in which subtenon autologous platelet-rich plasma delivers growth factors and cytokines that modulate inflammatory signaling, enhance photoreceptor survival pathways, and support retinal homeostasis. In diseases characterized by residual retinal plasticity, such as RP, these mechanisms may translate into measurable functional improvement, whereas in advanced macular atrophic phenotypes such as EMAP, the predominant effect may be stabilization rather than recovery.
Taken together, the concordance between individual functional trajectories (Figures 2A–C), group-level change distributions (Figure 3), visual field preservation (Figure 4), and the proposed mechanistic framework (Figure 5) strengthens the internal consistency of the findings and supports the biological plausibility of subtenon PRP as a regenerative and immunomodulatory strategy in degenerative retinal diseases.
4.4. Functional Outcomes Versus Structural and Electrophysiological Measures
The dissociation observed between functional improvement (BCVA) and the absence of significant changes in visual field indices or flicker ERG amplitude highlights a common feature of early-phase regenerative or modulatory therapies. Functional gains may reflect enhanced neural efficiency, synaptic transmission, or metabolic support, rather than increases in photoreceptor number or global retinal output [13,14].
Electrophysiological measures such as 30-Hz flicker ERG may lack sensitivity in advanced degenerative states or small cohorts, particularly when baseline amplitudes are already markedly reduced [13,14]. Therefore, the absence of significant ERG changes should not be interpreted as evidence of therapeutic inefficacy, especially in exploratory studies.
4.5. Safety Considerations
Subtenon PRP injection demonstrated a favorable ocular safety profile in this cohort. The two adverse events observed were transient and manageable: one episode of mild anterior uveitis occurred in a patient with known HLA-B27–associated uveitis, and one episode of acute ocular hypertension in an EMAP patient was attributed to a pre-existing angle-closure mechanism rather than a direct inflammatory or toxic effect of PRP. No cases of infectious complications, sustained inflammation, or permanent ocular morbidity were observed. These findings are consistent with prior reports on the ocular use of autologous PRP and support the procedural safety and tolerability of the subtenon route [15,16,17,18,19,20,21,22].
The absence of treatment-emergent cystoid macular edema (CME) or choroidal neovascularization (CNV) on serial OCT examinations further supports the structural safety of repeated subtenon PRP administration in degenerative retinal diseases. OCT is a sensitive modality for detecting subclinical inflammatory, exudative, or angiogenic changes that could confound functional outcomes or indicate treatment-related toxicity. In both RP and EMAP, CME and CNV are recognized as potential secondary complications capable of independently affecting visual acuity and visual field performance, particularly in advanced disease stages [5,6]. The maintenance of macular structural stability throughout follow-up suggests that PRP did not exacerbate inflammatory or neovascular pathways. Ellipsoid zone (EZ) abnormalities were frequently present at baseline, reflecting established photoreceptor and outer retinal damage consistent with the natural history of both RP and EMAP [3,4,5,6,13,14]. Importantly, no qualitative worsening or new EZ disruption attributable to treatment was observed, supporting the interpretation that functional changes detected in this study likely reflect modulation of retinal physiology and microenvironment rather than structural regeneration or accelerated degeneration.
4.6. Limitations and Future Directions
This study has several limitations, including the small sample size, heterogeneity of disease stage, and absence of a control group, which limit definitive conclusions regarding efficacy. Nevertheless, the consistent directionality of visual acuity improvement in RP, coupled with strong biological plausibility and a favorable safety profile, provides a compelling rationale for further investigation.
Future studies should prioritize larger, controlled trial designs, longer follow-up durations, and the incorporation of quantitative structural biomarkers (e.g., macular atrophy area, ellipsoid zone mapping, fundus autofluorescence), as well as inflammatory and molecular profiling, to better define patient subgroups most likely to benefit from PRP-based therapies [23]. Exploration of combination strategies, integrating PRP with gene-independent neuroprotective or regenerative approaches, may further enhance therapeutic potential in degenerative retinal diseases.
5. Conclusions
In summary, this prospective comparative pilot study suggests that subtenon autologous PRP may confer a preferential functional benefit in retinitis pigmentosa, a condition characterized by residual viable retinal cells and functional plasticity, while providing functional stability in patients with EMAP, an aggressive macular atrophic phenotype dominated by irreversible structural loss. These findings support continued investigation of PRP as a regenerative and immunomodulatory strategy in degenerative retinal diseases and highlight the importance of disease-specific biological context in therapeutic response.
Author Contributions
Conceptualization: R.C.S.; Methodology: R.C.S., C.C.B.; Investigation: R.C.S., A.C.J.S., J.R.S., M.A.B., L.M.A., C.M.O., T.S.P., P.F.C.; Data Curation: R.C.S., C.C.B.; Formal Analysis: R.C.S.; Writing – Original Draft Preparation: R.C.S.; Writing – Review & Editing: R.C.S., C.C.B.; Supervision: R.C.S.; Project Administration: R.C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Brazilian National Research Ethics Committee (CONEP)(CAAE: 77066424.0.0000.0317).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available from the corresponding author upon reasonable request. The data are not publicly available due to ethical and privacy restrictions involving human participants.
Acknowledgments
The authors acknowledge the technical support provided by Criovida – Cell Biotechnology Center (Fleury Group, Brazil) in platelet-rich plasma processing and quality control procedures.
Conflicts of Interest
The authors declare no conflict of interest.
Clinical Trial Registration
This study was registered at ClinicalTrials.gov (Identifier: NCT07341919; Unique Protocol ID: RETINA-PRP Study).
References
- Hartong, DT; Berson, EL; Dryja, TP. Retinitis pigmentosa. Lancet 2006, 368(9549), 1795–1809. [Google Scholar] [CrossRef]
- Dias, MF; Joo, K; Kemp, JA; et al. Molecular genetics and emerging therapies for retinitis pigmentosa. Prog Retin Eye Res. 2018, 63, 107–131. [Google Scholar] [CrossRef]
- Hamel, CP; Defoort-Dhellemmes, S; Bron, A; et al. Extensive macular atrophy with pseudodrusen-like appearance: a new clinical and angiographic entity. Ophthalmology 2009, 116(4), 770–778. [Google Scholar] [CrossRef]
- Gliem, M; Hendig, D; Finger, RP; et al. Reticular pseudodrusen in eyes with extensive macular atrophy with pseudodrusen-like appearance. Retina 2013, 33(6), 1151–1158. [Google Scholar]
- Spaide, RF. Subretinal drusenoid deposits (reticular pseudodrusen): pathology and clinical significance. Retina 2010, 30(10), 1441–1451. [Google Scholar] [CrossRef] [PubMed]
- Balaratnasingam, C; et al. Progression of reticular pseudodrusen: a spectral domain OCT analysis. Invest Ophthalmol Vis Sci. 2014, 55(8), 5199–5205. [Google Scholar]
- Zarranz-Ventura, J; et al. Adalimumab for sight-threatening uveitis in patients with juvenile idiopathic arthritis. Br J Ophthalmol. 2014, 98(6), 736–741. [Google Scholar]
- Whitcup, SM; et al. Inflammation in retinal disease. Int J Inflam. 2013, 2013, 724648. [Google Scholar] [CrossRef] [PubMed]
- Parmeggiani, F; et al. Inflammation in retinal degenerations: epidemiology, pathogenetic role, and therapeutic implications. Prog Retin Eye Res. 2012, 31(5), 482–518. [Google Scholar]
- Rutar, M; Natoli, R; Provis, JM. Small interfering RNA targeting tumor necrosis factor-α in retinal microglia suppresses experimental photoreceptor degeneration. J Neuroinflammation 2012, 9, 221. [Google Scholar] [CrossRef]
- Siqueira, RC; Brandão, CC. The role of cytokines in degenerative retinal diseases: a comprehensive review. Biomedicines 2025, 13(7), 1724. [Google Scholar] [CrossRef] [PubMed]
- Forooghian, F; et al. TNF inhibition in the treatment of retinal disease: current status and future prospects. Eye 2010, 24(5), 747–753. [Google Scholar]
- Robson, AG; et al. Pattern and flicker ERGs in retinal and optic nerve disorders: diagnostic insights and applications. Prog Retin Eye Res. 2020, 79, 100859. [Google Scholar]
- Binns, AM; et al. Changes in implicit time of the cone flicker ERG in retinal degeneration. Doc Ophthalmol. 2012, 124(1), 1–12. [Google Scholar]
- Anitua, E; et al. Autologous platelet lysates for the treatment of ocular surface disorders. Curr Eye Res. 2016, 41(7), 873–882. [Google Scholar]
- López-Plandolit, S; et al. Autologous platelet-rich plasma eye drops in neurotrophic keratitis. Cornea 2011, 30(12), 1428–1430. [Google Scholar]
- Alio, JL; Arnalich-Montiel, F; Rodriguez, AE. The role of eye platelet-rich plasma in ophthalmology. Curr Pharm Biotechnol. 2012, 13(7), 1257–1265. [Google Scholar] [CrossRef]
- Arnalich, F; et al. Solid platelet-rich plasma in corneal surgery. Ophthalmol Ther. 2016, 5(1), 31–45. [Google Scholar] [CrossRef]
- Arslan, U; Özmert, E. Management of retinitis pigmentosa via platelet-rich plasma. Adv Ther. 2020, 37(5), 2390–2412. [Google Scholar] [CrossRef]
- Kahraman, N; Oner, A. Subtenon injection of autologous platelet-rich plasma in retinitis pigmentosa. Open J Ophthalmol. 2020, 10, 77–88. [Google Scholar] [CrossRef]
- Sahli, E; Arslan, U; Özmert, E; İdil, A. Subtenon autologous platelet-rich plasma injections in retinitis pigmentosa. Regen Med. 2021, 16(2), 131–143. [Google Scholar] [CrossRef] [PubMed]
- Sahli, E; Özmert, E; Günel, MD; Atilla, H. Factors affecting response to PRP therapy in retinitis pigmentosa. Int Ophthalmol. 2024, 44(1), 388. [Google Scholar] [CrossRef] [PubMed]
- Scholl, HPN; Strauss, RW; Singh, MS; et al. Emerging therapies for inherited retinal degeneration. Sci Transl Med. 2016, 8(368), 368rv6. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study design of a prospective, comparative, open-label pilot study evaluating the safety, feasibility, and functional outcomes of subtenon autologous platelet-rich plasma (PRP) in patients with degenerative retinal diseases. Two diagnostic groups were included: retinitis pigmentosa (RP; n = 6) and extensive macular atrophy with pseudodrusen-like appearance (EMAP; n = 7). All participants received three subtenon PRP injections (1.5 mL each) at baseline (M0), Month 2 (M2), and Month 4 (M4). Functional and structural outcomes were assessed from baseline to Month 6 (M6).
Figure 1.
Study design of a prospective, comparative, open-label pilot study evaluating the safety, feasibility, and functional outcomes of subtenon autologous platelet-rich plasma (PRP) in patients with degenerative retinal diseases. Two diagnostic groups were included: retinitis pigmentosa (RP; n = 6) and extensive macular atrophy with pseudodrusen-like appearance (EMAP; n = 7). All participants received three subtenon PRP injections (1.5 mL each) at baseline (M0), Month 2 (M2), and Month 4 (M4). Functional and structural outcomes were assessed from baseline to Month 6 (M6).
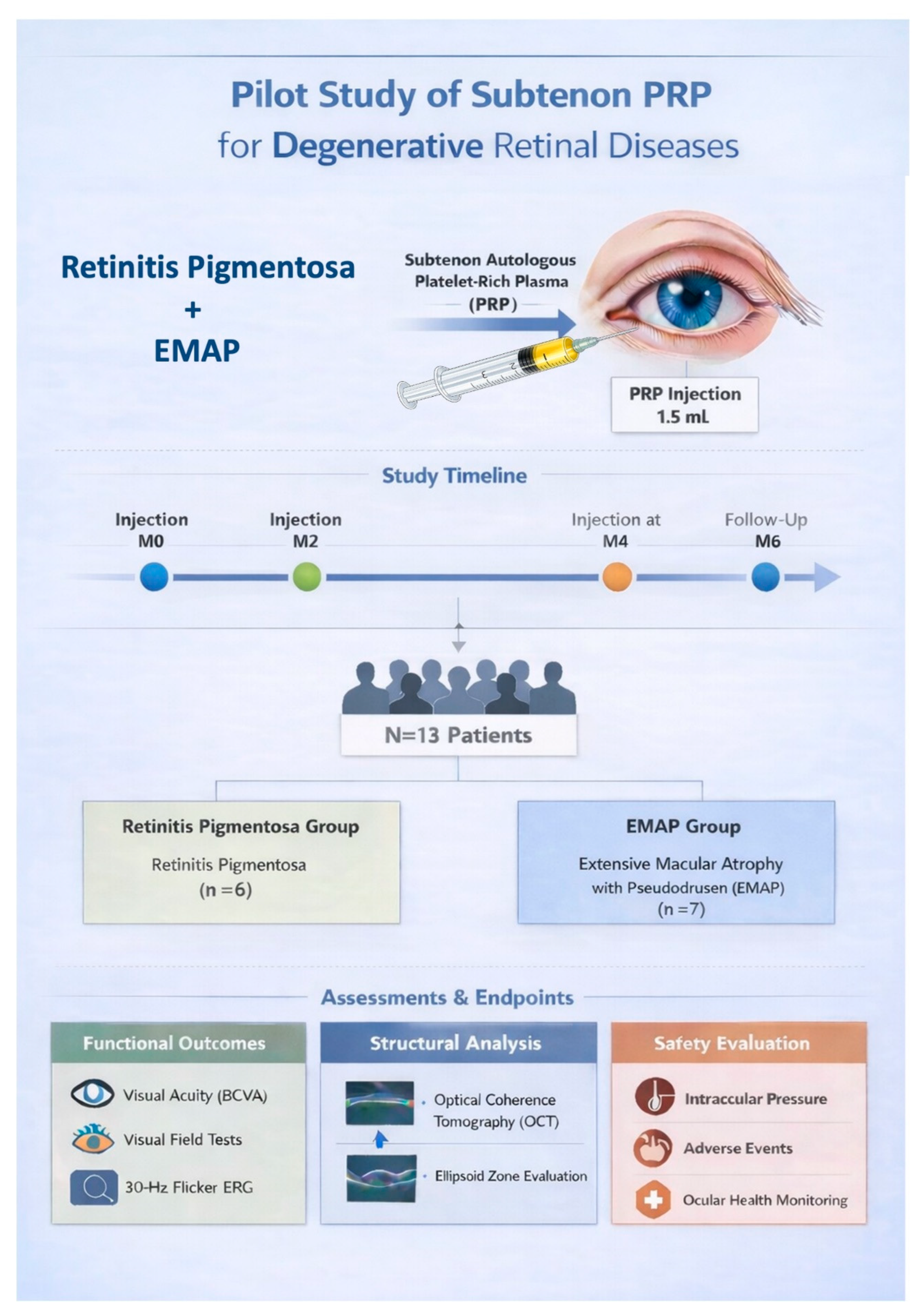
Figure 2.
A. Individual pre–post trajectories (spaghetti plot) of best-corrected visual acuity (BCVA), expressed in logMAR, in the overall cohort following subtenon autologous platelet-rich plasma (PRP) injections. Each line represents one patient, illustrating individual variability and overall functional trends from baseline to Month 6.
Figure 2.
A. Individual pre–post trajectories (spaghetti plot) of best-corrected visual acuity (BCVA), expressed in logMAR, in the overall cohort following subtenon autologous platelet-rich plasma (PRP) injections. Each line represents one patient, illustrating individual variability and overall functional trends from baseline to Month 6.
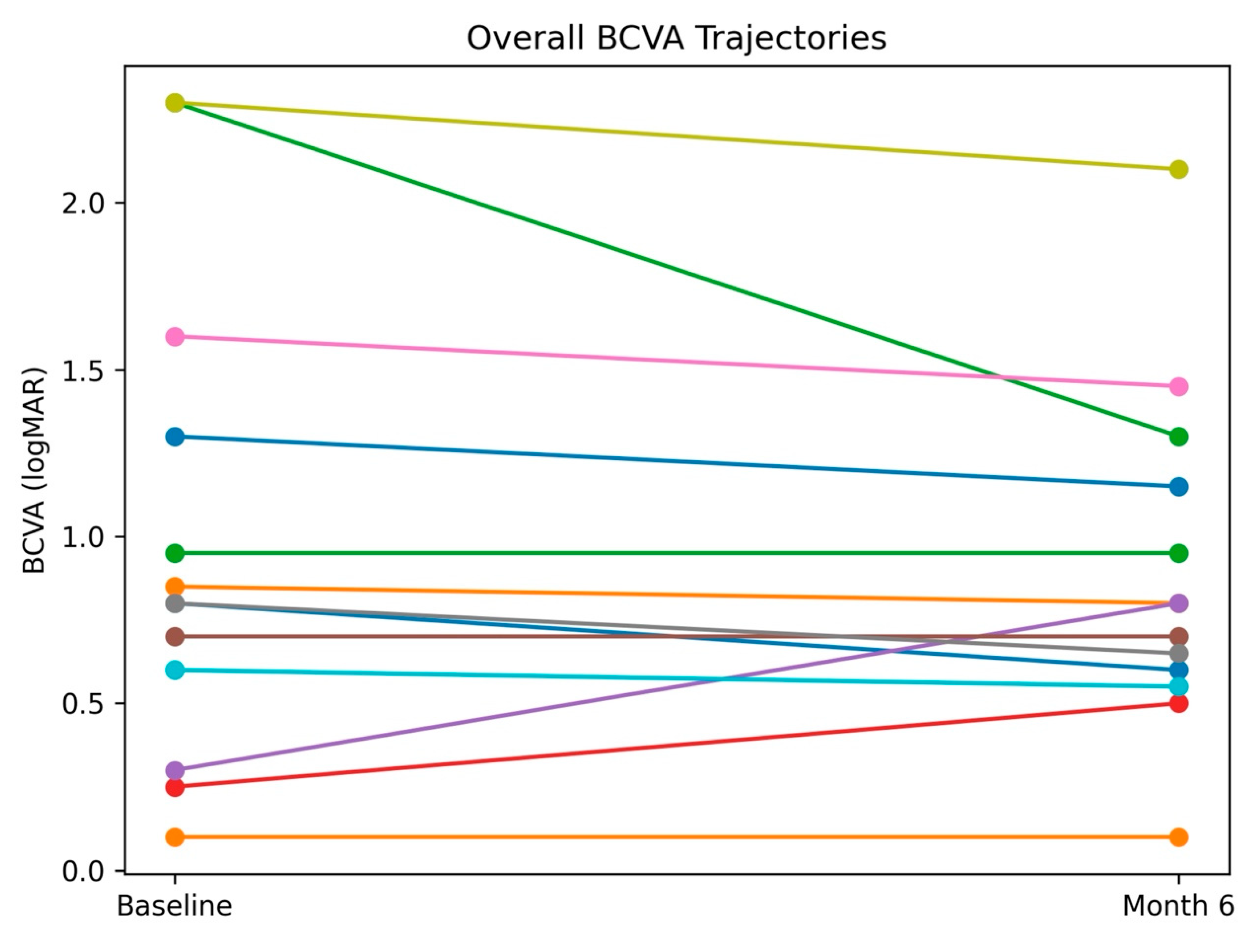
Figure 2.
B. Individual pre–post trajectories of best-corrected visual acuity (BCVA, logMAR) in patients with retinitis pigmentosa (RP) treated with subtenon autologous platelet-rich plasma. Most patients demonstrated functional stability or mild improvement over the 6-month follow-up period.
Figure 2.
B. Individual pre–post trajectories of best-corrected visual acuity (BCVA, logMAR) in patients with retinitis pigmentosa (RP) treated with subtenon autologous platelet-rich plasma. Most patients demonstrated functional stability or mild improvement over the 6-month follow-up period.
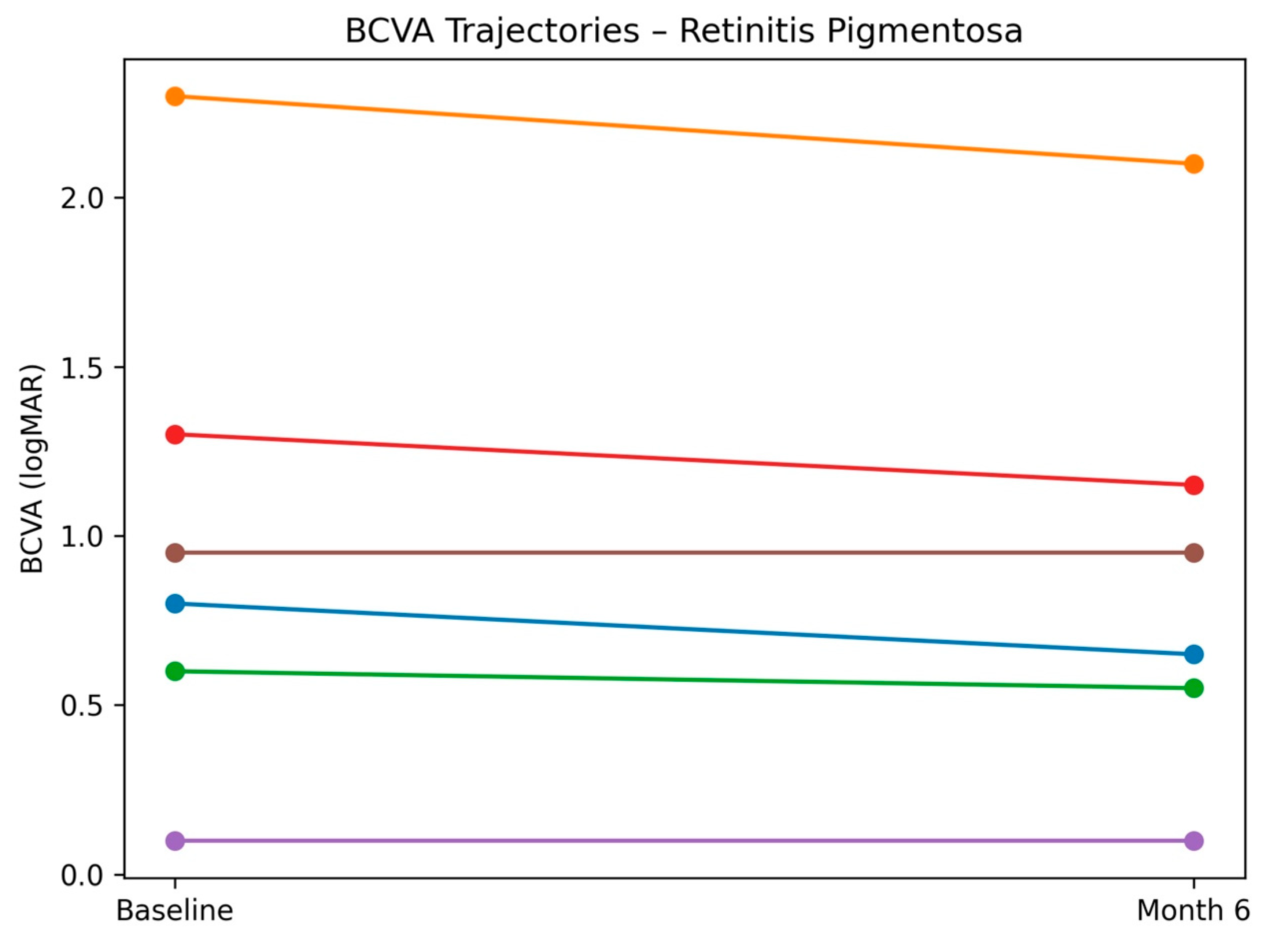
Figure 2.
C. Individual pre–post trajectories of best-corrected visual acuity (BCVA, logMAR) in patients with extensive macular atrophy with pseudodrusen-like appearance (EMAP) treated with subtenon autologous platelet-rich plasma. Visual acuity remained predominantly stable, consistent with the aggressive atrophic nature of the disease.
Figure 2.
C. Individual pre–post trajectories of best-corrected visual acuity (BCVA, logMAR) in patients with extensive macular atrophy with pseudodrusen-like appearance (EMAP) treated with subtenon autologous platelet-rich plasma. Visual acuity remained predominantly stable, consistent with the aggressive atrophic nature of the disease.
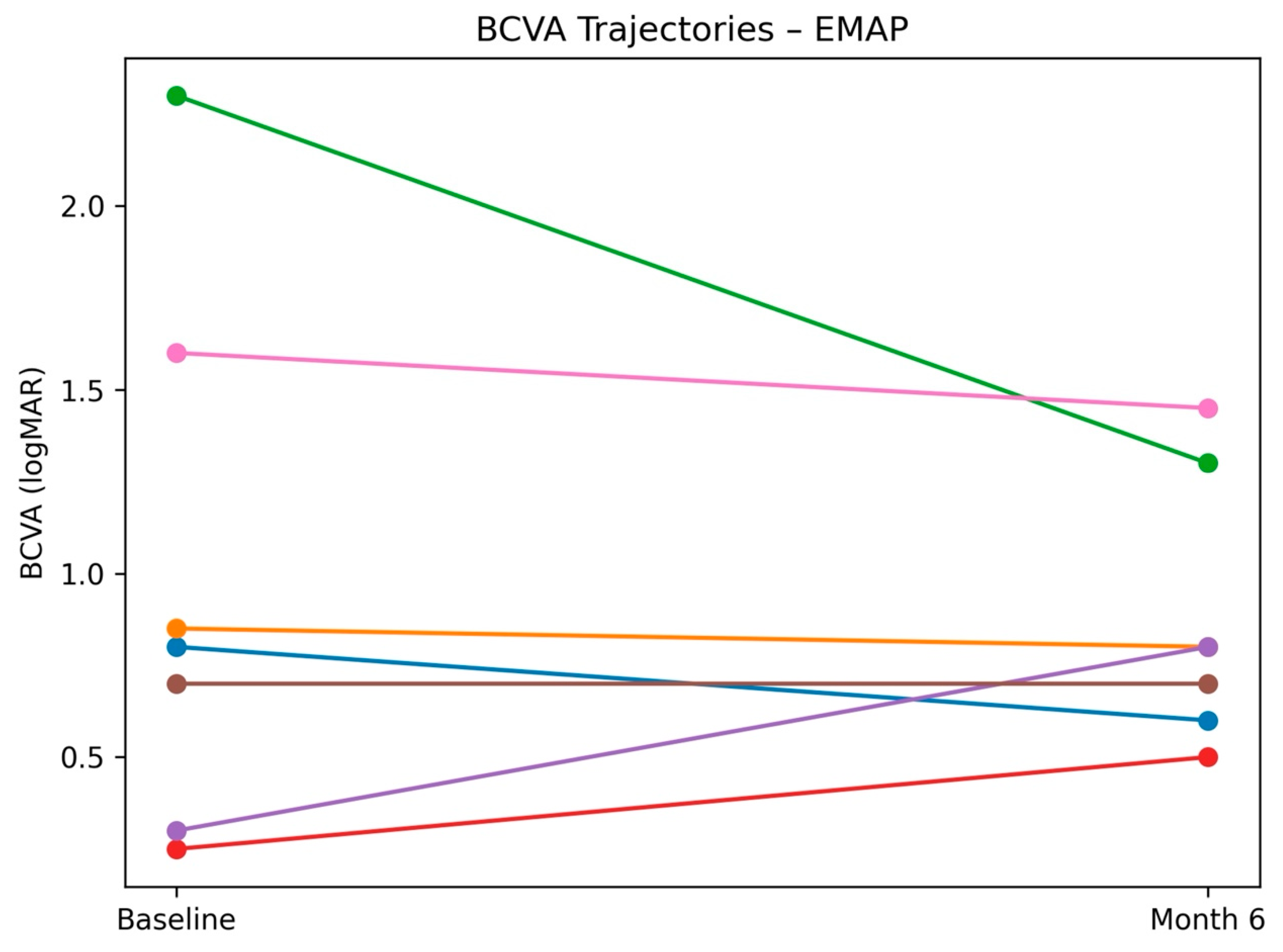
Figure 3.
Boxplot showing the distribution of changes in best-corrected visual acuity (ΔlogMAR) from baseline to Month 6 in patients with retinitis pigmentosa and EMAP. Negative values indicate improvement in visual acuity. The horizontal dashed line represents no change from baseline.
Figure 3.
Boxplot showing the distribution of changes in best-corrected visual acuity (ΔlogMAR) from baseline to Month 6 in patients with retinitis pigmentosa and EMAP. Negative values indicate improvement in visual acuity. The horizontal dashed line represents no change from baseline.
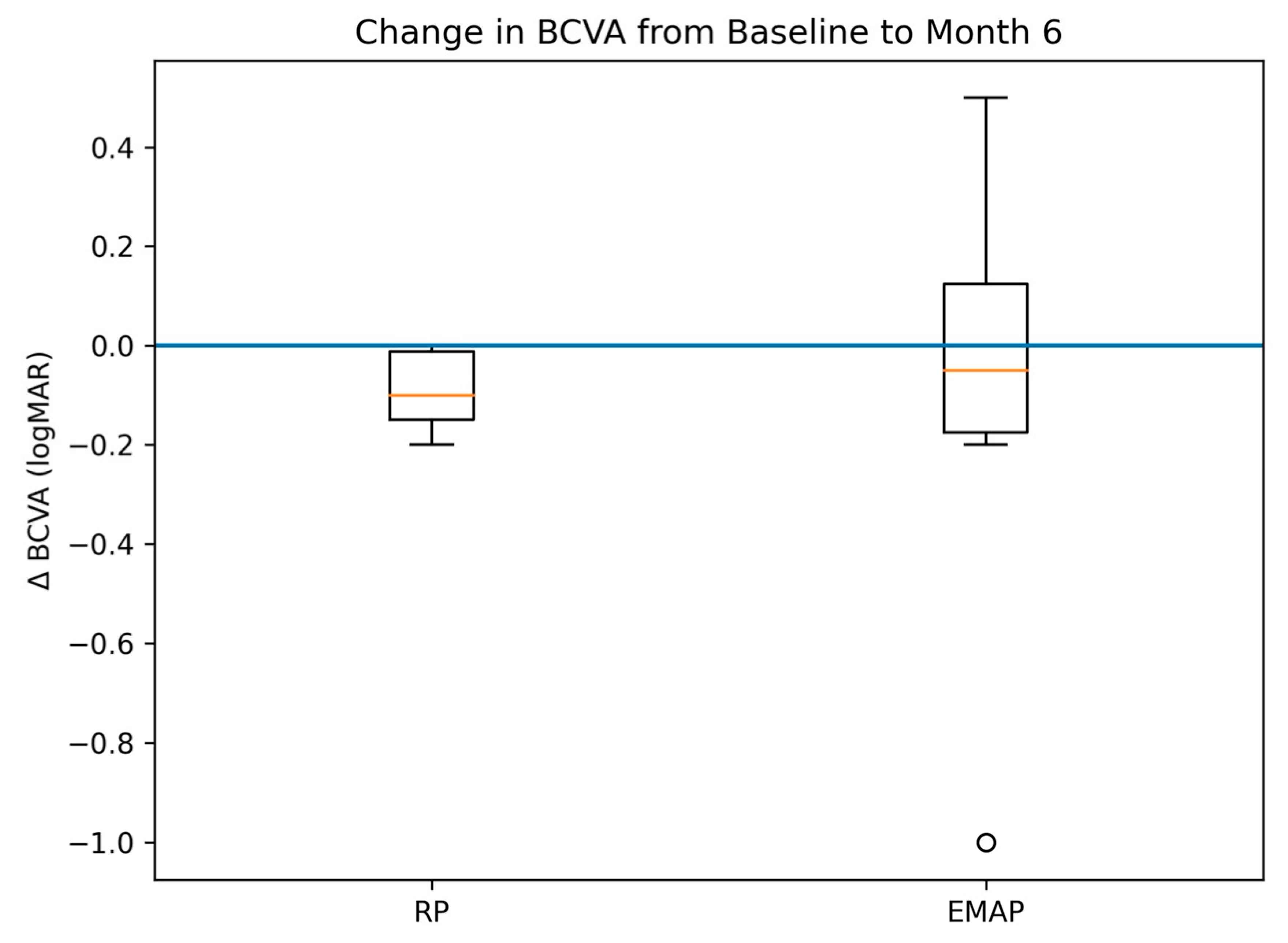
Figure 4.
Visual field preservation indices before and after subtenon autologous platelet-rich plasma injections, stratified by diagnosis. Bars represent mean values of the Field Preservation Deviation Index (FPDI), or Visual Field Index (VFI) when FPDI was unavailable, at baseline and at Month 6, derived from automated perimetry (iCare COMPASS).
Figure 4.
Visual field preservation indices before and after subtenon autologous platelet-rich plasma injections, stratified by diagnosis. Bars represent mean values of the Field Preservation Deviation Index (FPDI), or Visual Field Index (VFI) when FPDI was unavailable, at baseline and at Month 6, derived from automated perimetry (iCare COMPASS).
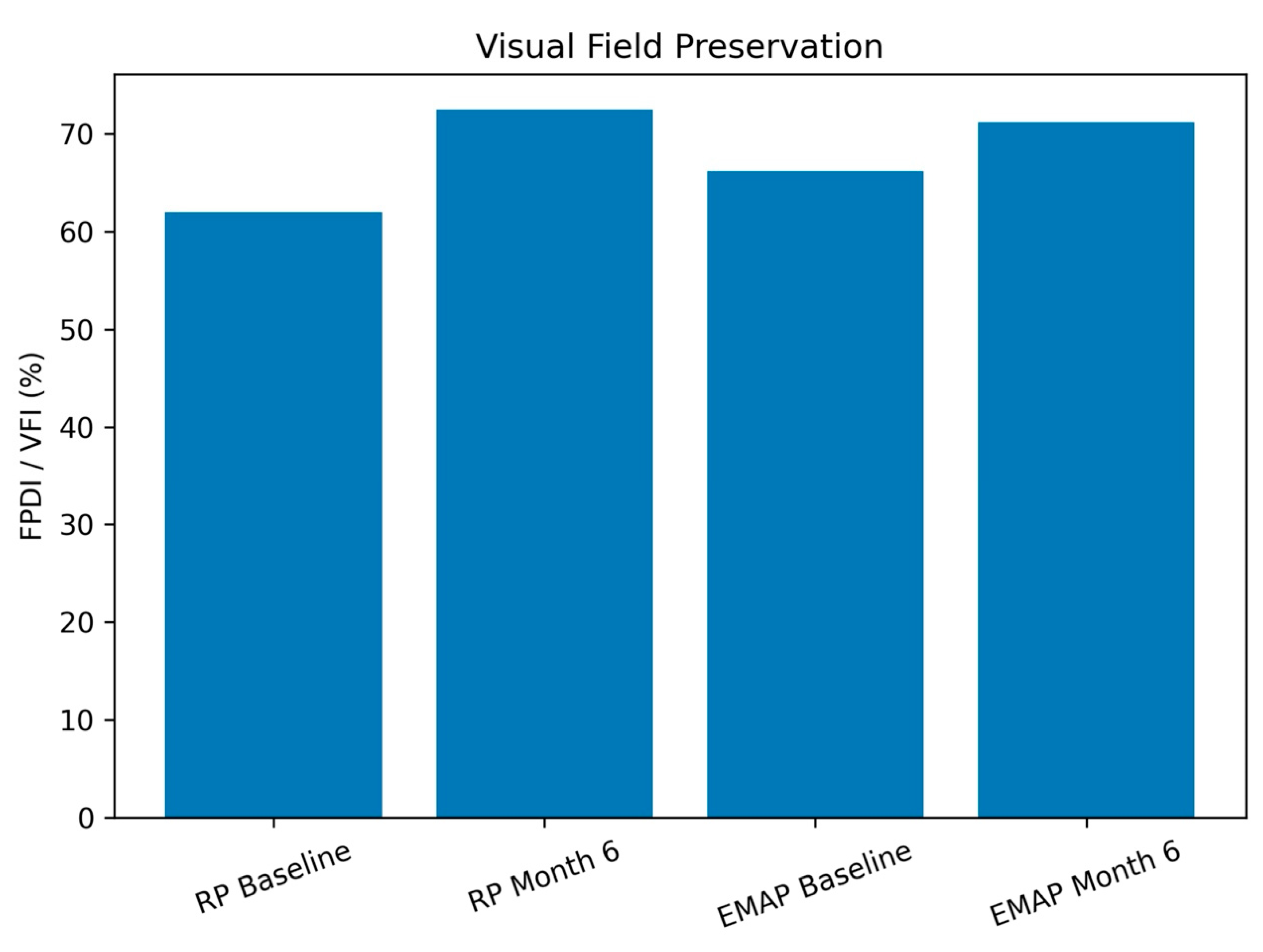
Figure 5.
Proposed mechanistic model of subtenon autologous platelet-rich plasma (PRP) in degenerative retinal diseases. PRP-derived growth factors and cytokines may modulate inflammatory signaling, support photoreceptor survival, and enhance retinal homeostasis. Functional benefits are more evident in conditions with residual retinal plasticity, such as retinitis pigmentosa, whereas stabilizing effects predominate in aggressive macular atrophic phenotypes such as EMAP.
Figure 5.
Proposed mechanistic model of subtenon autologous platelet-rich plasma (PRP) in degenerative retinal diseases. PRP-derived growth factors and cytokines may modulate inflammatory signaling, support photoreceptor survival, and enhance retinal homeostasis. Functional benefits are more evident in conditions with residual retinal plasticity, such as retinitis pigmentosa, whereas stabilizing effects predominate in aggressive macular atrophic phenotypes such as EMAP.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



